
Radial artery catheterization
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.; Ayokunle Olubaniyi, M.B,B.S [2]
Synonyms and Keywords: Radial first, Radialfirst, Radialfirst, Radial approach, Right radial, Left radial, Go radial
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ayokunle Olubaniyi, M.B,B.S [2]
Overview
The first introduction to the use of radial artery for cardiac catheterization was made by Radner in 1948.[1] Subsequently, a Canadian Cardiologist, Lucian Campeau, in 1989 re-introduced the practice.[2] There have been a gradual increase in its preference over the femoral approach internationally;[3] with United States experiencing a 10-fold increase (1 in every 6 PCIs performed) in the adoption of transradial procedures between 2007 and 2012,[4] largely as a result of reduced major bleeding, vascular complications, length of hospital stay and cost, and increased patient satisfaction and quality of care. The rationale for the choice of radial access include:
- Decreased risk of limb ischemia – The hand has a dual arterial supply i.e., radial and ulnar arteries, which unites to form the superficial and deep palmer arches. Therefore, the radial artery is not an end artery like the femoral artery, thus decreasing the risk of arterial occlusion post PCI.
- Decreased risk of bleeding – The superficial course of the distal radial artery allows for easy compressibility in order to minimize hemorrhage post PCI.
References
- ↑ RADNER, S. (1948). “Thoracal aortography by catheterization from the radial artery; preliminary report of a new technique”. Acta radiol. 29 (2): 178–80. PMID 18908938. Unknown parameter
|month=ignored (help) - ↑ Campeau, L. (1989). “Percutaneous radial artery approach for coronary angiography”. Cathet Cardiovasc Diagn. 16 (1): 3–7. PMID 2912567. Unknown parameter
|month=ignored (help) - ↑ Hamon, M.; Pristipino, C.; Di Mario, C.; Nolan, J.; Ludwig, J.; Tubaro, M.; Sabate, M.; Mauri-Ferré, J.; Huber, K. (2013). “Consensus document on the radial approach in percutaneous cardiovascular interventions: position paper by the European Association of Percutaneous Cardiovascular Interventions and Working Groups on Acute Cardiac Care** and Thrombosis of the European Society of Cardiology”. EuroIntervention. 8 (11): 1242–51. doi:10.4244/EIJV8I11A192. PMID 23354100. Unknown parameter
|month=ignored (help) - ↑ Feldman, DN.; Swaminathan, RV.; Kaltenbach, LA.; Baklanov, DV.; Kim, LK.; Wong, SC.; Minutello, RM.; Messenger, JC.; Moussa, I. (2013). “Adoption of radial access and comparison of outcomes to femoral access in percutaneous coronary intervention: an updated report from the national cardiovascular data registry (2007-2012)”. Circulation. 127 (23): 2295–306. doi:10.1161/CIRCULATIONAHA.112.000536. PMID 23753843. Unknown parameter
|month=ignored (help)
Radial Artery Anatomy
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
In human anatomy, the radial artery is the main blood vessel, with oxygenated blood, of the lateral aspect of the forearm.
Course
The radial artery arises from the bifurcation of the brachial artery in the cubital fossa. It runs distally down the anterior part of the forearm. There, it serves as a landmark for the division between the anterior and posterior compartments of the forearm, with the posterior compartment beginning just lateral to the artery. The artery winds laterally around the wrist, passing through the anatomical snuff box and between the heads of the first dorsal interosseous muscle. It passes anteriorly between the heads of the adductor pollicis, and becomes the deep palmar arch, which joins with the deep branch of the ulnar artery.
Along its course, it is accompanied by a similarly named vein, the radial vein.
Branches
The named branches of the radial artery may be divided into three groups, corresponding with the three regions in which the vessel is situated.
In the Forearm
- Radial recurrent artery – arises just after the radial artery comes off the brachial artery. It travels superiorly to anastomose with the radial collateral artery.
- Palmar carpal branch of radial artery – a small vessel which arises near the lower border of the pronator quadratus
- Superficial palmar branch of the radial artery – arises from the radial artery, just where this vessel is about to wind around the lateral side of the wrist.
At the Wrist
- Dorsal carpal branch of radial artery – a small vessel which arises beneath the extensor tendons of the thumb
- First dorsal metacarpal artery – arises just before the radial artery passes between the two heads of the first dorsal interosseous muscle and divides almost immediately into two branches which supply the adjacent sides of the thumb and index finger; the lateral side of the thumb receives a branch directly from the radial artery.
In the Hand
- Princeps pollicis artery – arises from the radial artery just as it turns medially to the deep part of the hand.
- Radialis indicis – arises close to the princeps pollicis. The two arteries may arise from a common trunk, the first palmar metacarpal artery.
- Deep palmar arch – terminal part of radial artery.
Clinical significance
The artery’s pulse is palpable in the anatomical snuff box and on the anterior aspect of the arm over the carpal bones (where it is commonly used to assess the heart rate and cardiac rhythm).
The radial artery is used for coronary artery bypass grafting and is growing in popularity among cardiac surgeons.[2] Recently, it has been shown to have a superior peri-operative and post-operative course when compared to saphenous vein grafts.[3]
See also
Additional images
-
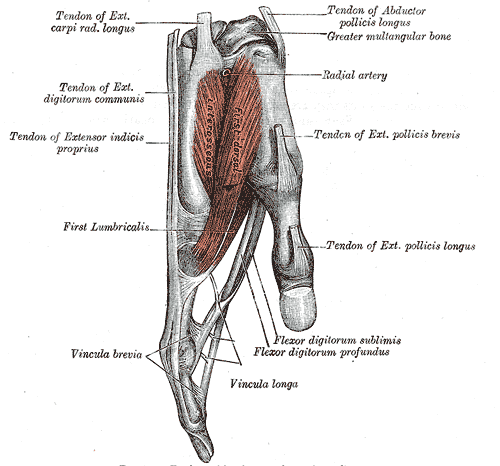 Tendons of forefinger and vincula tendina.
Tendons of forefinger and vincula tendina. -
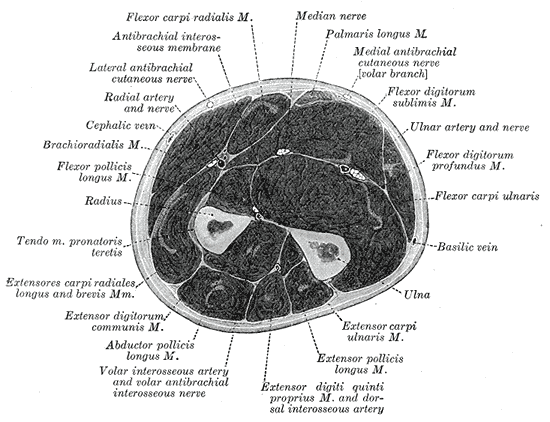 Cross-section through the middle of the forearm.
Cross-section through the middle of the forearm. -
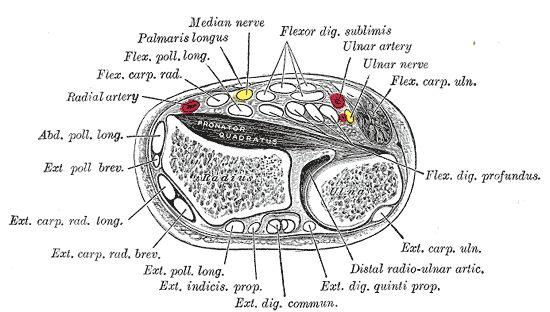 Transverse section across distal ends of radius and ulna.
Transverse section across distal ends of radius and ulna. -
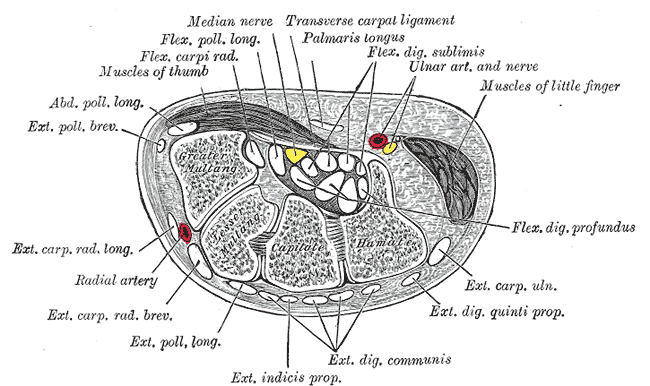 Transverse section across the wrist and digits.
Transverse section across the wrist and digits. -
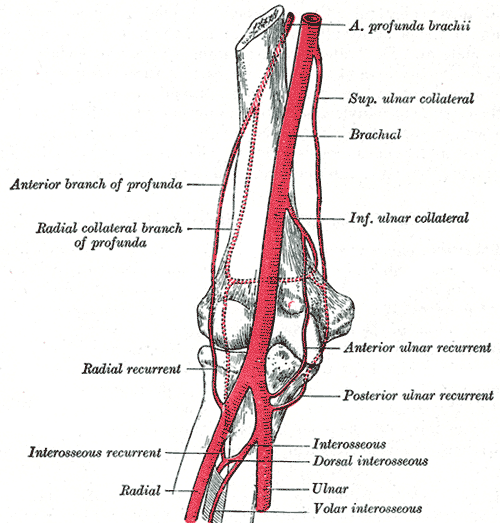 Diagram of the anastomosis around the elbow-joint.
Diagram of the anastomosis around the elbow-joint. -
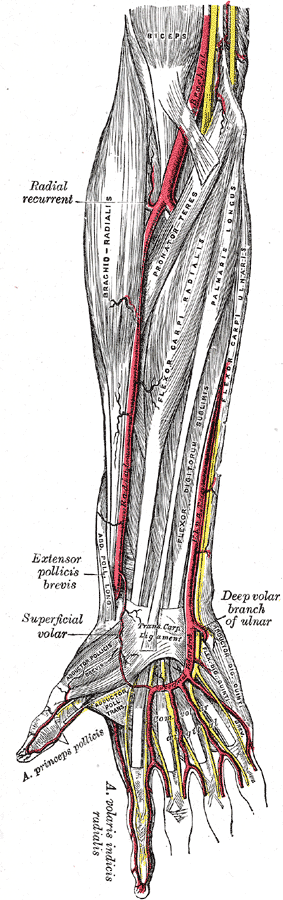 The radial and ulnar arteries.
The radial and ulnar arteries. -
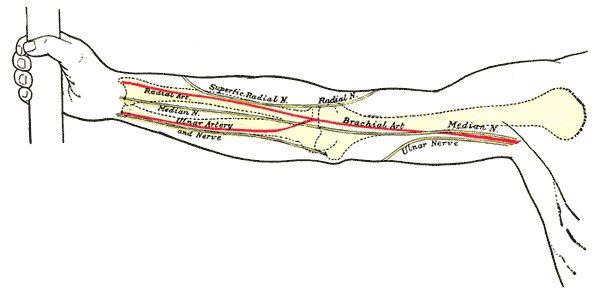 Front of right upper extremity, showing surface markings for bones, arteries, and nerves.
Front of right upper extremity, showing surface markings for bones, arteries, and nerves.






References
- ^ Sajja LR, Mannam G, Pantula NR, Sompalli S. Role of radial artery graft in coronary artery bypass grafting. Ann Thorac Surg. 2005 Jun;79(6):2180-8. PMID 15919345
- ^ Cohen G, Tamariz MG, Sever JY, Liaghati N, Guru V, Christakis GT, Bhatnagar G, Cutrara C, Abouzahr L, Goldman BS, Fremes SE. The radial artery versus the saphenous vein graft in contemporary CABG: a case-matched study. Ann Thorac Surg. 2001 Jan;71(1):180-5; discussion 185-6. PMID 11216742
External links
- Image at umich.edu – pulse
- Radial artery puncture – medicalstudents.com
Template:Gray’s Template:Arteries of upper limbs
Advantages
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.
Overview
Advantages of the Radial Approach to Cardiac Catheterization
Reduced Bleeding
Bleeding is a common complication of the available therapies for the treatment of acute coronary syndromes. There are increasing evidences showing that major bleeding is independently associated with increased risk for mortality and ischemic events among patients with acute coronary syndrome undergoing percutaneous coronary intervention.[1][2] The development of ischemic events (i.e., myocardial infarction and stroke) may be explained by the activation of coagulation cascade by major bleeding, cessation or inadequate antiplatelet and antithrombotic therapies, and depletion of coagulation factors as a complication of blood transfusion. According to a meta-analysis study, radial access was associated with a 73% reduction in major bleeding compared with femoral access; a similar trend was also observed with the risk of ischemic events.[3]
Reduced Time to Mobilization, Length of Hospital Stay and Cost
Transradial PCI has also been shown to be associated with a reduced time to mobilization (i.e., early mobilization),[4][5] cost and length of stay among patients with ACS. In a meta-analysis study, there was a reduction in the length of hospital stay by 0.4 days in the radial group when compared with the femoral group.[3] Consequently, there was reduced expenditure per patient and increased patient turnover at the hospitals.
Patients’ Preference and Increased Satisfaction
Among patients who had undergone both radial and femoral access procedures, there was a strong patient preference for transradial catheterization as well as improved quality of life measured by reduced body pain, back pain, and ease of walking.[6][7]
Other potential advantages of radial over femoral access include:
- Provides an opportunity for same day/outpatient PCI[8][9]
- Absence of retroperitoneal hematomas, femoral pseudo aneurysms, and arteriovenous fistulas
- Improved access in the obese patient
- Reduced incidence of limb threatening ischemia due to the dual blood supply of the hand (ulnar and radial arteries)
- Advantageous for patients with severe occlusive aortoiliac disease
- Advantageous for patients with back pain, obesity, congestive heart failure who have difficulty laying flat on their back.
- Less likelihood of local nerve injury
- Radial artery is easily compressible due to its superficial course
References
- ↑ Eikelboom, JW.; Mehta, SR.; Anand, SS.; Xie, C.; Fox, KA.; Yusuf, S. (2006). “Adverse impact of bleeding on prognosis in patients with acute coronary syndromes”. Circulation. 114 (8): 774–82. doi:10.1161/CIRCULATIONAHA.106.612812. PMID 16908769. Unknown parameter
|month=ignored (help) - ↑ Rao, SV.; O’Grady, K.; Pieper, KS.; Granger, CB.; Newby, LK.; Van de Werf, F.; Mahaffey, KW.; Califf, RM.; Harrington, RA. (2005). “Impact of bleeding severity on clinical outcomes among patients with acute coronary syndromes”. Am J Cardiol. 96 (9): 1200–6. doi:10.1016/j.amjcard.2005.06.056. PMID 16253582. Unknown parameter
|month=ignored (help) - ↑ 3.0 3.1 Jolly, SS.; Amlani, S.; Hamon, M.; Yusuf, S.; Mehta, SR. (2009). “Radial versus femoral access for coronary angiography or intervention and the impact on major bleeding and ischemic events: a systematic review and meta-analysis of randomized trials”. Am Heart J. 157 (1): 132–40. doi:10.1016/j.ahj.2008.08.023. PMID 19081409. Unknown parameter
|month=ignored (help) - ↑ Louvard, Y.; Lefèvre, T.; Allain, A.; Morice, M. (2001). “Coronary angiography through the radial or the femoral approach: The CARAFE study”. Catheter Cardiovasc Interv. 52 (2): 181–7. PMID 11170325. Unknown parameter
|month=ignored (help) - ↑ Suleiman K, Feldman A, Ilan-Bushari L, Turgeman Y (2008). “[Transradial diagnostic and interventional cardiac catheterization in daily practice: advantages, efficacy and safety]”. Harefuah. 147 (5): 388–93, 479. PMID 18770958.
- ↑ Cooper, CJ.; El-Shiekh, RA.; Cohen, DJ.; Blaesing, L.; Burket, MW.; Basu, A.; Moore, JA. (1999). “Effect of transradial access on quality of life and cost of cardiac catheterization: A randomized comparison”. Am Heart J. 138 (3 Pt 1): 430–6. PMID 10467191. Unknown parameter
|month=ignored (help) - ↑ Jolly, SS.; Yusuf, S.; Cairns, J.; Niemelä, K.; Xavier, D.; Widimsky, P.; Budaj, A.; Niemelä, M.; Valentin, V. (2011). “Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): a randomised, parallel group, multicentre trial”. Lancet. 377 (9775): 1409–20. doi:10.1016/S0140-6736(11)60404-2. PMID 21470671. Unknown parameter
|month=ignored (help) - ↑ Bertrand, OF.; De Larochellière, R.; Rodés-Cabau, J.; Proulx, G.; Gleeton, O.; Nguyen, CM.; Déry, JP.; Barbeau, G.; Noël, B. (2006). “A randomized study comparing same-day home discharge and abciximab bolus only to overnight hospitalization and abciximab bolus and infusion after transradial coronary stent implantation”. Circulation. 114 (24): 2636–43. doi:10.1161/CIRCULATIONAHA.106.638627. PMID 17145988. Unknown parameter
|month=ignored (help) - ↑ Gilchrist, IC.; Nickolaus, MJ.; Momplaisir, T. (2002). “Same-day transradial outpatient stenting with a 6-hr course of glycoprotein IIb/IIIa receptor blockade: a feasibility study”. Catheter Cardiovasc Interv. 56 (1): 10–3. doi:10.1002/ccd.10093. PMID 11979524. Unknown parameter
|month=ignored (help)
Potential Pitfalls
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hesham Bahaa El-Din, M.B.B.Ch., M.Sc.
Overview
The data that had been published up till now entails an incidence of about 2% to 34% of radial artery spasm, which would result in transfemoral approach being used instead. [1]. So some precautions should be made beforehand in anticipation of such complications.
Potential Pitfalls of the Radial Approach to Cardiac Catheterization
1- Radial artery spasm:-
- In order to decrease the incidence of radial artery spasm, some interventionist tend to give light sedation as well as intra-arterial Nitroglycerin and calcium channel blocker (verapamil or diltiazem) in order to relax the smooth muscles of the radial artery.
2- Vessel tortuosity. Some of the tortuous forms are:-
- Alpha shape radial artery.
- S-shaped radial artery.
- Proximal and distal omega shaped radial artery.
- Brachial alpha loop.
- High origin radial artery.
A lot of techniques has been used to overcome tortuosities. when a regular 0.35″ J-wire is unable to cross the tortuous vessel, a PTCA 0.014″ is used to cross this part. Then Balloon-Assisted Tracking (BAT) can be useful. It is a technique in which a small compliant balloon usually 2.0mm X 15.0 or 20.0 mm is inflated at the tip of the Guide-in catheter with half to one third of the balloon is inside the catheter. Balloon is inflated slightly over the nominal pressure, the catheter is then steered across the tortuous vessel over the PTCA wire. This technique can also be used in case of radial artery spasm.[2]
3- Guide catheter support and selection may be reduced.
4- Loss of radial artery pulse in 4% of cases.
5- Potential increase in the duration of the procedure and fluroscopy time
6- The radial artery has been instrumented should there be a desire to use it as a conduit for CABG
7- It is the second and not the first approach learned by trainees
8- There is a learning curve in treating spasm, navigating anatomy, and manipulating catheters
9- Anatomically there can be a loop in the artery near the brachial in about 10% of cases
10- Smaller sheaths are required (4-8F)
References
- ↑ Lapras C, Bret P, Capdeville J (1978). “[Diastematomyelia. About a series of 6 cases (author’s transl)]”. Neurochirurgie. 24 (6): 381–9. PMID 752811.
- ↑ Verouden NJ, Kiemeneij F (2014). “Balloon-Assisted Tracking to Overcome Radial Spasm during Transradial Coronary Angiography: A Case Report”. Case Rep Cardiol. 2014: 214310. doi:10.1155/2014/214310. PMC 4008174. PMID 24826306.
Contraindications
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Relative Contraindications
- Absence of palpable radial artery pulse
- Abnormal Allen test (oximetry/ plethysmography), indicating that only one artery supplies the hand
- Presence of upper extremity peripheral vascular disease such as Buerger’s disease and severe Raynaud’s disease
- Presence of arteriovenous shunt for dialysis
- Potential use of the radial artery as a conduit for aortocoronary bypass
- Cellulitis or other infections over the radial artery
- Coagulation defects
- Patients who may require intra-aortic balloon pump counterpulsation (IABP)
- Devices that are not compatible in 7F or smaller sheaths such as TEC, larger Rotoblator burrs, certain stents
- Congenital abnormalities of upper limb vasculature such as extreme tortuosity, anomalous take off of the radial artery, or severe atherosclerosis
References
Pre-procedure Assessment
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ayokunle Olubaniyi, M.B,B.S [2]
Overview
The hand is normally supplied by blood from the ulnar and radial arteries. The arteries undergo anastomosis in the hand. Thus, if the blood supply from one of the arteries is cut off, the other artery can supply adequate blood to the hand. A minority of people lack this dual blood supply. Allen’s test or oximetry/plethysmography should be performed before the procedure to confirm that there is sufficient blood flow in the ulnar artery should there be loss of patency in the radial artery due to either thrombosis or spasm which can result in gangrenous finger or had loss.
Pre-procedure Assessment
Patient Evaluation
This is the first step towards a successful transradial PCI. Effort should be made to assess the following:
- Age – Patients with ages <70 years are better suitable for r-PCI
- Patients’ hemodynamic status
- History of previous ipsilateral brachial or transradial procedure
- Strong radial arterial pulse and presence of a normal Allen’s test
Radial vs. Ulnar Approach
Although the ulnar artery is rarely used nowadays, it has been successfully attempted in the past with a high success rate comparable to the transradial approach.[1] Compared with the radial artery, the ulnar artery have been shown to be larger[2] and more prone to access site failures due to its higher rate of spasms and anatomical variations.[3] Therefore, the transulnar approach is generally reserved as an alternative option in selected cases, and especially when the radial artery is being preserved in anticipation of its usage as a coronary bypass conduit.[1]
Left vs. Right Radial Artery
Radial artery in right upper extremity is usually used in 90% of cases for catheterization due to both operator and patient convenience with typical catheterization.[4] Other factors to consider in making a choice between left and right radial artery include the presence of a left internal mammary artery (IMA) graft and the possible future need for a bypass graft conduit from the non-dominant hand.
The following factors favor the use of left radial artery for PCI:[5]
- Short statured patients
- Patients with abdominal obesity who tend to have compressed abdominal aortas
- Evaluation and treatment of infradiaphragmatic pathology
- Left subclavian and left vertebral interventions
- Reduced fluoroscopy time and radiation dose[6]
The Clinical Implication of Allen’s Test
This test is named after Edgar Van Nuys Allen.[7]. The utility of the Allen’s test has been questioned,[8] and no direct association with ischemic complications of radial artery cannulation has ever been demonstrated. In 1983, Slogoff and colleagues reviewed 1,782 radial artery cannulations and found that 25% of them resulted in complete radial artery occlusion, without apparent adverse effects.[9] A number of reports have been published in which permanent ischemic sequelae occurred even in the presence of a normal Allen’s test.[10][11] In addition, the results of Allen’s tests do not appear to correlate with distal blood flow as demonstrated by fluorescein dye injections[12] or photo plethysmography.[13]
Modifications to the test have been proposed to improve reliability.[14]
Despite this lack of association with outcomes, the Allen’s Test is often performed in clinical practice.
Performing the Allen’s Test
This is used to test the patency of the palmer arch.
- The hand is elevated and the patient/person is asked to make a fist for about 30 secs.
- Pressure is applied over the ulnar and the radial arteries so as to occlude both of them.
- Still elevated, the hand is then opened. It should appear blanched (pallor can be observed at the finger nails).
- Ulnar pressure is released and the color should return in 7 secs.
Inference: Ulnar artery supply to the hand is sufficient and it is safe to cannulate the radial artery
If color does not return or returns after 7 seconds, then the ulnar artery supply to the hand is not sufficient and the radial artery therefore cannot be safely cannulated.
Below is a video demonstrating Allen’s test
{{#ev:youtube|jq0ai5uXx68}}
Reverse Allen’s test may be performed in patients who require a second procedure through the same radial site. In reverse Allen’s test, the physician releases pressure over the radial artery rather than the ulnar. This may detect proximal radial artery disease/occlusion that may be asymptomatic. Patients with an abnormal Reverse Allen’s Test should not undergo a repeat transradial procedure from same radial site.
References
- ↑ 1.0 1.1 Aptecar, E.; Pernes, JM.; Chabane-Chaouch, M.; Bussy, N.; Catarino, G.; Shahmir, A.; Bougrini, K.; Dupouy, P. (2006). “Transulnar versus transradial artery approach for coronary angioplasty: the PCVI-CUBA study”. Catheter Cardiovasc Interv. 67 (5): 711–20. doi:10.1002/ccd.20679. PMID 16557601. Unknown parameter
|month=ignored (help) - ↑ Ashraf, T.; Panhwar, Z.; Habib, S.; Memon, MA.; Shamsi, F.; Arif, J. (2010). “Size of radial and ulnar artery in local population”. J Pak Med Assoc. 60 (10): 817–9. PMID 21381609. Unknown parameter
|month=ignored (help) - ↑ Vassilev, D.; Smilkova, D.; Gil, R. (2008). “Ulnar artery as access site for cardiac catheterization: anatomical considerations”. J Interv Cardiol. 21 (1): 56–60. doi:10.1111/j.1540-8183.2007.00314.x. PMID 18086137. Unknown parameter
|month=ignored (help) - ↑ Bertrand, OF.; Rao, SV.; Pancholy, S.; Jolly, SS.; Rodés-Cabau, J.; Larose, E.; Costerousse, O.; Hamon, M.; Mann, T. (2010). “Transradial approach for coronary angiography and interventions: results of the first international transradial practice survey”. JACC Cardiovasc Interv. 3 (10): 1022–31. doi:10.1016/j.jcin.2010.07.013. PMID 20965460. Unknown parameter
|month=ignored (help) - ↑ Caputo, RP.; Tremmel, JA.; Rao, S.; Gilchrist, IC.; Pyne, C.; Pancholy, S.; Frasier, D.; Gulati, R.; Skelding, K. (2011). “Transradial arterial access for coronary and peripheral procedures: executive summary by the Transradial Committee of the SCAI”. Catheter Cardiovasc Interv. 78 (6): 823–39. doi:10.1002/ccd.23052. PMID 21544927. Unknown parameter
|month=ignored (help) - ↑ Sciahbasi, A.; Romagnoli, E.; Burzotta, F.; Trani, C.; Sarandrea, A.; Summaria, F.; Pendenza, G.; Tommasino, A.; Patrizi, R. (2011). “Transradial approach (left vs right) and procedural times during percutaneous coronary procedures: TALENT study”. Am Heart J. 161 (1): 172–9. doi:10.1016/j.ahj.2010.10.003. PMID 21167351. Unknown parameter
|month=ignored (help) - ↑ Template:WhoNamedIt
- ↑ Jarvis MA, Jarvis CL, Jones PR, Spyt TJ (2000). “Reliability of Allen’s test in selection of patients for radial artery harvest”. Ann. Thorac. Surg. 70 (4): 1362–5. PMID 11081899. Unknown parameter
|month=ignored (help) - ↑ Slogoff s, Keats AS, Arlund C. On the safety of radial artery cannulation. Anesthesiology 1983; 59:42-7
- ↑ Thompson SR, Hirschberg A: Allen’s test re-examined. Crit Care Med 16:915, 1988
- ↑ Wilkins RG: Radial artery cannulation and ischaemic damage: A review. Anaesthesia 40:896-899, 1985
- ↑ McGregor AD: The Allen test-an investigation of its accuracy by fluorescein angiography. J Hand Surg [Br] 12:82-85, 1987
- ↑ Stead SW, Stirt JA: Assessment of digital blood flow and palmar collateral circulation. Int J Clin Monit Comput 2:29, 1985
- ↑ Asif M, Sarkar PK (2007). “Three-digit Allen’s test”. Ann. Thorac. Surg. 84 (2): 686–7. doi:10.1016/j.athoracsur.2006.11.038. PMID 17643672. Unknown parameter
|month=ignored (help)
Procedure
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.;Hesham Bahaa El-Din, M.B.B.Ch., M.Sc.
Overview
The transradial approach (TRA) for coronary/cardiac catheterization is slightly more challenging than the transfemoral route. It requires more maneuvers and catheter steering along the course of the radial artery to reach the level of the coronary sinus in the ascending aorta. The right transradial approach is usually preferred over the left side due to the ease of accessibility for the operating physician.
Catheter/GuideWire Selection
Catheter selection is an important key in the success of the procedure. Standard catheters (e.g Judkin’s Left and Judkin’s right) can be used for the TRA. However due to the common anomalies that could be seen along the course of the radial, subclavien, and axillary arteries, special “dedicated Radial Catheters” had been developed (e.g. Tiger, Jacky, and Kimmy). The most commonly used guidewires are those with hydrophilic coating, due to the expected tortuosity of the arterial course.
Procedure
- Before the start of the procedure a “time out” should be taken to revise the indication, important labs, and the patency of the wrist circulation as discussed previously. Allen’s test or Barbeau test.
- Make sure that all of the equipment is ready and recheck the sizes .
- The wrist should be shaved (if necessary) and cleansed in the usual sterile fashion. In addition, the groin should be prepped in case of access failure or the need for urgent IABP or a temporary venous pacemaker.
- Intravenous (IV) line should be started on the contralateral extremity. If an IV should be placed in the intervention extremity, it must be placed proximal to the wrist preferably at the level of the elbow.
- Sterilization of the whole arm should be done using the standard sterile techniques and covered in sterile drapes except for the region of the radial artery – distal part of the palmar surface of the forearm – which is left exposed for easier access.
- Most operators prefer to give anxiolytics e.g Midazolam (1-2 mg) before the start of the procedure to decrease patient anxiety and hence decrease radial spasm.
- The arm should be fully extended; slightly elevated with full supination, and the wrist hyperextended.
- Palpation of the radial artery against the styloid process of the radius with the middle three fingers to find the point of maximal impulse “PMI” is performed.
- An amount of 0.5cc to 1.0 cc of local anesthetic is injected superficially over the PMI.
- Two techniques are used to puncture the radial artery to obtain access:-
- Direct/single wall puncture : same technique used in the femoral approach.
- Transfixation/ double wall puncture: in which a special kind of puncture needle 18-21 guage is used to puncture the vessel. An indicator at the needle cap would show successful penetration of the artery. Penetrate the other wall of the vessel then withdraw the needle leaving the canula inside the double puncture. Slowly withdraw the canula until a pulsatile flow of blood is noticed.
- An exchange length 0.035-0.038 inch J-tip guidewire is inserted.
- A small incision is made to the skin at the entry of the wire to facilitate the sheath insertion.
- Radial sheath of 23 cm long and 4-6 Fr size should then be introduced.
- Through sidearm of the sheath, 5000 IU of heparin should be administered.
- To reduce spasm, 500 mcg of diltiazem can also be administered via the sidearm.
- Coronary catheters are then advanced along the guidewire into aorta.
- Left and right coronary arteries are then catheterized using a Judkins, Amplatz or multipurpose catheter.
- Hemostasis is achieved by direct pressure at the puncture site at the end of the procedure after removal of radial sheath.
- Radial pulse, and hand circulation should be monitored after the procedure for every 2 hours until discharge.
Radial sheath kits are now available which contain hydrophilic coated sheaths in sizes 4-6 Fr equipped with graduated introducers, various micropuncture needles and guidewires.
Radial Compression Devices
Radial Compression Devices are used for hemostasis after the removal of the radial sheath. In the picture below is one example of the devices used.

Steps




5. Continuously monitor radial artery pulsation distal to the wrist band, and check pulse oximeter for intact hand circulation.
6. Remove wrist band after 1-2 hours according to patient status.
Procedure Video
Below is a video demonstrating radial artery approach in cardiac catheterization followed by application of TR band {{#ev:youtube|XhZroo-_oUA}}
References
Achieving Hemostasis after Radial Artery Catheterization
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Achieving hemostasis after Radial Artery Catheterization
Instructions for the use of the TR Band
- Radial arterial sheath removal after cardiac catheterization or PCI, or peripheral angiography with or without intervention will be performed by trained personnel
- Radial sheaths placed by cardiologists must be removed by a trained or supervised Cardiology Fellow or attending. Radial sheaths placed by a vascular surgeon must be removed by a Vascular surgery attending, fellow, PA, NP or trained surgical resident as designated by vascular MD’s.
- Radial artery sheaths will be removed in the Cardiac Catheterization Laboratory prior to transfer to a medical surgical inpatient unit. A radial artery sheath may be removed in the ICU or VICU setting.
- This device is placed on the hyper extended wrist and tightened via a Velcro band.
- A small green box indicates where the band should be placed proximal to the radial percutaneous site. Single wall stick; place the green dot on the TR Band about 3-4 mm proximal to the skin insertion site. Double wall stick; place the green dot just 1 mm or two proximal to the skin insertion site
- The TR Band inflator syringe is filled with 18 cc of air and slowly injected into the one-way side port which inflates the balloon overlying the radial artery.
- Concomitantly, the radial sheath is slowly pulled out completely, as the balloon is inflated to the maximum of 18 cc of air.
- Then slowly, withdraw air back out via the syringe, 1cc at a time, until the operator observes for blood leaking out from the puncture site, at which time, 1 cc of air is re-injected into the balloon and the syringe is disconnected.
- Keep the plunger in place with your thumb when inflating/deflating the TR band. Releasing the plunger will cause air to expel out of the band to quickly
- Remember to keep the syringe for later deflation
Application tips to remember:
- Make sure the radial artery insertion site is 3 or more cm proximal to the wrist crease. If the site and thus the band are too close to the wrist, it may slip if the wrist bends
- Make sure the site is cleaned with sterile saline and dried completely before the band is placed on the wrist
- Place the green box proximal to the sheath insertion site(Terumo logo closest to the patients little finger)
- Pulling the sheath slowly as you are simultaneously inflating the TR Band to 18 cc’s. You should be completely removing the sheath at about the same time you hit 18cc’s.
- Once all 18cc’s are in the band and the sheath is removed, you slowly about 1cc per second begin reducing the amount of air in the band while visualizing the access site for a blood flash
- Once you visualize a blood flash you immediately put 1 to 2cc’s back into the band and disconnect the syringe confirming that the blood has ceased.
- If the air is released slowly out of the band, there is no need for gauze to be positioned under the TR Band. If you are removing the air slowly and at first sight of a blood flash 1 to 2 cc’s is put back into the band you will have a dry field. You want to have complete visualization of the access site, you do not want a gauze pad to block your visualization of the arteriotomy.
- Also, there is no need to make a skin nick when introducing the sheath (unless completely necessary). The Glidesheath is hydrophilic coated and has a near seamless transition and will not require a nick for insertion. The TR Band is designed to provide the least amount of pressure to gain hemostasis while maintaining flow through both the radial and ulnar arteries. The TR Band is not designed to provide hemostasis for both the arteriotomy of the access site as well as a large skin nick. That is why with the design of both these products a skin nick is not needed and you should never experience a situation in which you would need more than 18cc’s of air, which is occlusive pressure.
TR-Band used to achieve radial artery hemostasis

References
Complications
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.; Ayokunle Olubaniyi, M.B,B.S [2]
Overview
Like any other arterial puncture in any part of the body, complications are not uncommon, including radial artery spasms and occlusion, bleeding, radiation exposure, e.t.c. However, these complications can be minimized by the use of appropriate medications, radiation protective devices, and most importantly, by implementing efficient, high-quality, and personalized transradial training programs that educate the entire catheterization laboratory team.[1]
Complications
Radial Artery Spasm
Radial artery spasm (RAS) remains one of the major limitations of transradial approach for PCI.[2] The radial artery was demonstrated to have stronger contractions to common vasoactive substances, thus, increasing its propensity to spasm especially in situations of trauma.[3] The incidence of RAS varies from 12% among high risk patients in whom transfemoral approach was contraindicated[4] to 22% among patients without prior administration of intra-arterial vasodilators.[5] The increased incidence in RAS may be due to the small size of radial artery, female gender, long and difficult procedures with multiple catheter exchanges, sheath size, and operator inexperience.[6]
Some of the measures that have been shown to reduce the incidence and severity of RAS include:
- Generous patient sedation
- Use of spasmolytic cocktails such as verapamil, nitroprusside or combination of both[7][8][9]
- Use of a hydrophilic sheath of the smallest possible diameter
- Wiping and flushing catheters with solutions containing calcium channel blocker or nitrates
- Using a smaller catheter size
- Use of intra-arterial Papaverine for the treatment of severe arterial spasm[10]
- Adequate time should be given for the artery to relax before removing catheters or sheaths to prevent arterial evulsion
Radial Artery Occlusion
Although most cases of radial artery occlusion are asymptomatic, cases of hand ischemia have been reported.[11] As a result of this, coupled with the fact that a persistent RAO could make future access of the ipsilateral radial artery for angioplasty, intra-arterial pressure monitoring, coronary artery bypass surgery, or hemodialysis impossible or difficult, more aggressive measures should be implemented to prevent RAO, especially nowadays where greater than 50% of physicians performing transradial PCI do not routinely evaluate radial arterial patency before discharging their patients.[12]
According to the Best Practices for Transradial Angiography and Intervention (2013), the evidence-base practices associated with a reduced risk of RAO include:
| Anticoagulationa | Enoxaparin at 60 mg given through the radial arterial sheath | Sheath length |
| Patent (non-occlusive) hemostasisb | Hydrophillic sheaths | Sheathless guide catheters |
| Sheath diameter less than radial artery diameter | Routine use of drugs to reduce radial artery spasm | |
| Avoiding repeat access of the radial artery | Limiting the duration of radial artery compression |
aUnfractionated heparin 70 units/Kg up to 5000 units and bivalirudin 0.75 mg/kg bolus followed by 1.75 mg/kg/hr infusion during procedure. bThis is the most effective strategy to reduce the risk of RAO[1][13]
Below are the steps involved in the patent hemostasis process:
| “ | Step 1: Withdraw the arterial sheath 2–3 cm.
Step 2: Apply the hemostatic compression device, 2 to 3 mm proximal to the skin entry site, and tighten it or inflate it, then remove the sheath. Step 3: Decrease the pressure of the hemostatic compression device to the point of mild pulsatile bleeding at the skin entry site. After 2 to 3 cycles of pulsatile bleeding, retighten the hemostatic compression device gradually to eliminate this pulsatile bleeding. Step 4: Evaluate radial artery patency by using the reverse Barbeau’s test: Place the plethysmographic sensor on the index finger of the involved upper extremity with the observation of pulsatile waveforms Compress the Ulnar artery at the level of the wrist, and observe the behavior of the waveform. Absence of plethysmographic waveform is indicative of interruption of radial artery flow. If this occurs, the hemostatic compression pressure should be lowered to the point where plethysmographic waveform returns. This is evidence of antegrade radial artery flow. |
” |
Catheter Knot
Hematoma
Varying degrees and severities of hematomas have been reported. The most common location occurs at the puncture site, but rare cases involving the mediastinum,[14] mediastinum and neck,[15] or even the forearm muscle[12][16] have been reported in association with the transradial approach. A grading system similar to the femoral approach have also been used: Grade 1 (<5cm), grade 2 (<10cm), grade 3 (distal to the elbow) and grade 4 (proximal to the elbow). The independent predictors of bleeding were identified as: creatinine clearance <60 mL/min, procedure duration, and sheath size.[17]
Compartment Syndrome
Bleeding is a common complication of r-PCI which can result into devastating consequences. Compartment syndrome is a limb-threatening surgical emergency which requires a high index of suspicion and timely application of appropriate protocols once local bleeding is suspected such as discontinuation of anticoagulant therapy, pain and blood pressure control, external compression with a blood pressure cuff, close monitoring of distal perfusion of the hand (plethysmography) and consultation to a vascular surgeon is also recommended in cases of limb ischemia.[18]
Increased Exposure to Radiation
Some observational studies have shown that the transradial approach to PCI is associated with an increased radiation exposure in the patient, and especially, the operator.[19] According to a large study, radial artery catheterization was associated with a 23% increase in radiation exposure when compared with the transfemoral access.[20] This is largely dependent on operator proficiency. Two studies demonstrated that increasing operator experience with the transradial approach is associated with a lower patient and operator radiation exposure.[21][22] Some measures which have been shown to reduce exposure to radiation include the use of transradial protection board,[23] lead-free radiation shield over the right sheath insertion site,[24] and the use of left radial artery, which is associated with a lower fluoroscopy time and radiation dose compared with the right radial angiography.[25]
Other complications associated with the transradial approach are listed below:
- Local pain and swelling
- Thrombosis[26]
- Embolization[27]
- Infection[28]
- Pseudoaneurysm[29]
- Blood loss[30]
- Limb ischemia
- Arteriovenous fistula
- Cerebral embolization[31]
- Peripheral neuropathy
- Accelerated atherosclerosis
- Transient vocal cord paralysis
- Delayed reflex sympathetic dystrophy
- Subcutaneous granulomatous reaction (hydrophilic coating) or sheath-associated sterile abscesses
Optical coherence tomography (OCT) has been used by Yonetsu et al to define the damage to the radial artery in 73 arteries of 69 patients [32]. 32% of patients developed intimal tears and 16% of patients developed medial dissections. Repeat catheterization was associated with increased fibro-intimal hyperplasia. Cardiac catheterization via the radial approach may render the radial artery unsuitable for coronary artery bypass grafting. There can be a loss of pulse in about 4% of cases. Use of smaller guide catheters and sheathless guides may potentially reduce the risk of these complications.
References
- ↑ 1.0 1.1 Rao, SV.; Tremmel, JA.; Gilchrist, IC.; Shah, PB.; Gulati, R.; Shroff, AR.; Crisco, V.; Woody, W.; Zoghbi, G. (2013). “Best practices for transradial angiography and intervention: A consensus statement from the society for cardiovascular angiography and intervention’s transradial working group”. Catheter Cardiovasc Interv. doi:10.1002/ccd.25209. PMID 24123781. Unknown parameter
|month=ignored (help) - ↑ Varenne, O.; Jégou, A.; Cohen, R.; Empana, JP.; Salengro, E.; Ohanessian, A.; Gaultier, C.; Allouch, P.; Walspurger, S. (2006). “Prevention of arterial spasm during percutaneous coronary interventions through radial artery: the SPASM study”. Catheter Cardiovasc Interv. 68 (2): 231–5. doi:10.1002/ccd.20812. PMID 16819768. Unknown parameter
|month=ignored (help) - ↑ Chardigny, C.; Jebara, VA.; Acar, C.; Descombes, JJ.; Verbeuren, TJ.; Carpentier, A.; Fabiani, JN. (1993). “Vasoreactivity of the radial artery. Comparison with the internal mammary and gastroepiploic arteries with implications for coronary artery surgery”. Circulation. 88 (5 Pt 2): II115–27. PMID 8222146. Unknown parameter
|month=ignored (help) - ↑ Hildick-Smith, DJ.; Walsh, JT.; Lowe, MD.; Shapiro, LM.; Petch, MC. (2004). “Transradial coronary angiography in patients with contraindications to the femoral approach: an analysis of 500 cases”. Catheter Cardiovasc Interv. 61 (1): 60–6. doi:10.1002/ccd.10708. PMID 14696161. Unknown parameter
|month=ignored (help) - ↑ Kiemeneij, F.; Vajifdar, BU.; Eccleshall, SC.; Laarman, G.; Slagboom, T.; van der Wieken, R. (2003). “Evaluation of a spasmolytic cocktail to prevent radial artery spasm during coronary procedures”. Catheter Cardiovasc Interv. 58 (3): 281–4. doi:10.1002/ccd.10445. PMID 12594687. Unknown parameter
|month=ignored (help) - ↑ Varenne, O.; Jégou, A.; Cohen, R.; Empana, JP.; Salengro, E.; Ohanessian, A.; Gaultier, C.; Allouch, P.; Walspurger, S. (2006). “Prevention of arterial spasm during percutaneous coronary interventions through radial artery: the SPASM study”. Catheter Cardiovasc Interv. 68 (2): 231–5. doi:10.1002/ccd.20812. PMID 16819768. Unknown parameter
|month=ignored (help) - ↑ Attaran, S.; John, L.; El-Gamel, A. (2008). “Clinical and potential use of pharmacological agents to reduce radial artery spasm in coronary artery surgery”. Ann Thorac Surg. 85 (4): 1483–9. doi:10.1016/j.athoracsur.2007.10.042. PMID 18355566. Unknown parameter
|month=ignored (help) - ↑ Kiemeneij, F.; Vajifdar, BU.; Eccleshall, SC.; Laarman, G.; Slagboom, T.; van der Wieken, R. (2003). “Evaluation of a spasmolytic cocktail to prevent radial artery spasm during coronary procedures”. Catheter Cardiovasc Interv. 58 (3): 281–4. doi:10.1002/ccd.10445. PMID 12594687. Unknown parameter
|month=ignored (help) - ↑ Varenne, O.; Jégou, A.; Cohen, R.; Empana, JP.; Salengro, E.; Ohanessian, A.; Gaultier, C.; Allouch, P.; Walspurger, S. (2006). “Prevention of arterial spasm during percutaneous coronary interventions through radial artery: the SPASM study”. Catheter Cardiovasc Interv. 68 (2): 231–5. doi:10.1002/ccd.20812. PMID 16819768. Unknown parameter
|month=ignored (help) - ↑ Osman, F.; Buller, N.; Steeds, R. (2008). “Use of intra-arterial papaverine for severe arterial spasm during radial cardiac catheterization”. J Invasive Cardiol. 20 (10): 551–2. PMID 18830002. Unknown parameter
|month=ignored (help) - ↑ Rhyne, D.; Mann, T. (2010). “Hand ischemia resulting from a transradial intervention: successful management with radial artery angioplasty”. Catheter Cardiovasc Interv. 76 (3): 383–6. doi:10.1002/ccd.22460. PMID 20839353. Unknown parameter
|month=ignored (help) - ↑ 12.0 12.1 Bertrand, OF.; Rao, SV.; Pancholy, S.; Jolly, SS.; Rodés-Cabau, J.; Larose, E.; Costerousse, O.; Hamon, M.; Mann, T. (2010). “Transradial approach for coronary angiography and interventions: results of the first international transradial practice survey”. JACC Cardiovasc Interv. 3 (10): 1022–31. doi:10.1016/j.jcin.2010.07.013. PMID 20965460. Unknown parameter
|month=ignored (help) - ↑ Pancholy, S.; Coppola, J.; Patel, T.; Roke-Thomas, M. (2008). “Prevention of radial artery occlusion-patent hemostasis evaluation trial (PROPHET study): a randomized comparison of traditional versus patency documented hemostasis after transradial catheterization”. Catheter Cardiovasc Interv. 72 (3): 335–40. doi:10.1002/ccd.21639. PMID 18726956. Unknown parameter
|month=ignored (help) - ↑ Park, KW.; Chung, JW.; Chang, SA.; Kim, KI.; Chung, WY.; Chae, IH. (2008). “Two cases of mediastinal hematoma after cardiac catheterization: A rare but real complication of the transradial approach”. Int J Cardiol. 130 (3): e89–92. doi:10.1016/j.ijcard.2007.05.093. PMID 17673316. Unknown parameter
|month=ignored (help) - ↑ Jao, YT.; Chen, Y.; Fang, CC.; Wang, SP. (2003). “Mediastinal and neck hematoma after cardiac catheterization”. Catheter Cardiovasc Interv. 58 (4): 467–72. doi:10.1002/ccd.10476. PMID 12652496. Unknown parameter
|month=ignored (help) - ↑ Araki T, Itaya H, Yamamoto M (2010). “Acute compartment syndrome of the forearm that occurred after transradial intervention and was not caused by bleeding or hematoma formation”. Catheter Cardiovasc Interv. 75 (3): 362–5. doi:10.1002/ccd.22282. PMID 19821498.
- ↑ Bertrand, OF.; Larose, E.; Rodés-Cabau, J.; Gleeton, O.; Taillon, I.; Roy, L.; Poirier, P.; Costerousse, O.; Larochellière, RD. (2009). “Incidence, predictors, and clinical impact of bleeding after transradial coronary stenting and maximal antiplatelet therapy”. Am Heart J. 157 (1): 164–9. doi:10.1016/j.ahj.2008.09.010. PMID 19081414. Unknown parameter
|month=ignored (help) - ↑ Caputo, RP.; Tremmel, JA.; Rao, S.; Gilchrist, IC.; Pyne, C.; Pancholy, S.; Frasier, D.; Gulati, R.; Skelding, K. (2011). “Transradial arterial access for coronary and peripheral procedures: executive summary by the Transradial Committee of the SCAI”. Catheter Cardiovasc Interv. 78 (6): 823–39. doi:10.1002/ccd.23052. PMID 21544927. Unknown parameter
|month=ignored (help) - ↑ Rao, SV.; Bernat, I.; Bertrand, OF. (2012). “Clinical update: Remaining challenges and opportunities for improvement in percutaneous transradial coronary procedures”. Eur Heart J. 33 (20): 2521–6. doi:10.1093/eurheartj/ehs169. PMID 22815330. Unknown parameter
|month=ignored (help) - ↑ Mercuri, M.; Mehta, S.; Xie, C.; Valettas, N.; Velianou, JL.; Natarajan, MK. (2011). “Radial artery access as a predictor of increased radiation exposure during a diagnostic cardiac catheterization procedure”. JACC Cardiovasc Interv. 4 (3): 347–52. doi:10.1016/j.jcin.2010.11.011. PMID 21435615. Unknown parameter
|month=ignored (help) - ↑ Jolly, SS.; Cairns, J.; Niemela, K.; Steg, PG.; Natarajan, MK.; Cheema, AN.; Rao, SV.; Cantor, WJ.; Džavík, V. (2013). “Effect of radial versus femoral access on radiation dose and the importance of procedural volume: a substudy of the multicenter randomized RIVAL trial”. JACC Cardiovasc Interv. 6 (3): 258–66. doi:10.1016/j.jcin.2012.10.016. PMID 23517837. Unknown parameter
|month=ignored (help) - ↑ Lo, TS.; Ratib, K.; Chong, AY.; Bhatia, G.; Gunning, M.; Nolan, J. (2012). “Impact of access site selection and operator expertise on radiation exposure; a controlled prospective study”. Am Heart J. 164 (4): 455–61. doi:10.1016/j.ahj.2012.06.011. PMID 23067901. Unknown parameter
|month=ignored (help) - ↑ Behan, M.; Haworth, P.; Colley, P.; Brittain, M.; Hince, A.; Clarke, M.; Ghuran, A.; Saha, M.; Hildick-Smith, D. (2010). “Decreasing operators’ radiation exposure during coronary procedures: the transradial radiation protection board”. Catheter Cardiovasc Interv. 76 (1): 79–84. doi:10.1002/ccd.22466. PMID 20578091. Unknown parameter
|month=ignored (help) - ↑ Politi, L.; Biondi-Zoccai, G.; Nocetti, L.; Costi, T.; Monopoli, D.; Rossi, R.; Sgura, F.; Modena, MG.; Sangiorgi, GM. (2012). “Reduction of scatter radiation during transradial percutaneous coronary angiography: a randomized trial using a lead-free radiation shield”. Catheter Cardiovasc Interv. 79 (1): 97–102. doi:10.1002/ccd.22947. PMID 21520391. Unknown parameter
|month=ignored (help) - ↑ Sciahbasi, A.; Romagnoli, E.; Burzotta, F.; Trani, C.; Sarandrea, A.; Summaria, F.; Pendenza, G.; Tommasino, A.; Patrizi, R. (2011). “Transradial approach (left vs right) and procedural times during percutaneous coronary procedures: TALENT study”. Am Heart J. 161 (1): 172–9. doi:10.1016/j.ahj.2010.10.003. PMID 21167351. Unknown parameter
|month=ignored (help) - ↑ Zankl, AR.; Andrassy, M.; Volz, C.; Ivandic, B.; Krumsdorf, U.; Katus, HA.; Blessing, E. (2010). “Radial artery thrombosis following transradial coronary angiography: incidence and rationale for treatment of symptomatic patients with low-molecular-weight heparins”. Clin Res Cardiol. 99 (12): 841–7. doi:10.1007/s00392-010-0197-8. PMID 20625752. Unknown parameter
|month=ignored (help) - ↑ Downs JB, Rackstein AD, Klein EF, Hawkins IF (1973). “Hazards of radial-artery catheterization”. Anesthesiology. 38 (3): 283–6. PMID 4698148.
- ↑ Mimoz O, Pieroni L, Lawrence C, Edouard A, Costa Y, Samii K; et al. (1996). “Prospective, randomized trial of two antiseptic solutions for prevention of central venous or arterial catheter colonization and infection in intensive care unit patients”. Crit Care Med. 24 (11): 1818–23. PMID 8917031.
- ↑ Inan MB, Acikgoz B, Yazicioglu L, Kaya B, Ozyurda U (2011). “A rare complication of radial artery catheterization”. Vascular. 19 (3): 167–9. doi:10.1258/vasc.2010.cr0238. PMID 21652670.
- ↑ Smoller BR, Kruskall MS (1986). “Phlebotomy for diagnostic laboratory tests in adults. Pattern of use and effect on transfusion requirements”. N Engl J Med. 314 (19): 1233–5. doi:10.1056/NEJM198605083141906. PMID 3702919.
- ↑ Lund C, Nes RB, Ugelstad TP, Due-Tønnessen P, Andersen R, Hol PK; et al. (2005). “Cerebral emboli during left heart catheterization may cause acute brain injury”. Eur Heart J. 26 (13): 1269–75. doi:10.1093/eurheartj/ehi148. PMID 15716287.
- ↑ Yonetsu T, Kakuta T, Lee T, et al. Assessment of acute injuries and chronic intimal thickening of the radial artery after transradial coronary intervention by optical coherence tomography. Eur Heart J. 2010;Epub ahead of print.
Best Practices for Transradial Angiography
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ayokunle Olubaniyi, M.B,B.S [2]
Overview
The best practices on transradial angiography and intervention is a set of evidence-based recommendations regarding the practice of coronary angiography via access through the radial artery. The Society for Cardiovascular Angiography and Intervention (SCAI), through the radial committee, has come up with recommendation made by consensus with the aim of maximizing the benefits and standardizing certain methods to reduce potential complications in transradial procedures.[1]
Recommendations
Monitoring for and Reducing the Risk of Radial Artery Occlusion
| “ | 1. Patients undergoing transradial procedures should have radial artery patency assessed before discharge and at the first postprocedure visit.
2. Adequate anticoagulation should be administered to patients undergoing diagnostic transradial procedures. The recommended regimen is intra-arterial or intravenous unfractionated heparin at a dose of at least 50 u/kg or 5,000 units in patients without contraindications to unfractionated heparin. Patients with heparin-induced thrombocytopenia with or without thrombosis should receive intravenous bivalirudin 0.75 mg/kg bolus for diagnostic cases; for PCI, this bolus dose of bivalirudin should be followed by an infusion of 1.75 mg/kg/hr. 3. Transradial procedures should be performed using the lowest profile system available to successfully complete the procedure and obtain optimal angiography. 4. Patent hemostasis technique should be used in all patients who undergo transradial procedures. |
” |
Reducing Patient and Operator Radiation Exposure
| “ | 1. In addition to following SCAI recommendations for minimizing radiation exposure, operators performing transradial procedures should position the patient’s accessed arm next to the patient’s torso.
2. There is a relationship between radial proficiency and a decrease in patient and operator radiation exposure such that exposure between radial and femoral is comparable among experienced radial operators. Thus, operators should make an effort to maintain a high proportion of transradial procedures in their practice. 3. The use of extension tubing to increase the distance from the radiation source should be considered for transradial procedures. 4. Left radial approach has been associated with shorter fluoroscopy times and should be considered in patients where tortuous vascular anatomy is expected (e.g., age>75 years, short stature). 5. Operators should avoid fluoroscopically tracking the guidewire and/or catheters while traversing the arm unless resistance is felt. 6. Catheter exchanges should be performed without fluoroscopy whenever possible. 7. Documentation of angioplasty balloon and stent positioning should be done using “fluoro save” if available. |
” |
Transitioning to Transradial Primary PCI
| “ | 1. Operators and sites should not start performing transradial primary PCI until they have performed at least 100 elective PCI cases with a “radial first” approach and their femoral crossover rate is >4%.
2. An a priori left radial approach should be strongly considered in patients undergoing transradial primary PCI who are post-CABG with a pedicle LIMA graft. 3. An a priori left radial approach should be considered in patients undergoing transradial primary PCI who are older than age 75 years or who are 5’5″ (165 cm) or shorter. 4. Bailout to either contralateral radial or femoral access is recommended if the time to obtain radial access is >3 min, or the time from introducer sheath placement in the radial artery to engaging the infarct-related artery with the guide catheter is >10 min (including the time to inject the non-infarct artery), or the total time from radial artery introducer sheath placement to dilating the infarct lesion is >20 min. 5. Door-to-balloon times should be monitored closely when starting a transradial primary PCI program and cases with times that extend beyond recommended benchmarks should be reviewed to identify whether the radial approach was responsible for the delay. 6. Femoral access sites should be prepared routinely in patients with STEMI when the operator is early in their experience with transradial primary PCI or when the need for adjunctive devices like intra-aortic balloon counterpulsation is anticipated. |
” |
References
- ↑ Rao, SV.; Tremmel, JA.; Gilchrist, IC.; Shah, PB.; Gulati, R.; Shroff, AR.; Crisco, V.; Woody, W.; Zoghbi, G. (2013). “Best practices for transradial angiography and intervention: A consensus statement from the society for cardiovascular angiography and intervention’s transradial working group”. Catheter Cardiovasc Interv. doi:10.1002/ccd.25209. PMID 24123781. Unknown parameter
|month=ignored (help)
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH