Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Aarti Narayan, M.B.B.S [3]; Raviteja Guddeti, M.B.B.S. [4] Sahar Memar Montazerin, M.D.[5]
Overview
Overview
A CT scan can be used to diagnose aortic dissection if neither a TEE nor MRI is available in a timely fashion, or if there is a contraindication to their performance. An example would be after hours in an emergency room setting. If the results of the CT scan are non-diagnostic, then TEE or MRI should be performed to confirm the diagnosis.
CT
CT
Computed Tomography Angiography (CTA)
- Computed tomography angiography is a fast non-invasive test that will give an accurate three-dimensional view of the aorta. These images are produced by taking rapid thin cut slices of the chest and abdomen, and combining them in the computer to create cross-sectional slices.
- In order to delineate the aorta to the accuracy necessary to make the proper diagnosis, an iodinated contrast material is injected into a peripheral vein. Contrast is injected and the scan performed using a Bolus Tracking method. This is a type of scan timed to an injection, in order to capture the contrast as it enters the aorta.
- The scan will then follow the contrast as it flows though the vessel.
Differentiating a True Lumen from a False Lumen
CT Examples of Aortic dissection
CT Examples of Aortic dissection
Type A Dissection
-
Aortic dissection Type Stanford A
-
-
Another example of Stanford A type dissection
[1]
-
Aortic dissection Type Stanford A
[2]
-
Type B Dissection
2022ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the Diagnosis and Management of Patients with Thoracic Aortic Disease[4]
2022ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the Diagnosis and Management of Patients with Thoracic Aortic Disease[4]
Recommendations for HTAD: Genetic Testing and Screening of Family Members for TAD Referenced studies that support the recommendations are summarized in the Online Data Supplement
| Class I
|
| 4. In patients with TAD who have a pathogenic/likely pathogenic variant, genetic testing of at-risk biological relatives (ie, cascade testing) is recommended.6,10,11 In family members who are found by genetic screening to have inherited the pathogenic/likely pathogenic variant, aortic imaging with TTE (if aortic root and ascending aorta are adequately visualized, otherwise with CT or MRI) is recommended.(Level of Evidence: B-NR)
5. In a family with aortic root/ascending aortic aneurysms or aortic dissection, if the disease-causing variant is not identified with genetic testing, screening aortic imaging (as per recommendation 4) of at-risk biological relatives (ie, cascade testing) is recommended.(Level of Evidence: B-NR)
6. In patients with aortic root/ascending aortic aneurysms or aortic dissection, in the absence of either a known family history of TAD or pathogenic/likely pathogenic variant, screening aortic imaging (as per recommendation 4) of first-degree relatives is recommended.(Level of Evidence: C-LD)
7. In patients with acute type A aortic dissection, the diameter of the aortic root and ascending aorta should be recorded in the operative note and medical record to inform the management of affected relatives.(Level of Evidence: C-EO)
|
Recommendations for Aortic Imaging Techniques to Determine Presence and Progression of Aortic Disease Referenced studies that support the recommendations are summarized in the Online Data Supplement
| Class I
|
| 1.In patients with known or suspected aortic disease, when performing CT or MR imaging, it is recommended that the root and ascending aortic diameters be measured from inner-edge to inner-edge, using an electrocardiographic-synchronized technique. If there are aortic wall abnormalities, such as atherosclerosis or discrete wall thickening (more common in the distal aorta), the outer-edge to outer-edge diameter should be reported (Level of Evidence: C-EO)
|
Recommendations for Inflammatory Aortitis: Diagnosis and Treatment of Takayasu Arteritis and GCA Referenced studies that support the recommendations are summarized in the Online Data Supplement
| Class I
|
| 1.In patients with large vessel vasculitis (LVV), prompt evaluation of the entire aorta and branch vessels with MRI or CT, with or without 18F-FDG positron emission tomography (FDG-PET), is recommended.(Level of Evidence: C-LD)
|
Recommendations for Long-Term Surveillance Imaging After Aortic Dissection and IMH Referenced studies that support the recommendations are summarized in the Online Data Supplement
| Class I
|
| 1. In patients who have had an acute aortic dissection and IMH treated with either open or endovascular aortic repair and have residual aortic disease, surveillance imaging with a CT (or MRI) is recommended after 1 month, 6 months, and 12 months and then, if stable, annually thereafter.(Level of Evidence: B-NR)
2. In patients who have had an acute aortic dissection and IMH that was managed with medical therapy alone, surveillance imaging with a CT (or MRI) is recommended after 1 month, 6 months, and 12 months and then, if stable, annually thereafter.(Level of Evidence: B-NR)
|
2014 ESC Guidelines on the Diagnosis and Treatment of Aortic Diseases (DO NOT EDIT)[5]
2014 ESC Guidelines on the Diagnosis and Treatment of Aortic Diseases (DO NOT EDIT)[5]
Diagnostic Value of Computed Tomography in Aortic Dissection
| Class I
|
| “In unstabled patients with a suspicion of AAS, the following imaging modalities are recommended according to local availability and expertise:transoesophageal echocardiography; CT scan.(Level of Evidence: C)”
|
| “In stable patients with a suspicion of AAS, the following imaging modalities are recommended (or should be considered) according to local availability and expertise:CT scan; MRI.(Level of Evidence: C)”
|
Follow-up Imaging study
| Class I
|
| “In case of initially negative imaging with persistence of suspicion of AAS, repetitive imaging (CT or MRI) is recommended.(Level of Evidence: C)”
|
| “In case of uncomplicated Type B AD treated medically, repeated imaging (CT or MRI) during the first days is recommended. (Level of Evidence: C)”
|
2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the Diagnosis and Management of Patients with Thoracic Aortic Disease (DO NOT EDIT) [6]
2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the Diagnosis and Management of Patients with Thoracic Aortic Disease (DO NOT EDIT) [6]
Screening Tests (DO NOT EDIT)[6]
Determining the Presence and Measuring the Progression of Thoracic Aortic Disease (DO NOT EDIT)[6]
Takayasu Arteritis and Giant Cell Arteritis (DO NOT EDIT) [6]
Surveillance of Thoracic Aortic Disease or Previously Repaired Patients (DO NOT EDIT)[6]
References
References
- ↑ Case courtesy of A.Prof Frank Gaillard, Radiopaedia.org, rID: 8886
- ↑ Case courtesy of Dr Craig Hacking, Radiopaedia.org, rID: 34693
- ↑ Case courtesy of Prof Cláudio Souza, Radiopaedia.org, rID: 13783
- ↑ Isselbacher EM, Preventza O, Black JH, Augoustides JG, Beck AW, Bolen MA; et al. (2022). “2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines”. Circulation. doi:10.1161/CIR.0000000000001106. PMID 36322642 .
- ↑ Erbel R, Aboyans V, Boileau C, Bossone E, Bartolomeo RD, Eggebrecht H, Evangelista A, Falk V, Frank H, Gaemperli O, Grabenwöger M, Haverich A, Iung B, Manolis AJ, Meijboom F, Nienaber CA, Roffi M, Rousseau H, Sechtem U, Sirnes PA, Allmen RS, Vrints CJ (November 2014). “2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC)”. Eur. Heart J. 35 (41): 2873–926. doi:10.1093/eurheartj/ehu281. PMID 25173340.
- ↑ 6.0 6.1 6.2 6.3 6.4 Hiratzka LF, Bakris GL, Beckman JA; et al. (2010). “2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine”. Circulation. 121 (13): e266–369. doi:10.1161/CIR.0b013e3181d4739e. PMID 20233780.
Template:WH
Template:WS
CME Category::Cardiology

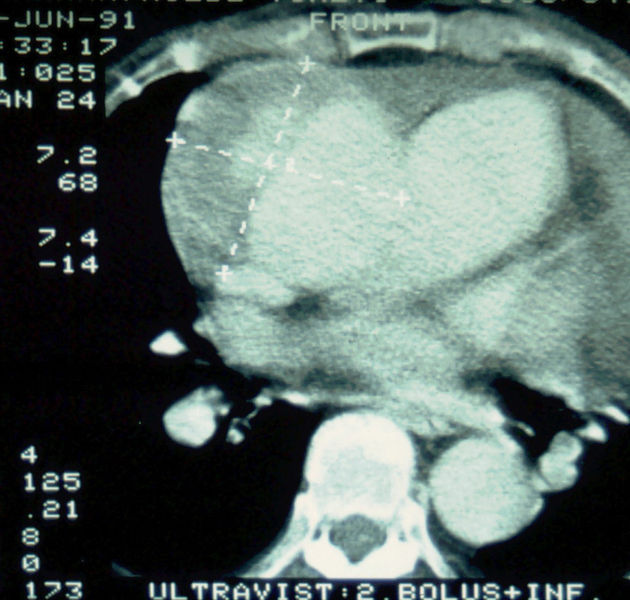 Aortic dissection Type Stanford A
Aortic dissection Type Stanford A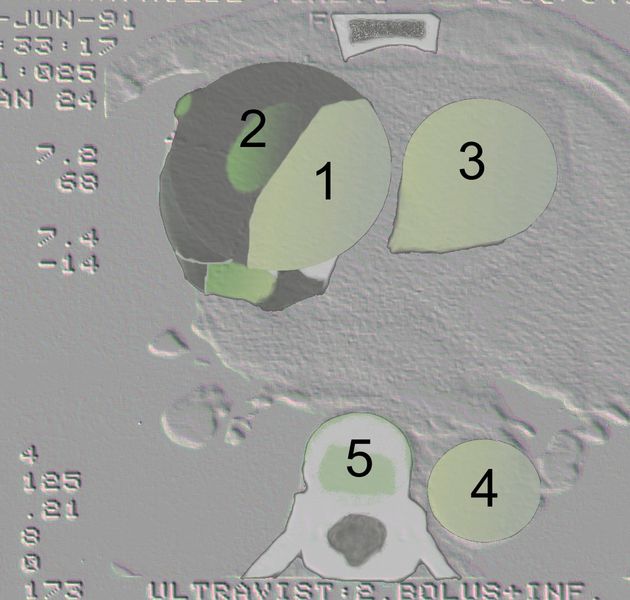 Aortic dissection Type Stanford A – ‘1 Aorta ascendens, true Lumen – 2 false lumen – 3 Pulmonary artery – 4 Aorta descendens – 5 thoracic vertebra
Aortic dissection Type Stanford A – ‘1 Aorta ascendens, true Lumen – 2 false lumen – 3 Pulmonary artery – 4 Aorta descendens – 5 thoracic vertebra![Another example of Stanford A type dissection[1]](https://www.wikidoc.org/images/b/be/Type-a-dissection-ct.jpg) Another example of Stanford A type dissection[1]
Another example of Stanford A type dissection[1]![Aortic dissection Type Stanford A[2]](https://www.wikidoc.org/images/e/eb/Type-a-aortic-dissection-4.png)
![[3]](https://www.wikidoc.org/images/5/5f/Aortic-dissection-debakey-type-1.jpg)


![Another example of Stanford A type dissection[1]](https://www.wikidoc.org/index.php/File%3AType-a-dissection-ct.jpg)
![Aortic dissection Type Stanford A[2]](https://www.wikidoc.org/index.php/File%3AType-a-aortic-dissection-4.png)
![[3]](https://www.wikidoc.org/index.php/File%3AAortic-dissection-debakey-type-1.jpg)






