
Diphyllobothriasis
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Kalsang Dolma, M.B.B.S.[2], Furqan M M. M.B.B.S[3]
Synonyms and keywords: Fish tapeworm infection, Broad tapeworm infection, Diphyllobothrium latum infection, Diphyllobothrium infection, Diphyllobothrium nihonkaiense infection, Diphyllobothrium dendriticum infection, Diphyllobothrium cameroni infection, Diphyllobothrium cordatum infection, Diphyllobothrium hians infection, Diphyllobothrium lanceolatum infection, Diphyllobothrium orcini infection, Diphyllobothrium pacificum infection, Diphyllobothrium stemmacephalum infection, Diphyllobothrium scoticum infection
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2], Kalsang Dolma, M.B.B.S.[3]
Overview
Diphyllobothriasis is an infection commonly caused by Diphyllobothrium latum. Eggs of Diphyllobothrium that date back to 4000 BC have been found in France and Germany. In 1592 AD, T. Dunus gave the first recognizable description of the disease and the life cycle was fully elucidated at the end of the 19th century. D. latum has an aquatic life cycle and it is usually transmitted to humans by ingestion of the affected aquatic intermediate host (freshwater or marine fish). It usually causes abdominal pain, diarrhea, and numbness of extremities. Diphyllobothriasis is common in areas with lakes and rivers where humans consume raw or undercooked freshwater fish particularly Japan, Scandinavia, Siberia, and sporadic cases in North and South America. A common risk factor in the development of diphyllobothriasis is consumption of raw or poorly cooked fish meat.The symptoms of diphyllobothriasis usually develop after eating undercooked or raw infected fish meat and start with symptoms such as abdominal pain, diarrhea, nausea, vomiting, and tiredness. If left untreated, patients with diphyllobothriasis may progress to develop complications such as megaloblastic anemia, cholecystitis/cholangitis, and intestinal obstruction. The prognosis of diphyllobothriasis is generally good. Patients with diphyllobothriasis are usually asymptomatic but may be irritated. Physical examination of patients with diphyllobothriasis is usually remarkable for abdominal tenderness, pale conjunctiva, pale skin, and decreased vibration and position senses. The diagnosis is made by identifying eggs of the parasite in stool. Blood tests may show megaloblastic anemia, eosinophilia, and a low vitamin B12 level. Diphyllobothriasis is medically treated with a single dose of praziquantel. The transmission of diphyllobothriasis can be prevented by avoiding undercooked or raw fish meat.
Historical Perspective
Eggs of Diphyllobothrium that date back to 4000 BC have been found in France and Germany. In 1592 AD, T. Dunus gave the first recognizable description of the disease and the life cycle was fully elucidated at the end of the 19th century.
Classification
There is no known classification for diphyllobothriasis but it may be classified on the basis of the organisms causing it.
Pathophysiology
Diphyllobothriasis is a disease caused by Diphyllobothrium latum. D. latum has an aquatic life cycle and is usually transmitted to the humans by ingestion of the affected aquatic intermediate host (freshwater or marine fish). D. latum decreases the intestinal absorption of vitamin B12, resulting in megaloblastic anemia in humans.
Causes
Diphyllobothrium is a genus of tapeworm that can cause Diphyllobothriasis in humans through consumption of raw or under cooked fish. The principal species causing diphyllobothriosis is Diphyllobothrium latum, known as the broad or fish tapeworm, or broad fish tapeworm. D. latum is a pseudophyllidea cestode that infects fish and mammals. D. latum is native to Scandinavia, western Russia, and the Baltics, though it is now also present in North America, especially the Pacific Northwest. Other members of the genus Diphyllobothrium include Diphyllobothrium dendriticum (the salmon tapeworm), which has a much larger range (the whole northern hemisphere), D. pacificum, D. cordatum, D. ursi, D. lanceolatum, D. dalliae, and D. yonagoensis, all of which infect humans only infrequently. In Japan, the most common species causing human infection is D. nihonkaiense, which was only identified as a separate species from D. latum in 1989.[1]
Differentiating (Disease name) from other Conditions
Diphyllobothriasis must be differentiated from tapeworm infections like taeniasis, hymenolepiasis, and schistosomiasis.
Epidemiology and Demographics
Diphyllobothriasis occurs in areas with lakes and rivers where humans consume raw or under cooked freshwater fish. It is particularly common in Japan, Scandinavia, Siberia, with sporadic cases in North and South America.
Risk Factors
A common risk factor in the development of diphyllobothriasis is consumption of raw or poorly cooked fish meat.
Screening
There is insufficient evidence to recommend routine screening for diphyllobothriasis.
Natural History, Complications and Prognosis
The symptoms of diphyllobothriasis usually develop after eating undercooked or raw infected fish meat and start with symptoms such as abdominal pain, diarrhea, nausea, vomiting, and tiredness. If left untreated, patients with diphyllobothriasis may progress to develop complications such as megaloblastic anemia, cholecystitis/cholangitis, and intestinal obstruction. The prognosis of diphyllobothriasis is generally good.
Diagnosis
History and Symptoms
The history of patients with diphyllobothriasis is significant for eating raw or poorly cooked fish meat. The symptoms of diphyllobothriasis may include abdominal pain, diarrhea, nausea, vomiting, and, less commonly, numbness of toes and fingers.
Physical Examination
Patients with diphyllobothriasis are usually asymptomatic but may be irritated. Physical examination of patients with diphyllobothriasis is usually remarkable for abdominal tenderness, pale conjunctiva, pale skin, and decreased vibration and position senses.
Laboratory Findings
Diphyllobothriasis can be diagnosed with the morphological identification of Diphyllobothrium eggs and adults in the stool exam. Molecular diagnosis can also be made with the PCR. Blood tests may show megaloblastic anemia, eosinophilia, and a low vitamin B12 level.
Chest X Ray
There are no X-ray findings associated with diphyllobothriasis.
CT
There are no CT findings associated with diphyllobothriasis.
MRI
There are no MRI findings associated with diphyllobothriasis.
Echocardiography or Ultrasound
There are no echocardiography or ultrasound findings associated with diphyllobothriasis.
Other Imaging Findings
There are no other imaging findings associated with diphyllobothriasis.
Other diagnostic findings
Colonoscopy can reveal Diphyllobothrium latum, usually located in the terminal ileum and extending to the sigmoid colon.
Treatment
Medical Therapy
Drugs used for diphyllobothriasis include praziquantel and niclosamide.
Surgery
Surgical intervention is not recommended for the management of diphyllobothriasis.
Primary Prevention
Effective measures for the primary prevention of diphyllobothriasis include avoiding/limiting consumption of raw fish and proper cooking and storing of fish meat.
Secondary Prevention
The secondary prevention strategies for diphyllobothriasis are similar to its primary preventive measures.
Reference
Historical perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
Eggs of Diphyllobothrium are found in France and Germany dates back to 4000 BC. In 1592 AD, T. Dunus gave the first recognizable description of the disease and the life cycle was fully elucidated at the end of 19th century.
Historical Perspective
Eggs of Diphyllobothrium found in France and Germany dates back to 4000 BC. In 1592 AD, T. Dunus made the first recognizable description of the disease in Locarno, Switzerland.[1][2]
History of the lifecycle of diphyllobothrium latum:
- In 1747 AD, H. D. Sporing recognized the link between the parasite and fish.
- 1758 AD, C. Linnaeus gave the name Taenia to the species.
- At the end of the 19th-century, transmission to humans through consumption of infected fish was elucidated.
- In 1917, Janicki and Rosen identified the role of the copepod as the first intermediate host.
References
- ↑ Scholz T, Garcia HH, Kuchta R, Wicht B (2009). “Update on the human broad tapeworm (genus diphyllobothrium), including clinical relevance”. Clin. Microbiol. Rev. 22 (1): 146–60, Table of Contents. doi:10.1128/CMR.00033-08. PMC 2620636. PMID 19136438.
- ↑ Guttowa A, Moskwa B (2005). “[The history of the exploration of the Diphyllobothrium latum life cycle]”. Wiad Parazytol (in Polish). 51 (4): 359–64. PMID 16913511.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
There is no known classification for diphyllobothriasis but it may be classified on the basis of the organisms causing it.
Classification
Diphyllobothriasis can be classified on the basis of various species responsible for it. The species of Diphyllobothrium involved in the development of Diphyllobothriasis are:[1][2]
- Diphyllobothrium latum (the fish or broad tapeworm)
- Diphyllobothrium nihonkaiense
- Diphyllobothrium dendriticum
- Diphyllobothrium cameroni
- Diphyllobothrium cordatum
- Diphyllobothrium hians
- Diphyllobothrium lanceolatum
- Diphyllobothrium orcini
- Diphyllobothrium pacificum
- Diphyllobothrium stemmacephalum
- Diphyllobothrium scoticum
Gallery
-
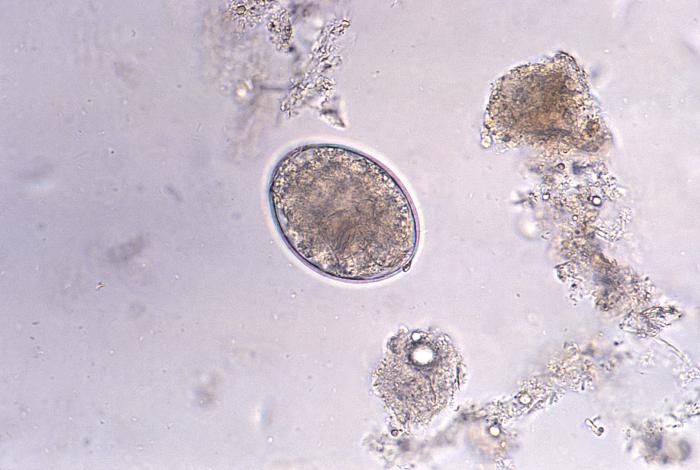 Photomicrograph reveals the presence of a cestode, Diphyllobothrium latum, or “broad” tapeworm, egg, which is described as oval or ellipsoidal, and range in size from 55µm to 75µm by 40µm to 50µm (400X mag). Source: https://phil.cdc.gov/phil/home.asp
Photomicrograph reveals the presence of a cestode, Diphyllobothrium latum, or “broad” tapeworm, egg, which is described as oval or ellipsoidal, and range in size from 55µm to 75µm by 40µm to 50µm (400X mag). Source: https://phil.cdc.gov/phil/home.asp -
 Micrograph reveals an egg of tapeworm cestode parasite Diphyllobothrium latum. Source: https://phil.cdc.gov/phil/home.asp
Micrograph reveals an egg of tapeworm cestode parasite Diphyllobothrium latum. Source: https://phil.cdc.gov/phil/home.asp -
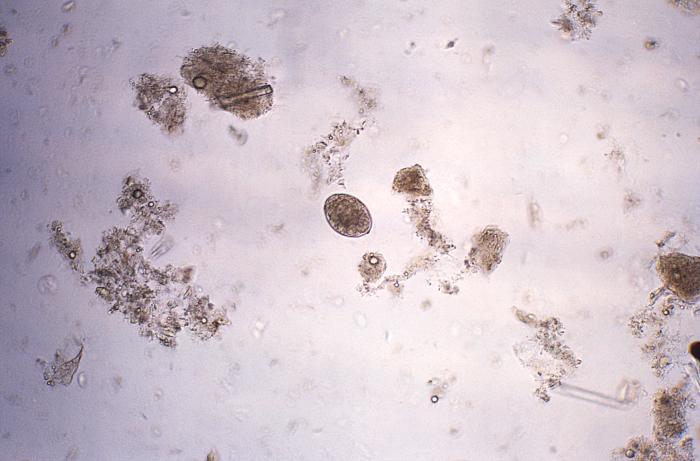 Photomicrograph revealed the presence of a cestode, Diphyllobothrium latum, or “fish” or “broad” tapeworm, egg (128X mag). Source: https://phil.cdc.gov/phil/home.asp
Photomicrograph revealed the presence of a cestode, Diphyllobothrium latum, or “fish” or “broad” tapeworm, egg (128X mag). Source: https://phil.cdc.gov/phil/home.asp



References
- ↑ Scholz T, Garcia HH, Kuchta R, Wicht B (2009). “Update on the human broad tapeworm (genus diphyllobothrium), including clinical relevance”. Clin. Microbiol. Rev. 22 (1): 146–60, Table of Contents. doi:10.1128/CMR.00033-08. PMC 2620636. PMID 19136438.
- ↑ Baron, Samuel (1996). Medical microbiology. Galveston, Tex: University of Texas Medical Branch at Galveston. ISBN 0963117211.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
Diphyllobothriasis is a disease caused by Diphyllobothrium latum. D. latum has an aquatic life cycle and it is usually transmitted to the humans by ingesting the affected aquatic intermediate host (freshwater or marine fish). D. latum decreases the intestinal absorption of vitamin B12 resulting in megaloblastic anemia in humans.
Pathophysiology
Pathogenesis
Diphyllobothrium latum causes the reduced host intake of vitamin B12 resulting in megaloblastic anemia. Like other tapeworms, it can cause local inflammation in the intestine as a result of physical presence.[1]
Lifecycle
The life cycle of Diphyllobothrium latum is completed in the human and marine hosts and comprises of the following stages:[1][2]
- Egg and coracidium:
- Immature eggs are passed in feces of the infected human (or bear, dog, cat, and raccoon).
- If passed into pond or lake water, the eggs mature (approximately 18 to 20 days) and yield coracidium that contains oncospheres.
- First intermediate host:
- After ingestion by a suitable freshwater crustacean (the copepod first intermediate host), the coracidia develop into procercoid larvae in 2-3 weeks.
- Second intermediate host:
- Following ingestion of the copepod by a suitable second intermediate host, typically minnows and other small freshwater fish, the procercoid larvae are released from the crustacean and migrate into the fish flesh where they develop into a plerocercoid larvae (sparganum).
- The plerocercoid larvae are the infective stage for humans. Because humans do not generally eat under cooked minnows and similar small freshwater fish, these do not represent an important source of infection. Nevertheless, these small second intermediate hosts can be eaten by larger predator species, e.g. trout, perch, walleyed pike.
- In this case, the sparganum can migrate to the musculature of the larger predator fish and humans can acquire the disease by eating these later intermediate infected host fish raw or undercooked. Plerocercoids usually lie un-encapsulated in the host tissue but they may be enclosed in connective tissue cysts.
- Definitive host:
- After ingestion of the infected fish, the plerocercoid develops into immature adults and then into mature adult tapeworms which will reside in the small intestine. The adults of D. latum attach to the intestinal mucosa by means of the two bilateral grooves (bothria) of their scolex.
- The adults can reach more than 10 m in length, with more than 3,000 proglottids. Immature eggs are discharged from the proglottids (up to 1,000,000 eggs per day per worm) and are passed in the feces.
- Eggs appear in the feces 5 to 6 weeks after infection. In addition to humans, many other mammals can also serve as definitive hosts for D. latum like the bear, dog, cat, raccoon, and fish-eating birds.

Mode of Transmission
D. latum is transmitted to humans by eating raw, uncooked or undercooked fish.
Gallery
-
![Illustration of the life cycle of Diphyllobothrium spp., the causal agents of Diphyllobothriasis. Source: Public Health Image Library (PHIL). [3]](https://www.wikidoc.org/images/c/cf/Diphyllobothriasis05.jpeg) Illustration of the life cycle of Diphyllobothrium spp., the causal agents of Diphyllobothriasis. Source: Public Health Image Library (PHIL). [3]
Illustration of the life cycle of Diphyllobothrium spp., the causal agents of Diphyllobothriasis. Source: Public Health Image Library (PHIL). [3] -
![Diagram depicts the various stages in the life cycle of the tapeworm Diphyllobothrium latum, a cestode. Source: Public Health Image Library (PHIL). [3]](https://www.wikidoc.org/images/8/85/Diphyllobothriasis03.jpeg) Diagram depicts the various stages in the life cycle of the tapeworm Diphyllobothrium latum, a cestode. Source: Public Health Image Library (PHIL). [3]
Diagram depicts the various stages in the life cycle of the tapeworm Diphyllobothrium latum, a cestode. Source: Public Health Image Library (PHIL). [3]
![Illustration of the life cycle of Diphyllobothrium spp., the causal agents of Diphyllobothriasis. Source: Public Health Image Library (PHIL). [3]](https://www.wikidoc.org/index.php/File%3ADiphyllobothriasis05.jpeg)
![Diagram depicts the various stages in the life cycle of the tapeworm Diphyllobothrium latum, a cestode. Source: Public Health Image Library (PHIL). [3]](https://www.wikidoc.org/index.php/File%3ADiphyllobothriasis03.jpeg)
References
- ↑ 1.0 1.1 Scholz T, Garcia HH, Kuchta R, Wicht B (2009). “Update on the human broad tapeworm (genus diphyllobothrium), including clinical relevance”. Clin. Microbiol. Rev. 22 (1): 146–60, Table of Contents. doi:10.1128/CMR.00033-08. PMC 2620636. PMID 19136438.
- ↑ Baron, Samuel (1996). Medical microbiology. Galveston, Tex: University of Texas Medical Branch at Galveston. ISBN 0963117211.
- ↑ 3.0 3.1 “Public Health Image Library (PHIL)”.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
For details about infections caused by Diphyllobothrium, click here.
Overview
Diphyllobothrium is a genus of tapeworm which can cause Diphyllobothriasis in humans through consumption of raw or undercooked fish. The principal species causing diphyllobothriosis is Diphyllobothrium latum, known as the broad or fish tapeworm, or broad fish tapeworm. D. latum is a pseudophyllid cestode that infects fish and mammals. D. latum is native to Scandinavia, western Russia, and the Baltics, though it is now also present in North America, especially the Pacific Northwest. Other members of the genus Diphyllobothrium include Diphyllobothrium dendriticum (the salmon tapeworm), which has a much larger range (the whole northern hemisphere), D. pacificum, D. cordatum, D. ursi, D. lanceolatum, D. dalliae, and D. yonagoensis, all of which infect humans only infrequently. In Japan, the most common species in human infection is D. nihonkaiense, which was only identified as a separate species from D. latum in 1989.[1]
History
The fish tapeworm has a long documented history of infecting people who regularly consume fish and especially those whose customs include the consumption of raw or undercooked fish. In the 1970’s, most of the known cases of diphyllobothriasis came from Europe (5 million cases), and Asia (4 million cases) with fewer cases coming from North America and South America, and no reliable data on cases from Africa or Australia [2]. Interestingly, despite the relatively small number of cases seen today in South America, some of the earliest archeological evidence of diphyllobothriasis comes from sites in South America. Evidence of Diphyllobothrium spp. has been found in 4,000-10,000 year old human remains on the western coast of South America [3]. There is no clear point in time when Diphyllobothrium latum and related species were “discovered” in humans, but it is clear that diphyllobothriasis has been endemic in human populations for a very long time. Due to the changing dietary habits in many parts of the world, autochthonous, or locally-acquired, cases of diphyllobothriasis have recently been documented in previously non-endemic areas, such as Brazil [4]. In this way, diphyllobothriasis represents an emerging infectious disease in certain parts of the world where cultural practices involving eating raw or undercooked fish are being introduced
Morphology
The adult worm is comprised of three fairly distinct morphological segments; the scolex, the neck and the lower body. The scolex is the head portion of the worm, and is equipped with a slit-like groove (the bothrium) for attachment to the intestine. The scolex attaches to the neck, or proliferative region. From the neck, grows many proglottid segments which contain the reproductive organs of the worm. D. latum is the longest tapeworm in humans, averaging ten meters long. Adults can shed up to a million eggs a day. In adults, proglottids are wider than they are long (hence the name broad tapeworm). As in all pseudophyllid cestodes, the genital pores open mid-ventrally.
Various other species of Diphyllobothrium include:
- Diphyllobothrium nihonkaiense
- Diphyllobothrium dendriticum
- Diphyllobothrium cameroni
- Diphyllobothrium cordatum
- Diphyllobothrium hians
- Diphyllobothrium lanceolatum
- Diphyllobothrium orcini
- Diphyllobothrium pacificum
- Diphyllobothrium stemmacephalum
- Diphyllobothrium scoticum
Life cycle

Adult tapeworms may infect humans, canids, felines, bears, pinnipeds, and mustelids, though the accuracy of the records for some of the nonhuman species is disputed. Immature eggs are passed in feces of the mammal host (the definitive host, where the worms reproduce). After ingestion by a suitable freshwater crustacean such as a copepod (the first intermediate host) the coracidia develop into procercoid larvae. Following ingestion of the copepod by a suitable second intermediate host, typically a minnow or other small freshwater fish, the procercoid larvae are released from the crustacean and migrate into the fish’s flesh where they develop into a plerocercoid larvae (sparganum). The plerocercoid larvae are the infective stage for the definitive host (including humans).
Because humans do not generally eat undercooked minnows and similar small freshwater fish, these do not represent an important source of infection. Nevertheless, these small second intermediate hosts can be eaten by larger predator species, for example, trout, perch, and walleyed pike. In this case, the sparganum can migrate to the musculature of the larger predator fish and mammals can acquire the disease by eating these later intermediate infected host fish raw or undercooked. After ingestion of the infected fish, the plerocercoids develop into immature adults and then into mature adult tapeworms which will reside in the small intestine. The adults attach to the intestinal mucosa by means of the two bilateral grooves (bothria) of their scolex. The adults can reach more than 10 m (up to 30 ft) in length in some species such as D. latum, with more than 3,000 proglottids. One or several of the tape-like proglottid segments (hence the name tape-worm) regularly detach from the main body of the worm and release immature eggs in fresh water to start the cycle over again. Immature eggs are discharged from the proglottids (up to 1,000,000 eggs per day per worm) and are passed in the feces. The incubation period in humans, after which eggs begin to appear in the feces is typically 4-6 weeks, but can vary from as short as 2 weeks to as long as 2 years[5]. The tapeworm can live up to 20 years.
Clinical Symptoms
Symptoms of diphyllobothriasis are generally mild, and can include diarrhea, abdominal pain, vomiting, weight loss, fatigue, constipation and discomfort[6]. Approximately four out of five cases are asymptomatic and may go many years without being detected[7]. In a small number of cases, this leads to severe vitamin B12 deficiency due to the parasite absorbing 80% or more of the host’s B12 intake, and a megaloblastic anemia indistinguishable from pernicious anemia[8]. The anemica can also lead to subtle demyelinative neurological symptoms (subacute combined degeneration of spinal cord). Infection for many years is ordinarily required to deplete the human body of vitamin B12 to the point that neurological symptoms appear.
Diagnosis
Diagnosis is usually made by identifying proglottid segments, or characteristic eggs in the feces[9]. These simple diagnostic techniques are able to identify the nature of the infection to the genus level, which is usually sufficient in a clinical setting [10]. However, when the species needs to be determined (in epidemiological studies, for example), restriction fragment length polymorphisms can be effectively used. PCR can be performed on samples of purified eggs, or native fecal samples following sonication of the eggs to release their contents [11].
Differential diagnosis
Diphyllobothrium infection must be differentiated from other causes of viral, bacterial, and parasitic gastroentritis.
| Organism | Age predilection | Travel History | Incubation Size (cell) | Incubation Time | History and Symptoms | Diarrhea type8 | Food source | Specific consideration | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fever | N/V | Cramping Abd Pain | Small Bowel | Large Bowel | Inflammatory | Non-inflammatory | |||||||||
| Viral | Rotavirus | <2 y | – | <102 | <48 h | + | + | – | + | + | – | Mostly in day cares, most common in winter. | |||
| Norovirus | Any age | – | 10 -103 | 24-48 h | + | + | + | + | + | – | Most common cause of gastroenteritis, abdominal tenderness, | ||||
| Adenovirus | <2 y | – | 105 -106 | 8-10 d | + | + | + | + | + | – | No seasonality | ||||
| Astrovirus | <5 y | – | 72-96 h | + | + | + | + | + | Seafood | Mostly during winter | |||||
| Bacterial | Escherichia coli | ETEC | Any age | + | 108 -1010 | 24 h | – | + | + | + | + | – | Causes travelers diarrhea, contains heat-labile toxins (LT) and heat-stable toxins (ST) | ||
| EPEC | <1 y | – | 10† | 6-12 h | – | + | + | + | + | Raw beef and chicken | – | ||||
| EIEC | Any ages | – | 10† | 24 h | + | + | + | + | + | Hamburger meat and unpasteurized milk | Similar to shigellosis, can cause bloody diarrhea | ||||
| EHEC | Any ages | – | 10 | 3-4 d | – | + | + | + | + | Undercooked or raw hamburger (ground beef) | Known as E. coli O157:H7, can cause HUS/TTP. | ||||
| EAEC | Any ages | + | 1010 | 8-18 h | – | – | + | + | + | – | May cause prolonged or persistent diarrhea in children | ||||
| Salmonella sp. | Any ages | + | 1 | 6 to 72 h | + | + | + | + | + | Meats, poultry, eggs, milk and dairy products, fish, shrimp, spices, yeast, coconut, sauces, freshly prepared salad. | Can cause salmonellosis or typhoid fever. | ||||
| Shigella sp. | Any ages | – | 10 – 200 | 8-48 h | + | + | + | + | + | Raw foods, for example, lettuce, salads (potato, tuna, shrimp, macaroni, and chicken) | Some strains produce enterotoxin and Shiga toxin similar to those produced by E. coli O157:H7 | ||||
| Campylobacter sp. | <5 y, 15-29 y | – | 104 | 2-5 d | + | + | + | + | + | Undercooked poultry products, unpasteurized milk and cheeses made from unpasteurized milk, vegetables, seafood and contaminated water. | May cause bacteremia, Guillain-Barré syndrome (GBS), hemolytic uremic syndrome (HUS) and recurrent colitis | ||||
| Yersinia enterocolitica | <10 y | – | 104 -106 | 1-11 d | + | + | + | + | + | Meats (pork, beef, lamb, etc.), oysters, fish, crabs, and raw milk. | May cause reactive arthritis; glomerulonephritis; endocarditis; erythema nodosum.
can mimic appendicitis and mesenteric lymphadenitis. | ||||
| Clostridium perfringens | Any ages | > 106 | 16 h | – | – | + | + | + | Meats (especially beef and poultry), meat-containing products (e.g., gravies and stews), and Mexican foods. | Can survive high heat, | |||||
| Vibrio cholerae | Any ages | – | 106-1010 | 24-48 h | – | + | + | + | + | Seafoods, including molluscan shellfish (oysters, mussels, and clams), crab, lobster, shrimp, squid, and finfish. | Hypotension, tachycardia, decreased skin turgor. Rice-water stools | ||||
| Parasites | Protozoa | Giardia lamblia | 2-5 y | + | 1 cyst | 1-2 we | – | – | + | + | + | Contaminated water | May cause malabsorption syndrome and severe weight loss | ||
| Entamoeba histolytica | 4-11 y | + | <10 cysts | 2-4 we | – | + | + | + | + | Contaminated water and raw foods | May cause intestinal amebiasis and amebic liver abscess | ||||
| Cryptosporidium parvum | Any ages | – | 10-100 oocysts | 7-10 d | + | + | + | + | + | Juices and milk | May cause copious diarrhea and dehydration in patients with AIDS especially with 180 > CD4 | ||||
| Cyclospora cayetanensis | Any ages | + | 10-100 oocysts | 7-10 d | – | + | + | + | + | Fresh produce, such as raspberries, basil, and several varieties of lettuce. | More common in rainy areas | ||||
| Helminths | Trichinella spp | Any ages | – | Two viable larvae (male and female) | 1-4 we | – | + | + | + | + | Undercooked meats | More common in hunters or people who eat traditionally uncooked meats | |||
| Taenia spp | Any ages | – | 1 larva or egg | 2-4 m | – | + | + | + | + | Undercooked beef and pork | Neurocysticercosis: Cysts located in the brain may be asymptomatic or seizures, increased intracranial pressure, headache. | ||||
| Diphyllobothrium latum | Any ages | – | 1 larva | 15 d | – | – | – | + | + | Raw or undercooked fish. | May cause vitamin B12 deficiency | ||||
8Small bowel diarrhea: watery, voluminous with less than 5 WBC/high power field
Large bowel diarrhea: Mucousy and/or bloody with less volume and more than 10 WBC/high power field
† It could be as high as 1000 based on patient’s immunity system.
The table below summarizes the findings that differentiate inflammatory causes of chronic diarrhea[12][13][14][15][15]
| Cause | History | Laboratory findings | Diagnosis | Treatment |
|---|---|---|---|---|
| Diverticulitis |
|
|
Abdominal CT scan with oral and intravenous (IV) contrast | bowel rest, IV fluid resuscitation, and broad-spectrum antimicrobial therapy which covers anaerobic bacteria and gram-negative rods |
| Ulcerative colitis |
|
|
Endoscopy | Induction of remission with mesalamine and corticosteroids followed by the administration of sulfasalazine and 6-Mercaptopurine depending on the severity of the disease. |
| Entamoeba histolytica |
|
cysts shed with the stool | detects ameba DNA in feces | Amebic dysentery
Luminal amebicides for E. histolytica in the colon:
For amebic liver abscess:
|
Treatment
Upon diagnosis, treatment is quite simple and effective. The standard treatment for diphyllobothriasis, as well as many other tapeworm infections is a single dose of Praziquantel, 5-10 mg/kg PO once for both adults and children. An alternative treatment is Niclosamide, 2 g PO once for adults or 50 mg/kg PO once [16]. Another interesting potential diagnostic tool and treatment is the contrast medium, Gastrografin, introduced into the duodenum, which allows both visualization of the parasite, and has also been shown to cause detachment and passing of the whole worm [17].
Side Effects of Treatment
Praziquantel has few side effects, many of which are similar to the symptoms of diphyllobothriasis. They include malaise, headache, dizziness, abdominal discomfort, nausea, rise in temperature and occasionally allergic skin reactions [18]. The side effects of Niclosamide are very rare, due to the fact that it is not absorbed in the gastrointestinal tract [19].
Epidemiology
People at high risk for infection have traditionally been those who regularly consume raw fish, including fishermen who eat the raw liver or roe of their catches and women preparing and tasting foods that contain raw fish [20]. Many regional cuisines include raw or undercooked food, including sushi and sashimi in Japanese cuisine, carpaccio di persico in Italian, tartare maison in French-speaking populations, gefilte fish in Jewish populations, ceviche in Latin American cuisine. With emigration and globalization, the practice of eating raw fish in these and other dishes has brought diphyllobothriasis to new parts of the world and created new endemic foci of disease[21].
Public Health Strategies
The most viable interventions include: prevention of water contamination both by raising public awareness of the dangers of defecating in recreational bodies of water and by implementation of basic sanitation measures; screening and successful treatment of people infected with the parasite; and prevention of infection of humans via consumption of raw, infected fish [22]. The last of these can most easily be changed via education about proper preparation of fish. Fish that is thoroughly cooked, brined, or frozen at -10˚C for 24-48 hours can be consumed without risk of D. latum infection.
See also
http://www.stanford.edu/class/humbio103/parasites.htm
References
- “DPDx – Diphyllobothriasis”. CDC Division of Parasitic Diseases.
- “UDiphyllobothrium spp”. S FDA/CFSAN – Bad Bug Book.
- Janovy, John; Roberts, Larry S. (2005). Foundations of Parasitology (7th ed.). McGraw-Hill Education (ISE Editions). ISBN 0-07-111271-5.
- ↑ Lou YS, Koga M, Higo H; et al. (1989). “A human infection of the cestode, Diphyllobothrium nihonkaiense“. Fukuoka Igaku Zasshi. 80: 446–50. PMID 2807129.
- ↑ Scholz, T; et al. (2009). “Update on the human broad tapeworm (genus Diphyllobothrium), including clinical relevance”. Clinical Microbiology Reviews. 22: 146–160. PMID 19136438.
- ↑ Reinhard, KJ (1992). “Parasitology as an interpretive tool in archaeology”. American Antiquity. 57: 231–245.
- ↑ Llaguno, Mauricio M., et al. “Diphyllobothrium latum infection in a non-endemic country: case report.” (2008) Revista da Sociedade Brasileira de Medicina Tropical, 41 (3), 301-303
- ↑ http://web.gideononline.com/web/epidemiology/
- ↑ http://www.dpd.cdc.gov/dpdx/HTML/diphyllobothriasis.htm
- ↑ Sholz, et al. (2009)
- ↑ John, David T. and Petri, William A. (2006)
- ↑ http://web.gideononline.com/web/epidemiology/
- ↑ Sholz, et al. (2009)
- ↑ Sholz, et al. (2009)
- ↑ Konvolinka CW (1994). “Acute diverticulitis under age forty”. Am J Surg. 167 (6): 562–5. PMID 8209928.
- ↑ Silverberg MS, Satsangi J, Ahmad T, Arnott ID, Bernstein CN, Brant SR; et al. (2005). “Toward an integrated clinical, molecular and serological classification of inflammatory bowel disease: report of a Working Party of the 2005 Montreal World Congress of Gastroenterology”. Can J Gastroenterol. 19 Suppl A: 5A–36A. PMID 16151544.
- ↑ Satsangi J, Silverberg MS, Vermeire S, Colombel JF (2006). “The Montreal classification of inflammatory bowel disease: controversies, consensus, and implications”. Gut. 55 (6): 749–53. doi:10.1136/gut.2005.082909. PMC 1856208. PMID 16698746.
- ↑ 15.0 15.1 Haque R, Huston CD, Hughes M, Houpt E, Petri WA (2003). “Amebiasis”. N Engl J Med. 348 (16): 1565–73. doi:10.1056/NEJMra022710. PMID 12700377.
- ↑ http://www.dpd.cdc.gov/dpdx/HTML/PDF_Files/MedLetter/TapewormInfection.pdf
- ↑ Ko, S.B. “Observation of deworming process in intestinal Diphyllobothrium latum parasitism by Gastrografin injection into jejunum through double-balloon enteroscope.” (2008) from Letter to the Editor; American Journal of Gastroenterology, 103; 2149-2150.
- ↑ Sholz, et al. (2009)
- ↑ Sholz, et al. (2009)
- ↑ Sholz, et al. (2009)
- ↑ Sholz, et al. (2009)
- ↑ Sholz, et al. (2009)
de:Fischbandwurm id:Cacing pita ikan la:Diphyllobothrium latum nl:Vislintworm fi:Lapamato sv:Bred binnikemask
Differentiating Diphyllobothriasis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
Diphyllobothriasis must be differentiated from tapeworm infections like taeniasis, hymenolepiasis, and schistosomiasis.
Differentiating diphyllobothriasis from other diseases
Diphyllobothriasis must be differentiated from tapeworm infections like taeniasis, hymenolepiasis, and schistosomiasis.[1]
| Infections | Common causative threadworms | Suggestive findings | Diagnostic approach | Treatment |
|---|---|---|---|---|
| Diphyllobothriasis |
|
|||
| Taeniasis |
|
|||
| Hymenolepiasis |
|
|||
| Schistosomiasis |
|
References
- ↑ Baron, Samuel (1996). Medical microbiology. Galveston, Tex: University of Texas Medical Branch at Galveston. ISBN 0-9631172-1-1.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
Diphyllobothriasis occurs in areas where lakes and rivers coexist with human consumption of raw or undercooked freshwater fish. It is particularly common in Japan, Scandinavia, Siberia, with sporadic cases in North and South America.
Epidemiology and Demographics
Diphyllobothriasis is more common in people eating raw or undercooked fish. Infection with the broad fish tapeworm is common in temperate and subarctic regions, wherever freshwater fish are eaten raw, as in Scandinavia, Siberia, the Great Lakes, Japan, central Europe, and Chile.
Prevalance
Worldwide, the prevalence of diphyllobothriasis was estimated in the early 1970s to affect 9 million humans globally. Most of the cases were in Europe and Asia with sporadic cases in America. More recent data indicate that 20 million people are infected worldwide but no recent estimation concerning the global prevalence of this parasitosis has been done.[1]
Incidence
Diphyllobothriasis is endemic in Japan and 100 cases are reported every year since the 1970s.[1]
Age
There is no age predilection for diphyllobothriasis.
Gender
There is no gender predilection for diphyllobothriasis.
Race
There is no racial predilection for diphyllobothriasis.
Developed Countries
It is endemic in Japan and Russia. Sporadic cases are reported in Europe and America.[1]
Developing Countries
Sporadic cases are reported in the developing countries of Asia. NO reports are present to suggest the presence of diphyllobothriasis in Africa.[1]
References
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
The common risk factors in the development of diphyllobothriasis are eating raw or poorly cooked fish meat.
Risk Factors
Common risk factors associated with diphyllobothriasis are:[1][2]
- Eating raw or poorly cooked freshwater and marine fish meat.
- Eating dishes made from raw meat (sushi, sashimi, carpaccio, and ceviche).
- Tasting foods containing raw fish, while cooking.
References
- ↑ Scholz T, Garcia HH, Kuchta R, Wicht B (2009). “Update on the human broad tapeworm (genus diphyllobothrium), including clinical relevance”. Clin. Microbiol. Rev. 22 (1): 146–60, Table of Contents. doi:10.1128/CMR.00033-08. PMC 2620636. PMID 19136438.
- ↑ Kuchta R, Brabec J, Kubáčková P, Scholz T (2013). “Tapeworm Diphyllobothrium dendriticum (Cestoda)–neglected or emerging human parasite?”. PLoS Negl Trop Dis. 7 (12): e2535. doi:10.1371/journal.pntd.0002535. PMC 3873255. PMID 24386497.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
There is insufficient evidence to recommend routine screening for diphyllobothriasis.
Screening
There is insufficient evidence to recommend routine screening for diphyllobothriasis.
References
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Kalsang Dolma, M.B.B.S.[2], Furqan M M. M.B.B.S[3]
Overview
The symptoms of diphyllobothriasis usually develop after eating undercooked or raw infected fish meat and start with symptoms such as abdominal pain, diarrhea, nausea, vomiting, and tiredness. If left untreated, patients with diphyllobothriasis may progress to develop complications such as megaloblastic anemia, cholecystitis/cholangitis, and intestinal obstruction. Prognosis is generally good.
Natural History
- The symptoms of diphyllobothriasis usually develop after eating undercooked or raw infected fish meat and start with symptoms such as abdominal pain, diarrhea, nausea, vomiting, and tiredness.[1][2]
- Human Diphyllobothrium infection becomes infectious (begins to pass eggs in stools) approximately 15 to 45 days after ingestion of plerocercoid larvae.[1]
- Without treatment, the patient will develop symptoms of intestinal obstruction and infections of the biliary tract.[1][2][3]
Complications
The complications associated with diphyllobothriasis include:
- Megaloblastic anemia
- Intestinal obstruction
- Cholecystitis or cholangitis (as a result of migration of proglottids)
Prognosis
- Diphyllobothriasis can be removed with a single treatment dose. There are no lasting effects.
References
- ↑ 1.0 1.1 1.2 Baron, Samuel (1996). Medical microbiology. Galveston, Tex: University of Texas Medical Branch at Galveston. ISBN 0-9631172-1-1.
- ↑ 2.0 2.1 Scholz T, Garcia HH, Kuchta R, Wicht B (2009). “Update on the human broad tapeworm (genus diphyllobothrium), including clinical relevance”. Clin. Microbiol. Rev. 22 (1): 146–60, Table of Contents. doi:10.1128/CMR.00033-08. PMC 2620636. PMID 19136438.
- ↑ Feng XF (1989). “[Cervical anastomosis of the stomach transposed through the esophageal bed–report of 536 cases]”. Zhonghua Zhong Liu Za Zhi (in Chinese). 11 (5): 374–6. PMID 2620636.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | X Ray | CT scan | MRI | Ultrasound | Other imaging findings | Other diagnostic studies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH