
Diphyllobothriasis laboratory tests
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
Overview
Diphyllobothriasis can be diagnosed with the morphological identification of Diphyllobothrium eggs and adults in the stool exam. Molecular diagnosis can also be made with the PCR. Blood tests may show megaloblastic anemia, eosinophilia, and low vitamin B12 level.
Laboratory Findings
Laboratory Findings
Eosinophilia may develop in the early stages of worm growth but the diagnosis is made by microscopy and molecular techniques.
Microscopy
Microscopic identification of eggs in the stool (stool examination) is the basis of specific diagnosis. Eggs are usually numerous and can be demonstrated without concentration techniques. Examination of proglottids passed in the stool is also of diagnostic value.[1][2][3]
Eggs:
- Diphyllobothrium sp. eggs are oval or ellipsoidal and range in size from 55 to 75 µm by 40 to 50 µm.
- There is an operculum at one end that can be inconspicuous, and at the opposite (abopercular) end is a small knob that can be barely discernible.
- The eggs are passed in the stool un-embryonated.
Adults:
- Adults of Diphyllobothrium sp. ranges from 3-12 meters in length.
- The scolex is elongated, 1mm by 3mm, with two shallow, longitudinal grooves. As proglottids mature, they may break off from the stroblia, in lengths containing few to many segments.
- Proglottids are broader than they are long and range from 2 to 4 mm long by 10 to 12 mm wide.
- The uterus is coiled in rosette appearance and the genital pore is at the center of the proglottid.
Molecular Diagnosis
Molecular diagnosis of diphyllobothriasis is based on the identification of nucleotide sequences on cox-1 gene. It is the sensitive method to identify the Diphyllobothrium to the species level. PCR is used to amplify the sequences for the diagnosis of diphyllobothriasis.[2]
Blood tests
Blood tests usually show:
Images
-
 Egg of Diphyllobothrium latum with an operculum. Source: https://www.cdc.gov/dpdx/diphyllobothriasis/index.html
Egg of Diphyllobothrium latum with an operculum. Source: https://www.cdc.gov/dpdx/diphyllobothriasis/index.html -
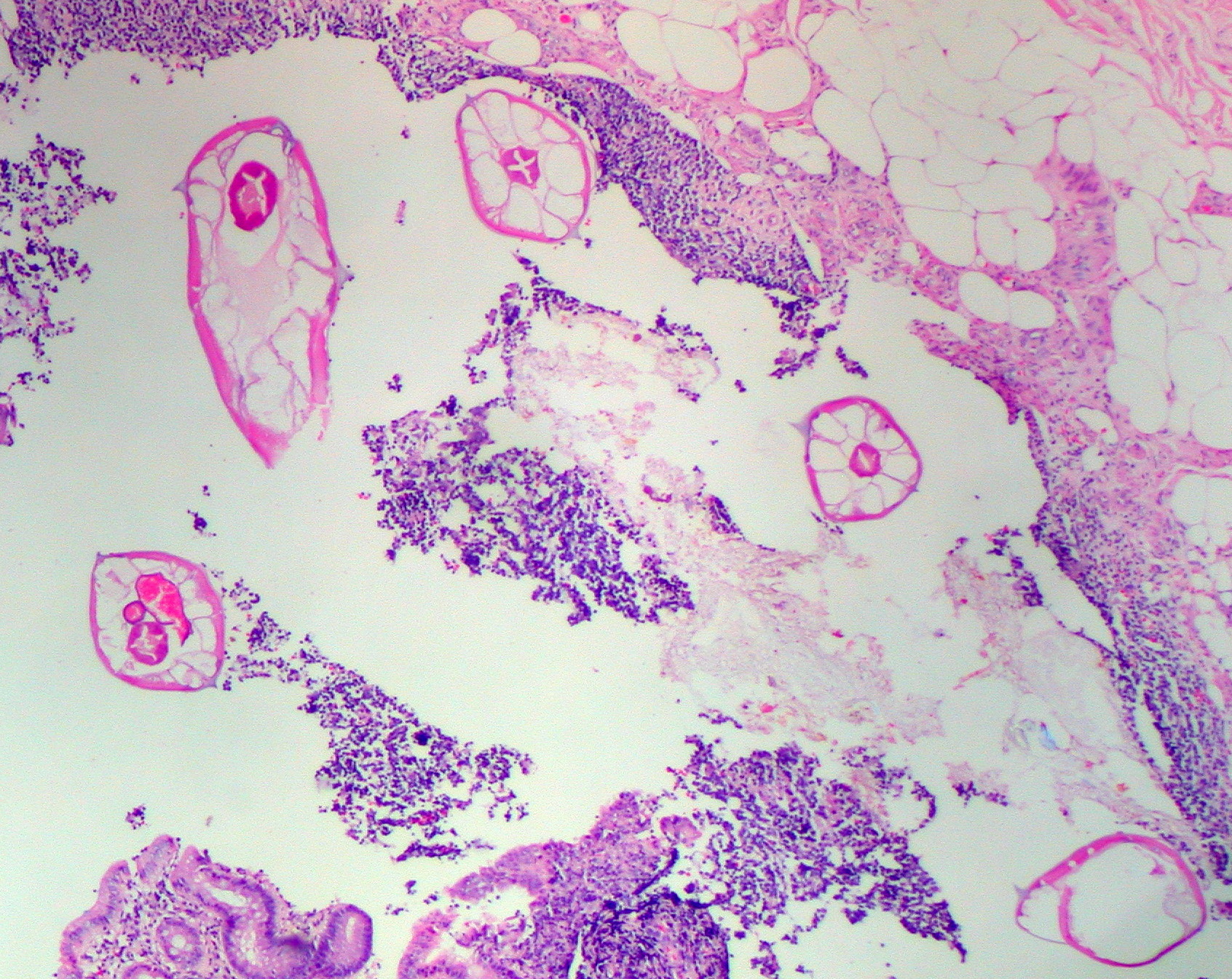 Pinworms are sometimes diagnosed incidentally by pathology. Micrograph of pinworms in the appendix. H&E stain.(By Ed Uthman, MD – http://www.flickr.com/photos/euthman/2395977781/, CC BY-SA 2.0, https://commons.wikimedia.org/w/index.php?curid=3850238)
Pinworms are sometimes diagnosed incidentally by pathology. Micrograph of pinworms in the appendix. H&E stain.(By Ed Uthman, MD – http://www.flickr.com/photos/euthman/2395977781/, CC BY-SA 2.0, https://commons.wikimedia.org/w/index.php?curid=3850238) -
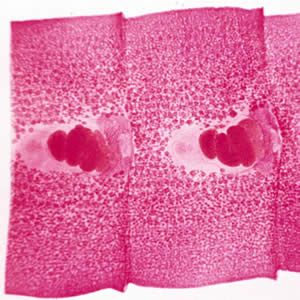
 Proglottids and the rosette-shaped uterus at the center of each proglottid. Source: https://www.cdc.gov/dpdx/diphyllobothriasis/index.html
Proglottids and the rosette-shaped uterus at the center of each proglottid. Source: https://www.cdc.gov/dpdx/diphyllobothriasis/index.html -
 Adult D. latum containing many proglottids. Source: https://www.cdc.gov/dpdx/diphyllobothriasis/index.html (Image courtesy of the Florida State Public Health Laboratory).
Adult D. latum containing many proglottids. Source: https://www.cdc.gov/dpdx/diphyllobothriasis/index.html (Image courtesy of the Florida State Public Health Laboratory). -
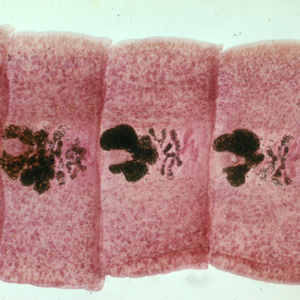
 Carmine-stained proglottids of D. latum, showing the rosette-shaped ovaries. Source: https://www.cdc.gov/dpdx/diphyllobothriasis/index.html
Carmine-stained proglottids of D. latum, showing the rosette-shaped ovaries. Source: https://www.cdc.gov/dpdx/diphyllobothriasis/index.html -
 Carmine-stained proglottids of D. latum, showing the rosette-shaped ovaries. Source: https://www.cdc.gov/dpdx/diphyllobothriasis/index.html
Carmine-stained proglottids of D. latum, showing the rosette-shaped ovaries. Source: https://www.cdc.gov/dpdx/diphyllobothriasis/index.html






References
References
- ↑ Scholz T, Garcia HH, Kuchta R, Wicht B (2009). “Update on the human broad tapeworm (genus diphyllobothrium), including clinical relevance”. Clin. Microbiol. Rev. 22 (1): 146–60, Table of Contents. doi:10.1128/CMR.00033-08. PMC 2620636. PMID 19136438.
- ↑ 2.0 2.1 Kuchta R, Brabec J, Kubáčková P, Scholz T (2013). “Tapeworm Diphyllobothrium dendriticum (Cestoda)–neglected or emerging human parasite?”. PLoS Negl Trop Dis. 7 (12): e2535. doi:10.1371/journal.pntd.0002535. PMC 3873255. PMID 24386497.
- ↑ Baron, Samuel (1996). Medical microbiology. Galveston, Tex: University of Texas Medical Branch at Galveston. ISBN 0-9631172-1-1.
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH