
Zika virus infection
For patient information, click here.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yazan Daaboul, M.D.; Nate Michalak, B.A.; Luke Rusowicz-Orazem, B.S.; Ilan Dock, B.S.; Serge Korjian M.D.; Yamuna Kondapally, M.B.B.S[2]; Tarek Nafee, M.D. [3]
Synonyms and keywords: Zika virus; ZIKV; ZIKV disease; Zika; Zika virus disease; Zika disease; Zika fever
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yazan Daaboul, M.D.; Serge Korjian M.D.; Nate Michalak, B.A.; Yamuna Kondapally, M.B.B.S[2]
Overview
Zika fever is an infectious disease caused by Zika virus (ZIKV), an enveloped, single-stranded, positive-sense RNA flavivirus. Zika virus is a vector-borne pathogen usually transmitted via the Aedes mosquito that also transmits the dengue and chikungunya viruses. Human-to-human transmission by blood transfusions, sexual intercourse, or vertical transmission has also been reported. Once rare, the incidence of Zika virus infection rose dramatically during the 2014-2016 outbreak that started in Brazil. Zika virus infection has a clinical presentation similar to Dengue fever, yellow fever, West Nile virus, and Japanese encephalitis, but it is distinct in its milder clinical manifestations and short length of infection. Only one-fifth of patients exposed to Zika virus will develop clinical manifestations, typically 3 to 12 days after contracting the disease. Symptoms will typically begin with a mild headache and fever, then progress to include maculopapular rash spread across the body within 24 hours, followed by conjunctivitis, malaise, and back pain. Symptoms typically last 4 to 7 days. The prognosis is usually excellent, with the majority of patients recovering fully. Complications may include neurological sequelae, particularly Guillain-Barré syndrome. It is also thought that Zika virus infection is teratogenic and may be associated with microcephaly in newborns of infected mothers; this association is strongly suspected but has not yet been confirmed. A diagnosis of Zika virus infection is usually made by either RT-PCR or ELISA. Treatment is usually supportive, and antiviral therapy is generally not recommended. There are no vaccines available to prevent Zika virus infection. Since the virus is usually transmitted through mosquitoes, effective measures to avoid mosquito bites include using insect repellent, installing mosquito bed nets and window/door screens, wearing long sleeves and long pants, and removing potential breeding sites from indoor/outdoor premises. It is also recommended that men practice sexual abstinence and/or wear condoms when Zika virus infected is suspected to prevent sexual transmission. Once infected, individuals may be re-infected in the future.
Historical Perspective
Zika virus was first isolated from a Rhesus Monkey in 1947 in Uganda. The virus was first isolated from humans in 1968 in Nigeria. Since then, viral circulation and outbreaks have been documented throughout Asia and Africa. The most recent outbreak occurred in Brazil in April 2015.
Pathophysiology
Zika virus is a vector-borne pathogen usually transmitted via the Aedes mosquito, which also transmits the dengue and chikungunya viruses. Human-to-human transmission is thought to occur via blood transfusions, sexual transmission, and vertical transmission. Zika virus initially replicates in dendritic cells near the site of inoculation before spreading to lymph nodes and then the bloodstream.
Causes
Zika virus infection is cause by Zika virus, an enveloped, single stranded positive sense RNA virus. Zika virus is a type of flavivirus and is primarily transmitted through mosquitoes.
Classification
A schema for the classification of Zika virus infection has yet to be developed.
Differential Diagnosis
The broad-ranging clinical symptoms characteristic of Zika virus infection often cause it to be commonly misdiagnosed with multiple similar diseases that are also from the Flaviviridae virus family. Zika virus infection has similar clinical presentation to Dengue fever, yellow fever, West Nile virus, and Japanese encephalitis. Zika virus infection is distinct in its milder clinical manifestations and short length of infection. The association between Zika virus infection and complications that include congenital anomalies and neurological syndromes is also distinctive. Of note, patients bitten by mosquitoes may be concomitantly infected with Zika virus and other mosquito-borne infections, and co-infection should always be considered.
Epidemiology and Demographics
In 2015, Zika virus infection outbreaks rose dramatically, particularly in Brazil as observed by the manifestation of a correlated complication, microcephaly, in infants born to mothers with Zika virus infection, an incidence of approximately 100 per 100,000 infants. The majority of Zika virus infection cases are reported in South Africa and Tropical Asia. As of 2014, Zika virus infection outbreaks have also become more common in South America. Cases reported in other regions of the world are attributed to travel from areas with outbreaks. Zika virus infection affects all age groups, though newborn infants are particularly vulnerable due to the risk of transmission from their mothers upon birth.
Risk Factors
The most potent risk factor in the development of Zika virus infection is travel to endemic areas. Other risk factors include exposure to infected individuals via blood transfusion, sexual intercourse, or vertically to fetuses from infected mothers.
Natural History, Complications & Prognosis
Patients exposed to Zika virus will develop symptoms between 3 and 12 days after contracting the disease. Symptoms will typically begin with a mild headache and progress to include a maculopapular rash that spreads across the body within 24 hours, followed by fever, malaise, and back pain. The symptoms typically last 4-7 days. The prognosis is excellent, with the majority of patients recovering fully. Complications include neurological and congenital sequelae, particularly Guillain-Barré syndrome and microcephaly. The association between Zika virus infection and microcephaly has not yet been confirmed.
Diagnosis
History and Symptoms
The most common symptoms of Zika virus include fever and maculopapular rash. Additional symptoms include arthralgia, conjunctivitis, myalgia, headache, retro-orbital pain, and vomiting.
Physical Examination
Physical examination of patients with Zika virus infection is usually remarkable for fever and a maculopapular rash that often includes the face, trunk, and extremities (may include the palms and soles). Other physical examination findings include non-purulent conjunctivitis and edema.
Laboratory Findings
The diagnosis of Zika virus infection is usually made by detection of elevated IgM and IgG Zika virus antibodies by ELISA or viral RNA by RT-PCR. Non-specific lab findings include elevated markers of inflammation, mild neutropenia, normal leukocyte count or mild leukocytosis with normal platelet count and liver function tests.
Evaluation of Pregnant Women
According to the CDC, pregnant women suspected to have Zika virus infection may be advised to undergo amniocentesis and testing of histopathologic samples of the placenta and umbilical cord, frozen placental tissue and cord tissue for Zika virus RNA, and cord serum for Zika and dengue virus IgM and neutralizing antibodies.
Evaluation of Infants
According to the CDC, Zika virus testing is recommended among 1) infants with microcephaly or intracranial calcifications born to women who traveled to or resided in an area with Zika virus transmission while pregnant, or 2) infants born to mothers with positive or inconclusive test results for Zika virus infection. When an infant is born with microcephaly or intracranial calcifications to a mother who was potentially infected with Zika virus during pregnancy, the infant should be tested for Zika virus infection and given an ophthalmologic examination. For an infant without microcephaly or intracranial calcifications born to a mother who was potentially infected with Zika virus during pregnancy, subsequent evaluation is dependent on results from maternal Zika virus testing. Developmental monitoring and screening during the first year of life is recommended for all children with congenital Zika virus infection.
Collection and Submission of Fetal Tissues for Zika Virus Testing
In the USA, all fetal tissue suspected to be infected with Zika virus must be collected and submitted to the Centers for Disease Control and Prevention (CDC) for testing. Histopathology, immunohistochemical staining, and reverse transcription-polymerase chain reaction (RT-PCR) will be performed on fixed tissues. RT-PCR can be performed on frozen tissues.
Sexual Transmission Risk Assessment
At present, Zika virus testing for the assessment of risk for sexual transmission is of uncertain value, because current understanding of the incidence and duration of shedding in the male genitourinary tract is limited to one case report in which Zika virus persisted longer than in blood.[1] The CDC does not recommend testing men for the purpose of assessing risk for sexual transmission.
Other Diagnostic Studies
There are no other diagnostic studies associated with Zika virus infection.
Treatment
Medical Therapy
The mainstay of therapy for Zika virus infection is supportive care. Supportive care includes includes rest, adequate fluids intake, and administration of antipyretics and analgesics. Aspirin and other NSAIDs should be avoided until Dengue fever is ruled out, as NSAIDs may increase the risk of hemorrhage in cases of Dengue fever. Antiviral treatment is not recommended for the management of Zika virus infection. The general principles of medical therapy for the management of Zika virus apply to pregnant women. Treatment of congenital Zika virus infection is supportive and should address specific medical and neurodevelopmental issues for the infant’s particular needs. Mothers are encouraged to breastfeed infants even in areas where Zika virus is found, as available evidence indicates that the benefits of breastfeeding outweigh any potential risks associated with Zika virus infection transmission through breastmilk.[2][3]
Surgery
Surgery is not recommended for the management of Zika virus infection.
Prevention
There are no vaccines available to prevent Zika virus infection. Since the virus is usually transmitted through mosquitoes, effective preventive measures revolve around avoiding mosquito bites, which can be achieved by using insect repellent, installing mosquito bed nets and window/door screens, wearing long sleeves and long pants, and removing potential breeding sites from indoor/outdoor premises. Once infected, individuals may be re-infected in the future. Men who reside in or have traveled to an area of active Zika virus transmission who have a pregnant partner should abstain from sexual activity or consistently and correctly use condoms during sex (i.e., vaginal intercourse, anal intercourse, or fellatio) for the duration of the pregnancy. Men who reside in or have traveled to an area of active Zika virus transmission who are concerned about sexual transmission of Zika virus might consider abstaining from sexual activity or using condoms consistently and correctly during sex.
Travel Notice
The CDC has issued level 2 alert (practice enhanced precautions) for travelers to Cape Verde, the Carribean, Central America, Mexico, Pacific Islands, and South America.
Blood Donation
Zika virus may be detected in blood for a short period of time. Although rare, there have been reports of Zika virus transmission via blood transfusions. The risk of Zika virus infection in the continental USA due to blood transfusion is extremely low. The U.S. Food and Drug Administration (FDA), the Red Cross, and the British National Health Service Blood and Transplant Agency announced that individuals who traveled to Zika-affected regions would be ineligible to donate blood for at least 28 days. The Canadian Blood Agency announced that individuals who traveled to Zika-affected regions would be ineligible to donate blood for at least 3 weeks (21 days).
CDC Response Planning Tips
Local, state, and territorial responses to Zika cases or an outbreak will differ in jurisdictions where Aedes species mosquitoes (Ae. aegypti and Ae. albopictus) are endemic, and, therefore, local mosquito populations could become infected with Zika virus. In the USA, the Centers for Disease Control and Prevention (CDC) has developed resources to help state, local, and territorial public health officials prepare for potential Zika virus cases.
Risk-based Preparedness for States
All states need to provide public health information, particularly to pregnant women, and to assess returning travelers who may have contracted Zika virus infection. States with known Aedes aegypti mosquitoes need to intensively monitor for cases in returning travelers and prepare to find and stop clusters of Zika before they become widespread. States with Aedes albopictus mosquitos need to presume transmission is possible and be ready to prevent, detect, and respond to cases and possible clusters of Zika infection. The objective of a phased, risk-based response using Zika virus surveillance data is to implement public health interventions appropriate to the level of Zika virus risk in a community, county, or state.
Future or Investigational Therapies
There is currently no vaccine in advanced development to prevent Zika virus infection.
References
- ↑ Musso D, Roche C, Robin E, Nhan T, Teissier A, Cao-Lormeau VM (2015). “Potential sexual transmission of Zika virus”. Emerg Infect Dis. 21 (2): 359–61. doi:10.3201/eid2102.141363. PMC 4313657. PMID 25625872.
- ↑ Besnard M, Lastere S, Teissier A, Cao-Lormeau V, Musso D (2014). “Evidence of perinatal transmission of Zika virus, French Polynesia, December 2013 and February 2014”. Euro Surveill. 19 (13). PMID 24721538.
- ↑ Gartner LM, Morton J, Lawrence RA, Naylor AJ, O’Hare D, Schanler RJ; et al. (2005). “Breastfeeding and the use of human milk”. Pediatrics. 115 (2): 496–506. doi:10.1542/peds.2004-2491. PMID 15687461.
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yazan Daaboul, M.D.; Nate Michalak, B.A.; Serge Korjian M.D.; Yamuna Kondapally, M.B.B.S[2]
Overview
Zika virus was first isolated from a Rhesus Monkey in 1947 in Uganda. The virus was first isolated from humans in 1968 in Nigeria. Since then, viral circulation and outbreaks have been documented throughout Asia and Africa. The most recent outbreak occurred in Brazil in April 2015.
Historical Perspective
- In 1947, Zika virus was first isolated from a Rhesus Monkey in the Zika Forest of Uganda.[1]
- In 1948, the virus was recovered from the mosquito Aedes africanus caught in the Zika forest.
- In 1952, the first human cases of Zika were detected in Uganda and the United Republic of Tanzania.
- In 1964, a researcher was accidentally infected with Zika and had mild symptoms. This event confirmed that Zika virus causes human infection.
- In 1968, the first human isolation of the virus occurred in Nigeria.[2]
- Between 1951 through 1981, evidence of human infection was additionally reported in the following countries:[2]
- Africa: Tanzania, Egypt, Central African Republic, Sierra Leone, and Gabon
- Asia: India, Malaysia, the Philippines, Thailand, Vietnam, and Indonesia
- Between 1969-1983, Zika virus is detected in mosquitos found in equatorial Asia, including India, Indonesia, Malaysia, and Pakistan.
- In April 2007, The first outbreak of Zika virus outside of Africa and Asia occurred on the Yap Island in the Federated States of Micronesia. The disease was initially thought to be dengue, but the Chikungunya and Ross River viruses were also suspected.[2]
- In 2008, the first documented case of sexual transmission of Zika virus was reported in Colorado.
- In 2012, researchers identified two distinct lineages of Zika virus.
- African strain
- Asian strain
- In 2013, Zika virus infection was first reported to be associated with Guillian-Barre syndrome in the French Polynesian outbreak.
- In 2014, the first South American outbreak was reported originating in Easter Island, Chile.
Global Attention on Zika
- In April 2015, a larger outbreak of Zika virus occurred in the Brazilian district of Camaçari and neighboring Salvador City. An unknown agent was causing flu-like symptoms, followed by rash and arthralgia, in approximately 500 individuals. RT-PCR techniques by researchers at the Federal University of Bahia confirmed the causative organism to be Zika virus.[3]
- In October 2015, Brazil reported an association between Zika virus infection and microcephaly.
- In the United States (U.S), the first local transmission of ZIKV was reported in December 2015, from Puerto Rico.[4]
- In January 2016, the first diagnosis of intrauterine transmission of the Zika virus was made in Brazil.
- In January 2016, Zika virus disease was added to the list of nationally notifiable conditions in the U.S.
- On February 1st, 2016, the World Health Organization (WHO) declared Zika virus a public health emergency.
- On April 13, 2016, CDC announced that Zika virus is a cause of microcephaly and other severe fetal birth defects.[5]
- In July, 2016, an association between ZIKV and Guillain-Barré syndrome was reported in Brazil.
- In July 2016, the first cases of local transmission of ZIKV occurring in the continental United States were reported from Miami-Dade County in Florida.

References
- ↑ History of Zika http://www.who.int/emergencies/zika-virus/history/en/ (2016) Accessed on September 16, 2016
- ↑ 2.0 2.1 2.2 Hayes EB (2009). “Zika virus outside Africa”. Emerg Infect Dis. 15 (9): 1347–50. doi:10.3201/eid1509.090442. PMC 2819875. PMID 19788800.
- ↑ Campos GS, Bandeira AC, Sardi SI (2015). “Zika Virus Outbreak, Bahia, Brazil”. Emerg Infect Dis. 21 (10): 1885–6. doi:10.3201/eid2110.150847. PMC 4593454. PMID 26401719.
- ↑ U.S Food and Drug http://www.fda.gov/BiologicsBloodVaccines/GuidanceComplianceRegulatoryInformation/Guidances/Blood/default.htm (August 26, 2016) Accessed on September 15, 2016
- ↑ CDC https://www.cdc.gov/zika/about/whatcdcisdoing.html (September, 2016) Accessed on September 14, 2016
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yazan Daaboul, M.D., Nate Michalak, B.A., Serge Korjian M.D., Yamuna Kondapally, M.B.B.S[2]
Overview
Zika virus is a vector-borne pathogen transmitted via the Aedes mosquito, which also transmits the dengue and chikungunya viruses. Human-to-human transmission by sexual intercourse has been confirmed. Zika virus is thought to initially replicate in dendritic cells near the site of inoculation before spreading to lymph nodes and then the bloodstream.
Pathophysiology
Transmission
Through mosquito bites
Zika virus is primarily transmitted to humans via the bite of an infected Aedes mosquito. These mosquitoes are also vectors for dengue and chikungunya viruses.[1][2]
From mother to child
- Infected pregnant women can transmit the Zika virus during the pregnancy or around the time of birth.[2]
- Intrauterine
- Perinatal
- Prolonged circulation of ZIKV RNA is demonstrated in serum of pregnant women.[3][4]
- There are no reports of infants acquiring Zika virus through breastfeeding. Due to the nutritional benefits of breastmilk, mothers are encouraged to breastfeed even in areas where Zika virus is endemic.
Sexual transmission
Zika virus has also been suspected to be sexually transmitted between humans.
- Asymptomatic males to their female partners
- Symptomatic female to her male partner
- Symptomatic or asymptomatic males to males
- Longer shedding of Zika virus is detected in semen
- The maximum documented time of Zika virus RNA detection in semen after onset of symptoms is 188 days (potentially for up to 6 months)
- Zika virus has been detected for up to 11 days in vaginal fluid[5]
Blood transfusion
- Transmission through blood transfusion is possible (very likely but not confirmed) as Zika virus has been identified in asymptomatic donors during an ongoing outbreak.[2][6][7][8]
- In non-pregnant individuals, the viremia with ZIKV may produce 8.1 million copies/ml in serum, which can last for 1-2 weeks.[9][10][11]
- Whole blood has a longer period of viremia than serum.
- ZIKV has been detected in whole blood as late as 58 days after onset of symptoms.[12]
Laboratory exposure
- There has been one reported laboratory-acquired Zika virus disease in United States.[2]
Pathogenesis
- Mosquito-borne Zika virus is thought to initially replicate in dendritic cells near the site of inoculation before spreading to lymph nodes and then the bloodstream.
- One study indicates that Zika virus replicates in cellular nuclei, as opposed to other flaviviruses that do so in the cytoplasm.[13]
- Virus is detectable in blood with in 3 to 4 days of symptom onset.
- The virus can be detected in blood, urine, cerebrospinal fluid, amniotic fluid, semen, and saliva.
- The maximum documented time of Zika virus RNA detection in semen after onset of symptoms is 188 days.
- Once a person has been infected with Zika, they are likely to be protected from future infections.
- Zika virus can be killed by potassium permanganate, ether, temperatures >60°C, but is not effectively neutralized by 10% ethanol.[1]
Fetus
- The exact pathogenesis of Zika virus infection in the fetus is not fully understood.[14]
- The crucial period for brain development is the first trimester of pregnancy. ZIKV infection during this period is more strongly associated with microcephaly than infections later in the pregnancy.
- Based on in vitro investigational studies, Zika virus infects the human embryonic cortical neural progenitor cells (hNPCs) which lead to disruption of cell cycle, increased cell death (via caspase-3-mediated apoptosis), and gene dysregulation resulting in cortical thinning and microcephaly.[15]
- Infected hNPCs also produce infectious Zika particles.
-
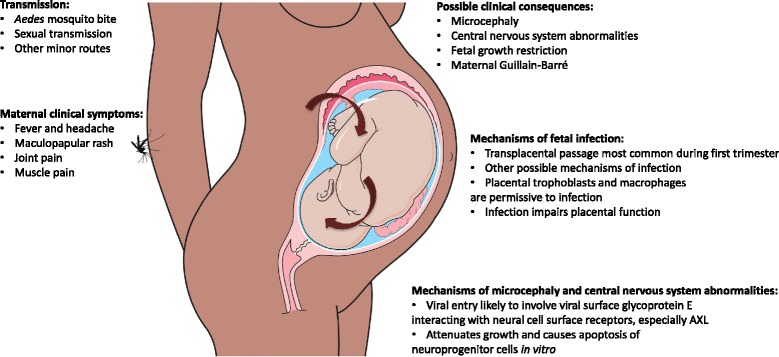 Zika pathogenesis – Source: https://bmcmedicine.biomedcentral.com/articles/10.1186/s12916-016-0660-0
Zika pathogenesis – Source: https://bmcmedicine.biomedcentral.com/articles/10.1186/s12916-016-0660-0

{{#ev:youtube|PpswPzFh5TI}}
Gross pathology
On gross pathology, the characteristic findings of Zika virus infection in neonates include:[16][17]
- Microcephaly
- Widespread brain calcifications in the cortex and sub-cortical white matter
- Ventricular enlargement secondary to cerebral atrophy
Associated Conditions
- There was a significant increase in patients with Guillain-Barré syndrome and congenital microcephaly during the 2014 Zika virus outbreak in French Polynesia and the 2015 Zika virus outbreak in Brazil.
- According to WHO, ZIKV infection during pregnancy is the cause of congenital brain abnormalities including microcephaly.[18]
- Current evidence does not show which specific environmental and host factors interact with Zika virus to increase the risk of an affected pregnancy or of GBS or whether there are specific factors that also have an effect in certain places.[18]
References
- ↑ 1.0 1.1 Hayes EB (2009). “Zika virus outside Africa”. Emerg Infect Dis. 15 (9): 1347–50. doi:10.3201/eid1509.090442. PMC 2819875. PMID 19788800.
- ↑ 2.0 2.1 2.2 2.3 Zika Virus Transmission. Centers for Disease Control and Prevention (June 1, 2015). http://www.cdc.gov/zika/transmission/index.html Accessed on December 17, 2015
- ↑ http://www.fda.gov/downloads/BiologicsBloodVaccines/GuidanceComplianceRegulatoryInformation/Guidances/Blood/UCM518213.pdf
- ↑ Meaney-Delman D, Oduyebo T, Polen KN, White JL, Bingham AM, Slavinski SA; et al. (2016). “Prolonged Detection of Zika Virus RNA in Pregnant Women”. Obstet Gynecol. 128 (4): 724–30. doi:10.1097/AOG.0000000000001625. PMID 27479770.
- ↑ http://www.fda.gov/downloads/BiologicsBloodVaccines/GuidanceComplianceRegulatoryInformation/Guidances/Blood/UCM518213.pdf
- ↑ Musso D, Nhan T, Robin E, Roche C, Bierlaire D, Zisou K; et al. (2014). “Potential for Zika virus transmission through blood transfusion demonstrated during an outbreak in French Polynesia, November 2013 to February 2014”. Euro Surveill. 19 (14). PMID 24739982.
- ↑ Motta IJ, Spencer BR, Cordeiro da Silva SG, Arruda MB, Dobbin JA, Gonzaga YB; et al. (2016). “Evidence for Transmission of Zika Virus by Platelet Transfusion”. N Engl J Med. 375 (11): 1101–3. doi:10.1056/NEJMc1607262. PMID 27532622.
- ↑ Barjas-Castro ML, Angerami RN, Cunha MS, Suzuki A, Nogueira JS, Rocco IM; et al. (2016). “Probable transfusion-transmitted Zika virus in Brazil”. Transfusion. 56 (7): 1684–8. doi:10.1111/trf.13681. PMID 27329551.
- ↑ Petersen LR, Jamieson DJ, Powers AM, Honein MA (2016). “Zika Virus”. N Engl J Med. 374 (16): 1552–63. doi:10.1056/NEJMra1602113. PMID 27028561.
- ↑ Anderson KB, Thomas SJ, Endy TP (2016). “The Emergence of Zika Virus: A Narrative Review”. Ann Intern Med. 165 (3): 175–83. doi:10.7326/M16-0617. PMID 27135717.
- ↑ Zika infection http://www.who.int/bulletin/online_first/16-174540.pdf(April, 2016) Accessed on September 27, 2016
- ↑ Lustig Y, Mendelson E, Paran N, Melamed S, Schwartz E (2016). “Detection of Zika virus RNA in whole blood of imported Zika virus disease cases up to 2 months after symptom onset, Israel, December 2015 to April 2016”. Euro Surveill. 21 (26). doi:10.2807/1560-7917.ES.2016.21.26.30269. PMID 27386894.
- ↑ Buckley A, Gould EA (1988). “Detection of virus-specific antigen in the nuclei or nucleoli of cells infected with Zika or Langat virus”. J Gen Virol. 69 ( Pt 8): 1913–20. doi:10.1099/0022-1317-69-8-1913. PMID 2841406.
- ↑ Tang H, Hammack C, Ogden SC, Wen Z, Qian X, Li Y, Yao B, Shin J, Zhang F, Lee EM, Christian KM, Didier RA, Jin P, Song H, Ming GL (2016). “Zika Virus Infects Human Cortical Neural Progenitors and Attenuates Their Growth”. Cell Stem Cell. 18 (5): 587–90. doi:10.1016/j.stem.2016.02.016. PMID 26952870.
- ↑ Boeuf P, Drummer HE, Richards JS, Scoullar MJ, Beeson JG (2016). “The global threat of Zika virus to pregnancy: epidemiology, clinical perspectives, mechanisms, and impact”. BMC Med. 14 (1): 112. doi:10.1186/s12916-016-0660-0. PMC 4973112. PMID 27487767.
- ↑ Sampathkumar P, Sanchez JL (2016). “Zika Virus in the Americas: A Review for Clinicians”. Mayo Clin. Proc. 91 (4): 514–21. doi:10.1016/j.mayocp.2016.02.017. PMID 27046524.
- ↑ Mlakar J, Korva M, Tul N, Popović M, Poljšak-Prijatelj M, Mraz J, Kolenc M, Resman Rus K, Vesnaver Vipotnik T, Fabjan Vodušek V, Vizjak A, Pižem J, Petrovec M, Avšič Županc T (2016). “Zika Virus Associated with Microcephaly”. N. Engl. J. Med. 374 (10): 951–8. doi:10.1056/NEJMoa1600651. PMID 26862926.
- ↑ 18.0 18.1 WHO Zika causality statement http://www.who.int/emergencies/zika-virus/causality/en/
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yazan Daaboul, M.D., Nate Michalak, B.A., Serge Korjian M.D., Yamuna Kondapally, M.B.B.S[2]
Overview
Zika virus infection is caused by Zika virus, an enveloped, single stranded positive sense RNA virus. Zika virus is a type of flavivirus. Mosquitoes are the primary disease vector of Zika virus.
Microbiological Characteristics
- Zika virus, also known as ZIKV is an enveloped, icosahedral virus with a single-stranded, positive sense RNA genome. The most closely related virus is the Spondweni virus and is one of the two viruses in the Spondweni virus clade.[1]
- The Zika virus genome consists of 10,794 nucleotides that encode 3,419 amino acids.[2]
- Zika virus is a member of the Flaviviridae family and of the flavivirus genus.
- There are two lineages for Zika virus: African and Asian.[2]
Transmission
Mosquito Vector Transmission
Transmission of Zika virus to humans is thought to occur mainly through infected mosquitoes.
- The following species have been identified as vectors for Zika virus:[3]
|
|
The table below compares the characteristics of 2 common Aedes species: Ae. aegypti and Ae. albopictus
| Aedes aegypti | Aedes albopictus |
| Bright, silvery, lyre-shaped dorsal pattern and white banded legs | Single longitudinal silvery dorsal stripe and white banded legs |
| Urban areas with or without vegetation | Associated with thickets and arboreal vegetation |
| Bites, rests, and lays eggs both indoors and outdoors | Mostly an outdoor (garden) mosquito |
| Sneaky biter | Aggressive biter |
| Blood from humans mainly, and domestic mammals to a lesser extent | Humans and domestic and wild vertebrates |
| Major production places are human-made containers, treeholes, and bamboo internodes holding water | Preference to treeholes and bamboo internodes with water, can also utilize human-made containers for its immature development |
| Most containers with water used for immature development are within or in close proximity to households | Utilizes water-filled containers around or further away from households |
  |
 
|
Table adapted from the Centers for Disease Control and Prevention (CDC)[3]
Read the CDC infographic on life cycle of Aedes aegypti mosquito here
Human-to-Human Transmission
Zika virus can be trasmitted via mother to child and sexual trasmission.
Mother to child
- A pregnant woman who is already infected with Zika virus can pass the virus to her fetus during the pregnancy or around the time of birth.
- Zika virus has been detected in amniotic fluid, which suggests that Zika virus may cross the placental barrier and vertical transmission is possible.[4] Mosquito-borne ZIKV is thought to initially replicate in dendritic cells near the site of inoculation before spreading to lymph nodes and then the bloodstream. ZIKV can be killed by potassium permanganate, ether, temperatures >60°C, but is not effectively neutralized by 10% ethanol.[2]
- There are no reported cases of Zika virus spread through breastfeeding. Due to the nutritional benefits of breastmilk, mothers are encouraged to breastfeed their infants even in areas where Zika virus is endemic.
Sexual transmission
- Zika virus can be sexually transmitted between humans.[5][6]
- It can be transmitted even if the infected person does not have symptoms.
- Zika virus remains in semen longer than in other body fluids (vaginal fluids, urine, and blood).[7]
Blood transfusion
- Zika virus can be transmitted via blood transfusion but there are no cases reported in United States.
- The transmission of virus through blood transfusion has been reported in Brazil. These cases are under investigation.
- On August 26, 2016, the US Food and Drug Administration (FDA) issued revised guidelines recommending universal testing of donated whole blood and blood components for Zika virus in the United States and its territories.
Laboratory exposure
- There has been one reported laboratory-acquired Zika virus disease in United States.[8]
Virology
- Following a mosquito bite, the incubation period for Zika virus in humans is approximately 3 to 12 days.
- Detection of Zika virus is primarily based on the isolation of RNA from blood serum through PCR in acutely ill patients.[9]
- An ELISA has also been developed by the Centers for Disease Control and Prevention to detect IgM against ZIKV.[2]
- Zika virus has a short viremic period, such that the virus may be detected in serum 3-5 days following the onset of symptoms. Zika virus can be detected in urine up to 10 days following the onset of symptoms.[9]
Refererences
- ↑ FIELDS, B. N., KNIPE, D. M., & HOWLEY, P. M. (2007). Fields virology. Philadelphia, Wolters Kluwer Health/Lippincott Williams & Wilkins.
- ↑ 2.0 2.1 2.2 2.3 Hayes EB (2009). “Zika virus outside Africa”. Emerg Infect Dis. 15 (9): 1347–50. doi:10.3201/eid1509.090442. PMC 2819875. PMID 19788800.
- ↑ Duffy, Mark R.; Chen, Tai-Ho; Hancock, W. Thane; Powers, Ann M.; Kool, Jacob L.; Lanciotti, Robert S.; Pretrick, Moses; Marfel, Maria; Holzbauer, Stacey; Dubray, Christine; Guillaumot, Laurent; Griggs, Anne; Bel, Martin; Lambert, Amy J.; Laven, Janeen; Kosoy, Olga; Panella, Amanda; Biggerstaff, Brad J.; Fischer, Marc; Hayes, Edward B. (2009). “Zika Virus Outbreak on Yap Island, Federated States of Micronesia”. New England Journal of Medicine. 360 (24): 2536–2543. doi:10.1056/NEJMoa0805715. ISSN 0028-4793.
- ↑ http://www.cdc.gov/zika/transmission/index.html CDC Transmission
- ↑ Musso D, Roche C, Robin E, Nhan T, Teissier A, Cao-Lormeau VM (2015). “Potential sexual transmission of Zika virus”. Emerg Infect Dis. 21 (2): 359–61. doi:10.3201/eid2102.141363. PMC 4313657. PMID 25625872.
- ↑ Foy, B. D.; Kobylinski, K. C.; Foy, J. L. C.; Blitvich, B. J.; Travassos Da Rosa, A.; Haddow, A. D.; Lanciotti, R. S.; Tesh, R. B. (2011). “Probable Non–Vector-borne Transmission of Zika Virus, Colorado, USA”. Emerging Infectious Diseases. 17 (5): 880–882. doi:10.3201/eid1705.101939. PMC 3321795. PMID 21529401.
- ↑ Zika virus transmission https://www.cdc.gov/zika/transmission/index.html (August 27, 2016) Accessed on September 15, 2016
- ↑ Zika Virus Transmission. Centers for Disease Control and Prevention (August 27, 2016). http://www.cdc.gov/zika/transmission/index.html Accessed on September 14, 2016
- ↑ 9.0 9.1 http://ecdc.europa.eu/en/healthtopics/zika_virus_infection/factsheet-health-professionals/Pages/factsheet_health_professionals.aspx ECDC Zika virus infection factsheet
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yazan Daaboul, M.D.; Nate Michalak, B.A.; Serge Korjian M.D.; Yamuna Kondapally, M.B.B.S[2]
Overview
A schema for the classification of Zika virus infection has yet to be developed.
Classification
A schema for the classification of Zika virus infection has yet to be developed.
References
Differentiating Zika virus infection from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yazan Daaboul, M.D.; Luke Rusowicz-Orazem, B.S.; Serge Korjian M.D.; Yamuna Kondapally, M.B.B.S[2]
Overview
The broad-ranging clinical symptoms associated with Zika virus infection commonly cause it to be misdiagnosed with multiple similar diseases that are also from the Flaviviridae virus family. Zika virus infection has similar clinical presentation to dengue fever, yellow fever, West Nile virus, and Japanese encephalitis. Zika virus infection is distinct in its milder clinical manifestations and shorter length of infection. The association between Zika virus infection and complications that include congenital anomalies and neurological syndromes is also distinctive. Of note, patients bitten by mosquitoes may be concomitantly infected with Zika virus and other mosquito-borne infections, and co-infection should always be considered.
Differentiating Zika Virus Infection from Other Diseases
- Zika virus infection manifests through a broad range of clinical symptoms shared with multiple different diseases from the Flaviviridae virus family, causing misdiagnosis to be common with the following diseases:[1]
- Of note, patients bitten by mosquitoes may be concomitantly infected with Zika virus and other mosquito-borne infections, and co-infection should always be considered.
- Zika virus infection is clinically distinct from similar diseases by its typically mild symptoms and short length, with symptoms typically lasting 4-7 days total and not requiring hospitalization.[2]
- Zika virus infection-related complications, such as microcephaly and Guillain-Barré syndrome, distinguish Zika virus infection from other Flaviviridae Virus diseases.[3]
Differentiating Zika Fever from Dengue Fever
The following table summarizes the distinguishing and common features between Zika fever and Dengue fever, both of which are transmitted by the Aedes mosquito:
| Dengue Fever | Zika Fever | |
| Common Clinical Features | Biphasic fever pattern, maculopapular rash, arthralgia, headache, and signs of hemorrhage | Fever, maculopapular rash, conjunctivitis, and headache |
| Hemorrhage Common? | Yes | No |
| Symptom Severity | May be severe | Usually mild |
| Symptom Duration | 2 to 7 days | 4 to 7 days |
| Incubation Period | 4 to 10 days | 3 to 12 days |
| Endemicity | Americas, Africa, Southeast Asia | Americas, Africa, Southeast Asia |
| Vector | Aedes mosquito | Aedes mosquito |
| Laboratory Findings | Leucopenia, rising hematocrit (suggestive of impending hemorrhage), thrombocytopenia, elevated liver function tests | Leucopenia but normal hematocrit, platelet count, and liver function tests |
| Diagnosis | RT-PCR or ELISA | RT-PCR or ELISA |
| Treatment | Supportive care, avoid aspirin and other NSAIDs | Supportive care |
References
- ↑ Zika virus. Center for Disease Control and Prevention for Medical Professionals. http://www.cdc.gov/zika/hc-providers/clinicalevaluation.html Accessed on December 10, 2015
- ↑ Outbreak of Exanthematous Illness Associated with Zika, Chikungunya, and Dengue Viruses, Salvador, Brazil. Emerging Infectious Diseases; Center for Disease Control. http://wwwnc.cdc.gov/eid/pdfs/vol21no12_pdf-version.pdf Accessed on December 16, 2015
- ↑ “Epidemiological Alert: Neurological Syndromes, Congenital Malformations, and Zika Virus Infection. Implications for Public Health in the Americas”. Pan American Health Organization. Pan American Health Organization. December 1, 2015. Retrieved December 11, 2015.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yazan Daaboul, M.D., Luke Rusowicz-Orazem, B.S., Serge Korjian M.D., Yamuna Kondapally, M.B.B.S[2], Tarek Nafee, M.D. [3], Shivani Chaparala M.B.B.S [4]
Overview
In 2015, Zika virus infection outbreaks rose dramatically, particularly in Brazil, as was observed by the manifestation of a correlated complication, microcephaly, in infants born to mothers with Zika virus infection at an incidence of approximately 100 per 100,000 infants. The majority of Zika virus infection cases are reported in South Africa and tropical Asia. As of 2014, Zika Virus infection outbreaks have also become more common in South America. Cases reported in other regions of the world are attributed to travel from areas with outbreaks. Zika virus infection affects all age groups, with newborn infants particularly vulnerable due to risk of transmission from the mothers upon birth.
Epidemiology
- Only 1 in 5 people with Zika virus infection usually becomes symptomatic, and symptoms are generally mild, thus it is hard to establish a clear incidence of the infection.
- The incidence of Zika virus infection is often correlated to one of its commonly associated complications, neonatal microcephaly.
- As of November 2015, it is estimated that 99.7/100,000 live births of infants displaying microcephaly may be attributed to Zika virus.
- This is a twenty-fold increase from 2010’s report of 5.7/100,000 cases.[1]
2017 India reported cases
- Between February 2016 and January 2017, 3 laboratory confirmed cases were discovered in India.
- The 3 cases were 1 male and 2 pregnant females.[2]
- The 3 cases did not give any history of recent travels.
- The 2 pregnant women gave birth to fully healthy babies and the male recovered without any complications.
- The government in India has been discrete about the cases and this attitude has been widely critisizesd.[3]
Worldwide Distribution
- According to WHO regional office for Americas, 75 countries and territories have confirmed indigenous vector-borne transmission of Zika virus in the region of Americas.(most recent update December 15, 2016).[4] The following world map shows the workdwide distribution of Zika as of December 2016:

Sexually transmitted Zika
The following table demonstrates the worldwide distribution of confirmed sexually transmitted Zika cases:
| Region | Countries | Number of Cases |
|---|---|---|
| Americas | Argentina, Canada, Chile, Peru, USA | 5 |
| Euro | France, Germany, Italy, Netherlands, Portugal, Spain, UK, Northern Ireland | 7 |
| Western Pacific | New Zealand | 1 |
North America
- Mexico: Showing downward trend on number of confirmed cases.
- United States of America: Zika transmission continues to expand.
- Florida: No new local transmission cases were reported since 7 December 2016. On 9 December, Miami beach area was declared clear of any ongoing active Zika transmission.
- Texas: Five additional cases of suspected locally transmitted Zika virus disease cases were detected in Cameron County.The cases were identified as part of the followup to state’s first case of Zika likely transmitted by mosquito, announced on 28 November, 2016.
Central America
- Central America has decreasing trend of cases except in Panama, where there has been increasing trend of cases since the beginning of outbreak.
- Between late 2015 and early 2016, there was greatest increase in Zika cases in Central America.
Caribbean
- The Caribbean countries are showing decreasing trends expect in Anguilla where, there has been an increasing trend in cases. In Saint Martin, a French oversea territory, the epidemic continues to decline erratically with a recent increase in the number of visits to emergency services.
South America
- All countries of South America are showing decreasing trends except in Paraguay and Peru,particularly in the city of Iquitos,where an increasing tendency is observed.
Africa
- Cape Verde is the only African country with confirmed active Zika transmission since 2015. 9 cases of Zika-associated microcephaly or CNS manifestations have been reported.
Southeast Asia
- On May 15 2017, the WHO has reported 3 confirmed cases of Zika virus in pregnant women in India.
Pacific Islands
- Countries in the pacific islands region with active transmission since 2015 include American Samoa, Kosrae/Micronesia, Fiji, Marshall Islands, New Caledonia, Palau, Papua New Guinea, Samoa, and Tonga.
Singapore
- According to the Centers for Disease Control and Prevention (CDC), the first local transmission of Zika virus infection (Zika) was reported in Singapore in August 2016. As of December 2016, Singapore is reported to be clear of active Zika transmission.
United States
- There have been cases of local level transmission within the continental United States.[5]
- By December 22,2016 – 215 locally-acquired cases have been reported in the United States (100% in Florida) and 34,463 in U.S. territories.
- 4541 travel associated cases have been reported in the United States and 131 in U.S. territories.
The following map demonstrates the distribution of zika virus infections in the United States:

Travel Associated cases of ZIKV

Locally Acquired cases of ZIKV
| State or Territory | Number of Cases |
|---|---|
| Puerto Rico | 33,487 |
| U.S Virgin Islands | 862 |
| Florida | 210 |
| American Samoa | 114 |
| Texas | 5 |
| Laboratory-confirmed Zika virus disease cases reported to ArboNET by state or territory (as of December 22, 2016).[5] | |
Congenital syndrome associated with Zika virus infection
- To date, 22 countries and territories in the Americas have reported confirmed cases of congenital syndrome associated with Zika virus infection. Since the Zika Epidemiological Update of 1 December 2016, Nicaragua has been added to the list of countries that have reported a case of congenital syndrome associated with Zika virus infection for the first time.
Guillain-Barre syndrome (GBS) and other neurological disorders
- Since the Zika Epidemiological Update of 1 December 2016, no new country or territory has reported for the first time cases of Guillan-Barré syndrome (GBS) associated with Zika virus infection.
| Increase in GBS with Zika virus lab confirmation in at least one case of GBS | Zika virus infection laboratory confirmation in at least one case of GBS | Increase in GBS with no Zika virus lab confirmation in any of the cases |
|---|---|---|
| Brazil | Bolivia | Paraguay |
| Colombia | Costa Rica | Saint Vincent and the Grenadines |
| Dominican Republic | Grenada | |
| El Salvador | Haiti | |
| French Guiana | Mexico | |
| Guadeloupe | Panama | |
| Guatemala | ||
| Honduras | ||
| Jamaica | ||
| Martinique | ||
| Puerto Rico | ||
| Suriname | ||
| Venezuela |
Demographics
Age
Gender
- Men and women are equally affected by Zika virus infection.
References
- ↑ 1.0 1.1 “Epidemiological Alert: Neurological Syndromes, Congenital Malformations, and Zika Virus Infection. Implications for Public Health in the Americas”. Pan American Health Organization. Pan American Health Organization. December 1, 2015. Retrieved December 11, 2015.
- ↑ “WHO | Zika virus infection – India”.
- ↑ “Did India hide its first cases of Zika virus? – BBC News”.
- ↑ WHO http://www.paho.org/hq/index.php?option=com_content&id=11599&Itemid=41691 (September 8, 2016) Accessed on September 15, 2016
- ↑ 5.0 5.1 Reported cases http://www.cdc.gov/zika/intheus/maps-zika-us.html (December 22, 2016) Accessed on December 27, 2016
- ↑ “Zika Virus: Geographical Distribution”. CIDRAP Center for Infectious Disease Research and Policy. University of Minnesota. December 1, 2015. Retrieved December 14, 2015.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Serge Korjian M.D., Ilan Dock, B.S., Nate Michalak, B.A., {{YD}], Yamuna Kondapally, M.B.B.S[2]
Overview
The most potent risk factor in the development of Zika virus infection is travel to endemic areas. Other risk factors include exposure to infected individuals via blood transfusion, sexual intercourse, or vertically to fetuses from infected mothers.
Common risk factors
Common risk factors in the development of Zika virus infection include:[1][2]
- Mosquito bites in endemic areas (as listed below as areas of prior outbreaks)
- The most potent risk factors related to contracting Zika virus are traveling to endemic areas, such as Asia and Africa (reported prior to 2007), the Federated States of Micronesia (reported in 2007), and most recently in the South American regions of Chile (reported in 2014), Brazil and Colombia (reported in 2015), Guatemala, El Salvador, Paraguay, Suriname, Venezuela, Puerto Rico, and Mexico (all cases were reported in 2015).
- Perinatal exposure
- Sexual intercourse with infected individuals
- Blood transfusion from an asymptomatic donor in an endemic area
- Accidental laboratory exposure (needle/sharps injury)
- Sickle cell disease
References
- ↑ “Epidemiological Alert: Neurological Syndromes, Congenital Malformations, and Zika Virus Infection. Implications for Public Health in the Americas”. Pan American Health Organization. Pan American Health Organization. December 1, 2015. Retrieved December 11, 2015.
- ↑ Arzuza-Ortega L, Polo A, Pérez-Tatis G, López-García H, Parra E, Pardo-Herrera LC; et al. (2016). “Fatal Sickle Cell Disease and Zika Virus Infection in Girl from Colombia”. Emerg Infect Dis. 22 (5): 925–7. doi:10.3201/eid2205.151934. PMC 4861530. PMID 27089120.
Natural History, Complications, and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yazan Daaboul, M.D., Luke Rusowicz-Orazem, B.S., Serge Korjian M.D., Yamuna Kondapally, M.B.B.S[2]
Overview
Patients who are exposed to Zika virus will develop symptoms 3 and 12 days after contracting the disease. Symptoms will typically begin with a mild headache and fever, then progress to include a maculopapular rash spreading across the body within 24 hours, followed by back pain and conjunctivitis. The symptoms typically last between 4 and 7 days. The prognosis is usually excellent, with the majority of patients recovering fully. Complications include neurological and possibly congenital sequelae, particularly Guillain-Barré syndrome and microcephaly. According to WHO, ZIKV infection during pregnancy is the cause of congenital brain abnormalities including microcephaly.
Natural History
- The symptoms of Zika virus infection usually develop between 3 and 12 days after an individual contracts the disease.[1]
- Zika virus infection symptoms will usually begin with a mild headache and fever. Within 24 hours, symptoms progress to include a maculopapular rash across the face, neck, trunk, upper arms, palms, and soles, malaise, and back pain follow shortly.[2]
- Zika virus infection is usually self-limited, and symptoms typically last 4-7 days.[1]
- Once a person has been infected, he or she is likely to be protected from future infections.
Complications
Complications that may develop from Zika virus infection include neurological disease and possibly congenital malformation:[3]
Infected males and non-pregnant women
Pregnant Women
Neonate
- Congenital microcephaly[5]
- Eye disorders[5]
- Brain lesions
- Brainstem dysfunction
- Other neurologic disorders include:[6]
- Brainstem and cerebellar hypoplasia
- Malformations of the head
- Involuntary movements
- Seizures
- Irritability
- Brainstem dysfunctions such as difficulty in swallowing
- Limb contractures
- Hearing and sight abnormalities
- Delayed myelination
- Severe ventriculomegaly
- Lissencephaly (absence of normal cerebral folds)
Prognosis
- The prognosis for Zika virus infection is excellent, with the majority of patients experiencing full recovery within 4-7 days after symptom manifestation.[1]
- Congenital or neurological sequelae are the main factors of poor prognosis.[3]
- Zika virus-related deaths are uncommon, but several deaths have been reported during outbreaks.
References
- ↑ 1.0 1.1 1.2 “Zika Virus Infection Factsheet for Health Professionals”. European Centre for Disease Prevention and Control. November 11, 2015. Retrieved December 11, 2015.
- ↑ 2.0 2.1 2.2 Hayes EB (2009). “Zika virus outside Africa”. Emerg Infect Dis. 15 (9): 1347–50. doi:10.3201/eid1509.090442. PMC 2819875. PMID 19788800.
- ↑ 3.0 3.1 “Epidemiological Alert: Neurological Syndromes, Congenital Malformations, and Zika Virus Infection. Implications for Public Health in the Americas”. Pan American Health Organization. Pan American Health Organization. December 1, 2015. Retrieved December 11, 2015.
- ↑ Lucas Masiero Araujo, Maria Lucia Brito Ferreira & Osvaldo Jm Nascimento (2016). “Guillain-Barre syndrome associated with the Zika virus outbreak in Brazil”. Arquivos de neuro-psiquiatria. 74 (3): 253–255. doi:10.1590/0004-282X20160035. PMID 27050856. Unknown parameter
|month=ignored (help) - ↑ 5.0 5.1 Boeuf P, Drummer HE, Richards JS, Scoullar MJ, Beeson JG (2016). “The global threat of Zika virus to pregnancy: epidemiology, clinical perspectives, mechanisms, and impact”. BMC Med. 14 (1): 112. doi:10.1186/s12916-016-0660-0. PMC 4973112. PMID 27487767.
- ↑ Complications http://www.who.int/mediacentre/factsheets/zika/en/ (September, 2016) Accessed on September 20, 2016
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Evaluation of Pregnant Women | Evaluation of Infants | Collection and Submission of Fetal Tissues | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Prevention | Guidelines for Pregnant Women | Travel Notice | CDC Response Planning Tips | Risk-based Preparedness for States
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH