
Myocardial rupture
For patient information, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2] Mahmoud Sakr, M.D. [3]
Synonyms and keywords: free wall rupture, ventricular septal rupture, VSR
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
Myocardial rupture is a laceration or tearing of the walls of the ventricles or atria of the heart, of the interatrial or interventricular septum, of the papillary muscles or chordae tendineae or of one of the valves of the heart. It is most commonly seen as a serious sequelae of an acute myocardial infarction (heart attack).
Pathophysiology
The most common cause of myocardial rupture is a recent myocardial infarction, with the rupture typically occurring three to five days after infarction. Other causes of rupture include cardiac trauma, endocarditis (infection of the heart),[1][2] cardiac tumors, infiltrative diseases of the heart,[1] and aortic dissection.
Epidemiology and Demographics
The incidence of myocardial rupture has decreased in the era of urgent revascularization and aggressive pharmacological therapy for the treatment of an acute myocardial rupture. However, the decrease in the incidence of myocardial rupture is not uniform; there is a slight increase in the incidence of rupture if thrombolytic agents are used to abort a myocardial infarction.[3] On the other hand, if primary percutaneous coronary intervention is performed to abort the infarction, the incidence of rupture is significantly lowered.[4] The incidence of myocardial rupture if PCI is performed in the setting of an acute myocardial infarction is about 1 percent.[5]
Risk Factors
Risk factors for rupture after an acute myocardial infarction include female gender, advanced age of the individual, and a low body mass index. Other presenting signs associated with myocardial rupture include a pericardial friction rub, sluggish flow in the coronary artery after it is opened, the left anterior descending artery being the cause of the acute MI,[6] and delay of revascularization greater than 2 hours.
Natural History, Complications and Prognosis
The prognosis of myocardial rupture is dependant on a number of factors, including which portion of the myocardium is involved in the rupture. In one case series, if myocardial rupture involved the free wall of the left ventricle, the mortality rate was 100 percent.[7] Even if the individual survives the initial hemodynamic sequelae of the rupture, the 30 day mortality is still significantly higher than if rupture did not occur.[7]
Diagnosis
History and Symptoms
Symptoms of myocardial rupture are recurrent or persistent chest pain, syncope, and distension of jugular veins. Due to the acute hemodynamic deterioration associated with myocardial rupture, the diagnosis is generally made based on physical examination, changes in the vital signs, and clinical suspicion. The diagnosis can be confirmed with echocardiography.
Physical Examination
Due to the acute hemodynamic deterioration associated with myocardial rupture, the diagnosis is generally made based on physical examination, changes in the vital signs, and clinical suspicion.
Echocardiography
The diagnosis can be confirmed with echocardiography.
Treatment
Medical Therapy
The treatment for myocardial rupture is supportive in the immediate setting and surgical correction of the rupture, if feasible. A certain small percentage of individuals do not seek medical attention in the acute setting survive. In this setting, it may be reasonable to treat the rupture medically and delay or avoid surgery completely, depending on the individual’s comorbid medical issues.
Surgery
The treatment for myocardial rupture is supportive in the immediate setting and surgical correction of the rupture, if feasible. A certain small percentage of individuals do not seek medical attention in the acute setting survive. In this setting, it may be reasonable to treat the rupture medically and delay or avoid surgery completely, depending on the individual’s comorbid medical issues.
References
- ↑ 1.0 1.1 Lin TH, Su HM, Voon WC, Lai HM, Yen HW, Lai WT, Sheu SH. (2006). “Association between hypertension and primary mitral chordae tendinae rupture”. Am J Hypertens. 19 (1): 75–9. PMID 16461195.
- ↑ de Diego C, Marcos-Alberca P, Pai RK. (2006). “Giant periprosthetic vegetation associated with pseudoaneurysmal-like rupture” (PDF). Eur Heart J. 27 (8): 912. PMID 16569654.
- ↑ Becker RC, Gore JM, Lambrew C, Weaver WD, Rubison RM, French WJ, Tiefenbrunn AJ, Bowlby LJ, Rogers WJ. (1996). “A composite view of cardiac rupture in the United States National Registry of Myocardial Infarction”. J Am Coll Cardiol. 27 (6): 1321–6. PMID 8626938.
- ↑ Moreno R, Lopez-Sendon J, Garcia E, Perez de Isla L, Lopez de Sa E, Ortega A, Moreno M, Rubio R, Soriano J, Abeytua M, Garcia-Fernandez MA. (2002). “Primary angioplasty reduces the risk of left ventricular free wall rupture compared with thrombolysis in patients with acute myocardial infarction”. J Am Coll Cardiol. 39 (4): 598–603. PMID 11849857.
- ↑ Yip HK, Wu CJ, Chang HW, Wang CP, Cheng CI, Chua S, Chen MC. (2003). “Cardiac rupture complicating acute myocardial infarction in the direct percutaneous coronary intervention reperfusion era” (PDF). Chest. 124 (2): 565–71. PMID 12907544.
- ↑ Sugiura T, Nagahama Y, Nakamura S, Kudo Y, Yamasaki F, Iwasaka T. (2003). “Left ventricular free wall rupture after reperfusion therapy for acute myocardial infarction”. Am J Cardiol. 92 (3): 282–4. PMID 12888132.
- ↑ 7.0 7.1 Yip HK, Wu CJ, Chang HW, Wang CP, Cheng CI, Chua S, Chen MC (2003). “Cardiac rupture complicating acute myocardial infarction in the direct percutaneous coronary intervention reperfusion era”. Chest. 124 (2): 565–71. PMID 12907544. Retrieved 2012-04-08. Unknown parameter
|month=ignored (help)
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Classification
Myocardial ruptures can be classified as one of three types.
Type I
An abrupt slit-like tear that generally occurs within 24 hours of an acute myocardial infarction.
Type II
An erosion of the infarcted myocardium, which is suggestive of a slow tear of the dead myocardium. Type II ruptures typically occur more than 24 hours after the infarction occurred.
Type III
These ruptures are characterized by early aneurysm formation and subsequent rupture of the aneurysm.[1]
Alternate Classification Scheme
Another method for classifying myocardial ruptures is by the anatomical portion of the heart that has ruptured. By far the most dramatic is rupture of the free wall of the left of right ventricles, as this is associated with immediate hemodynamic collapse and death secondary to acute pericardial tamponade. Rupture of the interventricular septum will cause a ventricular septal defect. Rupture of a papillary muscle will cause acute mitral regurgitation.
References
- ↑ Becker AE, van Mantgem JP. (1975). “Cardiac tamponade. A study of 50 hearts”. Eur J Cardiol. 3 (4): 349–58. PMID 1193118.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
The most common cause of myocardial rupture is a recent myocardial infarction, with the rupture typically occurring three to five days after infarction. Other causes of rupture include cardiac trauma, endocarditis (infection of the heart),[1][2] cardiac tumors, infiltrative diseases of the heart,[1] and aortic dissection.
Pathophysiology
Myocardial Rupture of the Free Wall
-
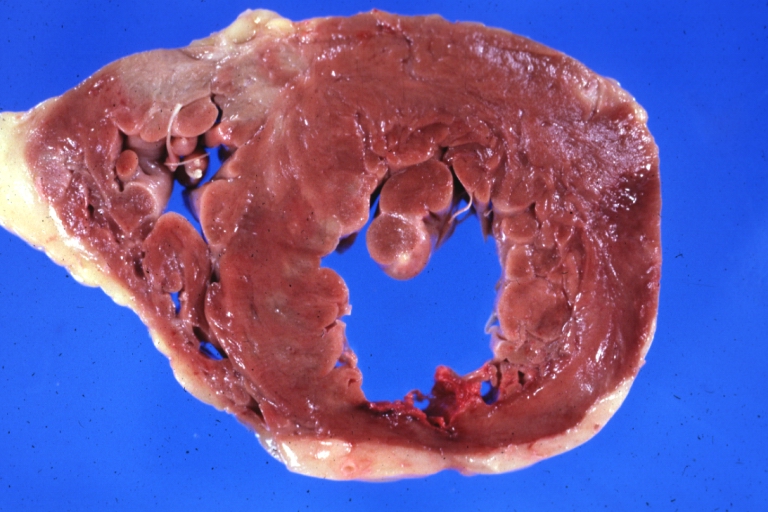
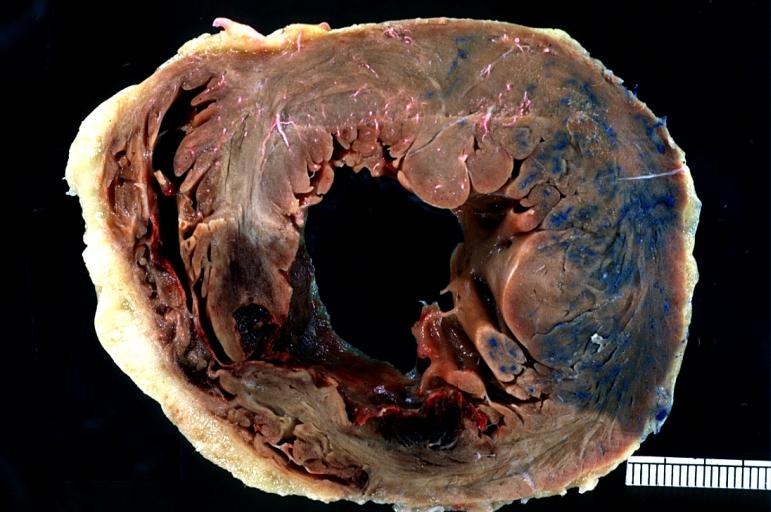
 Gross horizontal section of ruptured anterolateral infarct
Gross horizontal section of ruptured anterolateral infarct -
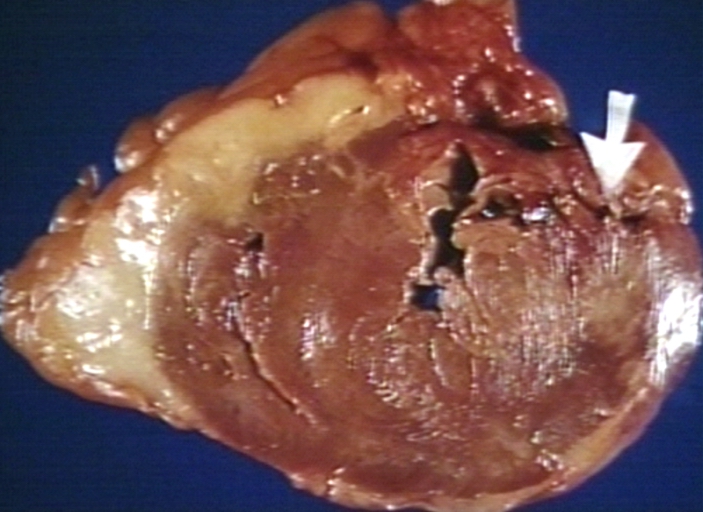
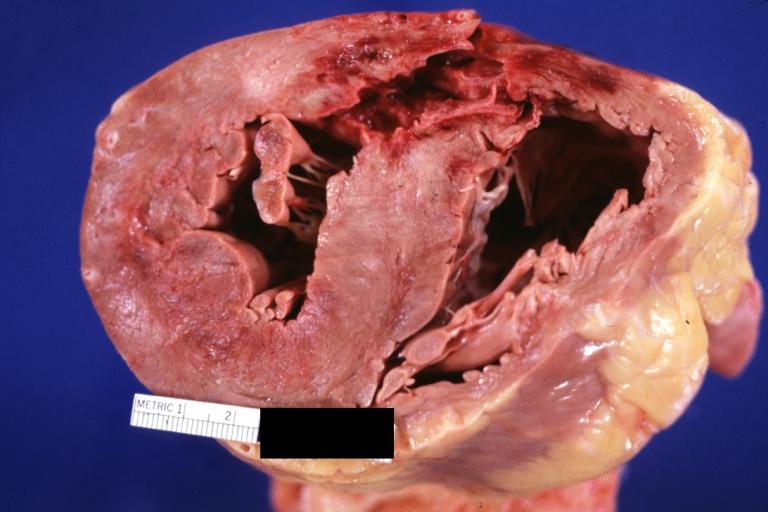
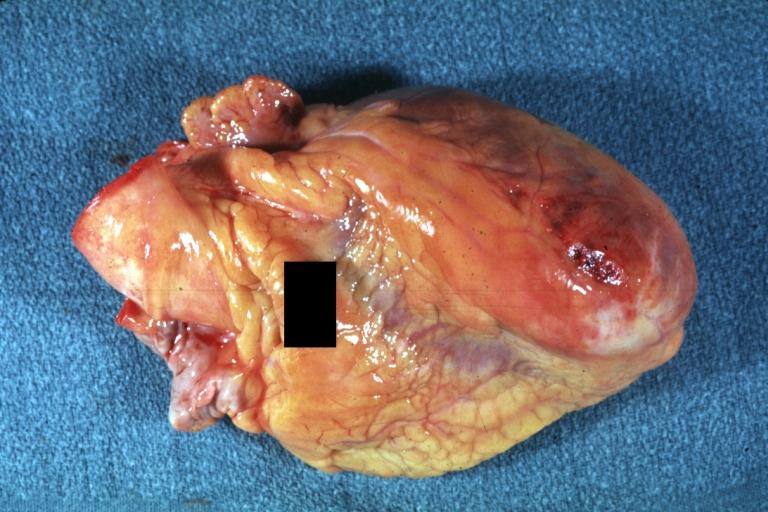 Gross, Acute MI, external view of ruptured myocardial infarction near apex
Gross, Acute MI, external view of ruptured myocardial infarction near apex


-
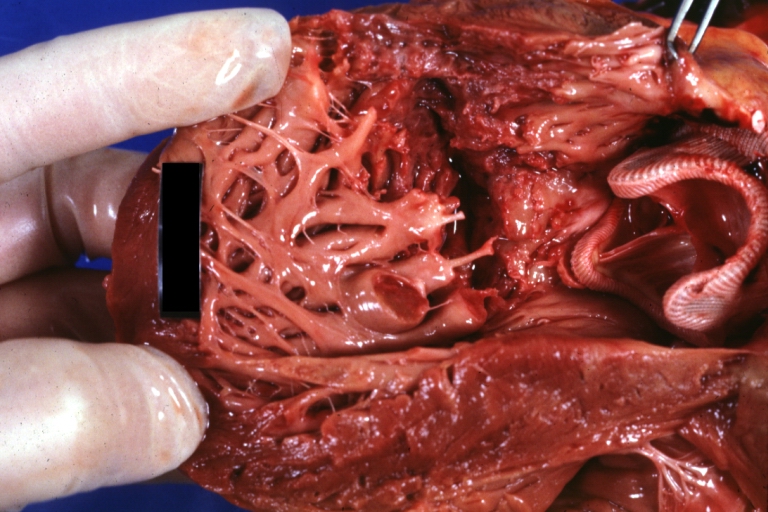
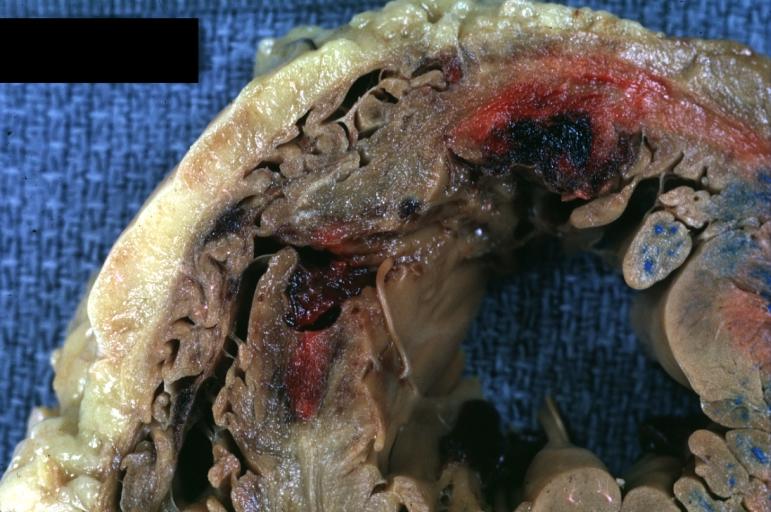
 Myocardial rupture
Myocardial rupture -
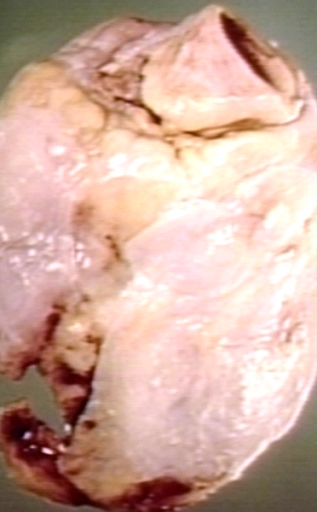
 Myocardial rupture
Myocardial rupture


-
 Myocardial rupture
Myocardial rupture -
 Myocardial rupture
Myocardial rupture


-
 Myocardial rupture
Myocardial rupture -
 Myocardial rupture
Myocardial rupture


-
 Myocardial rupture: Gun shot
Myocardial rupture: Gun shot

Ventricular Septal Rupture
-
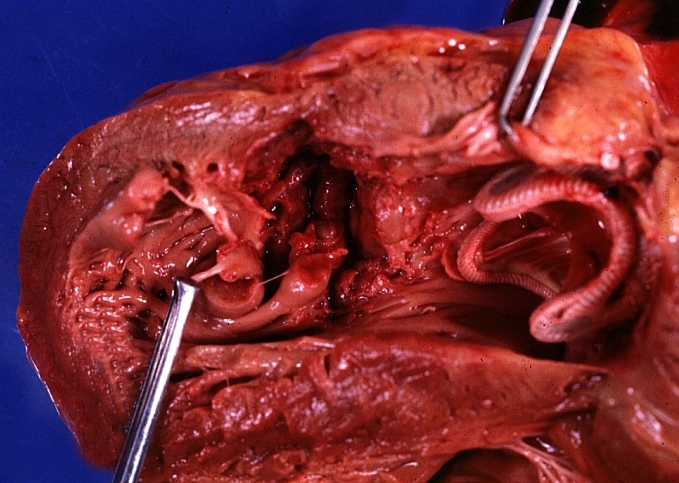
 Heart, Acute MI, Ventricular septum rupture at posterior wall.
Heart, Acute MI, Ventricular septum rupture at posterior wall.

-
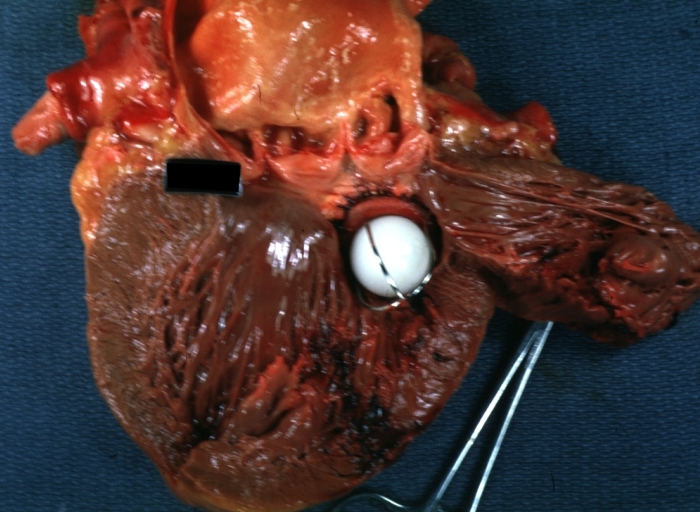
 Gross; acute myocardial infarction with ventricular septal rupture
Gross; acute myocardial infarction with ventricular septal rupture

-
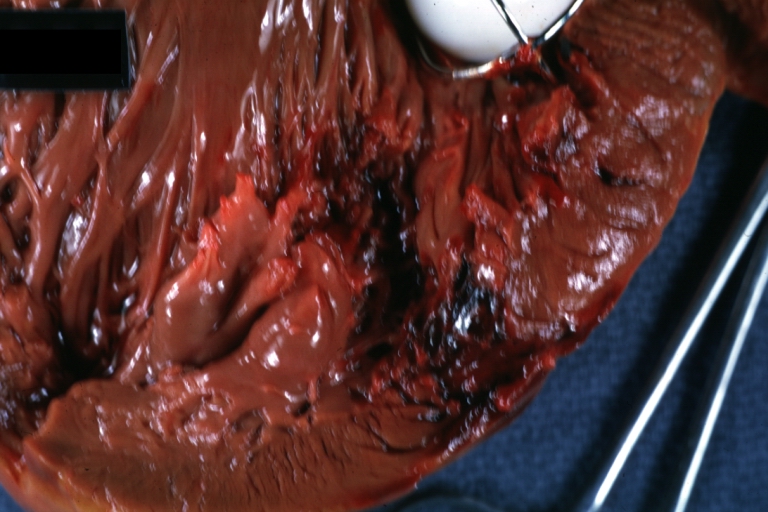
 Acute MI, rupture of the ventricular septum. A close up view.
Acute MI, rupture of the ventricular septum. A close up view.

References
- ↑ 1.0 1.1 Lin TH, Su HM, Voon WC, Lai HM, Yen HW, Lai WT, Sheu SH. (2006). “Association between hypertension and primary mitral chordae tendinae rupture”. Am J Hypertens. 19 (1): 75–9. PMID 16461195.
- ↑ de Diego C, Marcos-Alberca P, Pai RK. (2006). “Giant periprosthetic vegetation associated with pseudoaneurysmal-like rupture” (PDF). Eur Heart J. 27 (8): 912. PMID 16569654.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Kiran Singh, M.D. [2]
Causes
Drugs
Epidemiology and Demographics
Please help WikiDoc by adding more content here. It’s easy! Click here to learn about editing.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
The incidence of myocardial rupture has decreased in the era of urgent revascularization and aggressive pharmacological therapy for the treatment of an acute myocardial rupture. However, the decrease in the incidence of myocardial rupture is not uniform; there is a slight increase in the incidence of rupture if thrombolytic agents are used to abort a myocardial infarction.[1] On the other hand, if primary percutaneous coronary intervention is performed to abort the infarction, the incidence of rupture is significantly lowered.[2] The incidence of myocardial rupture if PCI is performed in the setting of an acute myocardial infarction is about 1 percent.[3]
References
- ↑ Becker RC, Gore JM, Lambrew C, Weaver WD, Rubison RM, French WJ, Tiefenbrunn AJ, Bowlby LJ, Rogers WJ. (1996). “A composite view of cardiac rupture in the United States National Registry of Myocardial Infarction”. J Am Coll Cardiol. 27 (6): 1321–6. PMID 8626938.
- ↑ Moreno R, Lopez-Sendon J, Garcia E, Perez de Isla L, Lopez de Sa E, Ortega A, Moreno M, Rubio R, Soriano J, Abeytua M, Garcia-Fernandez MA. (2002). “Primary angioplasty reduces the risk of left ventricular free wall rupture compared with thrombolysis in patients with acute myocardial infarction”. J Am Coll Cardiol. 39 (4): 598–603. PMID 11849857.
- ↑ Yip HK, Wu CJ, Chang HW, Wang CP, Cheng CI, Chua S, Chen MC. (2003). “Cardiac rupture complicating acute myocardial infarction in the direct percutaneous coronary intervention reperfusion era” (PDF). Chest. 124 (2): 565–71. PMID 12907544.
Risk Factors
Please help WikiDoc by adding content here. It’s easy! Click here to learn about editing.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
Risk factors for rupture after an acute myocardial infarction include female gender, advanced age of the individual, and a low body mass index. Other presenting signs associated with myocardial rupture include a pericardial friction rub, sluggish flow in the coronary artery after it is opened, the left anterior descending artery being the cause of the acute MI,[1] and delay of revascularization greater than 2 hours.
References
- ↑ Sugiura T, Nagahama Y, Nakamura S, Kudo Y, Yamasaki F, Iwasaka T. (2003). “Left ventricular free wall rupture after reperfusion therapy for acute myocardial infarction”. Am J Cardiol. 92 (3): 282–4. PMID 12888132.
Relative Contribution of Myocardial Rupture as a Cause of Sudden Cardiac Death Following STEMI
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Relative Contribution of Myocardial Rupture, Cardiac Arrest and Recurrent MI as a Cause of Sudden Death Following STEMI
Despite implantation of AICDs, there remains a high incidence of sudden death following ST elevation MI. This is due to the fact that not all sudden death is due to arrythmias in the period following ST elevation MI. Based upon autopsy findings, the relative frequency of various pathophysiologic events among 105 cases was as follows[1]:
- 3 Index MIs in the first 7 days (2.9%)
- 28 Recurrent MIs (26.6%)
- 13 Cardiac ruptures (12.4%)
- 4 Pump failures (3.8%)
- 2 Other cardiovascular causes (stroke or pulmonary embolism; 1.9%)
- 1 Noncardiovascular cause (1%)
- 54 cases (51.4%) had no acute specific autopsy evidence other than the index MI and were thus presumed arrhythmic.
The relative contribution of arrhythmic death was lowest in the first month, while the relative contribution of recurrent MI or cardiac rupture was highest in the first month following ST elevation MI. After three months, however, the relative contribution shifted so that the proportion of cases attributable to arrhythmias was significantly higher than recurrent MI or rupture (P<0.0001).
References
- ↑ Pouleur AC, Barkoudah E, Uno H, Skali H, Finn PV, Zelenkofske SL, Belenkov YN, Mareev V, Velazquez EJ, Rouleau JL, Maggioni AP, Køber L, Califf RM, McMurray JJ, Pfeffer MA, Solomon SD (2010). “Pathogenesis of Sudden Unexpected Death in a Clinical Trial of Patients With Myocardial Infarction and Left Ventricular Dysfunction, Heart Failure, or Both”. Circulation. doi:10.1161/CIRCULATIONAHA.110.940619. PMID 20660803. Retrieved 2010-08-10. Unknown parameter
|month=ignored (help)
Natural History, Complications and Prognosis
Please help WikiDoc by adding content here. It’s easy! Click here to learn about editing.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
The prognosis of myocardial rupture is dependant on a number of factors, including which portion of the myocardium is involved in the rupture. In one case series, if myocardial rupture involved the free wall of the left ventricle, the mortality rate was 100 percent.[1] Even if the individual survives the initial hemodynamic sequelae of the rupture, the 30 day mortality is still significantly higher than if rupture did not occur.[1]
References
- ↑ 1.0 1.1 Yip HK, Wu CJ, Chang HW, Wang CP, Cheng CI, Chua S, Chen MC (2003). “Cardiac rupture complicating acute myocardial infarction in the direct percutaneous coronary intervention reperfusion era”. Chest. 124 (2): 565–71. PMID 12907544. Retrieved 2012-04-08. Unknown parameter
|month=ignored (help)
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Echocardiography | Other Imaging Findings | Other Diagnostic Studies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH