
Cardiac tumors pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Varun Kumar, M.B.B.S. Dheeraj Makkar, M.D.[3]
Overview
Overview
The precise pathophysiology of cardiac tumors is unknown. Some cardiac tumors are associated with genetic predispositions or are components of genetic disorders.
- Cardiac rhabdomyomas are associated with Tuberous sclerosis, an autosomal dominant condition characterized by the development of various organ hamartomas.
- Cardiac fibromas may be associated with Gorlin syndrome, an autosomal dominant condition marked by congenital abnormalities and a propensity for neoplasia.
- Cardiac myxomas may be associated with the autosomal dominant condition Carney complex.
- Histiocytoid cardiomyopathy is sometimes inherited, however the underlying genetic disorders remain unknown.
- Most cardiac undifferentiated sarcomas share the same genetic profile as pulmonary artery intimal sarcomas, characterized by recurrent mutations in the MDM2, PDGFRA, and CDKN2A genes.
- There have been reports of papillary fibroelastomas following cardiac instrumentation and thoracic irradiation.
Pathophysiology
Pathophysiology
| Tumor | Macroscopic appearance | Microscopic appearance | Remarks |
|---|---|---|---|
| Myxoma(Images B, C) | Two Types Solid(round with a smooth, lustrous, undulating surface)/Villous(frequently fragile papillary surfaces) | Cells have eosinophilic cytoplasm and an oval or round nucleus. | Embolization is frequent.[1] |
| Cardiac Lipoma | Isolated lumps that are yellow, soft, smooth, well-circumscribed, and encapsulated | Fat cells exhibit minimal to no atypia, fibrous capsule | They can cause arrhythmias or conduction system disorders and heart failure symptoms.[2] |
| Papillary fibroelastoma(Images F,G) | Round, whitish appearance and soft consistency, sea anemone-like” appearance[3] | Thin avascular papillary fronds that frequently display complicated branching | Embolization is frequent.
|
| Rhabdomyomas | Nodular, unencapsulated, whitish, or grey, range in size from millimeters to several centimeters | Large vacuolated cells with transparent cytoplasm due to glycogen deposition, spider cells also present | Heart block or ventricular tachyarrhythmias, ventricular tachyarrhythmias may develop[4]
|
| Cardiac Fibromas(Image D) | Solitary well-defined formation, | Monomorphic fibroblasts exhibiting minimal or no atypia *Resembles fibromatosis or uterine leiomyomas | May manifest like heart failure, ventricular tachyarrhythmia, Can present as Sudden Cardiac Death[5]
|
| Angiosarcoma | Darkish brown or black hemorrhagic aggregates with invading margins | Vascular conduits, infiltrating cardiac muscle, anastomosing, uneven, *Pleomorphic lining cells displaying numerous mitotic figures[6] | Most commonly involves right atrium |
| Secondary Cardiac Tumors(Image A) | Direct tumor infiltration from the mediastinum or hematogenous spread[7] | Same as underlying Malignancy | Pericardial effusion is one of the most frequent findings in individuals with secondary tumors.
|
Papillary fibroelastoma
- Primary tumor of the heart that typically involves one of the valves of the heart
- Papillary fibroelastoma is generally considered benign, and represents 10% of all primary tumors of the heart
- Papillary fibroelastoma are the third most common type of primary tumor of the heart, behind cardiac myxomas and cardiac fibromas.[8]
- The pathogenesis of papillary fibroelastoma is characterised by the mechanical effects of the tumor and the transient occlusion of the left main coronary artery (by the tumor), while a heart attack or sudden cardiac death may be due to embolisation of a portion of the tumor into a coronary artery.[9]
Gross Pathology
Image shown below is courtesy of Professor Peter Anderson DVM PhD and published with permission. © PEIR, University of Alabama at Birmingham, Department of Pathology
-
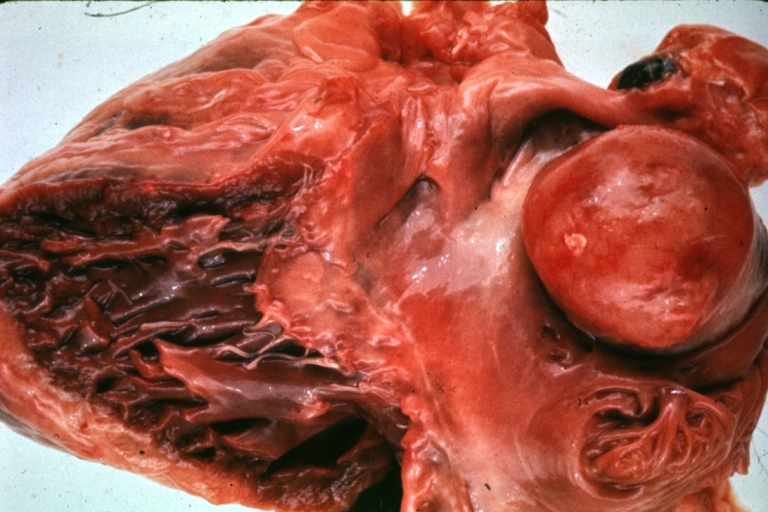 Image A HEART: Metastatic Tumor: Gross very unusual large metastatic carcinoid in right atrium
Image A HEART: Metastatic Tumor: Gross very unusual large metastatic carcinoid in right atrium -
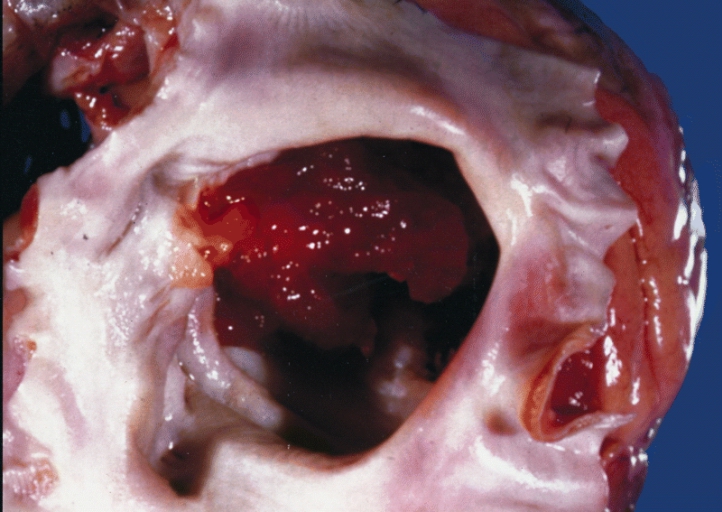 Image B Cardiac Myxoma A gelatinous tumor is attached by a narrow pedicle to the atrial septum. The myxoma has an irregular surface and nearly fills the left atrium.
Image B Cardiac Myxoma A gelatinous tumor is attached by a narrow pedicle to the atrial septum. The myxoma has an irregular surface and nearly fills the left atrium.


-
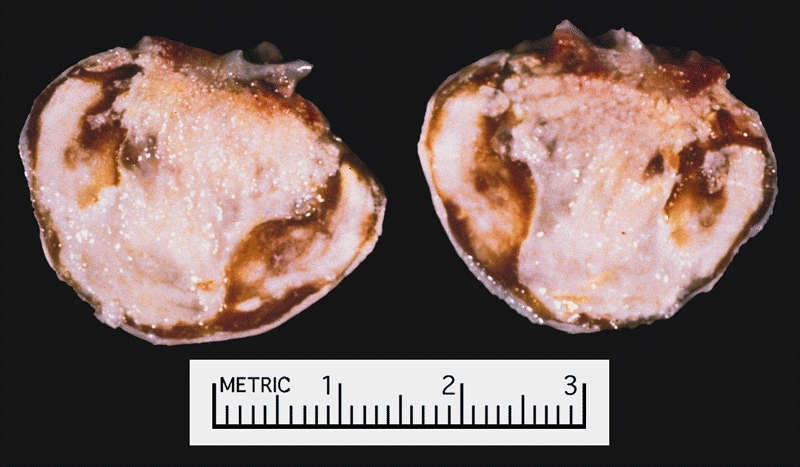 Image C Cardiac Myxoma There was a calcified right atrial mass on the X ray of a 47-year-old man. Resection demonstrated a smooth-surfaced tumor. The gritty material seen microscopically on cut section was calcified and ossified myxoma.
Image C Cardiac Myxoma There was a calcified right atrial mass on the X ray of a 47-year-old man. Resection demonstrated a smooth-surfaced tumor. The gritty material seen microscopically on cut section was calcified and ossified myxoma. -
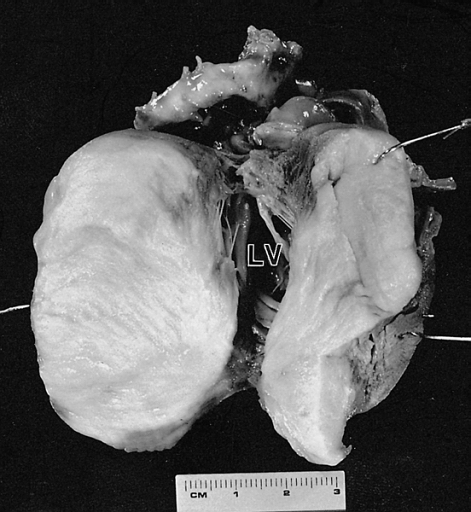 Image D Cardiac Fibroma Cut surface of the tumor shown in figure 6-2. The left ventricular (LV) cavity is present behind the mass. The patient was a 4-month-old child who died suddenly without a previous medical history.
Image D Cardiac Fibroma Cut surface of the tumor shown in figure 6-2. The left ventricular (LV) cavity is present behind the mass. The patient was a 4-month-old child who died suddenly without a previous medical history.


-
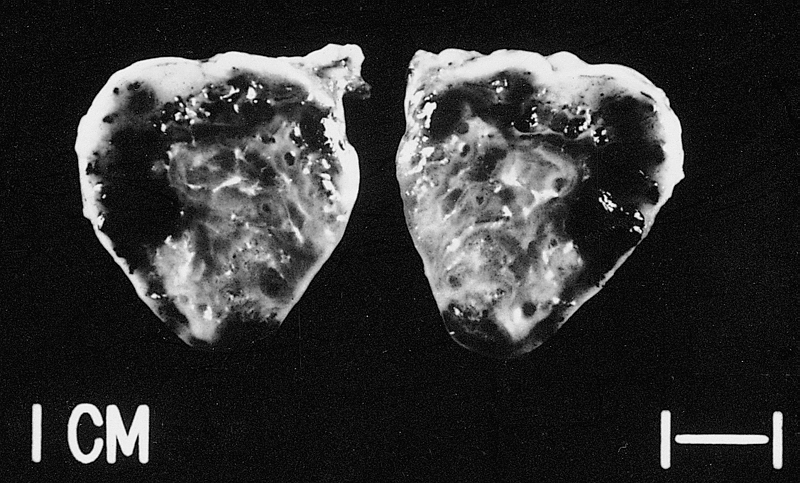 Image E This tumor was resected from the right atrium of a 1-year-old boy with pericardial effusions. Note areas of hemorrhage and dilated vessels. The patient was well 49 months postoperatively.
Image E This tumor was resected from the right atrium of a 1-year-old boy with pericardial effusions. Note areas of hemorrhage and dilated vessels. The patient was well 49 months postoperatively. -
 Image F Papillary fibroelastomas are often on the arterial surface and may project into the coronary ostium, causing ostial occlusion. This tumor is in the noncoronary sinus.
Image F Papillary fibroelastomas are often on the arterial surface and may project into the coronary ostium, causing ostial occlusion. This tumor is in the noncoronary sinus. -
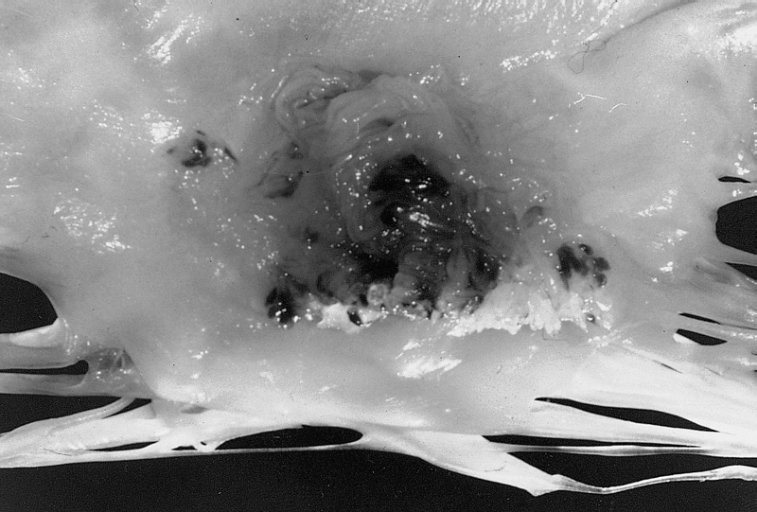 Image G Papillary Fibroelastoma: When located on the mitral valve, these tumors are usually on the anterior leaflet of the atrial surface.
Image G Papillary Fibroelastoma: When located on the mitral valve, these tumors are usually on the anterior leaflet of the atrial surface.



References
References
- ↑ Pinede L, Duhaut P, Loire R (2001). “Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases”. Medicine (Baltimore). 80 (3): 159–72. doi:10.1097/00005792-200105000-00002. PMID 11388092.
- ↑ Benvenuti LA, Mansur AJ, Lopes DO, Campos RV (1996). “Primary lipomatous tumors of the cardiac valves”. South Med J. 89 (10): 1018–20. doi:10.1097/00007611-199610000-00020. PMID 8865802.
- ↑ Burke A, Tavora F (2016). “The 2015 WHO Classification of Tumors of the Heart and Pericardium”. J Thorac Oncol. 11 (4): 441–52. doi:10.1016/j.jtho.2015.11.009. PMID 26725181.
- ↑ Basso C, Valente M, Poletti A, Casarotto D, Thiene G (1997). “Surgical pathology of primary cardiac and pericardial tumors”. Eur J Cardiothorac Surg. 12 (5): 730–7, discussion 737-8. doi:10.1016/s1010-7940(97)00246-7. PMID 9458144.
- ↑ Pacini D, Careddu L, Pantaleo A, Berretta P, Leone O, Marinelli G; et al. (2012). “Primary benign cardiac tumours: long-term results”. Eur J Cardiothorac Surg. 41 (4): 812–9. doi:10.1093/ejcts/ezr067. PMID 22219403.
- ↑ Orlandi A, Ferlosio A, Roselli M, Chiariello L, Spagnoli LG (2010). “Cardiac sarcomas: an update”. J Thorac Oncol. 5 (9): 1483–9. doi:10.1097/JTO.0b013e3181e59a91. PMID 20651614.
- ↑ Fred HL, van Dijk HA (2017). “Cardiac Metastases from Malignant Melanoma: The “Charcoal Heart““. Methodist Debakey Cardiovasc J. 13 (4): 254–255. doi:10.14797/mdcj-13-4-254. PMC 5935287. PMID 29744020.
- ↑ Matsumoto N, Sato Y, Kusama J, Matsuo S, Kinukawa N, Kunimasa T, Ichiyama I, Takahashi H, Kimura S, Orime Y, Saito S. (2007). “Multiple papillary fibroelastomas of the aortic valve: case report”. Int J Cardiol. 122 (1): e1–3. PMID 17196273.
- ↑ Takada A, Saito K, Ro A, Tokudome S, Murai T. (2000). “Papillary fibroelastoma of the aortic valve: a sudden death case of coronary embolism with myocardial infarction”. Forensic Sci Int. 113 (1–3): 209–14. PMID 10978627.
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH