
EKG abnormalities in central nervous system disease
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
Overview
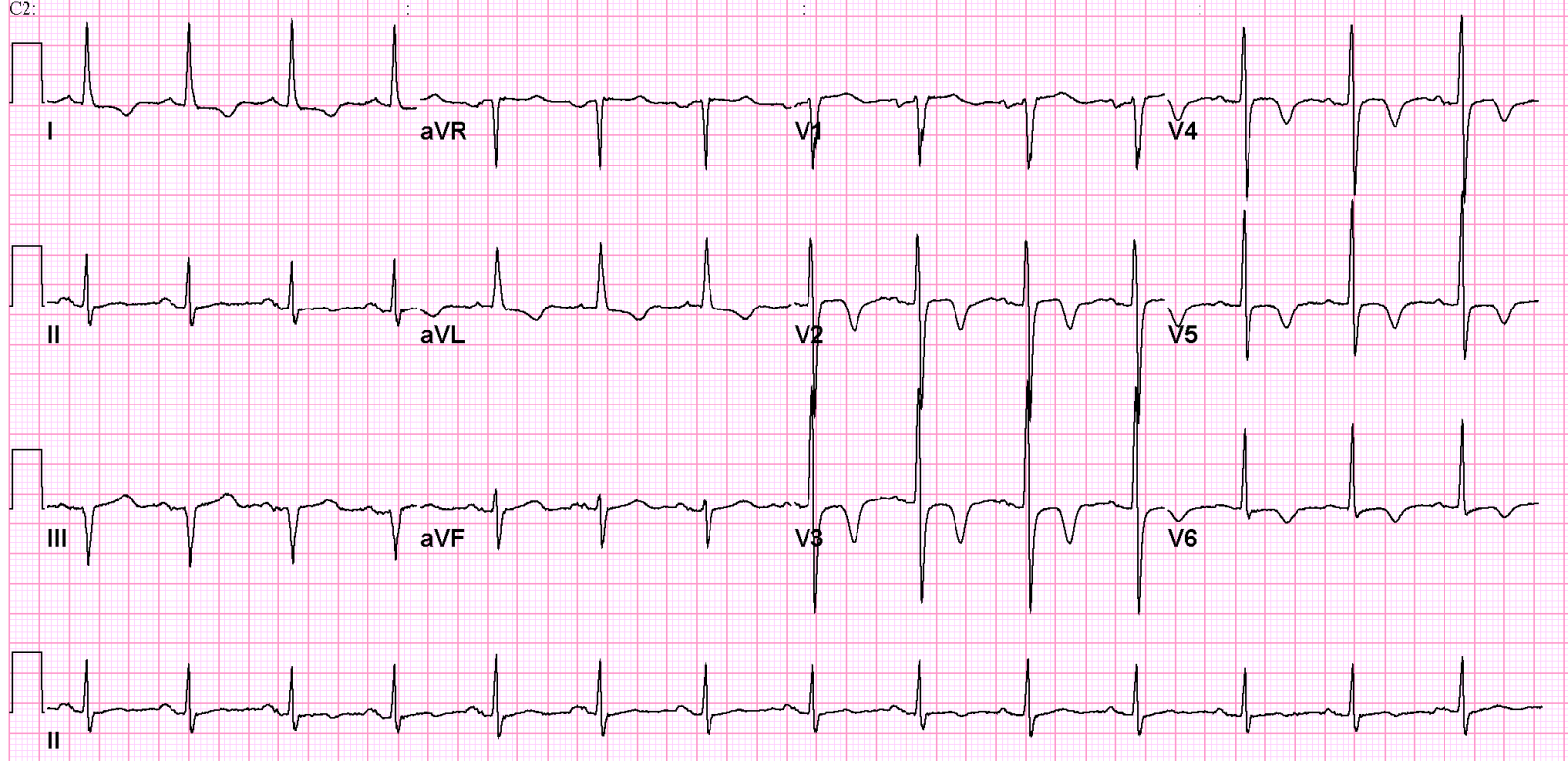
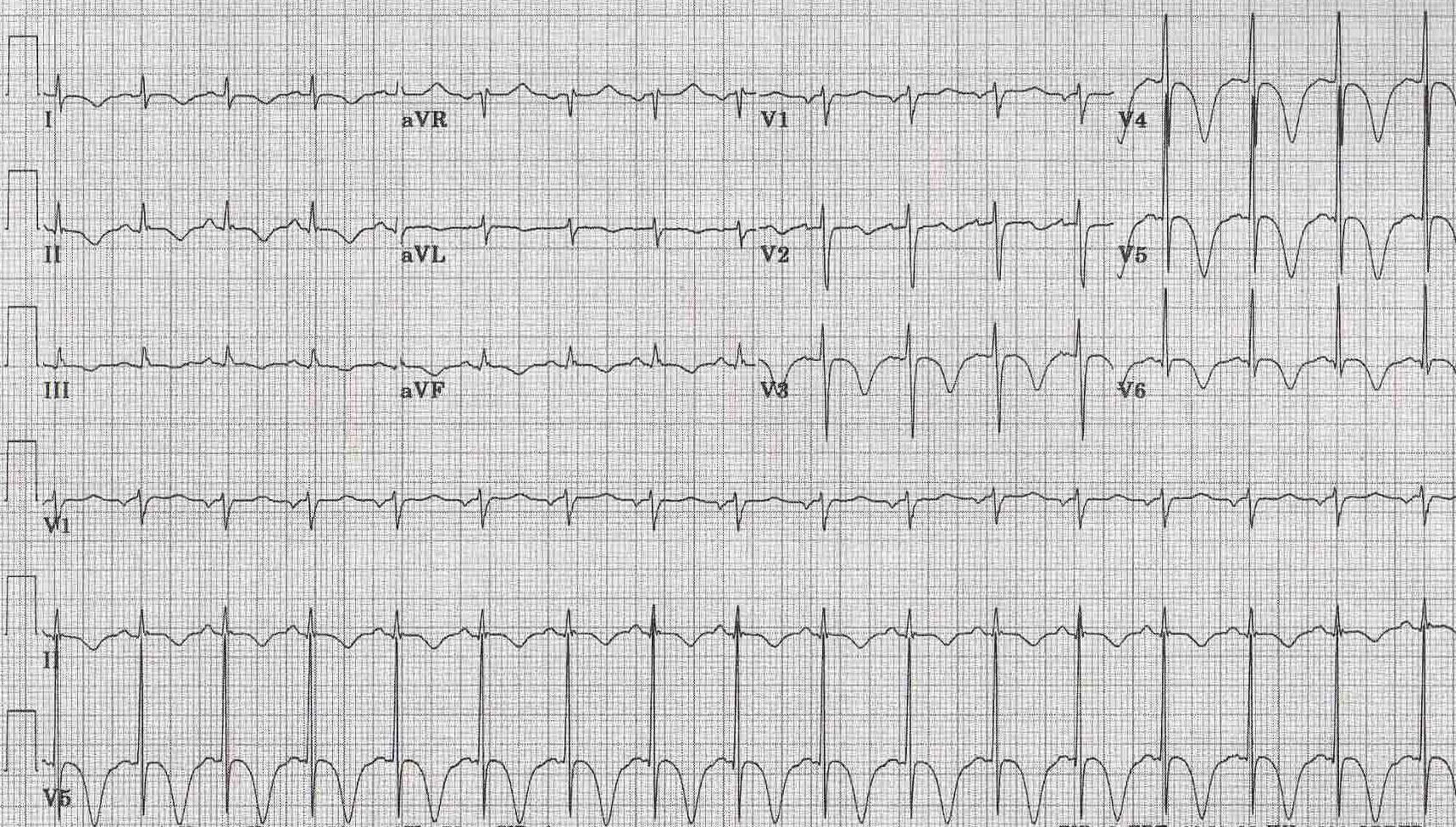
Classic manifestations on EKG of the so-called cerebrovascular accidents, (most commonly associated with subarachnoid hemorrhage or other intracranial bleeds) are symmetrically and deeply inverted giant T waves.
Pathophysiology
Pathophysiology
The mechanisms are not fully delineated but may relate to excessive catecholamine stimulation causing direct myocardial injury (myocytolysis).
Diagnosis
Diagnosis
Electrocardiographic Findings
The ECG may be notable for marked QT-U prolongation (sometimes a giant U wave appears to be embeded in the T wave, creating a slight discontinuity in the waveform morphology). The long QT-U may predispose to torsade(s) de pointes. Takostubo syndrome may occur in some cases. Apical hypertrophic cardiomyopathy (Yamaguchi’s syndrome) is associated with deep narrow (spade-like) T wave inversions, most marked in the mid-precordial leads.
- EKG changes seen in 71.5% of patients with subarachnoid hemorrhage, and 57.1% of those with cerebral hemorrhage.
- Most common abnormalities are
- Large, upright, or deeply inverted T waves
- Prolongation of the QTc interval
- Prominent U waves
- Can persist for 11 days
- Rarely can ST segment elevation or depression
- Rhythm disturbances
- Reason for changes is thought to be altered autonomic tone
Examples
-
 Patient with subaracnoidal hemorrhage
Patient with subaracnoidal hemorrhage -
 EKG of a patients with CNS Disorders
EKG of a patients with CNS Disorders -
 Inverted and deep T waves in the precordal leads due to subaracnoidal aneurysm [Image courtesy of Dr Jose Ganseman Dr Ganseman’s webpage: An ultimate source of EKG
Inverted and deep T waves in the precordal leads due to subaracnoidal aneurysm [Image courtesy of Dr Jose Ganseman Dr Ganseman’s webpage: An ultimate source of EKG



Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH