
Microsporidiosis
For the patient information, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ahmed Younes M.B.B.CH [2]
Synonyms and keywords: Microsporidial infection, Infection by microsporidia
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ahmed Younes M.B.B.CH [2]
Overview
Microsporidiosis is an opportunistic intestinal infection that causes diarrhea and wasting in immunocompromised individuals (HIV, for example). It results from different species of microsporidia, a group of protozoal parasites. In HIV infected individuals, microsporidiosis generally occurs when CD4+ T cell counts fall below 100. Microsporidiosis was first discovered in 1959 and its prevalence has increased in the late 20th century due to the worldwide spread of HIV. Immunodeficiency is the most common risk factor for developing microsporidiosis and leads to a worse outcome.
Microsporidiosis presents in many forms and can affect many systems. The most common form is intestinal microsporidiosis, which causes diarrhea and weight loss and can be complicated with nutritional deficiencies, weight loss, and acalculous cholecystitis. Diagnosis is confirmed by microscopic identification of the organism and positive PCR. The mainstay of therapy is HAART aiming for a CD4+ T cell > 100 cell/mcm.
Historical Perspective
Phylum Microsporidia were first described in the 19th century, while the first human case was described in 1959. The number of cases increased after the spread of AIDS.
Classification
There is no classification system established for Microsporidiosis.
Pathophysiology
Microsporidia are a group of obligate intracellular parasitic fungi with more than 1,200 species belonging to 143 genera that infect a wide range of vertebrate and invertebrate hosts. They are characterized by the production of resistant spores that vary in size, depending on the species. After ingestion, microsporidia infect intestinal epithelial cells and cause chronic diarrhea with the possibility of distant spread. The microorganism can be visualized in stool samples using “Quick-Hot Gram Chromotrope technique.”
Causes
Microsporidiosis is an infection caused by microsporidia.
Differentiating Microsporidiosis from other diseases
Microsporidiosis should be differentiated from other conditions that cause chronic diarrhea in immunocompromised patients.
Epidemiology and Demographics
The overall prevalence is not accurately estimated especially in the whole population (because microsporidiosis is usually investigated in immunocompromised patients with correlating gastrointestinal symptoms to microsporidiosis. The disease is present worldwide. In HIV patients with diarrhea, microsporidia were the most commonly isolated organism, with a prevalence of 39%.
Risk Factors
The most potent risk factor in the development of microsporidiosis is immunodeficiency. Other risk factors among immunodeficient patients include poor sanitation and contact with poultry droppings.[1][2]
Natural History, Complications, and Prognosis
If left untreated, immunocompetent patients resolve the disease completely within 2 weeks while immunocompromised patients might develop chronic diarrhea. Common complications of microsporidiosis include weight loss, dehydration, and acalculous cholecystitis. Prognosis is generally excellent in immunocompetent patients while immunocompromised patients are more vulnerable to developing chronic disease and complications.
Diagnosis
History and Symptoms
Symptoms of intestinal microsporidiosis include chronic diarrhea, abdominal pain, and weight loss.
Physical Examination
Patients with microsporidiosis usually appear ill. Physical examination of patients with microsporidiosis is usually remarkable for weight loss, wasting and abdominal tenderness.
Laboratory Findings
Laboratory findings consistent with the diagnosis of microsporidiosis include microscopic identification of the organism in fecal smears using chromotrope 2R method or “Quick-Hot Gram Chromotrope technique”, positive PCR, and positive serology using indirect immunofluorescence.
Imaging Findings
There are no imaging findings associated with microsporidiosis.
Treatment
Medical Therapy
The mainstay of therapy for microsporidiosis in immunocompromised patients is highly active antiretroviral therapy (HAART). Albendazole and fumagillin have demonstrated consistent activity against other microsporidia in vitro and in vivo.
Surgery
Surgical intervention is not recommended in the management of microsporidiosis.
Prevention
Effective measures for the primary prevention of microsporidiosis include HAART, avoiding contact with poultry and avoiding swimming pools while secondary prevention strategies following microsporidiosis include continuing treatment indefinitely after ocular microsporidiosis and continued HAART for HIV patients.
References
- ↑ Didier ES, Weiss LM (2006). “Microsporidiosis: current status”. Curr Opin Infect Dis. 19 (5): 485–92. doi:10.1097/01.qco.0000244055.46382.23. PMC 3109650. PMID 16940873.
- ↑ Anuar TS, Bakar NH, Al-Mekhlafi HM, Moktar N, Osman E (2016). “PREVALENCE AND RISK FACTORS FOR ASYMPTOMATIC INTESTINAL MICROSPORIDIOSIS AMONG ABORIGINAL SCHOOL CHILDREN IN PAHANG, MALAYSIA”. Southeast Asian J Trop Med Public Health. 47 (3): 441–9. PMID 27405127.
Historical perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ahmed Younes M.B.B.CH [2]
Overview
Phylum Microsporidia was first described in the 19th century while the first human case was described in 1959. The number of cases increased after the spread of AIDS.[1]
Historical perspective
Phylum microsporidia were first described in the 19th century while the first human case was described in 1959. The number of cases increased after the spread of AIDS.[1]
- In late 19th century, phylum microsporidia were first discovered.
- In 1959, the first human case was described in a Japanese child.
- In 1985, microsporidiosis was first described in an AIDS patient in France.
- With the spread of HIV, the number of cases was increased and microsporidiosis was almost always found in HIV and immunocompromised patients.
- In 1996, E. bieneusi was first described in pigs in Switzerland.
References
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ahmed Younes M.B.B.CH [2]
Overview
There is no classification system established for microsporidiosis.
Classification
There is no classification system established for microsporidiosis.
References
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ogheneochuko Ajari, MB.BS, MS [2] Ahmed Younes M.B.B.CH [3]
Overview
Microsporidia are a group of obligate intracellular protozoa with more than 1,200 species belonging to 143 genera that infect a wide range of vertebrate and invertebrate hosts. They are characterized by the production of resistant spores that vary in size, depending on the species. After ingestion, it infects intestinal epithelial cells and causes chronic diarrhea with the possibility of distant spread. The microorganism can be visualized in stool samples using “Quick-Hot Gram Chromotrope technique”.
Pathophysiology
Life Cycle
The infective form of microsporidia is the resistant spore and it can survive for an extended period of time in the environment.[1]
 |
- The spores enter the body via ingestion or inhalation.
- Spores penetrate host cell using its polar tubule.
- The spore uses its polar tubule for injecting its sarcoplasm into the infected cell.
- The sarcoplasm multiplies either by binary fission or multiple fission
- The sarcoplasm of microsporidia develops into mature spores either free in the cytoplasm or inside a vacuole.
- The process of development involves acquiring a thick capsule. This capsule provides protection against environmental stressors and is thought to play a role in its infectivity.
- After their number reaches a certain limit, the host cell ruptures releasing the spores to continue the life cycle.
Pathogenesis
- Microsporidia cause distortion of the villi without profound inflammatory findings.[2][3]
- With the progression of the disease, the microsporidia interfere with the intestinal absorption causing various symptoms of malabsorption (weight loss, chronic diarrhea, and vitamin deficiencies).
- Disseminated disease can cause symptoms in the biliary tract, respiratory system, the urinary tract or the eye.
Microscopic pathology
- Intestinal biopsy shows crypt hyperplasia and decreases in the absorptive surface of the intestine.[2]
- Stool examination using “Quick-Hot Gram Chromotrope technique” reveals the spores staining dark violet and containing gram-positive granules.
- Enterocytozoon bieneusi spores measure 0.8 – 1.4 µm while spores of Anncaliia algerae, Encephalitozoon spp., Vittaforma corneae, and Nosema spp measure 1.5 – 4 µm.
-
 Sporoblast of the Microsporidium Fibrillanosema crangonycis – By No machine-readable author provided. Javier martin assumed (based on copyright claims). – No machine-readable source provided. Own work assumed (based on copyright claims)., CC BY 2.5, https://commons.wikimedia.org/w/index.php?curid=919796
Sporoblast of the Microsporidium Fibrillanosema crangonycis – By No machine-readable author provided. Javier martin assumed (based on copyright claims). – No machine-readable source provided. Own work assumed (based on copyright claims)., CC BY 2.5, https://commons.wikimedia.org/w/index.php?curid=919796 -
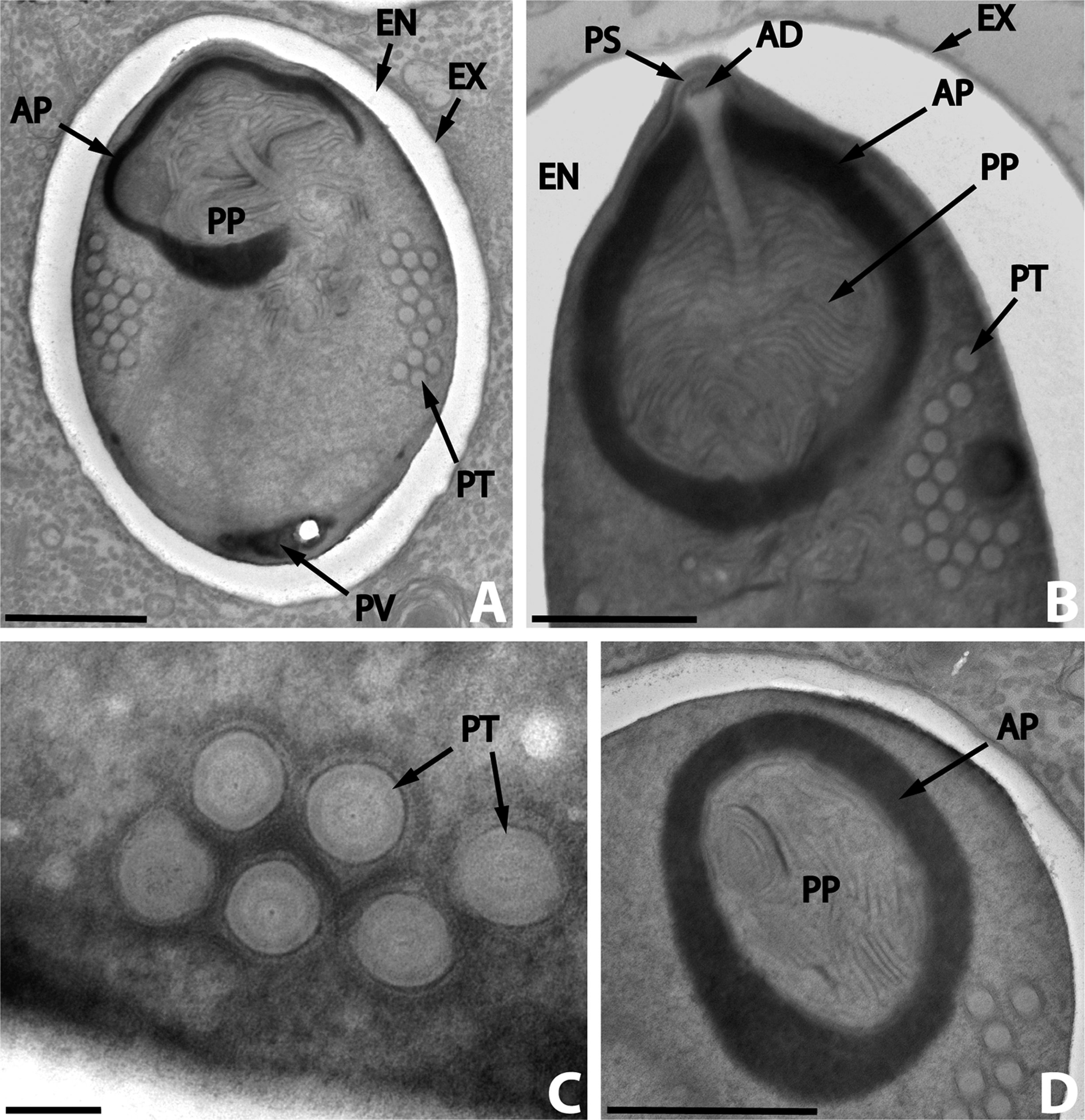 Dictyocoela diporeiae.A, meront and spore; B, spore wall; C, polar filament – By Andrew David Winters & Mohamed Faisal – Winters, A. D., Faisal, M. 2014. Molecular and ultrastructural characterization of Dictyocoela diporeiae n. sp. (Microsporidia), a parasite of Diporeia spp. (Amphipoda, Gammaridea). Parasite, 21, 26 doi:10.1051/parasite/2014028, CC BY 2.0, https://commons.wikimedia.org/w/index.php?curid=33448743
Dictyocoela diporeiae.A, meront and spore; B, spore wall; C, polar filament – By Andrew David Winters & Mohamed Faisal – Winters, A. D., Faisal, M. 2014. Molecular and ultrastructural characterization of Dictyocoela diporeiae n. sp. (Microsporidia), a parasite of Diporeia spp. (Amphipoda, Gammaridea). Parasite, 21, 26 doi:10.1051/parasite/2014028, CC BY 2.0, https://commons.wikimedia.org/w/index.php?curid=33448743 -
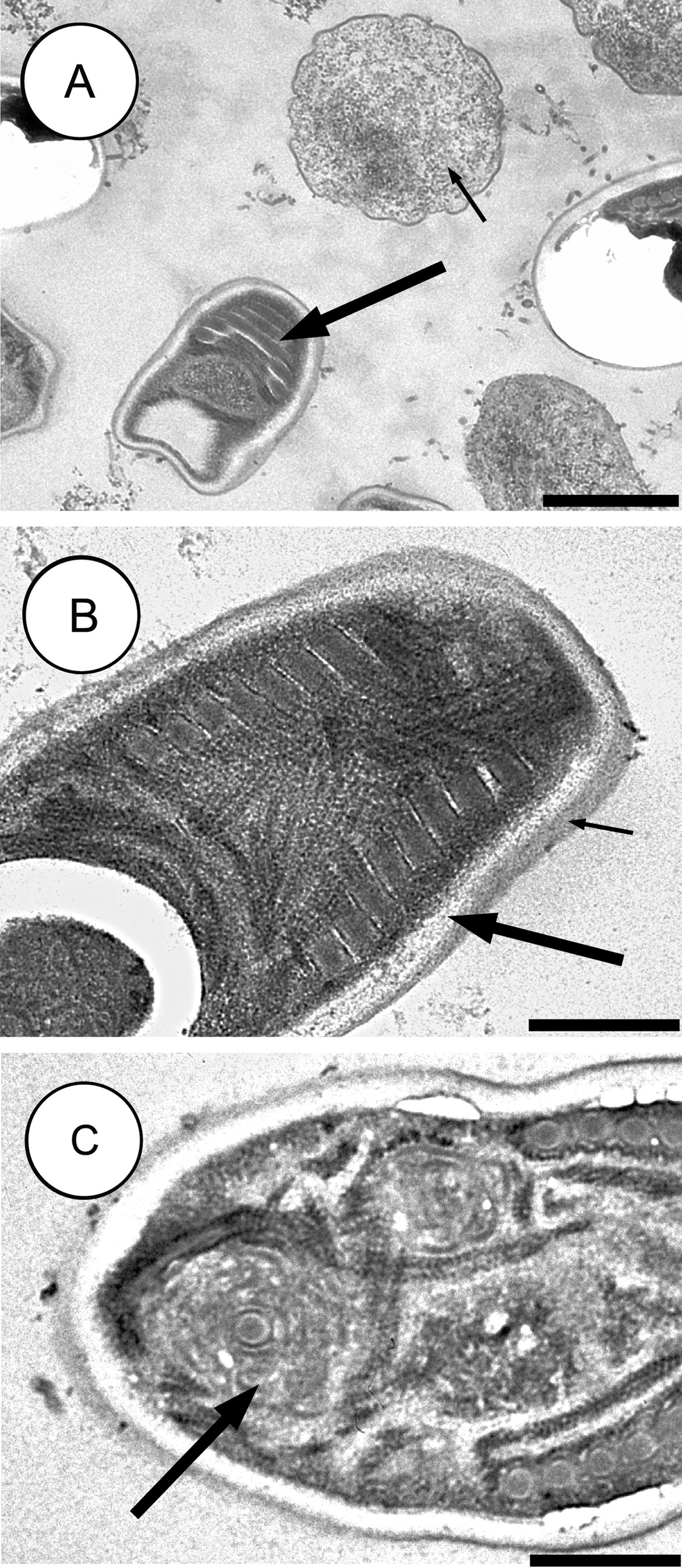 A hyperparasitic microsporidian, Nosema podocotyloidis – By Bhen Sikina Toguebaye, Yann Quilichini, Papa Mbagnick Diagne and Bernard Marchand – Toguebaye, B. S., Quilichini, Y., Diagne, P. M. & Marchand, B. 2014: Ultrastructure and development of Nosema podocotyloidis n. sp. (Microsporidia), a hyperparasite of Podocotyloides magnatestis (Trematoda), a parasite of Parapristipoma octolineatum (Teleostei). Parasite, 21, 44. doi:10.1051/parasite/2014044, CC BY 2.0, https://commons.wikimedia.org/w/index.php?curid=35088476
A hyperparasitic microsporidian, Nosema podocotyloidis – By Bhen Sikina Toguebaye, Yann Quilichini, Papa Mbagnick Diagne and Bernard Marchand – Toguebaye, B. S., Quilichini, Y., Diagne, P. M. & Marchand, B. 2014: Ultrastructure and development of Nosema podocotyloidis n. sp. (Microsporidia), a hyperparasite of Podocotyloides magnatestis (Trematoda), a parasite of Parapristipoma octolineatum (Teleostei). Parasite, 21, 44. doi:10.1051/parasite/2014044, CC BY 2.0, https://commons.wikimedia.org/w/index.php?curid=35088476



References
- ↑ “CDC – DPDx – Microsporidiosis”.
- ↑ 2.0 2.1 Franzen C, Müller A (2001). “Microsporidiosis: human diseases and diagnosis”. Microbes Infect. 3 (5): 389–400. PMID 11369276.
- ↑ Weber R, Bryan RT, Schwartz DA, Owen RL (1994). “Human microsporidial infections”. Clin. Microbiol. Rev. 7 (4): 426–61. PMC 358336. PMID 7834600.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Microsporidia are parasites of animals, now considered to be extremely reduced fungi. Most infect insects, but they are also responsible for common diseases of crustaceans and fish, and have been found in most other animal groups, including humans and other mammals which can be parasitized by species of Encephalitozoon. Replication takes place within the host’s cells, which are infected by means of unicellular spores. These vary from 1-40 μm, making them some of the smallest eukaryotes. They also have the shortest eukaryotic genomes.
Microsporidia are unusual in lacking mitochondria and in having mitosomes. They also lack motile structures such as flagella. The spores are protected by a layered wall including proteins and chitin. Their interior is dominated by a unique coiled structure called a polar tube (not to be confused with the polar filaments of Myxozoa). In most cases there are two closely associated nuclei, forming a diplokaryon, but sometimes there is only one.
During infection, the polar tube penetrates the host cell (the process has been compared by Patrick J. Keeling to “turning a garden hose inside out”), and the contents of the spore are pumped through it. Keeling likens the system to a combination of “harpoon and hypodermic syringe“, adding that it is “one of the most sophisticated infection mechanisms in biology”.
Once inside the host cell, the sporoplasm grows, dividing or forming a multinucleate plasmodium before producing new spores. The life cycle varies considerably. Some have a simple asexual life cycle, while others have a complex life cycle involving multiple hosts and both asexual and sexual reproduction. Different types of spores may be produced at different stages, probably with different functions including autoinfection (transmission within a single host). The Microsporidia often cause chronic, debilitating diseases rather than lethal infections. Effects on the host include reduced longevity, fertility, weight, and general vigor. Vertical transmission of microsporidia is frequently reported. In the case of insect hosts, vertical transmission often occurs as transovarial transmission, where the microsporidian parasites pass from the ovaries of the female host into eggs and eventually multiply in the infected larvae. Amblyospora salinaria n. sp. which infects the mosquito Culex salinarius Coquillett, and Amblyospora californica which infects the mosquito Culex tarsalis Coquillett, provide typical examples of transovarial transmission of microsporidia (Andreadis and Hall 1979a,b; Jahn et al. 1986; Becnel and Andreadis 1998).
Because they are unicellular, Microsporidia were traditionally treated as protozoa, and like other amitochondriate eukaryotes were considered to have diverged very early on. However, other genes place them alongside or within the Fungi, and this is supported by several chemical and morphological features. In particular, they appear to be allied with the Zygomycota or Ascomycota.
Microsporidium was once the vernacular name for a member of the class Microsporea (Corliss and Levine 1963).
Classification
- Subclass: Dihaplophasea
- Order: Meiodihaplophasida
- Superfamily Thelohanioidea
- Family Thelohaniidae
- Family Duboscqiidae
- Family Janacekiidae
- Family Pereziidae
- Family Striatosporidae
- Family Cylindrosporidae
- Superfamily Burenelloidea
- Family Burenellidae
- Superfamily Amblyosporoidae
- Family Amblyosporidae
- Superfamily Thelohanioidea
- Order Dissociodihaplophasida
- Superfamily Nosematoidea
- Family Nosematidae
- Family Ichthyosporidiidae
- Family Caudosporidae
- Family Pseudopleistophoridae
- Family Mrazekiidae
- Superfamily Culicosporoidea
- Family Culicosporidae
- Family Culicosporellidae
- Family Golbergiidae
- Family Spragueidae
- Superfamily Ovavesiculoidea
- Family Ovavesiculidae
- Family Tetramicridae
- Superfamily Nosematoidea
- Order: Meiodihaplophasida
- Subclass Haplophasea
- Order Glugeida
- Family Glugeidae
- Family Pleistophoridae
- Family Encephalitozoonidae
- Family Abelsporidae
- Family Tuzetiidae
- Family Microfilidae
- Family Unikaryonidae
- Order Chyridiopsida
- Family Chytridiopsida
- Family Buxtehudiidae
- Family Enterocytozoonidae
- Family Burkeidae
- Order Glugeida
Microsporidia causing human disease
Although phylum microsporidia have more than 1000 species and over 100 genres, Only 14 species were associated with human disease.
- Anncaliia (formerly Brachiola)[2]
- A. algerae, A. connori, A. vesicularum
- Encephalitozoon
- E. cuniculi, E. hellem, E. intestinalis (formerly Septata intestinalis)
- Enterocytozoon
- E. bieneusi
- Microsporidium
- M. ceylonensis, M. africanum
- Nosema
- N. ocularum
- Pleistophora sp.
- Trachipleistophora
- T. hominis, T. anthropophthera
- Vittaforma
- V. corneae.
- Tubulinosema
- T. acridophagus
Diseases caused by the different species
The clinical manifestations vary according to the causative species with diarrhea being the most common presentation.[3]
| Microsporidian species | Clinical manifestation |
| Anncaliia algerae | Keratoconjunctivitis, skin and deep muscle infection |
| Enterocytozoon bieneusi* | Diarrhea, acalculous cholecystitis |
| Encephalitozoon cuniculi and Encephalitozoon hellem | Keratoconjunctivitis, infection of respiratory and genitourinary tract, disseminated infection |
| Infection of the GI tract causing diarrhea, and dissemination to ocular, genitourinary and respiratory tracts | |
| Microsporidium (M. ceylonensis and M. africanum) | Infection of the cornea |
| Nosema sp. (N. ocularum), Anncaliia connori | Ocular infection |
| Pleistophora sp. | Muscular infection |
| Trachipleistophora anthropophthera | Disseminated infection |
| Trachipleistophora hominis | Muscular infection, stromal keratitis, (probably disseminated infection) |
| Tubulinosema acridophagus | Disseminated infection |
| Vittaforma corneae (syn. Nosema corneum) | Ocular infection, urinary tract infection |
*Two reports of E. bieneusi in respiratory samples have also been published, one in 1992 and the other in 1997.
See also
- List of Microsporidian Genera
- Nosema apis, a microsporidian parasite of bees
References
- ↑ Balbiani, G. (1882). “Sur les microsporides ou psorospermies des Articulés”. Comptes rendus de l’Académie des Sciences, Paris. 95: 1168–1171.
- ↑ Didier ES, Weiss LM (2006). “Microsporidiosis: current status”. Curr Opin Infect Dis. 19 (5): 485–92. doi:10.1097/01.qco.0000244055.46382.23. PMC 3109650. PMID 16940873.
- ↑ “CDC – DPDx – Microsporidiosis”.
- Andreadis, T. G., and Hall, D. W. 1979a. Development, ultrastructure, and mode of transmission of Amblyospora sp. (Microspora) in the mosquito. J. Protozool. 26, 444–452.
- Andreadis, T. G., and Hall, D. W. 1979b. Significance of transovarial infections of Amblyospora sp. (Microspora: Thelohaniidae) in relation to parasite maintenance in the mosquito Culex salinarius. J. Invertebr. Pathol. 34, 152–157.
- Becnel, J. J. and Andreadis, T. G. 1998. Amblyospora salinaria n. sp. (Microsporidia: Amblyosporidae): parasite of Culex salinarius (Diptera: Culicidae), its life stages in an intermediate host and establishment as a new species. J. Invertebr. Pathol. 71:258-262.
- Corliss, J.O. and Levine, N.D. 1963. Establishment of the Microsporidia as a new class in the protozoan subphylum Cnidospora.. J. Protozool., 10 (Suppl.), 26-27.
- Jahn, G. C., Hall, D.W., and Zam, S. G. 1986. A comparison of the life cycles of two Amblyospora (Microspora: Amblyosporidae) in the mosquitoes Culex salinarius and Culex tarsalis Coquillett. J. Florida Anti-Mosquito Assoc. 57, 24–27.
- Patrick J. Keeling et al. (2000). Evidence from Beta-Tubulin Phylogeny that Microsporidia Evolved From Within the Fungi. Molecular Biology and Evolution 17:23-31.
- Nature 414, 401 – 402 (22 November 2001); doi:10.1038/35106666
Differentiating Microsporidiosis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ogheneochuko Ajari, MB.BS, MS [2] Ahmed Younes M.B.B.CH [3]
Overview
Microsporidiosis should be differentiated from other conditions that cause chronic diarrhea in immunocompromised patients.
Differentiating Microsporidiosis from other Diseases
Differential Diagnosis
Microsporidiosis must be differentiated from other diseases that may cause chronic diarrhea, weight loss, and abdominal pain especially in immunocompromised patients.
| Disease | Prominent clinical findings | Laboratory or radiological findings |
|---|---|---|
| Chronic giardiasis[1] |
|
|
| Cryptosporidiosis[2] |
|
|
| Cystoisosporiasis (isosporiasis)[3] |
|
|
| Tropical sprue[4] |
|
|
References
- ↑ Thompson RC (2000). “Giardiasis as a re-emerging infectious disease and its zoonotic potential”. Int. J. Parasitol. 30 (12–13): 1259–67. PMID 11113253.
- ↑ Sánchez-Vega JT, Tay-Zavala J, Aguilar-Chiu A, Ruiz-Sánchez D, Malagón F, Rodríguez-Covarrubias JA, Ordóñez-Martínez J, Calderón-Romero L (2006). “Cryptosporidiosis and other intestinal protozoan infections in children less than one year of age in Mexico City”. Am. J. Trop. Med. Hyg. 75 (6): 1095–8. PMID 17172373.
- ↑ Current WL, Garcia LS (1991). “Cryptosporidiosis”. Clin. Microbiol. Rev. 4 (3): 325–58. PMC 358202. PMID 1889046.
- ↑ Klipstein FA, Schenk EA (1975). “Enterotoxigenic intestinal bacteria in tropical sprue. II. Effect of the bacteria and their enterotoxins on intestinal structure”. Gastroenterology. 68 (4 Pt 1): 642–55. PMID 1091526.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ogheneochuko Ajari, MB.BS, MS [2] Ahmed Younes M.B.B.CH [3]
Overview
The overall prevalence is not accurately estimated especially in the whole population (because microsporidiosis is usually investigated in immunocompromised patients with correlating gastrointestinal tract symptoms to microsporidiosis). The disease is present all over the world. In HIV patients with diarrhea, the prevalence of microsporidiosis was 39% being the most common isolated organism.
Epidemiology and Demographics
Prevalence:
- The overall prevalence is not accurately estimated especially in the whole population (because microsporidiosis is usually investigated in immunocompromised patients with correlating gastrointestinal tract symptoms to microsporidiosis).[1][2]
- In HIV patients with diarrhea, the prevalence of microsporidiosis was 39% being the most common isolated organism.
Case fatality rate:
- The case-fatality rate of intestinal microsporidiosis is approximately 56% among HIV patients.
Race
- There is no racial predilection to the microsporidiosis.[3]
Age
- Patients of all age groups may develop microsporidiosis.[3]
Sex
- Males and females are affected equally by microsporidiosis.[3]
Geographic distribution
- Microsporidiosis infections occur worldwide with no geographic predilection.[2]
References
- ↑ Kotler DP, Orenstein JM (1994). “Prevalence of intestinal microsporidiosis in HIV-infected individuals referred for gastroenterological evaluation”. Am. J. Gastroenterol. 89 (11): 1998–2002. PMID 7942725.
- ↑ 2.0 2.1 “CDC – DPDx – Microsporidiosis”.
- ↑ 3.0 3.1 3.2 Didier ES, Weiss LM (2006). “Microsporidiosis: current status”. Curr Opin Infect Dis. 19 (5): 485–92. doi:10.1097/01.qco.0000244055.46382.23. PMC 3109650. PMID 16940873.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ahmed Younes M.B.B.CH [2] Ogheneochuko Ajari, MB.BS, MS [3]
Overview
The most potent risk factor in the development of microsporidiosis is immunodeficiency. Other risk factors among immunodeficient patients include poor sanitation and contact with poultry droppings.[1][2]
Risk factors
Immunodeficiency is the most important risk factor for developing microsporidiosis. Microsporidiosis is almost always reported in immunodeficient patients:[1][2]
- People with an immune deficiency (e.g. as a result of AIDS/HIV)
- Organ transplantation patients
- Patients undergoing chemotherapy
- Patients undergoing radiotherapy
- Hematologic malignancies
Risk factors among HIV patients
Intestinal microsporidiosis in persons with HIV infection have been linked with:[3]
- Severe immunodeficiency with CD4+ count <100
- Male homosexuality
- Swimming in pools
- Poor sanitation
- Contact with poultry droppings
References
- ↑ 1.0 1.1 Didier ES, Weiss LM (2006). “Microsporidiosis: current status”. Curr Opin Infect Dis. 19 (5): 485–92. doi:10.1097/01.qco.0000244055.46382.23. PMC 3109650. PMID 16940873.
- ↑ 2.0 2.1 Anuar TS, Bakar NH, Al-Mekhlafi HM, Moktar N, Osman E (2016). “PREVALENCE AND RISK FACTORS FOR ASYMPTOMATIC INTESTINAL MICROSPORIDIOSIS AMONG ABORIGINAL SCHOOL CHILDREN IN PAHANG, MALAYSIA”. Southeast Asian J Trop Med Public Health. 47 (3): 441–9. PMID 27405127.
- ↑ Hutin YJ, Sombardier MN, Liguory O, Sarfati C, Derouin F, Modaï J; et al. (1998). “Risk factors for intestinal microsporidiosis in patients with human immunodeficiency virus infection: a case-control study”. J Infect Dis. 178 (3): 904–7. PMID 9728570.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ahmed Younes M.B.B.CH [2]
Overview
If left untreated, immunocompetent patients resolve the disease completely within 2 weeks while immunocompromised patients might develop chronic diarrhea. Common complications of microsporidiosis include weight loss, dehydration, and acalculous cholecystitis. Prognosis is generally excellent in immunocompetent patients while immunocompromised patients are more vulnerable to developing chronic disease and complications.
Natural History
If left untreated, microsporidiosis is self-resolving with complete recovery within 14 days in immunocompetent patients. While in immunocompromised patients, the disease is more prolonged and patients are more vulnerable to complications such as malnutrition and vitamin deficiencies.[1]
Complications
Complications might arise in immunocompromised patients due to chronic diarrhea:[2][1]
- Dehydration
- Weight loss
- Nutritional deficiencies
- Acalculous cholecystitis
- Systemic spread to the brain, respiratory tract, urinary tract, etc.
Prognosis
- The prognosis is excellent among immunocompetent patients and the disease is self-limited within 2 weeks.
- In immunocompromised patients, the prognosis is less favorable with more vulnerability to develop systemic spread of the disease and complications.
- Mortality due to microsporidiosis is mostly associated with systemic disease and in AIDS patients not receiving HAART.
References
- ↑ 1.0 1.1 van Hal SJ, Muthiah K, Matthews G, Harkness J, Stark D, Cooper D, Marriott D (2007). “Declining incidence of intestinal microsporidiosis and reduction in AIDS-related mortality following introduction of HAART in Sydney, Australia”. Trans. R. Soc. Trop. Med. Hyg. 101 (11): 1096–100. doi:10.1016/j.trstmh.2007.06.003. PMID 17662322.
- ↑ Ramanan P, Pritt BS (2014). “Extraintestinal microsporidiosis”. J. Clin. Microbiol. 52 (11): 3839–44. doi:10.1128/JCM.00971-14. PMC 4313212. PMID 24829239.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | X ray | CT | MRI | Other imaging studies | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Related Chapters
Related Chapters
External links
External links
- CDC’s microsporidiosis info page.
- Treating Opportunistic Infections Among HIV-Infected Adults and Adolescents, Recommendations from CDC, the National Institutes of Health, and the HIV Medicine Association/Infectious Diseases Society of America CDC’s [3]
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH