
Oesophagostomum
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Oesophagostomum species are free-living nematodes of the family Strongyloidae. These worms occur in Africa, Brazil, China, Indonesia and the Philippines. The majority of human infection with Oesophagostomum is localized to northern Togo and Ghana. Because the eggs may be indistinguishable from those of the hookworms (which are widely distributed and can also rarely cause helminthomas), the species causing human helminthomas are rarely identified with accuracy.Oesophagostomum, especially O. bifurcum, are common parasites of livestock and animals like goats, pigs, and non-human primates, although it seems that humans are increasingly becoming favorable hosts as well. The disease they cause, oesophagostomiasis, is known for the nodule formation it causes in the intestines of its infected hosts, which can lead to more serious problems such as dysentery. Although the routes of human infection have yet to be elucidated sufficiently, it is believed that transmission occurs through oral-fecal means, with infected humans unknowingly ingesting soil containing the infectious filariform larvae.
Oesophagostomum infection is largely localized to northern Togo and Ghana in western Africa where it is a serious public health problem. Because it is so localized research on intervention measures and the implementation of effective public health interventions have been lacking. In recent years, however, there have been advances in the diagnosis of Oesophagostomum infection with PCR assays and ultrasound and recent interventions involving mass treatment with albendazole shows promise for controlling and possibly eliminating Oesophagostomum infection in northern Togo and Ghana.
Classification
Oesophagostomum is part of the phylum Nematoda. This phylum is composed of five orders: Ascaridida, Enoplida, Oxyurida, Spirurida, Strongylida, and Rhabditida.[1] Strongylida has three superfamilies: Ancyclostomatoidea, Trichostrongyloidea, andStrongylidea. Oesophagostomum lie within the Strongyloidae.[2]
Pathophysiology
In oesophagostomiasis, larvae can invade the colon wall, potentially causing two pervading types of nodular pathology. Multinodular disease is characterized by the formation of many tiny nodular lesions containing worms and pus along the colon wall. About 15% of patients have this form of oesophagostomiasis.[3]
Differential Diagnosis
Oesophagostomum needs to be differentiated from common misdiagnosis which include carcinoma, appendicitis, amebiasis, and tuberculosis.[4]
Diagnosis
Laboratory Findings
A definitive diagnosis of Oesophagostomum infection is traditionally done by demonstrating the presence of the larval or young adult forms in nodules of the intestinal wall via surgical examination of tissue. The larvae usually found in tissues can be 500 nanometers or longer in length.[5] With microscopy, one can identify the larvae based on the presence of somatic musculature divided into four quarters, along with a multinucleated intestine as well as an immature reproductive system.
Echocardiography or Ultrasound
Recent advances have allowed for less invasive and more accurate methods of diagnosis by ultrasonographic imaging.
Treatment
Surgery
In the case of formation of abscesses or fistulae arising from Dapaong tumors, incision and drainage is performed, followed by a regimen of albendazole and antibiotic treatment.[6]
Primary Prevention
Given that infective Oesophagostomum larvae are most likely transmitted via oral-fecal routes, sufficiently cleaning and cooking meat and vegetables, as well as boiling all consumed water or only using potable water would help to complement a mass treatment program. Factors like religion, family size and wealth do not suffice in explaining the unique epidemiology of Oesophagostomum; geographic and geological factors must be explored in more detail.[7]
References
- ↑ John, David T., Krotoski, Wojciech A. and Markell, Edward K. Markell and Voge’s Medical Parasitology. St. Louis: Saunders Elsevier, 2006. 9th ed.
- ↑ Wooten, Darcy. “Oesophagostomum.” 5 Feb 2009 <http://www.stanford.edu/class/humbio103/ParaSites2002/oesophagostomiasis/Intro.html>.
- ↑ “GIDEON Infectious Diseases – Diseases.” GIDEON Infectious Disease Database. 5 Feb 2009. <http://web.gideononline.com/web/epidemiology/index.php?gdn_form=ZGlzZWFzZT0xMTY1MA==>.
- ↑ Sun, Tsieh. Parasitic Disorders: Pathology, Diagnosis, and Management. Baltimore: William and Wilkins, 1999. 2nd ed.
- ↑ Ziem, J.B. “Controlling human oesophagostomiasis in northern Ghana.” (Doctoral thesis) Leiden University. 2006. <https://openaccess.leidenuniv.nl/dspace/handle/1887/4917?mode=more>.
- ↑ Ziem, J.B. “Controlling human oesophagostomiasis in northern Ghana.” (Doctoral thesis) Leiden University. 2006.<https://openaccess.leidenuniv.nl/dspace/handle/1887/4917?mode=more>.
- ↑ Ziem, J.B. “Controlling human oesophagostomiasis in northern Ghana.” (Doctoral thesis) Leiden University. 2006. <https://openaccess.leidenuniv.nl/dspace/handle/1887/4917?mode=more>.
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Historical Perspective
The first case of infection by Oesophagostomum spp. was reported in 1905 by Railliet and Henry, describing parasites found in the tumors of the caecum and colon of a male hailing from the Omo river in Southern Ethiopia.[1] In 1910, H. Wolferstan Thomas reported the second known case, describing the macroscopical and microscopical pathology of Oesophagostomum stephanostomum. His descriptions were based on his observations regarding the post mortem of an infected Brazilian man who died from extreme dysentery.[2] In subsequent decades, several more cases of Oesophagostomum spp. infection in humans were found in Brazil, Indonesia, Canada, and several areas of Africa, particularly Northern Ghana, Nigeria and Brazil. Of all reported Oesophagostomum human infections, only O. aculeatum, O. bifurcum and O. stephanostomum have been identified with certainty. The prominent, single-nodule form of oesophagostomiasis is often referred to as Dapaong tumor named after a city in northern Togo. Within the villages of Togo, villagers often refer to it as ‘Kounkoul’, which means ‘turtle’ in the native Moba-language; the name aptly describes the hard, round mass in the patient’s abdomen.[3]
References
- ↑ Polderman, A M et al. “Oesophagostomiasis, a common infection of man in northern Togo and Ghana.” The American Journal of Tropical Medicine and Hygiene 44.3 (1991): 336-44.
- ↑ Thomas, H.W. (1910). The pathological report of a case of oesophagostomiasis in man. Annals of Tropical Medicine and Parasitology. 4: 57-88.
- ↑ Polderman, A. M., and J. Blotkamp. “Oesophagostomum infections in humans.” Parasitology Today 11.12 (1995): 451-456.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Please help WikiDoc by adding more content here. It’s easy! Click here to learn about editing.
Overview
Oesophagostomum is part of the phylum Nematoda. This phylum is composed of five orders: Ascaridida, Enoplida, Oxyurida, Spirurida, Strongylida, and Rhabditida.[1] Strongylida has three superfamilies: Ancyclostomatoidea, Trichostrongyloidea, andStrongylidea. Oesophagostomum lie within the Strongyloidae.[2]
References
- ↑ John, David T., Krotoski, Wojciech A. and Markell, Edward K. Markell and Voge’s Medical Parasitology. St. Louis: Saunders Elsevier, 2006. 9th ed.
- ↑ Wooten, Darcy. “Oesophagostomum.” 5 Feb 2009 <http://www.stanford.edu/class/humbio103/ParaSites2002/oesophagostomiasis/Intro.html>.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
In oesophagostomiasis, larvae can invade the colon wall, potentially causing two pervading types of nodular pathology. Multinodular disease is characterized by the formation of many tiny nodular lesions containing worms and pus along the colon wall. About 15% of patients have this form of oesophagostomiasis.[1]
Pathophysiology
Nodules themselves are usually not a problem, but they can give rise to further complications, such as bowel obstruction, peritonitis and intestinal volvulus. In rare cases serious disease can occur including emaciation, fluid in the pericardium, cardiomegaly, hepatosplenomegaly, perisplenitis, and enlargement of the appendix.
Single-nodular disease, more commonly known as Dapaong disease, is characterized by the development of a single mass that develops throughout the colon wall. This is the most common form of oesophagostomiasis, affecting 85% of patients.[2] This nodule can instigate intense tissue reactions that result in the formation of painful projecting masses.
Life Cycle

For non-human hosts, the life cycle of Oesophagostomum begins with the passing of eggs in the animal feces. From there the eggs develop into stage one larvae. These larvae then spend 6–7 days in the environment developing into stage two and then infectious stage three larvae.[3] Infection begins with the ingestion of soil contaminated with stage three larvae. After ingestion the larvae end up in the small intestine, unsheathing and penetrating the intestinal wall to form nodules. The resulting adult worms that remain in the intestinal lumen copulate; the eggs from the female are then deposited in the feces. Females usually lay around 5,000 eggs per day, which is on par with reproductive rates of other nematodes within Strongyloidea.[4]
For human hosts, the life cycle is very similar to that of Oesophagostomum in animals. It begins when an animal reservoir defecates into the soil, leaving feces infested with eggs that develop into rhabitiform larvae.[5] These larve then develop into stage two and then infectious stage three larvae in the environment over the course of 6–7 days. Human infection occurs when soil or water containing the third-stage larvae is ingested, presumably via contaminated meat obtained from infected livestock or crops with contaminated soil. Once ingested, the filariform larvae migrate to the submucosa of the small or large intestine, then to the lumen of the colon. The developing worms then penetrate the intestinal tissues, causing nodular lesion formation in the intestines and colon; it is in these nodules that the larvae mature to stage four larvae. These larvae may then emerge from their nodules and migrate back to the intestinal lumen, where they mature into adults. But many larvae often do not complete development and remain in their colon nodules, as humans are generally unsuitable hosts for Oesophagostomum. The instances whereOesophagostomum have completed development in humans seem to be dependent on certain environmental and host factors that have yet to be identified.[6]
Microscopic Pathology
Eggs
Eggs of Oesophagostomum bifurcum, the most-common species infecting humans, cannot be differentiated morphologically from the eggs of Necator or Ancylostoma (eggs of other animal oesophagostome species tend to be larger than typical hookworm eggs, however). The eggs of O. bifurcum measure 60-75 µm long by 35-40 µm wide. Eggs are often in a later stage of cleavage than hookworm species when shed in feces.
-
 Egg of Oesophagostomum sp.in an unstained wet mount of stool.
Egg of Oesophagostomum sp.in an unstained wet mount of stool. -
 Egg of Oesophagostomum sp.in an unstained wet mount of stool.
Egg of Oesophagostomum sp.in an unstained wet mount of stool.


Eggs are ovular in shape and range from 50 to 100 micrometres in size; they closely resembles those of hookworms, which renders diagnosis via stool analysis useless in areas co-infected with both Oesophagostomum and hookworm.[7]
Adults
Adult worms of all Oesophagostomum spp. exhibit a cephalic groove by its proximal gut as well as a visible secretory pore, or stomum, at the same level of the oesophagus19. Like other nematodes, Oesophagostomum spp. contain a developed, multi-nucleate digestive tract as well as a reproductive system. Their developed buccal capsule and club-shaped oesophagus are useful for distinguishing Oesophagostomum spp. from hookworms.[8]
Both sexes of adults have a cephalic inflation and an oral opening lined with both internal and external leaf crowns. Female adults, which have a length range of 6.5–24 mm, are generally larger than their male counterparts, with a length range of 6-16.6 mm. Males can be distinguished by their bell-like copulatory bursa, located in the tail, and their paired rodlike spicules.[9]

Adults of Oesophagostomum spp. are bursate nematodes, related to and morphologically-similar to, the hookworms. Females measure 1.5-3.0 cm in length; males are smaller. In both sexes, the anterior end has a cephalic inflation or vesicle, a transverse cephalic groove, and an oral opening guarded by external and internal leaf crowns (corona radiata). The cuticle is ringed with transverse striations. The posterior end of the female is short and pointed; the male possesses a symmetrical bursa and paired, equal spicules. Adults reside in the large intestine of the definitive host.
-
 Adult of Oesophagostomum sp.
Adult of Oesophagostomum sp. -
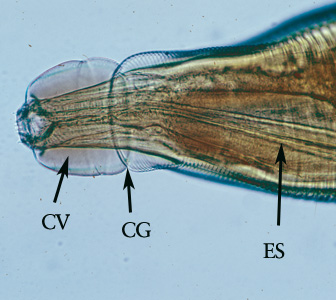 Higher magnification of the anterior end of the specimen. Note the presence of the cephalic vesicle (CV), cephalic groove (CG) and esophagus (ES).
Higher magnification of the anterior end of the specimen. Note the presence of the cephalic vesicle (CV), cephalic groove (CG) and esophagus (ES). -
Higher magnification of the anterior end of the specimen. Note the presence of the cephalic vesicle (CV) and corona radiata (CR).
-
 Posterior end of a female Oesophagostomum sp., showing the pointed tail.
Posterior end of a female Oesophagostomum sp., showing the pointed tail. -
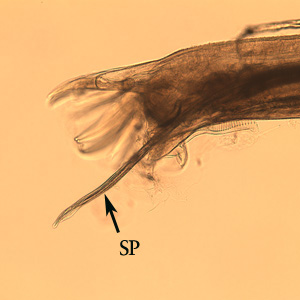 Posterior end of a male Oesophagostomum sp., Note the spicule (SP).
Posterior end of a male Oesophagostomum sp., Note the spicule (SP). -
 Posterior end of a male Oesophagostomum sp., Note the bursa (BU).
Posterior end of a male Oesophagostomum sp., Note the bursa (BU). -
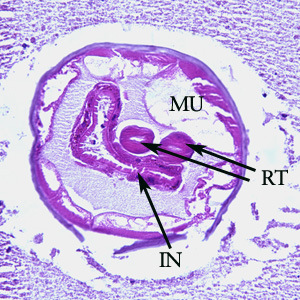 Cross-section of an adult of Oesophagostomum sp. in a colon biopsy specimen from a patient from Africa, stained with hematoxylin and eosin (H&E). Note the large, platymyarian muscle cells (MU), intestine with brush border (IN), paired reproductive tubes (RT). This image is taken at 200x magnification.
Cross-section of an adult of Oesophagostomum sp. in a colon biopsy specimen from a patient from Africa, stained with hematoxylin and eosin (H&E). Note the large, platymyarian muscle cells (MU), intestine with brush border (IN), paired reproductive tubes (RT). This image is taken at 200x magnification. -
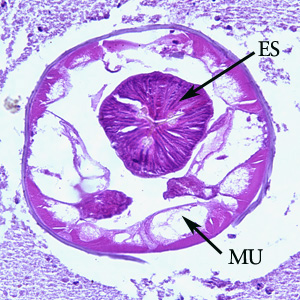 Cross-section of an adult of Oesophagostomum sp. in a colon biopsy specimen from a patient from Africa, stained with hematoxylin and eosin (H&E). Note the large, platymyarian muscle cells (MU) and thick, muscled esophagus (ES). Image taken at 200x magnification.
Cross-section of an adult of Oesophagostomum sp. in a colon biopsy specimen from a patient from Africa, stained with hematoxylin and eosin (H&E). Note the large, platymyarian muscle cells (MU) and thick, muscled esophagus (ES). Image taken at 200x magnification.







References
- ↑ “GIDEON Infectious Diseases – Diseases.” GIDEON Infectious Disease Database. 5 Feb 2009. <http://web.gideononline.com/web/epidemiology/index.php?gdn_form=ZGlzZWFzZT0xMTY1MA==>.
- ↑ “GIDEON Infectious Diseases – Diseases.” GIDEON Infectious Disease Database. 5 Feb 2009.<http://web.gideononline.com/web/epidemiology/index.php?gdn_form=ZGlzZWFzZT0xMTY1MA==>.
- ↑ Ziem, J.B. “Controlling human oesophagostomiasis in northern Ghana.” (Doctoral thesis) Leiden University. 2006. <https://openaccess.leidenuniv.nl/dspace/handle/1887/4917?mode=more>.
- ↑ Krepel, H P, and A M Polderman. “Egg production of Oesophagostomum bifurcum, a locally common parasite of humans in Togo.” The American Journal of Tropical Medicine and Hygiene 46.4 (1992): 469-72.
- ↑ Ziem, J.B. “Controlling human oesophagostomiasis in northern Ghana.” (Doctoral thesis) Leiden University. 2006.<https://openaccess.leidenuniv.nl/dspace/handle/1887/4917?mode=more>.
- ↑ Ziem, J.B. et al. “Impact of repeated mass treatment on human Oesophagostomum and hookworm infections in northern Ghana.” Tropical Medicine & International Health: TM & IH 11.11 (2006): 1764-72.
- ↑ Ziem, J.B. “Controlling human oesophagostomiasis in northern Ghana.” (Doctoral thesis) Leiden University. 2006.<https://openaccess.leidenuniv.nl/dspace/handle/1887/4917?mode=more>.
- ↑ Elmes, B et al. (1953). Helminthic abscess, a surgical complication of oesophagostomes and hookworms. Annals of Tropical Medicine and Parasitology. 48: 1-7.
- ↑ Ziem, J.B. “Controlling human oesophagostomiasis in northern Ghana.” (Doctoral thesis) Leiden University. 2006. <https://openaccess.leidenuniv.nl/dspace/handle/1887/4917?mode=more>.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Please help WikiDoc by adding content here. It’s easy! Click here to learn about editing.
References
Differentiating Oesophagostomum from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Please help WikiDoc by adding more content here. It’s easy! Click here to learn about editing.
Overview
Oesophagostomum needs to be differentiated from common misdiagnosis which include carcinoma, appendicitis, amebiasis, and tuberculosis.[1]
References
- ↑ Sun, Tsieh. Parasitic Disorders: Pathology, Diagnosis, and Management. Baltimore: William and Wilkins, 1999. 2nd ed.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Epidemiology and Demographics
Age
Prevalence is higher in children between ages 2-10. These age demographics are not yet sufficiently explained; possible factors include differential exposure to contaminated water and strength of immune response.
Gender
Females older than 5 years of ages have higher prevalence than males within the age group of 2-10. These gender discrepancies are not yet sufficiently explained; possible factors include differential exposure to contaminated water and strength of immune response.
Developing Countries
Oesophagostomiasis is endemic or potentially endemic to 35 countries; approximately 250,000 are infected worldwide, with 1 million more at risk according to the Gideon Infectious Diseases Database. Most of the cases originate in Africa, specifically in Ghana, Togo, Uganda, Nigeria, Zimbabwe, and other nearby countries. A few sporadic cases have been reported in countries in South America and Southeast Asia, including Brazil, Indonesia and Malaysia.[1] The vast majority of clinical cases have been collected from northern Togo and Ghana, in West Africa. 156 cases from the areas alone were collected in a 2000 study; before then, only 116 cases were recorded in the literature.[2] O. bifurcum infection in northern Togo and Ghana is found in virtually every village, with some rural areas exhibiting prevalence of as much as 90,000 per 100,000 population. A study done by Krepel in 1992 revealed a correlation between infection with O. bifurcum and N. americanus in that individuals living in endemic villages were either coinfected with both parasites or neither. This could be due to cofactors shared by both parasites, including poor hygiene, certain agricultural practices and the dearth of potable water suitable for consumption.
Below is a review of some epidemiological studies on the epidemiology of Oesophagostomum bifurcum in northern Togo and Ghana:
- “Human Oesophagostomum infection in northern Togo and Ghana: epidemiological aspects.” By: Krepel et al. Annals of Tropical Medicine and Parasitology.1992. 86:289-300.
A regional survey of O. bifurcum infection was carried out in Togo and Ghana. The parasite was found in 38 of the 43 villages surveyed, with the highest prevalence rates reaching 59% in some small, isolated villages. Infection was found to be positively correlated with hookworm infection; however, the difficulty in distinguishing these parasites may have had some confounding effect. Infection rates were low in children under 3 years of age, beyond that, rates of infection increased dramatically until 10 years of age. Interestingly, females showed higher prevalence of infection (34%)than men (24%). Based on these epidemiological studies, this group was ale to conclude that tribe, profession, or religion had no effect on the prevalence of infection in the different communities surveyed. The habitats and life cycle of this parasite do not explain its distribution.[3]
- “Clinical epidemiology and classification of human oesophagostomiasis.” By: P.A. Storey et al. Trans R Soc Trop Med Hyg. 2000. 94:177-182.
The study investigated the clinical epidemiology of oesophagostomiasis by observing 156 cases in the Nalerigu hospital between 1996-1998. About 1 patient/week presented with this disease over the course of two years and 1% of all surgeries carried out were related to oesophagostomiasis. 13% of the patients presented with the multinodular form of the disease in which they had several nodules in their small intestine, abdominal pain, diarrhea, and weight loss. The other 87% of the patients presented with the Dapaong, or single, tumor form of the disease that was associated with inflammation in the abdomen, fever, and pain.[4]
References
- ↑ “GIDEON Infectious Diseases – Diseases.” GIDEON Infectious Disease Database. 5 Feb 2009. <http://web.gideononline.com/web/epidemiology/index.php?gdn_form=ZGlzZWFzZT0xMTY1MA==>.
- ↑ “GIDEON Infectious Diseases – Diseases.” GIDEON Infectious Disease Database. 5 Feb 2009. <http://web.gideononline.com/web/epidemiology/index.php?gdn_form=ZGlzZWFzZT0xMTY1MA==>.
- ↑ “Human Oesophagostomum infection in northern Togo and Ghana: epidemiological aspects.” By: Krepel et al. Annals of Tropical Medicine and Parasitology.1992. 86:289-300.
- ↑ “Clinical epidemiology and classification of human oesophagostomiasis.” By: P.A. Storey et al. Trans R Soc Trop Med Hyg. 2000. 94:177-182.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Please help WikiDoc by adding more content here. It’s easy! Click here to learn about editing.
Natural History
Transmission
Transmission of Oesophagostomum is believed to be oral-fecal for both humans and animals, largely because percutaneous infection with Oesophagostomum has never been reported.[1] It is unclear whether or not parasite transmission is specifically waterborne, foodborne, or both. Regardless, introduction of the stage three infective larvae is necessary for human infection. Much about the biological mechanism of transmission is still unknown, and current knowledge of oral-fecal transmission mechanisms does not explain why Oesophagostomum are mostly localized to Northern Togo and Ghana. It is possible that there are behavioral factors or unique soil conditions that facilitate larval development and are not found outside the current endemic areas.[2] Oesophagostomiasis is generally classified as a zoonotic disease, which is an infectious disease that can be transmitted between animals and humans. This has been called into question recently, as recent research has found that human-to-human transmission is possible.
Reservoir
Oesophagostomum are carried predominantly by non-humans, infecting cattle, sheep, goats, wild pigs, and primates. Humans are largely presumed to be an accidental host, as they are not suitable for completion of the Oesophagostomum development; however, the extreme localization of oesophagostomiasis to northern Togo and Ghana in Africa suggests the possibility that the Oesophagostomum is increasingly exhibiting preference for human hosts.[3]
Until recently it was believed that primates were the main reservoirs of human-infecting Oesophagostomum in northern Togo and Ghana, as these particular species have a considerable concentration in non-human primate reservoirs. A 2005 study done by van Lieshout and de Grujiter found that O. bifurcum in humans from northern Ghana is distinct from the O. bifurcum found in olive baboons and mona monkeys outside the endemic area. They used species-specific PCR and microscopy to establish the identification of two separate species of O. bifurcum. [4] These results are significant, as they necessitate further research to determine the definitive reservoirs of human-infecting O. bifurcum. Oesophagostomiasis has no vector.[5]
Incubation Period
The life-cycle of Oesophagostomum can usually be completed in less than 60 days.[6] When the eggs are passed into the feces to the outside environment, they hatch into stage one larve. The stage two larve then molt twice, developing into infective stage three larva in 6–7 days. These stage three larvae can survive extended periods of desiccation by shrinking within their sheaths.
References
- ↑ Ziem, J.B. “Controlling human oesophagostomiasis in northern Ghana.” (Doctoral thesis) Leiden University. 2006.<https://openaccess.leidenuniv.nl/dspace/handle/1887/4917?mode=more>.
- ↑ Ziem, J.B. “Controlling human oesophagostomiasis in northern Ghana.” (Doctoral thesis) Leiden University. 2006. <https://openaccess.leidenuniv.nl/dspace/handle/1887/4917?mode=more>.
- ↑ Gasser, R B, J M de Gruijter, and A M Polderman. “Insights into the epidemiology and genetic make-up of Oesophagostomum bifurcum from human and non-human primates using molecular tools.” Parasitology 132.Pt 4 (2006): 453-60.
- ↑ van Lieshout, Lisette et al. “Oesophagostomum bifurcum in non-human primates is not a potential reservoir for human infection in Ghana.” Tropical Medicine & International Health: TM & IH 10.12 (2005): 1315-20.
- ↑ “GIDEON Infectious Diseases – Diseases.” GIDEON Infectious Disease Database. 5 Feb 2009.<http://web.gideononline.com/web/epidemiology/index.php?gdn_form=ZGlzZWFzZT0xMTY1MA==>.
- ↑ Ziem, J.B. “Controlling human oesophagostomiasis in northern Ghana.” (Doctoral thesis) Leiden University. 2006. <https://openaccess.leidenuniv.nl/dspace/handle/1887/4917?mode=more>.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Echocardiography or Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH