
Cardiomyopathy
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Lina Ya’qoub,MD; Mahshid Mir, M.D. [2], Cafer Zorkun, M.D., Ph.D. [3], Raviteja Guddeti, M.B.B.S. [4]; Edzel Lorraine Co, DMD, MD[5]
Synonyms and keywords: Myocardiopathy; cardiac muscle disease; heart muscle disease.
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Edzel Lorraine Co, DMD, MD[2] Muhammad Saad, M.B.B.S.[3]
Overview
Cardiomyopathy refers to diseases that involve the heart muscle and leads to its abnormal function and/or structure, in the absence of coronary artery disease, hypertension, valvular disease or congenital heart disease that would explain the myocardium dysfunction.
Classification
Cardiomyopathies can generally be categorized into two groups (based on World Health Organization guidelines): extrinsic cardiomyopathies and intrinsic cardiomyopathies [1]. Cardiomyopathy can also be classified from a clinical standpoint, as to whether it is restrictive, dilated, or hypertrophic.
Causes
There is a very wide range of factors that can cause cardiomyopathy, ranging from infectious causes, toxins, genetic causes and other disease processes.
Risk Factors
Some of the risk factors for developing cardiomyopathy include: a family history of cardiomyopathy, heart failure or sudden death, a history of other diseases that may lead to cardiomyopathy, obesity, alcoholism, and long standing high blood pressure. Certain diseases such as hemochromatosis, amyloidosis, and sarcoidosis also increase the risk of developing cardiomyopathy.
Natural History, Complications and Prognosis
Cardiomyopathy will continue to progressively worsen, unless intervened on. Complications and sequelae of cardiomyopathy include heart failure, arrythmia, thromboembolic disease, and sudden cardiac death.
Diagnosis
History and Symptoms
Patients may be asymptomatic in early stages of disease. When symptoms occur, they include: shortness of breath, edema of the lower extremities, fatigue, loss of consciousness, and palpitations due to arrythmias.
Physical Examination
A thorough physical examination can help in diagnosing cardiomyopathy. Particular attention should be given to the cardiac exam, the lung exam, the extremities for edema, and in assessing for other signs of heart failure such as jugular venous distension.
Chest X Ray
A chest x ray also shows fluid build-up, or a pleural effusion in the lungs, which can be a sign of the complication of heart failure.
Treatment
Medical Therapy
Treatment is phenotype-directed and includes guideline-directed medical therapy (GDMT) for heart failure syndromes and targeted therapy for specific cardiomyopathies such as hypertrophic cardiomyopathy (HCM). In HCM, management includes symptom-directed pharmacotherapy (beta-blocker or nondihydropyridine calcium-channel blocker, with disopyramide or a cardiac myosin inhibitor in selected adults with obstructive physiology), risk-based use of ICDs, and septal reduction therapy at experienced centers when symptoms persist despite medical therapy.[2] [3]For cardiomyopathy with HFrEF, foundational GDMT consists of an ARNI/ACE inhibitor/ARB, evidence-based beta-blocker, mineralocorticoid receptor antagonist, and SGLT2 inhibitor, with additional therapies and device-based treatment individualized by EF, QRS, symptoms, and comorbidities.[3] Goals include symptom relief, prevention of sudden cardiac death (when relevant, e.g., HCM), and modification of heart-failure trajectory; patients with advanced heart failure despite GDMT should be referred to an advanced HF team for consideration of transplant and/or durable mechanical circulatory support.[4] In HCM with atrial fibrillation, oral anticoagulation is recommended irrespective of CHA₂DS₂-VASc, and rhythm and/or rate control should be individualized.[2]
Surgery
Procedural and surgical options are phenotype-specific and should be performed at experienced centers when indicated.[2] For symptomatic obstructive HCM refractory to medical therapy, septal reduction therapy includes surgical septal myectomy or (in selected patients) alcohol septal ablation. Advanced heart failure may require durable mechanical circulatory support and/or heart transplantation after evaluation by an advanced HF team.[2][4]
Primary Prevention
Primary prevention focuses on ‘at risk’ (Stage A) and ‘pre-HF’ (Stage B) management: control hypertension, diabetes, obesity, and other cardiovascular risk factors; avoid cardiotoxins (including excess alcohol and illicit drugs); and treat structural heart disease early to prevent progression to symptomatic HF.[4][5]
Preferences
- ↑ Richardson, P.; et al. (1996). “Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the Definition and Classification of cardiomyopathies”. Circulation. 93 (5): 841–2. PMID 8598070. (Full text)
- ↑ 2.0 2.1 2.2 2.3 Ommen SR, Ho CY, Asif IM, Balaji S, Burke MA, Day SM, Dearani JA, Epps KC, Evanovich L, Ferrari VA, Joglar JA, Khan SS, Kim JJ, Kittleson MM, Krittanawong C, Martinez MW, Mital S, Naidu SS, Saberi S, Semsarian C, Times S, Waldman CB (June 2024). “2024 AHA/ACC/AMSSM/HRS/PACES/SCMR Guideline for the Management of Hypertrophic Cardiomyopathy: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines”. Circulation. 149 (23): e1239–e1311. doi:10.1161/CIR.0000000000001250. PMID 38718139 Check
|pmid=value (help). - ↑ 3.0 3.1 Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, Fang JC, Fedson SE, Fonarow GC, Hayek SS, Hernandez AF, Khazanie P, Kittleson MM, Lee CS, Link MS, Milano CA, Nnacheta LC, Sandhu AT, Stevenson LW, Vardeny O, Vest AR, Yancy CW (May 2022). “2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines”. Circulation. 145 (18): e895–e1032. doi:10.1161/CIR.0000000000001063. PMID 35363499 Check
|pmid=value (help). - ↑ 4.0 4.1 4.2 Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, Fang JC, Fedson SE, Fonarow GC, Hayek SS, Hernandez AF, Khazanie P, Kittleson MM, Lee CS, Link MS, Milano CA, Nnacheta LC, Sandhu AT, Stevenson LW, Vardeny O, Vest AR, Yancy CW (May 2022). “2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines”. Circulation. 145 (18): e876–e894. doi:10.1161/CIR.0000000000001062. PMID 35363500 Check
|pmid=value (help). - ↑ Joglar JA, Chung MK, Armbruster AL, Benjamin EJ, Chyou JY, Cronin EM, Deswal A, Eckhardt LL, Goldberger ZD, Gopinathannair R, Gorenek B, Hess PL, Hlatky M, Hogan G, Ibeh C, Indik JH, Kido K, Kusumoto F, Link MS, Linta KT, Marcus GM, McCarthy PM, Patel N, Patton KK, Perez MV, Piccini JP, Russo AM, Sanders P, Streur MM, Thomas KL, Times S, Tisdale JE, Valente AM, Van Wagoner DR (January 2024). “2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines”. Circulation. 149 (1): e1–e156. doi:10.1161/CIR.0000000000001193. PMC 11095842 Check
|pmc=value (help). PMID 38033089 Check|pmid=value (help).
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] ; Associate Editor(s)-in-Chief: Lina Ya’qoub,MD, Edzel Lorraine Co, DMD, MD[2]
Overview
In 1980, the World Health Organization (WHO) defined cardiomyopathies as “heart muscle diseases of unknown cause” to distinguish cardiomyopathy from cardiac dysfunction due to known cardiovascular causes such as hypertension, ischemic heart disease, or valvular disease. In clinical practice, however, the term “cardiomyopathy” had also been applied to diseases of known cardiovascular cause, including ischemic cardiomyopathy and hypertensive cardiomyopathy. As a result, the 1995 WHO/International Society and Federation of Cardiology (ISFC) Task Force on the Definition and Classification of the Cardiomyopathies expanded the classification to include all diseases affecting heart muscle and to take into consideration etiology as well as the dominant pathophysiology. In the 1995 classification, the cardiomyopathies were defined as “diseases of the myocardium associated with cardiac dysfunction.”
Historical Perspective
- In 1980, the World Health Organization (WHO) defined cardiomyopathies as “heart muscle diseases of unknown cause” to distinguish cardiomyopathy from cardiac dysfunction due to known cardiovascular causes such as hypertension, ischemic heart disease, or valvular disease.
- In clinical practice, however, the term “cardiomyopathy” had also been applied to diseases of known cardiovascular cause, including ischemic cardiomyopathy and hypertensive cardiomyopathy.
- As a result, the 1995 WHO/International Society and Federation of Cardiology (ISFC) Task Force on the Definition and Classification of the Cardiomyopathies expanded the classification to include all diseases affecting heart muscle and to take into consideration etiology as well as the dominant pathophysiology.
- In the 1995 WHO classification, the cardiomyopathies were defined as “diseases of the myocardium associated with cardiac dysfunction.”
References
References:
1-Report of the WHO/ISFC task force on the definition and classification of cardiomyopathies. Br Heart J 1980; 44:672.
2- Richardson P, McKenna W, Bristow M, et al. Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the Definition and Classification of cardiomyopathies. Circulation 1996; 93:841.
3- Maron BJ, Towbin JA, Thiene G, et al. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation 2006; 113:1807.
4- Elliott P, Andersson B, Arbustini E, et al. Classification of the cardiomyopathies: a position statement from the European Society Of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 2008; 29:270.
5- WRITING COMMITTEE MEMBERS, Yancy CW, Jessup M, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2013; 128:e240.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Lina Ya’qoub,MD; Edzel Lorraine Co, DMD, MD[2]
Overview
Incidence and prevalence differ based on cause. The incidence of DCM has been estimated to be 5-8 cases per 100,000 population, with a prevalence of 36 per 100,000. This could be explained by the incomplete disease expression, which goes unrecognized. The prevalence of HCM in the absence of aortic valve disease or systemic hypertension is at least 200 per 100,000 of the adult population. RCM is much less common than either DCM or HCM in the developed world, but is a frequent cause of death in the tropical countries, primarily because of the high incidence of endomyocardial fibrosis in those regions.
Cardiomyopathy Epidemiology and Demographics
Incidence and prevalence differ based on cause.[1]
- The incidence of DCM has been estimated to be 5-8 cases per 100,000 population, with a prevalence of 36 per 100,000. This could be explained by the incomplete disease expression, which goes unrecognized.[2]
- The prevalence of HCM in the absence of aortic valve disease or systemic hypertension is at least 200 per 100,000 of the adult population.[3]
- RCM is much less common than either DCM or HCM in the developed world, but is a frequent cause of death in the tropical countries, primarily because of the high incidence of endomyocardial fibrosis in those regions.[4]
- African–American individuals are approximately three times more prone to development of dilated cardiomyopathy.
- Hypertrophic cardiomyopathy has a prevalence of 400-800 per 100,0000 in adults. This prevalence seems to be similar in all races, but the disease age is mainly considered to be in adolescence and you adults.[4]
- Dilated cardiomyopathy has an approximate incidence of 4.58 per 100,000 in children less than 1 year old. The incidence decrease when the child ages and is 0.34 per 100,000 between 1 to 18 years old. [4]
- The incidence of dilated cardiomyopathy was estimated to be 400-800 cases per 100,000 individuals worldwide.[5]
References
- ↑ Richard P, Charron P, Carrier L, Ledeuil C, Cheav T, Pichereau C, Benaiche A, Isnard R, Dubourg O, Burban M, Gueffet JP, Millaire A, Desnos M, Schwartz K, Hainque B, Komajda M (May 2003). “Hypertrophic cardiomyopathy: distribution of disease genes, spectrum of mutations, and implications for a molecular diagnosis strategy”. Circulation. 107 (17): 2227–32. doi:10.1161/01.CIR.0000066323.15244.54. PMID 12707239.
- ↑ Kushwaha SS, Fallon JT, Fuster V (January 1997). “Restrictive cardiomyopathy”. N. Engl. J. Med. 336 (4): 267–76. doi:10.1056/NEJM199701233360407. PMID 8995091.
- ↑ Kawasaki K, Miyaji K, Kodera S, Suzuki Y, Kanda J, Ikeda M (May 2015). “Arrhythmogenic right ventricular cardiomyopathy in a patient with schizophrenia”. Clin Case Rep. 3 (5): 308–14. doi:10.1002/ccr3.230. PMID 25984311.
- ↑ 4.0 4.1 4.2 Maron BJ, Gardin JM, Flack JM, Gidding SS, Kurosaki TT, Bild DE (August 1995). “Prevalence of hypertrophic cardiomyopathy in a general population of young adults. Echocardiographic analysis of 4111 subjects in the CARDIA Study. Coronary Artery Risk Development in (Young) Adults”. Circulation. 92 (4): 785–9. PMID 7641357.
- ↑ Lipshultz SE, Sleeper LA, Towbin JA, Lowe AM, Orav EJ, Cox GF, Lurie PR, McCoy KL, McDonald MA, Messere JE, Colan SD (April 2003). “The incidence of pediatric cardiomyopathy in two regions of the United States”. N. Engl. J. Med. 348 (17): 1647–55. doi:10.1056/NEJMoa021715. PMID 12711739.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Edzel Lorraine Co, DMD, MD[2]
Overview
Some of the risk factors for developing cardiomyopathy include; a family history of cardiomyopathy, heart failure, or sudden death, a history of other diseases that may lead to cardiomyopathy, obesity, alcoholism, and long standing high blood pressure. Certain diseases such as hemachromotosis, amyloidosis, and sarcoidosis also increase the risk of developing cardiomyopathy.
Risk Factors
Certain diseases, conditions, or factors can raise the risk for cardiomyopathy. Major risk factors include:[1][2]
- A family history of cardiomyopathy, heart failure, or sudden cardiac arrest (SCA)
- A disease or condition that can lead to cardiomyopathy, such as coronary heart disease, heart attack, or a viral infection that inflames the heart muscle
- Diabetes or other metabolic diseases, or severe obesity
- Diseases that can damage the heart, such as hemochromatosis, sarcoidosis, or amyloidosis
- Long-term alcoholism
- Long-term high blood pressure
References
- ↑ Wexler RK, Elton T, Pleister A, Feldman D (May 2009). “Cardiomyopathy: an overview”. Am Fam Physician. 79 (9): 778–84. PMID 20141097.
- ↑ Sisakian H (June 2014). “Cardiomyopathies: Evolution of pathogenesis concepts and potential for new therapies”. World J Cardiol. 6 (6): 478–94. doi:10.4330/wjc.v6.i6.478. PMID 24976920.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Lina Ya’qoub, MD; Edzel Lorraine Co, DMD, MD[2]
Overview
Cardiomyopathy will continue to progressively worsen, unless intervened on. As the function of the heart deteriorates, symptoms of heart failure become apparent. On the other hand, defects in ion channels and hypertrophic cardiomyopathy can present with fatal arrhythmias and sudden cardiac death without the preceding symptoms of heart failure. In general, complications and sequelae of cardiomyopathy include heart failure, arrythmia, thromboembolic disease, and sudden cardiac death. Prognosis of patients depends on the etiology of the cardiomyopathy and the initiation of management, whether medical, surgical or device therapy. Patients with cardiomyopathy are usually treated with medical treatment similar to heart failure patients, although some patients do not respond well to medications and continue to have worsening heart function, which may require heart transplant eventually. Those patients at high risk for fatal arrhythmias and sudden cardiac death should receive device therapy with implantable cardioverter defibrillator (ICD) or cardiac resynchronization therapy (CRT).
Natural History
- The symptoms of cardiolyopathy usually develop secondary to a predisposing factor and an underlying cause and start with symptoms such as fatigue, fever, and shortness of breath.
- Cardiomyopathy will continue to progressively worsen, unless intervened on.[1][2]
Complications
Cardiomyopathy gets worse unless treated. The most likely complications are:[3]
Prognosis
Prognosis of patients depends on the etiology of the cardiomyopathy and the initiation of management, whether medical, surgical or device therapy:
- Patients with cardiomyopathy are usually treated with medical treatment similar to heart failure patients, although some patients do not respond well to medications and continue to have worsening heart function, which may require heart transplant eventually.
- Those patients at high risk for fatal arrhythmias and sudden cardiac death should receive device therapy with implantable cardioverter defibrillator (ICD) or cardiac resynchronization therapy (CRT).[1][2][3]
-
 Brain: Infarct: Healing large MCA and PICA probably embolic 64 year old female chronic obstructive pulmonary disease and cardiomyopathy with atrial fibrillation
Brain: Infarct: Healing large MCA and PICA probably embolic 64 year old female chronic obstructive pulmonary disease and cardiomyopathy with atrial fibrillation -
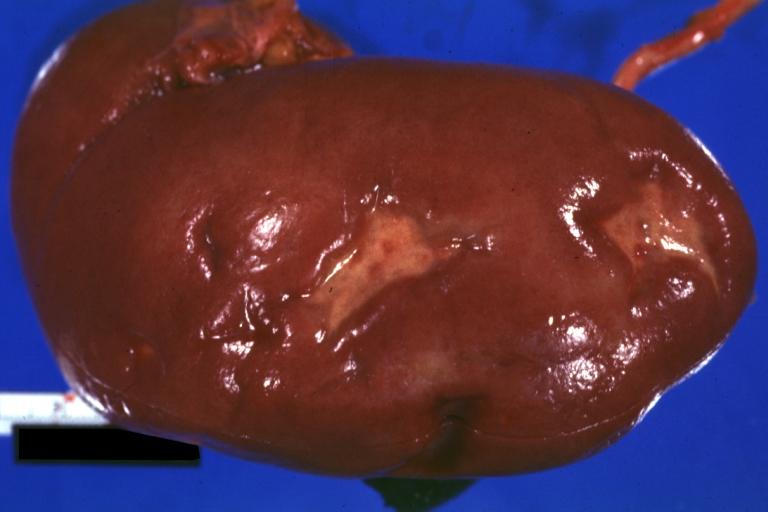 Kidney: Infarct Remote: Gross external view with capsule removed two old and very typical infarct scars 27yobf with dilated cardiomyopathy
Kidney: Infarct Remote: Gross external view with capsule removed two old and very typical infarct scars 27yobf with dilated cardiomyopathy -
 Excessive pedal edema due to right heart failure in a patient with hypertrophic cardiomyopathy (due to functional aortic stenosis from narrow outflow tract)
Excessive pedal edema due to right heart failure in a patient with hypertrophic cardiomyopathy (due to functional aortic stenosis from narrow outflow tract)



References
- ↑ 1.0 1.1 Sisakian H (June 2014). “Cardiomyopathies: Evolution of pathogenesis concepts and potential for new therapies”. World J Cardiol. 6 (6): 478–94. doi:10.4330/wjc.v6.i6.478. PMC 4072838. PMID 24976920.
- ↑ 2.0 2.1 Al-Khatib SM, Fonarow GC, Joglar JA, Inoue L, Mark DB, Lee KL, Kadish A, Bardy G, Sanders GD (June 2017). “Primary Prevention Implantable Cardioverter Defibrillators in Patients With Nonischemic Cardiomyopathy: A Meta-analysis”. JAMA Cardiol. 2 (6): 685–688. doi:10.1001/jamacardio.2017.0630. PMID 28355432. Vancouver style error: initials (help)
- ↑ 3.0 3.1 Wexler RK, Elton T, Pleister A, Feldman D (May 2009). “Cardiomyopathy: an overview”. Am Fam Physician. 79 (9): 778–84. PMID 20141097.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | CT | MRI | Echocardiography | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Guidelines
Guidelines
2023 ESC Guideline Recommendations | 2020 AHA/ACC Guideline for the Diagnosis and Treatment of Patients With Hypertrophic Cardiomyopathy
Case Studies
Case Studies
de:Kardiomyopathie nl:Cardiomyopathie no:Kardiomyopati simple:Cardiomyopathy sr:Кардиомиопатија sv:Hjärtmuskelsjukdom
References
References
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH