Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-in-Chief: Cafer Zorkun, M.D., Ph.D. [2], Mohammed A. Sbeih, M.D. Anahita Deylamsalehi, M.D.[3]
Overview
Overview
The choice of conduits (arteries and/or veins from elsewhere in the body) to bypass the blockages is highly surgeon and institution dependent. To choose the proper conduits for CABG both clinical and technical factors such as life expectancy, presence of diabetes, chronic renal failure, and degree of the target stenosis must be considered. Saphenous vein, internal thoracic artery, and radial artery are the most used vessels to harvest for grafting. The saphenous vein can be harvested by either direct visualization or via an endoscopic approach. Among these two methods the endoscopic approach has been associated with lower rates of wound infection, greater patient satisfaction, and earlier mobilization. However, non-randomized data from a much larger multicenter study does suggest that endoscopyendoscopic harvesting may be associated with a higher rate of failure and adverse events such as death and MI. Veins that are used either have their valves removed or are turned around so that the valves in them do not occlude blood flow in the graft. On the other hand, numerous studies support the use of the left internal thoracic artery (LITA) (also known as the left internal mammary artery (LIMA)) to graft the LAD in order to improve survival unless contraindicated. Evidence shows that the right IMA can be used to graft the LAD if the LIMA is impractical and unusable. Furthermore, the right IMA can be used in conjunction with the LIMA which is called bilateral internal mammary artery (BIMA) grafting. The latter method showed a better outcome based on multiple studies. In multiple arterial revascularization during Coronary artery bypass surgery, the right internal thoracic artery (RITA) has been proofed to be a better choice as a conduit than the radial artery. On the other hand, numerous clinical trials have demonstrated better patency rates (in mid- and long-term) when the radial artery is used in comparison with the saphenous vein.
Conduits used for bypass
Conduits used for bypass
- The choice of conduits (arteries and/or veins from elsewhere in the body) to bypass the blockages is highly surgeon and institution dependent.
- To choose the proper conduits for CABG both clinical and technical factors such as life expectancy, presence of diabetes, chronic renal failure, and degree of the target stenosis must be considered.[1]
- The following table published by 2021 ACA Revascularization Guideline presents the best practices for the Use of bypass conduits in CABG:[1]
Saphenous vein
Saphenous vein
Saphenous vein anatomy
Saphenous vein harvesting
- The saphenous vein can be harvested by either direct visualization or via an endoscopic approach. Veins that are used either have their valves removed or are turned around so that the valves in them do not occlude blood flow in the graft. The technique of saphenous vein harvesting may influence later SVG patency. The process of harvesting the vein and pressure testing the vein for a leak may damage the endothelium.[2][3]
- The endoscopic approach has been associated with lower rates of wound infection, greater patient satisfaction, and earlier mobilization.[4][5][6][7] One small randomized study of 144 patients showed no difference in histologic findings between the traditional and endoscopic techniques.[4]In another small study of 40 patients randomized to the two techniques, no difference was seen in angiographic patency at 3 months.[7]Another small randomized study of 144 patients who returned for angiography demonstrated an occlusion rate of 21.7% for the endoscopic approach vs 17.6% for the open approach.[6]
- However, non-randomized data from a much larger multicenter study does suggest that endoscopyendoscopic harvesting may be associated with a higher rate of failure and adverse events such as death and MI.[5]
- Complications associated with saphenous vein harvesting include the following:
The Internal Thoracic Artery
The Internal Thoracic Artery
- Numerous studies support the use of the left internal thoracic artery (LITA) (also known as the left internal mammary artery (LIMA)) to graft the LAD in order to improve survival unless contraindicated.[1][8][9][10]
- In a study evaluating almost 6,000 patients, LIMA grafting was able to reduce the rate of cardiac-related rehospitalization and revascularization. In addition, this study showed a lower rate of death and recurrent infarction in those who undergone LIMA grafting.[11]
- Evidence shows that the right IMA can be used to graft the LAD if the LIMA is impractical and unusable. Furthermore, the right IMA can be used in conjunction with the LIMA which is called bilateral internal mammary artery (BIMA) grafting.[1]
- In multiple arterial revascularization during Coronary artery bypass surgery, the right internal thoracic artery (RITA) has been proofed to be a better choice as a conduit than the radial artery. This has been published at the European Society of Cardiology (ESC) 2011 Congress, after a trial on more than 1000 patients who had the operation in 10 years trial.
- The left internal thoracic artery (LITA) (also known as the left internal mammary artery (LIMA)) is the best vessel to use for coronary artery bypass surgery when only one artery is required.
- There have been good clinical results with the single left internal thoracic artery grafting compared with saphenous vein grafting. This prompted surgeons to use both ITAs. Bilateral ITA grafting could improve long-term survival. Late complications like myocardial infarction and need to reoperate may be avoided. However, mathematical modeling is required to assist in developing a strategy for use of such grafts.[19]
- In a cohort study of 8123 patients who received single internal thoracic artery grafts and 2001 who received bilateral internal thoracic artery grafts for multivessel coronary artery disease for a duration of 20 years, it was found that the latter produces improved survival compared with single internal thoracic artery grafting during the second postoperative decade, and the magnitude of that benefit increases through 20 postoperative years.[20]
- It’s easy to harvest the radial artery, but it has a higher risk for vasospasm and atherosclerosis than the right internal thoracic artery (RITA). Some institution solves this problem (vasospasm) by preparing the radial arteries with phenoxybenzamine.
- Although the fact that using both internal thoracic arteries for coronary artery bypass surgery takes a longer time, it has better long-term results and perioperative outcomes. This has to be proofed and confirmed by more randomized and controlled trials.
Radial Artery
Radial Artery
Conduit Nomenclature
Conduit Nomenclature
- The terms single bypass, double bypass, triple bypass, quadruple bypass and quintuple bypass refer to the number of coronary arteries bypassed in the procedure. In other words, a double bypass means two coronary arteries are bypassed (such as left anterior descending (LAD) coronary artery and right coronary artery (RCA)); a triple bypass means three vessels are bypassed (such as LAD, RCA, and left circumflex artery (LCX)); a quadruple bypass means four vessels are bypassed (such as LAD, RCA, LCX, first diagonal artery of the LAD). Less commonly more than four coronary arteries may be bypassed.
- A greater number of bypasses does not imply a patient is “sicker,” nor does a lesser number imply a patient is “healthier”.[26]
- A patient with a large amount of coronary artery disease (CAD) may receive fewer bypass grafts owing to the lack of suitable “target” vessels.
- A patient with a single stenosis of the left main coronary artery often requires only two bypasses (to the LAD and the LCX). However, depending upon the anatomy, grafts may also need to be placed to a large diagonal artery, or to additional large obtuse marginal branches.
Assessment of Target Vessels for Bypass Grafting
Assessment of Target Vessels for Bypass Grafting
A coronary artery may be unsuitable for bypass grafting for the following reasons:
- Size: If the native target artery it is small (< 1 mm or < 1.5 mm depending on surgeon preference)
- Location: Some distal locations of the native target artery may not be accessible, or a conduit may not reach far down the native artery.
- Native artery calcification: Heavily calcified native arteries are sometimes technically not amenable to anastomosis of a conduit.
- Diffuse disease: The native artery may not have a section of the vessel that has a minimal disease where a conduit can be grafted to.
- The native artery lies in the heart muscle or is intramyocardial: In this scenario, the native coronary artery is located within the heart muscle rather than on the surface of the heart and a graft cannot be attached to it.
Although the cardiothoracic surgeon reviews the coronary angiogram prior to surgery and identifies the lesions (or “blockages”) in the coronary arteries and will estimate the number of bypass grafts prior to surgery, the final decision is made in the operating room based upon the direct examination of the heart and the suitability of the native target vessel for bypassing.
2021 ACA Revascularization Guideline
2021 ACA Revascularization Guideline
| Class 2a Recommendation, Level of Evidence: B-NR [1]
|
| Among patients undergoing CABG, grafting the bilateral IMA (BIMA) by experienced operators is beneficial in improving long-term cardiac outcomes (only if patients are selected appropriately).
|
2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery (DO NOT EDIT)[28]
2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery (DO NOT EDIT)[28]
References
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 Writing Committee Members. Lawton JS, Tamis-Holland JE, Bangalore S, Bates ER, Beckie TM; et al. (2022). “2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines”. J Am Coll Cardiol. 79 (2): e21–e129. doi:10.1016/j.jacc.2021.09.006. PMID 34895950 .
- ↑ Lawrie GM, Weilbacher DE, Henry PD. Endothelium-dependent relaxation in human saphenous vein grafts. Effects of preparation and clinicopathologic correlations. J Thorac Cardiovasc Surg 1990;100:612—20.
- ↑ Souza DS, Johansson B, Bojo¨ L, Karlsson R, Geijer H, Filbey D, Bodin L, Arbeus M, Dashwood MR. Harvesting the saphenous vein with surrounding tissue for CABG provides long-term graft patency comparable to the left internal thoracic artery: results of a randomized longitudinal trial. J Thorac Cardiovasc Surg 2006;132:373—8.
- ↑ 4.0 4.1 Kiaii B, Moon BC, Massel D, Langlois Y, Austin TW, Willoughby A, Guiraudon C, Howard CR, Guo LR (2002). “A prospective randomized trial of endoscopic versus conventional harvesting of the saphenous vein in coronary artery bypass surgery”. J. Thorac. Cardiovasc. Surg. 123 (2): 204–12. PMID 11828277. Retrieved 2010-07-23.
- ↑ 5.0 5.1 Lopes RD, Hafley GE, Allen KB, Ferguson TB, Peterson ED, Harrington RA, Mehta RH, Gibson CM, Mack MJ, Kouchoukos NT, Califf RM, Alexander JH (2009). “Endoscopic versus open vein-graft harvesting in coronary-artery bypass surgery”. The New England Journal of Medicine. 361 (3): 235–44. doi:10.1056/NEJMoa0900708. PMID 19605828. Retrieved 2010-07-12.
- ↑ 6.0 6.1 Yun KL, Wu Y, Aharonian V, Mansukhani P, Pfeffer TA, Sintek CF, Kochamba GS, Grunkemeier G, Khonsari S (2005). “Randomized trial of endoscopic versus open vein harvest for coronary artery bypass grafting: six-month patency rates”. J. Thorac. Cardiovasc. Surg. 129 (3): 496–503. doi:10.1016/j.jtcvs.2004.08.054. PMID 15746730. Retrieved 2010-07-23.
- ↑ 7.0 7.1 Perrault LP, Jeanmart H, Bilodeau L, Lespérance J, Tanguay JF, Bouchard D, Pagé P, Carrier M (2004). “Early quantitative coronary angiography of saphenous vein grafts for coronary artery bypass grafting harvested by means of open versus endoscopic saphenectomy: a prospective randomized trial”. J. Thorac. Cardiovasc. Surg. 127 (5): 1402–7. doi:10.1016/j.jtcvs.2003.10.040. PMID 15115999. Retrieved 2010-07-23.
- ↑ 8.0 8.1 8.2 Cameron A, Davis KB, Green G, Schaff HV (1996). “Coronary bypass surgery with internal-thoracic-artery grafts–effects on survival over a 15-year period”. N Engl J Med. 334 (4): 216–9. doi:10.1056/NEJM199601253340402. PMID 8531997.
- ↑ 9.0 9.1 9.2 Zeff RH, Kongtahworn C, Iannone LA, Gordon DF, Brown TM, Phillips SJ; et al. (1988). “Internal mammary artery versus saphenous vein graft to the left anterior descending coronary artery: prospective randomized study with 10-year follow-up”. Ann Thorac Surg. 45 (5): 533–6. doi:10.1016/s0003-4975(10)64526-2. PMID 3259128.
- ↑ 10.0 10.1 10.2 10.3 Boylan MJ, Lytle BW, Loop FD, Taylor PC, Borsh JA, Goormastic M; et al. (1994). “Surgical treatment of isolated left anterior descending coronary stenosis. Comparison of left internal mammary artery and venous autograft at 18 to 20 years of follow-up”. J Thorac Cardiovasc Surg. 107 (3): 657–62. PMID 8127094.
- ↑ 11.0 11.1 11.2 11.3 Loop FD, Lytle BW, Cosgrove DM, Stewart RW, Goormastic M, Williams GW; et al. (1986). “Influence of the internal-mammary-artery graft on 10-year survival and other cardiac events”. N Engl J Med. 314 (1): 1–6. doi:10.1056/NEJM198601023140101. PMID 3484393.
- ↑ 12.0 12.1 12.2 Gaudino M, Lorusso R, Rahouma M, Abouarab A, Tam DY, Spadaccio C; et al. (2019). “Radial Artery Versus Right Internal Thoracic Artery Versus Saphenous Vein as the Second Conduit for Coronary Artery Bypass Surgery: A Network Meta-Analysis of Clinical Outcomes”. J Am Heart Assoc. 8 (2): e010839. doi:10.1161/JAHA.118.010839. PMC 6497341. PMID 30636525.
- ↑ Yi G, Shine B, Rehman SM, Altman DG, Taggart DP (2014). “Effect of bilateral internal mammary artery grafts on long-term survival: a meta-analysis approach”. Circulation. 130 (7): 539–45. doi:10.1161/CIRCULATIONAHA.113.004255. PMID 24916209.
- ↑ Takagi H, Goto SN, Watanabe T, Mizuno Y, Kawai N, Umemoto T (2014). “A meta-analysis of adjusted hazard ratios from 20 observational studies of bilateral versus single internal thoracic artery coronary artery bypass grafting”. J Thorac Cardiovasc Surg. 148 (4): 1282–90. doi:10.1016/j.jtcvs.2014.01.010. PMID 24521973.
- ↑ 15.0 15.1 Gaudino M, Di Franco A, Rahouma M, Tam DY, Iannaccone M, Deb S; et al. (2018). “Unmeasured Confounders in Observational Studies Comparing Bilateral Versus Single Internal Thoracic Artery for Coronary Artery Bypass Grafting: A Meta-Analysis”. J Am Heart Assoc. 7 (1). doi:10.1161/JAHA.117.008010. PMC 5778975. PMID 29306899.
- ↑ Taggart DP, Benedetto U, Gerry S, Altman DG, Gray AM, Lees B; et al. (2019). “Bilateral versus Single Internal-Thoracic-Artery Grafts at 10 Years”. N Engl J Med. 380 (5): 437–446. doi:10.1056/NEJMoa1808783. PMID 30699314.
- ↑ Schwann TA, Habib RH, Wallace A, Shahian DM, O’Brien S, Jacobs JP; et al. (2018). “Operative Outcomes of Multiple-Arterial Versus Single-Arterial Coronary Bypass Grafting”. Ann Thorac Surg. 105 (4): 1109–1119. doi:10.1016/j.athoracsur.2017.10.058. PMID 29453002.
- ↑ Beach JM, Mihaljevic T, Svensson LG, Rajeswaran J, Marwick T, Griffin B; et al. (2013). “Coronary artery disease and outcomes of aortic valve replacement for severe aortic stenosis”. J Am Coll Cardiol. 61 (8): 837–48. doi:10.1016/j.jacc.2012.10.049. PMC 4262244. PMID 23428216.
- ↑ Buxton BF, Komeda M, Fuller JA, Gordon I (1998). “Bilateral internal thoracic artery grafting may improve the outcome of coronary artery surgery. Risk-adjusted survival”. Circulation. 98 (19 Suppl): II1–6. PMID 9852872.
- ↑ 20.0 20.1 Lytle BW, Blackstone EH, Sabik JF, Houghtaling P, Loop FD, Cosgrove DM (2004). “The effect of bilateral internal thoracic artery grafting on survival during 20 postoperative years”. Ann Thorac Surg. 78 (6): 2005–12, discussion 2012-4. doi:10.1016/j.athoracsur.2004.05.070. PMID 15561021.
- ↑ 21.0 21.1 Gaudino M, Benedetto U, Fremes S, Ballman K, Biondi-Zoccai G, Sedrakyan A; et al. (2020). “Association of Radial Artery Graft vs Saphenous Vein Graft With Long-term Cardiovascular Outcomes Among Patients Undergoing Coronary Artery Bypass Grafting: A Systematic Review and Meta-analysis”. JAMA. 324 (2): 179–187. doi:10.1001/jama.2020.8228. PMC 7361649 . PMID 32662861 .
- ↑ 22.0 22.1 Cao C, Manganas C, Horton M, Bannon P, Munkholm-Larsen S, Ang SC; et al. (2013). “Angiographic outcomes of radial artery versus saphenous vein in coronary artery bypass graft surgery: a meta-analysis of randomized controlled trials”. J Thorac Cardiovasc Surg. 146 (2): 255–61. doi:10.1016/j.jtcvs.2012.07.014. PMID 22871565.
- ↑ Benedetto U, Raja SG, Albanese A, Amrani M, Biondi-Zoccai G, Frati G (2015). “Searching for the second best graft for coronary artery bypass surgery: a network meta-analysis of randomized controlled trials†”. Eur J Cardiothorac Surg. 47 (1): 59–65, discussion 65. doi:10.1093/ejcts/ezu111. PMID 24686003.
- ↑ 24.0 24.1 Gaudino M, Benedetto U, Fremes S, Biondi-Zoccai G, Sedrakyan A, Puskas JD; et al. (2018). “Radial-Artery or Saphenous-Vein Grafts in Coronary-Artery Bypass Surgery”. N Engl J Med. 378 (22): 2069–2077. doi:10.1056/NEJMoa1716026. PMID 29708851.
- ↑ Abu-Omar Y, Mussa S, Anastasiadis K, Steel S, Hands L, Taggart DP (2004). “Duplex ultrasonography predicts safety of radial artery harvest in the presence of an abnormal Allen test”. Ann Thorac Surg. 77 (1): 116–9. doi:10.1016/s0003-4975(03)01515-7. PMID 14726046.
- ↑ Ohki S, Kaneko T, Satoh Y; et al. (2002). “[Coronary artery bypass grafting in octogenarian]”. Kyobu geka. The Japanese journal of thoracic surgery (in Japanese). 55 (10): 829–33, discussion 833–6. PMID 12233100.
- ↑ Magruder JT, Young A, Grimm JC, Conte JV, Shah AS, Mandal K; et al. (2016). “Bilateral internal thoracic artery grafting: Does graft configuration affect outcome?”. J Thorac Cardiovasc Surg. 152 (1): 120–7. doi:10.1016/j.jtcvs.2016.03.022. PMID 27343909.
- ↑ Hillis LD, Smith PK, Anderson JL, Bittl JA, Bridges CR, Byrne JG; et al. (2011). “2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines”. Circulation. doi:10.1161/CIR.0b013e31823c074e. PMID 22064599.
- ↑ 29.0 29.1 29.2 Sabik JF, Lytle BW, Blackstone EH, Houghtaling PL, Cosgrove DM (2005). “Comparison of saphenous vein and internal thoracic artery graft patency by coronary system”. Ann Thorac Surg. 79 (2): 544–51, discussion 544-51. doi:10.1016/j.athoracsur.2004.07.047. PMID 15680832.
- ↑ Lytle BW, Blackstone EH, Loop FD, Houghtaling PL, Arnold JH, Akhrass R; et al. (1999). “Two internal thoracic artery grafts are better than one”. J Thorac Cardiovasc Surg. 117 (5): 855–72. PMID 10220677.
- ↑ Sabik JF, Blackstone EH, Gillinov AM, Banbury MK, Smedira NG, Lytle BW (2006). “Influence of patient characteristics and arterial grafts on freedom from coronary reoperation”. J Thorac Cardiovasc Surg. 131 (1): 90–8. doi:10.1016/j.jtcvs.2005.05.024. PMID 16399299.
- ↑ 32.0 32.1 Sabik JF, Stockins A, Nowicki ER, Blackstone EH, Houghtaling PL, Lytle BW; et al. (2008). “Does location of the second internal thoracic artery graft influence outcome of coronary artery bypass grafting?”. Circulation. 118 (14 Suppl): S210–5. doi:10.1161/CIRCULATIONAHA.107.760827. PMID 18824756.
- ↑ Stevens LM, Carrier M, Perrault LP, Hébert Y, Cartier R, Bouchard D; et al. (2004). “Single versus bilateral internal thoracic artery grafts with concomitant saphenous vein grafts for multivessel coronary artery bypass grafting: effects on mortality and event-free survival”. J Thorac Cardiovasc Surg. 127 (5): 1408–15. doi:10.1016/j.jtcvs.2003.10.006. PMID 15116000.
- ↑ Sabik JF, Lytle BW, Blackstone EH, Khan M, Houghtaling PL, Cosgrove DM (2003). “Does competitive flow reduce internal thoracic artery graft patency?”. Ann Thorac Surg. 76 (5): 1490–6, discussion 1497. PMID 14602274.
- ↑ Acar C, Ramsheyi A, Pagny JY, Jebara V, Barrier P, Fabiani JN; et al. (1998). “The radial artery for coronary artery bypass grafting: clinical and angiographic results at five years”. J Thorac Cardiovasc Surg. 116 (6): 981–9. PMID 9832690.
- ↑ Maniar HS, Sundt TM, Barner HB, Prasad SM, Peterson L, Absi T; et al. (2002). “Effect of target stenosis and location on radial artery graft patency”. J Thorac Cardiovasc Surg. 123 (1): 45–52. PMID 11782755.
- ↑ Moran SV, Baeza R, Guarda E, Zalaquett R, Irarrazaval MJ, Marchant E; et al. (2001). “Predictors of radial artery patency for coronary bypass operations”. Ann Thorac Surg. 72 (5): 1552–6. PMID 11722042.
- ↑ Possati G, Gaudino M, Alessandrini F, Luciani N, Glieca F, Trani C; et al. (1998). “Midterm clinical and angiographic results of radial artery grafts used for myocardial revascularization”. J Thorac Cardiovasc Surg. 116 (6): 1015–21. PMID 9832694.
- ↑ Royse AG, Royse CF, Tatoulis J, Grigg LE, Shah P, Hunt D; et al. (2000). “Postoperative radial artery angiography for coronary artery bypass surgery”. Eur J Cardiothorac Surg. 17 (3): 294–304. PMID 10758391.
- ↑ Desai ND, Cohen EA, Naylor CD, Fremes SE, Radial Artery Patency Study Investigators (2004). “A randomized comparison of radial-artery and saphenous-vein coronary bypass grafts”. N Engl J Med. 351 (22): 2302–9. doi:10.1056/NEJMoa040982. PMID 15564545.
Template:WH
Template:WS

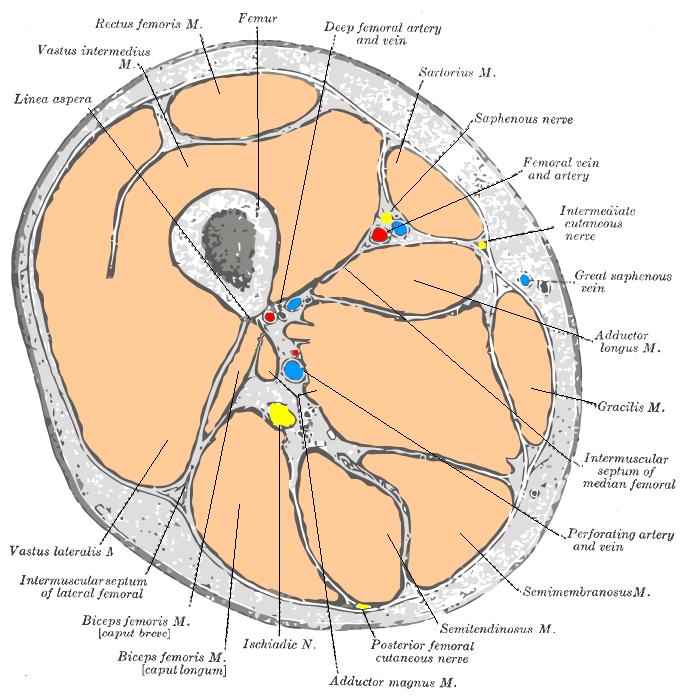 Cross-section through the middle of the thigh.
Cross-section through the middle of the thigh.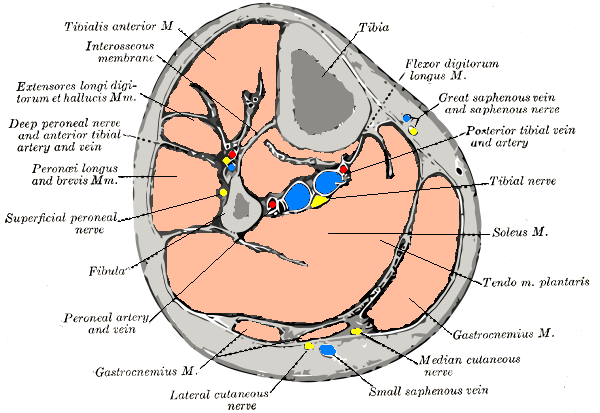 Cross-section through the middle of the leg.
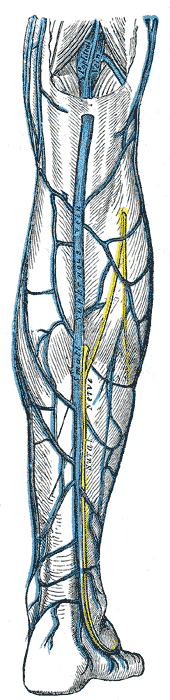
Cross-section through the middle of the leg.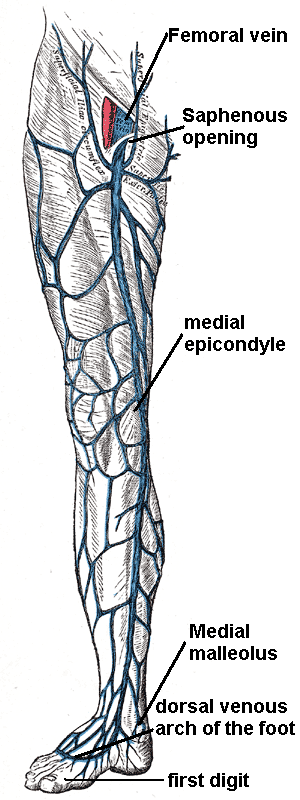 The great saphenous vein and landmarks along its course
The great saphenous vein and landmarks along its course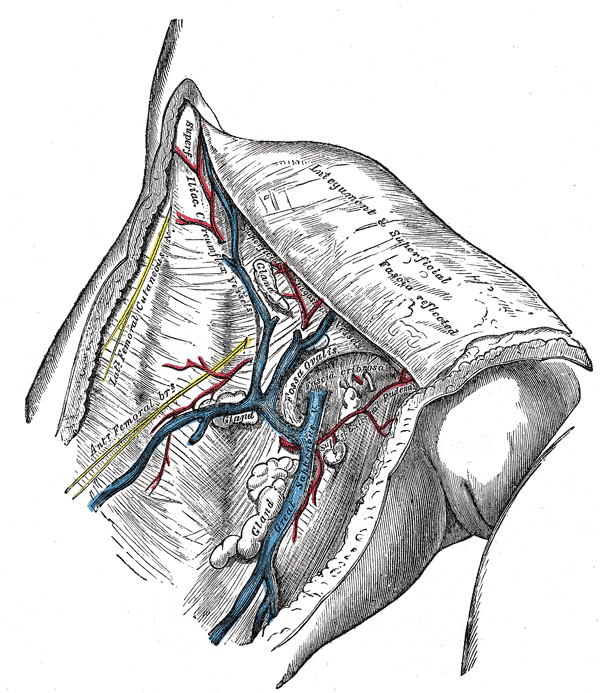
 Small saphenous vein and its tributaries.
Small saphenous vein and its tributaries.

