
Cerebral aneurysm
For patient information, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Kalsang Dolma, M.B.B.S.[3] Harmeet Kharoud M.D.[4] Anika Zahoor M.D.[5]
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Anika Zahoor M.D.[2]
Please help WikiDoc by adding more content here. It’s easy! Click here to learn about editing.
Overview
A cerebral aneurysm or brain aneurysm is a cerebrovascular disorder in which weakness in the wall of a cerebral artery or vein causes a localized dilation or ballooning of the blood vessel.
A common location of cerebral aneurysms is on the arteries at the base of the brain, known as the Circle of Willis. Approximately 85% of cerebral aneurysms develop in the anterior part of the Circle of Willis, and involve the internal carotid arteries and their major branches that supply the anterior and middle sections of the brain. The most common sites include the anterior communicating artery (30-35%), the bifurcation of the internal carotid and posterior communicating artery (30-35%), the bifurcation of the middle cerebral artery (20%), the bifurcation of the basilar artery, and the remaining posterior circulation arteries (5%).
Medical Therapy
Surgery
Emergency treatment for individuals with a ruptured cerebral aneurysm generally includes restoring deteriorating respiration and reducing intracranial pressure. Currently there are two treatment options for brain aneurysms. Either surgical clipping or endovascular coiling is usually performed within the first three days to occlude the ruptured aneurysm and reduce the risk of rebleeding.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: José Eduardo Riceto Loyola Junior, M.D.[2] Anika Zahoor M.D.[3]
Overview
Cerebral aneurysm was first described by X.
Historical Perspective
Cerebral aneurysm is defined as
- dilations that occur along the weak points along the arterial circulations within brain. [1]
Size:
- small less than 0.5mm
- Medium 6 to 25mm
- Large greater than 25mm
Types:
- Berry aneurysm
- Fusiform
- Mycotic
Prevalence:
The worldwide prevalence of cerebral aneurysms is approximately 3.2%, with a mean age of 50 and an overall 1:1 gender ratio. This ratio changes significantly after age 50, with an increasing female predominance approaching 2:1, thought to be due to decreased circulating estrogen causing a reduction in the collagen content of the vascular tissue.[1]
References
- Jersey AM, Foster DM. Cerebral Aneurysm. [Updated 2021 Aug 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] ;Associate Editor(s)-in-Chief: Anika Zahoor M.D.[2]
Overview
Cerebral aneurysms can be classified either by size or type.
Classification
Cerebral aneurysms can be classified either by size or type.
Classifying by size
- Small aneurysms have a diameter of less than 15mm.
- Larger aneurysms include those classified as large (15 to 25mm)
- Giant (25 to 50mm)
- Super giant (over 50mm)
Classifying by type
- Saccular aneurysms are those with a saccular outpouching and are the most common form of cerebral aneurysm.
- Berry aneurysms are saccular aneurysms with necks or stems resembling a berry.
- Fusiform aneurysms are aneurysms without stems.
References
1. Pritz MB. Cerebral aneurysm classification based on angioarchitecture. Journal of Stroke and Cerebrovascular Diseases. 2011 Mar 1;20(2):162-7.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] ;Associate Editor(s)-in-Chief: Anika Zahoor M.D.[2]
Overview
Genes involved in the pathogenesis of cerebral aneurysm include [gene1], [gene2], and [gene3]. The pathophysiology of [disease name] depends on the histological subtype.
Pathophysiology
Pathogenesis
Pathogenesis is the mechanism by which a certain factor causes disease (pathos = disease, genesis = development). The term can also be used to describe the development of the disease, whether it is acute, chronic, or recurrent. It can also be used to describe whether the disease causes inflammation, malignancy, necrosis etc.
Template Sentences
IF the pathogenesis of the disease is unclear:
- It is thought that [disease name] is the result of / is mediated by / is produced by / is caused by either hypertension, collagen diseases, or [hypothesis 3].
IF the disease has a known genetic component:
- [Disease name] is transmitted in [mode of genetic transmission] pattern.
- Genes involved in the pathogenesis of [disease name] include [gene1], [gene2], and [gene3].
IF certain pathology findings are characteristic of the disease:
- On gross pathology, [feature1], [feature2], and [feature3] are characteristic findings of [disease name].
- On microscopic histopathological analysis, [feature1], [feature2], and [feature3] are characteristic findings of [disease name].
Other relevant information may include the action of the pathogen on a molecular level, the body’s response, whether or not mutations play a role in the disease development, whether the pathophysiology of the disease is different among subgroups of the disease, etc. Additional template sentences are listed below. Due to the highly variable nature of pathophysiology among various diseases, this list is not comprehensive.
- [Disease or malignancy name] arises from [cell name]s, which are [cell type] cells that are normally involved in [function of cells].
- The development of [disease name] is the result of multiple genetic mutations.
- The progression to [disease name] usually involves the [molecular pathway].
- The pathophysiology of [disease/malignancy] depends on the histological subtype.
- For an example of a pathogenesis section within a pathophysiology page, click here
Pathological Findings
-
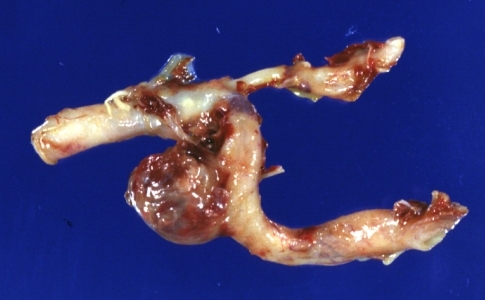
 Brain: Berry Aneurysm: Gross, natural color, close-up, an excellent view of typical berry aneurysm located on anterior cerebral artery
Brain: Berry Aneurysm: Gross, natural color, close-up, an excellent view of typical berry aneurysm located on anterior cerebral artery -
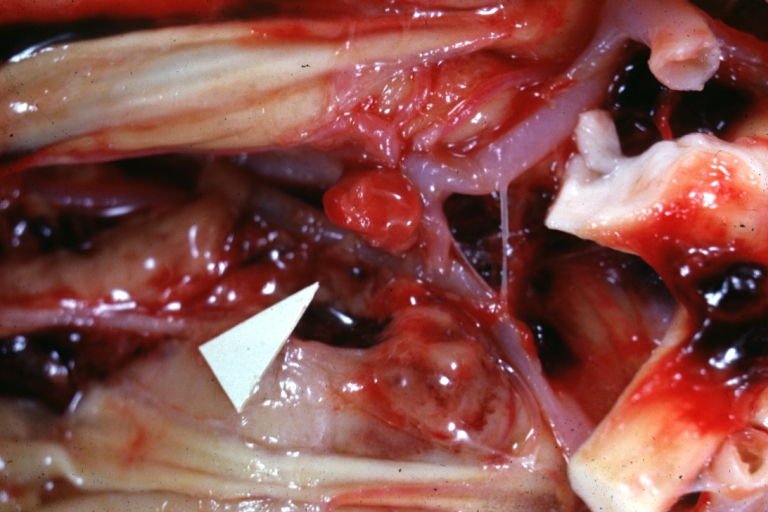
 Brain: Berry Aneurysm Ruptured: Gross fixed tissue aneurysm at junction internal carotid and middle cerebral arteries (an excellent close-up view)
Brain: Berry Aneurysm Ruptured: Gross fixed tissue aneurysm at junction internal carotid and middle cerebral arteries (an excellent close-up view)


References
1.Jung K. H. (2018). New Pathophysiological Considerations on Cerebral Aneurysms. Neurointervention, 13(2), 73–83. https://doi.org/10.5469/neuroint.2018.01011
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] ;Associate Editor(s)-in-Chief: Anika Zahoor M.D.[2]
Overview
Modifiable and non-modifiable risk factors leads to cerebral aneuyrsms.
Causes
Aneurysms may result from
- Congenital defects
- Preexisting conditions such as
The pursuit to identify Genetics of Intracranial Aneurysms has identified a number of locations, most recently 1p34-36, 2p14-15, 7q11, 11q25, and 19q13.1-13.3.
References
1. Jersey AM, Foster DM. Cerebral Aneurysm. [Updated 2022 Apr 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507902/
Differentiating Cerebral aneurysm from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] ;Associate Editor(s)-in-Chief: Anika Zahoor M.D.[2]
Overview
Consider the following differential diagnosis while making diagnosis of cerebral aneurysm
Differenting Cerebral Aneurysms from Other Diseases
- When making an diagnosis for cerebral aneurysm, the following conditions should be kept in mind:
- AV Malformations
- Cavernous sinus syndrome
- Carotid/Vertebral artery dissection
- Cerebral Venous Thrombosis
- Stroke (Ischemic or Hemorrhagic)
- Vein of Galen malformation
References
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Anika Zahoor M.D.[2]
Overview
Age and gender are important risk factor that leads to cerebral aneurysm.
Epidemiology and Demographics
Prevalence
- About 5% of the population has some type of aneurysm in the brain, but only a small number of these aneurysms cause symptoms or rupture.
Age
- Cerebral aneurysms occur more commonly in adults than in children but they may occur at any age.
Gender
- They are slightly more common in women than in men.
References
1. Caranci F, Briganti F, Cirillo L, Leonardi M, Muto M. Epidemiology and genetics of intracranial aneurysms. Eur J Radiol. 2013 Oct;82(10):1598-605. doi: 10.1016/j.ejrad.2012.12.026. Epub 2013 Feb 8. PMID: 23399038.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Anika Zahoor M.D.[2]
Please help WikiDoc by adding more content here. It’s easy! Click here to learn about editing.
Overview:
Following risk factors play an important role in diagnosis of cerebral aneurysm
Risk Factors
Following are risk factors for cerebral aneurysms:
- Family history of cerebral aneurysms
- Certain medical problems such as
References
1. Wang, G. X., Zhang, D., Wang, Z. P., Yang, L. Q., Yang, H., & Li, W. (2018). Risk factors for ruptured intracranial aneurysms. The Indian journal of medical research, 147(1), 51–57. https://doi.org/10.4103/ijmr.IJMR_1665_15
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] ;Associate Editor(s)-in-Chief: Anika Zahoor M.D.[2]
Overview:
Two important risk factors must be considered while screening Cerebral Aneurysm.
Screening:
Two important risk factors in which cerebral aneurysm screening is recommended includes:
1. Positive family history as two or more first-degree relatives with subarachnoid hemorrhages.
2. Polycystic kidney disease.
People who have these risk factors consider a potential candidate for screening.
References
1. Rinkel GJ. Intracranial aneurysm screening: indications and advice for practice. The Lancet Neurology. 2005 Feb 1; 4(2):122-8.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Anika Zahoor M.D.[2]
Please help WikiDoc by adding more content here. It’s easy! Click here to learn about editing.
Overview:
vasospasm is one of the most common complications of the aneurysmal subarachnoid hemorrhage
Complications
Vasospasm
One complication of aneurysmal subarachnoid hemorrhage is the development of vasospasm. Approximately 1 to 2 weeks following the initial hemorrhage, patients may experience ‘spasm’ of the cerebral arteries, which can result in stroke. The etiology of vasospasm is thought to be secondary to an inflammatory process that occurs as the blood in the subarachnoid space is resorbed. It appears that macrophages and neutrophils that enter the subarachnoid space to phagocytose senescent erythrocytes and clear extracorpuscular hemoglobin, remain trapped in the subarachnoid space, die and degranulate 3-4 days after their arrival, and release massive quantities of endothelins and free radicals that in turn induce vasospasm.[1] Vascular narrowing, however, is only one component of the transient inflammatory injury, which is extensive.
Vasospasm is monitored in a variety of ways. Non-invasive methods include transcranial Doppler, which is a method of measuring the velocity of blood in the cerebral arteries using ultrasound. As the vessels narrow due to vasospasm, the velocity of blood increases. The amount of blood reaching the brain can also be measured by CT or MRI or nuclear perfusion scanning.
The definitive, but invasive method of detecting vasospasm is cerebral angiography. It is generally agreed that in order to prevent or reduce the risk of permanent neurological deficits, or even death, vasospasm should be treated aggressively. This is usually performed by early delivery of drug and fluid therapy, or ‘Triple H’ (hypertensive-hypervolemic-hemodilution therapy) (which elevates blood pressure, increases blood volume, and thins the blood) to drive blood flow through and around blocked arteries. For patients who are refractive (resistant) to Triple H therapy, narrowed arteries in the brain can be treated with medication delivered into the arteries that are in spasm and with balloon angioplasty to widen the arteries and increase blood flow to the brain. Although the effectiveness of these treatments is well established, angioplasty and other treatments delivered by interventional radiologists have been in evolution over the past several years. It is generally recommended that aneurysms be evaluated at specialty centers which provide both neurosurgical and interventional radiology treatment and which also permit angioplasty, if needed, without transfer.
Some individuals with a ruptured cerebral aneurysm die from the initial bleeding. Other individuals with cerebral aneurysm recover with little or no neurological deficit.
Prognosis
- The prognosis for a patient with a ruptured cerebral aneurysm depends on the extent and location of the aneurysm, age, general health and neurological condition.
- The most significant factors in determining outcome are grade (see Hunt and Hess grade above) and age. Generally patients with Hunt and Hess grade I and II hemorrhage on admission to the emergency room and patients who are younger within the typical age range of vulnerability can anticipate a good outcome, without death or permanent disability. Older patients and those with poorer Hunt and Hess grades on admission have a poor prognosis. Generally, about two thirds of patients have a poor outcome, death, or permanent disability.[2] [3]
References
- ↑ Gallo, GL (2006). “Leukocyte-endothelial cell interactions in chronic vasospasm after subarachnoid hemorrhage”. Neurol. Res. 28 (7): 750–758. PMID 17164038. Unknown parameter
|coauthors=ignored (help); Unknown parameter|month=ignored (help) - ↑ Hop, Jeanette (1997). “Case-Fatality Rates and Functional Outcome after Subarachnoid Hemorrhage: A Systematic Review”. Stroke. 28 (3): 660–664. PMID 11157554. Unknown parameter
|coauthors=ignored (help); Unknown parameter|month=ignored (help) - ↑ Ljunggren, B (1985). “Cognitive impairment and adjustment in patients without neurological deficit after aneurysmal SAH and early operation”. Journal of Neurosurgery. 62: 673–679. PMID 3989590. Unknown parameter
|coauthors=ignored (help)
Diagnosis
Diagnosis
Diagnostic Criteria | History and Symptoms | Physical Examination | Laboratory Findings | CT | MRI |Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Related Chapters
Related Chapters
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH