
Cerebral hypoxia
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
For patient information, click here.
Synonyms and keywords: Hypoxic encephalopathy; anoxic encephalopathy
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Please help WikiDoc by adding content here. It’s easy! Click here to learn about editing.
Overview
Cerebral hypoxia refers to deprivation of oxygen supply to brain tissue. Mild or moderate cerebral hypoxia is sometimes known as diffuse cerebral hypoxia. It can cause confusion and fainting, but its effects are reversible. Total deprivation of oxygen to the brain is called cerebral anoxia. Extended periods of cerebral hypoxia can lead to brain death or permanent brain damage.
Most cases of cerebral hypoxia are caused by a sudden change in brain oxygen levels. The body can normally respond to mild gradual changes in blood oxygen with little or no noticeable effect on brain function. The acclimatization process used by high altitude climbers is an example of such adjustment.
The presence of cerebral hypoxia symptoms indicates that the brain has been overwhelmed by a change in its oxygen supply. Consequently, even mild symptoms of cerebral hypoxia require immediate medical attention.
References
Historical Perspective
Overview
The relationship between brain function and blood flow has been studied since the classical paper of Roy and Sherrington (61) at the end of the 19th century.
Historical Perspective
- Despite the absence of quantitative methods, early investigators were able to establish some of the basic principles of the cerebral circulation; among these was a recognition of the dominating influence of carbon dioxide and the reciprocal effect of oxygen (72).
- Interestingly, even the idea that local cerebral blood flow (CBF) was transiently augmented with increased neuronal activation, alluded to by Roy and Sherrington, had received additional qualitative experimental support.
- A listing of the qualitative methods in use at the time, including methods such as venous outflow, radium emanation, and thermocouple, can be found in the 1936 Wolff review (72).
- Nevertheless, despite more than 100 years of effort, there are still major areas concerning the control of the cerebral circulation that remain unknown.
- The observations that decreasing oxygen led to increased blood flow and that the increase was blunted perhaps by the accompanying hypoxia-induced hyperventilation and resultant decreased carbon dioxide remained wholly qualitative until a useful quantitative method, based on inert gases, was developed for measuring CBF and oxygen metabolism by Kety and Schmidt (33, 35).
References
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Please help WikiDoc by adding content here. It’s easy! Click here to learn about editing.
Classification
Cerebral hypoxia is typically grouped into four categories depending on the severity and location of the brain’s oxygen deprivation:[1]
- Diffuse cerebral hypoxia: A mild to moderate impairment of brain function due to low oxygen levels in the blood.
- Focal cerebral ischemia: A small localized reduction in the flow of oxygen from the blood to the brain. Damage to neurons is usually irreversible. Mild strokes.
- Cerebral infarction: A complete stoppage of the flow of oxygen from the blood to a region of the brain. Significant irreversible brain damage occurs in the region around the blockage. Major strokes are an example of cerebral infarction.
- Global cerebral ischemia: A complete stoppage of blood flow to the brain.
Cerebral hypoxia can also be classified by the cause of the reduced brain oxygen:[2]
- Hypoxic hypoxia: Hypoxic hypoxia occurs when limited oxygen in the environment causes reduced brain function. Divers, aviators,[3] mountain climbers and fire fighters are all at risk for this kind of cerebral hypoxia. The term also includes oxygen deprivation due to obstructions in the lungs. Choking, strangulation, the crushing of the windpipe all cause this sort of hypoxia. Severe asthmatics may also experience symptoms of hypoxic hypoxia.
- Hypemic hypoxia: Reduced brain function is caused by inadequate oxygen in the blood despite adequate environmental oxygen. Anemia and carbon monoxide poisoning are common causes of hypemic hypoxia.
- Ischemic hypoxia (a.k.a. stagnant hypoxia): Reduced brain oxygen is caused by inadequate blood flow to the brain. Stroke, shock, and heart attacks are common causes of stagnant hypoxia. Ischemic hypoxia can also be created by pressure on the brain. Cerebral edema, brain hemorrhages and hydrocephalus exert pressure on brain tissue and impede their absorption of oxygen.
- Histotoxic hypoxia: Histotoxic hypoxia is when oxygen is present in brain tissue, but cannot be metabolized. Cyanide poisoning is a well known example.
References
- ↑ “Hypoxia”. The Gale Encyclopedia of Neurological Disorders. The Gale Group, Inc. 2005. Retrieved on 2007-04-13 from Answers.com.
- ↑ “What is Hypoxia?”. Gray Laboratory Cancer Research Trust. August 1, 1999. Retrieved on 2007-04-13 from Archive.org.
- ↑ Brooks, Kevin E. (May–June 2005). “Are you a hypoxia expert?”. Approach. United States Navy Naval Safety Center. Retrieved 2007-04-13. This website provides hypoxia related safety tips for aviators working for the United States Navy aviators.
Pathophysiology
Overview
The brain consumes significant amount of the energy compared to its size and weight. Cellular injury can begin within minutes, and permanent brain injury will follow if prompt intervention does not occur.
Pathophysiology
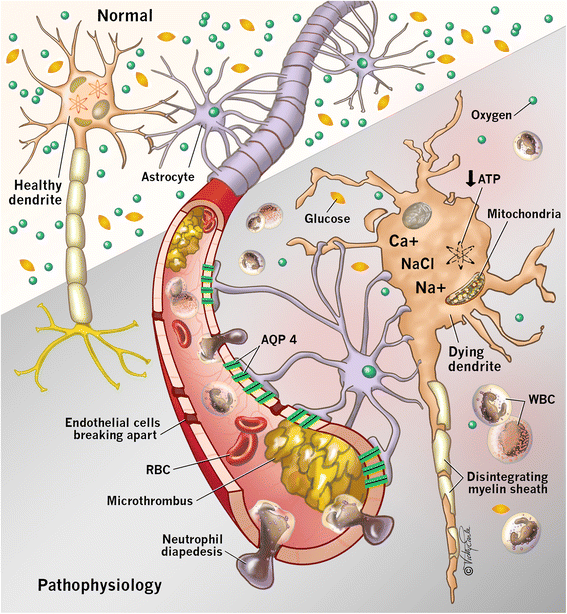
- The brain depends on a constant energy supply provided by glucose and oxygen but is unable to store energy. With the cessation of blood flow, intracellular production of adenosine triphosphate is diminished. This results in dysfunction of energy-dependent ion channels, which contributes to intracellular sodium accumulation and cytotoxic edema. Ongoing ischemia results in the release of glutamate, an excitatory neurotransmitter, which promotes calcium influx through N-methyl-D-aspartate (NMDA) receptors. Calcium influx exacerbates neuronal injury by activating lytic enzymes, precipitating free radical formation, and interfering with mitochondrial function. This process, known as excitotoxicity, can ultimately lead to cell death. [6][7]
Histopathology
- The mechanisms that lead to delayed cell death following hypoxic-ischemic injury in the brain are complex. Ischemic cell death occurs via two different pathways: necrosis and apoptosis. During hypoxia-ischemia of the brain, acute energy failure leads to loss of ion homeostasis where intracellular sodium and calcium accumulate creating osmotic swelling which, can lead to cell lysis.[8]
- This process releases glutamate and free radicals which are cytotoxic and exacerbate the injury. A secondary phase of neuronal death can occur hours later. Moderate global ischemia leads to infarcts in watershed areas (e.g., the area lying between regions fed by the anterior and middle cerebral artery).
- These infarcts can damage the highly vulnerable areas such as pyramidal neurons of the hippocampus (CA1 region), pyramidal neurons of the cerebral cortex (layers 3, 5, and 6) which leads to laminar necrosis, the death of neurons in the basal ganglia (caudate nucleus and putamen), and the Purkinje cell layer of the cerebellum.[9]
- The cells of these areas are high in metabolic demand and contain a high concentration of excitatory neurotransmitter receptors.
- Other histologic findings include a shrunken eosinophilic neuron (anoxic neuron) and a red neuron which represents neuronal cells that die because of hypoxia.
Pathophysiology

References
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Causes
Cerebral hypoxia can be caused by any event that severely interferes with the brain’s ability to receive or process oxygen. This event may be internal or external to the body.
Mild and moderate forms of cerebral hypoxia may be caused by various diseases that interfere with breathing and blood oxygenation. Severe asthma and various sorts of anemia can cause some degree of diffuse cerebral hypoxia. Other causes include work in nitrogen rich environments, ascent from a deep water dive, flying at high altitudes in an un-pressurized cabin, and intense exercise at high altitudes prior to acclimatization.Severe cerebral hypoxia and anoxia is usually caused by traumatic events. Examples include choking, drowning, strangulation, smoke inhalation, drug overdoses, crushing of the trachea, status asthmaticus, and shock.[1]
It is also recreationally self-induced in the choking game and in autoerotic asphyxiation.
References
- ↑ National Institute of Neurological Disorders and Stroke (February 8, 2007). “Cerebral Hypoxia Information Page”. U.S. National Institutes of Health. Retrieved 2007-04-13.
Differentiating Cerebral hypoxia from other Diseases
Overview
The following conditions should be ruled out while making diagnosis of cerebral hypoxia
Differential Diagnosis
- Epidural Hemorrhage
- Ischemic Stroke
- Seizure or Post-Ictal State
- Subarachnoid Hemorrhage
- Subdural Hemorrhage
- Traumatic Brain Injury
References
Risk Factors
Overview
The risk factors for cerebral hypoxia are vast. All these risk factors lead to interruption of blood flow to the brain.
Risk Factors
- Anoxic and hypoxic brain injury can occur whenever oxygen delivery to the brain is compromised.
- Oxygen delivery is a function of the blood flow to the brain and the oxygen content of the blood.[1]
- Consequently, hypoxic brain injury can result from interruption of blood flow to the brain, such as cardiac arrest or strangulation, or from systemic derangements that affect the oxygen content of the blood.
- Severe anemia, systemic hypotension, and systemic hypoxia can result in hypoxic brain injury if left untreated.
- In the United States, cardiac arrest is the most common cause of hypoxic brain injury.
Other Causes:
- Traumatic vascular injuries
- Drowning
- Smoke inhalation or carbon monoxide poisoning
- Shock, including hemorrhagic and septic shock
- Drug overdoses
- Acute lung injury
References
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Please help WikiDoc by adding more content here. It’s easy! Click here to learn about editing.
Prognosis
Mild and moderate cerebral hypoxia generally has no impact beyond the episode of hypoxia. Severe cerebral hypoxia is another matter. Outcome will depend on the success of damage control measures, the amount of brain tissue deprived of oxygen, and the speed with which oxygen was restored to the brain.
If cerebral hypoxia was localized to a specific part of the brain, brain damage will be localized to that region. The long term effects will depend on the purpose of that portion of the brain. Damage to the Broca and Wernicke’s areas of the brain (left side) typically causes problems with speech and language. Damage to the right side of the brain may interfere with the ability to express emotions or interpret what one sees. Damage on either side can cause paralysis of the opposite side of the body.
The effects of certain kinds of severe generalized hypoxias may take time to develop. For example, the long term effects of serious carbon monoxide poisoning usually may take several weeks to appear. Recent research suggests this may be due to an autoimmune response caused by CO induced changes in the myelin sheath surrounding neurons.[1]
If hypoxia results in coma, the length of unconsciousness is often used as an indication of long term damage. In some cases coma can give the brain an opportunity to heal and regenerate,[2] but, in general, the longer a coma continues the greater the likelihood that the person will remain in a vegetative state until death. Even if the patient wakes up, brain damage is likely to be significant enough to prevent a return to normal functioning.
The effects of long term comas are not limited to the comatose person. Long term coma can have significant impact on their families.[3] Families of coma victims often have idealized images of the outcome based on Hollywood movie depictions of coma.[4] Adjusting to the realities of ventilators, feeding tubes, bedsores and muscle wasting may be difficult.[5] Treatment decision often involve complex ethical choices and can strain family dynamics.[6]
References
- ↑ University Of Pennsylvania Medical Center (September 6, 2004). “Long-term Effects Of Carbon Monoxide Poisoning Are An Autoimmune Reaction”. ScienceDaily. Retrieved 2007-04-13.
- ↑ Phillips, Helen (July 3, 2006). “‘Rewired brain’ revives patient after 19 years”. New Scientist. Retrieved 2007-04-13.
- ↑ Mayo Clinic staff (May 17, 2006). “Coma: Coping skills”. Mayo Clinic. Retrieved 2007-04-13.
- ↑ Wijdicks EFM, Wijdicks CA (2006). “The portrayal of coma in contemporary motion pictures”. Neurology 66 (9): 1300–1303. PMID 16682658.
- ↑ Konig P et al (1992). “Psychological counseling of the family of patients with craniocerebral injuries (psychological family counseling of severely ill patients)”. Zentralbl Neurochir 53 (2): 78–84. PMID 1636327.
- ↑ Montgomery V et al (2002). “The effect of severe traumatic brain injury on the family”. J Trauma 52 (6): 1121–4. PMID 12045640.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | EKG | CT | MRI | Echocardiography or Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH