
Left ventricle
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Overview
The left ventricle is one of four chambers (two atria and two ventricles) in the human heart. It receives oxygenated blood from the left atrium via the mitral valve, and pumps it into the aorta via the aortic valve.
Shape
Shape
The left ventricle is longer and more conical in shape than the right, and on transverse section its concavity presents an oval or nearly circular outline. It forms a small part of the sternocostal surface and a considerable part of the diaphragmatic surface of the heart; it also forms the apex of the heart.
Development
Development
By teenage and adult ages, its walls have thickened to three to six times greater than that of the right ventricle. This reflects the typical five times greater pressure workload this chamber performs while accepting blood returning from the lungs veins at ~8mmHg pressure and pushing it forward to the typical ~120mmHg pressure in the aorta during each heartbeat. (The pressures stated are resting values and stated as relative to surrounding atmospheric which is the typical “0” reference pressure used in medicine.)
Function
Function
For excellence of health, the left ventricular muscle must:
- (a) relax very rapidly after each contraction so as to fill rapidly with oxygenated blood flowing from the lung veins, i.e. diastolic relaxation and filling.
- (b) contract rapidly and forcibly to force the majority of this blood into the aorta, overcoming the much higher aortic pressure and the extra pressure required to stretch the aorta and other major arteries enough to expand and make room for the sudden increase in blood volume, i.e. systolic contraction and ejection.
- (c) be able to rapidly increase or decrease its pumping capacity under nervous system control.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
In cardiovascular physiology, ejection fraction (Ef) is the fraction of blood pumped out of a ventricle with each heart beat. The term ejection fraction applies to both the right and left ventricles; one can speak equally of the left ventricular ejection fraction (LVEF) and the right ventricular ejection fraction (RVEF). Without a qualifier, the term ejection fraction refers specifically to that of the left ventricle.
By definition, the volume of blood within a ventricle immediately before a contraction is known as the end-diastolic volume. Similarly, the volume of blood left in a ventricle at the end of contraction is end-systolic volume. The difference between end-diastolic and end-systolic volumes is the stroke volume, the volume of blood ejected with each beat. Ejection fraction (Ef) is the fraction of the end-diastolic volume that is ejected with each beat; that is, it is stroke volume (SV) divided by end-diastolic volume (EDV):
- <math>E_f = \frac{SV}{EDV} = \frac{EDV – ESV}{EDV}</math>
Normal values
In a healthy 70-kg (154-lb) man, the SV is approximately 70 ml and the left ventricular EDV is 120 ml, giving an ejection fraction of 70/120, or 58%. Right ventricular volumes being roughly equal to those of the left ventricle, the ejection fraction of the right ventricle is normally equal to that of the left ventricle within narrow limits.
Healthy individuals typically have ejection fractions greater than 0.55. However, normal values depend upon the modality being used to calculate the ejection fraction. Damage to the muscle of the heart (myocardium), such as that sustained during myocardial infarction or in cardiomyopathy, impairs the heart’s ability to eject blood and therefore reduces ejection fraction. This reduction in the ejection fraction can manifest itself clinically as heart failure. The ejection fraction is one of the most important predictors of prognosis; those with significantly reduced ejection fractions typically have a poorer prognoses.
Measurement
Ejection fraction is commonly measured by echocardiography, in which the volumes of the heart’s chambers are measured during the cardiac cycle. Ejection fraction can then be obtained by dividing stroke volume by end-diastolic volume as described above.
Other methods of measuring ejection fraction include cardiac MRI, fast scan cardiac computed axial tomography (CT) imaging, ventriculography, Gated SPECT, and the MUGA scan. A MUGA scan involves the injection of a radioisotope into the blood and detecting its flow through the left ventricle. The historical gold standard for the measurement of ejection fraction is ventriculography.
ACC/AHA/ESC 2006 Guidelines (DO NOT EDIT) [1]
Left Ventricular Function and Imaging Recommendations
| Class I |
| “1 Echocardiography is recommended in patients with ventricular arrhythmias who are suspected of having structural heart disease. (Level of Evidence: B) ” |
| “2 Echocardiography is recommended for the subset of patients at high risk for the development of serious ventricular arrhythmias or SCD, such as those with dilated, hypertrophic, or RV cardiomyopathies, AMI survivors, or relatives of patients with inherited disorders associated with SCD. (Level of Evidence: B) ” |
| “3 Exercise testing with an imaging modality (echocardiography or nuclear perfusion [single-photon emission computed tomography (SPECT)]) is recommended to detect silent ischemia in patients with ventricular arrhythmias who have an intermediate probability of having CHD by age, symptoms, and gender and in whom ECG assessment is less reliable because of digoxin use, LVH, greater than 1-mm ST-segment depression at rest, WPW syndrome, or LBBB. (Level of Evidence: B) ” |
| “4 Pharmacological stress testing with an imaging modality (echocardiography or myocardial perfusion SPECT) is recommended to detect silent ischemia in patients with ventricular arrhythmias who have an intermediate probability of having CHD by age, symptoms, and gender and are physically unable to perform a symptomlimited exercise test. (Level of Evidence: B) ” |
| Class IIa |
| “1 MRI, cardiac computed tomography (CT), or radionuclide angiography can be useful in patients with ventricular arrhythmias when echocardiography does not provide accurate assessment of LV and RV function and/or evaluation of structural changes. (Level of Evidence: B)” |
| “2 Coronary angiography can be useful in establishing or excluding the presence of significant obstructive CHD in patients with life-threatening ventricular arrhythmias or in survivors of SCD, who have an intermediate or greater probability of having CHD by age, symptoms, and gender. (Level of Evidence: C)” |
| “3 LF imaging can be useful in patients undergoing biventricular pacing. (Level of Evidence: C) ” |
See also
References
- Berne, Robert M., Levy, Matthew N. (2001). Cardiovascular Physiology. Philadelphia, PA: Mosby. ISBN 0-323-01127-6.
- Boron, Walter F., Boulpaep, Emile L. (2005). Medical Physiology: A Cellular and Molecular Approach. Philadelphia, PA: Elsevier/Saunders. ISBN 1-4160-2328-3.
- ↑ Zipes DP, Camm AJ, Borggrefe M, Buxton AE, Chaitman B, Fromer M; et al. (2006). “ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: a report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (writing committee to develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society”. Circulation. 114 (10): e385–484. doi:10.1161/CIRCULATIONAHA.106.178233. PMID 16935995.
Pumping volume
Pumping volume
Typical healthy adult heart pumping volume is ~5 liters/min, resting. Maximum capacity pumping volume extends from ~25 liters/min for non-athletes to as high as ~45 liters/min for Olympic level athletes.
Additional images
Additional images
-
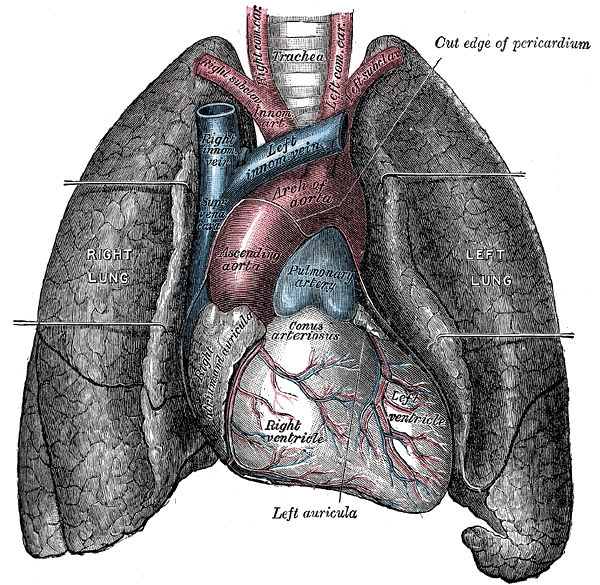 Front view of heart and lungs.
Front view of heart and lungs. -
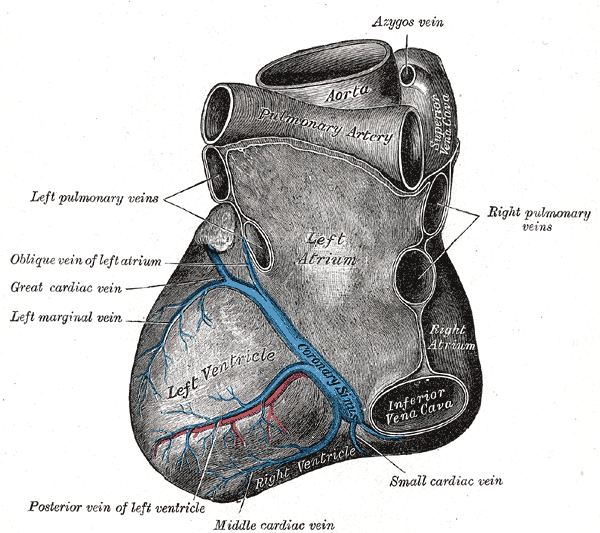 Base and diaphragmatic surface of heart.
Base and diaphragmatic surface of heart.


External links
External links
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH