
Angioimmunoblastic T-cell lymphoma
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sowminya Arikapudi, M.B,B.S. [2]
Synonyms and keywords: Immunoblastic lymphadenopathy; AILD-type T-cell lymphoma; Lymphogranulomatosis X T-cell lymphoma; AILD-type (lymphogranulomatosis X) T-cell lymphoma
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Raviteja Guddeti, M.B.B.S. [2] Sowminya Arikapudi, M.B,B.S. [3]
Overview
Angioimmunoblastic T-cell lymphoma (AILT) is a mature T-cell lymphoma characterized by a polymorphous lymph node infiltrate showing a marked increase in follicular dendritic cells (FDCs) and high endothelial venules (HEVs). It is also known as immunoblastic lymphadenopathy (Lukes-Collins Classification) and AILD-type (lymphogranulomatosis X) T-cell lymphoma (Kiel Classification). Clonal T-cell receptor and immunoglobulin gene rearrangements are involved in the pathogenesis of angioimmunoblastic T-cell lymphoma. On gross pathology, aborization and proliferation of high endothelial venules are characteristic findings of angioimmunoblastic T-cell lymphoma. On microscopic histopathological analysis, CD4+ T-cells, CD8+ T-cells, and polyclonal plasma cells are characteristic findings of angioimmunoblastic T-cell lymphoma. There are no established causes for angioimmunoblastic T-cell lymphoma. Angioimmunoblastic T-cell lymphoma must be differentiated from other diseases such as peripheral T-cell lymphoma-not otherwise specified, classical Hodgkin’s lymphoma, diffuse large B cell lymphoma, and nodal marginal zone lymphoma. Angioimmunoblastic T-cell lymphoma commonly affects middle-aged or elderly individuals. Angioimmunoblastic T-cell lymphoma affects men and women equally. There are no established risk factors for angioimmunoblastic T-cell lymphoma. According to the the U.S. Preventive Service Task Force (USPSTF), there is insufficient evidence to recommend routine screening for angioimmunoblastic T-cell lymphoma. Common complications of angioimmunoblastic T-cell lymphoma include rheumatoid arthritis, autoimmune hemolytic anemia, vasculitis, and autoimmune thyroid disease. According to the Lugano classification, there are four stages of angioimmunoblastic T-cell lymphoma based on the number of nodes and extranodal involvement. The most common symptoms of angioimmunoblastic T-cell lymphoma include fever, weight loss, skin rash, night sweats, edema, chest pain, abdominal pain, bone pain, fatigue, dark urine, shortness of breath, chronic pain, swelling of joints, and painless swelling of the neck, axilla, groin, thorax, and abdomen. Common physical examination findings of angioimmunoblastic T-cell lymphoma include fever, rash, ulcer, splenomegaly, hepatomegaly, pleural effusion, ascites, chest tenderness, abdomen tenderness, bone tenderness, arthritis, peripheral lymphadenopathy, and central lymphadenopathy. Laboratory tests for angioimmunoblastic T-cell lymphoma include complete blood count (CBC), polyclonal hypergammaglobulinemia, FISH, blood chemistry studies, flow cytometry, immunohistochemistry, and immunophenotyping. Abdominal CT scan may be helpful in the diagnosis of angioimmunoblastic T-cell lymphoma. Findings on CT scan suggestive of angioimmunoblastic T-cell lymphoma include mediastinal lymphadenopathy, inguinal lymphadenopathy, aortal lymphadenopathy, and bilaterally enlarged kidneys. MRI may be helpful in the diagnosis of angioimmunoblastic T-cell lymphoma. Lymph node or extranodal tissue biopsy is diagnostic of angioimmunoblastic T-cell lymphoma. Abdominal ultrasound may be helpful in the diagnosis of angioimmunoblastic T-cell lymphoma. Findings on ultrasound of the abdomen suggestive of angioimmunoblastic T-cell lymphoma include hepatomegaly and splenomegaly. Positron emission tomographic scan may be helpful in the diagnosis of angioimmunoblastic T-cell lymphoma. Findings on positron emission tomographic scan suggestive of angioimmunoblastic T-cell lymphoma include lymphadenopathy and bilaterally enlarged kidneys. Other diagnostic studies for angioimmunoblastic T-cell lymphoma include laparoscopy, laparotomy, bone marrow aspiration, and bone marrow biopsy. The predominant therapy for angioimmunoblastic T-cell lymphoma is chemotherapy. Adjunctive stem cell transplantation may be required in certain cases.
Pathophysiology
Clonal T-cell receptor and immunoglobulin gene rearrangements are involved in the pathogenesis of angioimmunoblastic T-cell lymphoma. On gross pathology, aborization and proliferation of high endothelial venules are characteristic findings of angioimmunoblastic T-cell lymphoma. On microscopic histopathological analysis, CD4+ T-cells, CD8+ T-cells, and polyclonal plasma cells are characteristic findings of angioimmunoblastic T-cell lymphoma.
Causes
There are no established causes for angioimmunoblastic T-cell lymphoma.
Differential Diagnosis
Angioimmunoblastic T-cell lymphoma must be differentiated from other diseases such as peripheral T-cell lymphoma-not otherwise specified, classical Hodgkin’s lymphoma, diffuse large B cell lymphoma, and nodal marginal zone lymphoma.
Epidemiology and demographics
Angioimmunoblastic T-cell lymphoma commonly affects middle-aged or elderly patients. Angioimmunoblastic T-cell lymphoma affects males and females equally.
Risk Factors
There are no established risk factors for angioimmunoblastic T-cell lymphoma.
Screening
According to the the U.S. Preventive Service Task Force (USPSTF), there is insufficient evidence to recommend routine screening for angioimmunoblastic T-cell lymphoma.
Complications
Common complications of angioimmunoblastic T-cell lymphoma include rheumatoid arthritis, autoimmune hemolytic anemia, vasculitis, and autoimmune thyroid disease.
Diagnosis
Staging
According to the Lugano classification, there are four stages of angioimmunoblastic T-cell lymphoma based on the number of nodes and extranodal involvement.
Symptoms
The most common symptoms of angioimmunoblastic T-cell lymphoma include fever, weight loss, skin rash, night sweats, edema, chest pain, abdominal pain, bone pain, fatigue, dark urine, shortness of breath, chronic pain, swelling of joints, and painless swelling of the neck, axilla, groin, thorax, and abdomen.
Physical Examination
Common physical examination findings of angioimmunoblastic T-cell lymphoma include fever, rash, ulcer, splenomegaly, hepatomegaly, pleural effusion, ascites, chest tenderness, abdomen tenderness, bone tenderness, peripheral lymphadenopathy, and central lymphadenopathy.
Laboratory Tests
Laboratory tests for angioimmunoblastic T-cell lymphoma include complete blood count (CBC), polyclonal hypergammaglobulinemia, FISH, blood chemistry studies, flow cytometry, immunohistochemistry, and immunophenotyping.
CT
Abdominal CT scan may be helpful in the diagnosis of angioimmunoblastic T-cell lymphoma. Findings on CT scan suggestive of angioimmunoblastic T-cell lymphoma include mediastinal lymphadenopathy, inguinal lymphadenopathy, aortal lymphadenopathy, and bilaterally enlarged kidneys.
MRI
MRI may be helpful in the diagnosis of angioimmunoblastic T-cell lymphoma.
Biopsy
Lymph node or extranodal tissue biopsy is diagnostic of angioimmunoblastic T-cell lymphoma.
Ultrasound
Abdominal ultrasound may be helpful in the diagnosis of angioimmunoblastic T-cell lymphoma. Findings on ultrasound of the abdomen suggestive of angioimmunoblastic T-cell lymphoma include hepatomegaly and splenomegaly.
Other Imaging Studies
Positron emission tomographic scan may be helpful in the diagnosis of angioimmunoblastic T-cell lymphoma. Findings on positron emission tomographic scan suggestive of angioimmunoblastic T-cell lymphoma include lymphadenopathy and bilaterally enlarged kidneys.
Other Diagnostic Studies
Other diagnostic studies for angioimmunoblastic T-cell lymphoma include laparoscopy, laparotomy, bone marrow aspiration, and bone marrow biopsy.
Treatment
Medical Therapy
The predominant therapy for angioimmunoblastic T-cell lymphoma is chemotherapy. Adjunctive stem cell transplantation may be required.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Sabawoon Mirwais, M.B.B.S, M.D.[2]
Overview
There is limited information about the historical perspective of angioimmunoblastic T-cell lymphoma.
Historical Perspective
There is limited information about the historical perspective of angioimmunoblastic T-cell lymphoma.
References
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Sabawoon Mirwais, M.B.B.S, M.D.[2]
Overview
There is no established system for the classification of angioimmunoblastic T-cell lymphoma.
Classification
There is no established system for the classification of angioimmunoblastic T-cell lymphoma.
References
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [7]; Associate Editor(s)-in-Chief: Raviteja Guddeti, M.B.B.S. [8] Sowminya Arikapudi, M.B,B.S. [9]
Overview
Clonal T-cell receptor and immunoglobulin gene rearrangements are involved in the pathogenesis of angioimmunoblastic T-cell lymphoma. On gross pathology, aborization and proliferation of high endothelial venules are characteristic findings of angioimmunoblastic T-cell lymphoma. On microscopic histopathological analysis, CD4+ T-cells, CD8+ T-cells, and polyclonal plasma cells are characteristic findings of angioimmunoblastic T-cell lymphoma.
Genetics
- Clonal T-cell receptor gene rearrangements are detected in 75% of the cases.[1]
- immunoglobin gene rearrangements are detected in 10% of the cases.[2]
- The Epstein–Barr virus (EBV) is observed in the majority of cases, where the virus has been found in both reactive B-cells (that comprise part of the polymorphous infiltrate) and the neoplastic T-cells.[3][4][5]
- Trisomy 3, trisomy 5, and +X are the most frequent chromosomal abnormalities found in cases.[6][7]
Gross Pathology
A classic morphological finding is the aborization and proliferation of high endothelial venules.[4]
Microscopic Pathology
- Angioimmunoblastic T-cell lymphoma typically has the phenotype of a mixture of CD4+ and CD8+ T-cells, with a CD4:CD8 ratio greater than unity.
- Polyclonal plasma cells, lymphocytes, eosinophils, histiocytes, blast-like B-cells, and CD21+ follicular dendritic cells are also seen.[4]
- Due to the systemic nature of this disease, neoplastic cells can be found in lymph nodes, liver, spleen, skin, and bone marrow.
- Hyperplastic germinal centers and Reed-Sternberg cells can also be seen.[8][9]
Gallery
-
 A kidney biopsy showing effacement of the renal structure by diffuse leukocytic infiltrate, represented mostly by elongated cells with marked artifactual changes.<ref name = casereport>Angioimmunoblastic T-cell lymphoma presenting as giant kidneys: a case report
A kidney biopsy showing effacement of the renal structure by diffuse leukocytic infiltrate, represented mostly by elongated cells with marked artifactual changes.<ref name = casereport>Angioimmunoblastic T-cell lymphoma presenting as giant kidneys: a case report -
![A biopsy of an inguinal lymph node was remarkable for obliteration of the node architecture.[10]](https://www.wikidoc.org/images/6/63/Angioimmunoblastic_T-cell_lymphoma_Biopsy_2.jpg) A biopsy of an inguinal lymph node was remarkable for obliteration of the node architecture.[10]
A biopsy of an inguinal lymph node was remarkable for obliteration of the node architecture.[10] -
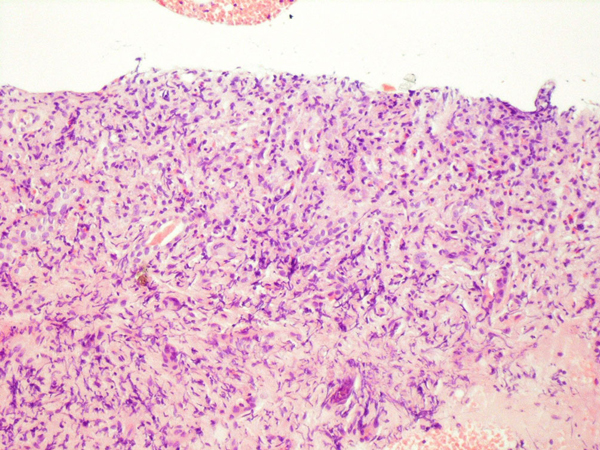
![The paracortical area was infiltrated by cells that were positive for CD3 and CD4.[10]](https://www.wikidoc.org/images/3/3a/Angioimmunoblastic_T-cell_lymphoma_Biopsy_3.jpg) The paracortical area was infiltrated by cells that were positive for CD3 and CD4.[10]
The paracortical area was infiltrated by cells that were positive for CD3 and CD4.[10]

![A biopsy of an inguinal lymph node was remarkable for obliteration of the node architecture.[10]](https://www.wikidoc.org/index.php/File%3AAngioimmunoblastic_T-cell_lymphoma_Biopsy_2.jpg)
![The paracortical area was infiltrated by cells that were positive for CD3 and CD4.[10]](https://www.wikidoc.org/index.php/File%3AAngioimmunoblastic_T-cell_lymphoma_Biopsy_3.jpg)
References
- ↑ [1] Feller AC, Griesser H, Schilling CV, Wacker HH, Dallenbach F, Bartels H, Kuse R, Mak TW, Lennert K. “Clonal gene rearrangement patterns correlate with immunophenotype and clinical parameters in patients with angioimmunoblastic lymphadenopathy.” Am J Pathol. 1988 Dec;133(3):549-56. PMID: 2849301
- ↑ [2] Lipford EH, Smith HR, Pittaluga S, Jaffe ES, Steinberg AD, Cossman J. “Clonality of angioimmunoblastic lymphadenopathy and implications for its evolution to malignant lymphoma.” J Clin Invest. 1987 Feb;79(2):637-42. PMID: 3805286
- ↑ Weiss LM, Jaffe ES, Liu XF, Chen YY, Shibata D, Medeiros LJ (April 1992). “Detection and localization of Epstein-Barr viral genomes in angioimmunoblastic lymphadenopathy and angioimmunoblastic lymphadenopathy-like lymphoma”. Blood. 79 (7): 1789–95. PMID 1373088.
- ↑ 4.0 4.1 4.2 Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Stein, H.; Thiele, J.; Vardiman, J.W (2008). “11 Mature T- and NK-cell neoplasms: Angioimmunoblastic T-cell lymphoma”. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. IARC WHO Classification of Tumours. 2 (4th ed.). IARC. ISBN 9283224310.
- ↑ Anagnostopoulos I, Hummel M, Finn T; et al. (October 1992). “Heterogeneous Epstein-Barr virus infection patterns in peripheral T-cell lymphoma of angioimmunoblastic lymphadenopathy type”. Blood. 80 (7): 1804–12. PMID 1327284.
- ↑ [3] Kaneko Y, Maseki N, Sakurai M, Takayama S, Nanba K, Kikuchi M, Frizzera G. “Characteristic karyotypic pattern in T-cell lymphoproliferative disorders with reactive “angioimmunoblastic lymphadenopathy with dysproteinemia-type” features.” Blood. 1988 Aug;72(2):413-21. PMID: 3261178
- ↑ [4] Schlegelberger B, Zhang Y, Weber-Matthiesen K, Grote W. “Detection of aberrant clones in nearly all cases of angioimmunoblastic lymphadenopathy with dysproteinemia-type T-cell lymphoma by combined interphase and metaphase cytogenetics.” Blood. 1994 Oct 15;84(8):2640-8. PMID: 7919378
- ↑ [5] Quintanilla-Martinez L, Fend F, Moguel LR, Spilove L, Beaty MW, Kingma DW, Raffeld M, Jaffe ES. “Peripheral T-cell lymphoma with Reed-Sternberg-like cells of B-cell phenotype and genotype associated with Epstein-Barr virus infection.” Am J Surg Pathol. 1999 Oct;23(10):1233-40. PMID: 10524524
- ↑ [6] Ree HJ, Kadin ME, Kikuchi M, Ko YH, Go JH, Suzumiya J, Kim DS. “Angioimmunoblastic lymphoma (AILD-type T-cell lymphoma) with hyperplastic germinal centers.” Am J Surg Pathol. 1998 Jun;22(6):643-55. PMID: 9630171
- ↑ 10.0 10.1 Angioimmunoblastic T-cell lymphoma presenting as giant kidneys: a case report http://www.jmedicalcasereports.com/content/3/1/9258 Accessed on November,25 2015
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Raviteja Guddeti, M.B.B.S. [2] Sowminya Arikapudi, M.B,B.S. [3]
Overview
There are no established causes for angioimmunoblastic T-cell lymphoma.
Causes
There are no established causes for angioimmunoblastic T-cell lymphoma.
References
Differential Diagnosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sowminya Arikapudi, M.B,B.S. [2]
Overview
Angioimmunoblastic T-cell lymphoma must be differentiated from other diseases such as peripheral T-cell lymphoma-not otherwise specified, classical Hodgkin’s lymphoma, diffuse large B cell lymphoma, and nodal marginal zone lymphoma.
Differential Diagnosis
Angioimmunoblastic T-cell lymphoma must be differentiated from other diseases such as:
- Peripheral T-cell lymphoma-not otherwise specified
- Classical Hodgkin’s lymphoma
- Diffuse large B cell lymphoma
- Nodal marginal zone lymphoma
References
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [2]; Associate Editor(s)-in-Chief: Raviteja Guddeti, M.B.B.S. [3] Sowminya Arikapudi, M.B,B.S. [4]
Overview
Angioimmunoblastic T-cell lymphoma commonly affects middle-aged or elderly. Angioimmunoblastic T-cell lymphoma affects men and women equally. [1]
Age
Angioimmunoblastic T-cell lymphoma commonly affects middle-aged or elderly.
Gender
Angioimmunoblastic T-cell lymphoma affects men and women equally.
References
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sowminya Arikapudi, M.B,B.S. [2]
Overview
There are no established risk factors for angioimmunoblastic T-cell lymphoma.
Risk Factors
There are no established risk factors for angioimmunoblastic T-cell lymphoma.
References
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sowminya Arikapudi, M.B,B.S. [2]
Overview
According to the the U.S. Preventive Service Task Force (USPSTF), there is insufficient evidence to recommend routine screening for angioimmunoblastic T-cell lymphoma.
Screening
According to the the U.S. Preventive Service Task Force (USPSTF), there is insufficient evidence to recommend routine screening for angioimmunoblastic T-cell lymphoma.[1]
References
- ↑ Recommendations. U.S Preventive Services Task Force. http://www.uspreventiveservicestaskforce.org/BrowseRec/Search?s=angioimmunoblastic+T-cell+lymphoma Accessed on November 27, 2015
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1], Associate Editor(s)-in-Chief: Sowminya Arikapudi, M.B,B.S. [2]
Overview
Common complications of angioimmunoblastic T-cell lymphoma include rheumatoid arthritis, autoimmune hemolytic anemia, vasculitis, and autoimmune thyroid disease.
Complications
Common complications of angioimmunoblastic T-cell lymphoma include:
- Rheumatoid arthritis
- Autoimmune hemolytic anemia
- Vasculitis
- Autoimmune thyroid disease
References
Diagnosis
Diagnosis
Staging | History and Symptoms | Physical Examination | Laboratory Findings | Chest X Ray | CT | MRI | Biopsy | Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH