
Splenic infarction
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] ; Associate Editor-In-Chief: Asiri Ediriwickrema, M.D., M.H.S. [2] Cafer Zorkun, M.D., Ph.D. [3]
Synonyms and keywords: Spleen infarct, splenic artery thrombosis, splenic artery occlusion,
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Asiri Ediriwickrema, M.D., M.H.S. [2]
Overview
A splenic infarct occurs when the vascular supply for the spleen becomes occluded leading to tissue hypoxia and necrosis. It can be the result of either arterial or venous compromise, and it is associated with multiple of disease states. The most common etiologies include malignancy, hypercoagulable disorders, and embolic disorders.[1][2] It is also common that splenic infarctions are the presenting signs of a previously unknown condition.[3] Patients can be asymptomatic, however, most develop left upper quadrant abdominal pain. Splenic infarction is often diagnosed with computed tomography. Splenic infarcts can be managed medically, however, surgical intervention is indicated if the patient develops complications including hemorrhage, rupture, abscess, or pseudocyst.[4]
Historical Perspective
Classification
Pathophysiology
Causes
Differentiating Splenic infarction overview from Other Diseases
Epidemiology and Demographics
Risk Factors
Screening
Natural History, Complications, and Prognosis
Natural History
Complications
Prognosis
Diagnosis
Diagnostic Criteria
History and Symptoms
Physical Examination
Laboratory Findings
Imaging Findings
Other Diagnostic Studies
Treatment
Medical Therapy
Surgery
Prevention
References
- ↑ Splenic infarction. Radiopedia.org (2015-2016). http://radiopaedia.org/articles/splenic-infarction Accessed on August 27, 2016
- ↑ Antopolsky M, Hiller N, Salameh S, Goldshtein B, Stalnikowicz R (2009). “Splenic infarction: 10 years of experience”. Am J Emerg Med. 27 (3): 262–5. doi:10.1016/j.ajem.2008.02.014. PMID 19328367.
- ↑ Lawrence YR, Pokroy R, Berlowitz D, Aharoni D, Hain D, Breuer GS (2010). “Splenic infarction: an update on William Osler’s observations”. Isr Med Assoc J. 12 (6): 362–5. PMID 20928991.
- ↑ Jaroch MT, Broughan TA, Hermann RE (1986). “The natural history of splenic infarction”. Surgery. 100 (4): 743–50. PMID 3764696. Unknown parameter
|month=ignored (help)
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief:
Please help WikiDoc by adding content here. It’s easy! Click here to learn about editing.
Overview
Historical Perspective
References
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief:
Please help WikiDoc by adding content here. It’s easy! Click here to learn about editing.
Overview
Classification
References
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Pathophysiology
Related Anatomy
The arterial supply to the spleen consists of the splenic artery (a branch of the celiac axis) and the short gastric arteries (branches of the left gastroepiploic artery), which supply the upper pole of the spleen. Even with occlusion of the main splenic artery, collateral flow from the short gastric arteries often may preserve some or all of the splenic parenchyma.
Within the spleen, the arterial supply is segmental. Occlusion of these secondary branches results in the classic wedge-shaped infarct. Most commonly, these infarcts contract and fibrose over time, as demonstrated by the sickle hemoglobinopathies in which repeated episodes of infarction ultimately result in auto-infarction of the spleen.
Pathophysiology
- In diseases such as chronic myeloid leukemia that result in massive splenomegaly secondary to the malignant infiltrative process, segmental infarcts are considered the result of outstripping the available blood supply.
- Splenic vein thrombosis, most commonly the result of pancreatitis or surgery, can result in venous infarction.
- Unusual causes of splenic infarction include malaria, pancreatitis, cocaine use, and splenic infarction occurring as a late complication of liver transplantation.
- An anatomic variant that renders the spleen more susceptible to global infarction is that of the wandering spleen. The spleen is attached by a long vascular pedicle, without the usual fixating ligaments, to the diaphragm, colon, left kidney, and lateral abdominal wall. This allows torsion of the freely mobile spleen around its vascular pedicle, occluding the blood supply and leading to infarction. The treatment is surgical fixation of the spleen (i.e., splenopexy), allowing preservation of the spleen if it has not infarcted as a result of occlusion of the splenic hilum. Techniques include suturing the spleen to the surrounding structures, wrapping it in omentum or mesh prior to suture fixation, or placing it in a surgically created retroperitoneal pouch.
Pathology
A. Brief Descriptions:
- Nearly 99% of infarcts are caused by thromboembolic events, and almost all are the result of arterial occlusions.
- White infarcts are encountered with arterial occlusion and in solid tissues.
B. Gross Findings:
- Recent infarcts are hemorrhagic,whereas older, more fibrotic infarcts are pale yellow-gray.
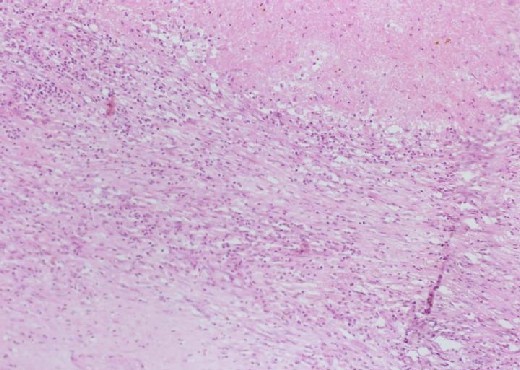
C. Micro Findings:
- Necrotic area with homogenous pinkish appearance.
- Hematoidin crystals can be found in this section.
- Inflammatory cells seated on the margin of infarct area.
Histolopathological Findings
- Pathologic examination of the resected spleen may provide information regarding the pathogenesis of the infarct, e.g. evidence of septic or atheromatous emboli or the presence of an infectious etiology.
-

-
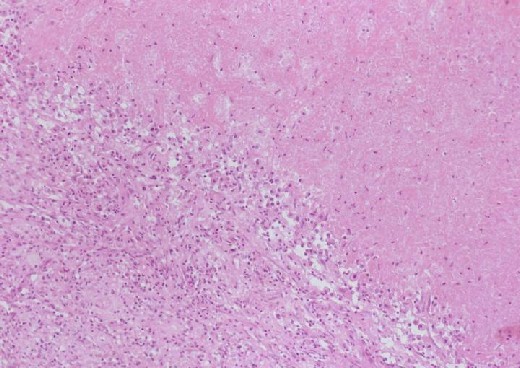 Inflammatory cells seated on the margin of infarct area
Inflammatory cells seated on the margin of infarct area


-
 Inflammatory cells
Inflammatory cells -
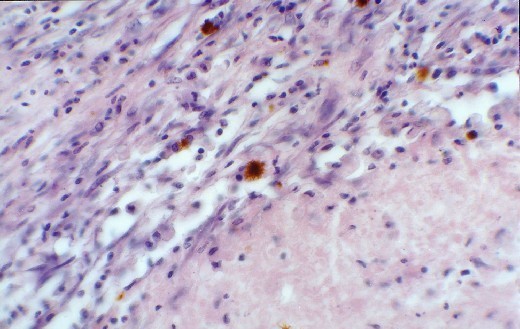 Hemosiderin laden macrophages in the more fibrous areas (junction of infarction)
Hemosiderin laden macrophages in the more fibrous areas (junction of infarction)


-
 Multiple infarcts in a spleen greatly enlarged by malignant lymphoma. The multiple areas of infarction are well demarcated
Multiple infarcts in a spleen greatly enlarged by malignant lymphoma. The multiple areas of infarction are well demarcated

References
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Causes
[1] [2] [3] [4] [5] [6] [7] [8]
Hematologic disorders – Malignant
- Lymphoma (i.e., Hodgkin lymphoma, Non-Hodgkin lymphoma)
Hematologic disorders – Benign
Embolic disorders
- Paradoxical emboli from right heart
- Left ventricular mural thrombus following myocardial infarct
- Infected thoracic aortic graft
- HIV-associated mycobacterial infections
Vascular disorders
Autoimmune/collagen vascular disease
Trauma
- Blunt trauma
- Torsion of the wandering spleen
- Pitressin infusion
- Embolization for splenic bleeding
Operative etiologies
Infections
Medications
Miscellaneous etiologies
- Postpartum toxic shock syndrome
Therapeutic splenic infarction
Splenic infarction can be induced for the treatment of such conditions as portal hypertension or splenic injury[9]. It can also be used prior to splenectomy for the prevention of blood loss.
References
- ↑ Suzuki Y, Shichishima T, Mukae M; et al. (2007). “Splenic infarction after Epstein-Barr virus infection in a patient with hereditary spherocytosis”. Int. J. Hematol. 85 (5): 380–3. doi:10.1532/IJH97.07208. PMID 17562611. Unknown parameter
|month=ignored (help) - ↑ Bonnard P, Guiard-Schmid JB, Develoux M, Rozenbaum W, Pialoux G (2005). “Splenic infarction during acute malaria”. Trans. R. Soc. Trop. Med. Hyg. 99 (1): 82–6. doi:10.1016/j.trstmh.2004.06.005. PMID 15550267. Unknown parameter
|month=ignored (help) - ↑ Florescu D, Sordillo PP, Glyptis A; et al. (2008). “Splenic infarction in human babesiosis: two cases and discussion”. Clin. Infect. Dis. 46 (1): e8–11. doi:10.1086/524081. PMID 18171204. Unknown parameter
|month=ignored (help) - ↑ Breuer C, Janssen G, Laws HJ; et al. (2008). “Splenic infarction in a patient hereditary spherocytosis, protein C deficiency and acute infectious mononucleosis”. Eur. J. Pediatr. 167 (12): 1449–52. doi:10.1007/s00431-008-0781-3. PMID 18604554. Unknown parameter
|month=ignored (help) - ↑ Almeida JA, Riordan SM (2008). “Splenic infarction complicating percutaneous transluminal coeliac artery stenting for chronic mesenteric ischaemia: a case report”. J Med Case Reports. 2: 261. doi:10.1186/1752-1947-2-261. PMC 2533016. PMID 18684317.
- ↑ Rentsch J, McColl G (2000). “Splenic infarction in Wegener’s granulomatosis”. J. Rheumatol. 27 (6): 1554–5. PMID 10852290. Unknown parameter
|month=ignored (help) - ↑ Arora A, Arora S (2006). “Spontaneous splenic infarction associated with sumatriptan use”. J Headache Pain. 7 (4): 214–6. doi:10.1007/s10194-006-0291-5. PMID 16767537. Unknown parameter
|month=ignored (help) - ↑ Malka D, Van den Eynde M, Boige V, Dromain C, Ducreux M (2006). “Splenic infarction and bevacizumab”. Lancet Oncol. 7 (12): 1038. doi:10.1016/S1470-2045(06)70980-9. PMID 17138227. Unknown parameter
|month=ignored (help) - ↑ Haan JM, Bochicchio GV, Kramer N, Scalea TM (2005). “Nonoperative management of blunt splenic injury: a 5-year experience”. J Trauma. 58 (3): 492–8. PMID 15761342. Unknown parameter
|month=ignored (help)
Differentiating Splenic Infarction from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief:
Please help WikiDoc by adding content here. It’s easy! Click here to learn about editing.
Overview
Differential Diagnosis
References
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Epidemiology and Demographics
Splenic infarction is associated most commonly with hematologic disorders. The propensity for splenic infarction in sickle hemoglobinopathies is well known. The mechanism of splenic infarction in sickle cell disease is attributed to crystallization of the abnormal hemoglobin during periods of hypoxia or acidosis.
The rigid erythrocyte leads to rouleaux formation and occlusion of the splenic circulation. In homozygous sickle cell disease, multiple infarcts during childhood commonly result in a scarred, contracted, auto-infarcted spleen by adulthood.
Exposure to low oxygen tension, such as unpressurized airplane travel, or vigorous activity, such as skiing in high altitude locations, also can precipitate sickling and splenic infarction in individuals heterozygous for the sickle trait. Many of these altitude-related episodes can be safely treated with supportive care rather than with splenectomy (Sheikha, 2005).
Although splenic infarct rates of 50% and 72% have been reported in chronic myelogenous leukemia and myelofibrosis respectively, few large series describing this entity exist.
In 1998, Nores reported 59 cases treated over a 30-year period at the University of California, Los Angeles (UCLA) and Cedars-Sinai Medical Center. In 1986, Jaroch identified 75 patients through clinical or autopsy reports at the Cleveland Clinic and found only an additional 77 cases in the literature. Most of the current literature consists of case reports.
Systemic embolization also can result in splenic infarct. It occurs most commonly in the setting of a left atrial or ventricular mural thrombus formed as the result of acute myocardial infarction.
While autopsy series report a 9% incidence of splenic infarction in early deaths following an acute myocardial infarction, clinical series report a much lower incidence of splenic embolization, probably reflecting the silent clinical course of many splenic infarcts.
References
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief:
Please help WikiDoc by adding content here. It’s easy! Click here to learn about editing.
Overview
Risk Factors
References
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief:
Please help WikiDoc by adding content here. It’s easy! Click here to learn about editing.
Overview
Screening
References
Natural History, Complications and Prognosis
Please help WikiDoc by adding more content here. It’s easy! Click here to learn about editing.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Natural History, Complications and Prognosis
Natural History
Complications
- Hemorrhage: Hemorrhage can follow splenectomy due to the intense perisplenic inflammation.
- Splenic bed and/or subphrenic abscess: Abscess is not an uncommon complication. The first line of treatment is radiologic-guided percutaneous drainage.
- Pancreatic fistula: Because of the intimate association of the pancreatic tail and splenic hilum, pancreatic injury can occur, especially in the setting of intense inflammation and/or abscess. The majority of these resolve with nonoperative management, which includes wide drainage, use of a somatostatin analog to decrease exocrine pancreatic function, and either total parenteral nutrition (TPN) or enteral alimentation distal to the ligament of Treitz.
- Gastric fistula: Due to the intense inflammatory reaction that can accompany splenic abscess, the dissection of the spleen from the greater curve of the stomach can be difficult, and inadvertent unrecognized injuries to the greater curve of the stomach do occur. With adequate external drainage and with no obstruction to normal gastric emptying, these can be treated expectantly with TPN or distal luminal alimentation and nasogastric tube decompression.
- Overwhelming postsplenectomy sepsis: As discussed above, the incidence is unknown. The overall postoperative sepsis rate is high because splenectomy often is undertaken for treatment of splenic abscess. The rate of sepsis is due to the cause for the abscess rather than the splenectomy.
Prognosis
References
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | CT | MRI | Ultrasound | Other Imaging Studies | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH