
Rheumatic fever
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Lance Christiansen, D.O.; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Varun Kumar, M.B.B.S. [3]; Anthony Gallo, B.S. [4]
Synonyms and Keywords: RF; Rheumatic heart disease; RHD; Acute rheumatic fever; Chronic rheumatic fever; Rheumatic carditis
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Varun Kumar, M.B.B.S. [2]; Anthony Gallo, B.S. [3]
Overview
Rheumatic fever is a systemic immune disease that may develop after an infection with Streptococcus bacteria, such as strep throat and scarlet fever. It usually affects the heart, joints, blood vessels, and brain. Based on the duration of symptoms, rheumatic fever may be classified into either acute or chronic. The most common cause of rheumatic fever is Group A beta-hemolytic streptococci infection. If left untreated, rheumatic fever may cause valvular diseases including stenosis, regurgitation of mitral/aortic valves and myocarditis. This may lead to decreased cardiac output, pulmonary edema, and ultimately cardiac failure. For cases without carditis, the prognosis is excellent, demonstrating no residual heart disease. In cases with preexisting heart disease, the prognosis is poor, leading to mortality. Common complications of rheumatic fever include arrhythmias, systemic emboli, and stroke. Common physical examination findings include fever, cardiac murmurs, and erythema marginatum. Echocardiogram and radiograph may be diagnostic of rheumatic fever. The Jones criteria is used to establish the diagnosis of rheumatic fever. Rheumatic fever is usually treated using antibiotics to control Streptococcus infection and medications such as aspirin and corticosteroids to decrease inflammation. A long-lasting dose of penicillin is important and effective to prevent further complications and recurrence.
Historical Perspective
Rheumatic fever was first described by Hippocrates, a Greek physician, between 400-370 B.C. The term was first used post-Renaissance by Guillaume de Baillou, a French physician, in the early 1600s. T. Duckett Jones, MD was the first to publish a set of diagnostic criteria in 1944.
Classification
Based on the duration of symptoms, rheumatic fever may be classified into either acute or chronic.
Pathophysiology
Rheumatic fever is the result of an autoimmunological sequelae to a virulent Streptococcus pyogenes infection in a patient who was immunologically sensitized from prior infections. During a streptococcal infection, activated antigen-presenting cells, such as macrophages, present the bacterial antigen to helper T cells. Helper T cells subsequently activate B cells and induce the production of antibodies against the cell wall of Streptococcus. However the antibodies also act against the myocardium and joints, producing the symptoms of rheumatic fever.
Causes
Rheumatic fever is usually caused by an infection with Group A beta-hemolytic Streptococcus pyogenes.
Differentiating Rheumatic Fever from Other Diseases
Rheumatic fever must be differentiated from other diseases that cause fever, skin rash, nausea and fatigue, such as typhoid fever, malaria, lassa fever, ebola, and scarlet fever.
Epidemiology and Demographics
The incidence of rheumatic fever among developed countries such as the USA and Canada was approximately 20-40 per 100,000 individuals during the period 1970-1990 with rheumatic heart disease occurring sporadically. Over past two decades, the prevalence of rheumatic fever has decreased to 5-20 per 100,000 individuals in Canada and <5 per 100,000 individuals in the USA with no new cases of rheumatic heart disease. Rheumatic fever is endemic in many developing countries and is usually observed among children between the ages of 5-15.
Risk Factors
Common risk factors in the development of rheumatic fever include low socioeconomic status, inadequate healthcare, and poor sanitation.
Screening
Screening of rheumatic fever is important as many cases of rheumatic heart disease are subclinical. Echocardiography among inhabitants of high risk regions is recommended. If any abnormality is detected on echocardiography, further cardiac evaluation is performed followed by antimicrobial therapy.
Natural History, Complications, and Prognosis
If left untreated, patients with rheumatic fever may progress to develop arrhythmias, systemic emboli, and endocarditis, which may lead to cardiac failure. Common complications of rheumatic fever include stenosis, carditis, and stroke. Prognosis is generally poor if left untreated.
Diagnosis
Jones Criteria
The Jones criteria can be used to establish the diagnosis of rheumatic fever. The Jones Criteria for definitive rheumatic fever require evidence of streptococcal infection: elevated or rising antistreptolysin O titre or DNAase and either:
- Two major criteria
OR
- One major and two minor criteria
History and Symptoms
A detailed and thorough history from the patient is necessary. Specific areas of focus when obtaining a history from the patient include prior rheumatic fever infection, family history of rheumatic fever, and recent streptococcal infection. Common symptoms of rheumatic fever include fever, nose bleeds, and skin rash.
Physical Examination
Examination of patients with rheumatic fever is usually remarkable for fever, Sydenham’s chorea, cardiac murmurs, and erythema marginatum.
Laboratory Findings
Laboratory findings consistent with the diagnosis of rheumatic fever include elevated inflammatory markers, presence of streptococcal infection, and elevated or rising antistreptolysin O antibody titer.
Electrocardiogram
On electrocardiogram, rheumatic fever is characterized by PR interval prolongation, conduction abnormalities, arryhthmias or P mitrale depending on the structures involved and the extent of cardiac damage.
Chest X Ray
On chest x-ray, rheumatic fever is characterized by cardiomegaly and pulmonary edema secondary to heart failure.
Echocardiography
Echocardiography may be helpful in establishing the diagnosis of carditis and monitoring the progress of valve defects present in rheumatic fever.
Treatment
Medical Therapy
The mainstay of therapy for rheumatic fever includes antimicrobial therapy combined with anti-inflammatory medications. The drug of choice is penicillin but ampicillin and amoxicillin are equally as effective. Supportive therapy for rheumatic fever includes continuous use of low dose antibiotics (such as penicillin, sulfadiazine, or erythromycin) to prevent recurrence.
Primary Prevention
Effective measures for the primary prevention of rheumatic fever include reducing exposure to group A streptococci and antibiotic prophylaxis for streptococcal pharyngitis. Intramuscular benzathine penicillin G and oral penicillin V are the recommended antibiotics in treatment of group A streptococcal infection in absence of penicillin allergy.
Secondary Prevention
Secondary prevention strategies following rheumatic fever include antibiotic prophylaxis immediately after the antibiotic course in treatment of rheumatic fever. Duration of prophylactic treatment varies with degree of cardiac damage secondary to rheumatic fever.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Lance Christiansen, D.O.; Anthony Gallo, B.S. [2]
Overview
Rheumatic fever was first described by Hippocrates, a Greek physician, between 400-370 B.C.[1] The term “rheumatic fever” was first used post-Renaissance by Guillaume de Baillou, a French physician, in the early 1600s. T. Duckett Jones, MD was the first person to publish a set of diagnostic criteria in 1944.[2]
Historical Perspective
- Between 400-370 B.C., rheumatic fever was first described by Hippocrates, a Greek physician.[1]
- In the early 1600s, the term “rheumatic fever” was first used post-Renaissance by Guillaume de Baillou, a French physician.
- In the late 1600s, Thomas Sydenham described a case of severe rheumatic fever.
- In 1771, the term “rheumatic fever” first appeared with a description in Encyclopedia Britannica’s first edition.
- In the 1850s, the number of cases of rheumatic fever began to decline worldwide.
- In the 1900s, high-grade cases of rheumatic fever became less common in modernized parts of the world.[3]
- In World War II, conditions of over-crowding developed in military training sites and rheumatic fever became more common.
- In 1944, U.S. Naval leaders hired T. Duckett Jones, MD to study rheumatic fever’s epidemiology and clinical development. Dr. Jones devised certain a criteria for the diagnosis of rheumatic fever that is still in use today, albeit in a modified form.[4] The disease was not common in the United States, and usually occurs in isolated outbreaks.
- In the 1980s, the most recent outbreak of rheumatic fever occurred in the United States.
- In the present day, rheumatic fever is more common worldwide, especially in overcrowded areas.
References
- ↑ 1.0 1.1 Quinn RW (1991). “Did scarlet fever and rheumatic fever exist in Hippocrates’ time?”. Rev Infect Dis. 13 (6): 1243–4. PMID 1775859.
- ↑ THE DIAGNOSIS OF RHEUMATIC FEVER. JAMA (2015). http://jama.jamanetwork.com/article.aspx?articleid=271116 Accessed on October 9, 2015
- ↑ Bejiqi RA, Retkoceri R, Zeka N, Bejiqi H, Retkoceri A (2015). “Heart lesion after the first attack of the rheumatic Fever 22 years experience in single centre”. Med Arch. 69 (1): 49–53. doi:10.5455/medarh.2015.69.49-53. PMC 4384842. PMID 25870479.
- ↑ “Guidelines for the diagnosis of rheumatic fever. Jones Criteria, 1992 update. Special Writing Group of the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young of the American Heart Association”. JAMA. 268 (15): 2069–73. 1992. PMID 1404745.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Anthony Gallo, B.S. [2]
Overview
Based on the duration of symptoms, rheumatic fever may be classified into either acute or chronic. Acute rheumatic fever may be characterized by Group A beta-hemolytic streptococcal infection and cardiac lesions. Acute Rheumatic fever is diagnosed by JONES criteria. Chronic rheumatic fever may be characterized by cardiac valvular lesions and mitral stenosis.
Classification
Based on the duration of symptoms and the outcome of the disease, rheumatic fever may be classified into either acute or chronic.[1][2][3]
| Types | Characterestics |
|---|---|
| Acute rheumatic fever |
|
| Chronic rheumatic fever |
|
References
- ↑ Nasonova VA, Kuz’mina NN, Belov BS (2004). “[Present-day classification and nomenclature of rheumatic fever]”. Klin Med (Mosk). 82 (8): 61–6. PMID 15468729.
- ↑ Gewitz MH, Baltimore RS, Tani LY, Sable CA, Shulman ST, Carapetis J; et al. (2015). “Revision of the Jones Criteria for the diagnosis of acute rheumatic fever in the era of Doppler echocardiography: a scientific statement from the American Heart Association”. Circulation. 131 (20): 1806–18. doi:10.1161/CIR.0000000000000205. PMID 25908771.
- ↑ Shivakumarswamy U, Sinhasan SP, Purushotham R, Nagesha KR (2010). ““MacCallum Plaque of the Heart”: A Medicolegal Case”. Heart Views. 11 (2): 71–3. doi:10.4103/1995-705X.73220. PMC 3000917. PMID 21188002.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Lance Christiansen, D.O.; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Anthony Gallo, B.S. [3]
Overview
Rheumatic fever is the result of an autoimmunological sequela to a virulent Streptococcus pyogenes infection in a patient who was immunologically sensitized from prior infections. During a streptococcal infection, activated antigen-presenting cells, such as macrophages, present the bacterial antigen to helper T cells. Helper T cells subsequently activate B cells and induce the production of antibodies against the cell wall of Streptococcus. However the antibodies also act against the myocardium and joints, producing the symptoms of rheumatic fever.
Pathophysiology
Pathogenesis
- Rheumatic fever is the result of an autoimmunological sequelae to a virulent Streptococcus pyogenes infection in a patient who was immunologically sensitized from prior infections, affecting periarteriolar connective tissue.
- During a streptococcal infection, activated antigen-presenting cells, such as macrophages, present the bacterial antigen to helper T cells.
- Helper T cells subsequently activate B cells and induce the production of antibodies against the cell wall of Streptococcus.
- However the antibodies may also act against the myocardium and joints, producing the symptoms of rheumatic fever.
- Contrary to the immunological protection developed during most infections, infections by Streptococcus pyogenes cause both a protective immunological and pathological autoimmunological stimulation.
- Repeated infections by Streptococcus pyogenes will cause both a heightened protective and pathological immune response
Acute rheumatic fever
- Lesions may occur in endocardium, myocardium, or pericardium.
- The inflammation may cause serofibrinous pericardial exudates described as “bread-and-butter” pericarditis, which usually resolves without sequelae.
- Involvement of the endocardium typically results in fibrinoid necrosis and verrucae formation along the lines of closure of the heart valves.
- These warty projections and irregular thickenings are known as MacCallum plaques.[1]
Chronic rheumatic fever
- Lesions may occur in the mitral valve.
- Valve thickening may result in stenosis or regurgitation.
Gross
On gross pathology, the following are characteristic findings of rheumatic fever:[2]
- “Fish-mouth appearance”
- Slit-like morphology; elliptical cross-sectional flow area (mitral valve) with abnormally small semi-minor axis
- Significant valvular thickening
- Thickening and shortening of the chorda tympani
Microscopic histopathological analysis
On microscopic histopathological analysis, the following are characteristic findings of rheumatic fever:[2][3]
- Caterpillar cells
- Aschoff bodies found within the heart
- Jumbled, eosinophilic collagen
- Surrounded by T cells
Images
The following are gross and microscopic images associated with rheumatic fever:[4]
-
 Aortic stenosis (Tricuspid aorta): gross, an example of aortic stenosis due to rheumatic fever.
Aortic stenosis (Tricuspid aorta): gross, an example of aortic stenosis due to rheumatic fever. -
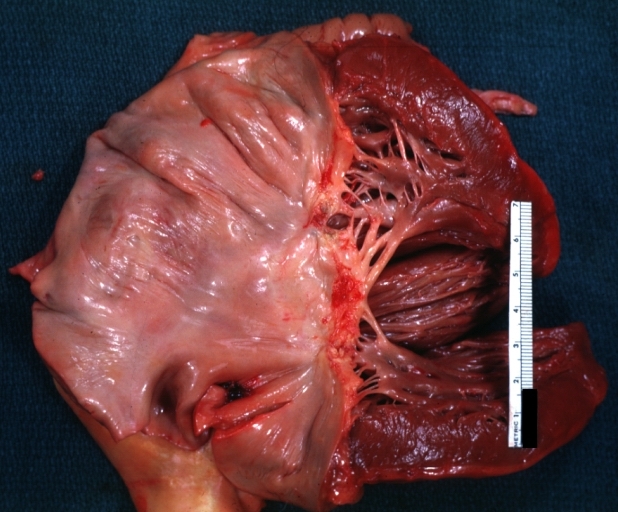
 Mitral scarring: gross, an example of mitral scarring due to rheumatic fever (healing phase of an infectious lesion).
Mitral scarring: gross, an example of mitral scarring due to rheumatic fever (healing phase of an infectious lesion). -
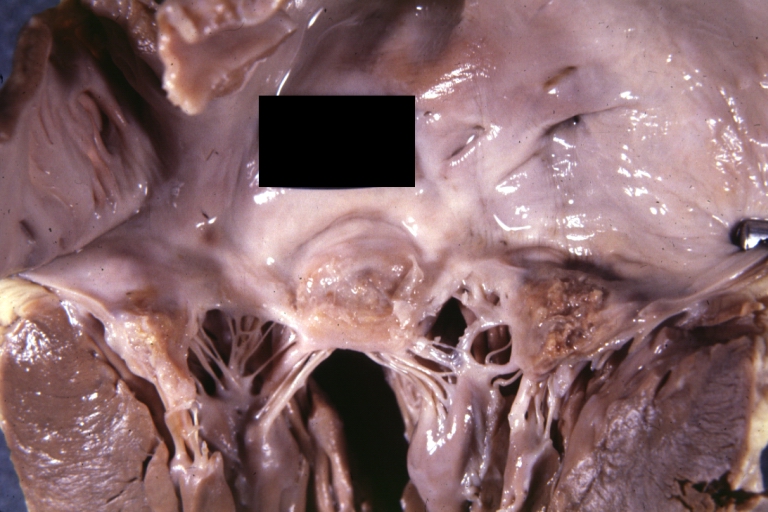
 Rheumatic mitral valvulitis: gross, an example of fibrosis, chorda thickening and shortening with thrombus around the large left atrium.
Rheumatic mitral valvulitis: gross, an example of fibrosis, chorda thickening and shortening with thrombus around the large left atrium. -
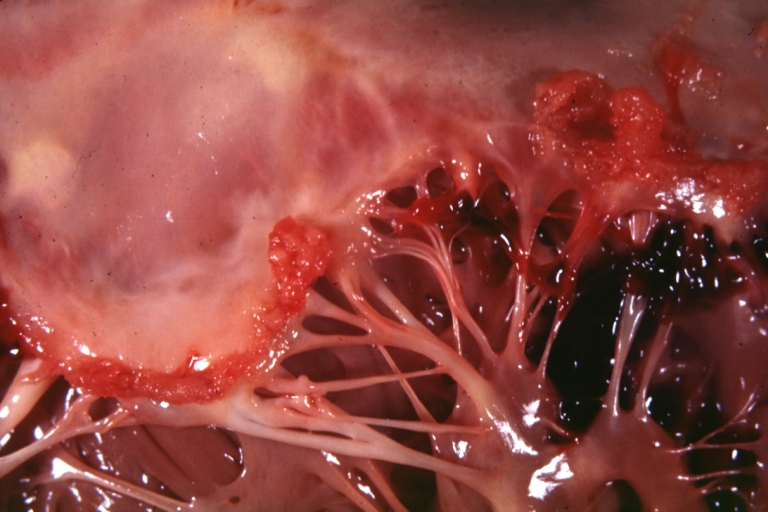
 Rheumatic mitral valvulitis: gross, an example of acute rheumatic fever lesion along line of closure of mitral valve.
Rheumatic mitral valvulitis: gross, an example of acute rheumatic fever lesion along line of closure of mitral valve. -
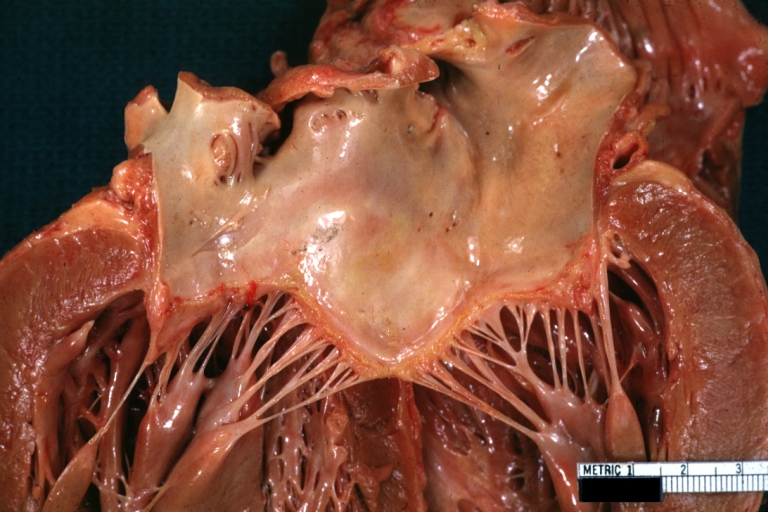
 Mitral valve: gross, acute rheumatic fever.
Mitral valve: gross, acute rheumatic fever. -
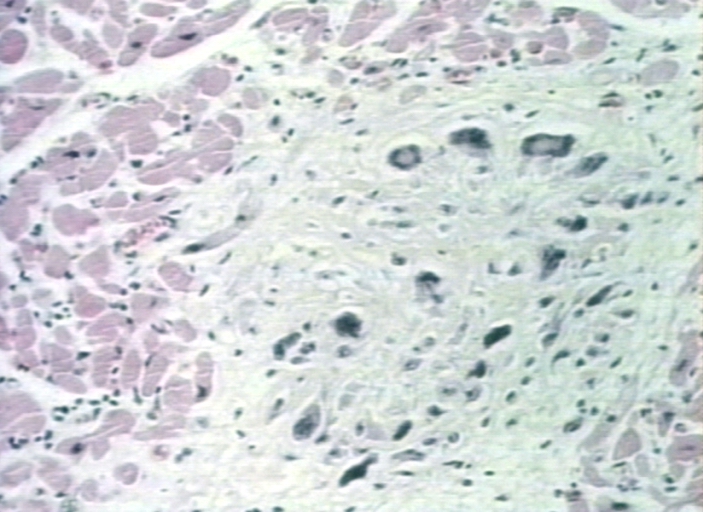 Aschoff bodies: microscopic histopathological analysis, Aschoff bodies in rheumatic heart disease.
Aschoff bodies: microscopic histopathological analysis, Aschoff bodies in rheumatic heart disease.






References
- ↑ Chopra P, Gulwani H (2007). “Pathology and pathogenesis of rheumatic heart disease”. Indian J Pathol Microbiol. 50 (4): 685–97. PMID 18306530.
- ↑ 2.0 2.1 Rheumatic Heart Disease. Libre Pathology (2015). http://librepathology.org/wiki/index.php/Heart_valves#Rheumatic_heart_disease Accessed on October 12, 2015
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease. St. Louis, MO: Elsevier Saunders. ISBN 0-7216-0187-1.
- ↑ Pathology Education Instructional Resource. University of Alabama at Birmingham (2014). Images courtesy of Propessor Peter Anderson DVM PhD and published with permission of PEIR, Department of Pathology, University of Alabama at Birmingham. http://www.peir.net Accessed on October 12, 2015.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Varun Kumar, M.B.B.S. [2]; Anthony Gallo, B.S. [3]
Overview
Rheumatic fever is usually caused by an infection with Group A beta-hemolytic Streptococcus pyogenes.
Causes for rheumatic fever
Common causes of rheumatic fever include:[1][2][3]
- Group A beta-hemolytic Streptococcus pyogenes pharyngitis
- Mistreated or untreated scarlet fever
- Antibody type II hypersensitivity reaction
References
- ↑ Coburn AF, Pauli RH (1932). “Studies on the relationship of streptococcus hemolyticus to the rheumatic process: III. Observations on the immunological responses of rheumatic subjects to hemolytic streptococcus”. J Exp Med. 56 (5): 651–76. PMC 2132197. PMID 19870091.
- ↑ Martin JM, Barbadora KA (2006). “Continued high caseload of rheumatic fever in western Pennsylvania: Possible rheumatogenic emm types of streptococcus pyogenes”. J Pediatr. 149 (1): 58–63. doi:10.1016/j.jpeds.2006.03.006. PMID 16860129.
- ↑ DIAMOND EF (1957). “Hereditary and environmental factors in the pathogenesis of rheumatic fever”. Pediatrics. 19 (5): 908–15. PMID 13431316.
Differentiating Rheumatic Fever from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: João André Alves Silva, M.D. [2]; Anthony Gallo, B.S. [3]
Overview
Rheumatic fever must be differentiated from other diseases that cause fever, skin rash, nausea and fatigue, such as typhoid fever, malaria, lassa fever, ebola, and scarlet fever.
Differentiating Rheumatic Fever from Other Diseases
Mitral stenosis must be differentiated from the following:[1][2][3][4][5][6][7][8][9][10][11][12][13][14][15][16][17][18][19][20][21][22][23]
| Diseases | History | Symptoms | Physical Examination | Murmur | Diagnosis | Other Findings | |||
|---|---|---|---|---|---|---|---|---|---|
| ECG | CXR | Echocardiogram | Cardiac Catheterization | ||||||
| Mitral Stenosis |
|
|
|
|
|
|
|
Right heart catheterization:
Left heart catheterization:
|
|
| Mitral Regurgitation |
|
|
Palpation
Auscultation
|
|
|
Acute MR
Chronic MR
|
|
|
|
| Atrial septal defect |
|
|
Inspection
Palpation
Auscultation
|
|
|
|
|
|
|
| Left Atrial Myxoma |
|
|
Skin
Auscultation:
|
|
|
Rare findings:
|
|
|
|
| Prosthetic Valve Obstruction |
|
|
Ausculation
Muffling of murmur |
|
|
Causes:
| |||
| Cor Triatriatum |
|
|
Auscultation
Other findings
|
|
Non specific but may have
|
|
|
|
Types
|
| Congenital Mitral Stenosis |
|
Infants:
Older patients:
|
Auscultation
Other findings
|
Mild-Moderate
Severe
|
|
|
|
Very rare condition | |
| Supravalvular Ring Mitral Stenosis |
|
|
Auscultation:
Lungs: Fine, crepitant rales and rhonchi or wheezes may be present Heart: Murmur |
|
|
Supramitral ring:
Intramitral ring:
(Difficult to visualize membrane <1mm in size) |
|
Types
It is attached between the opening of the atrial appendage and the mitral annulus which helps in differentiating with Cor triatriatum sinister.
| |
References
- ↑ Nassar PN, Hamdan RH (2011). “Cor Triatriatum Sinistrum: Classification and Imaging Modalities”. Eur J Cardiovasc Med. 1 (3): 84–87. doi:10.5083/ejcm.20424884.21. PMC 3286827. PMID 22379596.
- ↑ Roudaut R, Serri K, Lafitte S (2007). “Thrombosis of prosthetic heart valves: diagnosis and therapeutic considerations”. Heart. 93 (1): 137–42. doi:10.1136/hrt.2005.071183. PMC 1861363. PMID 17170355.
- ↑ Apostolakis EE, Baikoussis NG (2009). “Methods of estimation of mitral valve regurgitation for the cardiac surgeon”. J Cardiothorac Surg. 4: 34. doi:10.1186/1749-8090-4-34. PMC 2723095. PMID 19604402.
- ↑ Alboliras ET, Edwards WD, Driscoll DJ, Seward JB (1987). “Cor triatriatum dexter: two-dimensional echocardiographic diagnosis”. J Am Coll Cardiol. 9 (2): 334–7. PMID 3805524.
- ↑ Gibson DG, Honey M, Lennox SC (1974). “Cor triatriatum. Diagnosis by echocardiography”. Br Heart J. 36 (8): 835–8. PMC 458901. PMID 4412638.
- ↑ Cor triatrium https://radiopaedia.org/articles/cor-triatriatum (2016) Accessed on November 29, 2016
- ↑ Sosland RP, Vacek JL, Gorton ME (2007). “Congenital mitral stenosis: a rare presentation and novel approach to management”. J Thorac Cardiovasc Surg. 133 (2): 572–3. doi:10.1016/j.jtcvs.2006.10.025. PMID 17258606.
- ↑ Driscoll DJ, Gutgesell HP, McNamara DG (1978). “Echocardiographic features of congenital mitral stenosis”. Am J Cardiol. 42 (2): 259–66. PMID 685838.
- ↑ Bonou M, Lampropoulos K, Barbetseas J (2012). “Prosthetic heart valve obstruction: thrombolysis or surgical treatment?”. Eur Heart J Acute Cardiovasc Care. 1 (2): 122–7. doi:10.1177/2048872612451169. PMC 3760527. PMID 24062899.
- ↑ Maganti K, Rigolin VH, Sarano ME, Bonow RO (2010). “Valvular heart disease: diagnosis and management”. Mayo Clin Proc. 85 (5): 483–500. doi:10.4065/mcp.2009.0706. PMC 2861980. PMID 20435842.
- ↑ DEXTER L (1956). “Atrial septal defect”. Br Heart J. 18 (2): 209–25. PMC 479579. PMID 13315850.
- ↑ Webb G, Gatzoulis MA (2006). “Atrial septal defects in the adult: recent progress and overview”. Circulation. 114 (15): 1645–53. doi:10.1161/CIRCULATIONAHA.105.592055. PMID 17030704.
- ↑ Geva T, Martins JD, Wald RM (2014). “Atrial septal defects”. Lancet. 383 (9932): 1921–32. doi:10.1016/S0140-6736(13)62145-5. PMID 24725467.
- ↑ Demir M, Akpinar O, Acarturk E (2005). “Atrial myxoma: an unusual cause of myocardial infarction”. Tex Heart Inst J. 32 (3): 445–7. PMC 1336732. PMID 16392241.
- ↑ MacGowan SW, Sidhu P, Aherne T, Luke D, Wood AE, Neligan MC; et al. (1993). “Atrial myxoma: national incidence, diagnosis and surgical management”. Ir J Med Sci. 162 (6): 223–6. PMID 8407260.
- ↑ Circulation http://circ.ahajournals.org/content/119/7/1034 (2016) Accessed on December 7, 2016
- ↑ Alphonso N, Nørgaard MA, Newcomb A, d’Udekem Y, Brizard CP, Cochrane A (2005). “Cor triatriatum: presentation, diagnosis and long-term surgical results”. Ann Thorac Surg. 80 (5): 1666–71. doi:10.1016/j.athoracsur.2005.04.055. PMID 16242436.
- ↑ circulation http://circ.ahajournals.org/content/36/1/101 (1967) Accessed on 7 December, 2016
- ↑ Moore P, Adatia I, Spevak PJ, Keane JF, Perry SB, Castaneda AR; et al. (1994). “Severe congenital mitral stenosis in infants”. Circulation. 89 (5): 2099–106. PMID 8181134.
- ↑ Uva MS, Galletti L, Gayet FL, Piot D, Serraf A, Bruniaux J; et al. (1995). “Surgery for congenital mitral valve disease in the first year of life”. J Thorac Cardiovasc Surg. 109 (1): 164–74, discussion 174-6. doi:10.1016/S0022-5223(95)70432-9. PMID 7815793.
- ↑ Banerjee A, Kohl T, Silverman NH (1995). “Echocardiographic evaluation of congenital mitral valve anomalies in children”. Am J Cardiol. 76 (17): 1284–91. PMID 7503011.
- ↑ Sullivan ID, Robinson PJ, de Leval M, Graham TP (1986). “Membranous supravalvular mitral stenosis: a treatable form of congenital heart disease”. J Am Coll Cardiol. 8 (1): 159–64. PMID 3711511.
- ↑ Subramaniam V, Herle A, Mohammed N, Thahir M (2011). “Ortner’s syndrome: case series and literature review”. Braz J Otorhinolaryngol. 77 (5): 559–62. PMID 22030961.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Lance Christiansen, D.O.; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Varun Kumar, M.B.B.S. [3]; Anthony Gallo, B.S. [4]
Overview
The incidence of rheumatic fever among developed countries such as the USA and Canada was approximately 20-40 per 100,000 individuals between 1970-1990 with rheumatic heart disease occurring sporadically. Over past two decades, the prevalence of rheumatic fever has decreased to 5-20 per 100,000 individuals in Canada and <5 per 100,000 individuals in the USA with no new cases of rheumatic heart disease.
Epidemiology and Demographics
Prevalence
Between 1990 and the present, the prevalence of rheumatic fever has decreased to 5-20 per 100,000 individuals in Canada and <5 per 100,000 individuals in the USA with no new cases of rheumatic heart disease.[1] More information regarding prevalence of rheumatic fever can be found here.
Incidence
Between 1970-1990, the incidence of rheumatic fever among developed countries such as the USA and Canada was approximately 20-40 per 100,000 individuals between 1970-1990 with rheumatic heart disease occurring sporadically. More information regarding incidence of rheumatic fever can be found here.
Age
Rheumatic fever tends to affect a younger age group, generally between the ages of 5-15.[2] Group A beta-hemolytic streptococcus pharyngitis is uncommon in children less than 3 years of age, and rheumatic fever is extremely rare. Rheumatic fever among adults is less frequent and accounts for approximately 20% of cases.
Gender
No predilection towards either gender exists. However, certain manifestations of rheumatic fever such as mitral valve prolapse, carditis, and Sydenham chorea are commonly often observed among females than males.[3]
Developed Countries
The incidence of rheumatic fever among developed countries such as the USA and Canada was approximately 20-40 per 100,000 individuals during the period 1970-1990 with rheumatic heart disease occurring sporadically. Over past two decades, the prevalence of rheumatic fever has decreased to 5-20 per 100,000 individuals in Canada and <5/100,000 individuals in the USA with no new cases of rheumatic heart disease.[1] The incidence of rheumatic fever among developed nations is low, likely due to improved hygienic standards and routine use of antibiotics for acute pharyngitis.[4]
Developing Countries
The rates of rheumatic fever and rheumatic heart diseases among developing nations have mixed trends. Recently, the incidence rate of rheumatic fever has decreased in India, China, and African countries, which has been mainly attributed to improved access to medical treatment. This has led to improved survival rates even among individuals with rheumatic heart disease. As a result, an increase in prevalence rate has been observed.[1] Newer studies relying on echocardiography in the diagnosis of rheumatic heart disease have demonstrated that rates of subclinical carditis are up to 10x higher than that diagnosed by clinical examination.[5][6][7][8] India, Pakistan, Russia, and African countries have higher prevalence rates of rheumatic heart disease. It is estimated that approximately there are 62-78 million rheumatic heart disease patients worldwide, which could potentially result in 1.4 million deaths per year.[9][10] Occurrence of rheumatic fever is associated with low socioeconomic and over crowded conditions.
References
- ↑ 1.0 1.1 1.2 Seckeler MD, Hoke TR (2011). “The worldwide epidemiology of acute rheumatic fever and rheumatic heart disease”. Clin Epidemiol. 3: 67–84. doi:10.2147/CLEP.S12977. PMC 3046187. PMID 21386976.
- ↑ Grover A, Dhawan A, Iyengar SD, Anand IS, Wahi PL, Ganguly NK (1993). “Epidemiology of rheumatic fever and rheumatic heart disease in a rural community in northern India”. Bull World Health Organ. 71 (1): 59–66. PMC 2393425. PMID 8440039.
- ↑ Bisno AL. Rheumatic fever. In: Goldman L, Ausiello D, eds. Cecil Medicine. 23rd ed. Philadelphia, Pa: Saunders Elsevier; 2007:chap 313
- ↑ Miyake CY, Gauvreau K, Tani LY, Sundel RP, Newburger JW (2007). “Characteristics of children discharged from hospitals in the United States in 2000 with the diagnosis of acute rheumatic fever”. Pediatrics. 120 (3): 503–8. doi:10.1542/peds.2006-3606. PMID 17766522.
- ↑ Marijon E, Ou P, Celermajer DS, Ferreira B, Mocumbi AO, Jani D; et al. (2007). “Prevalence of rheumatic heart disease detected by echocardiographic screening”. N Engl J Med. 357 (5): 470–6. doi:10.1056/NEJMoa065085. PMID 17671255.
- ↑ Bhaya M, Panwar S, Beniwal R, Panwar RB (2010). “High prevalence of rheumatic heart disease detected by echocardiography in school children”. Echocardiography. 27 (4): 448–53. doi:10.1111/j.1540-8175.2009.01055.x. PMID 20345448.
- ↑ Sadiq M, Islam K, Abid R, Latif F, Rehman AU, Waheed A; et al. (2009). “Prevalence of rheumatic heart disease in school children of urban Lahore”. Heart. 95 (5): 353–7. doi:10.1136/hrt.2008.143982. PMID 18952636.
- ↑ Carapetis JR, Hardy M, Fakakovikaetau T, Taib R, Wilkinson L, Penny DJ; et al. (2008). “Evaluation of a screening protocol using auscultation and portable echocardiography to detect asymptomatic rheumatic heart disease in Tongan schoolchildren”. Nat Clin Pract Cardiovasc Med. 5 (7): 411–7. doi:10.1038/ncpcardio1185. PMID 18398402.
- ↑ Paar JA, Berrios NM, Rose JD, Cáceres M, Peña R, Pérez W; et al. (2010). “Prevalence of rheumatic heart disease in children and young adults in Nicaragua”. Am J Cardiol. 105 (12): 1809–14. doi:10.1016/j.amjcard.2010.01.364. PMC 2895982. PMID 20538135.
- ↑ Carapetis JR, Steer AC, Mulholland EK, Weber M (2005). “The global burden of group A streptococcal diseases”. Lancet Infect Dis. 5 (11): 685–94. doi:10.1016/S1473-3099(05)70267-X. PMID 16253886.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Varun Kumar, M.B.B.S. [2]; Anthony Gallo, B.S. [3]
Overview
Common risk factors in the development of rheumatic fever include poor sanitation, low socioeconomic status, and family history.
Risk Factors
Common risk factors in the development of rheumatic fever include:[1][2][3]
- Poor sanitation
- Low socioeconomic status
- Positive family history
- Inadequate healthcare
- Dampness at home
- Overcrowding
- Malnutrition
- Traveling to endemic regions, such as developing countries
References
- ↑ Vlajinac H, Adanja B, Marinković J, Jarebinski M (1991). “Influence of socio-economic and other factors on rheumatic fever occurrence”. Eur J Epidemiol. 7 (6): 702–4. PMID 1783067.
- ↑ DIAMOND EF (1957). “Hereditary and environmental factors in the pathogenesis of rheumatic fever”. Pediatrics. 19 (5): 908–15. PMID 13431316.
- ↑ Martin JM, Barbadora KA (2006). “Continued high caseload of rheumatic fever in western Pennsylvania: Possible rheumatogenic emm types of streptococcus pyogenes”. J Pediatr. 149 (1): 58–63. doi:10.1016/j.jpeds.2006.03.006. PMID 16860129.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Varun Kumar, M.B.B.S. [2]; Anthony Gallo, B.S. [3]
Overview
Screening of rheumatic fever is important as many cases of rheumatic heart disease are subclinical. Echocardiography among inhabitants of high risk regions is recommended. If any abnormality is detected on echocardiography, further cardiac evaluation is performed followed by antimicrobial therapy.
Screening
- According to the World Health Organization, screening for rheumatic fever by echocardiogram is recommended among patients with from high risk communities with abnormal auscultatory findings. Early detection of subclinical disease process helps in early treatment and improves prognosis by preventing recurrence.[1] Screening is performed to prevent significant valvular disease.[2]
- Screening of rheumatic heart disease involves:
- Eliciting history of rheumatic fever
- Cardiac auscultation for murmurs
- Echocardiography
References
- ↑ Marijon E, Ou P, Celermajer DS, Ferreira B, Mocumbi AO, Sidi D; et al. (2008). “Echocardiographic screening for rheumatic heart disease”. Bull World Health Organ. 86 (2): 84. PMC 2647380. PMID 18297157.
- ↑ Meira ZM, Goulart EM, Colosimo EA, Mota CC (2005). “Long term follow up of rheumatic fever and predictors of severe rheumatic valvar disease in Brazilian children and adolescents”. Heart. 91 (8): 1019–22. doi:10.1136/hrt.2004.042762. PMC 1769032. PMID 16020588.
Natural History, Complications, and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Lance Christiansen, D.O.; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Varun Kumar, M.B.B.S. [3]; Anthony Gallo, B.S. [4]
Overview
If left untreated, patients with rheumatic fever may progress to develop arrhythmias, systemic emboli, and endocarditis, which may lead to cardiac failure. Common complications of rheumatic fever include mitral/aortic valve stenosis, carditis, and stroke. Prognosis is generally poor if left untreated.
Natural History, Complications, and Prognosis
Natural History
If left untreated, rheumatic fever may cause valvular diseases including stenosis, regurgitation of mitral/aortic valves and myocarditis. This may lead to decreased cardiac output, pulmonary edema, and ultimately cardiac failure. If an individual develops rheumatic fever, they will develop an increased sensitization to Streptococcus pyogenes autoantigens. Future infection will likely cause an elevated, autoimmunological response and a more severe case of rheumatic fever will develop.
It is estimated that the recurrence rate of rheumatic fever is decreased by about 85% by providing prophylactic penicillin therapy. Recurrence rate of 0.2/patient/year follow-up was noted among those not receiving regular treatment.[1]
Complications
Complications to rheumatic fever include:[1][2][3]
- Mitral stenosis
- Aortic stenosis
- Endocarditis
- Myocarditis
- Pericarditis
- Cardiac failure
- Arrhythmias
- Systemic emboli
- Stroke
- Recurrence of rheumatic fever
Prognosis
For cases without carditis, the prognosis is excellent, demonstrating no residual heart disease. In cases with preexisting or developing heart disease, the prognosis is poor, leading to mortality.[4]
References
- ↑ 1.0 1.1 Majeed HA, Yousof AM, Khuffash FA, Yusuf AR, Farwana S, Khan N (1986). “The natural history of acute rheumatic fever in Kuwait: a prospective six year follow-up report”. J Chronic Dis. 39 (5): 361–9. PMID 3700577.
- ↑ Garg N, Kandpal B, Garg N, Tewari S, Kapoor A, Goel P; et al. (2005). “Characteristics of infective endocarditis in a developing country-clinical profile and outcome in 192 Indian patients, 1992-2001”. Int J Cardiol. 98 (2): 253–60. doi:10.1016/j.ijcard.2003.10.043. PMID 15686775.
- ↑ Carapetis JR, Steer AC, Mulholland EK, Weber M (2005). “The global burden of group A streptococcal diseases”. Lancet Infect Dis. 5 (11): 685–94. doi:10.1016/S1473-3099(05)70267-X. PMID 16253886.
- ↑ The Natural History of Rheumatic Fever and Rheumatic Heart Disease, Rheumatic Fever Working Party of the Medical Research Council of Great Britain and the American Heart Association (1965). http://circ.ahajournals.org/content/32/3/457 Accessed on October 12, 2015
Diagnosis
Diagnosis
Jones Criteria | History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | Echocardiography
Case Studies
Case Studies
Template:Bacterial diseases Template:Hypersensitivity and autoimmune diseases
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH