
St. Louis encephalitis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Anthony Gallo, B.S. [2]; Contributor(s): Vishnu Vardhan Serla M.B.B.S. [3]
For patient information, click here
Synonyms and keywords: SLE; SLEV; Saint Louis encephalitis
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Anthony Gallo, B.S. [2]; Contributor(s): Irfan Dotani [3], Vishnu Vardhan Serla M.B.B.S. [4]
Overview
St. Louis encephalitis is a moderate infection of the central nervous system. St. Louis encephalitis virus is a Group IV positive-sense ssRNA virus within the Flaviviridae family of viruses, and the genus Flavivirus. St. Louis encephalitis virus is closely related to Yellow fever virus, Dengue virus, West Nile virus, and Japanese encephalitis.[1] St. Louis encephalitis is also known as an arbovirus, or an arthropod-borne virus. St. Louis encephalitis is usually transmitted via mosquitoes to the human host. St. Louis encephalitis must be differentiated from other diseases that cause nondescript symptoms, which include fever, headache, and vomiting. Prognosis is generally poor. Approximately 5-30% of patients progress to mortality. Among patients who survive, approximately 50% suffer severe neurological, cognitive, and psychological deficits.[2] The diagnostic method of choice for St. Louis encephalitis is laboratory testing. Laboratory findings consistent with the diagnosis of leukocytosis, mild anemia, and hyponatremia. There is no treatment for St. Louis encephalitis; the mainstay of therapy is supportive care.
Historical Perspective
St. Louis encephalitis was first discovered by Dr. Joseph F. Bredeck, an American Director of Public Health for the City of St. Louis, in 1933 following a major outbreak in the city. During Autumn of 1933, over 1,000 cases were reported to local health departments and the National Institute of Health.[3] The previously unknown virus that caused the epidemic was isolated by the NIH team first in monkeys and then in white mice.[4]
Classification
St. Louis encephalitis may be classified according to location of the disease into 2 subtypes: systemic or encephalitic.[5] St. Louis encephalitis may also be classified according to neuroinvasiveness of the disease into two subtypes: neuroinvasive and non-neuroinvasive. St. Louis encephalitis virus is a Group IV positive-sense ssRNA virus within the Flaviviridae family of viruses, and the genus Flavivirus. St. Louis encephalitis is also known as an arbovirus, or an arthopod-borne virus.[6]
Pathophysiology
St. Louis encephalitis virus is usually transmitted via mosquitos (generally from the genus Culex) to the human host. St. Louis encephalitis virus contains positive-sense viral RNA. Transmission to humans requires mosquito species capable of creating a “bridge” between infected animals and uninfected humans. The incubation period is 5-15 days. Humans are dead-end hosts for the virus, meaning there is an insufficient amount of St. Louis encephalitis virus in the blood stream to infect a mosquito; there is also no evidence of person to person spread.[7]
Causes
St. Louis encephalitis may be caused by St. Louis encephalitis virus. St. Louis encephalitis virus is closely related to the West Nile virus, Dengue virus, Murray Valley encephalitis virus, and Japanese encephalitis virus.[8]
Differentiating St. Louis encephalitis from other Diseases
St. Louis encephalitis must be differentiated from other diseases that cause nondescript symptoms, which include fever, headache, myalgia, and vomiting, such as meningitis, brain abscess, and demyelinating diseases.[9]
Epidemiology and Demographics
The incidence of St. Louis encephalitis is approximately 192 per 100,000 individuals worldwide. The majority of St. Louis encephalitis cases are reported in the United States. In the United States, the annual number of reported St. Louis encephalitis cases reported fluctuate widely, as a result of periodic epidemics. St. Louis encephalitis infection is thought to confer lifelong immunity against reinfection. The case fatality rate of St. Louis encephalitis ranges between 5-30%, with higher rates among the elderly, worldwide. St. Louis encephalitis affects men and women equally. There is no racial predilection to the development of St. Louis encephalitis. Patients of all age groups may develop St. Louis encephalitis.[10]
Risk Factors
The most potent risk factor in the development of St. Louis encephalitis is old age. Common risk factors include immunosuppression, mosquito contact, and visits to Central and South America.[11]
Screening
According to the Centers for Disease Control and Prevention, there is insufficient evidence to recommend routine screening for St. Louis encephalitis.[12]
Natural History, Complications and Prognosis
If left untreated, approxomatly 40% of patients with St. Louis encephalitis may progress to develop fever, headache, or aseptic meningitis.[13] Common complications of St. Louis encephalitis include seizures, coma, disorientation, spastic paralysis, and hemorrhage.[14] Prognosis is generally poor. Approximately 5-15% of patients progress to mortality. Among patients who survive, approximately 50% suffer severe neurological, cognitive, or psychological deficits.
Diagnosis
History and Symptoms
If possible, a detailed and thorough history from the patient is necessary. Most patients infected with St. Louis encephalitis remain asymptomatic. Less than 1% of St. Louis encephalitis infections are clinically apparent and the vast majority of infections remain undiagnosed.[5] The incubation period for St. Louis encephalitis is usually 5-15 days. Common symptoms of St. Louis encephalitis include fever, headache, and dizziness.[15]
Physical Examination
Patients with St. Louis encephalitis are usually ill-appearing. Physical examination of patients with St. Louis encephalitis is usually remarkable for fever, convulsions, and hemorrhage.[13][15]
Laboratory Findings
The diagnostic method of choice for St. Louis encephalitis is laboratory testing. In St. Louis encephalitis, cerebrospinal fluid examination shows a moderate (typically lymphocytic) pleocytosis. 2/3 of patients with St. Louis encephalitis may have elevated concentration of CSF protein, which usually indicative of neuroinvasive disease. In the absence of a sensitive and non-invasive virus detection method, serologic testing is the primary method for diagnosing St. Louis encephalitis.[5][13][16]
Imaging Findings
Electrocardiogram
There are no electrocardiogram findings associated with St. Louis encephalitis.
X Ray
There are no x ray findings associated with St. Louis encephalitis.
CT
There are no CT findings associated with St. Louis encephalitis.[17][18]
MRI
MRI is the imaging modality of choice for St. Louis encephalitis. Findings of St. Louis encephalitis include substantia nigra edema, hemorrhage, and restricted diffusion in the basal ganglia and thalamus.[18][19][20]
Echocardiography or Ultrasound
There are no echocardiography or ultrasound findings associated with St. Louis encephalitis.[21]
EEG
On other imaging findings, St. Louis encephalitis is characterized by generalized slowing without focal activity, a persistent vegetative state, and brain death.[22]
Other Diagnostic Studies
Ultrasound-guided aspiration, via transdural insonation, has proven to show excellent abscess visualization when performed through a burr hole.
At the time of aspiration, specimens should be sent for Gram stain and routine aerobic and anaerobic cultures.[23]
Treatment
Medical Therapy
There is no treatment for St. Louis encephalitis; the mainstay of therapy for St. Louis encephalitis is supportive care.[5][13]
Surgery
Surgical intervention is not recommended for the management of St. Louis encephalitis.
Primary Prevention
There are no available vaccines against St. Louis encephalitis virus. Primary prevention strategies include the use of repellent, protective clothing, window screens, and the reduction of uncontrolled mosquito populations.[12][24]
Secondary Prevention
There are no secondary preventative measures available for St. Louis encephalitis.[12]
References
- ↑ Flavivirus. SIB Swiss Institute of Bioinformatics (2015). http://viralzone.expasy.org/viralzone/all_by_species/24.html Accessed on April 12, 2016
- ↑ Khandaker G, Zurynski Y, Buttery J, Marshall H, Richmond PC, Dale RC; et al. (2012). “Neurologic complications of influenza A(H1N1)pdm09: surveillance in 6 pediatric hospitals”. Neurology. 79 (14): 1474–81. doi:10.1212/WNL.0b013e31826d5ea7. PMC 4098823. PMID 22993280.
- ↑ “ENCEPHALITIS IN ST. LOUIS”. Am J Public Health Nations Health. 23 (10): 1058–60. 1933. PMC 1558319. PMID 18013846.
- ↑ Diaz LA, Nemeth NM, Bowen RA, Almiron WR, Contigiani MS (2011). “Comparison of argentinean saint louis encephalitis virus non-epidemic and epidemic strain infections in an avian model”. PLoS Negl Trop Dis. 5 (5): e1177. doi:10.1371/journal.pntd.0001177. PMC 3101189. PMID 21629729.
- ↑ 5.0 5.1 5.2 5.3 Saint Louis Encephalitis Virus (SLEV). Wisonsin Department of Health Services (2015). https://www.dhs.wisconsin.gov/arboviral/stlouisencephalitis.htm Accessed on July 28, 2016.
- ↑ May FJ, Li L, Zhang S, Guzman H, Beasley DW, Tesh RB; et al. (2008). “Genetic variation of St. Louis encephalitis virus”. J Gen Virol. 89 (Pt 8): 1901–10. doi:10.1099/vir.0.2008/000190-0. PMC 2696384. PMID 18632961.
- ↑ Saint Louis Encephalitis Transmission. Centers for Disease Control and Prevention (CDC), National Center for Emerging and Zoonotic Infectious Diseases, Division of Vector-Borne Diseases. (2010) http://www.cdc.gov/sle/technical/transmission.html Accessed on May 3, 2016.
- ↑ Rastogi M, Sharma N, Singh SK (2016). “Flavivirus NS1: a multifaceted enigmatic viral protein”. Virol J. 13 (1): 131. doi:10.1186/s12985-016-0590-7. PMID 27473856.
- ↑ Burgueño A, Spinsanti L, Díaz LA, Rivarola ME, Arbiza J, Contigiani M; et al. (2013). “Seroprevalence of St. Louis encephalitis virus and West Nile virus (Flavivirus, Flaviviridae) in horses, Uruguay”. Biomed Res Int. 2013: 582957. doi:10.1155/2013/582957. PMC 3891745. PMID 24490165.
- ↑ Bell RL, Christensen B, Holguin A, Smith O (1981). “St. Louis encephalitis: a comparison of two epidemics in Harris county, Texas”. Am J Public Health. 71 (2): 168–70. PMC 1619618. PMID 6109458.
- ↑ ST. LOUIS ENCEPHALITIS VIRUS. Public Health Agency of Canada(2011). http://www.phac-aspc.gc.ca/lab-bio/res/psds-ftss/st-louis-encephalit-eng.php Accessed on August 1, 2016.
- ↑ 12.0 12.1 12.2 Japanese encephalitis – Frequently Asked Questions. CDC Centers for Disease Control and Prevention. (2015) http://www.cdc.gov/japaneseencephalitis/qa/index.html Accessed on April 12, 2016
- ↑ 13.0 13.1 13.2 13.3 Saint Louis Encephalitis. Centers for Disease Control, and Prevention (2010). https://www.cdc.gov/sle/technical/symptoms.html Accessed on July 29, 2016.
- ↑ Flavivirus encephalitis. Radiopaedia.org (2015). http://radiopaedia.org/articles/flavivirus-encephalitis Accessed on July 29, 2016.
- ↑ 15.0 15.1 Carballo C, Cabana M, Ledezma F, Pascual C, Cazes C, Mistchenko A; et al. (2016). “[Saint Louis encephalitis: case report]”. Arch Argent Pediatr. 114 (4): e268–71. doi:10.5546/aap.2016.e268. PMID 27399031.
- ↑ Day JF, Shaman J (2009). “Severe winter freezes enhance St. Louis encephalitis virus amplification and epidemic transmission in peninsular Florida”. J Med Entomol. 46 (6): 1498–506. PMID 19960704.
- ↑ Brain Imaging. American Journal of Neuroradiology(2016). http://www.ajnr.org/content/20/7/1281.full Accessed on July 27, 2016
- ↑ 18.0 18.1 Flavivirus encephalitis. Radiopaedia.org(2015).http://radiopaedia.org/articles/flavivirus-encephalitis Accessed on July 27, 2016
- ↑ St. Louis Encephalitis and the Substantia Nigra: MR Imaging Evaluation.(1999). http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.321.6020&rep=rep1&type=pdf Accessed on July 27, 2016
- ↑ Wasay M, Diaz-Arrastia R, Suss RA, Kojan S, Haq A, Burns D; et al. (2000). “St Louis encephalitis: a review of 11 cases in a 1995 Dallas, Tex, epidemic”. Arch Neurol. 57 (1): 114–8. PMID 10634457.
- ↑ Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Disease. (2015). Accessed on July 27, 2016
- ↑ Zhao J, Vijay R, Zhao J, Gale M, Diamond MS, Perlman S (2016). “MAVS Expressed by Hematopoietic Cells Is Critical for Control of West Nile Virus Infection and Pathogenesis”. J Virol. 90 (16): 7098–108. doi:10.1128/JVI.00707-16. PMID 27226371.
- ↑ John E. Bennett, Raphael Dolin, Martin J. Blaser “Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases” (2014): 1171.
- ↑ McAuley AJ, Torres M, Plante JA, Huang CY, Bente DA, Beasley DW (2016). “Recovery of West Nile Virus Envelope Protein Domain III Chimeras with Altered Antigenicity and Mouse Virulence”. J Virol. 90 (9): 4757–70. doi:10.1128/JVI.02861-15. PMC 4836310. PMID 26912625.
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Anthony Gallo, B.S. [2]; Contributor(s): Irfan Dotani [3]
Overview
St. Louis encephalitis was first discovered by Dr. Joseph F. Bredeck, an American Director of Public Health for the City of St. Louis, in 1933 following a major outbreak in the city. During Autumn of 1933, over 1,000 cases were reported to local health departments and the National Institute of Health.[1][2][3] The previously unknown virus that caused the epidemic was isolated by the NIH team first in monkeys and then in white mice.[4]
Historical Perspective
St. Louis encephalitis was first discovered by Dr. Joseph F. Bredeck, an American Director of Public Health for the City of St. Louis, in 1933 following a major outbreak in the city. During Autumn of 1933, over 1,000 cases were reported to local health departments and the National Institute of Health. The previously unknown virus that caused the epidemic was isolated by the NIH team first in monkeys and then in white mice.[4] There have been several outbreaks of St. Louis encephalitis which are summarized below:[1][2][3][5][6]
| Year of Epidemic | Description of Epidemic |
|---|---|
| 1933 | In 1933, St. Louis encephalitis was first founded by Dr. Joseph F. Bredeck after 77 cases and 14 deaths were confirmed. |
| 1959 | In 1959, an outbreak of St. Louis encephalitis resulted in 31 confirmed cases, including 24 deaths. |
| 1961 | In 1961, an outbreak of St. Louis encephalitis in Tampa Bay, Florida resulted in 32 cases, including 7 deaths. |
| 1965 | In 1965, an outbreak of St. Louis encephalitis resulted in 265 confirmed cases, including 43 deaths. |
| 1977 | In 1977, an outbreak of St. Louis encephalitis resulted in 110 confirmed cases, including 32 presumptive cases. |
| 1980 | In 1980, an outbreak of St. Louis encephalitis resulted in 729 cases, including 4 deaths. |
| 1990 | In 1990, an outbreak of St. Louis encephalitis resulted in 64 confirmed, including 26 presumptive cases. |
References
- ↑ 1.0 1.1 “ENCEPHALITIS IN ST. LOUIS”. Am J Public Health Nations Health. 23 (10): 1058–60. 1933. PMC 1558319. PMID 18013846.
- ↑ 2.0 2.1 Bredeck JF (1933). “The Story of the Epidemic of Encephalitis in St. Louis”. Am J Public Health Nations Health. 23 (11): 1135–40. PMC 1558406. PMID 18013860.
- ↑ 3.0 3.1 Epidemiologic Notes and Reports St. Louis Encephalitis — Baytown and Houston, Texas. Centers for Disease Control and Prevention (1998). http://www.cdc.gov/mmwr/preview/mmwrhtml/00000817.htm Accessed July 28, 2016.
- ↑ 4.0 4.1 Edward A. Beeman: Charles Armstrong, M.D.: A Biography; 2007; p. 305; also online here (PDF).
- ↑ SAINT LOUIS ENCEPHALITIS: A FLORIDA PROBLEM. Florida Medical Entomology Laboratory. http://mosquito.ifas.ufl.edu/SLE.htm Accessed on May 3, 2016.
- ↑ Current Trends Update: St. Louis Encephalitis — Florida and Texas, 1990. Centers for Disease Control and Prevention (1998). http://www.cdc.gov/mmwr/preview/mmwrhtml/00001813.htm Accessed on July 28, 2016.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Anthony Gallo, B.S. [2]; Contributor(s): Irfan Dotani [3]
Overview
St. Louis encephalitis may be classified according to location of the disease into 2 subtypes: systemic or encephalitic.[1][2] St. Louis encephalitis may also be classified according to neuroinvasiveness of the disease into two subtypes: neuroinvasive and non-neuroinvasive. St. Louis encephalitis virus is a Group IV positive-sense ssRNA virus within the Flaviviridae family of viruses, and the genus Flavivirus. St. Louis encephalitis is also known as an arbovirus, or an arthopod-borne virus.[3]
Classification
St. Louis encephalitis may be classified according to location of the disease into 2 subtypes: systemic or encephalitic.[1][2] St. Louis encephalitis may also be classified according to neuroinvasiveness of the disease into two subtypes: neuroinvasive and non-neuroinvasive. St. Louis encephalitis virus is a Group IV positive-sense ssRNA virus within the Flaviviridae family of viruses, and the genus Flavivirus. St. Louis encephalitis is also known as an arbovirus, or an arthopod-borne virus.[3]
References
- ↑ 1.0 1.1 Saint Louis Encephalitis. Centers for Disease Control and Prevention (2010). http://www.cdc.gov/sle/ Accessed on July 28, 2016.
- ↑ 2.0 2.1 Saint Louis Encephalitis Virus (SLEV). Wisonsin Department of Health Services (2015). https://www.dhs.wisconsin.gov/arboviral/stlouisencephalitis.htm Accessed on July 28, 2016.
- ↑ 3.0 3.1 Genetic variation of St. Louis encephalitis virus. Journal of General Virology (2008). http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2696384/ Accessed on July 28, 2016.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Anthony Gallo, B.S. [2]; Contributor(s): Irfan Dotani [3], Vishnu Vardhan Serla M.B.B.S. [4]
Overview
St. Louis encephalitis virus is usually transmitted via mosquitos (generally from the genus Culex) to the human host. St. Louis encephalitis virus contains positive-sense viral RNA. Transmission to humans requires mosquito species capable of creating a “bridge” between infected animals and uninfected humans. The incubation period is 5-15 days.[1] Humans are dead-end hosts for the virus, meaning there is an insufficient amount of St. Louis encephalitis virus in the blood stream to infect a mosquito; there is also no evidence of person to person spread.[2]
Pathophysiology
St. Louis encephalitis virus is usually transmitted via mosquitos to the human host. St. Louis encephalitis virus contains positive-sense viral RNA; this RNA has its genome directly utilized as if it were mRNA, producing a single protein which is modified by host and viral proteins to form the various proteins needed for replication. The following table is a summary of the St. Louis encephalitis virus:[3][4]
| Characteristic | Data |
|---|---|
| Nucleic acid | RNA |
| Sense | ssRNA(+) |
| Virion | Enveloped |
| Capsid | Spherical |
| Symmetry | Yes; T=3-like organization; icosahedral-like |
| Capsid monomers | Unknown |
| Envelope length (diameter) | 50 nm |
| Additional envelope information | Mature virons contain 2 virus-encoded membrane proteins (M and E); immature virons contain a protein precursor |
| Genome shape | Linear |
| Genome length | 10-11 kb |
| Nucleotide cap | Yes |
| Polyadenylated tail | No; a loop structure is formed instead |
| Incubation period | 5-15 days |
St. Louis encephalitis is contracted by the bite of an infected mosquito, primarily Culex pipiens, Culex tarsalis, or Culex nigripalpus. St. Louis encephalitis virus circulates between a mosquito vector and birds in the United States and South America.[5] Transmission to humans requires mosquito species capable of creating a “bridge” between infected animals and uninfected humans; this occurs when humans become part of the enzootic cycle.[1] Humans are dead-end hosts for the virus, meaning there is an insufficient amount of St. Louis encephalitis virus in the blood stream to infect another human. There is no evidence of St. Louis encephalitis transmission from person to person.[2]
St. Louis encephalitis virus is transmitted in the following pattern:[3]
- Attachment of the viral envelope protein E to host receptors mediates internalization into the host cell by clathrin-mediated endocytosis, or by apoptotic mimicry.
- Fusion of virus membrane with host endosomal membrane. RNA genome is released into the cytoplasm.
- The positive-sense ssRNA virus is translated into a polyprotein, which is cleaved into all structural and non-structural proteins necessary for RNA synthesis (replication and transcription).
- Replication takes place at the surface of endoplasmic reticulum in cytoplasmic viral factories. A dsRNA genome is synthesized from the genomic ssRNA(+).
- The dsRNA genome is transcribed/replicated, thereby providing viral mRNAs/new ssRNA(+) genomes.
- Virus assembly occurs at the endoplasmic reticulum. The virion buds via the host endosomal sorting complexes required for transport (ESCRT), and is sent to the Golgi apparatus.
- The prM protein is cleaved in the Golgi, thereby maturing the virion which is fusion competent.
- New virions are released by exocytosis.
Histopathological
On microscopic histopathological analysis, the enveloped, spherical, and icosahedral-like virion shape are characteristic findings of St. Louis encephalitis.
Genetics
The phylogeny, genetic variation, and recombination dynamics, and envelope protein genes St. Louis encephalitis virion have been sequenced.[6][7][8][9]
Evolutionary evidence suggests that North American strains of St. Louis encephalitis virus belonged to a single clade.[10] Furthermore, this study found an increase in the effective population size of the St. Louis encephalitis virus around the end of the 19th century that corresponds to the split of the latest North American clade; this finding suggests a northwards colonization of St. Louis encephalitis virus in the Americas. The virus is believed to have originated northern Mexico and migrated northwards with birds.
Gallery
-
 Culex tarsalis, one of the major vectors of St. Louis encephalitis virus.
Culex tarsalis, one of the major vectors of St. Louis encephalitis virus. -
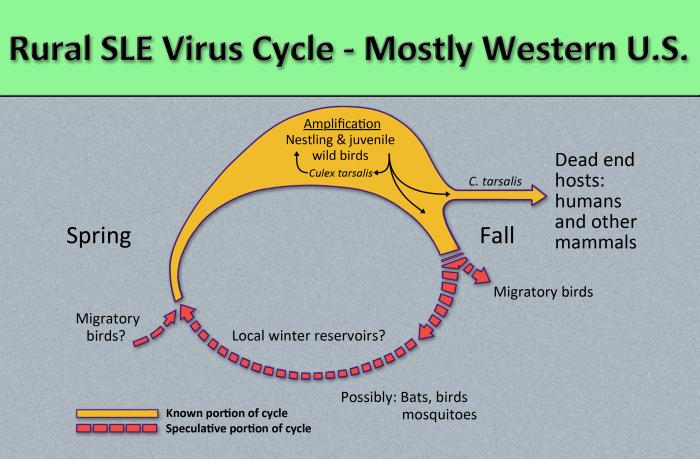
![Diagram illustrates the methods by which the arbovirus, St. Louis encephalitis virus, reproduces and amplifies itself in urban avian populations, and transmitted to dead end hosts including humans and other mammals by Culex spp. mosquitos. From Public Health Image Library (PHIL). [11]](https://www.wikidoc.org/images/5/56/Flavivirus03.jpeg) Diagram illustrates the methods by which the arbovirus, St. Louis encephalitis virus, reproduces and amplifies itself in urban avian populations, and transmitted to dead end hosts including humans and other mammals by Culex spp. mosquitos. From Public Health Image Library (PHIL). [11]
Diagram illustrates the methods by which the arbovirus, St. Louis encephalitis virus, reproduces and amplifies itself in urban avian populations, and transmitted to dead end hosts including humans and other mammals by Culex spp. mosquitos. From Public Health Image Library (PHIL). [11] -
 title = Public Health
title = Public Health

![Diagram illustrates the methods by which the arbovirus, St. Louis encephalitis virus, reproduces and amplifies itself in urban avian populations, and transmitted to dead end hosts including humans and other mammals by Culex spp. mosquitos. From Public Health Image Library (PHIL). [11]](https://www.wikidoc.org/index.php/File%3AFlavivirus03.jpeg)

References
- ↑ 1.0 1.1 Saint Louis Encephalitis. Centers for Disease Control and Prevention (CDC), National Center for Emerging and Zoonotic Infectious Diseases, Division of Vector-Borne Diseases. (2010) http://www.cdc.gov/sle/general/qa.html Accessed on May 3, 2016.
- ↑ 2.0 2.1 Saint Louis Encephalitis Transmission. Centers for Disease Control and Prevention (CDC), National Center for Emerging and Zoonotic Infectious Diseases, Division of Vector-Borne Diseases. (2010) http://www.cdc.gov/sle/technical/transmission.html Accessed on May 3, 2016.
- ↑ 3.0 3.1 Flavivirus. SIB Swiss Institute of Bioinformatics. (2015) http://viralzone.expasy.org/viralzone/all_by_species/24.html Accessed on April 12, 2016
- ↑ Japanese encephalitis – Frequently Asked Questions. CDC Centers for Disease Control and Prevention. (2015) http://www.cdc.gov/japaneseencephalitis/qa/index.html Accessed on April 12, 2016
- ↑ The Management of Encephalitis: Clinical Practice Guidelines by the Infectious Diseases Society of America. http://www.idsociety.org/uploadedFiles/IDSA/Guidelines-Patient_Care/PDF_Library/Encephalitis.pdf Accessed on May 3, 2016.
- ↑ Kramer LD, Presser SB, Hardy JL, Jackson AO. (1997) Genotypic and phenotypic variation of selected Saint Louis encephalitis viral strains isolated in California. American Journal of Tropical Medicine and Hygiene 57(2):222–229. Abstract
- ↑ Kramer LD, Chandler LJ. (2001) Phylogenetic analysis of the envelope gene of St. Louis encephalitis virus. Archives of Virology 146(12):2341–2355. doi:10.1007/s007050170007.
- ↑ Twiddy SS, Holmes EC. (2003) The extent of homologous recombination in members of the genus Flavivirus. Journal of General Virology 84:429-440. doi:10.1099/vir.0.18660-0.
- ↑ May FJ, Li L, Zhang S, Guzman H, Beasley DW, Tesh RB, Higgs S, Raj P, Bueno R Jr, Randle Y, Chandler L, Barrett AD. (2008) Genetic variation of St. Louis encephalitis virus. Journal of General Virology 89(8):1901-1910. doi:10.1099/vir.0.2008/000190-0.
- ↑ Baillie GJ, Kolokotronis SO, Waltari E, Maffei JG, Kramer LD, Perkins SL. (2008) Phylogenetic and evolutionary analyses of St. Louis encephalitis virus genomes. Molecular Phylogenetics and Evolution 47(2):717-728. doi:10.1016/j.ympev.2008.02.015.
- ↑ “Public Health Image Library (PHIL)”.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Anthony Gallo, B.S. [2]; Contributor(s): Irfan Dotani [3], Vishnu Vardhan Serla M.B.B.S. [4]
Overview
St. Louis encephalitis may be caused by St. Louis encephalitis virus. St. Louis encephalitis virus is closely related to the West Nile virus, Dengue virus, Murray Valley encephalitis virus, and Japanese encephalitis virus.[1]
Causes
St. Louis encephalitis may be caused by St. Louis encephalitis virus. St. Louis encephalitis virus is closely related to the West Nile virus, Dengue virus, Murray Valley encephalitis virus, and Japanese encephalitis virus.[1]
References
- ↑ 1.0 1.1 Flavivirus. SIB Swiss Institute of Bioinformatics (2015). http://viralzone.expasy.org/viralzone/all_by_species/24.html Accessed on July 29, 2016
Differentiating St. Louis encephalitis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Anthony Gallo, B.S. [2]; Contributor(s): Irfan Dotani [3]
Overview
St. Louis encephalitis must be differentiated from other diseases that cause nondescript symptoms, which include fever, headache, myalgia, and vomiting, such as meningitis, brain abscess, and demyelinating diseases.
Differentiating St. Louis encephalitis from Other Diseases
St. Louis encephalitis must be differentiated from other diseases that cause fever, headache, myalgia, and vomiting, such as:[1][2][3][4][5]
| Disease | Similarities | Differentials |
|---|---|---|
| Meningitis | Classic triad of fever, nuchal rigidity, and altered mental status | Photophobia, phonophobia, rash associated with meningococcemia, concomitant sinusitis or otitis, swelling of the fontanelle in infants (0-6 months) |
| Brain abscess | Fever, headache, hemiparesis | Varies depending on the location of the abscess; clinically, visual disturbance including papilledema, decreased sensation; on imaging, a lesion demonstrates both ring enhancement and central restricted diffusion |
| Demyelinating diseases | Ataxia, lethargy | Multiple sclerosis: clinically, nystagmus, internuclear ophthalmoplegia, Lhermitte’s sign; on imaging, well-demarcated ovoid lesions with possible T1 hypointensities (“black holes”)
Acute disseminated encephalomyelitis: clinically, somnolence, myoclonic movements, and hemiparesis ; on imaging, diffuse or multi-lesion enhancement, with indistinct lesion borders |
| Substance abuse | Tremor, headache, altered mental status | Varies depending on type of substance: prior history, drug-seeking behavior, attention-seeking behavior, paranoia, sudden panic, anxiety, hallucinations |
| Electrolyte disturbance | Fatigue, headache, nausea | Varies depending on deficient ions; clinically, edema, constipation, hallucinations; on EKG, abnormalities in T wave, P wave, QRS complex; possible presentations include arrhythmia, dehydration, renal failure |
| Stroke | Ataxia, aphasia, dizziness | Varies depending on classification of stroke; presents with positional vertigo, high blood pressure, extremity weakness |
| Intracranial hemorrhage | Headache, coma, dizziness | Lobar hemorrhage, numbness, tingling, hypertension, hemorrhagic diathesis |
| Trauma | Headache, altered mental status | Amnesia, loss of consciousness, dizziness, concussion, contusion |
References
- ↑ M.D. JE, Dolin R, Blaser MJ. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, Expert Consult Premium Edition. Saunders; 2014.
- ↑ Kennedy PG (2004). “Viral encephalitis: causes, differential diagnosis, and management”. J Neurol Neurosurg Psychiatry. 75 Suppl 1: i10–5. PMC 1765650. PMID 14978145.
- ↑ Arboviral Infections (arthropod-borne encephalitis, eastern equine encephalitis, St. Louis encephalitis, California encephalitis, Powassan encephalitis, West Nile encephalitis). New York State Department of Health (2006). https://www.health.ny.gov/diseases/communicable/arboviral/fact_sheet.htm Accessed on February 23, 2016
- ↑ Eckstein C, Saidha S, Levy M (2012). “A differential diagnosis of central nervous system demyelination: beyond multiple sclerosis”. J Neurol. 259 (5): 801–16. doi:10.1007/s00415-011-6240-5. PMID 21932127.
- ↑ De Kruijk JR, Twijnstra A, Leffers P (2001). “Diagnostic criteria and differential diagnosis of mild traumatic brain injury”. Brain Inj. 15 (2): 99–106. doi:10.1080/026990501458335. PMID 11260760.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Anthony Gallo, B.S. [2]; Contributor(s): Irfan Dotani [3], Vishnu Vardhan Serla M.B.B.S. [4]
Overview
The incidence of St. Louis encephalitis is approximately 192 per 100,000 individuals worldwide. The majority of St. Louis encephalitis cases are reported in the United States. In the United States, the annual number of reported St. Louis encephalitis cases reported fluctuate widely, as a result of periodic epidemics. St. Louis encephalitis infection is thought to confer lifelong immunity against reinfection. The case fatality rate of St. Louis encephalitis ranges between 5-30%, with higher rates among the elderly, worldwide.[1] St. Louis encephalitis affects men and women equally. There is no racial predilection to the development of St. Louis encephalitis.[2] Patients of all age groups may develop St. Louis encephalitis.[1]
Epidemiology and Demographics
Incidence
The incidence of St. Louis encephalitis is approximately 192 per 100,000 individuals worldwide. The majority of St. Louis encephalitis cases are reported in the United States. In the United States, the annual number of reported St. Louis encephalitis neuroinvasive disease cases reported fluctuates widely, as a result of periodic epidemics. St. Louis encephalitis infection is thought to confer lifelong immunity against reinfection.[2] From 2004-2013, an average of 7 cases were reported annually.[2]


Case Fatality Rate
The case fatality rate of St. Louis encephalitis ranges between 5-30%, with higher rates among the elderly, worldwide.[1]
Age
St. Louis encephalitis is a rare disease that tends to affect the elderly and patients <6 months of age. Patients of all age groups may develop St. Louis encephalitis.[1]
Race
There is no racial predilection to the development of St. Louis encephalitis.[2]
Gender
St. Louis encephalitis affects men and women equally.[2]
Geographical Region
In temperate areas of the United States, St. Louis encephalitis primarily occurs in late summer or early fall. In Southern states, where the climate is milder, cases may occur year round. Although the geographic range of the virus extends from Canada to Argentina, human cases have almost exclusively occurred in the United States. The majority of cases have occurred in Eastern and Central states, where episodic urban-centered outbreaks have recurred since the 1930s. The largest epidemic of St. Louis encephalitis occurred in the United States in 1975, with nearly 2,000 cases reported, primarily from the Central states in the Ohio-Mississippi River Basin.[3]



References
- ↑ 1.0 1.1 1.2 1.3 St. Louis Encephalitis. http://www.gcmad.org/Documents/St_Louis_Encephalitis.pdf Accessed July 28, 2016.
- ↑ 2.0 2.1 2.2 2.3 2.4 Saint Louis Encephalitis. Centers for Disease Control and Prevention (2009). https://www.cdc.gov/sle/technical/fact.html Accessed July 28, 2016.
- ↑ Impact of the West Nile virus on the Natural History of St. Louis Encephalitis. (2008). http://scholarcommons.usf.edu/cgi/viewcontent.cgi?article=1437&context=etd Accessed on July 28, 2016.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Anthony Gallo, B.S. [2]; Contributor(s): Vishnu Vardhan Serla M.B.B.S. [3], Irfan Dotani [4]
Overview
The most potent risk factor in the development of St. Louis encephalitis is old age. Common risk factors include immunosuppression, mosquito contact, and visits to Central and South America.
Risk Factors
The most potent risk factor in the development of St. Louis encephalitis is old age. Other risk factors in the development of St. Louis encephalitis are:[1][2][3]
- Immunosuppression
- Residing or visiting woodland areas
- Mosquito contact
- Bird contact
- Outdoor recreational activities
- Low income
- Travel to Central and South America
- Children
- Summer season
References
- ↑ Japanese encephalitis – Frequently Asked Questions. CDC Centers for Disease Control and Prevention. (2015) http://www.cdc.gov/japaneseencephalitis/qa/index.html Accessed on April 12, 2016
- ↑ Bagdure D, Custer JW, Rao S, Messacar K, Dominguez S, Beam BW; et al. (2016). “Hospitalized Children With Encephalitis in the United States: A Pediatric Health Information System Database Study”. Pediatr Neurol. doi:10.1016/j.pediatrneurol.2016.04.014. PMID 27353693.
- ↑ Day JF, Tabachnick WJ, Smartt CT (2015). “Factors That Influence the Transmission of West Nile Virus in Florida”. J Med Entomol. 52 (5): 743–54. doi:10.1093/jme/tjv076. PMID 26336216.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Anthony Gallo, B.S. [2]; Contributor(s): Irfan Dotani [3]
Overview
According to the Centers for Disease Control and Prevention, there is insufficient evidence to recommend routine screening for St. Louis encephalitis.
Screening
According to the Centers for Disease Control and Prevention, there is insufficient evidence to recommend routine screening for St. Louis encephalitis.[1]
References
- ↑ Japanese encephalitis – Frequently Asked Questions. CDC Centers for Disease Control and Prevention. (2015) http://www.cdc.gov/japaneseencephalitis/qa/index.html Accessed on April 12, 2016
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Anthony Gallo, B.S. [2]; Contributor(s): Irfan Dotani [3], Vishnu Vardhan Serla M.B.B.S. [4]
Overview
If left untreated, approxomatly 40% of patients with St. Louis encephalitis may progress to develop fever, headache, or aseptic meningitis.[1] Common complications of St. Louis encephalitis include seizures, coma, disorientation, spastic paralysis, and hemorrhage.[2] Prognosis is generally poor. Approximately 5-15% of patients progress to mortality. Among patients who survive, approximately 50% suffer severe neurological, cognitive, or psychological deficits.[1][3]
Natural History
If left untreated, approxomatly 40% of patients with St. Louis encephalitis may progress to develop fever, headache, or aseptic meningitis.[1]
Complications
Common complications of St. Louis encephalitis include:[2]
Prognosis
Prognosis is generally poor. Approximately 5-15% of patients progress to mortality. Among patients who survive, approximately 50% suffer severe neurological, cognitive, or psychological deficits.[3][4]
References
- ↑ 1.0 1.1 1.2 Saint Louis Encephalitis. Centers for Disease Control, and Prevention (2010). https://www.cdc.gov/sle/technical/symptoms.html Accessed on July 29, 2016.
- ↑ 2.0 2.1 Flavivirus encephalitis. Radiopaedia.org (2015). http://radiopaedia.org/articles/flavivirus-encephalitis Accessed on July 29, 2016.
- ↑ 3.0 3.1 Yellow Fever. MedlinePlus (2015). https://medlineplus.gov/ency/article/001365.htm Accessed on July 29, 2016.
- ↑ Meningitis and Encephalitis Fact Sheet. National Institute of Neurological Disorders and Stroke (2016). http://www.ninds.nih.gov/disorders/encephalitis_meningitis/detail_encephalitis_meningitis.htm#3083_9 Accessed on July 29, 2016.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | X Ray | CT | MRI | Echocardiography or Ultrasound | Other Imaging Findings |Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH