
Acute bronchitis
For Acute bronchitis patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]; Nate Michalak, B.A.
Overview
Acute bronchitis is a self-limited lower respiratory tract infection that is more common in young children and the elderly, especially during cold seasons.[1][2][3] Viruses, especially influenza, are the most common causative agents.[4][2][5] Symptoms include: cough, sputum production and wheezing as well as constitutional symptoms. It must be differentiated from pneumonia, asthma, and GERD.[3] Reassurance and symptomatic medications are mainstays of acute bronchitis.[2][6] Acute bronchitis may be prevented by hand hygiene, vaccination, and environmental control.[3][7] Smoking cessation plays a great role in reducing the course of the disease.[8]
Historical Perspective
Acute bronchitis was first described by Charles Badham in 1808 in England.[9] In 1821, Dr. Rene Laennec, known as the “father of chest medicine,” described bronchitis in details.[10]
Pathophysiology
The causative agent is transmitted through the large and medium size airway tracts and inoculates the tracheobranchial epithelium. This leads to inflammation, thickening, and increased mucus production in the airways.[1] Epithelial-cell desquamation and denuding of the airway to the level of the basement membrane in association with the presence of a lymphocytic cellular infiltrate have been demonstrated on microscopic examination.[1]
Causes
Common causes of acute bronchitis include viruses, bacteria and environmental factors. Among them, influenza is common.[4][2][5]
When bronchitis is prolonged, consider:
Also consider pneumonia and atypical pneumonia.
Differential Diagnosis of Acute Bronchitis
Acute bronchitis must be differentiated from other diseases that may cause cough, dyspnea, and wheezing[3] including, pneumonia,[11] Asthma[12] Chronic bronchitis,[13] and GERD[14][15]
Epidemiology
Acute bronchitis is the ninth most common illness among outpatient visits in the U.S. It’s prevalence depends on season of the year, vaccination status and outbreaks during that particular year. It is common among young children and the elderly.[16][2][17]
Risk factors
The main determining risk factors for acute bronchitis are age, season of the year and the immunization status[1][2][3].
Natural History
If left untreated, acute bronchitis usually resolves within 2 weeks but may last up to 2 months.[1][18] Prognosis is generally excellent and majority of patients recover after 5-10 days.[2] Recurrent episodes of acute bronchitis in subsequent years occur in 20% of patients.[3]
Diagnosis
- Bronchial irritation symptoms including: cough, hoarseness, and phlegm production
- Constitutional symptoms including: Chest pain, Fever, malaise, and Myalgia
Physical examination
- Acute bronchitis presents with signs of prolonged expiration, wheezing, fever and abnormal breath sounds.[3][2]
Laboratory Tests
- Diagnostic tests are rarely needed to confirm the diagnosis of acute bronchitis. In very specific conditions, serologic tests, viral cultures or sputum analyses may be applied. Generally, inflammatory markers, such as CRP, rise during the course of acute bronchitis. Procalcitonin is helpful to differentiate bacterial from other causes.
Chest x-ray
Treatment
Medical therapy
- Reassurance and symptomatic therapy are the mainstay of treatment. NSAIDs, albuterol and antitussives may help alleviate symptoms.
- The most important treatment aspect is to NOT routinely prescribe antibiotics.[20][21][7][2][22]
- Azithromycin can treat:
Primary prevention
- The major preventive measures for acute bronchitis include: hands hygiene, environmental control, wearing physical barriers, and vaccination for preventable pathogens, such as influenza and pertussis[3][7].
Secondary prevention
- Smoking cessation or reduction is helpful in reducing the severity of acute bronchitis symptoms.[23]
References
- ↑ 1.0 1.1 1.2 1.3 1.4 Gonzales R, Sande MA (2000). “Uncomplicated acute bronchitis”. Ann. Intern. Med. 133 (12): 981–91. PMID 11119400.
- ↑ 2.00 2.01 2.02 2.03 2.04 2.05 2.06 2.07 2.08 2.09 Wenzel RP, Fowler AA (2006). “Clinical practice. Acute bronchitis”. N. Engl. J. Med. 355 (20): 2125–30. doi:10.1056/NEJMcp061493. PMID 17108344.
- ↑ 3.0 3.1 3.2 3.3 3.4 3.5 3.6 3.7 3.8 Albert RH (2010). “Diagnosis and treatment of acute bronchitis”. Am Fam Physician. 82 (11): 1345–50. PMID 21121518.
- ↑ 4.0 4.1 Boldy DA, Skidmore SJ, Ayres JG (1990). “Acute bronchitis in the community: clinical features, infective factors, changes in pulmonary function and bronchial reactivity to histamine”. Respir Med. 84 (5): 377–85. PMID 2174179.
- ↑ 5.0 5.1 Jonsson JS, Sigurdsson JA, Kristinsson KG, Guthnadóttir M, Magnusson S (1997). “Acute bronchitis in adults. How close do we come to its aetiology in general practice?”. Scand J Prim Health Care. 15 (3): 156–60. PMID 9323784.
- ↑ 6.0 6.1 Graffelman AW, le Cessie S, Knuistingh Neven A, Wilemssen FE, Zonderland HM, van den Broek PJ (2007). “Can history and exam alone reliably predict pneumonia?”. J Fam Pract. 56 (6): 465–70. PMID 17543257.
- ↑ 7.0 7.1 7.2 Braman SS (2006). “Chronic cough due to acute bronchitis: ACCP evidence-based clinical practice guidelines”. Chest. 129 (1 Suppl): 95S–103S. doi:10.1378/chest.129.1_suppl.95S. PMID 16428698.
- ↑ The American Academy of Family Physicians: Acute Bronchitis. January 2006. Accessed 20 March 2007.
- ↑ Klippe HJ, Kirsten D (2009). “[200 years of bronchitis–from 1808 to 2008]”. Pneumologie (in German). 63 (4): 228–30. doi:10.1055/s-0028-1119572. PMID 19343614.
- ↑ terms(2016)https://lunginstitute.com/blog/history-of-chronic-bronchitis/accessed on September,13 2016
- ↑ Prina E, Ranzani OT, Torres A (2015). “Community-acquired pneumonia”. Lancet. 386 (9998): 1097–108. doi:10.1016/S0140-6736(15)60733-4. PMID 26277247.
- ↑ Busse WW (2011). “Asthma diagnosis and treatment: filling in the information gaps”. J. Allergy Clin. Immunol. 128 (4): 740–50. doi:10.1016/j.jaci.2011.08.014. PMID 21875745.
- ↑ Celli BR, MacNee W (2004). “Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper”. Eur. Respir. J. 23 (6): 932–46. PMID 15219010.
- ↑ Singh A (2009). “Asthma in older adults”. CMAJ. 181 (12): 929. doi:10.1503/cmaj.109-2049. PMC 2789137. PMID 19969583.
- ↑ Irwin RS, Baumann MH, Bolser DC, Boulet LP, Braman SS, Brightling CE, Brown KK, Canning BJ, Chang AB, Dicpinigaitis PV, Eccles R, Glomb WB, Goldstein LB, Graham LM, Hargreave FE, Kvale PA, Lewis SZ, McCool FD, McCrory DC, Prakash UB, Pratter MR, Rosen MJ, Schulman E, Shannon JJ, Smith Hammond C, Tarlo SM (2006). “Diagnosis and management of cough executive summary: ACCP evidence-based clinical practice guidelines”. Chest. 129 (1 Suppl): 1S–23S. doi:10.1378/chest.129.1_suppl.1S. PMC 3345522. PMID 16428686.
- ↑ Macfarlane J, Holmes W, Gard P, Macfarlane R, Rose D, Weston V, Leinonen M, Saikku P, Myint S (2001). “Prospective study of the incidence, aetiology and outcome of adult lower respiratory tract illness in the community”. Thorax. 56 (2): 109–14. PMC 1746009. PMID 11209098.
- ↑ Ferri FF. Ferri’s Clinical Advisor 2016, 5 Books in 1. Elsevier Health Sciences; 2015.
- ↑ Landau LI (2006). “Acute and chronic cough”. Paediatr Respir Rev. 7 Suppl 1: S64–7. doi:10.1016/j.prrv.2006.04.172. PMID 16798599.
- ↑ Gonzales R, Bartlett JG, Besser RE, Cooper RJ, Hickner JM, Hoffman JR, Sande MA (2001). “Principles of appropriate antibiotic use for treatment of uncomplicated acute bronchitis: background”. Ann. Intern. Med. 134 (6): 521–9. PMID 11255532.
- ↑ Little P, Rumsby K, Kelly J, Watson L, Moore M, Warner G, Fahey T, Williamson I (2005). “Information leaflet and antibiotic prescribing strategies for acute lower respiratory tract infection: a randomized controlled trial”. JAMA. 293 (24): 3029–35. doi:10.1001/jama.293.24.3029. PMID 15972565.
- ↑ Smith SM, Fahey T, Smucny J, Becker LA (2014). “Antibiotics for acute bronchitis”. Cochrane Database Syst Rev (3): CD000245. doi:10.1002/14651858.CD000245.pub3. PMID 24585130.
- ↑ Wong DM, Blumberg DA, Lowe LG (2006). “Guidelines for the use of antibiotics in acute upper respiratory tract infections”. Am Fam Physician. 74 (6): 956–66. PMID 17002029.
- ↑ The American Academy of Family Physicians: Acute Bronchitis. January 2006. Accessed 20 March 2007.
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]; Nate Michalak, B.A.
Overview
Acute bronchitis was first described by Charles Badham in 1808. Dr. Rene Laennec described this disease in greater detail in 1821.
Historical Perspective

- Acute bronchitis was first described by Charles Badham in 1808 in England. He classified acute bronchitis into three forms by his definition (Br.acuta, asthenica and chronica).[1]
- In 1821, Dr. Rene Laennec, known as the “father of chest medicine,” in part to his invention of the stethoscope, described bronchitis in terms of emphysema and chronic bronchitis.[2]
References
- ↑ Klippe HJ, Kirsten D (2009). “[200 years of bronchitis–from 1808 to 2008]”. Pneumologie (in German). 63 (4): 228–30. doi:10.1055/s-0028-1119572. PMID 19343614.
- ↑ terms(2016)https://lunginstitute.com/blog/history-of-chronic-bronchitis/accessed on September,13 2016
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
The pathologic process starts with the inoculation of tracheobranchial epithelium with invading organism, which leads to inflammation, thickening and increased mucus production.
Pathophysiology
Pathogenesis
- The causative agent is transmitted through the large and medium size airway tracts.[1]
- Following transmission, the agent inoculates the tracheobronchial epithelium.
- This process leads to inflammation, thickening, and increased mucus production in the airways compared to normal bronchi as shown below:
-
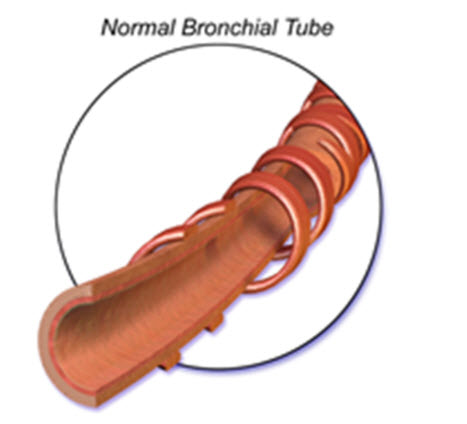 Normal Bronchi
Normal Bronchi -
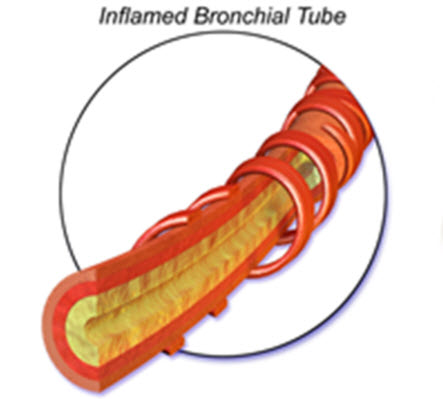 Inflamed Bronchi
Inflamed Bronchi


Microscopy
- On microscopic analysis, epithelial-cell desquamation and denuding of the airway to the level of the basement membrane, in association with the presence of a lymphocytic cellular infiltrate, have been demonstrated.[2]
References
- ↑ Gonzales R, Sande MA (2000). “Uncomplicated acute bronchitis”. Ann. Intern. Med. 133 (12): 981–91. PMID 11119400.
- ↑ WALSH JJ, DIETLEIN LF, LOW FN, BURCH GE, MOGABGAB WJ (1961). “Bronchotracheal response in human influenza. Type A, Asian strain, as studied by light and electron microscopic examination of bronchoscopic biopsies”. Arch. Intern. Med. 108: 376–88. PMID 13782910.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Common causes of acute bronchitis include viruses, bacteria and environmental factors. Among these causes, influenza virus is the most common cause, especially during the winter.[1]
Causes
- Acute Bronchitis may be caused by either viral, bacterial or environmental factors.
- Influenza virus is the most common overall cause.[1][2][3]
| Causes | |||||||||||||||||||||||||||||||||||||||||||||
| Viruses[3][4][5] | Bacteria[2] | Environmental causes[6] | |||||||||||||||||||||||||||||||||||||||||||
| Influenza virus Parainfluenza virus Respiratory syncytial virus Coronavirus Adenovirus Enterovirus Rhinovirus Coxsackievirus Human metapneumovirus | Mycoplasma pneumoniae Chlamydophila pneumoniae Bordetella pertussis | Toxic fume inhalation Tobacco Dust Aerosol | |||||||||||||||||||||||||||||||||||||||||||
Common Causes
- Adenovirus
- Bordetella pertussis
- Hemophilus influenzae
- Influenza virus
- Moraxella catarrhalis
- Mycoplasma pneumoniae
- Rhinovirus
- Streptococcus pneumoniae
Causes by Organ System
| Cardiovascular | No underlying causes | |
| Chemical/Poisoning | Vanadium poisoning | |
| Dental | No underlying causes | |
| Dermatologic | No underlying causes | |
| Drug Side Effect | No underlying causes | |
| Ear Nose Throat | No underlying causes | |
| Endocrine | No underlying causes | |
| Environmental | No underlying causes | |
| Gastroenterologic | No underlying causes | |
| Genetic | No underlying causes | |
| Hematologic | No underlying causes | |
| Iatrogenic | No underlying causes | |
| Infectious Disease | Adenovirus, bordetella pertussis, chickenpox, chlamydia pneumoniae, coronavirus , gram-negative bacilli, haemophilus influenzae, human metapneumovirus, influenza A, influenza B, moraxella catarrhalis, mycoplasma pneumoniae, parainfluenza, respiratory syncytial virus, rhinovirus, staphylococcus aureus, streptococcus pneumoniae | |
| Musculoskeletal/Orthopedic | No underlying causes | |
| Neurologic | No underlying causes | |
| Nutritional/Metabolic | No underlying causes | |
| Obstetric/Gynecologic | No underlying causes | |
| Oncologic | No underlying causes | |
| Ophthalmologic | No underlying causes | |
| Overdose/Toxicity | No underlying causes | |
| Psychiatric | No underlying causes | |
| Pulmonary | No underlying causes | |
| Renal/Electrolyte | No underlying causes | |
| Rheumatology/Immunology/Allergy | No underlying causes | |
| Sexual | No underlying causes | |
| Trauma | No underlying causes | |
| Urologic | No underlying causes | |
| Miscellaneous | No underlying causes |
Causes in Alphabetical Order
References
- ↑ 1.0 1.1 Boldy DA, Skidmore SJ, Ayres JG (1990). “Acute bronchitis in the community: clinical features, infective factors, changes in pulmonary function and bronchial reactivity to histamine”. Respir Med. 84 (5): 377–85. PMID 2174179.
- ↑ 2.0 2.1 Wenzel RP, Fowler AA (2006). “Clinical practice. Acute bronchitis”. N. Engl. J. Med. 355 (20): 2125–30. doi:10.1056/NEJMcp061493. PMID 17108344.
- ↑ 3.0 3.1 Jonsson JS, Sigurdsson JA, Kristinsson KG, Guthnadóttir M, Magnusson S (1997). “Acute bronchitis in adults. How close do we come to its aetiology in general practice?”. Scand J Prim Health Care. 15 (3): 156–60. PMID 9323784.
- ↑ Boivin G, Abed Y, Pelletier G, Ruel L, Moisan D, Côté S, Peret TC, Erdman DD, Anderson LJ (2002). “Virological features and clinical manifestations associated with human metapneumovirus: a new paramyxovirus responsible for acute respiratory-tract infections in all age groups”. J. Infect. Dis. 186 (9): 1330–4. doi:10.1086/344319. PMID 12402203.
- ↑ Louie JK, Hacker JK, Gonzales R, Mark J, Maselli JH, Yagi S, Drew WL (2005). “Characterization of viral agents causing acute respiratory infection in a San Francisco University Medical Center Clinic during the influenza season”. Clin. Infect. Dis. 41 (6): 822–8. doi:10.1086/432800. PMID 16107980.
- ↑ Irwin RS, Madison JM (2000). “The diagnosis and treatment of cough”. N. Engl. J. Med. 343 (23): 1715–21. doi:10.1056/NEJM200012073432308. PMID 11106722.
Differentiating Acute bronchitis from other Disorders
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]; Nate Michalak, B.A.
Overview
Acute bronchitis must be differentiated from other causes of cough and wheezing including: acute exacerbation of chronic bronchitis, asthma and pneumonia.
Differential Diagnosis of Acute Bronchitis
The acute bronchitis must be differentiated from other diseases that may cause cough, dyspnea and wheezing.[1]
| Disease | Findings |
|---|---|
| Chronic Bronchitis | Presents with chronic cough, dyspnea and sputum production for more than three months for two years.[2] |
| Pneumonia | Presents with acute fever, cough and shortness of breath, although pulmonary infiltrate on chest x-ray is an imaging finding.[3] |
| Asthma | Presents with cough, dyspnea and wheezing and typically is a chronic condition which has started from childhood.[4] |
| Gastroesophageal Reflux Disease | May present with chronic, dry cough but the typical symptom is heart burn.[5][6] |
References
- ↑ Albert RH (2010). “Diagnosis and treatment of acute bronchitis”. Am Fam Physician. 82 (11): 1345–50. PMID 21121518.
- ↑ Celli BR, MacNee W (2004). “Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper”. Eur. Respir. J. 23 (6): 932–46. PMID 15219010.
- ↑ Prina E, Ranzani OT, Torres A (2015). “Community-acquired pneumonia”. Lancet. 386 (9998): 1097–108. doi:10.1016/S0140-6736(15)60733-4. PMID 26277247.
- ↑ Busse WW (2011). “Asthma diagnosis and treatment: filling in the information gaps”. J. Allergy Clin. Immunol. 128 (4): 740–50. doi:10.1016/j.jaci.2011.08.014. PMID 21875745.
- ↑ Singh A (2009). “Asthma in older adults”. CMAJ. 181 (12): 929. doi:10.1503/cmaj.109-2049. PMC 2789137. PMID 19969583.
- ↑ Irwin RS, Baumann MH, Bolser DC, Boulet LP, Braman SS, Brightling CE, Brown KK, Canning BJ, Chang AB, Dicpinigaitis PV, Eccles R, Glomb WB, Goldstein LB, Graham LM, Hargreave FE, Kvale PA, Lewis SZ, McCool FD, McCrory DC, Prakash UB, Pratter MR, Rosen MJ, Schulman E, Shannon JJ, Smith Hammond C, Tarlo SM (2006). “Diagnosis and management of cough executive summary: ACCP evidence-based clinical practice guidelines”. Chest. 129 (1 Suppl): 1S–23S. doi:10.1378/chest.129.1_suppl.1S. PMC 3345522. PMID 16428686.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]; Nate Michalak, B.A.
Overview
Acute bronchitis is the ninth most common illness among outpatient visits in the U.S. It’s prevalence depends on season of the year, vaccination status and outbreaks during that particular year. It is common among young children and the elderly.
Epidemiology
Acute bronchitis, as a lower respiratory tract infection, is one of the most common illnesses seen among outpatient visits especially in young children.[1][2][3]
Incidence
- Acute bronchitis affects approximately 5% of adults in the U.S. annually and it becomes more common during cold seasons. Generally, it depends on the season of the year, vaccination status and presence of an epidemic.
- Acute bronchitis affects around 44 in 1000 adults (age over 16 years) per year in the UK, with around 82% of episodes occurring in autumn or winter.[4]
Age
- Acute bronchitis is most common among young children.
Gender
- Acute bronchitis affects men and women equally.
Race
- There is no racial predilection for acute bronchitis.
References
- ↑ Macfarlane J, Holmes W, Gard P, Macfarlane R, Rose D, Weston V, Leinonen M, Saikku P, Myint S (2001). “Prospective study of the incidence, aetiology and outcome of adult lower respiratory tract illness in the community”. Thorax. 56 (2): 109–14. PMC 1746009. PMID 11209098.
- ↑ Wenzel RP, Fowler AA (2006). “Clinical practice. Acute bronchitis”. N. Engl. J. Med. 355 (20): 2125–30. doi:10.1056/NEJMcp061493. PMID 17108344.
- ↑ Ferri FF. Ferri’s Clinical Advisor 2016, 5 Books in 1. Elsevier Health Sciences; 2015.
- ↑ incidence(2016).http://clinicalevidence.bmj.com/x/systematic-review/1508/background.html accessed on September,13 2016
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]; Nate Michalak, B.A.
Overview
Age, season of the year, and the immunization statusare the main determining risk factors for acquiring acute bronchitis.
Risk Factors
Age
- Very young and very old persons are at greatest risk.[1]
Season
Immunization Status
References
- ↑ 1.0 1.1 Gonzales R, Sande MA (2000). “Uncomplicated acute bronchitis”. Ann. Intern. Med. 133 (12): 981–91. PMID 11119400.
- ↑ Wenzel RP, Fowler AA (2006). “Clinical practice. Acute bronchitis”. N. Engl. J. Med. 355 (20): 2125–30. doi:10.1056/NEJMcp061493. PMID 17108344.
- ↑ Albert RH (2010). “Diagnosis and treatment of acute bronchitis”. Am Fam Physician. 82 (11): 1345–50. PMID 21121518.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Screening is not recommended for acute bronchitis.
References
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Acute bronchitis is a self limited respiratory disease with an excellent prognosis which resolves within two weeks in majority of patients.
Natural History
If left untreated, acute bronchitis usually resolves within 2 weeks although it may last up to 2 months.[1][2]
When bronchitis is prolonged, consider:
- Mycoplasma pneumonia
- Chlamydia pneumoniae
- Bordetella pertussis. 13% to 32% of adolescents and adults with a cough lasting six days or more may have B. pertussis.[3][4]
Also consider pneumonia and atypical pneumonia.
Complications
The most common complication of acute bronchitis is persistent cough that my last for 6 weeks.[5] Rarely, in patients with immunosuppression or other debilitating disease, pneumonia occurs as a complication.[6]
Prognosis
Prognosis is generally excellent and most of patients recover after 5-10 days.[5] Recurrent episodes of acute bronchitis in subsequent years occur in 20% of patients.[6]
References
- ↑ Gonzales R, Sande MA (2000). “Uncomplicated acute bronchitis”. Ann. Intern. Med. 133 (12): 981–91. PMID 11119400.
- ↑ Landau LI (2006). “Acute and chronic cough”. Paediatr Respir Rev. 7 Suppl 1: S64–7. doi:10.1016/j.prrv.2006.04.172. PMID 16798599.
- ↑ Hewlett EL, Edwards KM (2005). “Clinical practice. Pertussis–not just for kids”. N. Engl. J. Med. 352 (12): 1215–22. doi:10.1056/NEJMcp041025. PMID 15788498.
- ↑ Cornia PB, Lipsky BA, Saint S, Gonzales R (2007). “Clinical problem-solving. Nothing to cough at–a 73-year-old man presented to the emergency department with a 4-day history of nonproductive cough that worsened at night”. N. Engl. J. Med. 357 (14): 1432–7. doi:10.1056/NEJMcps062357. PMID 17914045.
- ↑ 5.0 5.1 Wenzel RP, Fowler AA (2006). “Clinical practice. Acute bronchitis”. N. Engl. J. Med. 355 (20): 2125–30. doi:10.1056/NEJMcp061493. PMID 17108344.
- ↑ 6.0 6.1 Albert RH (2010). “Diagnosis and treatment of acute bronchitis”. Am Fam Physician. 82 (11): 1345–50. PMID 21121518.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | | Chest X Ray | CT | MRI | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH