
Tuberculosis
For patient information, click here.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mashal Awais, M.D.[2]; Mohamed Riad, M.D.[3]; Maheep Singh Sangha, M.B.B.S.; Somal Khan; João André Alves Silva, M.D. [4]; Alejandro Lemor, M.D. [5]; Ammu Susheela, M.D. [6]; Tarek Nafee, M.D. [7]; Sara Mehrsefat, M.D. [8]; Marjan Khan M.B.B.S.[9]; Zaida Obeidat, M.D. Synonyms and keywords: TB, Tb, tb
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Alejandro Lemor, M.D. [2]; João André Alves Silva, M.D. [3]; Ammu Susheela, M.D. [4]
Overview
Tuberculosis (abbreviated as TB or Tuberculosis) is a common infectious disease caused by Mycobacterium tuberculosis. Tuberculosis most commonly involves the lungs as the organism thrives in high oxygen environments, but it can also cause disease in the central nervous system, the lymphatic system, the circulatory system, the genitourinary system, bones, joints and even the skin. Over one-third of the world’s population has been exposed to M. tuberculosis, and new infections occur at a rate of one per second. Not all individuals exposed to the bacterium develop clinically overt tuberculosis infection; in fact, asymptomatic, latent TB infection discovered by screening is more common. Approximately, one in ten latent infections progresses to active (symptomatic) TB disease, which, if left untreated, carries mortality rates of up to 50%. Symptoms include shortness of breath, hemoptysis, fever, chills, night sweats, and weight loss. Several treatment regimens are available for the latent and active forms of TB. Classically, a prolonged course of 6-9 months of a single agent (rifampin or isoniazid) is administered to patients with latent TB, while a more aggressive course that consists of 4 major anti-tuberculous agents (rifampin, isoniazid, ethambutol, pyrazinamide) is reserved for patients with active disease.
Historical Perspective
- Tuberculosis has been present in humans for thousands of years.
- The earliest unambiguous detection of Mycobacterium tuberculosis was in the remains of bison, dated 18,000 BC.
- Tuberculosis originated in cattle and then transferred to humans, or diverged from a common ancestor.
- Tuberculosis has had many names including phthisis and Wasting disease.
- Some hypotheses demonstrate that the origin of the genus, Mycobacterium tuberculosis, was more than 150 million years ago.
- TB with its different names and presentations throughout its history was detected on skeletal deformities of Ancient Egyptian mummies, dating back to 2400 BC.
- The first written record of TB, found in India and China, dated back to 3300 and 2300 years ago.
- In the Middle Ages as well as during the Renaissance, TB was referenced to as the “King’s Evil”.
- During this period if time, the contagious nature, pathology and anatomical afflictions were described.
- An English physician named Benjamin Marten, supposed the anticipated origins for this disease by 1720.
- Years later, there were a number of proposed cures but the most significant milestone in the fight against TB was achieved by renowned scientist, Robert Koch.
- Robert Koch discovered the Mycobacterium tuberculosis in 1882.
- In the 19th and early 20th centuries, tuberculosis caused the most widespread public concern, being considered an endemic disease of the urban poor.
- An effective therapy became possible with the development of the antibiotic streptomycin in 1946.
- The drug-resistant strains began to increase in the 1980s.
Classification
- According to exposure, clinical symptoms, and adjunct diagnostic testing tuberculosis is classified into 6 main classes .
- The classification ranges from Class 0, in people without previous exposure to TB and negative tuberculin skin testing and/or interferon-gamma release assays (2 methods of screening for TB), to Class 3 for active TB and Class 5 for suspected TB based on signs and symptoms of the disease.
- The U.S. Citizenship and Immigration Services also made a special classification for immigrants and refugees according to the risk of infection.
TB Classification System
- As per CDC (Centers of Disease Control and Prevention), the clinical classification system for TB used in the United States is based on the pathogenesis of the disease.
- This classification system provides clinicians the opportunity to keep an eye on the development of TB in their patients.
- Health care providers should follow with state and local laws and regulations requiring the reporting of TB disease.
- All persons with Class 3 or Class 5 TB should be reported directly to the local or state health department.
- A patient should not have a Class 5 classification for more than 3 months.
| Class | Type | Description |
|---|---|---|
| 0 | *No TB exposure *Not infected |
*No history of TB exposure and no evidence of M. tuberculosis infection or disease *Negative reaction to TST or IGRA |
| 1 | *TB exposure *No evidence of infection |
*History of exposure to M. tuberculosis *Negative reaction to TST (Tuberculin skin tests) or IGRA (an interferon gamma release assay blood test) (given at least 8 to 10 weeks after exposure) |
| 2 | *TB infection *No TB disease |
*Positive reaction to TST or IGRA *Negative bacteriological studies (smear and cultures) *No bacteriological or radiographic evidence of active TB disease |
| 3 | *TB clinically active | *Positive culture for M. tuberculosis OR *Positive reaction to TST or IGRA, plus clinical, bacteriological, or radiographic evidence of current active TB |
| 4 | *Previous TB disease (not clinically active) | *May have past medical history of TB disease *Abnormal but stable radiographic findings *Positive reaction to the TST or IGRA *Negative bacteriologic studies (smear and cultures) *No clinical or radiographic evidence of current active TB disease |
| 5 | *TB suspected | *Signs and symptoms of active TB disease, but medical evaluation not complete |
Pathophysiology
- Tuberculosis is a granulomatous infection that is chiefly transmitted through droplets.
- The granuloma encloses mycobacteria and prevents their spreading and facilitates immune immune cell communication.
- Within the granuloma, T lymphocytes (CD4) releases cytokines, such as interferon gamma, that activates local macrophages.
- It is asymptomatic in 90% of immunocompetent individuals.
- In symptomatic patients, it can present as pulmonary or extrapulmonary manifestations. The primary infection may turn into disseminated infection.
- Tuberculosis usually has an impact the progression of HIV if present together. Depending on the age of the patient, tuberculosis may have different clinical manifestations, progression, and prognosis.
Causes
- Mycobacterium tuberculosis is the bacterium responsible for tuberculosis.
- It is an aerobic, non-encapsulated, non-motile, acid-fast bacillus.
- M. tuberculosis is one of the Mycobacterium tuberculosis complex, which also includes bacteria, such as M. bovis and M. africanum.
- The bacterium has a very slow rate of replication, and its genetic variations account for the geographical distribution of different strains, and are involved in drug resistance.
- M. tuberculosis has tropism for different kinds of human cells, with preference for cells of the lung.
- It may infect different species, but human beings are its frequent natural reservoir.
Epidemiology and Demographics
- In 2015, about 10.4 million people developed symptomatic TB and 1.8 million died from the disease.
- There were 9,421 reported cases in the United States in 2014 with an incidence of 3.0 per 100,000 persons.
- Since 1990, the mortality rate was steadily decreasing.
- The prevalence of TB increases with age and it is higher in older men. TB is more prevalent in racial and ethnic minorities than non-Hispanic whites.
- TB is an major cause of death in people coinfected with HIV.
- A third of deaths among these patients is due to TB.
- In 2015, 60% of TB cases worldwide occurred in 6 countries: South Africa, Indonesia, Nigeria, Pakistan, India, and China.
- The WHO has identified 24 other high-burden TB countries including Bangladesh, Congo, Columbia, Lesotho, Cambodia, Korea, Brazil, Ethiopia, Myanmar, Mozambique, Thailand, Angola, Zambia, Vietnam, Kenya, Central Africa, Russia, Liberia, Tanzania, Zimbabwe, Namibia, Philippines, Sierra Leone, Papua New Guinea.
Risk Factors
- The risk factors for the development of tuberculosis include:
- weakened immune system (patients taking immunosuppressive medication or with immunosuppressive diseases, such as HIV or diabetes
- History of contact with infected patients
- Bad hygiene conditions
- Evidence of previous tuberculosis.
- Risk factors for multidrug-resistant TB include:
- Non-adherence to the treatment regimen
- Insufficient medication for that strain of bacteria
- Contact with patients with multidrug-resistant TB.
Screening
- Screening for tuberculosis is generally done by using a mantoux tuberculin skin test, also known as a tuberculin skin test or a PPD.
- The test involves injecting a small amount of a purified protein derivative of the tuberculosis bacterium intradermally and watching for a reaction in the following days.
Natural history, complications and prognosis
- Tuberculosis has been classified as a primary or secondary (post-primary) infection.
- It can have pulmonary and extra pulmonary manifestations as well as severe parenchymal, vascular, pleural, and chest wall complications.
- Pulmonary complications include pleural effusions, cavitations, lymphadenopathy, airway obstruction, pneumonia and bronchiectasis.
- The hematogenous dissemination of infection can lead to miliary tuberculosis.
- The post-primary infection can be due to a recent infection or reactivation of an old infection. Without treatment, 1/3 of patients with active tuberculosis dies within 1 year of the diagnosis, and more than 50% during the first 5 years.
- But with early diagnosis and treatment, it has a good prognosis.
Diagnosis
History and Symptoms
- The general symptoms of tuberculosis include weakness, weight loss, fever, and night sweats.
- Symptoms of pulmonary tuberculosis include cough, chest pain, and hemoptysis.
- Tuberculosis is particularly difficult to diagnose in children, as these may not present with common findings.
Physical Examination
- A physical examination can give an overview about the general condition and other factors that may influence the tuberculosis response to treatment, such as HIV infection or other diseases.
- The most common physical findings include fever, decreased breath sounds, tachypnea and tachycardia.
- Physical findings will depend on the location of the tuberculosis infection.
Laboratory findings
- Routine laboratory exams are usually in the normal ranges.
- The presence of acid-fast-bacilli (AFB) on a sputum smear or another specimen often indicates TB disease and a positive culture for M. tuberculosis confirms the diagnosis.
- Other laboratory tests include peritoneal fluid or CSF analysis, urinalysis, and Interferon–Gamma release assays.
Electrocardiogram
- Echocardiography or Ultrasound can be helpful in patients who develop pericardial effusion secondary to TB. In rare occasions TB may lead to congestive heart failure, in which case echocardiograph may also help in the diagnosis.
- Common findings in CHF on the echocardiogram include: hypokinesia; valvular insufficiency; and enlargement of all heart chambers.
Chest X-Ray
- A chest X-ray is one of the important diagnostic tools in tuberculosis.
- A chest radiograph may be used to rule out the possibility of pulmonary TB in a person who are symptomatic or had a positive reaction to a tuberculin test or QFT-G and no symptoms of the disease.
- The findings on chest x-ray can be divided into parenchymal and pleural.
- The early parenchymal findings can be infiltrated, and cavity.
- A healed tuberculotic lesion can present as fibrosis, and calcification.
- Pleural lesions in form of pleural effusion can also be seen.
- An advanced tuberculosis lesion can present a combination of these early lesions and termed fibrocavitary lesions.
CT
- The majority of patients with pulmonary tuberculosis will have abnormal findings in a chest CT, which include micronodules, interlobular septal thickening, cavitation and consolidation.
- CT scan is more sensitive than an X-ray to detect lymphadenopathies.
MRI
- MRI is used for the assessment of extrapulmonary tuberculosis, such as CNS tuberculosis, Pott’s disease, and parotid gland tuberculosis.
Echocardiography or Ultrasound
- Echocardiography or Ultrasound can be helpful in patients who develop pericardial effusion secondary to TB.
- In rare occasions TB may lead to congestive heart failure, in which case echocardiograph may also help in the diagnosis.
- Common findings in CHF on the echocardiogram include: hypokinesia; valvular insufficiency; and enlargement of all heart chambers.
Other Imaging findings
- The abreugraphy is a smaller variant of the chest X-ray that allows the identification of lung abnormalities that may suggest the diagnosis of TB.
- With the decrease of incidence of TB, the abreugraphy is no longer recommended in most countries for low-risk populations.
- However, depending on the screening resources of each country, it may be used for the screening of high-risk groups, such as HIV-positive patients and alcoholics.
Other Diagnostic Studies
- Because of difficulties with the Tuberculin skin test, many laboratory methods of diagnosis are emerging.
Treatment
Medical Therapy
- If there is a high probability of infection, presumptively treat the patient even if the stain is negative, while waiting for the culture results.
- The patient should be brought back in a few weeks.
- Patients usually feel better a few weeks post-treatment.
- Patients must be monitored for adverse effects and treatment failure.
- In the U.S., all TB is tested for drug resistance.
Special conditions
- Medical therapy for tuberculosis in special conditions include HIV co-infection and extra pulmonary manifestations.
- Different approaches are taken for patients taking ART and those who do not take ART.
- Although WHO recommends the same drug regimen for pulmonary and extrapulmonary manifestations, various stages of skeletal tuberculosis are managed differently.
- For patients with renal or liver diseases, the first line of drugs are substituted with second-line drugs to prevent complications.
Drug-resistant
- Drug-resistant tuberculosis is caused by M. tuberculosis organisms that are resistant to at least one first-line anti-TB drug.
- Multidrug-resistant TB (MDR TB) is resistant to more than one anti-TB drug and at least isoniazid (INH) and rifampin (RIF).
- Treatment should be started with an empirical treatment of at least 4 drugs based on expert advice as soon as drug-resistant TB disease is suspected.
Children
- Tuberculosis in children aged 15 years or younger is a public health problem of special significance because it is a marker for recent transmission of TB. *Infants and young children are more likely to develop life-threatening forms of tuberculosis, such as miliary TB or TB meningitis.
- Screening in children is very important, as the clinical manifestations are usually poor or non-specific.
- History of close contact with tuberculosis patients has an important role in the diagnosis of TB in children.
- The treatment is similar to adults, with adjusted dosing according to the child’s weight.
Surgery
- Surgery may be necessary, especially to drain abscesses , empyema, venticular shunt in tubercular meningitis, surgical resection of tissues affected in abdominal tuberculosis, stabilize the spine in case of Pott’s disease, lobectomy, pneumonectomy, pericardiocentesis or surgical repair of pericardium.
Primary Prevention
- Primary prevention in tuberculosis is targeted to avoid disease transmission and infection of healthy individuals. The BCG vaccine is used in children susceptible to TB infections, such as children living in endemic areas or having close contact with a confirmed case of TB.
- Several preventive measures are used to avoid the transmission of the mycobacteria, such as respiratory isolation, use of respiratory masks among health-care professionals, and advising respiratory hygiene and cough etiquette.
Secondary Prevention
- Secondary prevention for tuberculosis includes methods for screening and early diagnosis, such as tuberculin skin test (TST) and IGRAs; and to guarantee the correct treatment regimen at the right time to prevent disease progression.
Cost effectiveness of therapy
- Treatment of tuberculosis must be analyzed for relative cost effectiveness of inpatient and outpatient models of care as it will benefit regions where tuberculosis is highly prevalent.
- Unless there is severe complications it is highly recommended to treat the TB patient in ambulatory care rather than inpatient services.
Future or investigational therapy
- Since new drug-resistant tuberculosis has been emerging, the role of future therapies is vital in curbing outbreaks.
- The new drugs should be more effective than the current regimen and a few drugs in clinical trials have been showing good results.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mashal Awais, M.D.[2]; João André Alves Silva, M.D. [3]
Overview
Tuberculosis has been detected for a long time. The earliest unambiguous detection of Mycobacterium tuberculosis was in the remains of bison, dated 18,000 BC.[1] However, whether tuberculosis originated in cattle and then transferred to humans, or diverged from a common ancestor, is unclear.[2] Through history tuberculosis has had many names including phthisis and Wasting disease, which were mostly derived from its symptoms. Robert Koch identified the Mycobacterium tuberculosis 1882. In the 19th and early 20th centuries, tuberculosis was considered an endemic disease of the urban poor and a public healthcare issue. In 1946, the development of the antibiotic streptomycin made the cure possible. In the 1980s, the drug-resistant strains appeared increasingly eliminating the hope of cure.
Historical Perspective

TB was present in prehistoric humans and the evidence of infection was found in the skeletal remains 4000 BC, in addition to the spines of mummies showing tubercular decay from 3000-2400 BC.[4] Phthisis is a Greek term for tuberculosis; around 460 BC. In terms of Hippocrates point of view, phthisis was the most widespread disease of the time involving fever and coughing up blood, which was almost always fatal.[5] TB was present in South America for about 2,000 years evidenced by some genetic studies.[6] In South America, the earliest evidence of tuberculosis was linked to the Paracas-Caverna culture (circa 750 BC to circa 100 AD).[7]
Egyptian mummies, that dates back to 2400 BC, showed skeletal deformities characteristic of tuberculosis of spine (Pott’s lesions) and those findings were documented clearly in early Egyptian art.[8]
In the Ancient Greece TB was identified and named Phtisis. Hippocrates recognized it as a fatal disease especially for young adults. Isocrates was the first to suggest that TB is considered an infectious disease, while Aristotle suggested its contagious in oxes and pigs.[9]
Along time ago, Since tuberculosis was similar to the idea of consumption of the infected patients with fever, hemoptysis, pallor, and severe wasting, tuberculosis was called consumption. Other names are:[10][11][10][12]
- Phthisis (Greek for consumption)
- Phthisis pulmonalis
- Scrofula (in adults) – TB of the lymphatic system, resulting in swollen cervical lymph nodes
- Tabes mesenterica – TB of the abdomen
- Lupus vulgaris – TB of the skin
- Wasting disease
- White plague – due to paleness of the sufferers
- King’s evil – as people had a false belief that that scrofula would heal by the king’s touch
- Pott’s disease – TB of the spine
- Miliary tuberculosis – also called disseminated TB, occurs when the infection spreads in the blood stream, resulting in lesions in multiple organs with the appearance of millet seeds on x-ray.
Folklore
tuberculosis was sometimes considered as as vampirism before the industrial revolution. When one family member died from it, the other members became infected and died slowly. People had a false belief that this occurs because the first victim drains the life from the other family members. Moreover, people who had TB had symptoms such as red, swollen eyes (which also causes photosensitivity), pale skin and hemoptysis that are similar to what people knew about vampires. This suggested the idea that the only way for the afflicted to replenish this loss of blood was by sucking blood.[13] people also attributed it to being forced, nightly, to attend fairy revels, so that the victim wasted away due to lack of rest.[14] Similarly, but rarely, it was attributed to the victims being ‘hagridden’ – being transformed into horses by witches (hags) to travel to their nightly meetings leading to lack of rest.[14]
In the 19th century. Many people believed TB caused a sensation of euphoria called ”Spes phthisica” or ”hope of the consumptive”. It was believed that artists affected with TB had bursts of creativity with TB progression. It was also believed that TB sufferers were having a final burst of energy just before their death that made women more beautiful and men more creative.[15]
Study and Treatment

In 1020s, Ibn Sina (Avicenna), with his book The Canon of Medicine, was the first physician to identify pulmonary tuberculosis as a contagious disease and suggest that it could spread through contact with soil and water.[16][17] He developed the method of quarantine to reduce the spread of tuberculosis.[18]
Although Dr Richard Morton established that the pulmonary form was associated with ‘tubercles’ in 1689,[19][20] due to the variation of its symptoms, TB was not identified as a single disease until the 1820s and was not named ‘tuberculosis‘ until 1839 by J. L. Schönlein.[21] During the years 1838-1845, Dr. John Croghan, the owner of Mammoth Cave, brought some tuberculosis sufferers into the cave to treat them with the constant temperature and purity of the cave air; however, they died within a year.[22] The first TB sanatorium opened in 1859 in Görbersdorf, Germany (today Sokołowsko, Poland) by Hermann Brehmer.[23]
Hermann Lebert published his project Traite Pratique des Maladies Scrofuleuses et Tuberculeuses in 1849, reporting that the TB or “King’s evil” was a childhood disease that can affect multiple body’s sites such as skin, eyes, ears, joints, and bones, causing ulceration and suppuration.[24]
Robert Koch identified and deascribed the bacillus causing tuberculosis, Mycobacterium tuberculosis, on March 24, 1882 for which He received the Nobel Prize in physiology or medicine in 1905.[25] Koch did not identify that bovine (cattle) and human tuberculosis were the same infection, which delayed considering infected milk as a source of infection. Later on, this source was eliminated by the process of milk pasteurization. Koch identified a glycerine extract of the tubercle bacilli as in 1890, calling it ‘tuberculin’. It was not accurate, but was later adapted as a test for pre-symptomatic tuberculosis.[26]
The first achievement in tuberculosis immunization was ‘BCG’ (Bacillus of Calmette and Guerin) that was developed from attenuated bovine-strain tuberculosis by Albert Calmette and Camille Guerin in 1906. The BCG vaccine was first used on humans in 1921 in France, and after World War II, BCG received approval in the USA, Great Britain, and Germany.
Tuberculosis, or ‘consumption’ was considered an endemic disease of the urban poor and a public healthcare issue. In 1815, one in four deaths in England was of consumption; by 1918 one in six deaths in France were still caused by TB. In the 20th century, the number of deaths due to TB was 100 million people.[27] After the establishment in the 1880s that the disease was contagious, TB was reported as a notifiable disease in Britain.[23]

In the United States, concern about the spread of tuberculosis played a role in the movement to prohibit public spitting except into spittoons.
In Europe, deaths from TB decreased from 500 out of 100,000 in 1850 to 50 out of 100,000 by 1950. public health improvements had an impact regarding decreasing tuberculosis cases even before the development of antibiotics, but the disease was still representing a significant harm to public health.[28]
In 1946, the development of the antibiotic streptomycin made the cure possible. Before the discovery of this drug, the only treatment besides sanatoria were surgical interventions, such as the pneumothorax technique – in the form of collapsing an infected lung to rest it and allow lesions to heal – which was of little benefit and was largely stopped by the 1950s.[29] The emergence of multidrug-resistant TB has again introduced surgery as part of the treatment for these infections. Here, surgical removal of lung cavities will reduce the number of bacteria in the lungs, as well as increase the exposure of the remaining bacteria to drugs in the bloodstream, which is thought to increase the effectiveness of the chemotherapy.[30]
In the 1980s, the drug-resistant strains appeared increasingly eliminating the hope of cure. For example, tuberculosis cases in Britain, numbering around 117,000 in 1913, had fallen to around 5,000 in 1987, but cases increased again, reaching 6,300 in 2000 and 7,600 cases in 2005.[31] As a result of the elimination of public health facilities in New York and the emergence of HIV, there was another TB resurgence in the late 1980s.[32]
References
- ↑ Rothschild B, Martin L, Lev G, Bercovier H, Bar-Gal G, Greenblatt C, Donoghue H, Spigelman M, Brittain D (2001). “Mycobacterium tuberculosis complex DNA from an extinct bison dated 17,000 years before the present”. Clin Infect Dis. 33 (3): 305–11. PMID 11438894.
- ↑ Pearce-Duvet J (2006). “The origin of human pathogens: evaluating the role of agriculture and domestic animals in the evolution of human disease”. Biol Rev Camb Philos Soc. 81 (3): 369–82. PMID 16672105.
- ↑ 3.0 3.1 3.2 “Wikimedia Commons”.
- ↑ Zink A, Sola C, Reischl U, Grabner W, Rastogi N, Wolf H, Nerlich A (2003). “Characterization of Mycobacterium tuberculosis complex DNAs from Egyptian mummies by spoligotyping”. J Clin Microbiol. 41 (1): 359–67. PMID 12517873.
- ↑ Hippocrates. Aphorisms. Accessed 07 October 2006.
- ↑ Konomi N, Lebwohl E, Mowbray K, Tattersall I, Zhang D (2002). “Detection of mycobacterial DNA in Andean mummies”. J Clin Microbiol. 40 (12): 4738–40. PMID 12454182.
- ↑ “South America: Prehistoric Findings”. Memorias do Instituto Oswaldo Cruz, Vol. 98 (Suppl.I) January 2003. Retrieved on 2007-02-08.
- ↑ MORSE D, BROTHWELL DR, UCKO PJ (1964). “TUBERCULOSIS IN ANCIENT EGYPT”. Am Rev Respir Dis. 90: 524–41. doi:10.1164/arrd.1964.90.4.524. PMID 14221665.
- ↑ Barberis I, Bragazzi NL, Galluzzo L, Martini M (2017). “The history of tuberculosis: from the first historical records to the isolation of Koch’s bacillus”. J Prev Med Hyg. 58 (1): E9–E12. PMC 5432783. PMID 28515626.
- ↑ 10.0 10.1 Tuberculosis Encyclopedia Britannica, 11th ed.
- ↑ Rudy’s List of Archaic Medical Terms English Glossary of Archaic Medical Terms, Diseases and Causes of Death. Accessed 09 Oct 06
- ↑ Disseminated tuberculosis NIH Medical Encyclopedia. Accessed 09 Oct 06
- ↑ Sledzik P, Bellantoni N (1994). “Brief communication: bioarcheological and biocultural evidence for the New England vampire folk belief”. Am J Phys Anthropol. 94 (2): 269–74. PMID 8085617.
- ↑ 14.0 14.1 Katharine Briggs, An Encyclopedia of Fairies “Consumption” (Pantheon Books, 1976) p. 80. ISBN 0-394-73467-X
- ↑ Lawlor, Clark. “Transatlantic Consumptions: Disease, Fame and Literary Nationalism in the Davidson Sisters, Southey, and Poe”. Studies in the Literary Imagination, Fall 2003. Available at findarticles.com. Retrieved on 2007-06-08.
- ↑ Y. A. Al-Sharrah (2003), “The Arab Tradition of Medical Education and its Relationship with the European Tradition”, Prospects 33 (4), Springer.
- ↑ George Sarton, Introduction to the History of Science.
(cf. Dr. A. Zahoor and Dr. Z. Haq (1997). Quotations From Famous Historians of Science, Cyberistan.) - ↑ David W. Tschanz, MSPH, PhD (August 2003). “Arab Roots of European Medicine”, Heart Views 4 (2).
- ↑ Who Named It? Léon Charles Albert Calmette. Retrieved on 6 October 2006.
- ↑ Trail R (1970). “Richard Morton (1637–1698)”. Med Hist. 14 (2): 166–74. PMID 4914685.
- ↑ Zur Pathogenie der Impetigines. Auszug aus einer brieflichen Mitteilung an den Herausgeber. [Müller’s] Archiv für Anatomie, Physiologie und wissenschaftliche Medicin. 1839, page 82.
- ↑ Kentucky: Mammoth Cave long on history. CNN. 27 February 2004. Accessed 08 October 2006.
- ↑ 23.0 23.1 McCarthy OR (2001). “The key to the sanatoria”. J R Soc Med. 94 (8): 413–7. PMID 11461990.
- ↑ Barberis I, Bragazzi NL, Galluzzo L, Martini M (2017). “The history of tuberculosis: from the first historical records to the isolation of Koch’s bacillus”. J Prev Med Hyg. 58 (1): E9–E12. PMC 5432783. PMID 28515626.
- ↑ Nobel Foundation. The Nobel Prize in Physiology or Medicine 1905. Accessed 07 October 2006.
- ↑ Waddington K (2004). “To stamp out “so terrible a malady”: bovine tuberculosis and tuberculin testing in Britain, 1890–1939″. Med Hist. 48 (1): 29–48. PMID 14968644.
- ↑ Torrey EF and Yolken RH. 2005. Their bugs are worse than their bite. Washington Post, April 3, p. B01.
- ↑ [[Medical Research Council (UK)|]]. MRC’s contribution to Tuberculosis research. Accessed 02 July 2007.
- ↑ Wolfart W (1990). “[Surgical treatment of tuberculosis and its modifications—collapse therapy and resection treatment and their present-day sequelae]”. Offentl Gesundheitswes. 52 (8–9): 506–11. PMID 2146567.
- ↑ Lalloo U, Naidoo R, Ambaram A (2006). “Recent advances in the medical and surgical treatment of multi-drug resistant tuberculosis”. Curr Opin Pulm Med. 12 (3): 179–85. PMID 16582672.
- ↑ “Tuberculosis – Respiratory and Non-respiratory Notifications, England and Wales, 1913-2005”. Health Protection Agency Centre for Infections. 21 March 2007. Retrieved 2007-08-01.
- ↑ Paolo W, Nosanchuk J (2004). “Tuberculosis in New York city: recent lessons and a look ahead”. Lancet Infect Dis. 4 (5): 287–93. PMID 15120345.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mashal Awais, M.D.[2]; João André Alves Silva, M.D. [3]
Overview
Tuberculosis can be classified into 6 main categories according to exposure, symptoms, and diagnostic testing. The classification ranges from Class 0, in people with no previous exposure to TB and negative tuberculin skin testing and/or interferon-gamma release assay (2 methods of screening for TB), to Class 3 for active TB infection and Class 5 for suspected TB infection based on signs and symptoms of the disease. The U.S. Citizenship and Immigration Services has also designed a special classification for immigrants and refugees according to the risk of infection.
Classification
Below is a table of the current classification system of tuberculosis (TB), according to its pathogenesis:[1]
| Class | Type of Tuberculosis | Description |
|---|---|---|
|
0 |
No TB exposure |
|
|
1 |
History of TB exposure | |
|
2 |
Positive TST or IGRA | |
|
3 |
Clinically active TB |
Positive culture (if done) for M. tuberculosis |
|
4 |
Previous TB disease (not clinically active) |
Medical history of TB disease |
|
5 |
Suspected TB |
Clinical manifestations of TB disease, but incomplete evaluation. The diagnosis s pending. The patient should not be in this class for more than three months. |
CDC TB Classification for Immigrants and Refugees
Based on the U.S. Citizenship and Immigration Services, developed by the Centers for Disease Control and Prevention (CDC), tuberculosis for immigrants and refugees s classified into the following categories: [2]
| Class | Description | Travel Clearance |
|---|---|---|
|
No TB Classification |
Applicants with normal tuberculosis screening examinations. No discernible HIV infection and normal CXR. |
Valid for 6 months from evaluation |
|
Class A TB |
All applicants who have tuberculosis disease including applicants with extrapulmonary TB. In addition, CXR indicates pulmonary TB disease, regardless of sputum smear and culture results. |
Not cleared for travel until treatment is completed. Exceptions are available for granted waivers. |
| Class B0 TB, Pulmonary | Applicants who were previously diagnosed with TB or came to the physician during the TB treatment course. Additionally, successful completion of the Division of Global Migration and Quarantine (DGMQ) prior to immigration is required. | It can be valid for 3 months from the last negative culture results. |
|
No treatment:
Completed treatment:
|
It can be valid for 3 months from the last negative culture results. | |
|
Class B1 TB, Extrapulmonary |
Applicants with evidence of extrapulmonary tuberculosis, with normal CXR and negative sputum smears and cultures. |
It can be Valid for 3 months from the last negative culture results. |
|
Class B2 TB, LTBI Evaluation |
Applicants who have a TST ≥10 mm or positive IGRA but otherwise tuberculosis evaluation is negative |
Valid for 6 months from completion of evaluation. |
|
Class B3 TB, Contact Evaluation |
Applicants who have been in contact of a known tuberculosis case |
Valid for 6 months from completion of the evaluation. |
| Risk Classification | Necessity of testing | Frequency of testing | |
|---|---|---|---|
| Low Risk | Settings where Tb infected individuals are unlikely to be present | Not required unless there has been exposure to TB | |
| Medium Risk | Settings where health care workers (HCWs) are likely to encounter individuals with TB | Testing should be repeated every year | |
| Potential Ongoing Transmission | Settings wehere person to person transmission of TB was documented in the past year | Testing should be repeated every 8 weeks until making sure that there has been no ongoing transmission. |
References
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mashal Awais, M.D.[2], João André Alves Silva, M.D. [3]
Overview
Transmission of M. tuberculosis occurs when individuals with active pulmonary disease cough, speak, sneeze or sing expelling the infectious droplets. The mycobacterium tuberculosis favors the upper lung lobes due to the high oxygen level. Tuberculosis is a prototypical granulomatous infection. The granuloma surrounds the mycobacteria and prevents their dissemination and facilitates the immune cell interaction. Within the granuloma, CD4 T lymphocytes release chemokines that activate local macrophages and recruit other immune cells..
Pathogenesis
Transmission of M. tuberculosis occurs when individuals with active pulmonary disease cough, speak, sneeze or sing expelling the infectious droplets that can pass to the terminal bronchioles and alveoli then phagocytosed by alveolar macrophages where they can replicate in the endosomes of alveolar macrophages. As a part of the immune response by these macrophages, the alveolar macrophages release cytokines that recruits further macrophages, neutrophils, and monocytes, surrounding the bacilli. Despite having a very low infectious dose (ID<200 bacteria), 90% of the infected immunocompetent individuals are asymptomatic. In most cases, the bacteria may either be eliminated or enclosed within a granuloma. The granuloma is a structured, radial aggregation of macrophages, epithelioid cells, T lymphocytes, B lymphocytes, and fibroblasts that prevents the spreading of mycobacteria and enhances interaction of the immune cells.[1] The primary site of infection in the lung is called the Ghon focus that is mainly located in either the upper part of the lower lobe, or the lower part of the upper lobe.[1][2]
Primary Infection
The infected macrophages are transported through the lymphatics to the regional lymph nodes in the immunocompetent individuals. However, with impaired immune response, these macrophages can pass through the bloodstream to enter any part of the body. Those foci of primary infection usually resolve without any consequences, but they can act as a foci of M. tuberculosis dissemination. There are particular organs that are more susceptible to bacterial replication as well as being potential metastatic foci which include:[1][2]
- Apical-posterior regions of the lungs
- Lymph nodes
- Kidneys
- Vertebral bodies
- Extremities of long bones
- Juxta ependymal meningeal regions
Although TB is a systemic disease and all organs can be affected, the heart, pancreas, skeletal muscles and thyroid are rarely involved.[3] In a few cases, when the infectious dose is high and antigens concentration in the primary focus is high, the immune response and hypersensitivity can lead to necrosis and calcification of this lesion, and these primary calcified foci are then called Ranke complex.[1][4]
Progression of the Primary Infection
Primary foci of infection can enter the large pulmonary lymph nodes. These may lead to:[1]
- Bronchial collapse
- atelectasis
- Bronchial erosion, with more dissemination of infection
- In non-caucasian children, elderly patients and HIV/AIDS, the immune response is impaired, consequently the primary focus of infection can deteriorate into progressive primary disease, with advancing pneumonia.
- In addition,the infection may result in cavity formation with transmission of the infection through the bronchi.[1][5][6]
- In young children, the onset of immune response may be delayed after the bacterial dissemination resulting in military tuberculosis. Bacteria can spread directly from the primary focus, or from the Weigart focus (metastatic focus adjacent to a pulmonary vein) through the blood.[1][7]
- In younger patients, rupture of subpleural foci into the pleural space may occur leading to serofibrinous pleurisy.[1] The most serious site of the M. tuberculosis dissemination is the postero-apical regions of the lung where it can replicate hidden from the immune system.[1]
Immunopathogenesis
There are two types of immune response against tuberculosis that include the innate and acquired immune responses. However, the cell-mediated immune response predominates over the humoral type.
Innate Immune Response
Initially, The immune response generated against M. tuberculosis is minimal, enabling it to replicate inside the alveolar macrophages forming the Ghon focus, or metastatic foci. Recognition and phagocytosis of the M. tuberculosis bacilli by the alveolar macrophages occurs through interaction with certain receptors that are located on the surface of macrophages:[8]
- Toll-like Receptor 2 (TLR2)
- TLR4
- TLR9
- Dectin-1
- DC-SIGN
- Mannose receptor
- Complement receptors
- NOD2
Acquired Immunity and Granuloma Formation
- The granuloma control the infection; however, it enables the mycobacterium to survive inside for a long time.
- It is important to maintain a balance between the pro-inflammatory and anti-inflammatory cytokines released to decrease or control the mycobacterial proliferation.
- TNF-α and IFN-γ stimulate granuloma formation. On the other hand, IL-10 is one of the major negative regulators and inhibitors of granuloma formation.
- The granuloma is structured by blood-derived macrophages (derived from monocytes), epithelioid cells (differentiated macrophages), and multinucleated giant cells (also known as Langhans giant cells), surrounded by T lymphocytes.
- Caseous granulomas are the main characteristic of tuberculosis. The caseous granulomas include epithelioid macrophages and some lymphocytes with a necrotic center. Other types of granuloma include non-necrotizing granulomas, that are mainly formed of macrophages and a few lymphocytes, necrotic neutrophilic granulomas, and completely fibrotic granulomas.[9]
- Several chemokines are involved in granuloma formation released either from the respiratory tract epithelium or the immune cells themselves.
- Interaction with CCR2 receptor with (CCL2/MCP-1, CCL12, and CCL13) is necessary for the initial recruitment of macrophages.
- Macrophages and lymphocytes release a chemokine called osteopontin that enhances the adhesion and recruitment of the immune cells.
- CCL19 and CCL21 are important for recruitment of IFN–producing T cells.
- In TNF-deficient mice, absence of these chemokines as a result of inhibition of the expression of the CC and CXC chemokines prevents the recruitment of other macrophages and T lymphocytes. This finding sheds the light on the role of TNF in granuloma formation.[9]

Molecular Pathogenesis
- The mycobacterial antigens are presented on thee surfaces of alveolar macrophages and dendritic cells through class II major histocompatibility complex. These antigens are recognized by CD4 lymphocytes through αβ T-cell receptors. Following that, CD4 lymphocytes release chemokines that recruit more macrophages to the foci of infection.
- Interferon gamma (IFN-γ) and tumor necrosis factor alpha (TNF-α) signaling activates additional macrophages. [10]
- Metalloproteinase converts the transmembrane protein to soluble TNF-α which interacts with the TNFR1 and TNFR2 receptors inducing apoptosis through caspase-dependent pathways
- TNF along side the synergistic action of interferon-gamma enhances the phagocytic activity of the macrophages and facilitates the intracellular killing of mycobacteria by reactive nitrogen and oxygen intermediates.
- Neutralization of the TNF-α activity leads to the mycobacteria survival within the granuloma in latent infection.
- TNF activates release of CCL2, CCL3, CCL4, CCL5, CCL8 chemokines and increases CD54 leading to accumulation of immune cells and it is the main element in the process of granuloma formation and maintenance. [10]
- The immune cells release large amounts of lytic enzymes leading to tissue necrosis.

Once within alveolar macrophages, M. tuberculosis uses multiple mechanisms in order to survive:[1]
- Urease – prevents acidification of macrophageal lysosomes, limiting action of cellular enzymes
- Secretion of antioxidants, for suppression of reactive oxygen species, such as:
Transmission
After contact with a patient having the active TB, and inhalation of the M. tuberculosis, the risk of developing active tuberculosis is low with a life-time risk of about 10%.[12] The probability of transmission between individuals depends on the number of expelled infectious droplets the ventilation, the duration of the exposure, immunity, and the virulence of the M. tuberculosis strain.[13] The probability of transmitting the infection is highest during the first years of getting the infection. After that, it decreases.[14]
In rare occasions, the mycobacteria can be transmitted by other ways apart from the respiratory route in which, the formation of foci in the regional lymph nodes frequently occurs. Those routes include:[1]
Associated Conditions
AIDS
- Tuberculosis influence the progression of HIV replication leading to an increase in in the mortality rate.[15]
- HIV infected patients, particularly those having low CD4 lymphocytes counts, are more likely to develop reactivation of latent tuberculosis. Moreover, when an individual has been recently infected with M. tuberculosis, they progress rapidly into active disease.[1][16][17] The correlation between AIDS and the risk of TB infection is still not fully understood.[1]
Patients with AIDS are more prone to get pulmonary and extrapulmonary tuberculosis. Extrapulmonary disease in AIDS patients has characteristic manifestations, such as:[1]
- Higher risk of progression into disseminated disease[18]
- DIC and acute respiratory failure
- Tuberculous pleuritis occurs bilaterally
- Abdominal and mediastinal lymphadenopathy frequently occurs
- Higher risk of Immune reconstitution inflammatory syndrome (IRIS)[19]
- Common abscesses of:[1]
Gallery
-
![Left lateral margin of a tongue of a tuberculosis patient, which had been retracted in order to reveal the lesion that had been caused by the Gram-positive bacterium Mycobacterium tuberculosisAdapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]](https://www.wikidoc.org/images/0/09/TB1.jpg) Left lateral margin of a tongue of a tuberculosis patient, which had been retracted in order to reveal the lesion that had been caused by the Gram-positive bacterium Mycobacterium tuberculosisAdapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]
Left lateral margin of a tongue of a tuberculosis patient, which had been retracted in order to reveal the lesion that had been caused by the Gram-positive bacterium Mycobacterium tuberculosisAdapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20] -
![Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection.[ http://phil.cdc.gov/phil/ Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.][20]](https://www.wikidoc.org/images/e/ed/TB2.jpg) Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection.[ http://phil.cdc.gov/phil/ Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.][20]
Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection.[ http://phil.cdc.gov/phil/ Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.][20] -
![Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]](https://www.wikidoc.org/images/7/79/Leprosy-35.jpg) Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]
Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20] -
![Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]](https://www.wikidoc.org/images/6/60/Leprosy-36.jpg) Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]
Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20] -
![Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]](https://www.wikidoc.org/images/9/93/Leprosy-37.jpg) Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]
Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20] -
![Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]](https://www.wikidoc.org/images/b/b5/Leprosy-38.jpg) Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]
Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20] -
![Photomicrograph describing tuberculosis of the placenta.Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]](https://www.wikidoc.org/images/b/be/TB3.jpg) Photomicrograph describing tuberculosis of the placenta.Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]
Photomicrograph describing tuberculosis of the placenta.Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20] -
![Histopathology of tuberculosis, endometrium. Ziehl-Neelsen stain.Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]](https://www.wikidoc.org/images/d/dd/TB4.jpg) Histopathology of tuberculosis, endometrium. Ziehl-Neelsen stain.Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]
Histopathology of tuberculosis, endometrium. Ziehl-Neelsen stain.Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20] -
![Histopathology of tuberculosis, placenta.Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]](https://www.wikidoc.org/images/9/97/TB5.jpg) Histopathology of tuberculosis, placenta.Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]
Histopathology of tuberculosis, placenta.Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20] -
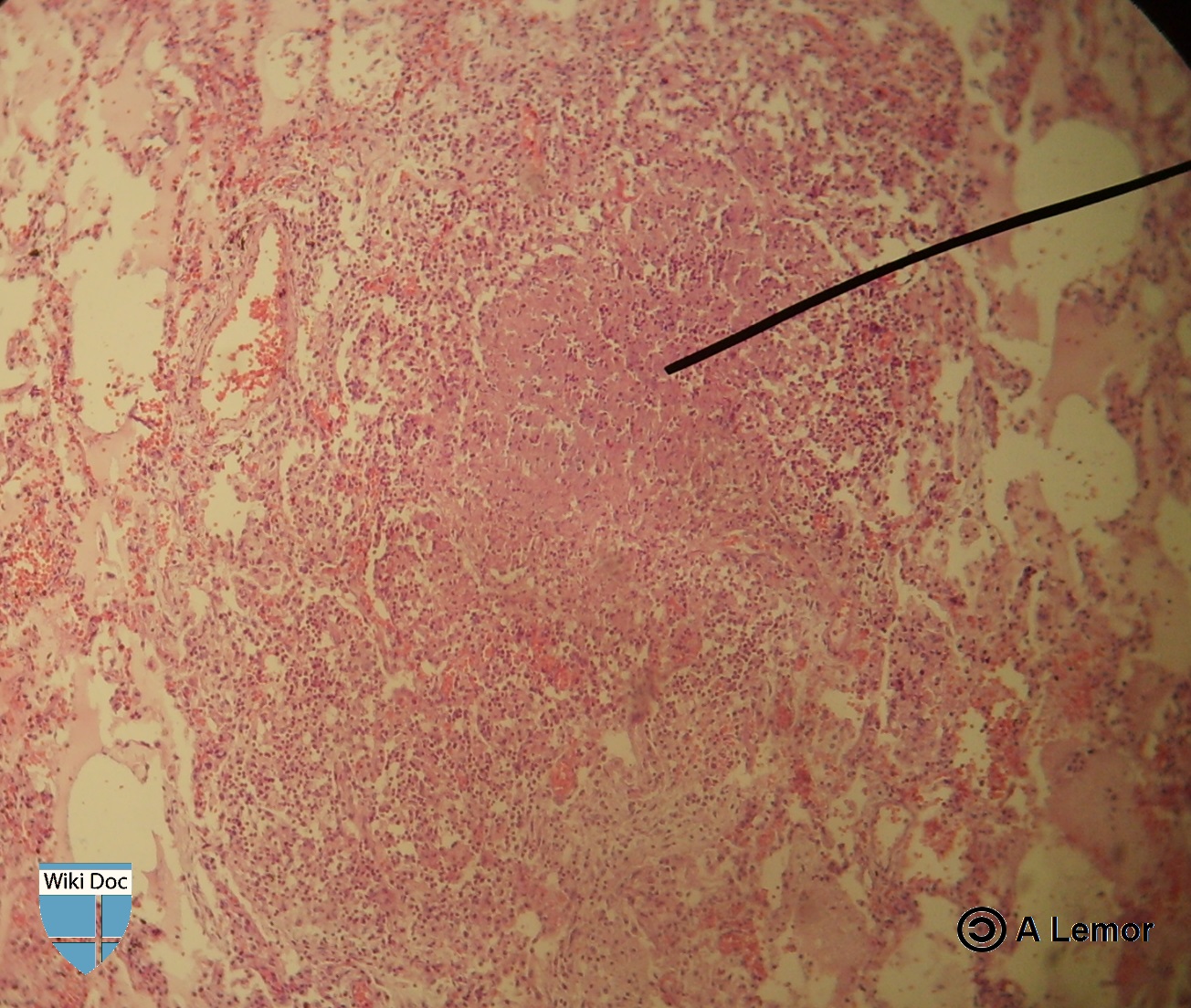 Miliar Tuberculosis
Miliar Tuberculosis -
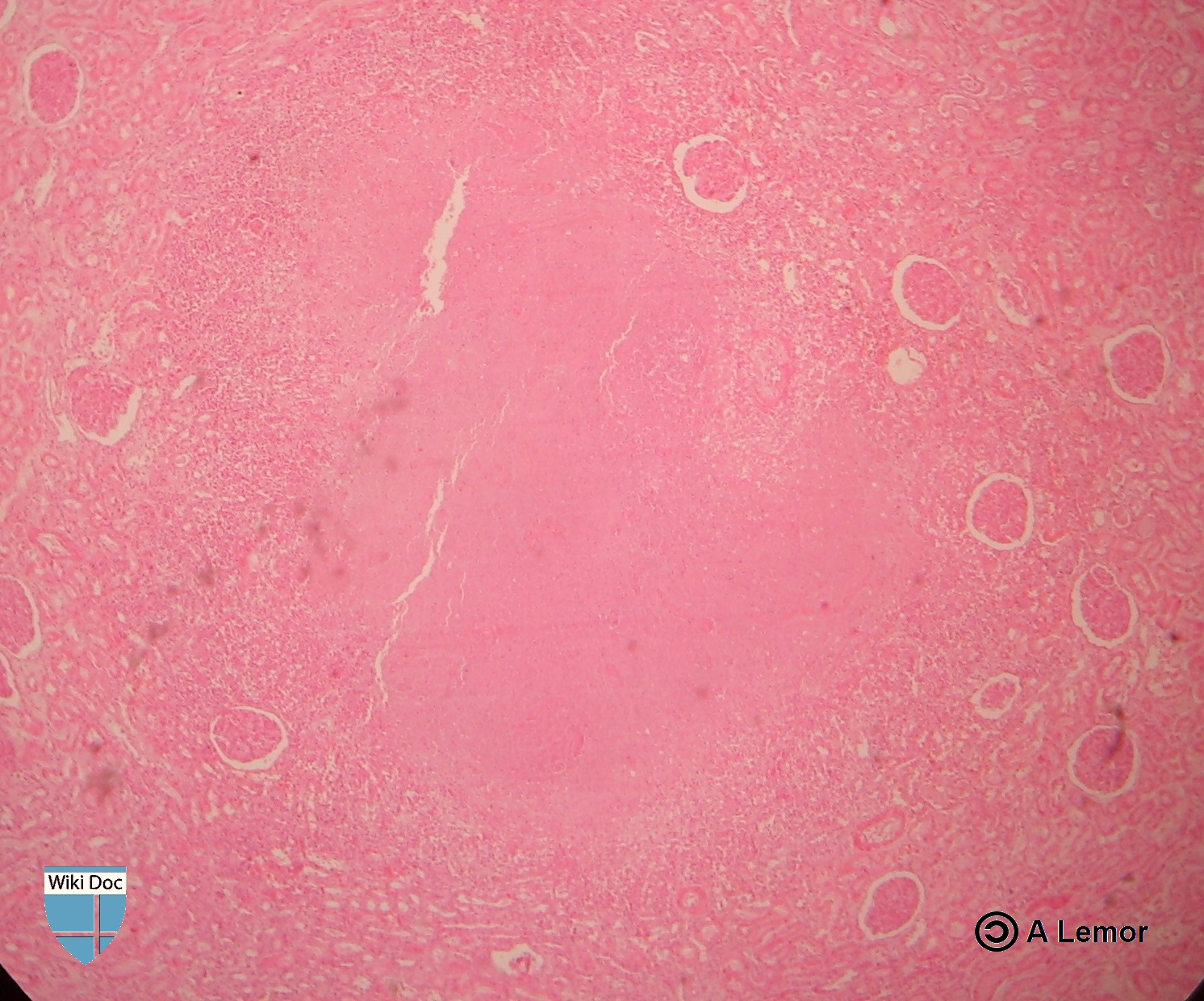 Renal Tuberculosis lesion
Renal Tuberculosis lesion
![Left lateral margin of a tongue of a tuberculosis patient, which had been retracted in order to reveal the lesion that had been caused by the Gram-positive bacterium Mycobacterium tuberculosisAdapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]](https://www.wikidoc.org/index.php/File%3ATB1.jpg)
![Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection.[ http://phil.cdc.gov/phil/ Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.][20]](https://www.wikidoc.org/index.php/File%3ATB2.jpg)
![Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]](https://www.wikidoc.org/index.php/File%3ALeprosy-35.jpg)
![Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]](https://www.wikidoc.org/index.php/File%3ALeprosy-36.jpg)
![Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]](https://www.wikidoc.org/index.php/File%3ALeprosy-37.jpg)
![Light photomicrograph revealing some of the histopathologic cytoarchitectural characteristics seen in a mycobacterial skin infection Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]](https://www.wikidoc.org/index.php/File%3ALeprosy-38.jpg)
![Photomicrograph describing tuberculosis of the placenta.Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]](https://www.wikidoc.org/index.php/File%3ATB3.jpg)
![Histopathology of tuberculosis, endometrium. Ziehl-Neelsen stain.Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]](https://www.wikidoc.org/index.php/File%3ATB4.jpg)
![Histopathology of tuberculosis, placenta.Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[20]](https://www.wikidoc.org/index.php/File%3ATB5.jpg)


References
- ↑ 1.00 1.01 1.02 1.03 1.04 1.05 1.06 1.07 1.08 1.09 1.10 1.11 1.12 1.13 1.14 Mandell, Gerald (2010). Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. Philadelphia, PA: Churchill Livingstone/Elsevier. ISBN 0443068399.
- ↑ 2.0 2.1 Herrmann J, Lagrange P (2005). “Dendritic cells and Mycobacterium tuberculosis: which is the Trojan horse?”. Pathol Biol (Paris). 53 (1): 35–40. PMID 15620608.
- ↑ Agarwal R, Malhotra P, Awasthi A, Kakkar N, Gupta D (2005). “Tuberculous dilated cardiomyopathy: an under-recognized entity?”. BMC Infect Dis. 5 (1): 29. PMID 15857515.
- ↑ Grosset J (2003). “Mycobacterium tuberculosis in the extracellular compartment: an underestimated adversary”. Antimicrob Agents Chemother. 47 (3): 833–6. PMID 12604509.
- ↑ Stead WW, Lofgren JP, Warren E, Thomas C (1985). “Tuberculosis as an endemic and nosocomial infection among the elderly in nursing homes”. N Engl J Med. 312 (23): 1483–7. doi:10.1056/NEJM198506063122304. PMID 3990748.
- ↑ Murray JF (1990). “Cursed duet: HIV infection and tuberculosis”. Respiration. 57 (3): 210–20. PMID 2274719.
- ↑ Kim J, Park Y, Kim Y, Kang S, Shin J, Park I, Choi B (2003). “Miliary tuberculosis and acute respiratory distress syndrome”. Int J Tuberc Lung Dis. 7 (4): 359–64. PMID 12733492.
- ↑ Aderem A, Underhill DM (1999). “Mechanisms of phagocytosis in macrophages”. Annu Rev Immunol. 17: 593–623. doi:10.1146/annurev.immunol.17.1.593. PMID 10358769.
- ↑ 9.0 9.1 9.2 Silva Miranda M, Breiman A, Allain S, Deknuydt F, Altare F (2012). “The tuberculous granuloma: an unsuccessful host defense mechanism providing a safe shelter for the bacteria?”. Clin Dev Immunol. 2012: 139127. doi:10.1155/2012/139127. PMC 3395138. PMID 22811737.
- ↑ 10.0 10.1 “Tumor Necrosis Factor alpha”.
- ↑ “TNF Alpha”. Missing or empty
|url=(help) - ↑ Glaziou P, Falzon D, Floyd K, Raviglione M (2013). “Global epidemiology of tuberculosis”. Semin Respir Crit Care Med. 34 (1): 3–16. doi:10.1055/s-0032-1333467. PMID 23460002.
- ↑ “Causes of Tuberculosis”. Mayo Clinic. 2006-12-21. Retrieved 2007-10-19.
- ↑ Lawn SD, Zumla AI (2011). “Tuberculosis”. Lancet. 378 (9785): 57–72. doi:10.1016/S0140-6736(10)62173-3. PMID 21420161.
- ↑ Zumla A, Raviglione M, Hafner R, von Reyn CF (2013). “Tuberculosis”. N Engl J Med. 368 (8): 745–55. doi:10.1056/NEJMra1200894. PMID 23425167.
- ↑ Daley CL, Small PM, Schecter GF, Schoolnik GK, McAdam RA, Jacobs WR; et al. (1992). “An outbreak of tuberculosis with accelerated progression among persons infected with the human immunodeficiency virus. An analysis using restriction-fragment-length polymorphisms”. N Engl J Med. 326 (4): 231–5. doi:10.1056/NEJM199201233260404. PMID 1345800.
- ↑ Bouvet E, Casalino E, Mendoza-Sassi G, Lariven S, Vallée E, Pernet M; et al. (1993). “A nosocomial outbreak of multidrug-resistant Mycobacterium bovis among HIV-infected patients. A case-control study”. AIDS. 7 (11): 1453–60. PMID 8280411.
- ↑ Shafer RW, Kim DS, Weiss JP, Quale JM (1991). “Extrapulmonary tuberculosis in patients with human immunodeficiency virus infection”. Medicine (Baltimore). 70 (6): 384–97. PMID 1956280.
- ↑ Meintjes G, Lawn SD, Scano F, Maartens G, French MA, Worodria W; et al. (2008). “Tuberculosis-associated immune reconstitution inflammatory syndrome: case definitions for use in resource-limited settings”. Lancet Infect Dis. 8 (8): 516–23. doi:10.1016/S1473-3099(08)70184-1. PMC 2804035. PMID 18652998.
- ↑ 20.0 20.1 20.2 20.3 20.4 20.5 20.6 20.7 20.8 “Public Health Image Library (PHIL), Centers for Disease Control and Prevention”.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mashal Awais, M.D.[2]; João André Alves Silva, M.D. [3]
Synonyms and keywords: M. Tuberculosis
Overview
Mycobacterium tuberculosis is the bacterium responsible for tuberculosis. M. tuberculosis is an obligate aerobe, non-encapsulated, non-motile, acid-fast bacillus. . M. tuberculosis is one of the Mycobacterium tuberculosis complex, which also includes bacteria, such as M. bovis and M. africanum. The bacterium has a very slow rate of replication, and its genetic variations account for the different strains and the growing drug resistance. M. tuberculosis has tropism for different kinds of human cells, with preference for cells of the lung. The main natural reservoir for M. tuberculosis are Human beings; however, the bacteria can also infect other species.
Taxonomy
 |
 |
Cellular organisms; bacteria; Actinobacteria; Actinobacteria; Actinobacteridae; Actinomycetales; Corynebacterineae; Mycobacteriaceae; Mycobacterium; Mycobacterium tuberculosis complex; M. tuberculosis[3]
Biology
- Mycobacterium tuberculosis belongs to the Mycobacterium tuberculosis complex. This complex includes M. tuberculosis, M. bovis, M. africanum, M. canetti, and M. microti.[4]
- M. tuberculosis is an obligate aerobe, non-encapsulated, non-motile, acid-fast bacillus.
- Its shape is slender, straight or slightly curved bacillus with rounded ends.
- It can be present singly, in pairs or in small groups or clumps.
- It cannot form spores.
- It favors tissues with high oxygen levels.
- Due to the high lipid and mycolic acid content of its cell wall, It stains weakly gram-positive or does not retain the dye.
- Microscopic examination of sputum samples cannot differentiate it from other acid-fast bacteria, such as Nocardia spp.[4]
- M. tuberculosis divides every 15-20 hours which is considered an extremely low rate of division. This feature, in addition to its ability to remain latent for long time, are responsible for the long treatment duration needed.[4]
- It can withstand dryness for weeks and also weak disinfectants.
- Genetic variations in the M. tuberculosis genome lead to important phenotypical changes. As a result, there are several variable strains of the bacteria, six of which have particular geographical distribution. Three strains, the Beijing family, strain W and the W-like strains, were reported to be associated with higher incidence of multi-drug resistance.[5][6]
Tropism
There is no particular tissue tropism for M. tuberculosis and it can infect almost all human tissues. However, M. tuberculosis prefers tissues with high levels of oxygen , hence, pulmonary tuberculosis has the highest rate. [4]
Natural Reservoir
The main natural reservoir for M. tuberculosis are Human beings; however, the bacteria can also infect other species.[4]
References
- ↑ “http://phil.cdc.gov/phil/details.asp”. External link in
|title=(help) - ↑ “http://phil.cdc.gov/phil/details.asp”. External link in
|title=(help) - ↑ “Mycobacterium tuberculosis”.
- ↑ 4.0 4.1 4.2 4.3 4.4 Lawn SD, Zumla AI (2011). “Tuberculosis”. Lancet. 378 (9785): 57–72. doi:10.1016/S0140-6736(10)62173-3. PMID 21420161.
- ↑ Smith NH, Hewinson RG, Kremer K, Brosch R, Gordon SV (2009). “Myths and misconceptions: the origin and evolution of Mycobacterium tuberculosis”. Nat Rev Microbiol. 7 (7): 537–44. doi:10.1038/nrmicro2165. PMID 19483712.
- ↑ Gagneux S, Small PM (2007). “Global phylogeography of Mycobacterium tuberculosis and implications for tuberculosis product development”. Lancet Infect Dis. 7 (5): 328–37. doi:10.1016/S1473-3099(07)70108-1. PMID 17448936.
Differentiating Tuberculosis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mashal Awais, M.D.[2]; Alejandro Lemor, M.D. [3]
Overview
Pulmonary tuberculosis should be distinguished from other diseases that cause cough, hemoptysis, fever, night sweat, and weight loss such as: bacterial pneumonia, atypical pneumonia, brucellosis, bronchogenic carcinoma, sarcoidosis, and Hodgkin lymphoma.
Differential Diagnosis
Pulmonary Tuberculosis
| Disease | Findings |
|---|---|
| Bacterial pneumonia | Sudden onset of symptoms, such as high fever, cough, purulent sputum, chest pain, leukocytosis, chest X-ray shows consolidation. |
| Bronchogenic carcinoma | may be asymptomatic, usually at older ages (> 50 years old), cough, hemoptysis, weight loss |
| Brucellosis | Fever, anorexia, night sweats, malaise,back pain , headache, and depression. History of exposure to infected animal |
| Hodgkin lymphoma | Fever, night sweats, pruritus, painless adenopathy, mediastinal mass |
| Mycoplasmal pneumonia | Gradual onset of dry cough, headache, malaise, sore throat. Diffuse bilateral infiltrates on chest X-ray. |
| Sarcoidosis | Non-caseating granulomas in lungs and other organs, bilateral hilar lymphadenopathy, mostly in African American females. |
| Adapted from Mandell, Douglas, and Bennett’s principles and practice of infectious diseases 2010 [1] | |
Extra-Pulmonary Tuberculosis
| Extra-Pulmonary Location | Differential Diagnosis |
|---|---|
| Tuberculous Lymphadenitis | Lymphoma, squamous cell carcinoma, papillary thyroid cancer, pyogenic infection |
| Skeletal Tuberculosis | Multiple myeloma, bone metastasis, spinal cord abscess, osteoporosis |
| Tuberculous Arthrits | Bacterial septic arthritis, pseudogout |
| Central Nervous System Tuberculosis | Bacterial meningitis, viral meningitis, encephalitis |
| Tuberculosis Peritonitis | Bacterial peritonitis, chronic peritoneal dialysis |
| Adapted from Asian Spine J. Feb 2014; 8(1): 97–111[2]; Handbook of Clinical Neurology[3]; Circulation Dec 2005 vol.112 no.23 3608-3616[4]; Am J Trop Med Hyg 2013 vol. 88 no. 1 54-64[5] Clin Infect Dis.(2011)53(6):555-562.[6] | |
| Causes of
lung cavities |
Differentiating Features | Differentiating radiological findings | Diagnosis
confirmation |
|---|---|---|---|
|
|
| |
|
|
|
|
|
|
| |
|
|
|
|
|
|
| |
|
|
| |
|
|
||
|
|
| |
|
|
|
| Disease | Prominent clinical features | Lab findings | Radiological findings |
|---|---|---|---|
| Neurocysticercosis |
|
|
|
| Brain abscess |
|
|
|
| Brain tumors |
|
| |
| Brain tuberculoma |
|
|
|
| Neurosarcoidosis |
|
|
|
 |
 |
 |
 |
|---|
Pulmonary tuberculosis must be distinguished from other cavitary lung lesions.
Differential Diagnosis
Pulmonary tuberculosis must be distinguished from other cavitary lung lesions.
| Causes of
lung cavities |
Differentiating Features | Differentiating radiological findings | Diagnosis
confirmation |
|---|---|---|---|
|
|
| |
|
|
|
|
|
|
| |
|
|
|
|
|
| ||
|
|
| |
|
|
||
|
|
| |
|
References
- ↑ Mandell, Gerald (2010). Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. Philadelphia, PA: Churchill Livingstone/Elsevier. ISBN 0443068399.
- ↑ Moon, Myung-Sang (2014). “Tuberculosis of Spine: Current Views in Diagnosis and Management”. Asian Spine Journal. 8 (1): 97. doi:10.4184/asj.2014.8.1.97. ISSN 1976-1902.
- ↑ Garcia-Monco, Juan Carlos (2014). “Tuberculosis”. 121: 1485–1499. doi:10.1016/B978-0-7020-4088-7.00100-0. ISSN 0072-9752.
- ↑ Mayosi, B. M. (2005). “Tuberculous Pericarditis”. Circulation. 112 (23): 3608–3616. doi:10.1161/CIRCULATIONAHA.105.543066. ISSN 0009-7322.
- ↑ Daher, E. D. F.; da Silva Junior, G. B.; Barros, E. J. G. (2013). “Renal Tuberculosis in the Modern Era”. American Journal of Tropical Medicine and Hygiene. 88 (1): 54–64. doi:10.4269/ajtmh.2013.12-0413. ISSN 0002-9637.
- ↑ Fontanilla, J.-M.; Barnes, A.; von Reyn, C. F. (2011). “Current Diagnosis and Management of Peripheral Tuberculous Lymphadenitis”. Clinical Infectious Diseases. 53 (6): 555–562. doi:10.1093/cid/cir454. ISSN 1058-4838.
- ↑ 7.0 7.1 7.2 7.3 Chaudhuri MR (1973). “Primary pulmonary cavitating carcinomas”. Thorax. 28 (3): 354–66. PMC 470041. PMID 4353362.
- ↑ 8.0 8.1 Mouroux J, Padovani B, Elkaïm D, Richelme H (1996). “Should cavitated bronchopulmonary cancers be considered a separate entity?”. Ann. Thorac. Surg. 61 (2): 530–2. doi:10.1016/0003-4975(95)00973-6. PMID 8572761.
- ↑ 9.0 9.1 Onn A, Choe DH, Herbst RS, Correa AM, Munden RF, Truong MT, Vaporciyan AA, Isobe T, Gilcrease MZ, Marom EM (2005). “Tumor cavitation in stage I non-small cell lung cancer: epidermal growth factor receptor expression and prediction of poor outcome”. Radiology. 237 (1): 342–7. doi:10.1148/radiol.2371041650. PMID 16183941.
- ↑ 10.0 10.1 10.2 10.3 Langford CA, Hoffman GS (1999). “Rare diseases.3: Wegener’s granulomatosis”. Thorax. 54 (7): 629–37. PMC 1745525. PMID 10377211.
- ↑ 11.0 11.1 Lee KS, Kim TS, Fujimoto K, Moriya H, Watanabe H, Tateishi U, Ashizawa K, Johkoh T, Kim EA, Kwon OJ (2003). “Thoracic manifestation of Wegener’s granulomatosis: CT findings in 30 patients”. Eur Radiol. 13 (1): 43–51. doi:10.1007/s00330-002-1422-2. PMID 12541109.
- ↑ 12.0 12.1 Baughman RP, Teirstein AS, Judson MA, Rossman MD, Yeager H, Bresnitz EA, DePalo L, Hunninghake G, Iannuzzi MC, Johns CJ, McLennan G, Moller DR, Newman LS, Rabin DL, Rose C, Rybicki B, Weinberger SE, Terrin ML, Knatterud GL, Cherniak R (2001). “Clinical characteristics of patients in a case control study of sarcoidosis”. Am. J. Respir. Crit. Care Med. 164 (10 Pt 1): 1885–9. doi:10.1164/ajrccm.164.10.2104046. PMID 11734441.
- ↑ 13.0 13.1 Brauner MW, Grenier P, Mompoint D, Lenoir S, de Crémoux H (1989). “Pulmonary sarcoidosis: evaluation with high-resolution CT”. Radiology. 172 (2): 467–71. doi:10.1148/radiology.172.2.2748828. PMID 2748828.
- ↑ 14.0 14.1 Murphy J, Schnyder P, Herold C, Flower C (1998). “Bronchiolitis obliterans organising pneumonia simulating bronchial carcinoma”. Eur Radiol. 8 (7): 1165–9. doi:10.1007/s003300050527. PMID 9724431.
- ↑ 15.0 15.1 15.2 15.3 Al-Ghanem S, Al-Jahdali H, Bamefleh H, Khan AN (2008). “Bronchiolitis obliterans organizing pneumonia: pathogenesis, clinical features, imaging and therapy review”. Ann Thorac Med. 3 (2): 67–75. doi:10.4103/1817-1737.39641. PMC 2700454. PMID 19561910.
- ↑ 16.0 16.1 Cordier JF, Loire R, Brune J (1989). “Idiopathic bronchiolitis obliterans organizing pneumonia. Definition of characteristic clinical profiles in a series of 16 patients”. Chest. 96 (5): 999–1004. PMID 2805873.
- ↑ 17.0 17.1 Lee KS, Kullnig P, Hartman TE, Müller NL (1994). “Cryptogenic organizing pneumonia: CT findings in 43 patients”. AJR Am J Roentgenol. 162 (3): 543–6. doi:10.2214/ajr.162.3.8109493. PMID 8109493.
- ↑ 18.0 18.1 Suri HS, Yi ES, Nowakowski GS, Vassallo R (2012). “Pulmonary langerhans cell histiocytosis”. Orphanet J Rare Dis. 7: 16. doi:10.1186/1750-1172-7-16. PMC 3342091. PMID 22429393.
- ↑ 19.0 19.1 Moore AD, Godwin JD, Müller NL, Naidich DP, Hammar SP, Buschman DL, Takasugi JE, de Carvalho CR (1989). “Pulmonary histiocytosis X: comparison of radiographic and CT findings”. Radiology. 172 (1): 249–54. doi:10.1148/radiology.172.1.2787035. PMID 2787035.
- ↑ Brouwer MC, Tunkel AR, McKhann GM, van de Beek D (2014). “Brain abscess”. N. Engl. J. Med. 371 (5): 447–56. doi:10.1056/NEJMra1301635. PMID 25075836.
- ↑ “Brain Abscess — NEJM”.
- ↑ 22.0 22.1 “Primary Brain Tumors in Adults – American Family Physician”.
- ↑ “The Journal of Association of Chest Physicians – Tuberculoma of the brain – A diagnostic dilemma: Magnetic resonance spectroscopy a new ray of hope : Download PDF”.
- ↑ 24.0 24.1 “Neurosarcoidosis”.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [2]; Associate Editor(s)-in-Chief: Mashal Awais, M.D.[3]; João André Alves Silva, M.D. [4], Dima Nimri, M.D. [5], Tarek Nafee, M.D. [6]
Overview
In 2019, about 8,920 TB cases were documented in the US with an incidence of 2.7 cases/100,000 persons. This represented a decrease by 1.1% from 2018. In 2015, about 10.4 million people developed symptomatic TB and 1.8 million died from the disease. In 2014, approximately 9,421 cases were documented in the United States, with an incidence of 3.0 cases/100 000 persons. Since 1990, there has been a decrease in the mortality rate . TB is more prevalent in older men. Racial and ethnic minorities have a higher prevalence of TB than non-Hispanic whites. Coinfection with HIV is an important leading cause of death in TB. In 2015, 60% of the worldwide TB cases were in 6 countries: South Africa, Indonesia, China, Pakistan, India, and Nigeria. The WHO reported 24 other high-burden TB countries including Bangladesh, Korea, Columbia, Cambodia, Congo, Brazil, Ethiopia, Myanmar, Philippines, Thailand, Liberia, Vietnam, Kenya, Central Africa, Russia, Angola, Zimbabwe, Namibia, Mozambique, Tanzania, Sierra Leone, Zambia, Papua New Guinea, and Lesotho.[1]
Epidemiology
- Worldwide, in 2018, there were approximately 10 million individuals with incident TB and about 1.5 million TB-related deaths.
- Approximately 862,000 of these cases were in patients coinfected with HIV [12]
- Worldwide, in 2015, approximately 10.4 million people had symptomatic TB.[2][3]
- 1.17 million of these cases occurred were in patients coinfected with HIV.[2][3]
- 400,000 of these cases were in patients coinfected with HIV.[2][3]
- In the United States, in 2014, approximately 9,421 cases were reported with an incidence of 3.0 cases/100 000 persons.[2][3]
Incidence and Mortality
Worldwide Tuberculosis
- Over 95% of TB deaths occur in low- and middle-income countries, and it is among the top three causes of death for women aged 15 to 44.
- The TB death rate dropped 45% between 1990 and 2012.
- In 2015, 3 million lives were saved by the global TB response.
-
![Incidence of All Forms of TB in 2015. - WHO 2016 TB Report)[1]](https://www.wikidoc.org/images/0/05/TB_incidence_all_forms.jpg) Incidence of All Forms of TB in 2015. – WHO 2016 TB Report)[1]
Incidence of All Forms of TB in 2015. – WHO 2016 TB Report)[1] -
![Trend in TB incidence from 2000 to 2015. - WHO 2016 TB Report)[1]](https://www.wikidoc.org/images/d/dd/TB_incidence_trends.jpg) Trend in TB incidence from 2000 to 2015. – WHO 2016 TB Report)[1]
Trend in TB incidence from 2000 to 2015. – WHO 2016 TB Report)[1] -
![TB mortality trends (2000-2015) - WHO 2016 TB Report)[1]](https://www.wikidoc.org/images/9/94/TB_mortality_trends.jpg) TB mortality trends (2000-2015) – WHO 2016 TB Report)[1]
TB mortality trends (2000-2015) – WHO 2016 TB Report)[1] -
![TB Global Mortality in 2015. - WHO 2016 TB Report)[1]](https://www.wikidoc.org/images/3/3d/TBmortality2015.jpg) TB Global Mortality in 2015. – WHO 2016 TB Report)[1]
TB Global Mortality in 2015. – WHO 2016 TB Report)[1] -
![Image 5 - TB is in the top 10 causes of death in 2015. - WHO 2016 TB Report)[1]](https://www.wikidoc.org/images/6/65/Topworldwidecauseofdeath.jpg) Image 5 – TB is in the top 10 causes of death in 2015. – WHO 2016 TB Report)[1]
Image 5 – TB is in the top 10 causes of death in 2015. – WHO 2016 TB Report)[1] -
![Trends in Estimated Incident Tuberculosis 2000-2018 (TB)[1]](https://www.wikidoc.org/images/c/c2/Screen_Shot_2021-01-19_at_8.30.45_PM.png) Trends in Estimated Incident Tuberculosis 2000-2018 (TB)[1]
Trends in Estimated Incident Tuberculosis 2000-2018 (TB)[1]
![Incidence of All Forms of TB in 2015. - WHO 2016 TB Report)[1]](https://www.wikidoc.org/index.php/File%3ATB_incidence_all_forms.jpg)
![Trend in TB incidence from 2000 to 2015. - WHO 2016 TB Report)[1]](https://www.wikidoc.org/index.php/File%3ATB_incidence_trends.jpg)
![TB mortality trends (2000-2015) - WHO 2016 TB Report)[1]](https://www.wikidoc.org/index.php/File%3ATB_mortality_trends.jpg)
![TB Global Mortality in 2015. - WHO 2016 TB Report)[1]](https://www.wikidoc.org/index.php/File%3ATBmortality2015.jpg)
![Image 5 - TB is in the top 10 causes of death in 2015. - WHO 2016 TB Report)[1]](https://www.wikidoc.org/index.php/File%3ATopworldwidecauseofdeath.jpg)
![Trends in Estimated Incident Tuberculosis 2000-2018 (TB)[1]](https://www.wikidoc.org/index.php/File%3AScreen_Shot_2021-01-19_at_8.30.45_PM.png)
Global Regional Incidence & Mortality
The following global regional trends in TB incidence are observed from 2000 to 2015:

| African Region | American Region | Eastern Mediterranean Region | European Region | South-East Asian Region | Western-Pacific Region | |
|---|---|---|---|---|---|---|
| Incidence (per 100 000) |
275 | 27 | 116 | 36 | 246 | 86 |
| Incidence of Multi-Drug Resistant TB (per 100 000) |
11 | 1.1 | 6 | 14 | 10 | 5.5 |
| Mortality (excluding HIV-TB coinfection) (per 100 000) |
45 | 1.9 | 12 | 3.5 | 37 | 4.8 |
| Mortality (only HIV-TB coinfection) (per 100 000) |
30 | 0.59 | 0.46 | 0.54 | 3.9 | 0.31 |
| Total new cases in 2016 | 1 333 504 | 230 519 | 484 733 | 297 448 | 2 656 560 | 1 361 430 |
| Table adapted from WHO Global Report 2016 [1] | ||||||
TB and HIV
Immunosuppression secondary to HIV is strongly associated with incidence of TB and its subsequent complications. Tuberculosis contributes to a considerable proportion of HIV/AIDS related deaths.
-
![Incidence of TB and HIV in 2015 - WHO 2016 TB Report)[1]](https://www.wikidoc.org/images/b/b0/TB_HIV_incidence.jpg) Incidence of TB and HIV in 2015 – WHO 2016 TB Report)[1]
Incidence of TB and HIV in 2015 – WHO 2016 TB Report)[1] -
![Trend in TB and HIV mortality (2000-2015) - WHO 2016 TB Report)[1]](https://www.wikidoc.org/images/c/c7/TrendinTBandHIVdeath.jpg) Trend in TB and HIV mortality (2000-2015) – WHO 2016 TB Report)[1]
Trend in TB and HIV mortality (2000-2015) – WHO 2016 TB Report)[1] -
![Estimated TB and HIV deaths in 2015 - WHO 2016 TB Report)[1]](https://www.wikidoc.org/images/b/b6/HIVandTBdeath2015.jpg) Estimated TB and HIV deaths in 2015 – WHO 2016 TB Report)[1]
Estimated TB and HIV deaths in 2015 – WHO 2016 TB Report)[1]
![Incidence of TB and HIV in 2015 - WHO 2016 TB Report)[1]](https://www.wikidoc.org/index.php/File%3ATB_HIV_incidence.jpg)
![Trend in TB and HIV mortality (2000-2015) - WHO 2016 TB Report)[1]](https://www.wikidoc.org/index.php/File%3ATrendinTBandHIVdeath.jpg)
![Estimated TB and HIV deaths in 2015 - WHO 2016 TB Report)[1]](https://www.wikidoc.org/index.php/File%3AHIVandTBdeath2015.jpg)
Tuberculosis in Endemic Countries
In 2015, 60% of the worldwide TB cases were reported in six countries:
South Africa
- The incidence of tuberculosis was reported as 834 per 100,000 of the general population.[1]
- The mortality rate of tuberculosis (excluding HIV-TB coinfection) was reported as 46 per 100,000 of the general population.[1]
Indonesia
- The incidence of tuberculosis was reported as 395 per 100,000 of the overall population.[1]
- The mortality rate of tuberculosis (excluding HIV–TB coinfection) was reported as 40 per 100,000 of the overall population.[1]
Nigeria
- The incidence of tuberculosis was reported as 322 per 100,000 of the general population.[1]
- The mortality rate of tuberculosis (excluding HIV–TB coinfection) was reported as 99 per 100,000 of the general population.[1]
Pakistan
- The incidence of tuberculosis was reported as 270 per 100,000 of the general population.[1]
- The mortality rate of tuberculosis (excluding HIV-TB coinfection) was reported as 23 per 100,000 of the general population.[1]
India
- The incidence of tuberculosis was reported as 217 per 100,000 of the general population.[1]
- The mortality rate of tuberculosis (excluding HIV-TB coinfection) was reported as 36 per 100,000 of the general population.[1]
China
- The incidence of tuberculosis was reported as 67 per 100,000 of the general population.[1]
- The mortality rate of tuberculosis (excluding HIV-TB coinfection) was reported as 2.6 per 100,000 of the general population.[1]
Tuberculosis in the United States
TB resurge occurred in the mid-1980s since when the number of cases steadily increased with a peak occurred in 1992. Following this peak, the number of reported TB cases has decreased annually. The year of 2014 represented the twenty-second year of decline in the reported TB cases in the United States since that peak. In 2014, approximately a total number of 9,421 cases were reported in the 50 states and the District of Columbia (DC). This was considered a decline of 1.5% from 2013. The number of TB cases per 100,000 in 2013 and 2014 was at a stable rate of 3.0.[1]
 |
 |
Demographics
Age
In 2014, TB cases in most age groups decreased by approximately 70% from the 1993 values. Below is the comparison between the case rates (per 100 000 persons) of these two years, according to different ages:[4]
| Age | Case rate in 1993 | Case rate in 2014 |
|---|---|---|
| >65 years | 17.7 | 4.8 |
| 45 – 64 years | 12.4 | 3.5 |
| 25 – 44 years | 11.5 | 3.4 |
| 15 – 24 years | 5.0 | 2.2 |
| < 15 years | 2.9 | 0.8 |
| Data provided by the CDC[2][3][4] | ||
 |
 |
Depending on the age of the patient, tuberculosis may have different clinical manifestations, progression, and prognosis:[6][7][8][9][7][10]
| Factor | Influence |
|---|---|
| Infants and Children |
|
| Adolescents |
|
| Midadulthood |
|
| Elderly |
|
Gender
In 2012, there were 410,000 total deaths in women as a result of TB in the United States, 160,000 of them were HIV-positive. Out of the total TB deaths among HIV-positive people, 50% were women.[2][3] TB rates tend to increase with age, ranging from a low rate of less than 1 per 100,000 in children aged 5 – 14 to a high rate of 6.9 per 100,000 in men aged 65 years and older. With age increasing, the case rate increases faster in men than in women; the rates in men aged 45 years and older were approximately more than double the case rate in women of the same age.[2][3]

Race
The highest TB rates was reported in Asians, a decline from 29.9 per 100,000 persons in 2003 to 17.8 in 2014.[2][11]
| Racial/ethnic groups | Case rate in 2003 | Case rate in 2014 |
|---|---|---|
| Non-Hispanic blacks or African-Americans | 11.7 | 5.1 |
| Hispanics | 10.3 | 5.0 |
| American Indians and Alaska Natives | 8.2 | 5.0 |
| Non-Hispanic whites | 1.4 | 0.6 |
| Native Hawaiian or Other Pacific Islanders | 16.2 | 16.9 |
| Data provided by the CDC[2][3][11] | ||
The disproportionate burden of TB in minorities is due to many factors. In persons who were born in countries where TB is endemic, the disease can be a result of an acquired infection in their country of origin. Unequal distribution of TB risk factors, such as HIV infection, leads to increased TB exposure or to an increased risk of developing TB after infection with with M. tuberculosis.[2]
- Image 8 shows that above the age of 5, there is an increased risk of TB with age across all racial and ethnic groups. The case rates were higher in minority racial and ethnic groups than in non-Hispanic whites and were highest in Asians, Native Hawaiians and Other Pacific Islanders, especially in the adult age groups.[5]
- Image 9 shows that in 2014, 85% of all reported TB cases occurred in racial and ethnic minorities, whereas 13% of cases occurred in non-Hispanic whites. Persons reporting two or more races accounted for 2% of all cases[5]
 |
 |
 |
References
- ↑ 1.00 1.01 1.02 1.03 1.04 1.05 1.06 1.07 1.08 1.09 1.10 1.11 1.12 1.13 1.14 1.15 1.16 1.17 1.18 1.19 1.20 1.21 1.22 1.23 1.24 “WHO 2016 TB Report” (PDF).
- ↑ 2.00 2.01 2.02 2.03 2.04 2.05 2.06 2.07 2.08 2.09 2.10 “Tuberculosis (TB)”.
- ↑ 3.0 3.1 3.2 3.3 3.4 3.5 3.6 3.7 3.8 “Tuberculosis”.
- ↑ 4.0 4.1 Center for Disease Control and Prevention http://www.cdc.gov/tb/statistics/reports/2014/pdfs/2014-surveillance-report_table4.pdf
- ↑ 5.0 5.1 5.2 5.3 5.4 5.5 5.6 5.7 5.8 “Center for Disease Control and Prevention (CDC)” (PDF).
- ↑ Stead WW, Lofgren JP, Warren E, Thomas C (1985). “Tuberculosis as an endemic and nosocomial infection among the elderly in nursing homes”. N Engl J Med. 312 (23): 1483–7. doi:10.1056/NEJM198506063122304. PMID 3990748.
- ↑ 7.0 7.1 DAHL RH (1952). “[The first appearance of a pulmonary cavity after primary infection with relation to time and age]”. Acta Tuberc Scand. 27 (1–2): 140–9. PMID 13007533.
- ↑ Stead WW (1967). “Pathogenesis of a first episode of chronic pulmonary tuberculosis in man: recrudescence of residuals of the primary infection or exogenous reinfection?”. Am Rev Respir Dis. 95 (5): 729–45. PMID 4960690.
- ↑ “Targeted tuberculin testing and treatment of latent tuberculosis infection. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, July 1999. This is a Joint Statement of the American Thoracic Society (ATS) and the Centers for Disease Control and Prevention (CDC). This statement was endorsed by the Council of the Infectious Diseases Society of America. (IDSA), September 1999, and the sections of this statement”. Am J Respir Crit Care Med. 161 (4 Pt 2): S221–47. 2000. doi:10.1164/ajrccm.161.supplement_3.ats600. PMID 10764341.
- ↑ Stead WW, Kerby GR, Schlueter DP, Jordahl CW (1968). “The clinical spectrum of primary tuberculosis in adults. Confusion with reinfection in the pathogenesis of chronic tuberculosis”. Ann Intern Med. 68 (4): 731–45. PMID 5642961.
- ↑ 11.0 11.1 Center for Disease Control and Prevention http://www.cdc.gov/tb/statistics/reports/2014/pdfs/2014-surveillance-report_table17.pdf
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mashal Awais, M.D.[2]; João André Alves Silva, M.D. [3]
Overview
The risk factors for developing tuberculosis include: living or traveling to endemic areas for TB, elderly people and infants, immunosuppression, history of frequent or prolonged contact with infected patients, IV drug users, smoking, bad hygiene, and poor nutrition. In addition, the risk factors for multidrug-resistant TB include: non-adherence to treatment regimen, inadequate treatment for that bacterial strain, and contact with patients with multidrug-resistant TB.
Risk Factors
Primary TB, which represents 1-5% cases, occurs after infection. However, most of the cases occur with latent infection which is asymptomatic. The dormant bacilli can cause tuberculosis in 2 to 23% of the latent cases, usually several years following the primary infection.[1] The risk of reactivation is much higher with immunosuppression, such as HIV. In patients with HIV coinfection, the risk of reactivation increases reaching up to 10% per year.
The following are risk factors for active TB:[2][3]
- Living or traveling to endemic areas (Sub-saharan African, Russia, India, Pakistan, China)
- Elderly
- Infants
- IV drug users
- Immunosuppression:
- AIDS
- Diabetes
- Silicosis
- Malignancy, such as head and neck cancers
- Hematologic and reticuloendothelial disease, such as leukemia and Hodgkin’s disease
- Or those taking medications, such as:
- Chemotherapy
- Immunosuppressive medications, such as prolonged corticosteroid therapy, tumor necrosis factor-alpha blockers[4]
- Tocilizumab
The risk of contracting TB increases in cases where there is:[2]
The following factors may increase the rate of TB infection in a population:[2]
- Chest X-ray with evidence of previous TB disease (fibrotic lesions and nodules)
- Increased number of HIV infections
- Increased number of homeless people
- The appearance of drug-resistant strains of TB
Drugs With Increased Risk of Tuberculosis Reactivation
- Treatment with the following drugs have been reported with increased risk of reactivation of latent tuberculosis.
Multidrug-Resistant Tuberculosis
Drug resistance is more common in people who:[5]
- Do not take their TB medicine regularly
- Do not take all of their TB medicine as told by their doctor or nurse
- Develop TB disease again, after having taken TB medicine in the past
- Come from areas of the world where drug-resistant TB is common
- Have spent time with someone known to have drug-resistant TB disease
References
- ↑ Parrish N, Dick J, Bishai W (1998). “Mechanisms of latency in Mycobacterium tuberculosis”. Trends Microbiol. 6 (3): 107–12. PMID 9582936.
- ↑ 2.0 2.1 2.2 “Tuberculosis Fact Sheet”.
- ↑ Griffith D, Kerr C (1996). “Tuberculosis: disease of the past, disease of the present”. J Perianesth Nurs. 11 (4): 240–5. PMID 8964016.
- ↑ Mutlu G, Mutlu E, Bellmeyer A, Rubinstein I (2006). “Pulmonary adverse events of anti-tumor necrosis factor-alpha antibody therapy”. Am J Med. 119 (8): 639–46. PMID 16887405.
- ↑ “Multidrug-resistant tuberculosis”.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mashal Awais, M.D.[2]; Alejandro Lemor, M.D. [3]; Marjan Khan M.B.B.S.[4]
Overview
Tuberculosis screening is performed using a mantoux tuberculin skin test, also known as a tuberculin skin test or a PPD. This test is done by intradermal injection of a small amount of a purified protein derivative (PPD) of the tuberculosis bacterium then observing the reaction in the following days.
Screening
Mantoux Tuberculin Skin Test
- The Mantoux tuberculin skin test (TST) is primarily used to evaluate a person whether they are infected with Mycobacterium tuberculosis.
- The TST is done by intradermal injection 0.1 ml of tuberculin purified protein derivative (PPD) into the inner surface of the forearm. The injection is done using a tuberculin syringe, with the needle bevel facing upward. In case of a correct injection, it produces a pale elevation of the skin (wheal) 6 to 10 mm in diameter.
- The reaction is read between 48 and 72 hours after administration. If the patient does not return within 72 hours, another TST should be rescheduled.
- The induration (palpable, raised, hardened area, or swelling) should be measured in millimeters not the erythema (redness), and the diameter of the indurated area is measured across the forearm (perpendicular to the long axis).
- The only contraindication for TST is in persons who had any severe reaction (e.g., necrosis, blistering, anaphylactic shock, or ulcerations) to another previous TST.
- TST is not contraindicated for any other individuals, including infants, children, pregnant women, HIV-infected patients, or individuals who received BCG vaccination.
- In some individuals with with previous M. tuberculosis infection, the reaction to tuberculin can wane over time, so if TST is done years after infection, it may yield false-negative reaction. However, the TST may activate the immune system, leading to a positive, or boosted reaction to the following tests. Doing a second TST after an initial negative TST reaction, that is known as two-step testing, is preferred especially for healthcare workers or nursing home residents (retested periodically).
Classification of Tuberculin Reaction
Interpretation of TST is based on on two elements:
- Measurement of the induration in millimeters.
- The individual’s risk of being infected with TB and also of progression to disease if infected.
   |
| Tuberculin Reaction | Considered a Positive Result in: |
|---|---|
| ≥ 5 mm |
|
| ≥ 10 mm |
|
| ≥ 15 mm |
|
| Table adapted from CDC[1] | |
| False-Positive Reactions | False-Negative Reactions |
|---|---|
In some cases, some individuals react to the TST positively although they are not infected with M. tuberculosis. The causes of these false-positive reactions involve, but are not limited to, the following:
|
On the other hand, Some individuals do not react to the TST although they are infected with M. tuberculosis. The causes for these false-negative reactions involve, but are not limited to, the following:
|
| Table adapted from CDC[1] | |
Recommendations for Human Immunodeficiency Virus (HIV) Screening in Tuberculosis Clinics Adapted from CDC[2]
- According to CDC, HIV screening is recommended for all TB patients after the patient notification that testing will be done unless the patient defers (i.e., opt-out screening). This includes patients with TB disease and with latent TB infection.
- HIV testing is also recommended for individuals who are suspected of having TB disease, patients with latent TB infection, and contacts of TB patients.
- Prevention counseling and separate written consent for HIV testing are no longer necessary.
- These recommendations are effective for eliminating missed opportunities for HIV screening and reducing significant barriers to HIV testing in health care settings by:
- Opt-out screening refers to performing HIV testing after informing the patient that the test will be done, and despite being declined by the patient, it is strongly recommended. Assent is inferred unless the patient defers HIV testing.
Quantiferon Gold testing
- The early identification of Mycobacterium tuberculosis infection is a complex issue regarding the control and prevention of TB.[3]
- Over several years, the tuberculin skin test (TST) was the most commonly used test for the diagnosis of TB infection due to its low cost and convenience in most countries.[4]
- However, PPD testing has several disadvantages, including low specificity in individuals who received the Bacillus Calmette-Guerin (BCG) vaccination.[5]
- In the last decade, interferon gamma release assays (IGRAs) have been used to detect Latent Tuberculosis.[6]
- Interferon-gamma release assays (IGRAs) are immunodiagnostics techniques that measure interferon-gamma (IFN-γ) released by T-cells in response to Mycobacterium tuberculosis-specific antigen.[7]
- There are two commercial in vitro IGRAs; including the QuantiFERON-TB Gold In-Tube (QFT-GIT) test and T-SPOT.TB that have been used for for the early detection of M. tuberculosis infection.[7]
- QuantiFERON-TB Gold includes proteins that are almost exclusively found in mycobacterium tuberculosis.[8]
- The QuantiFERON-TB Gold In-Tube test (QFT-GIT) assay measures the IFN-γ serum concentration following stimulation by specific TB antigens.[8]
- The Quantiferon Gold test is used on a large scale in developed countries.[6]
- The ability of QFT-GIT will be to monitor the response to anti-tuberculosis treatment is not fully-understood.[9]
| Category | 2005 Recommendation | 2019 Recommendation |
|---|---|---|
| Baseline (preplacement) screening and testing | TB screening of all HCP, in addition to a symptom evaluation and testing (TST or IGRA) for those without documented previous TB disease or LTBI. | TB screening of all HCP, in addition to a symptom evaluation and testing (TST or IGRA) for those without documented previous TB disease or LTBI (unchanged); individual TB risk assessment (new). |
| Postexposure screening and testing | Symptom evaluation for all HCP if exposure is identified. For HCP having a baseline negative TB test and no previous TB disease or LTBI, do a test (IGRA or TST) when the exposure is detected. If that test is negative, perform another test 8–10 weeks following the last exposure. | Symptom evaluation for all HCP if exposure is identified. For HCP having a baseline negative TB test and no previous TB disease or LTBI, do a test (IGRA or TST) when the exposure is detected. If that test is negative, perform another test 8–10 weeks following the last exposure (unchanged). |
| Serial screening and testing for HCP without LTBI | According to health care facility and setting risk assessment. Not recommended for HCP working in low-risk health care settings. Recommended for HCP working in medium-risk health care settings and settings with potential ongoing transmission. | Not routinely recommended (new); can consider for selected HCP groups (unchanged); recommend annual TB education for all HCP (unchanged), including information about TB exposure risks for all HCP (new emphasis). |
| Evaluation and treatment of positive test results | Referral to determine whether LTBI treatment is indicated. | Treatment is encouraged for all HCP with untreated LTBI, unless medically contraindicated (new). |
| Abbreviations: IGRA = interferon-gamma release assay; LTBI = latent tuberculosis infection; TST = tuberculin skin test.
| ||
References
- ↑ 1.0 1.1 “CDC Tuberculin Skin Testing”.
- ↑ “CDC Recommendations for Human Immunodeficiency Virus (HIV) Screening in Tuberculosis (TB) Clinics”.
- ↑ “WHO | Global tuberculosis report 2018, SYSTEM DO NOT MOVE OR EDIT”.
- ↑ Houben RM, Dodd PJ (October 2016). “The Global Burden of Latent Tuberculosis Infection: A Re-estimation Using Mathematical Modelling”. PLoS Med. 13 (10): e1002152. doi:10.1371/journal.pmed.1002152. PMC 5079585. PMID 27780211.
- ↑ Detjen AK, Keil T, Roll S, Hauer B, Mauch H, Wahn U, Magdorf K (August 2007). “Interferon-gamma release assays improve the diagnosis of tuberculosis and nontuberculous mycobacterial disease in children in a country with a low incidence of tuberculosis”. Clin. Infect. Dis. 45 (3): 322–8. doi:10.1086/519266. PMID 17599309.
- ↑ 6.0 6.1 Lu P, Chen X, Zhu LM, Yang HT (June 2016). “Interferon-Gamma Release Assays for the Diagnosis of Tuberculosis: A Systematic Review and Meta-analysis”. Lung. 194 (3): 447–58. doi:10.1007/s00408-016-9872-5. PMID 27039307.
- ↑ 7.0 7.1 Lalvani A (June 2007). “Diagnosing tuberculosis infection in the 21st century: new tools to tackle an old enemy”. Chest. 131 (6): 1898–906. doi:10.1378/chest.06-2471. PMID 17565023.
- ↑ 8.0 8.1 Dilektasli AG, Erdem E, Durukan E, Eyüboğlu FÖ (November 2010). “Is the T-cell-based interferon-gamma releasing assay feasible for diagnosis of latent tuberculosis infection in an intermediate tuberculosis-burden country?”. Jpn. J. Infect. Dis. 63 (6): 433–6. PMID 21099095.
- ↑ Dheda K, Pooran A, Pai M, Miller RF, Lesley K, Booth HL, Scott GM, Akbar AN, Zumla A, Rook GA (August 2007). “Interpretation of Mycobacterium tuberculosis antigen-specific IFN-gamma release assays (T-SPOT.TB) and factors that may modulate test results”. J. Infect. 55 (2): 169–73. doi:10.1016/j.jinf.2007.02.005. PMID 17448540.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mashal Awais, M.D.[2]; João André Alves Silva, M.D. [3]
Overview
Tuberculosis complications are pulmonary and extra-pulmonary. Moreover, they include severe parenchymal, vascular, pleural and chest wall complications. The pulmonary complications of tuberculosis include pneumonia, pleural effusions, bronchiectasis, cavitations, and lymphadenopathy. The hematogenous spread of infection resuts in miliary tuberculosis. Without effective medical therapy, 1/3 of patients with active tuberculosis die within 1 year of diagnosis, and more than 50% die during the first 5 years. However, M. tuberculosis infections carry a good prognosis if diagnosed early and treated effectively.
Natural History
Without proper medical therapy, 1/3 of patients with active tuberculosis die within 1 year of the diagnosis, and more than 50% during the first 5 years. The 5-year mortality rate in patients with a positive sputum smear test for M. tuberculosis is 65%. Patients who survive the 5 years have probability of 60% of spontaneous remission. [1]
Primary Pulmonary Tuberculosis
Primary tuberculosis occurs soon after infection with M. tuberculosis and differs from clinical illness. In endemic areas, primary TB is usually observed at a young age. Primary TB may be completely asymptomatic, or iinvolves mild symptoms, such as fever, cough, and chest pain, due to pleurisy. Some patients can have other symptoms, such as erythema nodosum in the lower limbs and phlyctenulosis. The initial lesion (Ghon focus) often resolves spontaneously, becoming a calcified nodule that may be identified on the chest X-Ray. Pleuritic chest pain usually occurs as a result of the pleural reaction to the underlying Ghon focus.[1]
The progression of primary TB is more rapidly in patients with impaired immunity and in children. Progression of primary tuberculosis results in the enlargement of the Ghon focus. The disease may have the following manifestations:[1]
- Pleural effusion – results from invasion of the pleural space by M. tuberculosis. Usually occurs with subpleural focus of infection.
- Cavitation – results from progressive enlargement of the Ghon focus and necrosis of its center.
- Lymphadenopathy – the dissemination of M. tuberculosis from the lungs to lymph leads to the enlargement of lymph nodes particularly the paratracheal and perihilar lymph nodes.
- Airway obstruction – presents with shortness of breath and wheezing. Usually occurs as a result of severe enlargement of the lymph nodes, compressing the airways resulting in distal collapse, partial obstruction, or hyperinflation.
- Pneumonia – results from rupture and leakage of lymph node content into the airways.
- Bronchiectasis – results from progressive pneumonia that damages a specific segment of the lung, or an entire lobe, leading to bronchiectasis.
Primary infection leads to dissemination of M. tuberculosis through the blood. With impaired immune response, miliary tuberculosis may occur resulting in the formation of granulomatous lesions in several organs.[1]

Secondary Pulmonary Tuberculosis
Also known as “adult-type” or “post-primary tuberculosis”. May result from recent infection with M. tuberculosis, or from the reactivation of an endogenous focus containing the latent form of the infection. Without effective medical therapy, approximately 1/3 of patients die within months of disease onset. Of the remaining 2/3, some can develop spontaneous remission, while others experience a chronic infection with severe symptoms. The survivors may have fibrotic and calcified lesions, and cavitations in some areas of the lungs, that can be detected later on a chest X-Ray.[1]
The onset of illness is insidious and nonspecific, and the symptoms include:
- Fever
- Night sweats
- Weakness
- Malaise
- Anorexia
- Weight loss
- Cough (90% cases) – nonproductive at the outset, more frequent during the morning, that gradually progresses to productive cough, with purulent sputum, with occasional streaks of blood
- Hemoptysis (20-30% cases) may occur in the following cases:
- Rupture of a blood vessel on a cavity wall leads to severe hemoptysis
- Rupture of a pulmonary artery aneurysm adjacent or within a tuberculous cavity (Rasmussen’s aneurysm)
- Formation of an aspergilloma in a lung cavity
- Pleuritic chest pain
- Dyspnea (in severe disease)
- ARDS
Complications
Tuberculosis may be localized to the lungs, or affects other organs of the body. Pulmonary TB can result in permanent damage of the lungs and affected organs. According to the pulmonary, or extrapulmonary nature of the lesions, the possible complications may include:[3][4]
Parenchymal Lesions
| Complication | Description |
|---|---|
| Tuberculoma |
|
| Cicatrization |
|
| Thin-walled cavity |
|
| Aspergilloma |
|
| Lung destruction[3] |
|
| Bronchogenic carcinoma[3] |
Airway Lesions
| Complication | Description |
|---|---|
| Bronchiectasis |
|
| Tracheobronchial stenosis |
|
| Broncholithiasis |
|
Vascular Lesions
| Complication | Description |
|---|---|
| Pulmonary or bronchial arteritis and thrombosis |
|
| Bronchial artery dilatation |
|
| Rasmussen’s aneurysm |
|
Mediastinal Lesions
| Complication | Description |
|---|---|
| Esophagobronchial fistula |
|
| Esophagomediastinal fistula |
|
| Constrictive pericarditis |
|
| Lymph node calcification |
|
| Fibrosing mediastinitis |
|
| Extranodal extension |
|
Pleural Lesions
| Complication | Description |
|---|---|
| Bronchopleural fistula |
|
| Fibrothorax and chronic empyema |
|
| Pneumothorax |
|
Chest Wall Lesions
| Complication | Description |
|---|---|
| Tuberculous spondylitis (Pott’s disease) |
|
| Rib tuberculosis |
|
| Malignancy |
|
Prognosis
- If untreated, active TB is often fatal. According to studies performed in several countries, 1/3 of the untreated patients died within 1 year after the diagnosis, while > 50% died within the first 5 years. However, with early diagnosis and adequate treatment, these patients have a good prognosis.[1]
- Symptoms of uncomplicated TB usually improve after 2-3 weeks of treatment initiation.[4]
- Improvements in the chest X-ray require several weeks to months to be noted.[4]
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 Longo, Dan (2012). Harrison’s principles of internal medicine. New York: McGraw-Hill. ISBN 007174889X.
- ↑ “Wikimedia Commons”.
- ↑ 3.0 3.1 3.2 3.3 Kim HY, Song KS, Goo JM, Lee JS, Lee KS, Lim TH (2001). “Thoracic sequelae and complications of tuberculosis”. Radiographics. 21 (4): 839–58, discussion 859-60. doi:10.1148/radiographics.21.4.g01jl06839. PMID 11452057.
- ↑ 4.0 4.1 4.2 “Prognosis of TB”.
- ↑ 5.0 5.1 Woodring JH, Vandiviere HM, Fried AM, Dillon ML, Williams TD, Melvin IG (1986). “Update: the radiographic features of pulmonary tuberculosis”. AJR Am J Roentgenol. 146 (3): 497–506. doi:10.2214/ajr.146.3.497. PMID 3484866.
- ↑ 6.0 6.1 6.2 6.3 Lee KS, Song KS, Lim TH, Kim PN, Kim IY, Lee BH (1993). “Adult-onset pulmonary tuberculosis: findings on chest radiographs and CT scans”. AJR Am J Roentgenol. 160 (4): 753–8. doi:10.2214/ajr.160.4.8456658. PMID 8456658.
- ↑ Palmer PE (1979). “Pulmonary tuberculosis–usual and unusual radiographic presentations”. Semin Roentgenol. 14 (3): 204–43. PMID 472765.
- ↑ Fraser, Richard (1994). Synopsis of diseases of the chest. Philadelphia: W.B. Saunders. ISBN 0721636691.
- ↑ Logan PM, Müller NL (1996). “CT manifestations of pulmonary aspergillosis”. Crit Rev Diagn Imaging. 37 (1): 1–37. PMID 8744521.
- ↑ Miller WT (1996). “Aspergillosis: a disease with many faces”. Semin Roentgenol. 31 (1): 52–66. PMID 8838945.
- ↑ Thompson BH, Stanford W, Galvin JR, Kurihara Y (1995). “Varied radiologic appearances of pulmonary aspergillosis”. Radiographics. 15 (6): 1273–84. doi:10.1148/radiographics.15.6.8577955. PMID 8577955.
- ↑ Snider GL, Placik B (1969). “The relationship between pulmonary tuberculosis and bronchogenic carcinoma. A topographic study”. Am Rev Respir Dis. 99 (2): 229–36. PMID 4975011.
- ↑ Ting YM, Church WR, Ravikrishnan KP (1976). “Lung carcinoma superimposed on pulmonary tuberculosis”. Radiology. 119 (2): 307–12. doi:10.1148/119.2.307. PMID 1265261.
- ↑ Lee KS, Hwang JW, Chung MP, Kim H, Kwon OJ (1996). “Utility of CT in the evaluation of pulmonary tuberculosis in patients without AIDS”. Chest. 110 (4): 977–84. PMID 8874255.
- ↑ Hatipoğlu ON, Osma E, Manisali M, Uçan ES, Balci P, Akkoçlu A; et al. (1996). “High resolution computed tomographic findings in pulmonary tuberculosis”. Thorax. 51 (4): 397–402. PMC 1090675. PMID 8733492.
- ↑ 16.0 16.1 Galdermans D, Verhaert J, Van Meerbeeck J, de Backer W, Vermeire P (1990). “Broncholithiasis: present clinical spectrum”. Respir Med. 84 (2): 155–6. PMID 2371439.
- ↑ 17.0 17.1 Kowal LE, Goodman LR, Zarro VJ, Haskin ME (1983). “CT diagnosis of broncholithiasis”. J Comput Assist Tomogr. 7 (2): 321–3. PMID 6833568.
- ↑ 18.0 18.1 Conces DJ, Tarver RD, Vix VA (1991). “Broncholithiasis: CT features in 15 patients”. AJR Am J Roentgenol. 157 (2): 249–53. doi:10.2214/ajr.157.2.1853800. PMID 1853800.
- ↑ Fraser, Richard (1994). Synopsis of diseases of the chest. Philadelphia: W.B. Saunders. ISBN 0721636691.
- ↑ 20.0 20.1 Song JW, Im JG, Shim YS, Park JH, Yeon KM, Han MC (1998). “Hypertrophied bronchial artery at thin-section CT in patients with bronchiectasis: correlation with CT angiographic findings”. Radiology. 208 (1): 187–91. doi:10.1148/radiology.208.1.9646812. PMID 9646812.
- ↑ Ramakantan R, Bandekar VG, Gandhi MS, Aulakh BG, Deshmukh HL (1996). “Massive hemoptysis due to pulmonary tuberculosis: control with bronchial artery embolization”. Radiology. 200 (3): 691–4. doi:10.1148/radiology.200.3.8756916. PMID 8756916.
- ↑ 22.0 22.1 Im JG, Kim JH, Han MC, Kim CW (1990). “Computed tomography of esophagomediastinal fistula in tuberculous mediastinal lymphadenitis”. J Comput Assist Tomogr. 14 (1): 89–92. PMID 2299003.
- ↑ Fraser, Richard (1994). Synopsis of diseases of the chest. Philadelphia: W.B. Saunders. ISBN 0721636691.
- ↑ Mönig SP, Schmidt R, Wolters U, Krug B (1995). “Esophageal tuberculosis: a differential diagnostic challenge”. Am J Gastroenterol. 90 (1): 153–4. PMID 7801924.
- ↑ Larrieu AJ, Tyers GF, Williams EH, Derrick JR (1980). “Recent experience with tuberculous pericarditis”. Ann Thorac Surg. 29 (5): 464–8. PMID 7377888.
- ↑ Agrons GA, Markowitz RI, Kramer SS (1993). “Pulmonary tuberculosis in children”. Semin Roentgenol. 28 (2): 158–72. PMID 8516692.
- ↑ Leung AN, Müller NL, Pineda PR, FitzGerald JM (1992). “Primary tuberculosis in childhood: radiographic manifestations”. Radiology. 182 (1): 87–91. doi:10.1148/radiology.182.1.1727316. PMID 1727316.
- ↑ Choyke PL, Sostman HD, Curtis AM, Ravin CE, Chen JT, Godwin JD; et al. (1983). “Adult-onset pulmonary tuberculosis”. Radiology. 148 (2): 357–62. doi:10.1148/radiology.148.2.6867325. PMID 6867325.
- ↑ Hopewell PC (1995). “A clinical view of tuberculosis”. Radiol Clin North Am. 33 (4): 641–53. PMID 7610236.
- ↑ 30.0 30.1 30.2 Atasoy C, Fitoz S, Erguvan B, Akyar S (2001). “Tuberculous fibrosing mediastinitis: CT and MRI findings”. J Thorac Imaging. 16 (3): 191–3. PMID 11428422.
- ↑ 31.0 31.1 Kushihashi T, Munechika H, Motoya H, Hamada K, Satoh I, Naitoh H; et al. (1995). “CT and MR findings in tuberculous mediastinitis”. J Comput Assist Tomogr. 19 (3): 379–82. PMID 7790546.
- ↑ Johnson TM, McCann W, Davey WN (1973). “Tuberculous bronchopleural fistula”. Am Rev Respir Dis. 107 (1): 30–41. PMID 4683320.
- ↑ Hulnick DH, Naidich DP, McCauley DI (1983). “Pleural tuberculosis evaluated by computed tomography”. Radiology. 149 (3): 759–65. doi:10.1148/radiology.149.3.6647852. PMID 6647852.
- ↑ Müller NL (1993). “Imaging of the pleura”. Radiology. 186 (2): 297–309. doi:10.1148/radiology.186.2.8421723. PMID 8421723.
- ↑ Schmitt WG, Hübener KH, Rücker HC (1983). “Pleural calcification with persistent effusion”. Radiology. 149 (3): 633–8. doi:10.1148/radiology.149.3.6647839. PMID 6647839.
- ↑ Kuhlman JE, Singha NK (1997). “Complex disease of the pleural space: radiographic and CT evaluation”. Radiographics. 17 (1): 63–79. doi:10.1148/radiographics.17.1.9017800. PMID 9017800.
- ↑ Schmoldt A, Benthe HF, Haberland G (1975). “Digitoxin metabolism by rat liver microsomes”. Biochem Pharmacol. 24 (17): 1639–41. PMID http://dx.doi.org/10.1148/radiology.175.1.2315473 Check
|pmid=value (help). - ↑ Im JG, Chung JW, Han MC (1993). “Milk of calcium pleural collections: CT findings”. J Comput Assist Tomogr. 17 (4): 613–6. PMID 8331232.
- ↑ Song JW, Im JG, Goo JM, Kim HY, Song CS, Lee JS (2000). “Pseudochylous pleural effusion with fat-fluid levels: report of six cases”. Radiology. 216 (2): 478–80. doi:10.1148/radiology.216.2.r00jl09478. PMID 10924573.
- ↑ Ridley N, Shaikh MI, Remedios D, Mitchell R (1998). “Radiology of skeletal tuberculosis”. Orthopedics. 21 (11): 1213–20. PMID 9845453.
- ↑ Sharif HS, Morgan JL, al Shahed MS, al Thagafi MY (1995). “Role of CT and MR imaging in the management of tuberculous spondylitis”. Radiol Clin North Am. 33 (4): 787–804. PMID 7610245.
- ↑ 42.0 42.1 Lee G, Im JG, Kim JS, Kang HS, Han MC (1993). “Tuberculosis of the ribs: CT appearance”. J Comput Assist Tomogr. 17 (3): 363–6. PMID 8491894.
- ↑ 43.0 43.1 Adler BD, Padley SP, Müller NL (1993). “Tuberculosis of the chest wall: CT findings”. J Comput Assist Tomogr. 17 (2): 271–3. PMID 8454753.
- ↑ Glicklich M, Mendelson DS, Gendal ES, Teirstein AS (1990). “Tuberculous empyema necessitatis. Computed tomography findings”. Clin Imaging. 14 (1): 23–5. PMID 2322879.
- ↑ 45.0 45.1 Roviaro GC, Sartori F, Calabrò F, Varoli F (1982). “The association of pleural mesothelioma and tuberculosis”. Am Rev Respir Dis. 126 (3): 569–71. PMID 7125345.
- ↑ 46.0 46.1 Iuchi K, Aozasa K, Yamamoto S, Mori T, Tajima K, Minato K; et al. (1989). “Non-Hodgkin’s lymphoma of the pleural cavity developing from long-standing pyothorax. Summary of clinical and pathological findings in thirty-seven cases”. Jpn J Clin Oncol. 19 (3): 249–57. PMID 2681886.
- ↑ 47.0 47.1 47.2 Minami M, Kawauchi N, Yoshikawa K, Itai Y, Kokubo T, Iguchi M; et al. (1991). “Malignancy associated with chronic empyema: radiologic assessment”. Radiology. 178 (2): 417–23. doi:10.1148/radiology.178.2.1987602. PMID 1987602.
- ↑ Hillerdal G, Berg J (1985). “Malignant mesothelioma secondary to chronic inflammation and old scars. Two new cases and review of the literature”. Cancer. 55 (9): 1968–72. PMID 3978576.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | CT | MRI | Echocardiography or Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Special Conditions | Drug-resistant | Children |Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Active tuberculosis will kill about two of every three people affected if left untreated. Treated tuberculosis has a mortality rate of less than 5% (or less in developed countries where intensive supportive measures are available).
The standard “short” course treatment for tuberculosis (TB), if it is active, is isoniazid, rifampicin, pyrazinamide, and ethambutol for two months, then isoniazid and rifampicin alone for a further four months. The patient is considered cured at six months (although there is still a relapse rate of 2 to 3%). For latent tuberculosis, the standard treatment is six to nine months of isoniazid alone.
If the organism is known to be fully sensitive, then treatment is with isoniazid, rifampicin, and pyrazinamide for two months, followed by isoniazid and rifampicin for four months. Ethambutol need not be used.
Drugs
| First line tuberculosis drugs | ||
| 3-letter | 1-letter | Drug |
|---|---|---|
| EMB | E | ethambutol |
| INH | H | isoniazid |
| PZA | Z | pyrazinamide |
| RMP | R | rifampicin |
| STM | S | streptomycin |
| Second line tuberculosis drugs | ||
| CIP | (none) | ciprofloxacin |
| MXF | (none) | moxifloxacin |
| PAS | P | p-aminosalicylic acid |
All first-line anti-tuberculous drug names have a standard three-letter and a single-letter abbreviation:
- streptomycin is STM or S,
- isoniazid is INH or H,
- rifampicin is RMP or R,
- ethambutol is EMB or E,
- pyrazinamide is PZA or Z.
The US commonly uses abbreviations and names that are not internationally recognised: rifampicin is called rifampin and abbreviated RIF; streptomycin is commonly abbreviated SM.
Drug regimens are similarly abbreviated in a standardised manner. The drugs are listed using their single letter abbreviations (in the order given above, which is roughly the order of introduction into clinical practice). A prefix denotes the number of months the treatment should be given for; a subscript denotes intermittent dosing (so 3 means three times a week) and no subscript means daily dosing. Most regimens have an initial high-intensity phase, followed by a continuation phase (also called a consolidation phase or eradication phase): the high-intensity phase is given first, then the continuation phase, the two phases divided by a slash.
So,
- 2HREZ/4HR3
means isoniazid, rifampicin, ethambutol, pyrazinamide daily for two months, followed by four months of isoniazid and rifampicin given three times a week.
These standard abbreviations are used in the rest of this article.
There are six classes of second-line drugs (SLDs) used for the treatment of TB. A drug may be classed as second-line instead of first-line for one of two possible reasons: it may be less effective than the first-line drugs (e.g., p-aminosalicylic acid); or, it may have toxic side-effects (e.g., cycloserine); or it may be unavailable in many developing countries (e.g., fluoroquinolones):
- aminoglycosides: e.g., amikacin (AK), kanamycin;
- polypeptides: e.g., capreomycin, viomycin, enviomycin;
- fluoroquinolones: e.g., ciprofloxacin (CIP), moxifloxacin (MXF);
- thioamides: e.g. ethionamide, prothionamide
- cycloserine (the only antibiotic in its class);
- p-aminosalicylic acid (PAS or P).
Other drugs that may be useful, but are not on the WHO list of SLDs:
- rifabutin
- macrolides: e.g., clarithromycin (CLR);
- linezolid (LZD);
- thioacetazone (T);
- thioridazine;
- arginine;
- vitamin D;
- R207910.
These drugs may be considered “third-line drugs” and are listed here either because they are not very effective (e.g., clarithromycin) or because their efficacy has not been proven (e.g., linezolid, R207910). Rifabutin is effective, but is not included on the WHO list because for most developing countries, it is impractically expensive.
The standard regimen
Rationale and evidence for the standard regimen
Tuberculosis has been treated with combination therapy for over fifty years. Drugs are not used singly (except in latent TB or chemoprophylaxis), and regimens that use only single drugs result in the rapid development of resistance and treatment failure.[1][2] The rationale for using multiple drugs to treat TB are based on simple probability. The frequency of spontaneous mutations that confer resistance to an individual drug are well known: 1 in 107 for EMB, 1 in 108 for STM and INH, and 1 in 1010 for RMP.[3]
A patient with extensive pulmonary TB has approximately 1012 bacteria in his body, and therefore will probably be harboring approximately 105 EMB-resistant bacteria, 104 STM-resistant bacteria, 104 INH-resistant bacteria and 10² RMP-resistant bacteria. Resistance mutations appear spontaneously and independently, so the chances of him harbouring a bacterium that is spontaneously resistant to both INH and RMP is 1 in 106, and the chances of him harbouring a bacterium that is spontaneously resistant to all four drugs is 1 in 1011. This is, of course, an oversimplification, but it is a useful way of explaining combination therapy.
There are other theoretical reasons for supporting combination therapy. The different drugs in the regimen have different modes of action: INH and EMB are bacteriostatic (they stop the bacteria replicating, but do not kill them); RMP is bacteriocidal (it actually kills bacteria).
All TB regimens in use were 18 months or longer until the appearance of rifampicin. In 1953, the standard UK regimen was 3SPH/15PH or 3SPH/15SH2. Between 1965 and 1970, EMB replaced PAS. RMP began to be used to treat TB in 1968 and the BTS study in the 1970s showed that 2HRE/7HR was efficacious. In 1984, a BTS study showed that 2HRZ/4HR was efficacious,[4] with a relapse rate of less than 3% after two years.[5] In 1995, with the recognition that INH resistance was increasing, the BTS recommended adding EMB or STM to the regimen: 2HREZ/4HR or 2SHRZ/4HR, which are the regimens currently recommended. The WHO also recommend a six month continuation phase of HR if the patient is still culture positive after 2 months of treatment (approximately 15% of patients with fully-sensitive TB) and for those patients who have extensive bilateral cavitation at the start of treatment.
Monitoring and DOTS
DOTS stands for “Directly Observed Therapy, Short-course” and is a major plank in the WHO global TB eradication programme. The WHO advises that all TB patients should have at least the first two months of their therapy observed (and preferably the whole of it observed): this means an independent observer watching tuberculosis patients swallow their anti-TB therapy. The independent observer is often not a healthcare worker and may be a shopkeeper or a tribal elder or similar senior person within that society. DOTS is used with intermittent dosing (thrice weekly or 2HREZ/4HR3). Twice weekly dosing is effective[6] but not recommended by the WHO, because there is no margin for error (accidentally omitting one dose per week results in once weekly dosing, which is ineffective).
Treatment with properly implemented DOTS has a success rate exceeding 95% and prevents the emergence of further multi-drug resistant strains of tuberculosis.
Some people recommend monthly surveillance until cultures convert to negative; this does not form any part of the UK or WHO recommendations for TB. If cultures are positive or symptoms do not resolve after three months of treatment, it is necessary to re-evaluate the patient for drug-resistant disease or nonadherence to drug regimen. If cultures do not convert to negative despite three months of therapy, consider initiating directly observed therapy.
Extra-pulmonary tuberculosis
Tuberculosis not affecting the lungs is called extra-pulmonary tuberculosis. Disease of the central nervous system is specifically excluded from this classification.
The UK and WHO recommendation is 2HREZ/4HR; the US recommendation is 2HREZ/7HR. There is good evidence from randomised-controlled trials to say that in tuberculous lymphadenitis[7] and in TB of the spine,[8][9][10] the six month regimen is equivalent to the nine month regimen; the US recommendation is therefore not supported by the evidence.
Up to 25% of patients with TB of the lymph nodes (TB lymphadenitis) will get worse on treatment before they get better and this usually happens in the first few months of treatment. A few weeks after starting treatment, lymph nodes often start to enlarge, and previously solid lymph nodes may become fluctuant. This should not be interpreted as failure of therapy and is a common reason for patients (and their physicians) to panic unnecessarily. With patience, two to three months into treatment the lymph nodes start to shrink again and re-aspiration or re-biopsy of the lymph nodes is unnecessary: if repeat microbiological studies are ordered, they will show the continued presence of viable bacteria with the same sensitivity pattern, which further adds to the confusion: physicians inexperienced in the treatment of TB will then often add second-line drugs in the belief that the treatment is not working. In these situations, all that is required is re-assurance. Steroids may be useful in resolving the swelling, especially if it is painful, but they are unnecessary. Additional antibiotics are unnecessary and the treatment regimen does not need to be lengthened.
Tuberculosis of the central nervous system
Tuberculosis may affect the central nervous system (meninges, brain or spinal cord) in which case it is called TB meningitis, TB cerebritis, and TB myelitis respectively; the standard treatment is 12 months of drugs (2HREZ/10HR) and steroid are mandatory. Diagnosis is difficult as CSF culture is positive in less than half of cases, and therefore a large proportion of cases are treated on the basis of clinical suspicion alone. PCR of CSF does not significantly improve the microbiology yield; culture remains the most sensitive method and a minimum of 5 ml (preferably 20 ml) of CSF should be sent for analysis. TB cerebritis (or TB of the brain) may require brain biopsy in order to make the diagnosis, because the CSF is commonly normal: this is not always available and even when it is, some clinicians would debate whether it is justified putting a patient through such an invasive and potentially dangerous procedure when a trial of anti-TB therapy may yield the same answer; probably the only justification for brain biopsy is when drug-resistant TB is suspected. It is possible that shorter durations of therapy (e.g. six months) may be sufficient to treat TB meningitis, but no clinical trial has addressed this issue. The CSF of patients with treated TB meningitis is commonly abnormal even at 12 months;[11] the rate of resolution of the abnormality bears no correlation with clinical progress or outcome,[12] and is not an indication for extending or repeating treatment; repeated sampling of CSF by lumbar puncture to monitor treatment progress should therefore not be done.
Although TB meningitis and TB cerebritis are classified together, the experience of many clinicians is that their progression and response to treatment is not the same. TB meningitis usually responds well to treatment, but TB cerebritis may require prolonged treatment (up to two years) and the steroid course needed is often also prolonged (up to six months). Unlike TB meningitis, TB cerebritis often required repeated CT or MRI imaging of the brain to monitor progress.
CNS TB may be secondary to blood-borne spread: therefore some experts advocate the routine sampling of CSF in patients with miliary TB.[13]
The anti-TB drugs that are most useful for the treatment of CNS TB are:
- INH (CSF penetration 100%)
- RMP (10–20%)
- EMB (25–50% inflamed meninges only)
- PZA (100%)
- STM (20% inflamed meninges only)
- LZD (20%)
- Cycloserine (80–100%)
- Ethionamide (100%)
- PAS (10–50%) (inflamed meninges only)
The use of steroids is routine in TB meningitis (see section below).
Steroids
The usefulness of corticosteroids (e.g., prednisolone or dexamethasone) in the treatment is TB is proven for TB meningitis and TB pericarditis. The dose for TB meningitis is dexamethasone 8 to 12mg daily tapered off over six weeks (for those who prefer more precise dosing, please see Thwaites, 2004[14]). The dose for pericarditis is prednisolone 60mg daily tapered off over four to eight weeks.
Steroids may be of temporary benefit in pleurisy, extremely advanced TB, and TB in children:
- Pleurisy: prednisolone 20 to 40mg daily tapered off over 4 to 8 weeks
- Extremely advanced TB: 40 to 60mg daily tapered off over 4 to 8 weeks
- TB in children: 2 to 5mg/kg/day for one week, 1mg/kg/day the next week, then tapered off over 5 weeks
Steroids may be of benefit in peritonitis, miliary disease, laryngeal TB, lymphadenitis and genitourinary disease, but the evidence is scant and the routine use of steroids cannot be recommended. Steroid treatment in these patients should be considered on a case by case basis by the attending physician.
Thalidomide may be of benefit in TB meningitis and has been used in cases where patients have failed to respond to steroid treatment.[15]
Non-compliance
Patients who take their TB treatment in an irregular and unreliable way are at greatly increased risk of treatment failure, relapse and the development of drug-resistant TB strains.
There are variety of reasons why patients fail to take their medication. The symptoms of TB commonly resolve within a few weeks of starting TB treatment and many patients then lose motivation to continue taking their medication. Regular follow-up is important to check on compliance and to identify any problems patients are having problems with their medication. Patients need to be told of the importance of taking their tablets regularly, and the importance of completing treatment, because of the risk of relapse or drug-resistance developing otherwise.
One of the main complaints is the bulkiness of the tablets. The main offender is PZA (the tablets being the size of horse tablets). PZA syrup may be offered as a substitute, or if the size of the tablets is truly an issue and liquid preparations are not available, then PZA can be omitted altogether. If PZA is omitted, the patient should be warned that this results in a significant increase in the duration of treatment (details of regimens omitting PZA are given below).
The other complaint is that the medicines must be taken on an empty stomach to facilitate absorption. This can be difficult for patients to follow (for example, shift workers who take their meals at irregular times) and may mean the patient waking up an hour earlier than usual everyday just to take medication. The rules are actually less stringent than many physicians and pharmacists realise: the issue is that the absorption of RMP is reduced if taken with fat, but is unaffected by carbohydrate, protein,[16] or antacids.[17] So the patient can in fact have his or her medication with food as long as the meal does not contain fat or oils (e.g., a cup of black coffee or toast with jam and no butter).[18] Taking the medicines with food also helps ease the nausea that many patients feel when taking the medicines on an empty stomach. The effect of food on the absorption of INH is not clear: two studies have shown reduced absorption with food[19][20] but one study showed no difference.[21] There is a small effect of food on the absorption of PZA and of EMB that is probably not clinically important.[22][23]
It is possible to test urine for isoniazid and rifampicin levels in order to check for compliance. The interpretation of urine analysis is based on the fact that isoniazid has a longer half-life than rifampicin:
- urine positive for isoniazid and rifampicin patient probably fully compliant
- urine positive for isoniazid only patient has taken his medication in the last few days preceding the clinic appointment, but had not yet taken a dose that day.
- urine positive for rifampicin only patient has omitted to take his medication the preceding few days, but did take it just before coming to clinic.
- urine negative for both isoniazid and rifampicin patient has not taken either medicine for a number of days
In countries where doctors are unable to compel patients to take their treatment (e.g., the UK), some say that urine testing only results in unhelpful confrontations with patients and does not help increase compliance. In countries where legal measures can be taken to force patients to take their medication (e.g., the US), then urine testing can a useful adjunct in assuring compliance.
RMP colours the urine and all bodily secretions (tears, sweat, etc.) an orange-pink colour and this can be a useful proxy if urine testing is not available (although this colour fades approximately six to eight hours after each dose).
Adverse effects
For information on adverse effects of individual anti-TB drugs, please refer to the individual articles for each drug.
The relative incidence of major adverse effects has been carefully described:[24]
- INH 0.49 per hundred patient months
- RMP 0.43
- EMB 0.07
- PZA 1.48
- All drugs 2.47
This works out to an 8.6% risk that any one patient will need to have his drug therapy changed during the course of standard short-course therapy (2HREZ/4HR). The people identified to be most at risk of major adverse side effects in this study were:
- age >60,
- females,
- HIV positive patients, and
- Asians.
It can be extremely difficult identifying which drug is responsible for which side effect, but the relative frequency of each is known.[25] The offending drugs are given in decreasing order of frequency:
- Thrombocytopaenia: RMP
- Neuropathy: INH
- Vertigo: STM
- Hepatitis: PZA, RMP, INH
- Rash: PZA, RMP, EMB
Thrombocytopaenia is only caused by RMP and no test dosing need be done. Regimens omitting RMP are discussed below. Please refer to the entry on rifampicin for further details.
The most frequent cause of neuropathy is INH. The peripheral neuropathy of INH is always a pure sensory neuropathy and finding a motor component to the peripheral neuropathy should always prompt a search for an alternative cause. Once a peripheral neuropathy has occurred, INH must be stopped and pyridoxine should be given at a dose of 50mg thrice daily. Simply adding high dose pyridoxine to the regimen once neuropathy has occurred will not stop the neuropathy from progressing. Patients at risk of peripheral neuropathy from other causes (diabetes mellitus, alcoholism, renal failure, malnutrition, pregnancy, etc.) should all be given pyridoxine] 10mg daily at the start of treatment. Please refer to the entry on isoniazid for details on other neurological side effects of INH.
Rashes are most frequently due to PZA, but can occur with any of the TB drugs. Test dosing using the same regimen as detailed below for hepatitis may be necessary to determine which drug is responsible.
Itching RMP commonly causes itching without a rash in the first two weeks of treatment: treatment should not be stopped and the patient should be advised that the itch usually resolves on its own. Short courses of sedative antihistamines such as chlorpheniramine may be useful in alleviating the itch.
Fever during treatment can be due to a number of causes. It can occur as a natural effect of tuberculosis (in which case it should resolve within three weeks of starting treatment). Fever can be a result of drug resistance (but in that case the organism must be resistant to two or more of the drugs). Fever may be due to a superadded infection or additional diagnosis (patients with TB are not exempt from getting influenza and other illnesses during the course of treatment). In a few patients, the fever is due to drug allergy. The clinician must also consider the possibility that the diagnosis of TB is wrong. If the patient has been on treatment for more than two weeks and if the fever had initially settled and then come back, it is reasonable to stop all TB medication for 72 hours. If the fever persists despite stopping all TB medication, then the fever is not due to the drugs. If the fever disappears off treatment, then the drugs need to be tested individually to determine the cause. The same scheme as is used for test dosing for drug-induced hepatitis (described below) may be used. The drug most frequently implicated as causing a drug fever is RMP: details are given in the entry on rifampicin.
Drug-induced hepatitis
The single biggest problem with TB treatment is drug-induced hepatitis, which has a mortality rate of around 5%.[26] Three drugs can induce hepatitis: PZA, INH and RMP (in decreasing order of frequency).[2][27] It is not possible to distinguish between these three causes based purely on of signs and symptoms. Test dosing must be carried out to determine which drug is responsible (this is discussed in detail below).
Liver function tests (LFTs) should be checked at the start of treatment, but, if normal, need not be checked again; the patient need only be warned of the symptoms of hepatitis. Some clinicians insist on regular monitoring of LFT’s while on treatment, and in this instance, tests need only be done two weeks after starting treatment and then every two months thereafter, unless any problems are detected.
Elevations in bilirubin must be expected with RMP treatment (RMP blocks bilirubin excretion) and usually resolve after 10 days (liver enzyme production increases to compensate). Isolated elevations in bilirubin can be safely ignored.
Elevations in liver transaminases (ALT and AST) are common in the first three weeks or treatment. If the patient is asymptomatic and the elevation is not excessive then no action need be taken; some experts suggest a cut-off of four times the upper limit of normal, but there is no evidence to support this particular number over and above any other number. Some experts consider that treatment should only be stopped if jaundice becomes clinically evident.
If clinically significant hepatitis occurs while on TB treatment, then all the drugs should be stopped until the liver transaminases return to normal. If the patient is so ill that TB treatment cannot be stopped, then STM and EMB should be given until the liver transaminases return to normal (these two drugs are not associated with hepatitis).
Fulminant hepatitis can occur in the course of TB treatment, but is fortunately rare; emergency liver transplantation may be necessary and deaths do occur.
Test dosing for drug-induced hepatitis
Drugs should be re-introduced individually. This cannot be done in an outpatient setting, and must be done under close observation. A nurse must be present to take patient’s pulse and blood pressure at 15 minutes intervals for a minimum or four hours after each test dose is given (most problems will occur within six hours of test dosing, if they are going to occur). Patients can become very suddenly unwell and access to intensive care facilities must be available. The drugs should be given in this order:
- Day 1: INH at 1/3 or 1/4 dose
- Day 2: INH at 1/2 dose
- Day 3: INH at full dose
- Day 4: RMP at 1/3 or 1/4 dose
- Day 5: RMP at 1/2 dose
- Day 6: RMP at full dose
- Day 7: EMB at 1/3 or 1/4 dose
- Day 8: EMB at 1/2 dose
- Day 9: EMB at full dose
No more than one test dose per day should be given, and all other drugs should be stopped while test dosing is being done. So on day 4, for example, the patient only receives RMP and no other drugs are given. If the patient completes the nine days of test dosing, then it is reasonable to assume that PZA has caused the hepatitis and no PZA test dosing need be done.
The reason for using the order for testing drugs is because the two most important drugs for treating TB are INH and RMP, so these are tested first: PZA is the most likely drug to cause hepatitis and is also the drug that can be most easily omitted. EMB is useful when the sensitivity pattern of the TB organism are not known and can be omitted if the organism is known to be sensitive to INH. Regimens omitting each of the standard drugs are listed below.
The order in which the drugs are tested can be varied according to the following considerations:
- The most useful drugs (INH and RMP) should be tested first, because the absence of these drugs from a treatment regimen severely impairs its efficacy.
- The drugs most likely to be causing the reaction should be tested as late as possible (and possibly need not be tested at all). The avoids rechallenging patients with a drug to which they have already had a (possibly) dangerous adverse reaction.
A similar scheme may be used for other adverse effects (such as fever and rash), using similar principles.
Deviations from the standard regimen
There is evidence supporting some deviations from the standard regimen when treating pulmonary TB. Sputum culture positive patients who are smear negative at the start of treatment do well with only 4 months of treatment (this has not been validated for HIV-positive patients); and sputum culture negative patients do well on only 3 months of treatment (possibly because some of these patients never had TB at all).[28] It is unwise to treat patients for only three or four months, but all TB physicians will have patients who stop their treatment early (for whatever reason), and it can be re-assuring to know that sometimes retreatment is unnecessary. Elderly patients who are already taking a large number of tablets may be offered 9HR, omitting PZA which is the bulkiest part of the regimen.
It may not always be necessary to treat with four drugs from the beginning. An example might be a close contact of a patient known to have a fully-sensitive strain of tuberculosis: in this case, it is acceptable to use 2HRZ/4HR (omitting EMB and STM) in the expectation that their strain will be INH susceptible also. Indeed, this was previously the recommended standard regimen in many countries until the early 1990s, when isoniazid-resistance rates increased.
TB involving the brain or spinal cord (meningitis, encephalitis, etc.) is currently treated with 2HREZ/10HR (12 months of treatment in total), but there is no evidence to say that this is superior to 2HREZ/4HR, it is merely that no-one has been brave enough to do the clinic trial that answers the question if the short course is equivalent.
Regimens omitting isoniazid
Isoniazid resistance in the UK accounts for approximately 6 to 7% of isolates at time of writing (25 Feb 2006). Worldwide, it is the most common type of resistance encountered, hence the current recommendation of using HREZ at the beginning of treatment until sensitivities are known. It is useful to know of current reported outbreaks (like the current outbreak of INH-resistant TB in London).
If a patient is discovered to be infected with an isoniazid-resistant strain of TB having completed 2 months of HREZ, then he should be changed to RE for a further 10 months. If the patient is intolerant to isoniazid, then a reasonable regimen is 2REZ/10RE (although 2REZ/7RE may be acceptable if the patient is well supervised). The US recommendation is 6RZE with the option of adding a quinolone such as moxifloxacin. The level of evidence for all these regimens is poor, and there is little to recommend one over the other.
Regimens omitting rifampicin
It is rare for TB strains to be resistant to rifampicin without being resistant to isoniazid, but rifampicin intolerance is not uncommon (hepatitis or thrombocytopaenia being the most common reasons for stopping rifampicin). Of the first-line drugs, rifampicin is also the most expensive, and in the poorest countries, regimens omitting rifampicin are therefore often used. Rifampicin is the most potent sterilising drug available for the treatment of tuberculosis and all treatment regimens that omit rifampicin are significantly longer than the standard regimen.
The UK recommendation is 18HE or 12HEZ. The US recommendation is 9 to 12HEZ, with option of adding a quinolone (for example, MXF).
Regimens omitting pyrazinamide
PZA is a common cause of rash, hepatitis and of painful arthralgia in the HREZ regimen, and can be safely stopped in those patients who are intolerant to it. Isolated PZA resistance is uncommon in M. tuberculosis, but M. bovis is innately resistant to PZA. PZA is not crucial to the treatment of fully-sensitive TB, and its main value is in shortening the total treatment duration from nine months to six.
There is good evidence from UK trials that a regimen of 9HR is adequate for M. tuberculosis; this is also the first-line regimen used to treat M. bovis.
Regimens omitting ethambutol
EMB intolerance or resistance is rare. If a patient is truly intolerant or is infected with TB that is resistant to EMB, then 2HRZ/4HR is a perfectly acceptable regimen. EMB has no part to play in the treatment of TB that is sensitive to both INH and RMP, and the only reason for including it in the initial regimen is because of increasing rates of INH resistance. If INH resistance rates are known to be low, or if the infecting TB strain is known to be INH-sensitive, then there is no need to use EMB anyway.
Tuberculosis and other conditions
Liver disease
It should be noted that patients with alcoholic liver disease are at an increased risk of tuberculosis. The incidence of tuberculous peritonitis is particularly high in patients with cirrhosis of the liver.
No dosing change needs to be made in the dosing of patients with known liver disease, unless the liver disease is thought to have been caused by TB treatment. Some authorities recommend avoiding PZA in patients with known liver disease, because of the five first-line drugs, PZA has the highest risk of producing drug-induced hepatitis.
Patients with pre-existing liver disease should have their liver function tests monitored regularly throughout TB treatment.
Drug-induced hepatitis is discussed in a separate section above.
Pregnancy
Pregnancy itself is not a risk factor for TB.
Rifampicin makes hormonal contraception less effective, so additional precautions need to be taken for birth control during tuberculosis treatment.
Untreated TB in pregnancy is associated with an increased risk of miscarriage and major foetal abnormality, and treatment of pregnant women. The US guidelines recommend omitting PZA when treating TB in pregnancy; the UK and WHO guidelines make no such recommendation. There is extensive experience with the treatment of pregnant women with TB and no toxic effect of PZA in pregnancy has ever been found. High doses of RMP (much higher than used in humans) causes neural tube defects in animals, but no such effect has ever been found in humans. There may be an increased risk of hepatitis in pregnancy and during the puerperium. It is prudent to advise all women of child-bearing age to avoid getting pregnant until TB treatment is completed.
Aminoglycosides (STM, capreomycin, amikacin) should be used with caution in pregnancy, because they may cause deafness in the unborn child. The attending physician must weigh the benefits of treating the mother against the potential harm to the baby, and good outcomes have been reported in children whose mothers were treated with aminoglycosides.[29]
Kidney disease
Patients with renal failure have a 10 to 30-fold increase in risk of getting TB. Patients with kidney disease who are being given immunosuppressive drugs or are being considered for transplant should be considered for treatment of latent tuberculosis if appropriate.
Aminoglycosides (STM, capreomycin and amikacin) should be avoided in patients with mild to severe kidney problems because of the increased risk of damage to the kidneys. If the use of aminoglycosides cannot be avoided (e.g., in treating drug-resistant TB) then serum levels must be closely monitored and the patient warned to report any side-effects (deafness in particular). If patient have end-stage renal failure and have no useful remaining kidney function, then aminoglycosides can be used, but only if drug levels can be easily measured (often only amikacin levels can be measured).
In mild renal impairment, no change needs to be made in dosing any of the other drugs routinely used in the treatment of TB. In severe renal insufficiency (GFR<30), the EMB dose should be halved (or avoided altogether). The PZA dose is 20mg/kg/day (UK recommendation) or three-quarters the normal dose (US recommendation), but not much published evidence is available to support this.
When using 2HRZ/4HR in patients on dialysis, the drugs should be given daily during the initial high-intensity phase. In the continuation phase, the drugs should be given at the end of each haemodialysis session and no dose should be taken on non-dialysis days.
HIV
In patients with HIV, treatment for the HIV should be delayed until TB treatment is completed, if possible.
The current UK guidance (provided by the British HIV Association) is
- CD4 count over 200—delay treatment until the six months of TB treatment are complete.
- CD4 count 100 to 200—delay treatment until the initial two month intensive phase of therapy is complete
- CD4 count less than 100—the situation is unclear and patients should be enrolled in clinical trials examining this question. There is evidence that if these patients are managed by a specialist in both TB and HIV then outcomes are not compromised for either disease.[30]
If HIV treatment has to be started while a patient is still on TB treatment, then the advice of a specialist HIV pharmacist should be sought. In general, there is no significant interactions with the NRTI‘s. Nevirapine should not be used with rifampicin. Efavirenz may be used, but dose used depends on the patient’s weight (600mg daily if weight less than 50kg; 800mg daily if weight greater than 50kg). Efavirenz levels should be checked early after starting treatment (unfortunately, this is not a service routinely offered in the US, but is readily available in the UK). The protease inhibitors must be avoided if at all possible.
Thioacetazone must not be used because the risk of potentially fatal exfoliative dermatitis.
Epilepsy
INH may be associated with an increased risk of seizures. Pyridoxine 10mg daily should be given to all epileptics taking INH. There is no evidence that INH causes seizures in patients who are not epileptic.
TB treatment involves numerous drug interactions with anti-epileptic drugs and serum drug levels should be closely monitored. There are serious interactions between rifampicin and carbamazepine, rifampicin and phenytoin, and rifampicin and sodium valproate. The advice of a pharmacist should always be sought.
Drug-resistant tuberculosis (MDR- and XDR-TB)
Definitions
Multi-drug resistant tuberculosis (MDR-TB) is defined as TB that is resistant at least to INH and RMP. Isolates that are multiply-resistant to any other combination of anti-TB drugs but not to INH and RMP are not classed as MDR-TB.
As of Oct 2006, “Extensively drug-resistant tuberculosis” (XDR-TB) is defined as MDR-TB that is resistant to quinolones and also to any one of kanamycin, capreomycin, or amikacin.[31] The old case definition of XDR-TB is MDR-TB that is also resistant to three or more of the six classes of second-line drugs.[32] This definition should no longer be used, but is included here because many older publications refer to it.
The principles of treatment for MDR-TB and for XDR-TB are the same. The main difference is that XDR-TB is associated with a much higher mortality rate than MDR-TB, because of a reduced number of effective treatment options.[32] The epidemiology of XDR-TB is currently not well studied, but it is believed that XDR-TB does not transmit easily in healthy populations, but is capable of causing epidemics in populations which are already stricken by HIV and therefore more susceptible to TB infection.[33]
Epidemiology of drug-resistant TB
A 1997 survey of 35 countries found rates above 2% in about a third of the countries surveyed. The highest rates were in the former USSR, the Baltic states, Argentina, India and China, and was associated with poor or failing national Tuberculosis Control programmes. Likewise, the appearance of high rates of MDR-TB in New York city the early 1990s was associated with the dismantling of public health programmes by the Reagan administration.[34][35]
MDR-TB can develop in the course of the treatment of fully sensitive TB and this is always the result of patients missing doses or failing to complete a course of treatment.
Thankfully, MDR-TB strains appear to be less fit and less transmissible. It has been known of many years that INH-resistant TB is less virulent in guinea pigs, and the epidemiological evidence is that MDR strains of TB do not dominate naturally. A study in Los Angeles found that only 6% of cases of MDR-TB were clustered. This should not be a cause for complacency: it must be remembered that MDR-TB has a mortality rate comparable to lung cancer. It must also be remembered that people who have weakened immune systems (because of diseases such as HIV or because of drugs) are more susceptible to catching TB.
There is currently an epidemic of XDR-TB South Africa. The outbreak was first reported as a cluster of 53 patients in a rural hospital in KwaZulu-Natal of whom 52 died.[33] What was particularly worrying was that the mean survival from sputum specimen collection to death was only 16 days and that the majority of patients had never previously received treatment for tuberculosis. This is the epidemic for which the acronym XDR-TB was first used, although TB strains that fulfil the current definition have been identified retrospectively,[36][37] this was the largest group of linked cases ever found. Since the initial report in September 2006,[38] cases have now been reported in most provinces in South Africa. As of 16 March 2007, there were 314 cases reported, with 215 deaths.[39] It is clear that the spread of this strain of TB is closely associated with a high prevalence of HIV and poor infection control; in other countries where XDR-TB strains have arisen, drug-resistance has arisen from mismanagement of cases or poor patient compliance with drug treatment instead of being transmitted from person to person.[40] This strain of TB does not respond to any of the drugs currently available in South Africa for first- or second-line treatment. It is now clear that the problem has been around for much longer than health department officials have suggested, and is far more extensive.[41] By 23 Nov 2006, 303 cases of XDR-TB had been reported, of which 263 were in KwaZulu-Natal.[42] Serious thought has been put to isolation procedures that may deny some patients their human rights, but which may be necessary to prevent further spread of this strain of TB.[43]
Treatment of MDR-TB
The treatment and prognosis of MDR-TB are much more akin to that for cancer than to that for infection. It has a mortality rate of up to 80%, which depends on a number of factors, including
- How many drugs the organism is resistant to (the fewer the better),
- How many drugs the patient is given (Patients treated with five or more drugs do better),
- Whether an injectable drug is given or not (it should be given for the first three months at least),
- The expertise and experience of the physician responsible,
- How co-operative the patient is with treatment (treatment is arduous and long, and requires persistence and determination on the part of the patient),
- Whether the patient is HIV positive or not (HIV co-infection is associated with an increased mortality).
Treatment courses are generally measured in months to years; it may require surgery, and despite that, the death rates remain still high despite optimal treatment. That said, good outcomes are still possible.[44]
The treatment of MDR-TB must be undertaken by a physician experienced in the treatment of MDR-TB. Mortality and morbidity in patients treated in non-specialist centres is significantly inferior to those patients treated in specialist centres.
In addition to the obvious risks (i.e., known exposure to a patient with MDR-TB), risk factors for MDR-TB include male sex, HIV infection, previous incarceration, failed TB treatment, failure to respond to standard TB treatment, and relapse following standard TB treatment.
Treatment of MDR-TB must be done on the basis of sensitivity testing: it is impossible to treat such patients without this information. If treating a patient with suspected MDR-TB, the patient should be started on SHREZ+MXF+cycloserine pending the result of laboratory sensitivity testing.
A gene probe for rpoB is available in some countries and this serves as a useful marker for MDR-TB, because isolated RMP resistance is rare (except when patients have a history of being treated with rifampicin alone). If the results of a gene probe (rpoB) are known to be positive, then it is reasonable to omit RMP and to use SHEZ+MXF+cycloserine. The reason for maintaining the patient on INH is that INH is so potent in treating TB that it is foolish to omit it until there is microbiological proof that it is ineffective (even though isoniazid resistance so commonly occurs with rifampicin resistance).
When sensitivities are known and the isolate is confirmed as resistant to both INH and RMP, five drugs should be chosen in the following order (based on known sensitivities):
- an aminoglycoside (e.g., amikacin, kanamycin) or polypeptide antibiotic (e.g., capreomycin)
- PZA
- EMB
- a fluoroquinolones: moxifloxacin is preferred to ciprofloxacin or ofloxacin;
- rifabutin
- cycloserine
- a thioamide: prothionamide or ethionamide
- PAS
- a macrolide: e.g., clarithromycin
- linezolid
- high-dose INH (if low-level resistance)
- interferon-γ
- thioridazine
Drugs are placed nearer the top of the list because they are more effective and less toxic; drugs are placed nearer the bottom of the list because they are less effective or more toxic, or more difficult to obtain.
Resistance to one drug within a class generally means resistance to all drugs within that class, but a notable exception is rifabutin: rifampicin-resistance does not always mean rifabutin-resistance and the laboratory should be asked to test for it. It is only possible to use one drug within each drug class. If it is difficult finding five drugs to treat then the clinician can request that high level INH-resistance be looked for. If the strain has only low level INH-resistance (resistance at 1.0mg/l INH, but sensitive at 0.2mg/l INH), then high dose INH can be used as part of the regimen. When counting drugs, PZA and interferon count as zero; that is to say, when adding PZA to a four drug regimen, you must still choose another drug to make five. It is not possible to use more than one injectable (STM, capreomycin or amikacin), because the toxic effect of these drugs is additive: if possible, the aminoglycoside should be given daily for a minimum of three months (and perhaps thrice weekly thereafter). Ciprofloxacin should not be used in the treatment of tuberculosis if other fluoroquinolones are available.[45]
There is no intermittent regimen validated for use in MDR-TB, but clinical experience is that giving injectable drugs for five days a week (because there is no-one available to give the drug at weekends) does not seem to result in inferior results. Directly observed therapy certainly helps to improve outcomes in MDR-TB and should be considered an integral part of the treatment of MDR-TB.[46]
Response to treatment must be obtained by repeated sputum cultures (monthly if possible). Treatment for MDR-TB must be given for a minimum of 18 months and cannot be stopped until the patient has been culture-negative for a minimum of nine months. It is not unusual for patients with MDR-TB to be on treatment for two years or more.
Patients with MDR-TB should be isolated in negative-pressure rooms, if possible. Patients with MDR-TB should not be accommodated on the same ward as immunosuppressed patients (HIV infected patients, or patients on immunosuppressive drugs). Careful monitoring of compliance with treatment is crucial to the management of MDR-TB (and some physicians insist on hospitalisation if only for this reason). Some physicians will insist that these patients are isolated until their sputum is smear negative, or even culture negative (which may take many months, or even years). Keeping these patients in hospital for weeks (or months) on end may be a practical or physical impossibility and the final decision depends on the clinical judgement of the physician treating that patient. The attending physician should make full use of therapeutic drug monitoring (particularly of the aminoglycosides) both to monitor compliance and to avoid toxic effects.
Some supplements may be useful as adjuncts in the treatment of tuberculosis, but the for the purposes of counting drugs for MDR-TB, they count as zero (if you already have four drugs in the regimen, it may be beneficial to add arginine or vitamin D or both, but you still need another drug to make five).
The drugs listed below have been used in desperation and it is uncertain whether they are effective at all. They are used when it is not possible to find five drugs from the list above.
The follow drugs are experimental compounds that are not commercially available, but which may be obtained from the manufacturer as part of a clinical trial or on a compassionate basis. Their efficacy and safety are unknown:
- PA-824[57] (manufactured by PathoGenesis Corporation, Seattle, Washington)
- R207910[58] (under development by Johnson & Johnson)
In extremely resistant disease, surgery is sometimes the last port of call. The centre with the largest experience in this is the National Jewish Medical and Research Center in Denver, Colorado. In 17 years of experience, they have performed 180 operations; of these, 98 were lobectomies, 82 were pneumonectomies. There is a 3.3% operative mortality, with an additional 6.8% dying following the operation; 12% experienced significant morbidity (particularly extreme breathlessness). Of 91 patients who were culture positive before surgery, only 4 were culture positive after surgery.
Patients who fail treatment
Patients who respond to treatment and appear to be cured after completing a course of TB treatment are not classed as treatment failures, but as relapses and are discussed in a separate section below.
Patients are said to have failed treatment if (1) they fail to respond to treatment (cough and sputum production persisting throughout the whole of treatment), or (2) who only experience a transient response to treatment (the patient gets better at first, but then get worse again, all the while on treatment). Patients who fail treatment must be distinguished from patients who relapse. A patient is said to relapse if he gets better while on treatment and only gets worse again after stopping treatment; patients who relapse are discussed in a separate section below.
It is very uncommon for patients not to respond to TB treatment at all (even transiently), because this implies resistance at base-line to all of the drugs in the regimen. Patients who fail to get any response at all while on treatment should first of all be questioned very closely about whether or not they have been taking their medicines, and perhaps even be admitted to hospital to be observed taking their treatment. Blood or urine samples may be taken to check for malabsorption of TB drugs. If it can be shown that they are fully compliant with their medication, then the probability that they have another diagnosis (perhaps in addition to the diagnosis of TB) is very high. These patients should have their diagnosis carefully reviewed and specimens obtained for TB culture and sensitivity testing. Patients who get better and then get worse again should likewise be question very closely about adherence to treatment. If adherence is confirmed then they should be investigated for resistant TB (including MDR-TB), even if a specimen has already been obtained for microbiology before commencing treatment.
Prescription or dispensing errors will account for a proportion of patients who fail to respond to treatment. Immune defects are a rare cause of non-response. In a tiny proportion of patients, treatment failure is a reflection of extreme biological variation and no cause is found.
Patients who relapse
A patient is said to relapse, if he improves while on treatment, but becomes ill again after stopping treatment. Patients who experience only a transient improvement while on treatment, or who never respond to treatment are said to have failed treatment and are discussed above.
There is a small relapse rate associated with all treatment regimens, even if the treatment has been taken religiously with 100% compliance (the standard regimen 2HREZ/4HR has a relapse rate of 2 to 3%). The majority of relapses occur within 6 months of finishing treatment. Patients who are more likely to relapse are those who took their medication in an unreliable and irregular fashion.
The probability of resistance is higher in those patients who relapse and every effort must be made to obtain a specimen that can be cultured for sensitivities. That said, most patients who relapse do so with a fully sensitive strain and it is possible that these patients have not relapsed, but have instead been re-infected; these patients can be re-treated with the same regimen as before (no drugs need to be added to the regimen and the duration need not be any longer).
The WHO recommends a regimen of 2SHREZ/6HRE when microbiology is not available (the majority of countries where TB is highly endemic). This regimen was designed to provide optimal treatment for fully-sensitive TB (the most common finding in patients who have relapsed) as well as to cover the possibility of INH-resistant TB (the most common form of resistance found).
Because of the life-long risk of relapse, all patients should be warned of the symptoms of TB relapse upon finishing treatment and given strict instructions to return to their doctor if symptoms recur.
Trial of TB treatment
In areas where TB is highly endemic, it is not unusual to encounter patient with a fever, but in whom no source of infection is found. The physician may then, after extensive investigation has excludes all other diseases, resort to a trial of TB treatment. The regimen used is HEZ for a minimum of three weeks; RMP and STM are omitted from the regimen because they are broad spectrum antibiotics, whereas the other three first-line drugs treat only mycobacterial infection. Resolution of the fever after three weeks of treatment is good evidence for occult TB and the patient should then be changed to conventional TB treatment (2HREZ/4HR). If the fever does not resolve after three weeks of treatment then it is reasonable to conclude that the patient has another cause for his fever.
Surgical treatment
Surgery has played an important part in the management of tuberculosis since the 1940s.
Historical surgical management
The first successful treatments for tuberculosis were all surgical. They were based on the observation that healed tuberculous cavities were all closed. Surgical management was therefore directed at closing open cavities in order to encourage healing. These procedures were all used in the pre-antibiotic era. There exists a myth that surgeons believed that the purpose was to deprive the organism of oxygen: it was however well known that the organism survives anaerobic conditions. Although these procedures may be considered barbaric by today’s standards, it must be remembered that these treatments represented a potential cure for a disease that at the time had a mortality at least as bad as lung cancer today.
- Recurrent or persistent pneumothorax
- The simplest and earliest procedure was to introduce air into the pleural space so as to collape the affected lung and therefore the open cavity. There was always spontaneous resolution of the pneumothorax and the procedure had to be repeated every few weeks.
- Phrenic nerve crush
- The phrenic nerve (which supplies the diaphragm) was cut or crushed so as to permanently paralyse the diaphragm on that side. The paralysed diaphragm would then rise up and the lung on that side would collapse, thus closing the cavity.
- Thoracoplasty
- When the cavity was located in the apex of the lung, thoracoplasty could be performed. Six to eight ribs were broken and pushed into the thoracic cavity to collapse the lung beneath. This was a disfiguring operation, but it avoided the need for repeated procedures.


- Plombage
- Plombage reduced the need for a disfiguring operation. It involved inserting porcelain balls into the thoracic cavity to collapse the lung underneath.
Surgical resection of infected lung was not possible in the 1940s and 1950’s, because the science of anaesthesia at the time was not sufficiently advanced to permit surgery on the lungs of an anaesthetised patient.
Modern surgical management
In modern times, the surgical treatment of tuberculosis is confined to the management of multi-drug resistant TB. A patient with MDR-TB who remains culture positive after many months of treatment may be referred for lobectomy or pneumonectomy with the aim of cutting out the infected tissue.[59] In addition, some complications of treated tuberculosis like recurrent hemoptysis, destroyed or bronchiectaic lungs and empyema (a collection of pus in the pleural cavity) are also amenable to surgical therapy
In extrapulmonary TB, surgery is often needed to make a diagnosis (rather than to effect a cure): surgical excision of lymph nodes, drainage of abscesses, tissue biopsy, etc. are all examples of this. Samples taken for TB culture should be sent to the laboratory in a sterile pot with no additive (not even water or saline) and must arrive in the laboratory as soon as possible. Where facilities for liquid culture are available, specimens from sterile sites may be inoculated directly following the procedure: this may improve the yield. In spinal TB, surgery is indicated for spinal instability (when there is extensive bony destriction) or when the spinal cord is threatened. Therapeutic drainage of tuberculous abscesses or collections is not routinely indicated and will resolve with adequate treatment. In TB meningitis, hydrocephalus is a potential complication and may necessitate the insertion of a ventricular shunt or drain.
Nutrition
It is well known that malnutrition is a strong risk factor for becoming unwell with TB,[60] that TB is itself a risk factor for malnutrition,[61][62] and that malnourished patients with TB (BMI less than 18.5) are at an increased risk of death even with appropriate antibiotic therapy.[63] Baldwin et al. (2004) underscore the importance of access to nutritional enhancements, which they show in turn interface well with a prevalent ethno-medical worldview that may minimize diagnostic delays, and fortify adherence to requisite TB treatment regimes.[64]
Vitamin D
Vitamin D supplementation appears to have a beneficial effect on the treatment of tuberculosis and appears to enhance immunity to tuberculosis,[65] That vitamin D deficiency appears to impair the body’s ability to fight tuberculosis was first noted by Professor Peter Davies in 1985,[66] and genetic differences in the vitamin D receptor in West African, Gujarati and Chinese populations have been noted.[67][68][69]
The mechanism by which this happens is not entirely clear. In mice, the mechanism appears to be up-regulation of nitric oxide-mediated killing,[70] but this appears not to be the case in humans. Instead, in humans, vitamin D-mediated killing appears to happen via an antimicrobial peptide called cathelicidin.[71] Indeed, reduced levels of vitamin D may explain the increased susceptibility of African-Americans to tuberculosis,[71] and may also explain why phototherapy is effective for lupus vulgaris (tuberculosis of the skin)[72] (a finding which won Niels Finsen the Nobel Prize in 1903), because skin exposed to sunlight naturally produces more vitamin D.
Latent tuberculosis
The treatment of latent tuberculosis infection (LTBI) is essential to controlling and eliminating TB by reducing the risk that TB infection will progress to disease.
The terms “preventive therapy” and “chemoprophylaxis” have been used for decades and are preferred in the UK because it involves giving medication to people who have no active disease and are currently well, the reason for treatment is primarily to prevent people from becoming unwell. The term “latent tuberculosis treatment” is preferred in the US because the medication does not actually prevent infection: it prevents an existing silent infection from becoming active. The feeling in the US is that the term “treatment of LTBI” promotes wider implementation by convincing people that they are receiving treatment for disease. There are no convincing reasons to prefer one term over the other.
It is essential that assessment to rule out active TB is carried out before treatment for LTBI is started. To give LTBI treatment to someone with active TB is a serious error: the TB will not be adequately treated and there is a risk of developing drug-resistant strains of TB.
There are several treatment regimens available:
- 9H—Isoniazid for 9 months is the gold standard and is 93% effective.
- 6H—Isoniazid for 6 months might be adopted by a local TB program based on cost-effectiveness and patient compliance. This is the regimen currently recommended in the UK for routine use. The US guidance exclude this regimen from use in children or persons with radiographic evidence of prior tuberculosis (old fibrotic lesions). (69% effective)
- 6 to 9H2—A twice-weekly regimen for the above 2 treatment regimens is an alternative if administered under Directly observed therapy (DOT).
- 4R—Rifampicin for 4-months is an alternative for those who are unable to take isoniazid or who have had known exposure to isoniazid-resistant TB.
- 3HR—Isoniazid and rifampicin may be given for three months.
- 2RZ—The two month regimen of rifampicin and pyrazinamide is no longer recommended for treatment of LTBI because of the greatly increased risk of drug-induced hepatitis and death.[73][74]
Current research
There is currently some evidence from animal[75] and clinical studies[76] that suggests that MXF-containing regimens as short as four months may be as effective as six months of conventional therapy.[77] Bayer is currently running a Phase II trial in collaboration with the TB Alliance to evaluate shorter treatment regimens for TB;[78] encouragingly, Bayer have also promised that if the trials are successful, Bayer will make moxifloxacin affordable and accessible in countries that need it.
The follow drugs are experimental compounds that are not commercially available, but which may be available from the manufacturer as part of a clinical trial or on a compassionate basis. Their efficacy and safety are unknown:
- PA-824[57] (manufactured by PathoGenesis Corporation, Seattle, Washington)
- R207910[58] (under development by Johnson & Johnson)
See also
National and International guidelines
- ^ Template:Cite paper
- ^ Tuberculosis Coalition for Technical Assistance (The Hague) (2006). “International Standards for Tuberculosis Care”.
- ^ Template:Cite paper
- ^ Template:Cite paper
- ^ Centers for Disease Control and Prevention (2000). “Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection” (PDF). American Thoracic Society. PMID 10764341.
Footnotes
- ↑ Medical Research Council Streptomycin in Tuberculosis Trials Committee (1948). “Streptomycin treatment for pulmonary tuberculosis”. Brit Med J. ii: 769&ndash, 82.
- ↑ Wang J-Y, Hsueh P-R, Jan I-S; et al. (2006). “Empirical treatment with a fluoroquinolone delays the treatment for tuberculosis and is associated with a poor prognosis in endemic areas”. Thorax. 61: 903&ndash, 8. doi:10.1136/thx.2005.056887.
- ↑ David H. L. (1970). “Probability Distribution of Drug-Resistant Mutants in Unselected Populations of Mycobacterium tuberculosis“. Appl Microbiol. 20 (5): 810–4. PMID 4991927.
- ↑ British Thoracic Society (1984). “A controlled trial fo six months’ chemotherapy in pulmonary tuberculosis. Final report: results during the 36 months after the end of chemotherapy and beyond”. Brit J Diseases Chest. 78 (4): 330&ndash, 36. PMID 6386028.
- ↑ Ormerod LP, Horsfield N (1987). “Short-course antituberculous chemotherapy for pulmonary and pleural disease: five years’ experience in clinical practice”. Brit J Diseases Chest. 81 (3): 268&ndash, 71.
- ↑ “A 62-dose, 6 month therapy for pulmonary and extrapulmonary tuberculosis: A twice-weekly, directly observed, and cost-effective regimen”. Ann Intern Med. 112 (6): 407&ndash, 415. 1990. PMID 2106816. Text ” Cohn DL, Catlin BJ, Peterson KL, et al. ” ignored (help)
- ↑ Campbell IA, Ormerod LP, Friend JA, Jenkins PA, Prescott RJ. (1993). “Six months versus nine months chemotherapy for tuberculosis of lymph nodes: final results”. Respir Med. 87 (8): 621&ndash, 3. PMID 8290746.
- ↑ Upadhyay SS, Saji MJ, Yau AC. (1996). “Duration of antituberculosis chemotherapy in conjunction with radical surgery in the management of spinal tuberculosis”. Spine. 21 (16): 1898&ndash, 1903.
- ↑ Medical Research Council Working Party on tuberculosis of the spine. “Five-year assessment of controlled trials of chort-course chemotherapy regimens of 6, 9 or 18 months’ duration for spinal tuberculosis in patients ambulatory from the start or undergoing radical surgery”. Int Orthopaed. 23 (2): 73&ndash, 81.
- ↑ Parthasarathy R, Sriram K, Santha T; et al. (1999). “Short-course chemotherapy for tuberculosis of the spine: a comparison between ambulant treatment and radical surgery—ten-year report”. J Bone Joint Surg Brit Vol. 81B (3): 464&ndash, 71.
- ↑ Kent SJ, Crowe SM, Yung A, Lucas CR, Mijch AM. “Tuberculous Meningitis: A 30-Year Review”. Clin Infect Dis: 987&ndash, 94. PMID 8110957. Text ” volume 17 ” ignored (help)
- ↑ Teoh R, O’Mahony G, Yeung VTF (1986). “Polymorphonuclear pleocytosis in the cerebrospinal fluid during chemotherapy for tuberculous meningitis”. J Neurol. 233 (4): 237–41.
- ↑ Chang AB; et al. (1998). “Central nervous system tuberculosis after resolution of miliary tuberculosis”. Pediatr Infect Dis J. 17 (6): 519–523. PMID 9655548.
- ↑ Thwaites GE; et al. (2004). “Dexamethasone for the treatment of tuberculous meningitis in adolescents and adults”. N Engl J Med. 351 (17): 1741&ndash, 51. PMID 15496623.
- ↑ Roberts MT, Mendelson M, Meyer P, Carmichael A, Lever AM (2003). “The use of thalidomide in the treatment of intracranial tuberculomas in adults: two case reports”. J Infect. 47 (3): 251&ndash, 5. PMID 12963389.
- ↑ Purohit SD, Sarkar SK, Gupta ML, Jain DK, Gupta PR, Mehta YR. (1987). “Dietary constituents and rifampicin absorption”. Tubercle. 68: 151&ndash, 2.
- ↑ Peloquin CA, Namdar R, Singleton MD, Nix DE. (1999). “Pharmacokinetics of rifampin under fasting conditions, with food, and with antacids”. Chest. 115: 12&ndash, 18.
- ↑ Sieger DI, Bryant M, Burley DM, Citron KM. (1974). “Effect of meals on rifampicin absorption”. Lancet. 2: 197&ndash, 8.
- ↑ Peloquin CA, Namdar R, Dodge AA, Nix DE. (1999). “Pharmacokinetics of isoniazid under fasting conditions, with food, and with antacids”. Int J Tuberc Lung Dis. 3 (8): 703&ndash, 10. PMID 10460103.
- ↑ Joshi MV, Saraf YS, Kshirsagar NA, Acharya VN. (1991). “Food reduces isoniazid bioavailability in normal volunteers”. J Assoc Physicians India. 39: 470&ndash, 1.
- ↑ Zent C, Smith P. “Study of the effect of concomitant food on the bioavailability of refampicin, isoniazid, and pyrazinamide”. Tubercle Lung Dis. 76: 109&ndash, 13.
- ↑ Peloquin CA, Bulpitt AE, Jaresko GS, Jelliffe RW, James GT, Nix DE. (1998). “Pharmacokinetics of pyrazinamide under fasting conditions, with food, and with antacids”. Pharmacotherapy. 18 (6): 1205&ndash, 11. PMID 9855317.
- ↑ Peloquin CA, Bulpitt AE, Jaresko GS, Jelliffe RW, Childs JM, Nix DE (1999). “Pharmacokinetics of ethambutol under fasting conditions, with food, and with antacids”. Antimicrob Agents Chemother. 43 (3): 568&ndash, 72. PMID 10049268.
- ↑ Yee D; et al. (2003). “Incidence of serious side effects from first-line antituberculosis drugs among patients treated for active tuberculosis”. Am J Resp Crit Care Med. 167 (11): 1472&ndash, 7. PMID 12569078.
- ↑ Ormerod L. P., Horsfield N. (1996). “Frequency and type of reactions to antituberculosis drugs: observations in routine treatment”. 77 (1): 37&ndash, 42. PMID 8733412. Unknown parameter
|tournal=ignored (help) - ↑ Forget EJ, Menzies D (2006). “Adverse reactions to first-line antituberculosis drugs”. Expert Opin Drug Saf. 5 (2): 231&ndash, 49. doi:10.1517/14740338.5.2.231. PMID 16503745.
- ↑ Steel M. A., Burk R. F., DesPrez R. M. (1991). “Toxic hepatitis with isoniazid and rifampin: a meta-analysis”. Chest. 99 (2): 465–471. PMID 1824929.
- ↑ Hong Kong Chest Service Tuberculosis Research Centre, British Medical Research Council. (1989). “A controlleed trial of 3-month, 4-month, and 6-moth regimens of chemotherapy for sputum smear-negative pulmonary tuberculosis: results at 5 years”. Am Rev Respir Dis. 139: 871&ndash, 76.
- ↑ Drobac PC; et al. “Treatment of Multidrug-Resistant Tuberculosis during Pregnancy: Long-Term Follow-Up of 6 Children with Intrauterine Exposure to Second-Line Agents”. Clin Infect Dis. 40 (11): 1689&ndash, 92. PMID 15889370.
- ↑ Breen RAM, Miller RF, Gorsuch T; et al. (2006). “Virological response to highly active antiretroviral therapy is unaffected by antituberculosis therapy”. J Infect Dis. 193 (10): 1437&ndash, 40. PMID 16619192.
- ↑ World Health Organisation. “WHO Global Task Force outlines measures to combat XDR-TB worldwide”. Retrieved 2006-10-21.
- ↑ 32.0 32.1 Center for Disease Control (2006). “Emergence of Mycobacterium tuberculosis with Extensive Resistance to Second-Line Drugs — Worldwide, 2000–2004”. MMWR Weekly. 55 (11): 301&ndash, 305.
- ↑ 33.0 33.1 Sarah McGregor. “New TB strain could fuel South Africa AIDS toll”. Reuters. Retrieved 2006-09-17.
- ↑ Frieden TR, Sterling T, Pablos-Mendez A; et al. (1993). “The emergence of drug-resistant tuberculosis in New York City”. N Engl J Med. 328 (8): 521&ndash, 56. PMID 8381207.
- ↑ Laurie Garrett (2000). Betrayal of trust: the collapse of global public health. New York: Hyperion. pp. 268ff. ISBN 0786884407 Check
|isbn=value: checksum (help). - ↑ Shah NS, Wright A, Drobniewski F; et al. (2005). “Extreme drug resistance in tuberculosis (XDR-TB): global survey of supranational reference laboratories for _Mycobacterium tuberculosis_ with resistance to second-line drugs”. Int J Tuberc Lung Dis. 9(Suppl 1): S77.
- ↑ Centers for Diseases Control (2006). “Emergence of Mycobacterium tuberculosis with extensive resistance to second-line drugs-worldwide, 2000-2004″. Morb Mort Wkly Rep. 55: 301&ndash, 5.
- ↑ Gandhi NR, Moll A, Sturm AW; et al. (2006). “Extensively drug-resistant tuberculosis as a cause of death in patients co-infected with
tuberculosis and HIV in a rural area of South Africa”. Lancet. 368: 1575&ndash, 80. line feed character in
|title=at position 90 (help) - ↑ Angela Quintal. “314 XDR-TB cases reported in SA”. Cape Times. Retrieved 2007-04-04.
- ↑ Migliori GB, Ortmann J, Girardi E; et al. (2007). “Extensively drug-resistant tuberculosis, Italy and Germany”. 13 (5).
- ↑ Sidley P. (2006). “South Africa acts to curb spread of lethal strain of TB”. Brit Med J. 333: 825.
- ↑ News24. “300+ cases of killer TB in SA”. Retrieved 2006-11-23.
- ↑ Singh JA, Upshur R, Padayatchi N. (2007). “XDR-TB in South Africa: No Time for Denial or Complacency”. PLoS Med. 4 (1): e50. doi:10.1371/journal.pmed.0040050.
- ↑ Mitnick C; et al. (2003). “Community-based therapy for multidrug-resistant tuberculosis in Lima, Peru”. N Eng J Med. 348 (2): 119–128. PMID 12519922.
- ↑ Ziganshina LE, Vizel AA, Squire SB. (2005). “Fluoroquinolones for treating tuberculosis”. Cochrane Database Sys Rev (3): CD004795. doi:10.1002/14651858.CD004795.pub2.
- ↑ Leimane V.; et al. (2005). “Clinical outcome of individualised treatment of multidrug-resistant tuberculosis in Latvia: a retrospective cohort study”. Lancet. 365 (9456): 318–26. PMID 15664227.
- ↑ Schön T, Elias D, Moges F; et al. (2003). “Arginine as an adjuvant to chemotherapy improves clinical outcome in active tuberculosis”. Eur Respir J. 21: 483&ndash, 88.
- ↑ Rockett KA, Brookes R, Udalova I; et al. (1998). “1,25-Dihydroxyvitamin D3 induces nitric oxide synthase and suppresses growth of Mycobacterium tuberculosis in a human macrophage-like cell line”. Infect Immunity. 66 (11): 5314&ndash, 21.
- ↑ Chambers HF, Turner J, Schecter GF, Kawamura M, Hopewell PC. (2005). “Imipenem for treatment of tuberculosis in mice and humans”. Antimicrob Agents Chemother. 49 (7): 2816&ndash, 21. PMID 15980354.
- ↑ Chambers HF, Kocagoz T, Sipit T, Turner J, Hopewell PC. (1998). “Activity of amoxicillin/clavulanate in patients with tuberculosis”. Clin Infect Dis. 26 (4): 874&ndash, 7. PMID 9564467.
- ↑ Donald PR, Sirgel FA, Venter A; et al. (2001). “Early bactericidal activity of amoxicillin in combination with clavulanic acid in patients with sputum smear-positive pulmonary tuberculosis”. Scand J Infect Dis. 33 (6): 466&ndash, 9. PMID 11450868.
- ↑ Jagannath C, Reddy MV, Kailasam S, O’Sullivan JF, Gangadharam PR. (1995). “Chemotherapeutic activity of clofazimine and its analogues against Mycobacterium tuberculosis. In vitro, intracellular, and in vivo studies”. Am J Respir Crit Care Med. 151 (4): 1083&ndash, 86.
- ↑ Adams LM, Sinha I, Franzblau SG; et al. (1999). “Effective treatment of acute and chronic murine tuberculosis with liposome-encapsulated clofazimine” (PDF). Antimicrob Agents Chemother. 43 (7): 1638&ndash, 43.
- ↑ “Lack of activity of orally administered clofazimine against intracellular Mycobacterium tuberculosis in whole-blood culture” (PDF). Antimicrob Agents Chemother. 48 (8): 3133&ndash, 35. 2004.
- ↑ Shubin H, Sherson J, Pennes E, Glaskin A, Sokmensuer A. (1958). “Prochlorperazine (compazine) as an aid in the treatment of pulmonary tuberculosis”. Antibiotic Med Clin Ther. 5 (5): 305&ndash, 9. PMID 13521769.
- ↑ Wayne LG, Sramek HA (1994). “Metronidazole is bactericidal to dormant cells of Mycobacterium tuberculosis“. Antimicrob Agents Chemother. 38 (9): 2054&ndash, 58.
- ↑ 57.0 57.1 Stover CK, Warrener P, VanDevanter DR; et al. (2000). “A small-molecule nitroimidazopyran drug candidate for the treatment of tuberculosis”. Nature. 405 (6789): 962&ndash, 6. PMID 10879539.
- ↑ 58.0 58.1 Andries K, Verhasselt P, Guillemont J; et al. (2005). “A diarylquinoline drug active on the ATP-synthase of Mycobacterium tuberculosis“. Science. 307 (5707): 223&ndash, 27. doi:10.1126/science.1106753.
- ↑ Chan ED, Laurel V, Strand MJ; et al. (2004). “Treatment and outcome analysis of 205 patients with multidrug-resistant tuberculosis”. Am J Resp Crit Care Med (10): 1103&ndash, 1109. doi:10.1164/rccm.200308-1159OC. Unknown parameter
|vol=ignored (|volume=suggested) (help) - ↑ Cegielski JP, McMurray DN. (2004). “The relationship between malnutrition and tuberculosis: evidence from studies in humans and experimental animals”. Int J Tubercul Lung Dis. 8 (3): 286&ndash, 98.
- ↑ Onwubalili JK. (1988). “Malnutrition among tuberculosis patients in Harrow, England”. Eur J Clin Nutr. 42 (4): 363&ndash, 6. PMID 3396528.
- ↑ Karyadi E, Schultink W, Nelwan RHH; et al. (2000). “Poor Micronutrient Status of Active Pulmonary Tuberculosis Patients in Indonesia”. J Nutrition. 130: 2953&ndash, 58.
- ↑ Zachariah R, Spielmann MP, Harries AD, Salaniponi FM. (2002). “Moderate to severe malnutrition in patients with tuberculosis is a risk factor associated with early death”. Trans R Soc Trop Med Hyg. 96 (3): 291&ndash, 4. PMID 12174782.
- ↑ Baldwin M. 2004 “Tuberculosis and nutrition: disease perceptions and health seeking behavior of household contacts in the Peruvian Amazon.” The International Journal of Tuberculosis and Lung Disease 8(12):1484-91.
- ↑ Martineau AR, Wilkinson RJ, Wilkinson KA, Newton SM, Kampmann B, Hall BM; et al. (2007). “A single dose of vitamin D enhances immunity to Mycobacteria”. Am J Respir Crit Care Med. doi:10.1164/rccm.200701-007OC. PMID 17463418.
- ↑ Davies PD (1985). “A possible link between vitamin D deficiency and impaired host defence to Mycobacterium tuberculosis”. Tubercle. 66 (4): 301&ndash, 6. PMID 3936248.
- ↑ Bellamy R, Ruwende C, Corrah T; et al. (1998). “Tuberculosis and chronic hepatitis B virus infection in africans and variation in the vitamin D receptor gene”. J Infect Dis. 179: 721&ndash, 24.
- ↑ “Influence of vitamin D deficiency and vitamin D receptor polymorphisms on tuberculosis among Gujarati Asians in west London: a case-control study”. Lancet. 355 (9204): 618&ndash, 21. PMID 10696983. Text “Wilkinson R, Llewelyn M, Toossi Z, et al.” ignored (help)
- ↑ 刘玮,张翠英,吴晓明; et al. (2003). “维生素D受体基因多态性与肺结核易感性的病例对照研究 (A case-control study on the vitamin D receptor gene polymorphisms and susceptibility to pulmonary tuberclosis)”. 中华流行病学杂志 (Chinese Journal of Epidemiology) (in Chinese). 24 (5): 389&ndash, 92. PMID 12820934.
- ↑ Rockett KA, Brookes R, Udalova I; et al. (1998). “1,25-Dihydroxyvitamin D3 induces nitric oxide synthase and suppresses growth of Mycobacterium tuberculosis in a human macrophage-like cell line”. Infect Immunity. 66 (11): 5314&ndash, 21.
- ↑ 71.0 71.1 Liu PT, Stenger S, Li H; et al. (2006). “Toll-like receptor triggering of a vitamin D-mediated human antimicrobial response”. Science. 311: 1770&ndash, 3. PMID 16497887.
- ↑ Finsen NR (1886). Om anvendelse i medicinen af koncentrerede kemiske lysstraaler. Copenhagen, Denmark: Gyldendalske Boghandels Forlag.
- ↑ Schechter M, Zajdenverg R, Falco G, Barnes G, Faulhaber J, Coberly J, Moore R, Chaisson R (2006). “Weekly rifapentine/isoniazid or daily rifampin/pyrazinamide for latent
tuberculosis in household contacts”. Am J Respir Crit Care Med. 173 (8): 922&ndash, 6. PMID 16474028. line feed character in
|title=at position 71 (help) - ↑ Ijaz K, Jereb JA, Lambert LA; et al. (2006). “Severe of fatal liver injury in 50 patients in the United States taking rifampin and pyrazinamide for latent tuberculosis”. Clin Infect Dis. 42 (3): 346&ndash, 55.
- ↑ Nuermberger EL, Yoshimatsu T, Tyagi S; et al. (2004). “Moxifloxacin-containing regimen greatly reduces time to culture conversion in murine Tuberculosis”. Am J Resp Crit Care Med. 169: 421&ndash, 26. doi:10.1164/rccm.200310-1380OC.
- ↑ Gosling RD, Uiso LO, Sam NE; et al. (2003). “The bactericidal activity of moxifloxacin in patients with pulmonary tuberculosis”. Am J Resp Crit Care Med. 168: 1342&ndash, 45. doi:10.1164/rccm.200305-682OC.
- ↑ Nuermberger EL, Yoshimatsu T, Tyagi S; et al. (2004). “Moxifloxacin-containing regimens of reduced duration produce a stable cure in murine tuberculosis”. Am J Resp Crit Care Med. 170: 1131&ndash, 34. doi:10.1164/rccm.200407-885OC.
- ↑ TB Alliance. “TB Alliance and Bayer launch historic global TB drug trials”. Retrieved 2006-10-17.
Related Chapters
Related Chapters
- Tuberculous pericarditis
- Pott’s disease
- Abreugraphy
- ATC code J04: Drugs for treatment of TB
- Buruli ulcer and leprosy: Other diseases caused by Mycobacteria
- Latent tuberculosis
- Mycobacterium Tuberculosis Structural Genomics Consortium
- National Center for HIV, STD, and TB Prevention
- Nontuberculous mycobacteria
- Philip D’Arcy Hart
- UNITAID
- Nosocomial infection
External Links
External Links
- (CDC) – Division of Tuberculosis Elimination. Core Curriculum on Tuberculosis: What the Clinician Should Know. 4th edition (2000). Updated Aug 2003.
- (CDC) – Division of Tuberculosis Elimination News and updates.
- (CDC) – Questions and Answers About TB, 2007.
- (CDC) – Treatment of Tuberculosis: American Thoracic Society, CDC, and Infectious Diseases Society of America
- “Tuberculosis”. Health at a Glance: Asia/Pacific 2020: Measuring Progress Towards Universal Health Care Coverage. OECD Publishing. Nov 27, 2020. Retrieved January 19, 2021.
|first1=missing|last1=in Authors list (help)
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH