
Human papillomavirus
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2],Aysha Aslam, M.B.B.S[3]
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2],Aysha Anwar, M.B.B.S[3]
Overview
Papillomaviruses are a diverse group of DNA-based viruses that infect the skin and mucous membranes of humans and a variety of animals. Over 100 different human papillomavirus (HPV) types have been identified. Some HPV types may cause condylomas (skin warts) while others may cause a subclinical infection resulting in precancerous lesions. All HPVs are transmitted by skin-to-skin contact. A group of about 30-40 HPVs is typically transmitted through sexual contact and infect the anogenital region. Some sexually transmitted HPVs — types 6, 11, may cause genital warts. However, other HPV types which may infect the genitals do not to cause any noticeable signs of infection.
Persistent infection with a subset of about 13 so-called “high-risk” sexually transmitted HPVs, including types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68 — different from the ones that cause warts — may lead to the development of cervical intraepithelial neoplasia (CIN), vulvar intraepithelial neoplasia (VIN), penile intraepithelial neoplasia (PIN), and/or anal intraepithelial neoplasia (AIN). These are precancerous lesions and can progress to invasive cancer. HPV infection is a necessary factor in the development of nearly all cases of cervical cancer.[1]
Historical Perspective
The fact that prostitutes have much higher rates of cervical cancer than nuns was a key early observation leading researchers to speculate about a causal link between sexually transmitted HPVs and cervical cancer.[2]
Classification
Human papilloma virus may have different presentations depending on the anatomical region of involvement and the virus type. Mainly it is classified to cutaneous, anogenital and other mucosal surfaces. Currently, 210 different types of HPV have been discovered and the number keeps increasing.[3][4] Clinical manifestations depend on which HPV type involve which anatomic area.[5][6]
Pathophysiology
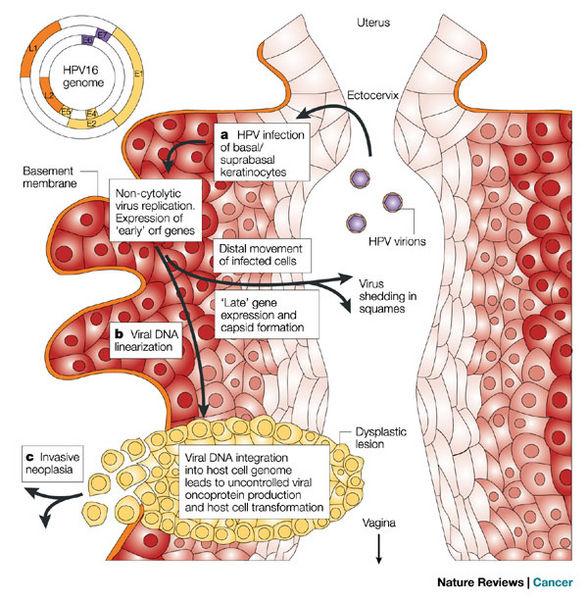
Human papilloma virus is usually transmitted via the sexual route to the human host.[7] HPV life cycle is linked to epithelial differentiation and maturation of host keratinocytes, with transcription of specific gene products at every level.[8][9] The pathogenesis of HPV infection causing cancer is mainly linked to high-risk types of HPV (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68). E6 and E7 protein products of HPV interact with two important cell cycle regulatory proteins, P53 and Rb proteins of the host cell, causing unchecked cellular replication accumulating mutations leading to cancer.[10][11][12]
Epidemiology and Demographics
Genital HPV infection is very common, with estimates suggesting that more than 50% of women will become infected with one or more of the sexually transmitted HPV types at some point during adulthood.[13]
Risk factors
Common risk factors for anogenital HPV infection are number of sex partners, having a new partner, duration of being sexually active, vaginal delivery and multiple deliveries. Close contact is the most potent factor for cutaneous infection.
Screening
High-risk HPV types are associated with 70% of cervical cancers in females having persistent infection.[14] Due to this strong association between HPV and cervical cancer, cervical cancer screening is recommended in all females from age 21. According to the US Preventive Services Task Force (USPSTF), specific screening guidelines for cervical cancer includes screening all females from age 21 to 65 for cervical cancer.[15][16]
Natural history, Complications, and Prognosis
Most infections with HPV are subclinical, asymptomatic and resolves without any complications in immunocompetent individuals. Time to develop symptoms and signs is not well defined but it may take 3 weeks to 3 months for genital warts, several months to years for cellular abnormalities (metaplasia and dysplasia) and years for development of cancers. 90% of infections resolve within 2 years due to host immune response.[17]Persistent HPV infection is associated with risk factors such as multiple sexual partners, alcohol consumption, immunosuppression, older age, and multiple types of HPV detected previously. Without treatment, persistent infection with low-risk types (low-grade intraepithelial lesions) may resolve spontaneously or persist and proliferate as warty lesions. However, high-risk HPV types (16,18,31,32) may lead to high-grade intraepithelial lesions which ultimately to carcinoma(cervical, anal, vaginal, vulvar, penile and oropharyngeal).[18][19][20][14]Prognosis of HPV infection depends primarily on the type of HPV causing infection.[21][22][23][24][25]
Diagnosis
History and physical examination
Detailed history about sexual activities and partners must be taken from every patient with anogenital involvement. Symptoms are mostly related to skin irritation and mucosal surface involvement. The hallmark of cutaneous involvement is pruritus however, the majority of the people acquiring HPV are asymptomatic. The clinical manifestation of HPV infection is wart that sometimes might be painful.[26]
Laboratory Findings
Certain types of sexually transmitted HPVs can cause cervical cancer. Persistent infection with one or more of about a dozen of these “high-risk” HPV types is an important factor in nearly all cases of cervical cancer. The development of HPV-induced cervical cancer is a slow process that generally takes many years. During this development phase, pre-cancerous cells can be detected by annual or semi-annual cervical cytology Papanicolaou screening, colloquially known as “Pap” smear testing. A cervical Pap smear with HPV DNA testing is used to detect cellular abnormalities and the presence of HPV. This allows targeted surgical removal of condylomatous and/or pre-cancerous lesions prior to the development of invasive cervical cancer. Although the widespread use of Pap testing has reduced the incidence and lethality of cervical cancer in developed countries, the disease still kills several hundred thousand women per year worldwide. A recently approved HPV vaccine, Gardasil, that blocks initial infection with several of the most common sexually transmitted HPV types may lead to further decreases in the incidence of HPV-induced cancer.[27]

Treatment
There is no definitive medical treatment of HPV infection. However, treatment is mainly aimed to treat warts or precancerous lesions. Two types of medical therapy which may be considered are cytodestructive therapy and immunotherapy. No treatment is considered superior to the other. However, selection of the treatment may depend on the wart size, number of warts, anatomic site of wart, wart morphology, patient preference, cost of treatment, convenience, adverse effects. Medical therapies for human papillomavirus infection include either imiquimod, sinecatechins, or podofilox.[28][29][30][31][32][33] Surgical removal of external genital warts may be an alternative regimen to pharmacologic therapy. Surgical therapies include either tangential scissor excision, tangential shave excision, curettage, laser, or electrosurgery.[34]
Prevention
Most people become infected with various cutaneous HPV types during childhood. Papillomaviruses have a sturdy outer protein shell or “capsid” that renders them capable of lingering in the environment for long periods of time. Avoiding contact with contaminated surfaces, such as the floors of communal showers or airport security lines, might reduce the risk of cutaneous HPV infection. Treating common warts soon after they first appear may also reduce the spread of the infection to additional sites.
Genital HPV infections may be distributed widely over genital skin and mucosal surfaces, and transmission can occur even when there are no overt symptoms. Several strategies should be employed to minimize the risk of developing diseases caused by genital HPVs:
References
- ↑ Walboomers JM, Jacobs MV, Manos MM; et al. (1999). “Human papillomavirus is a necessary cause of invasive cervical cancer worldwide”. J. Pathol. 189 (1): 12–9. doi:10.1002/(SICI)1096-9896(199909)189:1<12::AID-PATH431>3.0.CO;2-F. PMID 10451482.
- ↑ zur Hausen H, de Villiers EM (1994). “Human papillomaviruses”. Annu. Rev. Microbiol. 48: 427–47. PMID 7826013.
- ↑ “Reference clones at International HPV Reference Center”.
- ↑ Bernard HU, Burk RD, Chen Z, van Doorslaer K, zur Hausen H, de Villiers EM (2010). “Classification of papillomaviruses (PVs) based on 189 PV types and proposal of taxonomic amendments”. Virology. 401 (1): 70–9. doi:10.1016/j.virol.2010.02.002. PMC 3400342. PMID 20206957.
- ↑ Jenson AB, Kurman RJ, Lancaster WD (1985). “Detection of papillomavirus common antigens in lesions of skin and mucosa”. Clin. Dermatol. 3 (4): 56–63. PMID 2463866.
- ↑ Bzhalava D, Eklund C, Dillner J (2015). “International standardization and classification of human papillomavirus types”. Virology. 476: 341–4. doi:10.1016/j.virol.2014.12.028. PMID 25577151.
- ↑ Hernandez BY, Wilkens LR, Zhu X, Thompson P, McDuffie K, Shvetsov YB; et al. (2008). “Transmission of human papillomavirus in heterosexual couples”. Emerg Infect Dis. 14 (6): 888–94. doi:10.3201/eid1406.070616. PMC 2600292. PMID 18507898.
- ↑ Doorbar J (2005). “The papillomavirus life cycle”. J Clin Virol. 32 Suppl 1: S7–15. doi:10.1016/j.jcv.2004.12.006. PMID 15753007.
- ↑ Doorbar J, Quint W, Banks L, Bravo IG, Stoler M, Broker TR; et al. (2012). “The biology and life-cycle of human papillomaviruses”. Vaccine. 30 Suppl 5: F55–70. doi:10.1016/j.vaccine.2012.06.083. PMID 23199966.
- ↑ Moody CA, Laimins LA (2010). “Human papillomavirus oncoproteins: pathways to transformation”. Nat Rev Cancer. 10 (8): 550–60. doi:10.1038/nrc2886. PMID 20592731.
- ↑ Masuda H, Miller C, Koeffler HP, Battifora H, Cline MJ (1987). “Rearrangement of the p53 gene in human osteogenic sarcomas”. Proc Natl Acad Sci U S A. 84 (21): 7716–9. PMC 299371. PMID 2823272.
- ↑ Tommasino M, Adamczewski JP, Carlotti F, Barth CF, Manetti R, Contorni M; et al. (1993). “HPV16 E7 protein associates with the protein kinase p33CDK2 and cyclin A.” Oncogene. 8 (1): 195–202. PMID 8380917.
- ↑ Baseman JG, Koutsky LA (2005). “The epidemiology of human papillomavirus infections”. J. Clin. Virol. 32 Suppl 1: S16–24. doi:10.1016/j.jcv.2004.12.008. PMID 15753008. *Note: The authors state on page S17 “Overall, these DNA-based studies, combined with measurements of type-specific antibodies against HPV capsid antigens, have shown that most (>50%) sexually active women have been infected by one or more genital HPV types at some point in time.”
- ↑ 14.0 14.1 http://www.cdc.gov/vaccines/pubs/pinkbook/hpv.html#epi Accessed on October 13, 2016
- ↑ Moyer VA, U.S. Preventive Services Task Force (2012). “Screening for cervical cancer: U.S. Preventive Services Task Force recommendation statement”. Ann Intern Med. 156 (12): 880–91, W312. doi:10.7326/0003-4819-156-12-201206190-00424. PMID 22711081.
- ↑ McGraw SL, Ferrante JM (2014). “Update on prevention and screening of cervical cancer”. World J Clin Oncol. 5 (4): 744–52. doi:10.5306/wjco.v5.i4.744. PMC 4129537. PMID 25302174.
- ↑ Ault KA (2006). “Epidemiology and natural history of human papillomavirus infections in the female genital tract”. Infect Dis Obstet Gynecol. 2006 Suppl: 40470. doi:10.1155/IDOG/2006/40470. PMC 1581465. PMID 16967912.
- ↑ Castle PE, Schiffman M, Herrero R, Hildesheim A, Rodriguez AC, Bratti MC; et al. (2005). “A prospective study of age trends in cervical human papillomavirus acquisition and persistence in Guanacaste, Costa Rica”. J Infect Dis. 191 (11): 1808–16. doi:10.1086/428779. PMID 15871112.
- ↑ Woodman CB, Collins S, Winter H, Bailey A, Ellis J, Prior P; et al. (2001). “Natural history of cervical human papillomavirus infection in young women: a longitudinal cohort study”. Lancet. 357 (9271): 1831–6. doi:10.1016/S0140-6736(00)04956-4. PMID 11410191.
- ↑ Ho GY, Bierman R, Beardsley L, Chang CJ, Burk RD (1998). “Natural history of cervicovaginal papillomavirus infection in young women”. N Engl J Med. 338 (7): 423–8. doi:10.1056/NEJM199802123380703. PMID 9459645.
- ↑ Yang SH, Kong SK, Lee SH, Lim SY, Park CY (2014). “Human papillomavirus 18 as a poor prognostic factor in stage I-IIA cervical cancer following primary surgical treatment”. Obstet Gynecol Sci. 57 (6): 492–500. doi:10.5468/ogs.2014.57.6.492. PMC 4245343. PMID 25469338.
- ↑ No JH, Sung MW, Hah JH, Choi SH, Lee MC, Kim HS; et al. (2015). “Prevalence and prognostic value of human papillomavirus genotypes in tonsillar squamous cell carcinoma: a Korean multicenter study”. Cancer. 121 (4): 535–44. doi:10.1002/cncr.29086. PMID 25283642.
- ↑ Lin BM, Wang H, D’Souza G, Zhang Z, Fakhry C, Joseph AW; et al. (2013). “Long-term prognosis and risk factors among patients with HPV-associated oropharyngeal squamous cell carcinoma”. Cancer. 119 (19): 3462–71. doi:10.1002/cncr.28250. PMC 3788050. PMID 23861037.
- ↑ Beutner KR, Wiley DJ, Douglas JM, Tyring SK, Fife K, Trofatter K; et al. (1999). “Genital warts and their treatment”. Clin Infect Dis. 28 Suppl 1: S37–56. doi:10.1086/514722. PMID 10028109.
- ↑ Ferenczy A, Coutlée F, Franco E, Hankins C (2003). “Human papillomavirus and HIV coinfection and the risk of neoplasias of the lower genital tract: a review of recent developments”. CMAJ. 169 (5): 431–4. PMC 183297. PMID 12952805.
- ↑ Jablonska S, Orth G, Obalek S, Croissant O (1985). “Cutaneous warts. Clinical, histologic, and virologic correlations”. Clin. Dermatol. 3 (4): 71–82. PMID 2850861.
- ↑ Lowy DR, Schiller JT (2006). “Prophylactic human papillomavirus vaccines”. J. Clin. Invest. 116 (5): 1167–73. doi:10.1172/JCI28607. PMID 16670757.
- ↑ Workowski, Kimberly A.; Bolan, Gail A. (2015-06-05). “Sexually transmitted diseases treatment guidelines, 2015”. MMWR. Recommendations and reports: Morbidity and mortality weekly report. Recommendations and reports / Centers for Disease Control. 64 (RR-03): 1–137. ISSN 1545-8601. PMID 26042815.
- ↑ Gotovtseva EP, Kapadia AS, Smolensky MH, Lairson DR (2008). “Optimal frequency of imiquimod (aldara) 5% cream for the treatment of external genital warts in immunocompetent adults: a meta-analysis”. Sex Transm Dis. 35 (4): 346–51. doi:10.1097/OLQ.0b013e31815ea8d1. PMID 18360317.
- ↑ Garland SM, Waddell R, Mindel A, Denham IM, McCloskey JC (2006). “An open-label phase II pilot study investigating the optimal duration of imiquimod 5% cream for the treatment of external genital warts in women”. Int J STD AIDS. 17 (7): 448–52. doi:10.1258/095646206777689161. PMID 16820073.
- ↑ Edwards L, Ferenczy A, Eron L, Baker D, Owens ML, Fox TL; et al. (1998). “Self-administered topical 5% imiquimod cream for external anogenital warts. HPV Study Group. Human PapillomaVirus”. Arch Dermatol. 134 (1): 25–30. PMID 9449906.
- ↑ “Veregen: a botanical for treatment of genital warts”. Med Lett Drugs Ther. 50 (1280): 15–6. 2008. PMID 18292715.
- ↑ Eron LJ, Judson F, Tucker S, Prawer S, Mills J, Murphy K; et al. (1986). “Interferon therapy for condylomata acuminata”. N Engl J Med. 315 (17): 1059–64. doi:10.1056/NEJM198610233151704. PMID 3531860.
- ↑ Workowski, Kimberly A.; Bolan, Gail A. (2015-06-05). “Sexually transmitted diseases treatment guidelines, 2015”. MMWR. Recommendations and reports: Morbidity and mortality weekly report. Recommendations and reports / Centers for Disease Control. 64 (RR-03): 1–137. ISSN 1545-8601. PMID 26042815.
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Warts as a cutaneous manifestation of HPV infection were first described by Hippocrates. Dr. Harald Zur Hausen (father of HPV virology) in 1975 described the relationship between HPV and cervical cancer.
Historical Perspective
- Genital warts were first described by Hippocrates (460–377 B.C.). Since those days, the term condyloma (a word of Greek origin) has been used for genital warts meaning “a round swelling around the anus”.[1]
- In 1891 Infectious nature of common warts was noticed by Payne and Jadassohn.
- In 1943, Parson and Kidd published their milestone study where they showed that oral papillomatosis of rabbits is a viral disease and the oral papillomavirus was distinct from the skin papillomavirus
- In 1956, The concept of koilocytosis in PAP smears and cervical biopsies described by Koss & Durfee.
- EM demonstration of HPV particles in genital warts was shown by Dunn & Ogilvie in 1968 and Almeida et al in 1969.
- In 1975, Zur Hausen German physician presented the hypothesis on HPV as a potential cause of cervical cancer.[2]
- Nobel prize in medicine went to Dr. Harald Zur Hausen in 2008 regarding his discoveries in HPV relation to cervical cancer.
-
 Dr. Herald zur Hausen
Dr. Herald zur Hausen

References
- ↑ Gasparini R, Panatto D (2009). “Cervical cancer: from Hippocrates through Rigoni-Stern to Zur Hausen”. Vaccine. 27 Suppl 1: A4–5. doi:10.1016/j.vaccine.2008.11.069. PMID 19480961.
- ↑ zur Hausen H (2009). “Papillomaviruses in the causation of human cancers – a brief historical account”. Virology. 384 (2): 260–5. doi:10.1016/j.virol.2008.11.046. PMID 19135222.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Human papillomavirus may have different presentations depending on the anatomical region of involvement and the virus type. Mainly it is classified to cutaneous, anogenital and other mucosal surfaces.
Classification
Based on tissue involvement, human papillomavirus (HPV) is classified in to 3 main groups:
- Cutaneous
- Anogenital
- Other Mucosal surfaces
Currently, 210 different types of HPV have been discovered and the number keeps increasing.[1][2] Clinical manifestations depend on which HPV type involve which anatomic area.[3][4]
Cutaneous lesions
| Clinical presentation | Frequently found types | Less Frequently found types |
|---|---|---|
| Common wart | 1, 2, 4 | 4, 26, 27, 29, 41, 57, 63, 65, 77, 117, 125, 128, 129, 130, 131, 132, 133, 148, 149 |
| Plantar wart | 1, 2 | 26, 27, 29, 41, 57, 63, 65, 77, 117, 125, 128, 129, 130, 131, 132, 133, 148, 149 |
| Flat and intermediate warts | 3, 10 | 26, 27, 28, 38, 41, 49, 75, 76, 126 |
| Common warts of meat, poultry, and fish handlers | 2, 7 | 1, 3, 4, 10, 28 |
| Epidermodysplasia verruciformis | 3, 5, 8 | 9 , 12 , 14 , 15 , 17 , 19–25 , 36–38 , 47 , 49 , 50 |
Anogenital lesions
| Clinical presentation | Frequently found types | Less Frequently found types |
|---|---|---|
| Low grade intraepithelial neoplasia(squamous cell carcinoma) | 6, 11 | 16, 18, 31, 33, 35, 42, 43, 44, 45, 51, 52, 54, 61, 70, 72, 74 |
| High grade intraepithelial neoplasia(squamous cell carcinoma) | 16, 18 | 6, 11, 31, 33, 34, 35, 39, 42, 44, 45, 51, 52, 56, 58, 66, 67 |
| Condylomata acuminata | 6, 11 | 40, 42–44, 54, 61, 70, 72, 81 |
| Genital bowen’s disease | 16 |
Other mucosal lesions
| Clinical presentation | Frequently found types | Less Frequently found types |
|---|---|---|
| Buschke–Löwenstein tumor | 6, 11 | |
| Recurrent respiratory papillomatosis | 6, 11 | 16, 18, 31, 33, 35, 39 |
| Conjunctival papillomas and carcinomas | 6, 11, 16 |
References
- ↑ “Reference clones at International HPV Reference Center”.
- ↑ Bernard HU, Burk RD, Chen Z, van Doorslaer K, zur Hausen H, de Villiers EM (2010). “Classification of papillomaviruses (PVs) based on 189 PV types and proposal of taxonomic amendments”. Virology. 401 (1): 70–9. doi:10.1016/j.virol.2010.02.002. PMC 3400342. PMID 20206957.
- ↑ Jenson AB, Kurman RJ, Lancaster WD (1985). “Detection of papillomavirus common antigens in lesions of skin and mucosa”. Clin. Dermatol. 3 (4): 56–63. PMID 2463866.
- ↑ Bzhalava D, Eklund C, Dillner J (2015). “International standardization and classification of human papillomavirus types”. Virology. 476: 341–4. doi:10.1016/j.virol.2014.12.028. PMID 25577151.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Aysha Anwar, M.B.B.S[2],Seyedmahdi Pahlavani, M.D. [3]
Overview
Human papilloma virus is usually transmitted via the sexual route to the human host.[1] HPV life cycle is linked to epithelial differentiation and maturation of host keratinocytes, with transcription of specific gene products at every level.[2][3] The pathogenesis of HPV infection causing cancer is mainly linked to high risk types of HPV (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68). E6 and E7 protein products of HPV interact with two important cell cycle regulatory protiens, P53 and Rb proteins of host cell, causing unchecked cellular replication accumulating mutations leading to cancer.[4][5][6]
Pathophysiology
Transmission
- Human papilloma virus is usually transmitted via the sexual route to the human host.[1]
- Different types of HPV has a predilection for different types of epithelial tissue.[7]
HPV life cycle
- HPV life cycle is linked to epithelial differentiation and maturation of host keratinocytes, with transcription of specific gene products at every level.[2][3][8]
- HPV primarily infects basal cell layer of stratified squamous keratinised epithelium.[9]
- Following transmission, the HPV uses the microabrasions to enter the basal stem cells via tissue specific heparan sulfate proteoglycans through clathrin-mediated endocytosis and/or caveolin-mediated endocytosis depending on the type of HPV.[10]
- It than undergoes viral uncoating and viral DNA genome is than transported to nucleus maintaining a low copy number 10-200 viral genomes per cell (episome form).[11]
- A sophisticated transcriptional cascade then occurs as the host keratinocyte begins to divide and become increasingly differentiated in the upper layers of the epithelium.
- HPV uses host DNA replicative machinery to multiply as it lacks DNA polymerase activity.
- Specific viral genes are transcribed at every level of keratinocyte differention.
- Early proteins: E1, E2, E3, E4, E5, E6 and E7 proteins are synthesized primarily in middle layers, for reactivation of replication process in the differentiated cells.
- Late proteins: L1, L2 proteins are transcribed in the most superficial layers for virion assesmbly, release and reinfection, as they code for capsid proteins.[12]

Pathogenesis of HPV induced cancers
The pathogenesis of HPV infection causing cancer is mainly linked to high risk types of HPV (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68). Following HPV proteins play a significant role in the development of cancers associated with HPV.[13]
E6 and E7 proteins
E6 and E7 protein products of HPV interact with two important cell cycle regulatory protiens, P53 and Rb proteins of host cell, causing unchecked cellular replication accumulating mutations leading to cancer.[4]
- Inhibition of P53
- P53 protein is a cellular check point at G0/G1 to S phase of cell cycle and is also responsible for cell apoptosis for unrepaired DNA mutations. E6 protein binds P53 which results in degradation of P53, leaving cell without any check for mutations and unregulated cell.[5][14]
- growth.[15][16][17][18][19]
- Inhibition of Rb protein
- Rb protein is negative regulator of cell growth. It binds E2F transcription factor which controls DNA replication and cyclin protein induced entering of cell into S phase of cell cycle. E7 protein binds Rb/E2F, releasing E2F from the inhibitory effect of Rb causing increased cyclin induced entry of cell into S phase of cell cycle, resulting in increased replication rate of cells accumulating mutations.[19][20][6][21]
HPV-Induced Diseases
| Disease | HPV type |
|---|---|
| Common warts | 2, 7 |
| Plantar warts | 1, 2, 4 |
| Flat cutaneous warts | 3, 10 |
| Anogenital warts | 6, 11, 42, 43, 44, 55 and others |
| Genital malignancies | 16, 18, 31, 33, 35, 39, 45, 51 |
| Epidermodysplasia verruciformis | more than 15 types |
| Focal epithelial hyperplasia (oral) | 13, 32 |
| Oral papillomas | 6, 7, 11, 16, 32 |
References
- ↑ 1.0 1.1 Hernandez BY, Wilkens LR, Zhu X, Thompson P, McDuffie K, Shvetsov YB; et al. (2008). “Transmission of human papillomavirus in heterosexual couples”. Emerg Infect Dis. 14 (6): 888–94. doi:10.3201/eid1406.070616. PMC 2600292. PMID 18507898.
- ↑ 2.0 2.1 Doorbar J (2005). “The papillomavirus life cycle”. J Clin Virol. 32 Suppl 1: S7–15. doi:10.1016/j.jcv.2004.12.006. PMID 15753007.
- ↑ 3.0 3.1 Doorbar J, Quint W, Banks L, Bravo IG, Stoler M, Broker TR; et al. (2012). “The biology and life-cycle of human papillomaviruses”. Vaccine. 30 Suppl 5: F55–70. doi:10.1016/j.vaccine.2012.06.083. PMID 23199966.
- ↑ 4.0 4.1 Moody CA, Laimins LA (2010). “Human papillomavirus oncoproteins: pathways to transformation”. Nat Rev Cancer. 10 (8): 550–60. doi:10.1038/nrc2886. PMID 20592731.
- ↑ 5.0 5.1 Masuda H, Miller C, Koeffler HP, Battifora H, Cline MJ (1987). “Rearrangement of the p53 gene in human osteogenic sarcomas”. Proc Natl Acad Sci U S A. 84 (21): 7716–9. PMC 299371. PMID 2823272.
- ↑ 6.0 6.1 Tommasino M, Adamczewski JP, Carlotti F, Barth CF, Manetti R, Contorni M; et al. (1993). “HPV16 E7 protein associates with the protein kinase p33CDK2 and cyclin A.” Oncogene. 8 (1): 195–202. PMID 8380917.
- ↑ Rintala MA, Grénman SE, Puranen MH, Isolauri E, Ekblad U, Kero PO; et al. (2005). “Transmission of high-risk human papillomavirus (HPV) between parents and infant: a prospective study of HPV in families in Finland”. J Clin Microbiol. 43 (1): 376–81. doi:10.1128/JCM.43.1.376-381.2005. PMC 540188. PMID 15634997.
- ↑ Doorbar J (2007). “Papillomavirus life cycle organization and biomarker selection”. Dis Markers. 23 (4): 297–313. PMC 3851388. PMID 17627064.
- ↑ Kines RC, Thompson CD, Lowy DR, Schiller JT, Day PM (2009). “The initial steps leading to papillomavirus infection occur on the basement membrane prior to cell surface binding”. Proc Natl Acad Sci U S A. 106 (48): 20458–63. doi:10.1073/pnas.0908502106. PMC 2787115. PMID 19920181.
- ↑ Johnson KM, Kines RC, Roberts JN, Lowy DR, Schiller JT, Day PM (2009). “Role of heparan sulfate in attachment to and infection of the murine female genital tract by human papillomavirus”. J Virol. 83 (5): 2067–74. doi:10.1128/JVI.02190-08. PMC 2643729. PMID 19073722.
- ↑ Bedell MA, Hudson JB, Golub TR, Turyk ME, Hosken M, Wilbanks GD; et al. (1991). “Amplification of human papillomavirus genomes in vitro is dependent on epithelial differentiation”. J Virol. 65 (5): 2254–60. PMC 240574. PMID 1850010.
- ↑ Yang R, Yutzy WH, Viscidi RP, Roden RB (2003). “Interaction of L2 with beta-actin directs intracellular transport of papillomavirus and infection”. J Biol Chem. 278 (14): 12546–53. doi:10.1074/jbc.M208691200. PMID 12560332.
- ↑ de Sanjose S, Quint WG, Alemany L, Geraets DT, Klaustermeier JE, Lloveras B; et al. (2010). “Human papillomavirus genotype attribution in invasive cervical cancer: a retrospective cross-sectional worldwide study”. Lancet Oncol. 11 (11): 1048–56. doi:10.1016/S1470-2045(10)70230-8. PMID 20952254.
- ↑ Hinds P, Finlay C, Levine AJ (1989). “Mutation is required to activate the p53 gene for cooperation with the ras oncogene and transformation”. J Virol. 63 (2): 739–46. PMC 247745. PMID 2642977.
- ↑ Scheffner M, Huibregtse JM, Vierstra RD, Howley PM (1993). “The HPV-16 E6 and E6-AP complex functions as a ubiquitin-protein ligase in the ubiquitination of p53”. Cell. 75 (3): 495–505. PMID 8221889.
- ↑ Havre PA, Yuan J, Hedrick L, Cho KR, Glazer PM (1995). “p53 inactivation by HPV16 E6 results in increased mutagenesis in human cells”. Cancer Res. 55 (19): 4420–4. PMID 7671255.
- ↑ Werness BA, Levine AJ, Howley PM (1990). “Association of human papillomavirus types 16 and 18 E6 proteins with p53”. Science. 248 (4951): 76–9. PMID 2157286.
- ↑ Magal SS, Jackman A, Pei XF, Schlegel R, Sherman L (1998). “Induction of apoptosis in human keratinocytes containing mutated p53 alleles and its inhibition by both the E6 and E7 oncoproteins”. Int J Cancer. 75 (1): 96–104. PMID 9426696.
- ↑ 19.0 19.1 Demers GW, Foster SA, Halbert CL, Galloway DA (1994). “Growth arrest by induction of p53 in DNA damaged keratinocytes is bypassed by human papillomavirus 16 E7”. Proc Natl Acad Sci U S A. 91 (10): 4382–6. PMC 43789. PMID 8183918.
- ↑ Pagano M, Dürst M, Joswig S, Draetta G, Jansen-Dürr P (1992). “Binding of the human E2F transcription factor to the retinoblastoma protein but not to cyclin A is abolished in HPV-16-immortalized cells”. Oncogene. 7 (9): 1681–6. PMID 1323816.
- ↑ Brehm A, Nielsen SJ, Miska EA, McCance DJ, Reid JL, Bannister AJ; et al. (1999). “The E7 oncoprotein associates with Mi2 and histone deacetylase activity to promote cell growth”. EMBO J. 18 (9): 2449–58. doi:10.1093/emboj/18.9.2449. PMC 1171327. PMID 10228159.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
HPV is a double-stranded DNA, non-enveloped capsid virus. Currently, 210 subtypes of this virus have been recognized. It may cause cutaneous or mucosal lesions. Some types have strong relation to cervical cancer and some types are found in benign skin lesion.
Causes
- Human papillomavirus (HPV) is a DNA virus belonging to its own family, papillomaviridae. There are 210 types of HPV and as reflected in its name, species specific for humans. It is a double-stranded DNA, non-enveloped capsid virus that has 7900 base pairs which have 90% homology between the types.
- The base pairs are arranged in a circle which includes the codes for two key proteins known as L1 and L2.
- These two proteins act as the “immunogene” which is required for self-assembly and the infectivity protein, respectively.[1][2]
-
 HPV invasion cycle
HPV invasion cycle

- Some types of HPV cause local self-limited infections while others can be differentiated by their predilection towards the development of human cancers. For example, HPV 16 and 18 are most frequently associated with cervical cancer.
- HPV 16 accounts for up to 50% of HPV causing cervical and anal cancers worldwide.[3] In addition to those viruses associated with penile cancer, 70% are of the HPV 16 phenotype and occurs 6 times higher in males with histories of venereal warts or condylomata acuminata.
References
- ↑ Roden RB, Yutzy WH, Fallon R, Inglis S, Lowy DR, Schiller JT (2000). “Minor capsid protein of human genital papillomaviruses contains subdominant, cross-neutralizing epitopes”. Virology. 270 (2): 254–7. doi:10.1006/viro.2000.0272. PMID 10792983.
- ↑ Doorbar J (2005). “The papillomavirus life cycle”. J. Clin. Virol. 32 Suppl 1: S7–15. doi:10.1016/j.jcv.2004.12.006. PMID 15753007.
- ↑ Zaki SR, Judd R, Coffield LM, Greer P, Rolston F, Evatt BL (1992). “Human papillomavirus infection and anal carcinoma. Retrospective analysis by in situ hybridization and the polymerase chain reaction”. Am. J. Pathol. 140 (6): 1345–55. PMC 1886536. PMID 1318640.
Differentiating Human papillomavirus from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Aysha Anwar, M.B.B.S[2]
Overview
HPV infection must be differentiated from other diseases that causes warty lesions, pruritis, postcoital spotting or vaginal discharge, vaginal bleeding, painful sexual intercourse, respiratory distress
Differential diagnosis
HPV infection must be differentiated from other diseases that causes warty lesions, pruritis, postcoital spotting or vaginal discharge, vaginal bleeding, painful sexual intercourse, respiratory distress and stridor in infants:[1][2][3]
- Condylomata lata[1]
- Molluscum contagiosum
- Seborrheic keratosis
- Lichen planus
- Fibroepithelial polyp, adenoma
- Melanocytic nevus
- Neoplastic lesions
- Pink pearly penile papules
- Vestibular papillae (micropapillomatosis labialis)
- Skin tags (acrochordons)
- Squamous cell carcinoma in situ
- Bowenoid papulosis
- Erythroplasia of Queyrat
- Bowen’s disease of the genitalia
- Benign Cervical Lesions
- Benign Vulvar Lesions
- Head and Neck Cutaneous Squamous Cell Carcinoma
References
- ↑ 1.0 1.1 Deshpande DJ, Nayak CS, Mishra SN, Dhurat RS (2009). “Verrucous condyloma lata mimicking condyloma acuminata: An unusual presentation”. Indian J Sex Transm Dis. 30 (2): 100–2. doi:10.4103/0253-7184.62766. PMC 3168050. PMID 21938129.
- ↑ Tayal S, Shaban F, Dasgupta K, Tabaqchali MA (2015). “A case of syphilitic anal condylomata lata mimicking malignancy”. Int J Surg Case Rep. 17: 69–71. doi:10.1016/j.ijscr.2015.10.035. PMC 4701813. PMID 26555060.
- ↑ Wiley DJ, Douglas J, Beutner K, Cox T, Fife K, Moscicki AB; et al. (2002). “External genital warts: diagnosis, treatment, and prevention”. Clin Infect Dis. 35 (Suppl 2): S210–24. doi:10.1086/342109. PMID 12353208.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Aysha Anwar, M.B.B.S[2]
Overview
Genital HPV infection is very common, with estimates suggesting that more than 50% of women will become infected with one or more of the sexually transmitted HPV types at some point during adulthood.[1]
Epidemiology
Cutaneous warts
Genital warts
- Anogenital HPV is the most common sexually transmitted infection in the USA [2]
- In USA, the prevalence of anogenital HPV infection is estimated to be 79 million with incidence of 14 million new cases each year [2]
- Worldwide, 90% of genital warts is caused by the HPV 6 and 11[3]
- Prevalence of genital warts is 1% in USA as compared to 10% in Scandinavian countries
- In USA, the incidence of genital warts has slightly increased in the year 2013

Genital Warts — Initial Visits to Physicians’ Offices, United States, 1966–2013
†Data from CDC
HPV associated cancers
- In USA, the incidence of HPV associated cancer is 38,793 each year (data 2008-2012)[4]
- Cervical cancer
- Worldwide, the incidence of invasive cervical cancer is 500,000 cases each year.
- Worlwide, 70% of cervical cancer is caused by the HPV 16 and 18[3]
- In USA, more than 90% of cervical cancer is caused by HPV.[4]
- Oropharyngeal cancer
- Incidence of oropharyngeal cancer associated with HPV is showing an increasing trend in USA[5][6]
- 70% of oropharyngeal cancers are associated with HPV[4]
- Anal cancer
- Recurrent respiratory papillomatosis
- Rare with rates of about 2 cases per 100,000 children in the United States[11]
- Common in children born to females having active genital warts at the time of vaginal delivery
Demographics
Following demographic factors may affect the incidence and prevalence of HPV infection:
Age
Cutaneous warts
- More common in children aged 12-16 yrs of age[12] [13]
- 10% of children and 3.5% of adults are affected, worldwide
Genital warts
- Incidence of genital HPV infection increases at the age when individuals begin to engage in sexual activity.[14][15]
- Highest incidence of genital warts is seen in females aged 20-24 yrs and males aged 25-29 yrs of age[16] (CDC)
- Prevalence of cervical HPV in females may decline after age 30[17]
HPV associated cancer
Recurrent respiratory papillomatosis

Human Papillomavirus — Cervicovaginal Prevalence of Types 6, 11, 16 and 18 Among Women Aged 14–59 Years by Age Group and Time Period, National Health and Nutrition Examination Survey, 2003–2006 and 2007–2010
†Data from CDC
Gender
Genital warts
Prevalence per 1000 person-years Among participants in private health plans aged 10–39 years by sex, age group, and year, 2003–2010 is shown in the graph below:

†Data from CDC
HPV associated cancers
- Out of total 38,793 HPV-associated cancers that occur in the United States each year, 23,000 occur among women, and about 15,793 among men[4]
- Three fold increased prevalence of HPV associated anal and oropharyngeal cancer in men as compared to women.
- Increased incidence of oropharngeal and anal cancer among men who have sex with men (MSM)[23][24][25][26][27]
- Worldwide, the point prevalence of HPV in females is 10%, with highest prevalence among African females[28]
Race
- There may be increased incidence of high risk HPV infections in African American females as compared to Caucasian[15][29]
References
- ↑ Baseman JG, Koutsky LA (2005). “The epidemiology of human papillomavirus infections”. J. Clin. Virol. 32 Suppl 1: S16–24. doi:10.1016/j.jcv.2004.12.008. PMID 15753008. *Note: The authors state on page S17 “Overall, these DNA-based studies, combined with measurements of type-specific antibodies against HPV capsid antigens, have shown that most (>50%) sexually active women have been infected by one or more genital HPV types at some point in time.”
- ↑ 2.0 2.1 http://www.cdc.gov/vaccines/pubs/pinkbook/hpv.html#epi
- ↑ 3.0 3.1 http://www.cdc.gov/std/stats14/other.htm#hpv Accessed on October 12, 2016
- ↑ 4.0 4.1 4.2 4.3 https://www.cdc.gov/cancer/hpv/statistics/ Accessed on October 12, 2016
- ↑ 5.0 5.1 Jemal A, Simard EP, Dorell C, Noone AM, Markowitz LE, Kohler B; et al. (2013). “Annual Report to the Nation on the Status of Cancer, 1975-2009, featuring the burden and trends in human papillomavirus(HPV)-associated cancers and HPV vaccination coverage levels”. J Natl Cancer Inst. 105 (3): 175–201. doi:10.1093/jnci/djs491. PMC 3565628. PMID 23297039.
- ↑ Chaturvedi AK, Engels EA, Pfeiffer RM, Hernandez BY, Xiao W, Kim E; et al. (2011). “Human papillomavirus and rising oropharyngeal cancer incidence in the United States”. J Clin Oncol. 29 (32): 4294–301. doi:10.1200/JCO.2011.36.4596. PMC 3221528. PMID 21969503.
- ↑ Robinson D, Coupland V, Møller H (2009). “An analysis of temporal and generational trends in the incidence of anal and other HPV-related cancers in Southeast England”. Br J Cancer. 100 (3): 527–31. doi:10.1038/sj.bjc.6604871. PMC 2658550. PMID 19156144.
- ↑ Cook MB, Dawsey SM, Freedman ND, Inskip PD, Wichner SM, Quraishi SM; et al. (2009). “Sex disparities in cancer incidence by period and age”. Cancer Epidemiol Biomarkers Prev. 18 (4): 1174–82. doi:10.1158/1055-9965.EPI-08-1118. PMC 2793271. PMID 19293308.
- ↑ Shiels MS, Pfeiffer RM, Chaturvedi AK, Kreimer AR, Engels EA (2012). “Impact of the HIV epidemic on the incidence rates of anal cancer in the United States”. J Natl Cancer Inst. 104 (20): 1591–8. doi:10.1093/jnci/djs371. PMC 3611819. PMID 23042932.
- ↑ Daling JR, Weiss NS, Klopfenstein LL, Cochran LE, Chow WH, Daifuku R (1982). “Correlates of homosexual behavior and the incidence of anal cancer”. JAMA. 247 (14): 1988–90. PMID 7062503.
- ↑ Sinal SH, Woods CR (2005). “Human papillomavirus infections of the genital and respiratory tracts in young children”. Seminars in Pediatric Infectious Diseases. 16 (4): 306–16. doi:10.1053/j.spid.2005.06.010. PMID 16210110. Retrieved 2012-12-10. Unknown parameter
|month=ignored (help) - ↑ Allen AL, Siegfried EC (2000). “What’s new in human papillomavirus infection”. Curr Opin Pediatr. 12 (4): 365–9. PMID 10943818.
- ↑ Steele K, Irwin WG, Merrett JD (1989). “Warts in general practice”. Ir Med J. 82 (3): 122–4. PMID 2599836.
- ↑ Schiffman M, Castle PE (2005). “The promise of global cervical-cancer prevention”. N. Engl. J. Med. 353 (20): 2101–4. doi:10.1056/NEJMp058171. PMID 16291978.
- ↑ 15.0 15.1 Ho GY, Bierman R, Beardsley L, Chang CJ, Burk RD (1998). “Natural history of cervicovaginal papillomavirus infection in young women”. N Engl J Med. 338 (7): 423–8. doi:10.1056/NEJM199802123380703. PMID 9459645.
- ↑ Dunne EF, Unger ER, Sternberg M, McQuillan G, Swan DC, Patel SS; et al. (2007). “Prevalence of HPV infection among females in the United States”. JAMA. 297 (8): 813–9. doi:10.1001/jama.297.8.813. PMID 17327523.
- ↑ Wright TC, Schiffman M (2003). “Adding a test for human papillomavirus DNA to cervical-cancer screening”. N Engl J Med. 348 (6): 489–90. doi:10.1056/NEJMp020178. PMID 12571255.
- ↑ Gillison ML, D’Souza G, Westra W, Sugar E, Xiao W, Begum S; et al. (2008). “Distinct risk factor profiles for human papillomavirus type 16-positive and human papillomavirus type 16-negative head and neck cancers”. J Natl Cancer Inst. 100 (6): 407–20. doi:10.1093/jnci/djn025. PMID 18334711.
- ↑ Hoevenaars BM, van der Avoort IA, de Wilde PC, Massuger LF, Melchers WJ, de Hullu JA; et al. (2008). “A panel of p16(INK4A), MIB1 and p53 proteins can distinguish between the 2 pathways leading to vulvar squamous cell carcinoma”. Int J Cancer. 123 (12): 2767–73. doi:10.1002/ijc.23857. PMID 18798277.
- ↑ Chaux A, Cubilla AL (2012). “The role of human papillomavirus infection in the pathogenesis of penile squamous cell carcinomas”. Semin Diagn Pathol. 29 (2): 67–71. PMID 22641955.
- ↑ Derkay CS, Wiatrak B (2008). “Recurrent respiratory papillomatosis: a review”. Laryngoscope. 118 (7): 1236–47. doi:10.1097/MLG.0b013e31816a7135. PMID 18496162.
- ↑ Yuan H, Myers S, Wang J, Zhou D, Woo JA, Kallakury B; et al. (2012). “Use of reprogrammed cells to identify therapy for respiratory papillomatosis”. N Engl J Med. 367 (13): 1220–7. doi:10.1056/NEJMoa1203055. PMC 4030597. PMID 23013073.
- ↑ “STD Facts – HPV and Men”. Retrieved 2007-08-17.
- ↑ Gillison ML, Broutian T, Pickard RK, Tong ZY, Xiao W, Kahle L; et al. (2012). “Prevalence of oral HPV infection in the United States, 2009-2010”. JAMA. 307 (7): 693–703. doi:10.1001/jama.2012.101. PMID 22282321.
- ↑ Pickard RK, Xiao W, Broutian TR, He X, Gillison ML (2012). “The prevalence and incidence of oral human papillomavirus infection among young men and women, aged 18-30 years”. Sex Transm Dis. 39 (7): 559–66. doi:10.1097/OLQ.0b013e31824f1c65. PMID 22706220.
- ↑ Chaturvedi AK, Graubard BI, Pickard RK, Xiao W, Gillison ML (2014). “High-risk oral human papillomavirus load in the US population, National Health and Nutrition Examination Survey 2009-2010”. J Infect Dis. 210 (3): 441–7. doi:10.1093/infdis/jiu116. PMC 4110460. PMID 24625808.
- ↑ Fakhry C, Gillison ML, D’Souza G (2014). “Tobacco use and oral HPV-16 infection”. JAMA. 312 (14): 1465–7. doi:10.1001/jama.2014.13183. PMC 4266546. PMID 25291584.
- ↑ de Sanjosé S, Diaz M, Castellsagué X, Clifford G, Bruni L, Muñoz N; et al. (2007). “Worldwide prevalence and genotype distribution of cervical human papillomavirus DNA in women with normal cytology: a meta-analysis”. Lancet Infect Dis. 7 (7): 453–9. doi:10.1016/S1473-3099(07)70158-5. PMID 17597569.
- ↑ Banister CE, Messersmith AR, Cai B, Spiryda LB, Glover SH, Pirisi L; et al. (2015). “Disparity in the persistence of high-risk human papillomavirus genotypes between African American and European American women of college age”. J Infect Dis. 211 (1): 100–8. doi:10.1093/infdis/jiu394. PMC 4326315. PMID 25028692.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Common risk factors for anogenital HPV infection are number of sex partners, having a new partner, duration of being sexually active, vaginal delivery and multiple deliveries. Close contact is the most potent factor for cutaneous infection.
Risk Factors
The most potent risk factor in acquiring HPV skin infection is close contact,[1] while the most important risk factor for anogenital infection is sexual activity.[2]
Sexual transmission
Risk factors responsible for sexual transmission of HPV include:
- Number of sex partners[3][4]
- Acquisition of new partner[3]
- Having nonmonogamous sex partner[5][6]
- Starting sexual activity at young age[5]
- Vaginal delivery and multiple deliveries[7]
- Age over 40 for women[8]
- History of Chlamydia infection[9]
- Long term OCP use[10]
References
- ↑ Bennett, John (2015). Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. Philadelphia, PA: Elsevier/Saunders. ISBN 9781455748013.
- ↑ Ho GY, Bierman R, Beardsley L, Chang CJ, Burk RD (1998). “Natural history of cervicovaginal papillomavirus infection in young women”. N. Engl. J. Med. 338 (7): 423–8. doi:10.1056/NEJM199802123380703. PMID 9459645.
- ↑ 3.0 3.1 Bell MC, Schmidt-Grimminger D, Jacobsen C, Chauhan SC, Maher DM, Buchwald DS (2011). “Risk factors for HPV infection among American Indian and white women in the Northern Plains”. Gynecol. Oncol. 121 (3): 532–6. doi:10.1016/j.ygyno.2011.02.032. PMC 4498572. PMID 21414655.
- ↑ Tarkowski TA, Koumans EH, Sawyer M, Pierce A, Black CM, Papp JR, Markowitz L, Unger ER (2004). “Epidemiology of human papillomavirus infection and abnormal cytologic test results in an urban adolescent population”. J. Infect. Dis. 189 (1): 46–50. doi:10.1086/380466. PMID 14702152.
- ↑ 5.0 5.1 Koutsky L (1997). “Epidemiology of genital human papillomavirus infection”. Am. J. Med. 102 (5A): 3–8. PMID 9217656.
- ↑ Winer RL, Lee SK, Hughes JP, Adam DE, Kiviat NB, Koutsky LA (2003). “Genital human papillomavirus infection: incidence and risk factors in a cohort of female university students”. Am. J. Epidemiol. 157 (3): 218–26. PMID 12543621.
- ↑ Tseng CJ, Liang CC, Soong YK, Pao CC (1998). “Perinatal transmission of human papillomavirus in infants: relationship between infection rate and mode of delivery”. Obstet Gynecol. 91 (1): 92–6. PMID 9464728.
- ↑ Ting J, Kruzikas DT, Smith JS (2010). “A global review of age-specific and overall prevalence of cervical lesions”. Int. J. Gynecol. Cancer. 20 (7): 1244–9. PMID 21495248.
- ↑ Kjaer SK, van den Brule AJ, Bock JE, Poll PA, Engholm G, Sherman ME, Walboomers JM, Meijer CJ (1997). “Determinants for genital human papillomavirus (HPV) infection in 1000 randomly chosen young Danish women with normal Pap smear: are there different risk profiles for oncogenic and nononcogenic HPV types?”. Cancer Epidemiol. Biomarkers Prev. 6 (10): 799–805. PMID 9332762.
- ↑ Ley C, Bauer HM, Reingold A, Schiffman MH, Chambers JC, Tashiro CJ, Manos MM (1991). “Determinants of genital human papillomavirus infection in young women”. J. Natl. Cancer Inst. 83 (14): 997–1003. PMID 1649312.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Aysha Anwar, M.B.B.S[2]
Overview
Most infections with HPV are subclinical, asymptomatic and resolves without any complications in immunocompetent individuals. Time to develop symptoms and signs is not well defined but it may take 3 weeks to 3 months for genital warts, several months to years for cellular abnormalities (metaplasia and dysplasia) and years for development of cancers. 90% of infections resolve within 2 years due to host immune response.[1]Persistent HPV infection is associated with risk factors such as multiple sexual partners, alcohol consumption, immunosuppression, older age, and multiple types of HPV detected previously. Without treatment, persistent infection with low-risk types (low-grade intraepithelial lesions) may resolve spontaneously or persist and proliferate as warty lesions. However, high-risk HPV types (16,18,31,32) may lead to high-grade intraepithelial lesions which ultimately to carcinoma(cervical, anal, vaginal, vulvar, penile and oropharyngeal).[2][3][4][5]Prognosis of HPV infection depends primarily on type of HPV causing infection.[6][7][8][9][10]
Natural history
Most infections with HPV are subclinical, asymptomatic and resolves without any complications in immunocompetent individuals. Time to develop symptoms and signs is not well defined but it may take 3 weeks to 3 months for genital warts, several months to years for cellular abnormalities (metaplasia and dysplasia) and years for development of cancers. 90% of infections resolve within 2 years due to host immune response.[1]
Persistent HPV infection is associated with risk factors such as multiple sexual partners, alcohol consumption, immunosuppression, older age, and multiple types of HPV detected previously. Without treatment, persistent infection with low-risk types (low-grade intraepithelial lesions) may resolve spontaneously or persist and proliferate as warty lesions. However, high-risk HPV types (16,18,31,32) may lead to high-grade intraepithelial lesions which ultimately to carcinoma(cervical, anal, vaginal, vulvar, penile and oropharyngeal).[2][3][4][5]Complications associated with the human papillomavirus infection include:[11][12][13][14][15][16][17][18]genital warts, cervical cancer, vaginal cancer, vulvar cancer, anal cancer, penile cancer, head and neck cancer.
Complications
Complications associated with the human papilloma virus infection include:[11][12][13][14][15][16][17][18]
- Genital warts
- Cervical cancer
- Vaginal cancer
- Vulvar cancer
- Anal cancer
- Penile cancer
- Head and neck cancer
Prognosis
Prognosis of HPV infection depends primarily on type of HPV causing infection.[6][7][8][9][10][19][20][21][22]
Good prognostic factors
- Low risk HPV type (1, 2, 4, 6, 11)[9]
- Immunocompetent[10]
- Early diagnosis and treatment[9][19]
- Regular follow-up
- Safe sex behavior
Bad prognostic factors
- High risk HPV type(16, 18, 31, 32)[6][7]
- Immunocompromised[10]
- Multiple sexual partners[8][21]
- Repeated infection in past years
- Delay in seeking treatment[23]
- Lack of follow up and screening[23]
- Metastatic carcinoma (cervical, anal, vaginal, oropharyngeal)[8][24]
- Presence of other STDs (HIV, syphilis, chlamydia)[20][21][22]
- Tobacco and alcohol usage[8][25][26]
References
- ↑ 1.0 1.1 Ault KA (2006). “Epidemiology and natural history of human papillomavirus infections in the female genital tract”. Infect Dis Obstet Gynecol. 2006 Suppl: 40470. doi:10.1155/IDOG/2006/40470. PMC 1581465. PMID 16967912.
- ↑ 2.0 2.1 Castle PE, Schiffman M, Herrero R, Hildesheim A, Rodriguez AC, Bratti MC; et al. (2005). “A prospective study of age trends in cervical human papillomavirus acquisition and persistence in Guanacaste, Costa Rica”. J Infect Dis. 191 (11): 1808–16. doi:10.1086/428779. PMID 15871112.
- ↑ 3.0 3.1 Woodman CB, Collins S, Winter H, Bailey A, Ellis J, Prior P; et al. (2001). “Natural history of cervical human papillomavirus infection in young women: a longitudinal cohort study”. Lancet. 357 (9271): 1831–6. doi:10.1016/S0140-6736(00)04956-4. PMID 11410191.
- ↑ 4.0 4.1 Ho GY, Bierman R, Beardsley L, Chang CJ, Burk RD (1998). “Natural history of cervicovaginal papillomavirus infection in young women”. N Engl J Med. 338 (7): 423–8. doi:10.1056/NEJM199802123380703. PMID 9459645.
- ↑ 5.0 5.1 http://www.cdc.gov/vaccines/pubs/pinkbook/hpv.html Accessed on October 13, 2016
- ↑ 6.0 6.1 6.2 Yang SH, Kong SK, Lee SH, Lim SY, Park CY (2014). “Human papillomavirus 18 as a poor prognostic factor in stage I-IIA cervical cancer following primary surgical treatment”. Obstet Gynecol Sci. 57 (6): 492–500. doi:10.5468/ogs.2014.57.6.492. PMC 4245343. PMID 25469338.
- ↑ 7.0 7.1 7.2 No JH, Sung MW, Hah JH, Choi SH, Lee MC, Kim HS; et al. (2015). “Prevalence and prognostic value of human papillomavirus genotypes in tonsillar squamous cell carcinoma: a Korean multicenter study”. Cancer. 121 (4): 535–44. doi:10.1002/cncr.29086. PMID 25283642.
- ↑ 8.0 8.1 8.2 8.3 8.4 Lin BM, Wang H, D’Souza G, Zhang Z, Fakhry C, Joseph AW; et al. (2013). “Long-term prognosis and risk factors among patients with HPV-associated oropharyngeal squamous cell carcinoma”. Cancer. 119 (19): 3462–71. doi:10.1002/cncr.28250. PMC 3788050. PMID 23861037.
- ↑ 9.0 9.1 9.2 9.3 Beutner KR, Wiley DJ, Douglas JM, Tyring SK, Fife K, Trofatter K; et al. (1999). “Genital warts and their treatment”. Clin Infect Dis. 28 Suppl 1: S37–56. doi:10.1086/514722. PMID 10028109.
- ↑ 10.0 10.1 10.2 10.3 Ferenczy A, Coutlée F, Franco E, Hankins C (2003). “Human papillomavirus and HIV coinfection and the risk of neoplasias of the lower genital tract: a review of recent developments”. CMAJ. 169 (5): 431–4. PMC 183297. PMID 12952805.
- ↑ 11.0 11.1 http://www.cdc.gov/hpv/parents/vaccine.html Accessed on October 11, 2016
- ↑ 12.0 12.1 Tilston P (1997). “Anal human papillomavirus and anal cancer”. J Clin Pathol. 50 (8): 625–34. PMC 500098. PMID 9301544.
- ↑ 13.0 13.1 Palefsky JM, Holly EA, Ralston ML, Jay N (1998). “Prevalence and risk factors for human papillomavirus infection of the anal canal in human immunodeficiency virus (HIV)-positive and HIV-negative homosexual men”. J Infect Dis. 177 (2): 361–7. PMID 9466522.
- ↑ 14.0 14.1 Maden C, Sherman KJ, Beckmann AM, Hislop TG, Teh CZ, Ashley RL; et al. (1993). “History of circumcision, medical conditions, and sexual activity and risk of penile cancer”. J Natl Cancer Inst. 85 (1): 19–24. PMID 8380060.
- ↑ 15.0 15.1 Varma VA, Sanchez-Lanier M, Unger ER, Clark C, Tickman R, Hewan-Lowe K; et al. (1991). “Association of human papillomavirus with penile carcinoma: a study using polymerase chain reaction and in situ hybridization”. Hum Pathol. 22 (9): 908–13. PMID 1655618.
- ↑ 16.0 16.1 Gillison ML, Koch WM, Capone RB, Spafford M, Westra WH, Wu L; et al. (2000). “Evidence for a causal association between human papillomavirus and a subset of head and neck cancers”. J Natl Cancer Inst. 92 (9): 709–20. PMID 10793107.
- ↑ 17.0 17.1 Beachler DC, DʼSouza G (2013). “Oral human papillomavirus infection and head and neck cancers in HIV-infected individuals”. Curr Opin Oncol. 25 (5): 503–10. doi:10.1097/CCO.0b013e32836242b4. PMC 3896303. PMID 23852381.
- ↑ 18.0 18.1 de Sanjose S, Quint WG, Alemany L, Geraets DT, Klaustermeier JE, Lloveras B; et al. (2010). “Human papillomavirus genotype attribution in invasive cervical cancer: a retrospective cross-sectional worldwide study”. Lancet Oncol. 11 (11): 1048–56. doi:10.1016/S1470-2045(10)70230-8. PMID 20952254.
- ↑ 19.0 19.1 Zampronha Rde A, Freitas-Junior R, Murta EF, Michelin MA, Barbaresco AA, Adad SJ; et al. (2013). “Human papillomavirus types 16 and 18 and the prognosis of patients with stage I cervical cancer”. Clinics (Sao Paulo). 68 (6): 809–14. doi:10.6061/clinics/2013(06)14. PMC 3674251. PMID 23778490.
- ↑ 20.0 20.1 Tamim H, Finan RR, Sharida HE, Rashid M, Almawi WY (2002). “Cervicovaginal coinfections with human papillomavirus and Chlamydia trachomatis”. Diagn Microbiol Infect Dis. 43 (4): 277–81. PMID 12151187.
- ↑ 21.0 21.1 21.2 Martins AE, Lucena-Silva N, Garcia RG, Welkovic S, Barbosa A, Menezes ML; et al. (2014). “Prognostic evaluation of DNA index in HIV-HPV co-infected women cervical samples attending in reference centers for HIV-AIDS in Recife”. PLoS One. 9 (8): e104801. doi:10.1371/journal.pone.0104801. PMC 4140713. PMID 25144309.
- ↑ 22.0 22.1 Fitzgerald DW, Bezak K, Ocheretina O, Riviere C, Wright TC, Milne GL; et al. (2012). “The effect of HIV and HPV coinfection on cervical COX-2 expression and systemic prostaglandin E2 levels”. Cancer Prev Res (Phila). 5 (1): 34–40. doi:10.1158/1940-6207.CAPR-11-0496. PMC 3252428. PMID 22135046.
- ↑ 23.0 23.1 Yanofsky VR, Patel RV, Goldenberg G (2012). “Genital warts: a comprehensive review”. J Clin Aesthet Dermatol. 5 (6): 25–36. PMC 3390234. PMID 22768354.
- ↑ Fuller AF, Elliott N, Kosloff C, Hoskins WJ, Lewis JL (1989). “Determinants of increased risk for recurrence in patients undergoing radical hysterectomy for stage IB and IIA carcinoma of the cervix”. Gynecol Oncol. 33 (1): 34–9. PMID 2703164.
- ↑ Brennan JA, Boyle JO, Koch WM, Goodman SN, Hruban RH, Eby YJ; et al. (1995). “Association between cigarette smoking and mutation of the p53 gene in squamous-cell carcinoma of the head and neck”. N Engl J Med. 332 (11): 712–7. doi:10.1056/NEJM199503163321104. PMID 7854378.
- ↑ Maxwell JH, Kumar B, Feng FY, Worden FP, Lee JS, Eisbruch A; et al. (2010). “Tobacco use in human papillomavirus-positive advanced oropharynx cancer patients related to increased risk of distant metastases and tumor recurrence”. Clin Cancer Res. 16 (4): 1226–35. doi:10.1158/1078-0432.CCR-09-2350. PMC 2822887. PMID 20145161.
Treatment
Treatment
Medical Therapy | Surgery | Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
External Links
External Links
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH