
Candida vulvovaginitis
For patient information click here Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Kiran Singh, M.D. [2] Dima Nimri, M.D. [3]Aravind Kuchkuntla, M.B.B.S[4]
Synonyms and keywords: Yeast infection, candida vaginitis
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Candida vulvovagintis is an infection of the vagina and the vestibulum, common in women in the reproductive age group. It is caused by various Candida species with Candida albicans most common pathogen followed by other species like Candida glabarta, Candida krusei etc. Patients present with vulvar pruritus, burning micturition and vaginal discharge.The diagnosis of candidal infection requires a collaboration of clinical and diagnostic findings. Patients have typical white cottage chesee like discharge with hyphae and spores demonstrated on microscopy. Patients with uncomplicated infection respond well to topical and oral azole therapy. 5 to 8% of women develop recurrent vaginitis, which is defined as more than 4 episodes in a year. These patients require a longer duration of therapy with an induction and maintenance phase.
Historical Perspective
In 1839, B. Lagenbeck from Germany described a yeast-like fungus for the first time in the human oral infection thrush and its ability to cause it.
Classification
Candida vulvovaginitis can be classified based on the duration, as well as the strain of Candida causing the infection.
Pathophysiology
Several virulence factors of Candida are implicated in vulvovaginitis, but the process of transition from asymptomatic vaginal colonization to symptomatic vulvovaginitis is poorly understood. There may be genetic factors associated with Candida vulvovaginitis, as infection runs in families in many cases and is more common in African-American women.
Causes
Candida yeasts are usually present in most people, but uncontrolled multiplication resulting in disease symptoms is kept in check by other naturally occurring microorganisms, e.g., bacteria co-existing with the yeasts in the same locations, and by the human immune system.
In a study of 1009 women in New Zealand, the fungus, Candida albicans, was isolated from the vaginas of 19% of apparently healthy women. Carriers experienced few or no symptoms. However, external use of irritants (such as some detergents or douches) or internal disturbances (hormonal or physiological) can perturb the normal flora, constituting lactic acid bacteria, such as lactobacilli, and an overgrowth of yeast can result in noticeable symptoms. Pregnancy, the use of oral contraceptives, engaging in vaginal sex immediately and without cleansing after anal sex, and using lubricants containing glycerin have been found to be causally related to yeast infections. Diabetes mellitus and the use of antibiotics are also linked to an increased incidence of yeast infections. Candidiasis can be sexually transmitted from men to women, but not from a woman to a man. Diet has been found to be the cause in some animals. Hormone Replacement Therapy and infertility treatments may also be predisposing factors.
Differentiating candida vulvovaginitis from other Diseases
Candida Vulvovaginitis must be differentiated from diseases with similar presentation such as bacterial vaginosis, trichomonas vaginitis and atrophic vaginitis.
Epidemiology and Demographics
Candida vulvovaginitis is not a reportable disease and epidemiological studies on the prevalence of the disease are hard to perform.
Risk Factors
Antibiotics used to treat other types of infections change the normal balance between organisms in the vagina by decreasing the number of protective bacteria. Being pregnant, having diabetes, or being obese all create conditions that help yeast grow more easily.
Screening
There are no screening recommendations for candida vulvovaginitis.
Natural History, Complications and Prognosis
Candida vulvovaginitis is a self limiting disease with no complications, but few patients develop recurrence. Candida vulvovaginitis is very responsive to local or oral antifungals.
Diagnosis
History and Symptoms
Pruritus is the most significant symptom and candida infection is characterized by a thick, white “cottage cheese-like” vaginal discharge
Physical Examination
Physical examination of of the genitalia will demonstrate edema and erythema of the vulva and labia with fissures and excoriations of the external genitalia.Thick whitish vaginal discharge adherent to the vaginal walls may be present.
Laboratory Findings
A small amount of the vaginal discharge is examined using a microscope (called a wet mount and KOH test). Sometimes, a culture is taken when the infection does not improve with treatment or recurs many times.
Treatment
Medical Therapy
Antifungal agents are indicated in candidiasis. Commonly used drugs include Amphotericin, Clotrimazole, Nystatin, Fluconazole and Ketoconazole.
Surgery
There is no role for surgery in the treatment of Candida vulvovaginitis. Medical therapy with topical and/or oral anti-fungal drugs is the mainstay of treatment.
Prevention
Primary Prevention
There are no means to prevent Candida vulvovaginitis, but wearing a cotton underwear may help reduce the risk of infection.
Secondary Prevention
Prevention of recurrent vulvovaginal candidiasis, maintenance fluconazole prophylaxis may be used.[1] Treatment of a male sexual partner with oral ketoconazole does not seem to influence the cure or recurrence rates in women with Candida vulvovaginitis.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dima Nimri, M.D. [2], Aravind Kuchkuntla, M.B.B.S[3]
Overview
In 1839, B. Lagenbeck from Germany described a yeast-like fungus for the first time in the human oral infection thrush and its ability to cause it.
Historical Perspective
- In 1839, B. Lagenbeck from Germany described a yeast-like fungus for the first time in the human oral infection thrush and its ability to cause it.[1]
- In 1923 the Candida albicans was described by Christine Marie Berkhout. Over the years the classification of the genera and species has evolved. Obsolete names for this genus include Mycotorula and Torulopsis. The species has also been known in the past as Monilia albicans and Oidium albicans. The current classification is nomen conservandum, which means the name is authorized for use by the International Botanical Congress (IBC).
- The full current taxonomic classification is available at Candida albicans.
- The genus Candida includes about 150 different species. However, only a few of those are known to cause human infections. c. albicans is the most significant pathogenic (disease-causing) species. Other Candida species causing diseases in humans include c. tropicalis, c. glabrata, c. krusei, c. parapsilosis, c. dubliniensis, and c. lusitaniae.
References
- ↑ Barnett JA (2008). “A history of research on yeasts 12: medical yeasts part 1, Candida albicans”. Yeast. 25 (6): 385–417. doi:10.1002/yea.1595. PMID 18509848.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dima Nimri, M.D. [2], Aravind Kuchkuntla, M.B.B.S[3]
Overview
Candida vulvovaginitis can be classified based on the duration, as well as the strain of Candida causing the infection.
Classification
Candida vulvovaginitis can be classified based on the duration of the infection and based on the strain of Candida causing the infection.
Duration
Candida vulvovaginitis can be divided based on the duration and number of episodes of the infection into:[1][2][3][4]
- Acute, uncomplicated: these are usually sporadic cases of Candida vulvovaginitis, which respond to topical antifungal therapy and have a high cure rate.
- Acute, complicated: symptoms are more severe than uncomplicated infections and typically require a combination of oral and topical anti-fungal treatment.
- Recurrent Vulvovaginal Candidiasis (RVVC): defined as 4 or more episodes of Candida vulvovaginitis per year, usually caused by the same strain of Candida. Treatment also requires a combination of oral and topical antifungal agents.
- According to 2015, Treatment of STD guidelines – Candida vulvovaginitis can be classified into uncomplicated and complicated based on the following features:[5]
| Uncomplicated Candida Vulvovaginitis | Complicated Candida Vulvovaginitis |
|---|---|
|
|
References
- ↑ Eckert LO (2006). “Clinical practice. Acute vulvovaginitis”. N. Engl. J. Med. 355 (12): 1244–52. doi:10.1056/NEJMcp053720. PMID 16990387.
- ↑ Sobel JD, Faro S, Force RW, Foxman B, Ledger WJ, Nyirjesy PR, Reed BD, Summers PR (1998). “Vulvovaginal candidiasis: epidemiologic, diagnostic, and therapeutic considerations”. Am. J. Obstet. Gynecol. 178 (2): 203–11. PMID 9500475.
- ↑ Sobel JD (2007). “Vulvovaginal candidosis”. Lancet. 369 (9577): 1961–71. doi:10.1016/S0140-6736(07)60917-9. PMID 17560449.
- ↑ Vazquez JA, Sobel JD, Demitriou R, Vaishampayan J, Lynch M, Zervos MJ (1994). “Karyotyping of Candida albicans isolates obtained longitudinally in women with recurrent vulvovaginal candidiasis”. J. Infect. Dis. 170 (6): 1566–9. PMID 7995997.
- ↑ Workowski KA (2015). “Centers for Disease Control and Prevention Sexually Transmitted Diseases Treatment Guidelines”. Clin Infect Dis. 61 Suppl 8: S759–62. doi:10.1093/cid/civ771. PMID 26602614.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dima Nimri, M.D. [2], Aravind Kuchkuntla, M.B.B.S[3]
Overview
Several virulence factors of Candida are implicated in vulvovaginitis, but the process of transition from asymptomatic vaginal colonization to symptomatic vulvovaginitis is poorly understood. There may be genetic factors associated with Candida vulvovaginitis, as infection runs in families in many cases and is more common in African-American women.
Pathophysiology
Vaginal Defensive mechanisms aganist Candida
Innate Mechanisms
| Defense | Mechanism of protection | Evidence of protection |
|---|---|---|
| Vaginal epithelial cells | ||
| Mannose-binding lectin |
|
|
| Activated lactoferrin[4] |
|
|
| Vaginal bacterial flora |
|
|
| Phagocytic systems/polymononuclear leukocytes, mononuclear cells, complement |
|
|
Adaptive Mechanisms
| Defense | Mechanism | Role in Protection |
|---|---|---|
| Immunoglobulin mediated immunity | Systemic IgM, IgG, and local IgA antibodies are produced in response to the infection[6] | |
| Cell Mediated Immunity |
Interleukin 4 (Th2) inhibits anti-Candida activity of nitric oxide and protective pro-inflammatory Th1 cytokines.[8] |
|
Candida Virulence Factors
- C. albicans exists as blastospores, germ tubes, pseudomycelia, true mycelia and chlamydospores on special culture media. C. glabrata exists exclusively in blastospores.
- All strains of Candida species possess a yeast surface mannoprotein which helps in adhering to epithelial cells of the vagina.[10][11]
- Germination of the spores helps in colonizing the vagina.[12]
- Proteolytic enzymes, toxins and phospholipase destroy the proteins that normally impair fungal invasion, enhancing the ability of Candida to colonize the vagina.[10][11][13][14]
- Phenotypic switching of Candida is described in patients with recurrent vaginitis.[15]
- C. albicans can form biofilms on the intrauterine devices or sponges, causing disease recurrence.[16]
Pathogenesis
- Candida vulvovaginitis is a microbial disease and not all patients with detectable pathogen are symptomatic. Multiple risk factors and the imbalance in the protective vaginal defenses predispose patients to develop active disease.
- Candida vaginal infections are more common in the reproductive age group because of the high concentration of estrogen as it increases the amount of glycogen in the vagina providing a carbon source for Candida organisms to colonize. It also increases the adherence of Candida to the vaginal epithelial cells.[17]
- The most common source of the infection is from the perianal area. Other less common source is sexual transmission and persistence of organisms in the vagina after treatment which is responsible for recurrence.[18]
- The initial step of infection is colonization and symptoms appear with the invasion of the blastospores or pseudohyphae of the vaginal wall.[19]
- The understanding of the transition from asymptomatic vaginal colonization with Candida to symptomatic vulvovaginitis is not clear.[11][13]
Genetics
- Few genetic factors are thought to be involved in patients with recurrent Candida vulvovaginitis.[20]
- Supporting evidence is that Candida vaginitis is common in African-American women, runs in families and its association in patients with ABO-Lewis non-secretor phenotype (a rare blood group).
- In addition, women with recurrent Candida vulvovaginitis were found to have decreased concentrations of mannose binding lectin (MBL), hence, the variant (MBL) gene is thought to be a contributing factor in the development of Candida vulvovaginitis.[10][21][2]
Gross Pathology
On speculum examination typical curdy white discharge is present.
-
 This photograph is a speculum examination of the vagina with Candida infection and the typical thick, curdy vaginal discharge. – By Mikael Häggström – Own work, CC0, https://commons.wikimedia.org/w/index.php?curid=35323300
This photograph is a speculum examination of the vagina with Candida infection and the typical thick, curdy vaginal discharge. – By Mikael Häggström – Own work, CC0, https://commons.wikimedia.org/w/index.php?curid=35323300 -
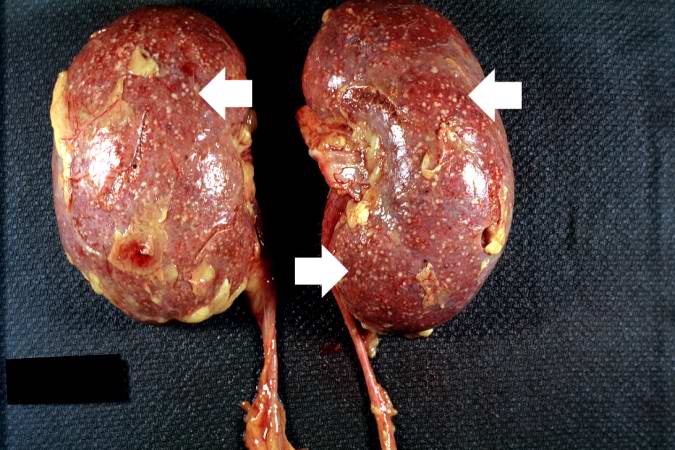 This autopsy photograph of the kidneys demonstrates the multifocal punctate lesions visible on the serosal surface (arrows). Don’t confuse these small yellow punctate lesions with the fat that is adherent to the renal capsule. – © Copyright UAB and the UAB Research Foundation, 1999-2013. All rights reserved
This autopsy photograph of the kidneys demonstrates the multifocal punctate lesions visible on the serosal surface (arrows). Don’t confuse these small yellow punctate lesions with the fat that is adherent to the renal capsule. – © Copyright UAB and the UAB Research Foundation, 1999-2013. All rights reserved -
 This photograph of the cut surface of these kidneys shows that these multifocal punctate lesions are primarily in the cortex (arrows). – © Copyright UAB and the UAB Research Foundation, 1999-2013. All rights reserved
This photograph of the cut surface of these kidneys shows that these multifocal punctate lesions are primarily in the cortex (arrows). – © Copyright UAB and the UAB Research Foundation, 1999-2013. All rights reserved



Microscopic Pathology
Microscopic examination of the wet mount with 10% KOH or saline demonstrates hyphae, pseudohyphae and blastospores.
-
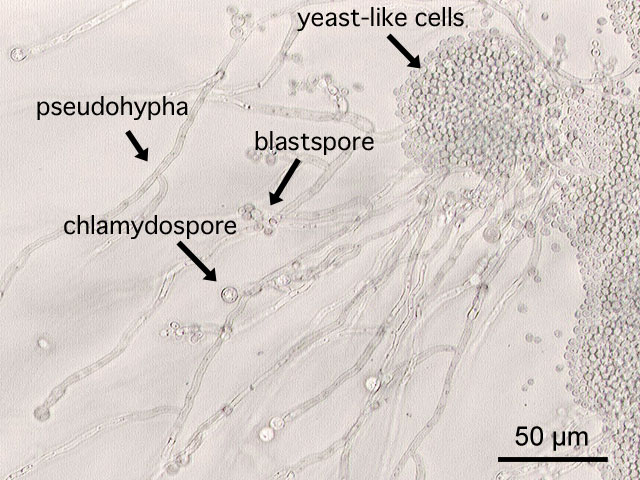 This is a a microscopic image of Candida albicans, grown on cornmeal agar medium. – By Y tambe – Y tambe’s file, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=233284
This is a a microscopic image of Candida albicans, grown on cornmeal agar medium. – By Y tambe – Y tambe’s file, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=233284 -
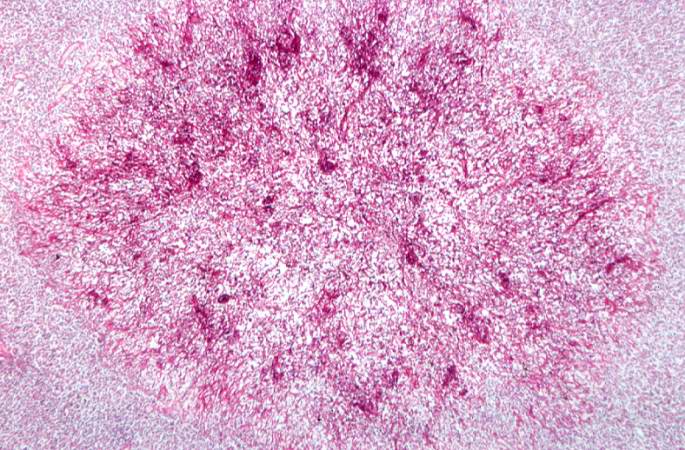
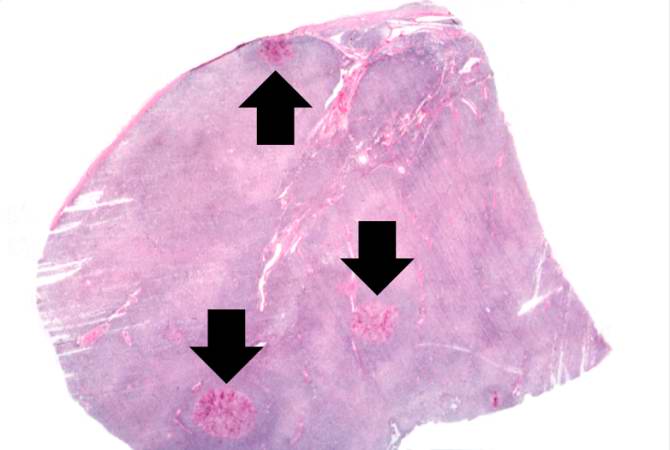 This is a low-power photomicrograph of lymph node with three prominent areas of Candida colonies (arrows). Even at this low magnification, the purple-staining yeast and pseudohyphae can be easily seen. This section was stained with Periodic Acid-Schiff Hematoxylin (PASH), which stains the cell wall of fungi to make them more easily visible. – © Copyright UAB and the UAB Research Foundation, 1999-2013. All rights reserved
This is a low-power photomicrograph of lymph node with three prominent areas of Candida colonies (arrows). Even at this low magnification, the purple-staining yeast and pseudohyphae can be easily seen. This section was stained with Periodic Acid-Schiff Hematoxylin (PASH), which stains the cell wall of fungi to make them more easily visible. – © Copyright UAB and the UAB Research Foundation, 1999-2013. All rights reserved -
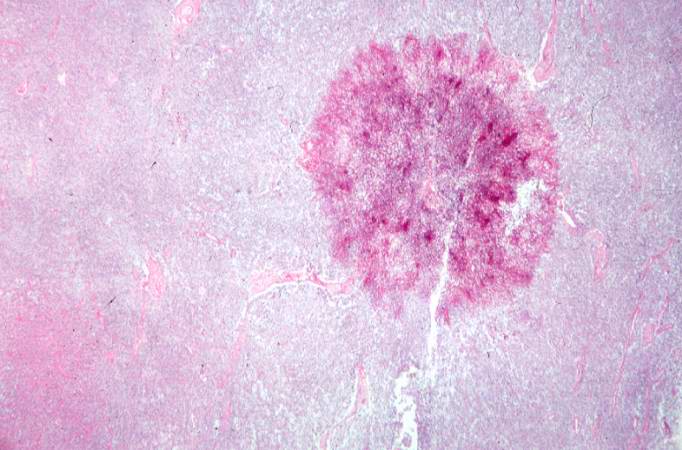 This is a low-power photomicrograph of one of the Candida colonies from this lymph node. The chains of yeast which are termed “pseudohyphae” are apparent at this magnification. – © Copyright UAB and the UAB Research Foundation, 1999-2013. All rights reserved
This is a low-power photomicrograph of one of the Candida colonies from this lymph node. The chains of yeast which are termed “pseudohyphae” are apparent at this magnification. – © Copyright UAB and the UAB Research Foundation, 1999-2013. All rights reserved -
 This higher-power photomicrograph shows the yeasts and pseudohyphae in this focus of Candida organisms. – © Copyright UAB and the UAB Research Foundation, 1999-2013. All rights reserved
This higher-power photomicrograph shows the yeasts and pseudohyphae in this focus of Candida organisms. – © Copyright UAB and the UAB Research Foundation, 1999-2013. All rights reserved -
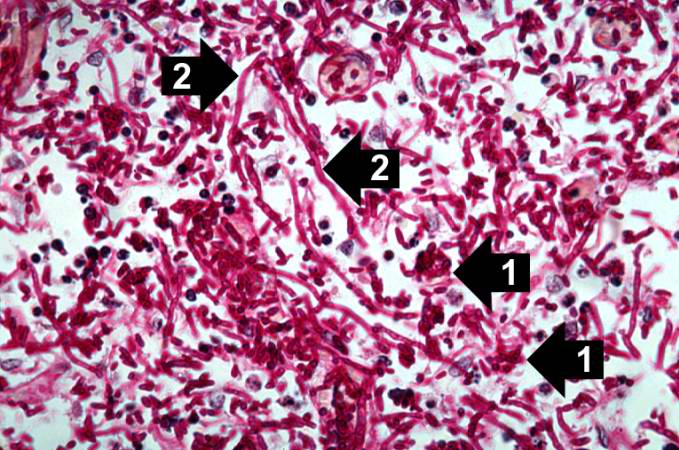 This high-power photomicrograph shows the yeasts (1) and pseudohyphae (2). – © Copyright UAB and the UAB Research Foundation, 1999-2013. All rights reserved
This high-power photomicrograph shows the yeasts (1) and pseudohyphae (2). – © Copyright UAB and the UAB Research Foundation, 1999-2013. All rights reserved





Associated Conditions
- Candida vulvovaginitis may be associated with other pathogens that cause vulvovaginitis. These include Trichomonas vaginalis and Gardnerella vaginalis. The association may be a mixed infection, where 2 or more pathogens are symptomatic, or a co-infection, in which there are 2 or more pathogens but some are not symptomatic.[22][23]
References
- ↑ Barousse MM, Espinosa T, Dunlap K, Fidel PL (2005). “Vaginal epithelial cell anti-Candida albicans activity is associated with protection against symptomatic vaginal candidiasis”. Infect Immun. 73 (11): 7765–7. doi:10.1128/IAI.73.11.7765-7767.2005. PMC 1273905. PMID 16239581.
- ↑ 2.0 2.1 Donders GG, Babula O, Bellen G, Linhares IM, Witkin SS (2008). “Mannose-binding lectin gene polymorphism and resistance to therapy in women with recurrent vulvovaginal candidiasis”. BJOG. 115 (10): 1225–31. doi:10.1111/j.1471-0528.2008.01830.x. PMID 18715406.
- ↑ Ip WK, Lau YL (2004). “Role of mannose-binding lectin in the innate defense against Candida albicans: enhancement of complement activation, but lack of opsonic function, in [[phagocytosis]] by human dendritic cells”. J Infect Dis. 190 (3): 632–40. doi:10.1086/422397. PMID 15243942. URL–wikilink conflict (help)
- ↑ Naidu AS, Chen J, Martinez C, Tulpinski J, Pal BK, Fowler RS (2004). “Activated lactoferrin’s ability to inhibit Candida growth and block yeast adhesion to the vaginal epithelial monolayer”. J Reprod Med. 49 (11): 859–66. PMID 15603095.
- ↑ Diamond RD, Krzesicki R, Jao W (1978). “Damage to pseudohyphal forms of Candida albicans by neutrophils in the absence of serum in vitro”. J Clin Invest. 61 (2): 349–59. doi:10.1172/JCI108945. PMC 372545. PMID 340470.
- ↑ Waldman RH, Cruz JM, Rowe DS (1972). “Immunoglobulin levels and antibody to Candida albicans in human cervicovaginal secretions”. Clin Exp Immunol. 10 (3): 427–34. PMC 1713147. PMID 4556009.
- ↑ Fidel PL, Sobel JD (1996). “Immunopathogenesis of recurrent vulvovaginal candidiasis”. Clin Microbiol Rev. 9 (3): 335–48. PMC 172897. PMID 8809464.
- ↑ Fidel PL (2005). “Immunity in vaginal candidiasis”. Curr Opin Infect Dis. 18 (2): 107–11. PMID 15735412.
- ↑ Fidel PL, Barousse M, Espinosa T, Ficarra M, Sturtevant J, Martin DH; et al. (2004). “An intravaginal live Candida challenge in humans leads to new hypotheses for the immunopathogenesis of vulvovaginal candidiasis”. Infect Immun. 72 (5): 2939–46. PMC 387876. PMID 15102806.
- ↑ 10.0 10.1 10.2 Sobel JD (2007). “Vulvovaginal candidosis”. Lancet. 369 (9577): 1961–71. doi:10.1016/S0140-6736(07)60917-9. PMID 17560449.
- ↑ 11.0 11.1 11.2 Sobel JD (1985). “Epidemiology and pathogenesis of recurrent vulvovaginal candidiasis”. Am. J. Obstet. Gynecol. 152 (7 Pt 2): 924–35. PMID 3895958.
- ↑ Sobel JD, Muller G, Buckley HR (1984). “Critical role of germ tube formation in the pathogenesis of candidal vaginitis”. Infect Immun. 44 (3): 576–80. PMC 263631. PMID 6327527.
- ↑ 13.0 13.1 Sobel JD (1989). “Pathogenesis of Candida vulvovaginitis”. Curr Top Med Mycol. 3: 86–108. PMID 2688924.
- ↑ Schaller M, Bein M, Korting HC, Baur S, Hamm G, Monod M; et al. (2003). “The secreted aspartyl proteinases Sap1 and Sap2 cause tissue damage in an in vitro model of vaginal candidiasis based on reconstituted human vaginal epithelium”. Infect Immun. 71 (6): 3227–34. PMC 155757. PMID 12761103.
- ↑ Soll DR (1988). “High-frequency switching in Candida albicans and its relations to vaginal candidiasis”. Am J Obstet Gynecol. 158 (4): 997–1001. PMID 3284370.
- ↑ Muzny CA, Schwebke JR (2015). “Biofilms: An Underappreciated Mechanism of Treatment Failure and Recurrence in Vaginal Infections”. Clin Infect Dis. 61 (4): 601–6. doi:10.1093/cid/civ353. PMC 4607736. PMID 25935553.
- ↑ Dennerstein GJ, Ellis DH (2001). “Oestrogen, glycogen and vaginal candidiasis”. Aust N Z J Obstet Gynaecol. 41 (3): 326–8. PMID 11592551.
- ↑ Miles MR, Olsen L, Rogers A (1977). “Recurrent vaginal candidiasis. Importance of an intestinal reservoir”. JAMA. 238 (17): 1836–7. PMID 333134.
- ↑ Fidel PL, Vazquez JA, Sobel JD (1999). “Candida glabrata: review of epidemiology, pathogenesis, and clinical disease with comparison to C. albicans”. Clin Microbiol Rev. 12 (1): 80–96. PMC 88907. PMID 9880475.
- ↑ Calderon L, Williams R, Martinez M, Clemons KV, Stevens DA (2003). “Genetic susceptibility to vaginal candidiasis”. Med Mycol. 41 (2): 143–7. PMID 12964847.
- ↑ Liu F, Liao Q, Liu Z (2006). “Mannose-binding lectin and vulvovaginal candidiasis”. Int J Gynaecol Obstet. 92 (1): 43–7. doi:10.1016/j.ijgo.2005.08.024. PMID 16256117.
- ↑ Sobel JD, Subramanian C, Foxman B, Fairfax M, Gygax SE (2013). “Mixed vaginitis-more than coinfection and with therapeutic implications”. Curr Infect Dis Rep. 15 (2): 104–8. doi:10.1007/s11908-013-0325-5. PMID 23354954.
- ↑ Anderson MR, Klink K, Cohrssen A (2004). “Evaluation of vaginal complaints”. JAMA. 291 (11): 1368–79. doi:10.1001/jama.291.11.1368. PMID 15026404.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dima Nimri, M.D. [2], Aravind Kuchkuntla, M.B.B.S[3]
Overview
Candida vulvovaginitis is caused by many different species of Candida. They are divided into Candida albicans and Candida non-albicans species based on the causative pathogen.
Causes
Common Causes
- Candida albicans: These strains are isolated in 85 to 95% patients with yeast infection.[1]
- Candida non albicans: Candida glabrata is the most common isolated pathogen in this group affecting 10 to 20% of women and is associated with recurrent Candida vulvovaginitis.[2]
Less Common Causes
These are less commonly isolated in patients but is important to identify the species as they are less sensitive to standard azole therapy and cause recurrent infection.[3][4]
References
- ↑ Corsello S, Spinillo A, Osnengo G, Penna C, Guaschino S, Beltrame A; et al. (2003). “An epidemiological survey of vulvovaginal candidiasis in Italy”. Eur J Obstet Gynecol Reprod Biol. 110 (1): 66–72. PMID 12932875.
- ↑ Okungbowa FI, Isikhuemhen OS, Dede AP (2003). “The distribution frequency of Candida species in the genitourinary tract among symptomatic individuals in Nigerian cities”. Rev Iberoam Micol. 20 (2): 60–3. PMID 15456373.
- ↑ Bauters TG, Dhont MA, Temmerman MI, Nelis HJ (2002). “Prevalence of vulvovaginal candidiasis and susceptibility to fluconazole in women”. Am J Obstet Gynecol. 187 (3): 569–74. PMID 12237629.
- ↑ Holland J, Young ML, Lee O, C-A Chen S (2003). “Vulvovaginal carriage of yeasts other than Candida albicans”. Sex Transm Infect. 79 (3): 249–50. PMC 1744683. PMID 12794215.
- ↑ Nyirjesy P, Alexander AB, Weitz MV (2005). “Vaginal Candida parapsilosis: pathogen or bystander?”. Infect Dis Obstet Gynecol. 13 (1): 37–41. doi:10.1080/10647440400025603. PMC 1784559. PMID 16040326.
- ↑ Singh S, Sobel JD, Bhargava P, Boikov D, Vazquez JA (2002). “Vaginitis due to Candida krusei: epidemiology, clinical aspects, and therapy”. Clin Infect Dis. 35 (9): 1066–70. doi:10.1086/343826. PMID 12384840.
Differentiating Candidiasis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dima Nimri, M.D. [2], Aravind Kuchkuntla, M.B.B.S[3]
Overview
Candida Vulvovaginitis must be differentiated from diseases with similar presentation such as bacterial vaginosis, trichomonas vaginitis and atrophic vaginitis.
Differentiating Candida Vulvovaginitis from other Diseases
Candida Vulvovaginitis must be differentiated from the following diseases which have a similar presentation:[1][2][3][4][5]
| Disease | Findings |
|---|---|
| Trichomoniasis |
|
| Atrophic vaginitis |
|
| Desquamative inflammatory vaginitis |
|
| Bacterial Vaginosis |
|
References
- ↑ Centers for Disease Control and Prevention. 2015 Sexually Transmitted Diseases Treatment Guidelines. Bacterial Vaginosis. http://www.cdc.gov/std/tg2015/bv.htm Accessed on October 13, 2016
- ↑ Bachmann GA, Nevadunsky NS (2000). “Diagnosis and treatment of atrophic vaginitis”. Am Fam Physician. 61 (10): 3090–6. PMID 10839558.
- ↑ Krieger JN, Tam MR, Stevens CE, Nielsen IO, Hale J, Kiviat NB; et al. (1988). “Diagnosis of trichomoniasis. Comparison of conventional wet-mount examination with cytologic studies, cultures, and monoclonal antibody staining of direct specimens”. JAMA. 259 (8): 1223–7. PMID 2448502.
- ↑ Sobel JD, Reichman O, Misra D, Yoo W (2011). “Prognosis and treatment of desquamative inflammatory vaginitis”. Obstet Gynecol. 117 (4): 850–5. doi:10.1097/AOG.0b013e3182117c9e. PMID 21422855.
- ↑ Eckert LO, Hawes SE, Stevens CE, Koutsky LA, Eschenbach DA, Holmes KK (1998). “Vulvovaginal candidiasis: clinical manifestations, risk factors, management algorithm”. Obstet Gynecol. 92 (5): 757–65. PMID 9794664.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dima Nimri, M.D. [2], Aravind Kuchkuntla, M.B.B.S[3]
Overview
Candida vulvovaginitis is not a reportable disease and epidemiological studies on the prevalence of the disease are hard to perform.
Epidemiology and Demographics
- Epidemiological studies on Candida vulvovaginitis are hard to perform, because of several factors:[1][2]
- Candida vulvovaginitis is not a reportable disease.
- The diagnosis of Candida vulvovaginitis is based on clinical presentation and positive laboratory findings. Relying on a positive culture alone would likely overestimate the prevalence of Candida vulvovaginitis.
- The use of over-the-counter (OTC) topical anti-fungals makes it difficult to conduct epidemiological studies.
- Candida is the second most common cause of vaginal infection in young women following bacterial Vaginosis.[3]
Age
- Incidence of Candida vulvovaginitis is higher in pregnant women.[4][5]
- Women in reproductive age group are prone for Candida vulvovaginits and at least one episode is reported in 70 to 75% in this population group.[6]
- 40 to 50% of patients with a prior yeast infection have multiple episodes of yeast infection.[4]
- Among the adult population 5 to 8% women have more than four episodes of infection.[7]
- In 20% asymptomatic healthy adolescent women, Candida species can be isolated from the vagina.[8]
Race
Candida vulvovaginitis is more prevalent among African American women than white American women.[7]
References
- ↑ Sobel JD, Faro S, Force RW, Foxman B, Ledger WJ, Nyirjesy PR, Reed BD, Summers PR (1998). “Vulvovaginal candidiasis: epidemiologic, diagnostic, and therapeutic considerations”. Am. J. Obstet. Gynecol. 178 (2): 203–11. PMID 9500475.
- ↑ Sobel JD (2007). “Vulvovaginal candidosis”. Lancet. 369 (9577): 1961–71. doi:10.1016/S0140-6736(07)60917-9. PMID 17560449.
- ↑ Allsworth JE, Peipert JF (2007). “Prevalence of bacterial vaginosis: 2001-2004 National Health and Nutrition Examination Survey data”. Obstet Gynecol. 109 (1): 114–20. doi:10.1097/01.AOG.0000247627.84791.91. PMID 17197596.
- ↑ 4.0 4.1 Hurley R, De Louvois J (1979). “Candida vaginitis”. Postgrad Med J. 55 (647): 645–7. PMC 2425644. PMID 523355.
- ↑ García Heredia M, García SD, Copolillo EF, Cora Eliseth M, Barata AD, Vay CA; et al. (2006). “[Prevalence of vaginal candidiasis in pregnant women. Identification of yeasts and susceptibility to antifungal agents]”. Rev Argent Microbiol. 38 (1): 9–12. PMID 16784126.
- ↑ Zuckerman, Andrea; Romano, Mary (2016). “Clinical Recommendation: Vulvovaginitis”. Journal of Pediatric and AdolescentGynecology. 29 (6): 673–679. doi:10.1016/j.jpag.2016.08.002. ISSN 1083-3188.
- ↑ 7.0 7.1 Foxman B, Marsh JV, Gillespie B, Sobel JD (1998). “Frequency and response to vaginal symptoms among white and African American women: results of a random digit dialing survey”. J Womens Health. 7 (9): 1167–74. PMID 9861594.
- ↑ Barousse, M M (2004). “Vaginal yeast colonisation, prevalence of vaginitis, and associated local immunity in adolescents”. Sexually Transmitted Infections. 80 (1): 48–53. doi:10.1136/sti.2002.003855. ISSN 1368-4973.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Dima Nimri, M.D. [2], Aravind Kuchkuntla, M.B.B.S[3]
Overview
Some of the risk factors associated with the development of Candida vulvovaginitis include diabetes mellitus, immunosuppression and recent antibiotic use.
Risk Factors
The following risk factors have been implicated in predisposing patients to Candida vulvovaginitis:
- Previous infection with Candida vulvovaginitis[1]
- Previous infection with neisseria gonorrhea[2]
- Nulliparity[3]
- Luteal phase of the menstrual cycle [3]
- Recent antibiotic use[4]
- Pregnancy[3]
- Diabetes mellitus[5][6]
- Obesity
- Immunosuppression, such as HIV or glucocorticoid use[7]
- Condom use[8]
Risk Factors for Recurrent Candida Vulvovaginitis[9]
| Microbial Factors | Genetic Factors | Host Behavioural Factors | Other Risk Factors |
|---|---|---|---|
|
|
|
|
Table adopted from Vulvovaginal candidiasis Lancet 2007; 369: 1961–71[11]
References
- ↑ Foxman B (1990). “The epidemiology of vulvovaginal candidiasis: risk factors”. Am J Public Health. 80 (3): 329–31. PMC 1404680. PMID 2305918.
- ↑ Eckert LO, Hawes SE, Stevens CE, Koutsky LA, Eschenbach DA, Holmes KK (1998). “Vulvovaginal candidiasis: clinical manifestations, risk factors, management algorithm”. Obstet Gynecol. 92 (5): 757–65. PMID 9794664.
- ↑ 3.0 3.1 3.2 Eckert LO (2006). “Clinical practice. Acute vulvovaginitis”. N. Engl. J. Med. 355 (12): 1244–52. doi:10.1056/NEJMcp053720. PMID 16990387.
- ↑ Wilton L, Kollarova M, Heeley E, Shakir S (2003). “Relative risk of vaginal candidiasis after use of antibiotics compared with antidepressants in women: postmarketing surveillance data in England”. Drug Saf. 26 (8): 589–97. PMID 12825971.
- ↑ de Leon EM, Jacober SJ, Sobel JD, Foxman B (2002). “Prevalence and risk factors for vaginal Candida colonization in women with type 1 and type 2 diabetes”. BMC Infect. Dis. 2: 1. PMC 65518. PMID 11835694.
- ↑ Donders GG (2002). “Lower Genital Tract Infections in Diabetic Women”. Curr Infect Dis Rep. 4 (6): 536–539. PMID 12433331.
- ↑ Duerr A, Heilig CM, Meikle SF, Cu-Uvin S, Klein RS, Rompalo A, Sobel JD (2003). “Incident and persistent vulvovaginal candidiasis among human immunodeficiency virus-infected women: Risk factors and severity”. Obstet Gynecol. 101 (3): 548–56. PMID 12636961.
- ↑ Eckert LO, Hawes SE, Stevens CE, Koutsky LA, Eschenbach DA, Holmes KK (1998). “Vulvovaginal candidiasis: clinical manifestations, risk factors, management algorithm”. Obstet Gynecol. 92 (5): 757–65. PMID 9794664.
- ↑ Sobel JD (2016). “Recurrent vulvovaginal candidiasis”. Am J Obstet Gynecol. 214 (1): 15–21. doi:10.1016/j.ajog.2015.06.067. PMID 26164695.
- ↑ Reed BD, Zazove P, Pierson CL, Gorenflo DW, Horrocks J (2003). “Candida transmission and sexual behaviors as risks for a repeat episode of Candida vulvovaginitis”. J Womens Health (Larchmt). 12 (10): 979–89. doi:10.1089/154099903322643901. PMID 14709186.
- ↑ Sobel JD (2007). “Vulvovaginal candidosis”. Lancet. 369 (9577): 1961–71. doi:10.1016/S0140-6736(07)60917-9. PMID 17560449.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dima Nimri, M.D. [2], Aravind Kuchkuntla, M.B.B.S[3]
Overview
Candida vulvovaginitis is a self limiting disease with no complications. Candida vulvovaginitis is very responsive to local or oral antifungals.
Natural History, Complications and Prognosis
Natural History
Candida vulvovaginitis is a common infection of women in reproductive age group. Patients present with vulvar pruritus, dysuria, and vaginal discharge. Half of the affected patients have multiple episodes of the infection and less than 10% have recurrent infection.[1]
Prognosis
Candida albicans vulvovaginitis has excellent prognosis with azole therapy. Patients with non-Candida albicans infections are prone to have recurrence and treatment with boric acid and oral fluconazole has good prognosis.[2]
Complications
Candida vulvovaginitis is a self limiting disease with no complications.
References
- ↑ Fidel PL, Vazquez JA, Sobel JD (1999). “Candida glabrata: review of epidemiology, pathogenesis, and clinical disease with comparison to C. albicans”. Clin Microbiol Rev. 12 (1): 80–96. PMC 88907. PMID 9880475.
- ↑ Fidel PL, Vazquez JA, Sobel JD (1999). “Candida glabrata: review of epidemiology, pathogenesis, and clinical disease with comparison to C. albicans”. Clin Microbiol Rev. 12 (1): 80–96. PMC 88907. PMID 9880475.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | X Ray | CT | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
External Links
External Links
- National Institute of Allergies and Infections (June 27, 2007). “Vaginitis”. Retrieved 2008-02-21. – fact sheet on vaginitis/vaginal infections
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH