
Chronic bronchitis
For Chronic bronchitis patient information click here
see also: Acute bronchitis, COPD
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Bronchitis is an inflammation of the bronchi (medium-size airways) in the lungs. Chronic bronchitis is not necessarily caused by infection and is generally part of a syndrome called chronic obstructive pulmonary disease (COPD); it is defined clinically as persistent cough that produces sputum (phlegm) and mucus for at least three months in two consecutive years. Smoking is the most important risk factor. Typically, it progress to debilitating disease if left untreated. The corner stones for medical therapy are, inhaled bronchodilators and steroids. Smoking cessation and decrease environmental exposure to pollutants are effective measures to control its progression and decrease mortality.
Historical Perspective
Bronchitis was first described by Charles Badham in 1808. Rene Laennec described COPD in details and categorized it as emphysema and chronic bronchitis.[1][2]
Pathophysiology
Hyperplasia and hypertrophy of the goblet cells (mucous gland) of the airway are the common pathologic features of chronic bronchitis. Chronic inflammation due to lymphocyte infiltration is seen on microscopy.[3] On microscopic histopathological analysis there is infiltration of the airway walls with inflammatory cells, particularly CD8+ T-lymphocytes and neutrophils.[4] Inflammation is followed by scarring and remodeling that thickens the walls resulting in narrowing of the small airways.
Causes
Chronic bronchitis, as a subtype of COPD, is caused by multiple environmental and genetic factors. Smoking is the leading cause of chronic bronchitis. Other causes include: air pollutants, occupational exposures to dusts and coal, and auto-immune diseases.[5][6][7][8]
Differentiating Chronic bronchitis from other Diseases
Chronic bronchitis must be differentiated from other causes of chronic cough and dyspnea which include: congestive heart failure, chronic asthma, bronchiectasis, and bronchiolitis obliterans.[9][10]
Epidemiology and Demographics
COPD occurs in 34 out of 1000 patients greater than 65 years old[11] or approximately 25 million people if undiagnosed cases are included.[12] COPD is the third cause of death in the U.S.[13] Hispanics are less likely to report COPD than non-Hispanic whites and blacks (4.0% compared with 6.3% and 6.1%, respectively).[14] Chronic bronchitis mortality rates are higher among Caucasian than among African American or persons of all other races. Women were more likely to report COPD than men (6.7% compared with 5.2%).[14][15] Age adjusted death rates of men decreased between 1999 and 2014 but this rate was stable among women.
Risk Factors
Common risk factors in the development of chronic bronchitis include cigarette smoking, air pollution, genetic factors, increasing age, male gender, allergy, and repeated airway infections.[16][17][18][17][19]
Screening
There is no recommendation for routine screening for adults who do not present with features of chronic bronchitis, such as cough, dyspnea or chest pain, because asymptomatic decreases in lung capacity does not require treatment.[20]
Natural History, Complications, and Prognosis
Prognosis may vary depending on the time of diagnosis and severity of airflow obstruction, which may be measured by FEV1, FVC, or FEV1/FVC. Chronic Bronchitis has a wide range of severity from well controlled chronic bronchitis to severe obstructed airways with multiple exacerbations that require hospitalization and even may develop into lung cancer.[21] COPD gradually deteriorates over time and can lead to death if left untreated. Common complications of chronic bronchitis include: recurrent pneumonia, depression, cor pulmonale, anemia, polycythemia. A good prognosis of COPD relies on an early diagnosis and prompt treatment. Most patients will have improvement in lung function once treatment is started.
Diagnosis
Chronic bronchitis is defined clinically as persistent cough that produces sputum (phlegm), for at least three months in two consecutive years. Bronchitis may be indicated by an expectorating cough (also known as a productive cough, i.e. one that produces sputum), shortness of breath (dyspnea) and wheezing. Occasionally chest pains, fever, and fatigue or malaise may also occur.[22]
History and Symptoms
The hallmark of chronic bronchitis is dyspnea. A positive history of chronic productive cough and shortness of breath is suggestive of chronic bronchitis. Some patients describe the dyspnea as air hunger due to the sensation of gasping for air.[23]
Physical Examination
Chronic bronchitis can be diagnostically evaluated by physical examination through auscultation. Physical examination is quite specific and sensitive for severe disease. The signs are usually difficult to detect in cases of mild to moderate diseases. Findings on general physical examination can be cyanosis, tachypnea, use of accessory respiratory muscles, paradoxical indrawing of lower intercostal spaces (known as the Hoover sign), elevated jugular venous pulse and peripheral edema. Pulmonary examination findings include barrel chest (emphysema), wheezing, hyperresonance, crackles and rhonchi.[18]
Laboratory Findings
Cronic bronchitis has irreversible airflow limitation, especially during forced expiration. This is due to the destruction of lung tissue and increase in resistance to flow in the conducting airways. Thus, it doesn’t show an improvement in FEV1 post bronchodilator administration, unlike asthma. This characteristic feature is used as an diagnostic criteria for COPD (i.e. a COPD is diagnosed by spirometry if FEV1/FVC < 70% for a matched control).[24] Arterial blood gas may show hypoxemia with or without hypercapnia depending on the disease severity. pH may be normal due to renal compensation. A pH less than 7.3 usually indicate severe respiratory compromise. A blood sample taken from an artery (i.e. Arterial Blood Gas (ABG)), can be tested for blood gas levels which may show hypoxemia and/or hypercapnia (respiratory acidosis if pH is also decreased). A blood sample taken from a vein may show a high blood count (reactive polycythemia), a reaction to long-term hypoxemia.
Electrocardiogram
Electrocardiographic findings in chronic bronchitis includes: P pulmonale, Right ventricular strain, Right ventricular hypertrophy, and S1S2S3 pattern.[25]
X Ray
Generally, chest x ray is not recommended for chronic bronchitis diagnosis, but it is common to order it to rule out other causes of dyspnea and productive cough such as: pneumonia and heart failure. The common findings for chronic bronchitis include: hyperinflation and hyperlucency of the lungs.[18]
CT
CT scan is not generally required for chronic bronchitis but it is helpful to rule out other causes of dyspnea and chronic cough.
Echocardiography
Echocardiography is helpful to diagnose pulmonary hypertension in patients with long standing chronic bronchitis.
Treatment
The main goal of chronic bronchitis treatment is to improve the lung function and slow down the loss of its function. In this regard the treatment plan is divided in to two main categories:
- Reduce symptoms: by relief of dyspnea and improve exercise tolerance
- Reduce risks: by treating exacerbations, preventing disease progression and reducing mortality
Medical Therapy
Inhaled bronchodilators and steroids are the corner stones of medical therapy for chronic bronchitis.
Primary Prevention
Smoking cessation, control of air pollutants and decreased job exposure to dusts or fumes are the main preventative measures for chronic bronchitis.[26]
Secondary Prevention
Smoking cessation and decreased occupational exposure are the corner stones to decreasing the mortality and morbidity of chronic bronchitis.
References
- ↑ terms(2016)https://lunginstitute.com/blog/history-of-chronic-bronchitis/accessed on September,13 2016
- ↑ Klippe HJ, Kirsten D (2009). “[200 years of bronchitis–from 1808 to 2008]”. Pneumologie (in German). 63 (4): 228–30. doi:10.1055/s-0028-1119572. PMID 19343614.
- ↑ Hogg JC (2004). “Pathophysiology of airflow limitation in chronic obstructive pulmonary disease”. Lancet. 364 (9435): 709–21. doi:10.1016/S0140-6736(04)16900-6. PMID 15325838.
- ↑ Baraldo S, Turato G, Badin C, Bazzan E, Beghé B, Zuin R, Calabrese F, Casoni G, Maestrelli P, Papi A, Fabbri LM, Saetta M (2004). “Neutrophilic infiltration within the airway smooth muscle in patients with COPD”. Thorax. 59 (4): 308–12. PMC 1763819. PMID 15047950.
- ↑ MedicineNet.com – COPD causes
- ↑ Young RP, Hopkins RJ, Christmas T, Black PN, Metcalf P, Gamble GD (2009). “COPD prevalence is increased in lung cancer, independent of age, sex and smoking history”. Eur. Respir. J. 34 (2): 380–6. doi:10.1183/09031936.00144208. PMID 19196816. Unknown parameter
|month=ignored (help) - ↑ Devereux, Graham (2006). “Definition, epidemiology, and risk factors”. BMJ. 332 (7550): 1142–4. doi:10.1136/bmj.332.7550.1142. PMC 1459603. PMID 16690673. Unknown parameter
|month=ignored (help) - ↑ Kennedy SM, Chambers R, Du W, Dimich-Ward H (2007). “Environmental and occupational exposures: do they affect chronic obstructive pulmonary disease differently in women and men?”. Proceedings of the American Thoracic Society. 4 (8): 692–4. doi:10.1513/pats.200707-094SD. PMID 18073405. Unknown parameter
|month=ignored (help) - ↑ Busse WW (2011). “Asthma diagnosis and treatment: filling in the information gaps”. J. Allergy Clin. Immunol. 128 (4): 740–50. doi:10.1016/j.jaci.2011.08.014. PMID 21875745.
- ↑ Prina E, Ranzani OT, Torres A (2015). “Community-acquired pneumonia”. Lancet. 386 (9998): 1097–108. doi:10.1016/S0140-6736(15)60733-4. PMID 26277247.
- ↑ wrongdiagnosis.com > Prevalence and Incidence of COPD Retrieved on Mars 14, 2010
- ↑ MORBIDITY & MORTALITY: 2009 CHART BOOK ON CARDIOVASCULAR, LUNG, AND BLOOD DISEASES National Heart, Lung, and Blood Institute
- ↑ Kenneth D. Kochanek, M.A.; Jiaquan Xu, M.D.; Sherry L. Murphy, B.S.; Arialdi M. Minin˜o, M.P.H.; and Hsiang-Ching Kung, Ph.D., Division of Vital Statistics, Deaths: Final Data for 2009, 2011, 60,National Vital Statistics Reports, http://www.cdc.gov/nchs/data/nvsr/nvsr60/nvsr60_03.pdf
- ↑ 14.0 14.1 Morbidity and Mortality Weekly Report (MMWR).(2011).https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6146a2.htm Accessed on September 19,2016
- ↑ Hogg JC, Chu F, Utokaparch S, Woods R, Elliott WM, Buzatu L, Cherniack RM, Rogers RM, Sciurba FC, Coxson HO, Paré PD (2004). “The nature of small-airway obstruction in chronic obstructive pulmonary disease”. N. Engl. J. Med. 350 (26): 2645–53. doi:10.1056/NEJMoa032158. PMID 15215480.
- ↑ PIERCE JA, HOCOTT JB, EBERT RV (1961). “The collagen and elastin content of the lung in emphysema”. Ann. Intern. Med. 55: 210–22. PMID 13735539.
- ↑ 17.0 17.1 Raherison C, Girodet PO (2009). “Epidemiology of COPD”. Eur Respir Rev. 18 (114): 213–21. doi:10.1183/09059180.00003609. PMID 20956146.
- ↑ 18.0 18.1 18.2 Mehta GR, Mohammed R, Sarfraz S, Khan T, Ahmed K, Villareal M, Martinez D, Iskander J, Mohammed R (2016). “Chronic obstructive pulmonary disease: A guide for the primary care physician”. Dis Mon. 62 (6): 164–87. doi:10.1016/j.disamonth.2016.03.002. PMID 27087562.
- ↑ Jeffery PK (2000). “Comparison of the structural and inflammatory features of COPD and asthma. Giles F. Filley Lecture”. Chest. 117 (5 Suppl 1): 251S–60S. PMID 10843939.
- ↑ Amir Qaseem, Timothy J. Wilt, Steven E. Weinberger, Nicola A. Hanania, Gerard Criner, Thys van der Molen, Darcy D. Marciniuk, Tom Denberg, Holger Schunemann, Wisia Wedzicha, Roderick MacDonald & Paul Shekelle (2011). “Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society”. Annals of internal medicine. 155 (3): 179–191. doi:10.7326/0003-4819-155-3-201108020-00008. PMID 21810710. Unknown parameter
|month=ignored (help) - ↑ Mannino DM, Buist AS, Petty TL, Enright PL, Redd SC (2003). “Lung function and mortality in the United States: data from the First National Health and Nutrition Examination Survey follow up study”. Thorax. 58 (5): 388–93. PMC 1746680. PMID 12728157.
- ↑ Vanfleteren LE, Spruit MA, Wouters EF, Franssen FM (2016). “Management of chronic obstructive pulmonary disease beyond the lungs”. Lancet Respir Med. doi:10.1016/S2213-2600(16)00097-7. PMID 27264777.
- ↑ Festic E, Bansal V, Gajic O, Lee AS (2014). “Prehospital use of inhaled corticosteroids and point prevalence of pneumonia at the time of hospital admission: secondary analysis of a multicenter cohort study”. Mayo Clin. Proc. 89 (2): 154–62. doi:10.1016/j.mayocp.2013.10.028. PMC 3989069. PMID 24485129.
- ↑ Brusasco V, Martinez F (2014). “Chronic obstructive pulmonary disease”. Compr Physiol. 4 (1): 1–31. doi:10.1002/cphy.c110037. PMID 24692133.
- ↑ Lazović B, Svenda MZ, Mazić S, Stajić Z, Delić M (2013). “Analysis of electrocardiogram in chronic obstructive pulmonary disease patients”. Med Pregl. 66 (3–4): 126–9. PMID 23653989.
- ↑ Joy M (2004). “Management of chronic obstructive pulmonary disease”. N. Engl. J. Med. 351 (14): 1461–3, author reply 1461–3. PMID 15459997.
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Bronchitis was first described by Charles Badham in 1808. Rene Laennec, described COPD in details and categorized it as emphysema and chronic bronchitis.
Historical Perspective
- Bronchitis was first described by Charles Badham in 1808 in England. He classified acute bronchitis to three forms by his definition (Br. acuta, asthenica and chronica)[1]
- In 1821, Dr. Rene Laennec, known as the father of chest medicine, thanks in part to his invention of the stethoscope, described bronchitis in terms of emphysema and chronic bronchitis[2]
- John Hutchinson, by inventing Spirometer in 1846, established a new era for diagnosis of lung diseases by measuring the lung capacities
References
- ↑ Klippe HJ, Kirsten D (2009). “[200 years of bronchitis–from 1808 to 2008]”. Pneumologie (in German). 63 (4): 228–30. doi:10.1055/s-0028-1119572. PMID 19343614.
- ↑ terms(2016)https://lunginstitute.com/blog/history-of-chronic-bronchitis/accessed on September,13 2016
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
There is no classification system established for chronic bronchitis.
Classification
There is no classification system established for chronic bronchitis.
References
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Hyperplasia and hypertrophy of the goblet cells (mucous gland) of the airway are the common pathologic features of chronic bronchitis. Chronic inflammation due to lymphocyte infiltration is seen on microscopy.
Pathophysiology
Pathogenesis
- Hallmark features include: hyperplasia (increased number) and hypertrophy (increased size) of the goblet cells (mucous gland) of the airway, resulting in an increase in secretion of mucus, which contributes to the airway obstruction.[1]
- Narrowing of the airways reduces the rate at which air can flow to and from the air sacs (alveoli) and limits the effectiveness of the lungs.
Microscopy
- On microscopic histopathological analysis, there is infiltration of the airway walls with inflammatory cells, particularly CD8+ T-lymphocytes and neutrophils.[2] Inflammation is followed by scarring and remodeling that thickens the walls resulting in narrowing of the small airways.
References
- ↑ Hogg JC (2004). “Pathophysiology of airflow limitation in chronic obstructive pulmonary disease”. Lancet. 364 (9435): 709–21. doi:10.1016/S0140-6736(04)16900-6. PMID 15325838.
- ↑ Baraldo S, Turato G, Badin C, Bazzan E, Beghé B, Zuin R, Calabrese F, Casoni G, Maestrelli P, Papi A, Fabbri LM, Saetta M (2004). “Neutrophilic infiltration within the airway smooth muscle in patients with COPD”. Thorax. 59 (4): 308–12. PMC 1763819. PMID 15047950.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Chronic bronchitis as a main category of COPD is caused by multiple environmental and genetic factors. Smoking is the leading cause of chronic bronchitis.
Causes
Common Causes
Smoking
- The primary risk factor for COPD is chronic tobacco smoking. In the United States, 80 to 90% of cases of COPD are due to smoking.[1][2]
- Exposure to cigarette smoke is measured in pack-years,[3] the average number of packages of cigarettes smoked daily multiplied by the number of years of smoking.
- The likelihood of developing COPD increases with age and cumulative smoke exposure. Majority of life-long smokers will develop COPD, provided that smoking-related extrapulmonary diseases (cardiovascular, diabetes, cancer) do not claim their lives beforehand.[4]
Occupational Exposures
- Intense and prolonged exposure to workplace dusts found in coal mining, gold mining, and the cotton textile industry and chemicals such as cadmium, isocyanates, and fumes from welding have been implicated in the development of airflow obstruction, even in nonsmokers.[5]
- Workers who smoke and are exposed to these particles and gases are even more likely to develop COPD.
- Intense silica dust exposure causes silicosis, a restrictive lung disease distinct from COPD; however, less intense silica dust exposures have been linked to a COPD-like condition.[6]
- The effect of occupational pollutants on the lungs appears to be substantially less important than the effect of cigarette smoking.[7]
Air Pollution
- People who live in large cities have a higher rate of COPD compared to people who live in rural areas.[8]
- Urban air pollution may be a contributing factor for COPD, as it is thought to slow the normal growth of the lungs. Long-term research is needed to confirm this link.
- Studies have demonstrated a direct relationship between the waste gas and COPD/asthma-aggravating compound, sulfur dioxide, and an inverse relationship between the blue lichen Xanthoria (usually found abundantly in the countryside, but never in towns or cities) and the exacerbation of COPD.
- In many developing countries, indoor air pollution from cooking fire smoke (often using biomass fuels such as wood and animal dung) is a common cause of COPD, especially in women.[9]
Genetics
- A genetic component appears to be required for susceptibility in developing COPD, even in heavy smokers. COPD is more common among relatives of COPD patients who smoke than unrelated smokers.[10]
- The genetic differences that make some peoples’ lungs susceptible to the effects of tobacco smoke are mostly unknown.
- Alpha 1-antitrypsin deficiency is a genetic condition that is responsible for about 2% of COPD cases. In this condition, the body does not make enough of a protein, alpha 1-antitrypsin. Alpha 1-antitrypsin protects the lungs from damage caused by protease enzymes, such as elastase and trypsin, that can be released as a result of an inflammatory response to tobacco smoke.[11]
Autoimmune Disease
- There is mounting evidence that there may be an autoimmune component to COPD, triggered by lifelong smoking.[12]
- Many individuals with COPD who have stopped smoking have active inflammation in the lungs.[13] The disease may continue to progress for many years after smoking cesssation due to this ongoing inflammation.[13] This sustained inflammation is thought to be mediated by autoantibodies and autoreactive T cells.[13][14][15]
Other Risk Factors
- A characteristic of asthma, also common in COPD patients is the tendency for airways to suddenly constrict in response to inhaled irritants (bronchial hyperresponsiveness). In COPD, the presence of bronchial hyperresponsiveness predicts poorer prognosis of the disease.[7] It is not known if bronchial hyperresponsiveness is a cause or a consequence of COPD.
- Other risk factors such as repeated lung infection and possibly a diet high in cured meats (possibly due to the preservative sodium nitrite) may be related to the development of COPD.
Causes by Organ System
| Cardiovascular | No underlying causes |
| Chemical / poisoning | Silicosis, Isocyanates, Cigarette smoking, Cadmium, Sulfur dioxide |
| Dermatologic | No underlying causes |
| Drug Side Effect | Goserelin, Pramipexole, Zanamivir |
| Ear Nose Throat | No underlying causes |
| Endocrine | No underlying causes |
| Environmental | Use of biomass fuels for cooking, Second hand smoking, Occupational pollution exposure to dusts and chemicals, Fumes from welding, Environmental air pollution such as coal, grain |
| Gastroenterologic | No underlying causes |
| Genetic | Tumor necrosis factor-alpha (TNF-a) gene polymorphisms, Several SNPs of the leptin receptor (LEPR) gene,
Several gene polymorphisms of Transforming growth factor beta 1, Metalloproteinase dysregulation, Increased Matrix metalloproteinases ( MMP)-9 (gelatinase B), Increased Matrix metalloproteinases (MMP)-8 (Collagenase 2), Increased Matrix metalloproteinases (MMP)-2 (gelatinase A), Heredity, Genetic influences, Excess elastase, Decreased glutathione S-transferase P1 activity, Decreased glutathione levels, Decreased function of microsomal epoxide hydrolase, Decreased function of microsomal epoxide hydrolase, Alpha-1-antitrypsin deficiency, Abnormal activity of tissue inhibitors of metalloproteinase (TIMP-1) |
| Hematologic | No underlying causes |
| Iatrogenic | No underlying causes |
| Infectious Disease | Pulmonary tuberculosis, History of childhood respiratory infections |
| Musculoskeletal / Ortho | No underlying causes |
| Neurologic | No underlying causes |
| Nutritional / Metabolic | Vitamin C deficiency, Deficiency of antioxidant vitamins, Vitamin E deficiency |
| Obstetric/Gynecologic | No underlying causes |
| Oncologic | No underlying causes |
| Opthalmologic | No underlying causes |
| Overdose / Toxicity | No underlying causes |
| Psychiatric | No underlying causes |
| Pulmonary | Bronchitis, Bronchiectasis, Bronchiolitis obliterans, Early childhood recurrent Pneumonia, Silicosis, Increased airway responsiveness, Bronchopulmonary dysplasia, Asthma (controversial), Pulmonary tuberculosis |
| Renal / Electrolyte | No underlying causes |
| Rheum / Immune / Allergy | Atopy |
| Sexual | Gender (controversial), more common in male |
| Trauma | No underlying causes |
| Urologic | No underlying causes |
| Miscellaneous | Nicotine addiction, Low socioeconomic status, First-degree relatives with severe premature COPD, Age |
Causes in Alphabetical Order
External Links
http://www.cdc.gov/copd/index.htm
References
- ↑ MedicineNet.com – COPD causes
- ↑ Young RP, Hopkins RJ, Christmas T, Black PN, Metcalf P, Gamble GD (2009). “COPD prevalence is increased in lung cancer, independent of age, sex and smoking history”. Eur. Respir. J. 34 (2): 380–6. doi:10.1183/09031936.00144208. PMID 19196816. Unknown parameter
|month=ignored (help) - ↑ “Definition of pack year – NCI Dictionary of Cancer Terms”.
- ↑ Template:Cite doi
- ↑ Devereux, Graham (2006). “Definition, epidemiology, and risk factors”. BMJ. 332 (7550): 1142–4. doi:10.1136/bmj.332.7550.1142. PMC 1459603. PMID 16690673. Unknown parameter
|month=ignored (help) - ↑ Hnizdo E, Vallyathan V (2003). “Chronic obstructive pulmonary disease due to occupational exposure to silica dust: a review of epidemiological and pathological evidence”. Occup Environ Med. 60 (4): 237–43. doi:10.1136/oem.60.4.237. PMC 1740506. PMID 12660371. Unknown parameter
|month=ignored (help) - ↑ 7.0 7.1 Loscalzo, Joseph; Fauci, Anthony S.; Braunwald, Eugene; Dennis L. Kasper; Hauser, Stephen L; Longo, Dan L. (2008). Harrison’s Principles of Internal Medicine (17th ed.). McGraw-Hill Professional. ISBN 0-07-146633-9.
- ↑ Halbert RJ, Natoli JL, Gano A, Badamgarav E, Buist AS, Mannino DM (2006). “Global burden of COPD: systematic review and meta-analysis”. Eur. Respir. J. 28 (3): 523–32. doi:10.1183/09031936.06.00124605. PMID 16611654. Unknown parameter
|month=ignored (help) - ↑ Kennedy SM, Chambers R, Du W, Dimich-Ward H (2007). “Environmental and occupational exposures: do they affect chronic obstructive pulmonary disease differently in women and men?”. Proceedings of the American Thoracic Society. 4 (8): 692–4. doi:10.1513/pats.200707-094SD. PMID 18073405. Unknown parameter
|month=ignored (help) - ↑ Silverman EK, Chapman HA, Drazen JM; et al. (1998). “Genetic epidemiology of severe, early-onset chronic obstructive pulmonary disease. Risk to relatives for airflow obstruction and chronic bronchitis”. Am. J. Respir. Crit. Care Med. 157 (6 Pt 1): 1770–8. PMID 9620904. Unknown parameter
|month=ignored (help) - ↑ MedlinePlus Encyclopedia 000091
- ↑ Agustí A, MacNee W, Donaldson K, Cosio M. (2003). “Hypothesis: Does COPD have an autoimmune component?”. Thorax. 58 (10): 832–4. doi:10.1136/thorax.58.10.832. PMC 1746486. PMID 14514931.
- ↑ 13.0 13.1 13.2 Rutgers SR, Postma DS, ten Hacken NH; et al. (2000). “Ongoing airway inflammation in patients with COPD who do not currently smoke”. Thorax. 55 (1): 12–8. doi:10.1136/thorax.55.1.12. PMC 1745599. PMID 10607796. Unknown parameter
|month=ignored (help) - ↑ Feghali-Bostwick CA, Gadgil AS, Otterbein LE; et al. (2008). “Autoantibodies in Patients with Chronic Obstructive Pulmonary Disease”. Am. J. Respir. Crit. Care Med. 177 (2): 156–63. doi:10.1164/rccm.200701-014OC. PMC 2204079. PMID 17975205. Unknown parameter
|month=ignored (help) - ↑ Lee SH, Goswami S, Grudo A; et al. (2007). “Antielastin autoimmunity in tobacco smoking-induced emphysema”. Nat. Med. 13 (5): 567–9. doi:10.1038/nm1583. PMID 17450149. Unknown parameter
|month=ignored (help)
Differentiating Chronic bronchitis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Chronic bronchitis must be differentiated from congestive heart failure, chronic asthma, bronchiectasis, and bronchiolitis obliterans.
Differential Diagnosis
| Disease | Findings |
|---|---|
| Congestive heart failure | Features with orthopnea, paroxysmal nocturnal dyspnea, fine crackles on auscultation, and chest x ray findings of cardiac enlargement and pulmonary congestion (Kerley B lines, and pleural effusion) |
| Bronchiectasis | Presents copious purulent sputum, coarse crackles, clubbing and CT findings suggestive of bronchiectasis[1] |
| Asthma | Presents with cough, dyspnea and wheezing and typically is a chronic condition which has started from childhood[1] |
| Bronchiolitis obliterans | Has history of collagen vascular disease, usually young patient without a history of smoking and CT scan shows finding of mosaic attenuation and no evidence of emphysema |
| Pneumonia | Presents with acute fever, cough and shortness of breath, although pulmonary infiltrate on chest X-ray is an imaging finding[2]. |
References
- ↑ 1.0 1.1 Busse WW (2011). “Asthma diagnosis and treatment: filling in the information gaps”. J. Allergy Clin. Immunol. 128 (4): 740–50. doi:10.1016/j.jaci.2011.08.014. PMID 21875745.
- ↑ Prina E, Ranzani OT, Torres A (2015). “Community-acquired pneumonia”. Lancet. 386 (9998): 1097–108. doi:10.1016/S0140-6736(15)60733-4. PMID 26277247.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Chronic bronchitis is a part of COPD and its epidemiology is discussed as a sub-group of COPD. COPD occurs in 34 out of 1000 patients greater than 65 years old. In England, an estimated 842,100 of 50 million people have a diagnosis of COPD; translating into approximately one person in 59 receiving a diagnosis of COPD at some point in their lives. In the most socioeconomically deprived parts of the country, one in 32 people were diagnosed with COPD, compared with one in 98 in the most affluent areas. In the United States, the prevalence of COPD is approximately 1 in 20 or 5%, totaling approximately 13.5 million people in USA,[1][2] or approximately 25 million people if undiagnosed cases are included.[3]
Epidemiology and Demographics
Mortality
- COPD is the third cause of death in the U.S.[4]
- In 2005, approximately one in 20 deaths in the United States had COPD as the underlying cause.
- Smoking is estimated to be responsible for at least 75% of COPD deaths.
Age
- Chronic bronchitis occurs in old ages especially in persons over 65 years old.
Race
- Hispanics were less likely to report COPD than non-Hispanic whites and blacks (4.0% compared with 6.3% and 6.1%, respectively).[1]
- Chronic bronchitis mortality rates are higher among whites than among blacks or persons of all other races.
Gender
- Women were more likely to report COPD than men (6.7% compared to 5.2%)[1][5].
- Age adjusted death rates of men have decreased between 1999 and 2014 but this rate was stable among women.
-
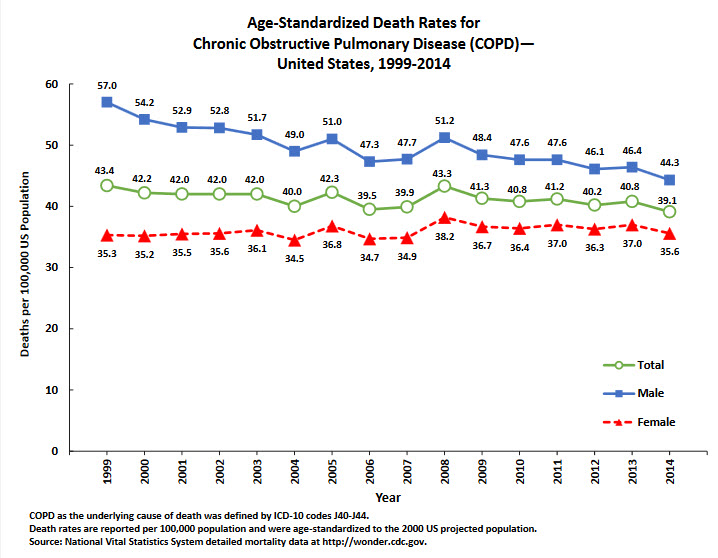 COPD adjusted death rates
COPD adjusted death rates -
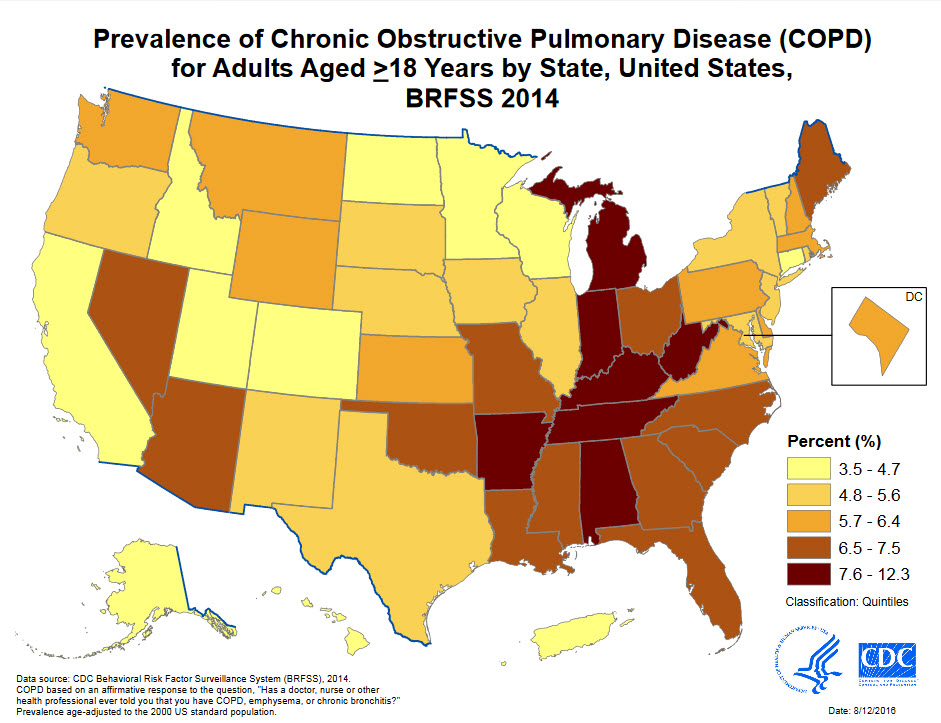 COPD Prevalence
COPD Prevalence


Source: https://www.cdc.gov/
References
- ↑ 1.0 1.1 1.2 Morbidity and Mortality Weekly Report (MMWR).(2011).https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6146a2.htm Accessed on September 19,2016
- ↑ wrongdiagnosis.com > Prevalence and Incidence of COPD Retrieved on Mars 14, 2010
- ↑ MORBIDITY & MORTALITY: 2009 CHART BOOK ON CARDIOVASCULAR, LUNG, AND BLOOD DISEASES National Heart, Lung, and Blood Institute
- ↑ Kenneth D. Kochanek, M.A.; Jiaquan Xu, M.D.; Sherry L. Murphy, B.S.; Arialdi M. Minin˜o, M.P.H.; and Hsiang-Ching Kung, Ph.D., Division of Vital Statistics, Deaths: Final Data for 2009, 2011, 60,National Vital Statistics Reports, http://www.cdc.gov/nchs/data/nvsr/nvsr60/nvsr60_03.pdf
- ↑ Hogg JC, Chu F, Utokaparch S, Woods R, Elliott WM, Buzatu L, Cherniack RM, Rogers RM, Sciurba FC, Coxson HO, Paré PD (2004). “The nature of small-airway obstruction in chronic obstructive pulmonary disease”. N. Engl. J. Med. 350 (26): 2645–53. doi:10.1056/NEJMoa032158. PMID 15215480.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Common risk factors in the development of chronic bronchitis include cigarette smoking, air pollution, genetic factors, increasing age, male gender, allergy, and repeated airway infections.
Risk Factors
The most potent risk factor for development of chronic bronchitis is smoking. Other risk factors include: environmental exposures, genetic susceptibility, air pollution and respiratory infections.
Cigarette smoking
Occupational exposure
- Dusts, gases, fumes, or organic antigens can contribute to increased airways responsiveness.[3][2][4]
Genetic factors
- Alpha-1 antitrypsin (AAT) deficiency is the leading genetic risk factor for developing chronic bronchitis.[3][2][5] Some novel risk factors such as, small nucleotide polymorphisms and gene clusters, are assumed to be involved in developing chronic airway diseases.[6]
Developmentally abnormal lungs
- Frequent childhood infection may cause scarring of lungs, decrease elasticity, thereby increasing risk for COPD.
References
- ↑ PIERCE JA, HOCOTT JB, EBERT RV (1961). “The collagen and elastin content of the lung in emphysema”. Ann. Intern. Med. 55: 210–22. PMID 13735539.
- ↑ 2.0 2.1 2.2 Raherison C, Girodet PO (2009). “Epidemiology of COPD”. Eur Respir Rev. 18 (114): 213–21. doi:10.1183/09059180.00003609. PMID 20956146.
- ↑ 3.0 3.1 Mehta GR, Mohammed R, Sarfraz S, Khan T, Ahmed K, Villareal M, Martinez D, Iskander J, Mohammed R (2016). “Chronic obstructive pulmonary disease: A guide for the primary care physician”. Dis Mon. 62 (6): 164–87. doi:10.1016/j.disamonth.2016.03.002. PMID 27087562.
- ↑ Jeffery PK (2000). “Comparison of the structural and inflammatory features of COPD and asthma. Giles F. Filley Lecture”. Chest. 117 (5 Suppl 1): 251S–60S. PMID 10843939.
- ↑ Gadek JE, Fells GA, Crystal RG (1979). “Cigarette smoking induces functional antiprotease deficiency in the lower respiratory tract of humans”. Science. 206 (4424): 1315–6. PMID 316188.
- ↑ Han MK, Agusti A, Calverley PM, Celli BR, Criner G, Curtis JL, Fabbri LM, Goldin JG, Jones PW, Macnee W, Make BJ, Rabe KF, Rennard SI, Sciurba FC, Silverman EK, Vestbo J, Washko GR, Wouters EF, Martinez FJ (2010). “Chronic obstructive pulmonary disease phenotypes: the future of COPD”. Am. J. Respir. Crit. Care Med. 182 (5): 598–604. doi:10.1164/rccm.200912-1843CC. PMID 20522794.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Screening does not apply to chronic bronchitis.
Screening
There is no recommendation for routine screening for adults who do not present with any chronic bronchitis features such as, cough, dyspnea or chest pain, because an asymptomatic decrease in lung capacity does not require treatment.[1]
References
- ↑ Amir Qaseem, Timothy J. Wilt, Steven E. Weinberger, Nicola A. Hanania, Gerard Criner, Thys van der Molen, Darcy D. Marciniuk, Tom Denberg, Holger Schunemann, Wisia Wedzicha, Roderick MacDonald & Paul Shekelle (2011). “Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society”. Annals of internal medicine. 155 (3): 179–191. doi:10.7326/0003-4819-155-3-201108020-00008. PMID 21810710. Unknown parameter
|month=ignored (help)
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Several determining factors have been known to influence the course of chronic bronchitis including: cigarette smoking, level of airflow obstruction, and recurrent infection. It may be complicated by pneumonia, cor-pulmonale or anemia. Also, because of chronic nature of this disease, depression and increased risk of lung cancer are expected to seen in the disease course. Prognosis depends on early diagnosis and adequate treatment. However, FEV1 level is the most important prognostic factor.
Natural History
Prognosis may vary depending on the time of diagnosis and severity of airflow obstruction, which may be measured by FEV1, FVC and FEV1/FVC. Chronic Bronchitis has a wide range of severity from well controlled chronic bronchitis to severe obstructed airways with multiple exacerbations that require hospitalization and even may develop into lung cancer.[1] COPD gradually deteriorates over time and can lead to death if left untreated.
Complications
Common complications of chronic bronchitis include:
- Recurrent pneumonia: chronic inflammation and airways damage predispose chronic bronchitis patients to recurrent pneumonia either viral or bacterial infections. Additionally, chronic use of inhaled corticosteroids may cause recurrent infections[2]
- Depression: may require psychiatry consultation[3]
- Cor pulmonale: chronic hypoxia and subsequent vasoconstriction in pulmonary vasculature results in pulmonary hypertension and right sided heart failure, termed cor pulmonale[4]
- Anemia: anemia of chronic disease may develop in this patients and indicates a poor prognosis.
- Polycythemia: secondary to chronic hypoxemia, Hematocrit level may rise up to 60 (normal range: adult men: 46±4, adult women:40±4).
Prognosis
A good prognosis of COPD relies on an early diagnosis and prompt treatment. Majority of patients will have improvement in lung function once treatment is started. The most important prognostic factor is the FEV1 level. Other determining factors include:[5]
- Cigarette smoking
- BMI ≤ 21
- Decreased exercise capacity
- Increased C-reactive protein level
- Co-morbid diseases
References
- ↑ Mannino DM, Buist AS, Petty TL, Enright PL, Redd SC (2003). “Lung function and mortality in the United States: data from the First National Health and Nutrition Examination Survey follow up study”. Thorax. 58 (5): 388–93. PMC 1746680. PMID 12728157.
- ↑ Singh S, Amin AV, Loke YK (2009). “Long-term use of inhaled corticosteroids and the risk of pneumonia in chronic obstructive pulmonary disease: a meta-analysis”. Arch. Intern. Med. 169 (3): 219–29. doi:10.1001/archinternmed.2008.550. PMID 19204211.
- ↑ Ohayon MM (2014). “Chronic Obstructive Pulmonary Disease and its association with sleep and mental disorders in the general population”. J Psychiatr Res. 54: 79–84. doi:10.1016/j.jpsychires.2014.02.023. PMID 24656426.
- ↑ Klinger JR, Hill NS (1991). “Right ventricular dysfunction in chronic obstructive pulmonary disease. Evaluation and management”. Chest. 99 (3): 715–23. PMID 1995228.
- ↑ Vanfleteren LE, Spruit MA, Wouters EF, Franssen FM (2016). “Management of chronic obstructive pulmonary disease beyond the lungs”. Lancet Respir Med. doi:10.1016/S2213-2600(16)00097-7. PMID 27264777.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | CT | Echocardiography or Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Related Chapters
Related Chapters
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH