
Pericarditis
For patient information, click here.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Homa Najafi, M.D.[2]Varun Kumar, M.B.B.S.; Cafer Zorkun, M.D., Ph.D. [3]
Synonyms and keywords:acute pericarditis, chronic pericarditis, idiopathic pericarditis, recurrent pericarditis, chronic effusive pericarditis, chronic constrictive pericarditis, inflammation of the pericardium, pericardial inflammation, inflammation of the pericardial sac, serous pericarditis, purulent pericarditis, hemorrhagic pericarditis, fibrinous pericarditis, caseous pericarditis, bacterial pericarditis, viral pericarditis, fungal pericarditis, parasitic pericarditis, autoimmune pericarditis, neoplastic pericarditis, metabolic pericarditis, traumatic pericarditis, iatrogenic pericarditis, drug-related pericarditis, postoperative pericarditis, post-operative pericarditis, post-surgery pericarditis, postsurgery pericarditis, acute recurrent pericarditis, radiation induced pericarditis, radiation-induced pericarditis, uremic pericarditis, radiation induced constrictive pericarditis, children pericarditis, pericarditis in children
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Homa Najafi, M.D.[2]
Overview
Pericarditis is a condition in which the sac-like covering surrounding the heart (the pericardium) becomes inflamed. Symptoms of pericarditis include chest pain which increases with deep breathing and lying flat.
Historical Perspective
The pericardium is a double-walled sac that contains the heart and the roots of the great vessels. Morphologically, it is a conical-shaped, double-walled fibro-serous membrane. It rests posteriorly to the sternum at the level of second to sixth costal cartilages and T5-T8 vertebrae.
Classification
Pericarditis may be classified according to duration of the disease and recurrence into acute, Incessant, recurrent and chronic. Moreover, pericarditis can be classified based on the etiology in two groups of infectious and non-infectious causes.
Pathophysiology
Pericarditis is inflammation of the pericardium, which is the double-walled sac that contains the heart and the roots of the great vessels. There can be an accompanying accumulation of fluid that can be either serous (free flowing fluid) or fibrinous (an exudate, which is a thick fluid composed of proteins, fibrin strands, inflammatory cells, cell breakdown products, and sometimes bacteria). Vascular congestion of the pericardium is also present. The underlying myocardium may or may not be inflamed as well. If the myocardium is involved in the inflammatory process, it is called myopericarditis, and CK and troponin levels may be elevated. Cardiotropic viruses usually spread to the myocardium and pericardium hematogenously and cause acute inflammation with infiltration of polymorphonuclear (PMN) leukocytes and pericardial vascularization. Most patients with viral pericarditis recover completely with few developing recurrences. Some patients develop constrictive pericarditis which could be disabling. Bacterial pericarditis results from contiguous spread of infection within the chest, either de novo or after surgery or trauma, spread from infective endocarditis, hematogenous, or direct inoculation as a result of penetrating injury or cardiothoracic surgery.
Causes
The causes of pericarditis can be divided into infectious and non-infectious ones. Infectious causes include bacterial, viral, fungal and, parasitic. While, non-infectious causes include autoimmune, neoplastic, metabolic, traumatic and iatrogenic, and drug-related. Acute myocardial infarction, Addisonian crisis, aortic dissection and rupture, blunt or penetrating chest trauma, esophageal perforation, gastric perforation, and myocardial rupture are life threatening causes of pericarditis. Common causes of pericarditis include viral, bacterial organisms, neoplasms, autoimmune and renal failure.
Differentiating Pericarditis from other Diseases
Pericarditis must be differentiated from diseases presenting with chest pain, shortness of breath and tachypnea which include myocardial infarction, pulmonary embolism, congestive heart failure, pneumonia, vasculitis, and chronic obstructive pulmonary disease (COPD). Manifestation of the pericarditis can help in differentiation from myocardial infarction. Moreover, other differential diagnosis include aortic stenosis, coronary artery vasospasm, esophageal rupture, esophageal spasm, esophagitis,acute gastritis, gastroesophageal reflux disease, and peptic ulcer disease should be considered.
Epidemiology and Demographics
The incidence of acute pericarditis is approximately 27.7 per 100,000 individuals annually. The recurrence of disease is seen in almost 30% of patients after first episode. The mortality rate of acute pericarditis is approximately 1.1% in developed countries. Patients of all age groups may develop acute pericarditis. Although it commonly affects men in 20 to 50 years of age. Pericarditis in developed countries is most commonly due to malignancy or viral infection. It usually follows respiratory infections, most commonly echovirus or coxsackie virus. In children, it is most commonly caused by adenovirus or coxsackie virus. In developing countries pericarditis is usually secondary to tuberculosis or HIV infection. Tuberculous pericarditis, caused by Mycobacterium tuberculosis, is found in approximately 1% of all autopsied cases of TB and in 1% to 2% of instances of pulmonary TB.
Risk Factors
Screening
There is insufficient evidence to recommend routine screening for pericarditis.
Natural History, Complications and Prognosis
Pericarditis is often self-limited and most people recover in 2 weeks to 3 months. However, the condition can be complicated by significant fluid buildup around the heart (a pericardial effusion or cardiac tamponade) and may require urgent intervention including pericardiocentesis. If scarring of the sac around the heart (the pericardium) occurs, then this is called constrictive pericarditis which may require surgical stripping of the scar.
Diagnosis
Diagnostic Study of Choice
History and Symptoms
Patients with pericarditis commonly present with chest pain that changes with position, cough, fever, breathlessness, and fatigue are the other common symptoms. Less common symptoms include palpitations, hiccup, odynophagia, faint, dizziness, and abdominal pain which is seen mostly in children.
Physical Examination
A careful physical examination must be performed to exclude the presence of cardiac tamponade, a dangerous complication of pericarditis. If cardiac tamponade is present, then pulsus paradoxus, hypotension, an elevated jugular venous pressure and peripheral edema may be present.
Laboratory Findings
Non-specific markers of inflammation are generally elevated in pericarditis. These include the leukocyte count, C-reactive protein, and ESR. The cardiac troponin is elevated if there is an injury to the underlying myocardium, a condition termed as myopericarditis. Diagnostic pericardiocentesis and biopsy help in identifying an underlying infectious or malignant process.Non-specific markers of inflammation are generally elevated in pericarditis. These include the leukocyte count, C-reactive protein, and ESR. The cardiac troponin is elevated if there is an injury to the underlying myocardium, a condition termed as myopericarditis. Diagnostic pericardiocentesis and biopsy help in identifying an underlying infectious or malignant process.
Electrocardiogram
In the presence of a large effusion or tamponade, there may be diminished voltage and electrical alternans (alternation of QRS complex amplitude or axis between beats).
X-ray
A flask-shaped, enlarged cardiac silhouette will be observed on chest x-ray in pericarditis complicated with pericardial effusion or tamponade. A mass may also be seen when malignancy is the cause. Calcification of pericardium may be noted in constrictive pericarditis.
Echocardiography and Ultrasound
Echocardiography is generally performed to assess for the presence of a pericardial effusion and to assess and monitor its size. Echocardiography is critical in confirming the clinical suspicion cardiac tamponade.
CT scan
On CT, pericardial fluid adds to the thickness of pericardium as both have the similar signal intensities. In pericarditis, pericardium can generate an intermediate signal intensity and may enhance after gadolinium administration. In pericardial effusion, hemorrhagic effusions can be differentiated from a transudate or an exudate based on signal characteristics (high signal on T1-weighted images) or density (high-density clot on CT). CT is superior to MRI in the visualization of pericardial calcification which is often seen in the patient with pericardial constriction. CT imaging also helps in detecting the presence of tumors and the extent of metastasis of the neoplasm.
MRI
On MRI, normal pericardium appears as a thin dark band that is bordered by a bright band on both sides on T1 weighted spin imaging. These surrounding bright bands are associated with the surrounding epicardial and pericardial fat. Following the administration of gadolinium, pericardium may appear thick and inflamed in the setting of pericarditis. Lower intensity signal is observed in constrictive pericarditis than in acute pericarditis. Comprehensive visualization of the LV endocardium and the physiologic consequences of abnormal pericardial thickening can also be obtained without exposure to ionizing radiation.
Other Imaging Findings
Other diagnostic studies
Echocardiography guided pericardiocentesis may be helpful in the diagnosis of the pericarditis etiology. Pericardial fluid aspiration for cytology and immunohistochemistry analysis should be done in pericarditis with effusion. Pericardiocentesis should be done in patients with high susceptibility of neoplastic pericarditis which cytology analysis for malignancy was negative.
Treatment
Medical Therapy
The management of pericarditis depends on whether the patient has an uncomplicated vs. complicated disease course. Uncomplicated pericarditis is generally treated with non-steroidal anti-inflammatory drugs, such as Ibuprofen in cases of either viral or idiopathic pericarditis, and Aspirin in cases of post-MI pericarditis. Pericarditis complicated with either effusion or cardiac tamponade is generally treated with urgent pericardiocentesis in the case of cardiac tamponade, antibiotics in the case of purulent pericardial effusion, and either steroids or colchicine among patients with recurrent or refractory disease.
Interventions
Surgery
Pericardiocentesis
Percutaneous pericardiocentesis is a procedure where fluid is aspirated from the pericardium (the sac enveloping the heart) using a needle via a percutaneous approach. Pericardiocentesis can provide a diagnostic sampling of pericardial fluid and can be used as a therapeutic maneuver to evacuate pericardial fluid and lower the pericardial pressure.
Pericardial Window
Creation of a pericardial window is a cardiac surgical procedure in which an opening is made in the pericardium to drain fluid that has accumulated around the heart by creating a fistula or “window” from the pericardial space to the peritoneal cavity. Flow of fluid into the peritoneal cavity prevents the accumulation of fluid around the heart (a pericardial effusion), which might cause compression and impaired filling of the heart (cardiac tamponade), a dangerous complication. The procedure is performed for both diagnostic and therapeutic purposes. The creation of a pericardial window is usually performed by a cardiac surgeon or thoracic surgeon who makes an incision, commonly sub-xiphoid, and cuts a small hole in the pericardium. This surgery is performed with local anesthesia. An incision is made either below the sternum, or alternately between the ribs of the left chest. The resection can be with scissors, cautery, a stapling device, or a harmonic scalpel, with no one technique demonstrably better than another. It is best to have a combination of techniques available to resect the pericardium adequately. The surgeon may place a catheter in the pericardial window so that fluid can continue to drain for a short period of time after the surgery. Chest tubes are removed in 2-3 days once the drainage is less than 200cc/24hrs.
Pericardial Stripping
Pericardiectomy is the surgical removal of part or most of the pericardium. This operation is performed to relieve constrictive pericarditis or to remove a pericardium that is calcified and fibrous. Constrictive pericarditis is a progressive disease without spontaneous reversal of pericardial thickening. Some patients can be medically managed for several years. Edema can be controlled with diuretics and slowing the heart rate can maximize the diastolic filling time. Many patients eventually develop significant debility from impaired cardiac output and elevated right and left sided filling pressures. The definitive treatment for constrictive pericarditis is pericardiectomy which is also known as pericardial stripping. This is a surgical procedure where the entire pericardium is peeled away from the heart. Due to the significant risks involved with pericardial stripping, many patients are treated medically, with judicious use of diuretics.
Primary Prevention
Secondary Prevention
References
Pericardial Anatomy
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Assistant Editor(s)-in-Chief: Rim Halaby
Overview
The pericardium is a double-walled sac that contains the heart and the roots of the great vessels. Morphologically, it is a conical-shaped, double-walled fibro-serous membrane. It rests posteriorly to the sternum at the level of second to sixth costal cartilages and T5-T8 vertebrae.
Layers
- The pericardium is made up of two layers:
- Fibrous pericardium
- Serous pericardium
- Smooth internal layer made up of 2 components:
- Parietal: reflects onto fibrous pericardium
- Visceral: reflects onto heart and great vessels and forms the epicardium, the external layer of the heart wall
- Smooth internal layer made up of 2 components:
- Pericardial cavity: Potential space between parietal and visceral layers. It contains a serous fluid film that occupies the cavity and functions as lubricant against friction by all chest movements.[1][2][3]
Pericardial Sinuses
- There are two small chambers or sinuses located where the visceral and parietal pericardia are continuous with one another within the pericardial cavity.
- Transverse sinus:
- Located posterior to the pulmonary trunk and ascending aorta at the level between the superior vena cava and aortic arch
- Formed after dorsal mesocardium rupture embryonically
- Functional role is to allow the unhindered expansion of great arteries posteriorly during cardiac systole
- Utilized surgically to pass surgical clamps or place ligatures around great arteries.
- Oblique sinus:
- A blind recess (cul-de-sac) posterior to the left atrium between superior vena cava, right and left pulmonary veins inferior to the transverse sinus
- Formed embryonically by the incorporation of the pulmonary vein tributaries into the left atrium
- Functional role believed to be the expansion of the left atrium upon normal collapse of the thorax[4][5][6]


Diseases of the Pericardium
- Pericarditis is an inflammatory condition of the pericardium.
- Pericardial effusion is fluid accumulation in the pericardial sac.
- Constrictive pericarditis occurs when there is a scar encasing, the heart that chronically constricts the filling of the heart.
- Cardiac tamponade is a medical emergency in which fluid in the pericardial sac acutely restricts the filling of the heart. This requires surgical drainage or pericardiocentesis.
Additional Images
-
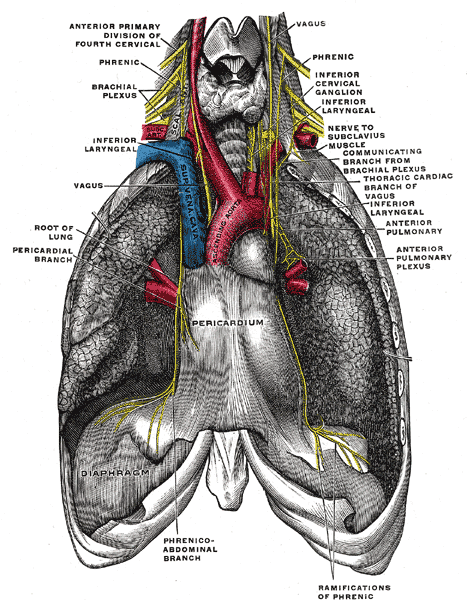 The phrenic nerve and its relations with the vagus nerve.
The phrenic nerve and its relations with the vagus nerve. -
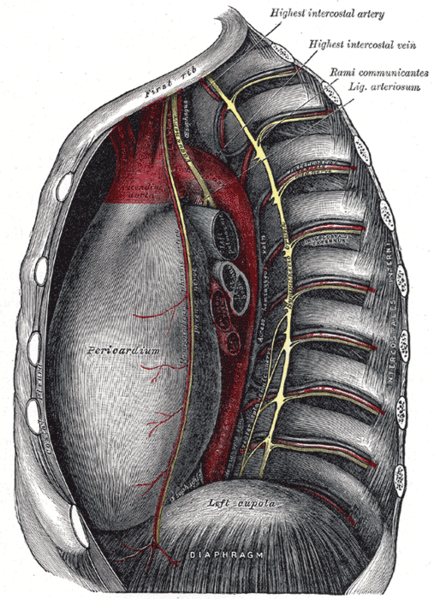 Thoracic portion of the sympathetic trunk.
Thoracic portion of the sympathetic trunk. -
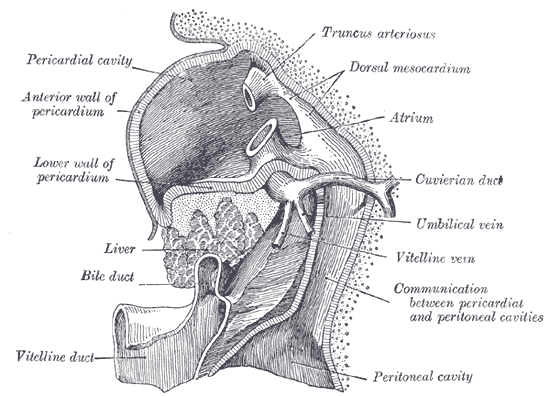 Liver with the septum transversum. Human embryo 3 mm long.
Liver with the septum transversum. Human embryo 3 mm long. -
 The thymus of a full-time fetus, exposed in situ.
The thymus of a full-time fetus, exposed in situ.




References
- ↑ Kishore, K. (2003). The Heart of Structural Development: The Functional Basis of the Location and Morphology of the Human Vascular Pump. J Postgrad Med, 49:282-4.
- ↑ Moore, K. L., Agur, A. M., & Dalley, A. F. (2011). Essential Clinical Anatomy – Fourth Edition. Lippincott Williams & Wilkins.
- ↑ Tank, P. W. (2009). Grant’s Dissector – Fourteenth Edition. Lippincott Williams & Wilkins.
- ↑ Kishore, K. (2003). The Heart of Structural Development: The Functional Basis of the Location and Morphology of the Human Vascular Pump. J Postgrad Med, 49:282-4.
- ↑ Moore, K. L., Agur, A. M., & Dalley, A. F. (2011). Essential Clinical Anatomy – Fourth Edition. Lippincott Williams & Wilkins.
- ↑ Tank, P. W. (2009). Grant’s Dissector – Fourteenth Edition. Lippincott Williams & Wilkins.
de:Herzbeutel it:Pericardio la:Pericardium ms:Perikardium nl:Pericard nn:Hjartepose fi:Perikardium
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Homa Najafi, M.D.[2]
Overview
Pericarditis may be classified according to duration of the disease and recurrence into acute, Incessant, recurrent and chronic. Moreover, pericarditis can be classified based on the etiology in two groups of infectious and non-infectious causes.
Classification
- Pericarditis may be classified according to duration of the disease and recurrence into four groups:[1][2][3][4]
| Pericarditis classification based on duration | |||||||||||||||||||||||||||||||||||||||||||||||||
| Acute: New-onset disease which lasts < 4-6 weeks | Incessant: Pericarditis lasting for >4–6 weeks but <3 months without remission | Recurrent: Recurrence after the first episode of acute pericarditis 4–6 weeks or longer interval | Chronic: Pericarditis lasts for >3 months | ||||||||||||||||||||||||||||||||||||||||||||||
- Moreover, pericarditis can be classified based on the etiology in two groups:[1][2][3][5]
- Infectious:
- Non-infectious:
- Autoimmune
- Neoplastic
- Metabolic
- Traumatic and iatrogenic
- Drug-related
| Pericarditis classification based on etiology | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Infectious causes | Non-infectious causes | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Viral:
Enteroviruses(coxsackieviruses, echoviruses) Herpes viruses(EBV, CMV, HHV-6) Adenoviruses Parvovirus B19 | Bacterial:
Mycobacterium tuberculosis Coxiella burnetii Borrelia burgdorferi | Fungal:
Histoplasma species Aspergillus species Blastomyces species Candida species | Parasitic:
Echinococcus species Toxoplasma species | Autoimmune:
Systemic autoimmune and auto-inflammatory diseases Systemic vasculitides Sarcoidosis Familial Mediterranean fever IBD Still disease | Neoplastic:
Primary tumours (pericardial mesothelioma) secondary metastatic tumors( lung and breast cancer, lymphoma) | Metabolic:
Uraemia Myxoedema Anorexia nervosa | Traumatic and Iatrogenic | Drug-related | Others:
Amyloidosis Aortic dissection Pulmonary arterial Hypertension Chronic heart failure Congenital absence of the pericardium | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
References
- ↑ 1.0 1.1 Imazio, Massimo (2012). “Contemporary management of pericardial diseases”. Current Opinion in Cardiology. 27 (3): 308–317. doi:10.1097/HCO.0b013e3283524fbe. ISSN 0268-4705.
- ↑ 2.0 2.1 Imazio, Massimo; Spodick, David H.; Brucato, Antonio; Trinchero, Rita; Adler, Yehuda (2010). “Controversial Issues in the Management of Pericardial Diseases”. Circulation. 121 (7): 916–928. doi:10.1161/CIRCULATIONAHA.108.844753. ISSN 0009-7322.
- ↑ 3.0 3.1 Imazio, Massimo; Brucato, Antonio; DeRosa, Francesco Giuseppe; Lestuzzi, Chiara; Bombana, Enrico; Scipione, Federica; Leuzzi, Stefano; Cecchi, Enrico; Trinchero, Rita; Adler, Yehuda (2009). “Aetiological diagnosis in acute and recurrent pericarditis: when and how”. Journal of Cardiovascular Medicine. 10 (3): 217–230. doi:10.2459/JCM.0b013e328322f9b1. ISSN 1558-2027.
- ↑ Imazio, Massimo; Belli, Riccardo; Brucato, Antonio; Cemin, Roberto; Ferrua, Stefania; Beqaraj, Federico; Demarie, Daniela; Ferro, Silvia; Forno, Davide; Maestroni, Silvia; Cumetti, Davide; Varbella, Ferdinando; Trinchero, Rita; Spodick, David H; Adler, Yehuda (2014). “Efficacy and safety of colchicine for treatment of multiple recurrences of pericarditis (CORP-2): a multicentre, double-blind, placebo-controlled, randomised trial”. The Lancet. 383 (9936): 2232–2237. doi:10.1016/S0140-6736(13)62709-9. ISSN 0140-6736.
- ↑ Sliwa, Karen; Mocumbi, Ana Olga (2009). “Forgotten cardiovascular diseases in Africa”. Clinical Research in Cardiology. 99 (2): 65–74. doi:10.1007/s00392-009-0094-1. ISSN 1861-0684.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Varun Kumar, M.B.B.S., Cafer Zorkun, M.D., Ph.D. [2], Rim Halaby Homa Najafi, M.D.[3]
Overview
Pericarditis is inflammation of the pericardium, which is the double-walled sac that contains the heart and the roots of the great vessels. There can be an accompanying accumulation of fluid that can be either serous (free flowing fluid) or fibrinous (an exudate, which is a thick fluid composed of proteins, fibrin strands, inflammatory cells, cell breakdown products, and sometimes bacteria). Vascular congestion of the pericardium is also present. The underlying myocardium may or may not be inflamed as well. If the myocardium is involved in the inflammatory process, it is called myopericarditis, and CK and troponin levels may be elevated. Cardiotropic viruses usually spread to the myocardium and pericardium hematogenously and cause acute inflammation with infiltration of polymorphonuclear (PMN) leukocytes and pericardial vascularization. Most patients with viral pericarditis recover completely with few developing recurrences. Some patients develop constrictive pericarditis which could be disabling. Bacterial pericarditis results from contiguous spread of infection within the chest, either de novo or after surgery or trauma, spread from infective endocarditis, hematogenous, or direct inoculation as a result of penetrating injury or cardiothoracic surgery.
Pathophysiology
Anatomy and Physiology of Pericardium
Layers of the Pericardium
- The pericardium is made up of two layers:[1][2][3]
- Fibrous pericardium:
- Hard protective external layer
- Attached to sternum anteriorly by sterno–pericardial ligaments and fused with the central tendon of the diaphragm and great vessels to allow mobility of the pericardial sac against sudden cardiac overfilling
- Serous pericardium:
- Smooth internal layer made up of 2 components:
- Parietal: reflects onto fibrous pericardium
- Visceral: reflects onto heart and great vessels and forms the epicardium, the external layer of the heart wall
- Smooth internal layer made up of 2 components:
- Fibrous pericardium:
- Pericardial cavity: Potential space between parietal and visceral layers. It contains a serous fluid film that occupies the cavity and functions as lubricant against friction by all chest movements.
Pericardial Sinuses
- There are two small chambers or sinuses located where the visceral and parietal pericardium are continuous with one another within the pericardial cavity.[4][5][6]
- Transverse sinus:
- Located posterior to the pulmonary trunk and ascending aorta at the level between the superior vena cava and aortic arch
- Formed after dorsal myocardium ruptured embryonically
- Functional role is to allow the unhindered expansion of great arteries posteriorly during cardiac systole
- Utilized surgically to pass surgical clamps or place ligatures around great arteries.
- Oblique sinus:
- A blind recess (cul-de-sac) posterior to the left atrium between superior vena cava, right and left pulmonary veins inferior to the transverse sinus
- Formed embryonically by the incorporation of the pulmonary vein tributaries into the left atrium
- Functional role believed to be the expansion of the left atrium upon normal collapse of the thorax
Diseases of the Pericardium
- Pericarditis is an inflammatory condition of the pericardium.
- Pericardial effusion is fluid accumulation in the pericardial sac.
- Constrictive pericarditis occurs when there is a scar encasing, the heart that chronically constricts the filling of the heart.
- Cardiac tamponade is a medical emergency in which fluid in the pericardial sac acutely restricts the filling of the heart. This requires surgical drainage or pericardiocentesis.
Additional Images
-
The phrenic nerve and its relations with the vagus nerve.
-
Thoracic portion of the sympathetic trunk.
-
Liver with the septum transversum. Human embryo 3 mm long.
-
The thymus of a full-time fetus, exposed in situ.
Pathogenesis
- Cardiotropic viruses usually spread to the myocardium and pericardium hematogenously and cause acute inflammation with infiltration of polymorphonuclear (PMN) leukocytes and pericardial vascularization. This may cause pericardial effusion and fibrinous change of the pericardium. The pericardium may also develop a serous or hemorrhagic effusion. Most patients with viral pericarditis recover completely with few developing recurrences. Some patients develop constrictive pericarditis which could be disabling.[7][8][9]
- Contiguous spread of infection within the chest, either de novo or after surgery or trauma.
- Spread from infective endocarditis
- Hematogenous spread of infection
- Direct inoculation as a result of penetrating injury or cardiothoracic surgery
- Tuberculous pericarditis develops from lymphatic spread of peritracheal, peribronchial or mediastinal lymph nodes or by contiguous spread from a focus of infection in the lung or pleura. There are four pathologic stages observed:[15][16][17]
- Stage 1: Presence of diffuse fibrin deposition, granulomas and abundant mycobacterium.
- Stage 2: Development of serous or serosanguineous pericardial effusion with a predominantly lymphocytic exudate with monocytes and foam cells.
- Stage 3: Absorption of effusion with the organization of granulomatous caseation and thickening of pericardium secondary to deposition of fibrin and collagen.
- Stage 4: Development of constrictive pericarditis. The pericardial space is obliterated by dense adhesions with marked thickening of the parietal layer and replacement of granulomas by fibrous tissue.
- These types of granulomatous pericarditis also occur with fungal infections, rheumatoid arthritis (RA), and sarcoidosis.
- Pericarditis in renal failure is thought to result from inflammation of the visceral and parietal layers of the pericardium by metabolic toxins such as urea, creatinine, uric acid, methylguanidine, guanidinoacetate, parathyroid hormone, beta2-microglobulin, and others. It may be associated with hemorrhagic or serous effusion.
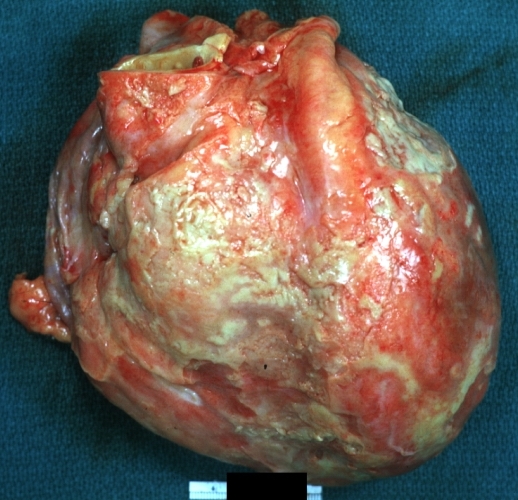
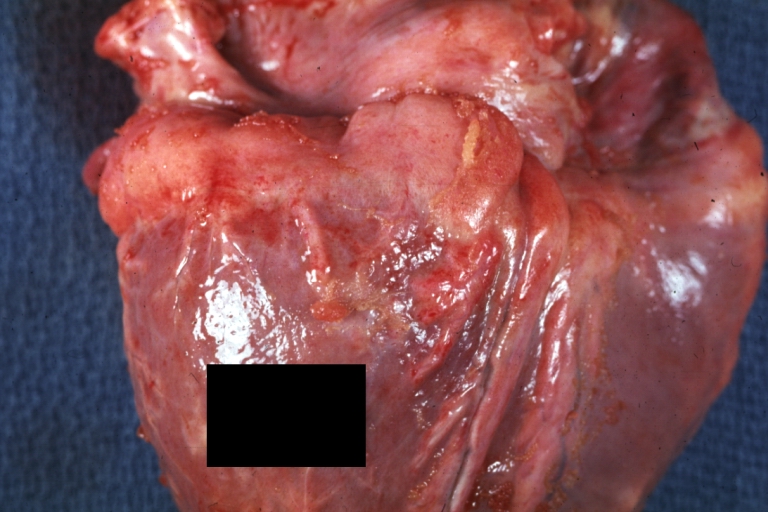
Gross Pathology Images
-
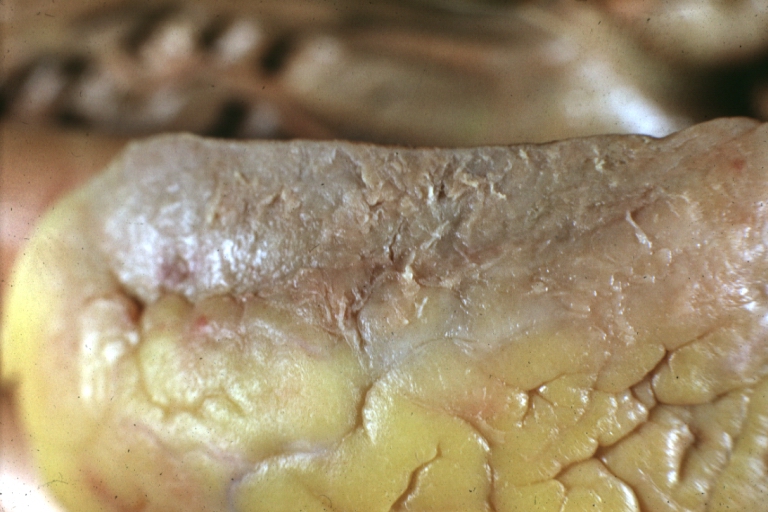
 Fibrinous pericarditis: Gross, natural color, an excellent example of bread and butter appearance. Uremia, chronic glomerulonephritis and sepsis.
Fibrinous pericarditis: Gross, natural color, an excellent example of bread and butter appearance. Uremia, chronic glomerulonephritis and sepsis. -
 Fibrinous pericarditis: Gross, a good example (bread and butter appearance).
Fibrinous pericarditis: Gross, a good example (bread and butter appearance). -
 Fibrinous pericarditis: Gross, an excellent example.
Fibrinous pericarditis: Gross, an excellent example.



-
 Fibrinous pericarditis: Gross, an excellent example, close-up view of fibrin.
Fibrinous pericarditis: Gross, an excellent example, close-up view of fibrin. -
 Fibrinous pericarditis: Gross, an excellent example, close-up view.
Fibrinous pericarditis: Gross, an excellent example, close-up view. -
 Fibrinous pericarditis: Gross, an excellent example.
Fibrinous pericarditis: Gross, an excellent example.



-
 Fibrinous pericarditis: Gross, external view of localized pericarditis over an acute infarction.
Fibrinous pericarditis: Gross, external view of localized pericarditis over an acute infarction. -
 Fibrinous pericarditis: Gross, intact heart, good example.
Fibrinous pericarditis: Gross, intact heart, good example. -
 Fibrinous pericarditis: Gross, good example, mild, with small amount of fibrin.
Fibrinous pericarditis: Gross, good example, mild, with small amount of fibrin.



-
 Fibrinous pericarditis: Gross, close-up, an excellent example of color and detail.
Fibrinous pericarditis: Gross, close-up, an excellent example of color and detail. -
 Fibrinous pericarditis: Gross, a good example.
Fibrinous pericarditis: Gross, a good example. -
 Fibrinous pericarditis: Gross, a good example, very mild case.
Fibrinous pericarditis: Gross, a good example, very mild case.



-
 Fibrinous pericarditis: Gross, an excellent example.
Fibrinous pericarditis: Gross, an excellent example. -
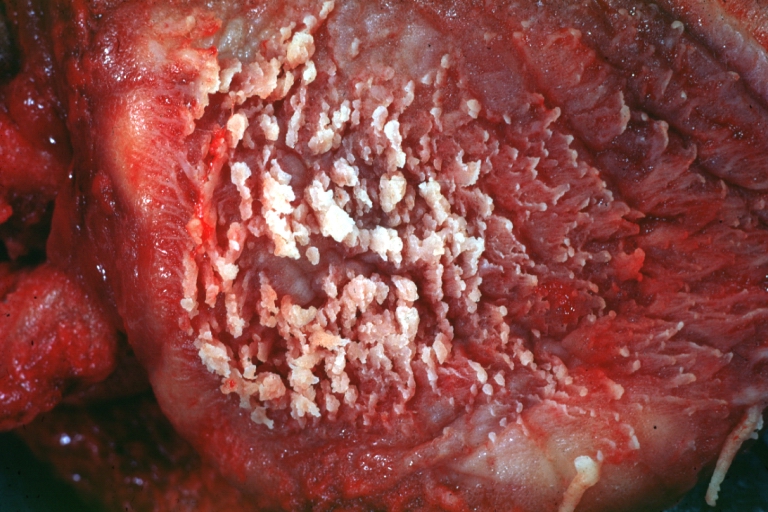
 Fibrinous pericarditis: Gross, a close-up view, an excellent illustration of fibrinous exudate.
Fibrinous pericarditis: Gross, a close-up view, an excellent illustration of fibrinous exudate. -
 Pericarditis in uremia.
Pericarditis in uremia.



-
 Fibrinous pericarditis: Gross, fixed tissue (note to color changes), a close-up view of fibrin on epicardial surface of heart, a typical example.
Fibrinous pericarditis: Gross, fixed tissue (note to color changes), a close-up view of fibrin on epicardial surface of heart, a typical example. -
 Fibrinous pericarditis: Gross, natural color, large right atrial thrombus and fibrinous pericarditis. Normal tricuspid valve with some aging changes (good example).
Fibrinous pericarditis: Gross, natural color, large right atrial thrombus and fibrinous pericarditis. Normal tricuspid valve with some aging changes (good example). -
 Fibrinous pericarditis: Gross, natural color.
Fibrinous pericarditis: Gross, natural color.



-
 Fibrinous pericarditis: Gross, natural color, an excellent example.
Fibrinous pericarditis: Gross, natural color, an excellent example. -
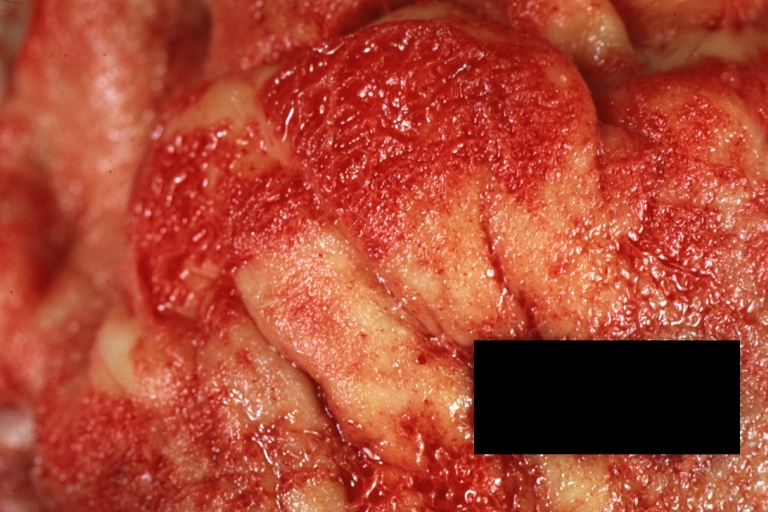
 Fibrinous pericarditis: Gross, natural color, very close-up photo showing fibrinous exudate simulating frost (an excellent example).
Fibrinous pericarditis: Gross, natural color, very close-up photo showing fibrinous exudate simulating frost (an excellent example). -
 Rheumatoid fibrinous pericarditis: Gross, natural color, a typical lesion in 22 years old white female due to juvenile rheumatoid arthritis.
Rheumatoid fibrinous pericarditis: Gross, natural color, a typical lesion in 22 years old white female due to juvenile rheumatoid arthritis.



-
 Fibrinous pericarditis: Gross, natural color, close-up view of minimal fibrinous exudate on epicardial surface due to terminal renal failure.
Fibrinous pericarditis: Gross, natural color, close-up view of minimal fibrinous exudate on epicardial surface due to terminal renal failure. -
 Fibrinous pericarditis: Gross, natural color, anterior view of heart with mild fibrinous exudate over epicardium due to terminal renal failure.
Fibrinous pericarditis: Gross, natural color, anterior view of heart with mild fibrinous exudate over epicardium due to terminal renal failure. -
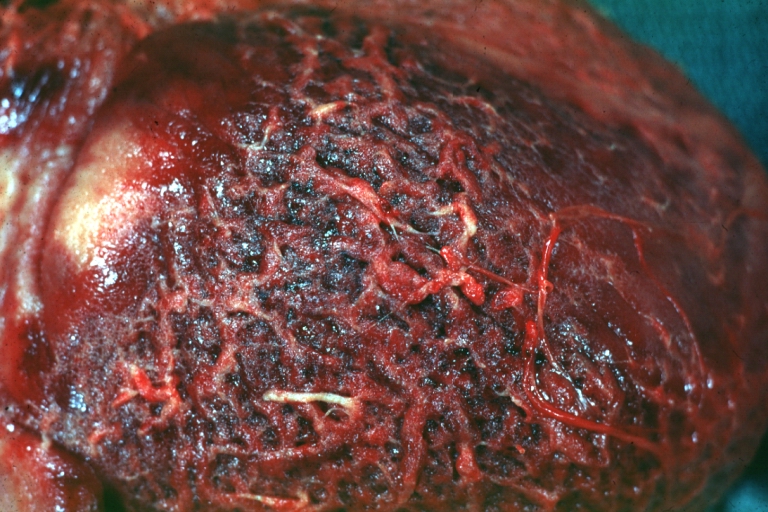
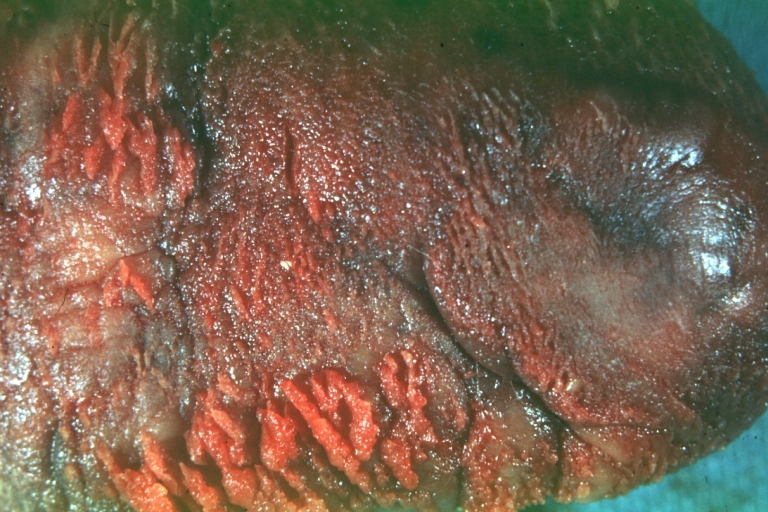
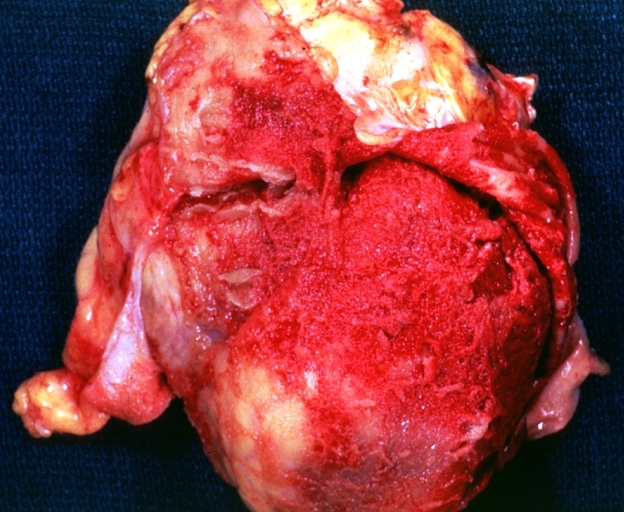
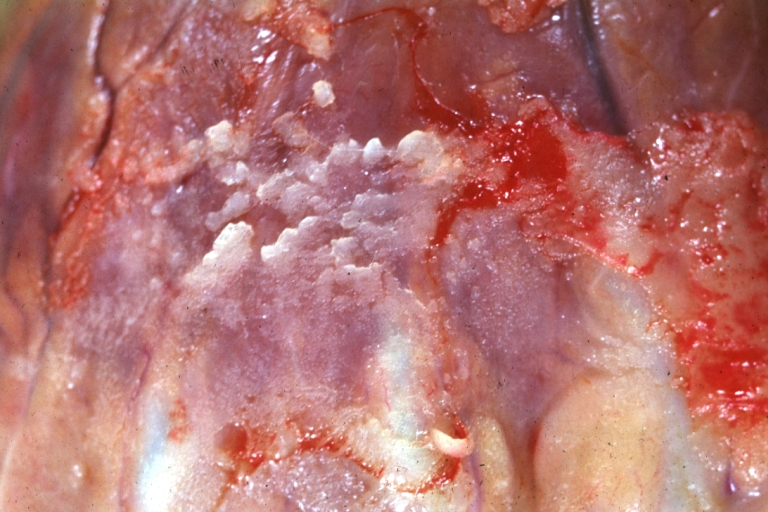
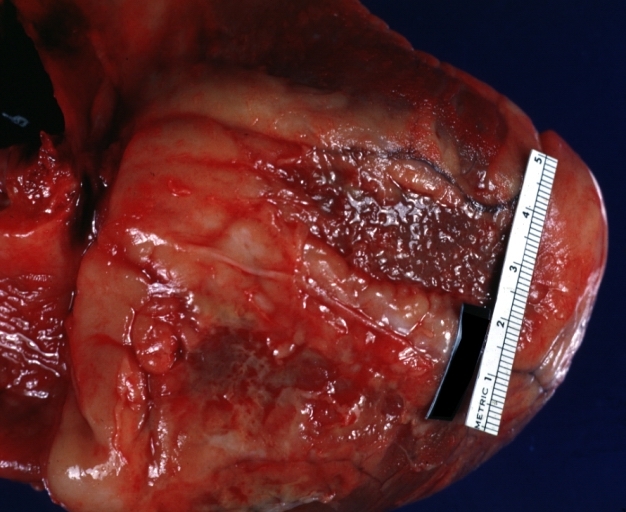
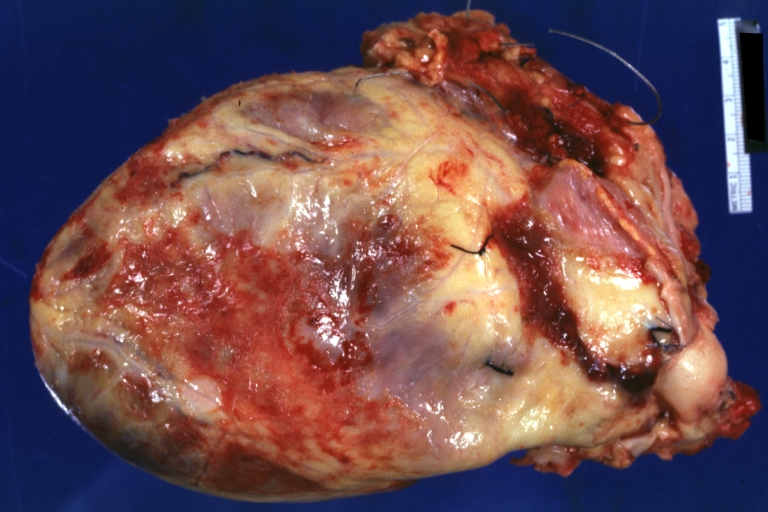
 Tuberculous pericarditis: Gross, natural color, shaggy hemorrhagic exudate. This case is much more hemorrhagic than the typical tuberculous pericarditis.
Tuberculous pericarditis: Gross, natural color, shaggy hemorrhagic exudate. This case is much more hemorrhagic than the typical tuberculous pericarditis.



-
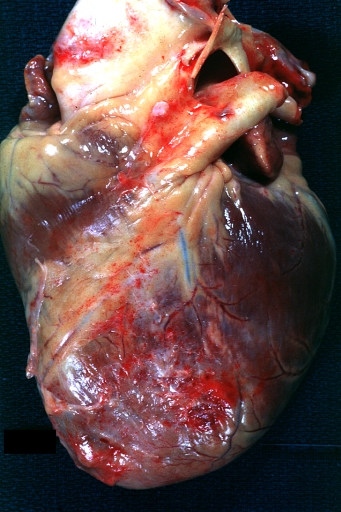
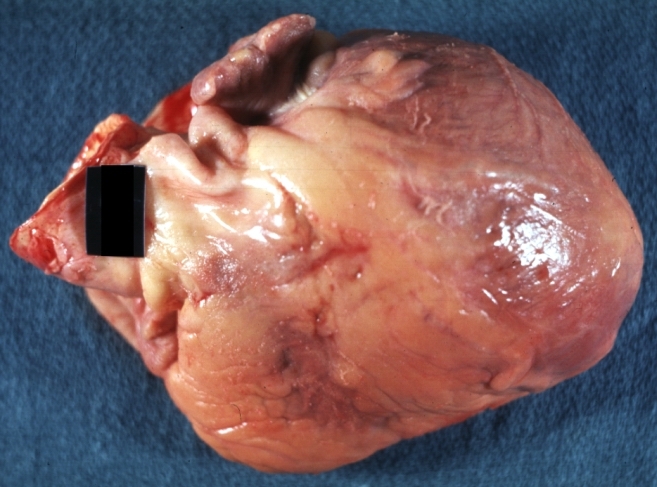
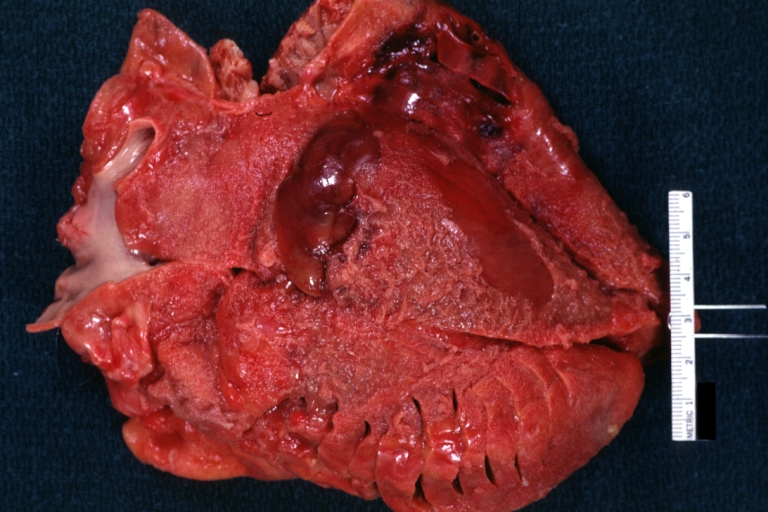
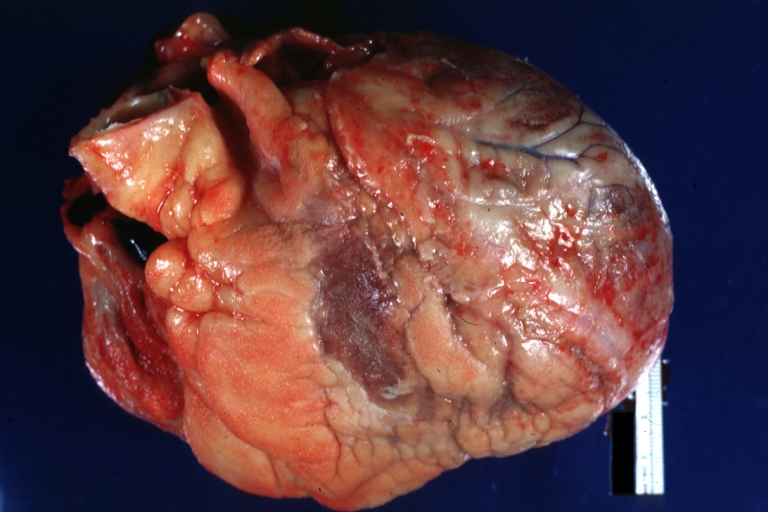
 Heart transplant: Gross, natural color, external view of heart. Two months after transplantation with fibrinous pericarditis.
Heart transplant: Gross, natural color, external view of heart. Two months after transplantation with fibrinous pericarditis. -
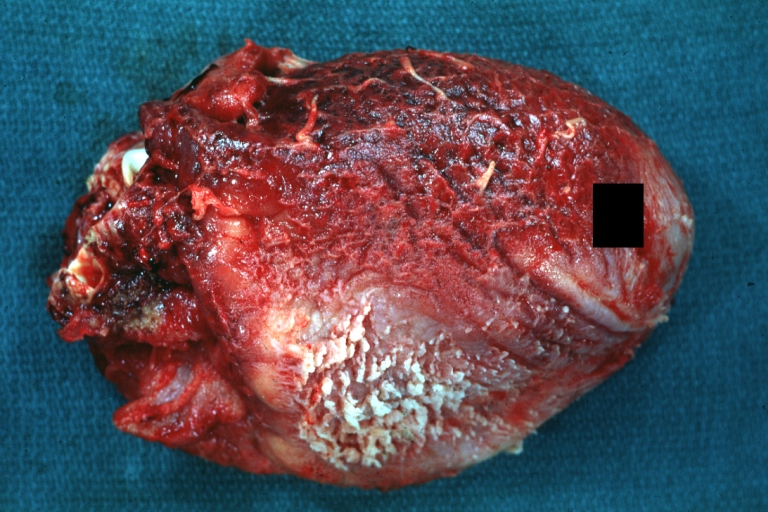
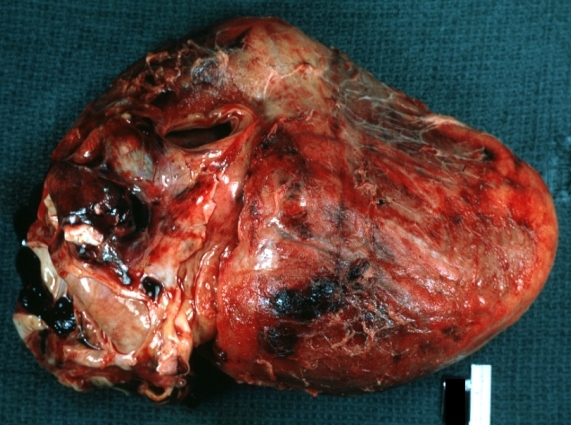
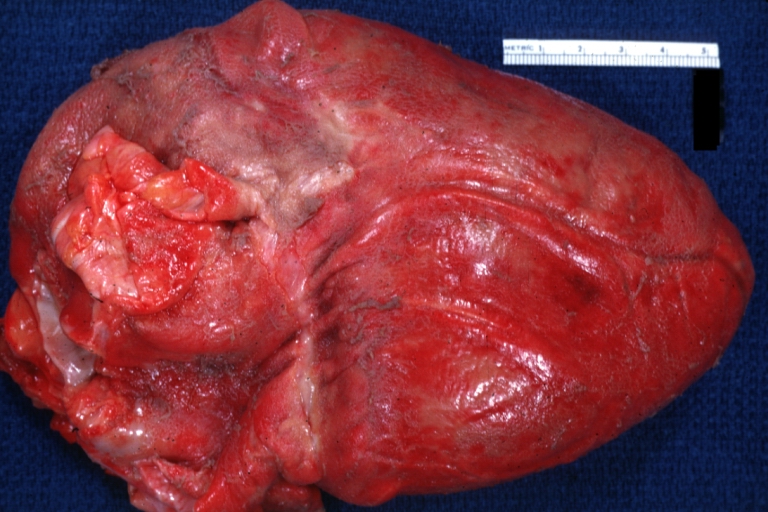
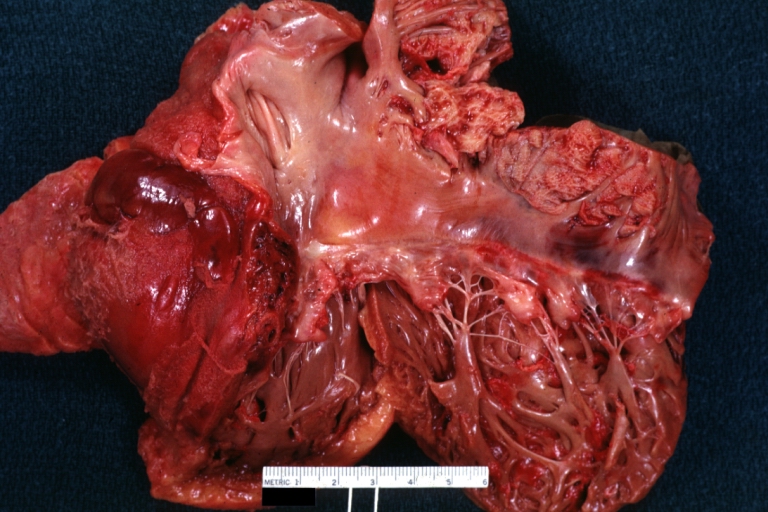
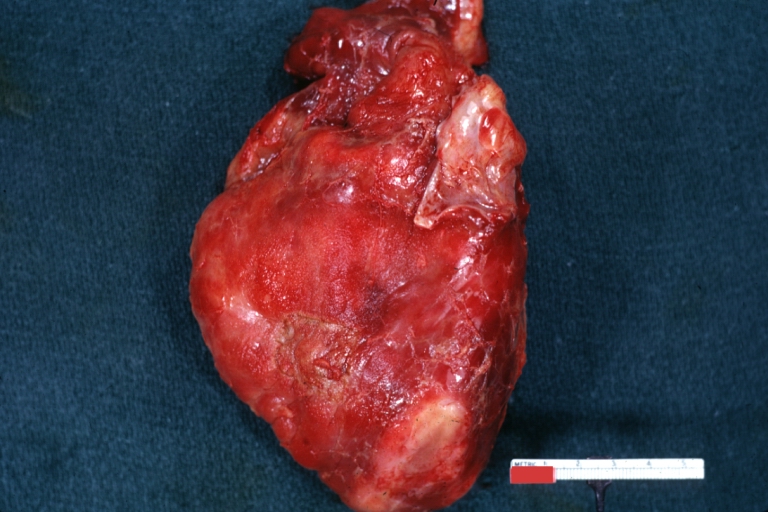
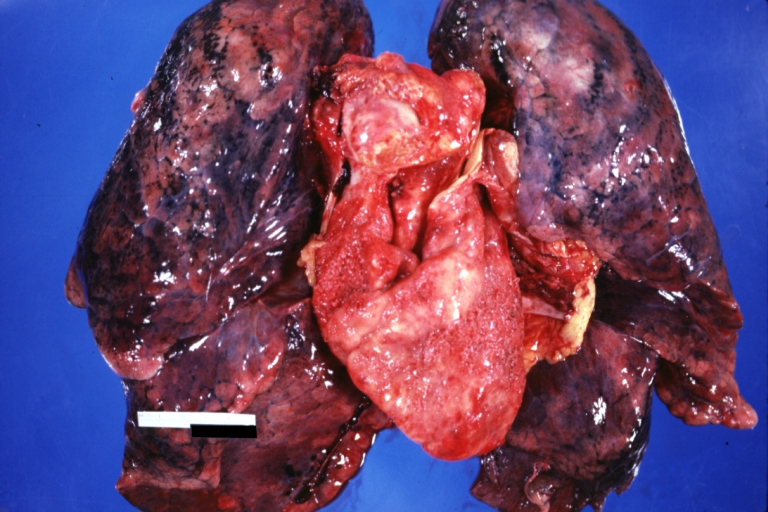 Neoplastic pericarditis: Gross, natural color, shaggy pericarditis. Primer is adenocarcinoma of the lung.
Neoplastic pericarditis: Gross, natural color, shaggy pericarditis. Primer is adenocarcinoma of the lung. -
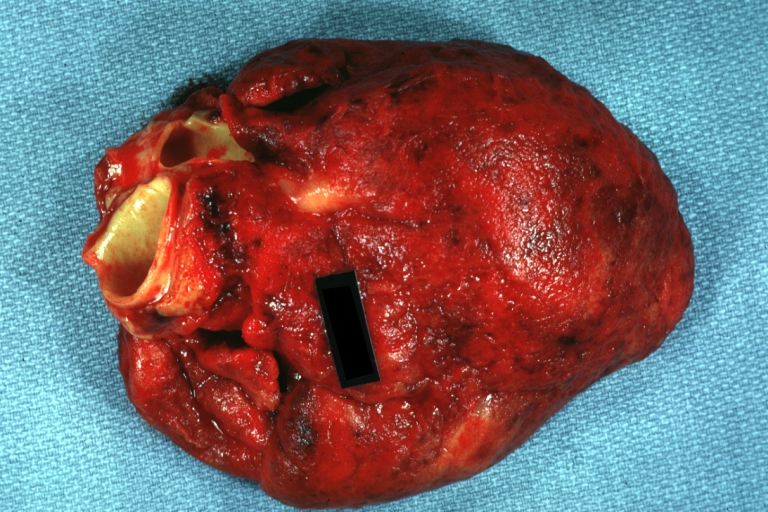
 Heart: Septic pericarditis.
Heart: Septic pericarditis.



Microscopic Pathology Images
-
 Tuberculous pericarditis.
Tuberculous pericarditis. -
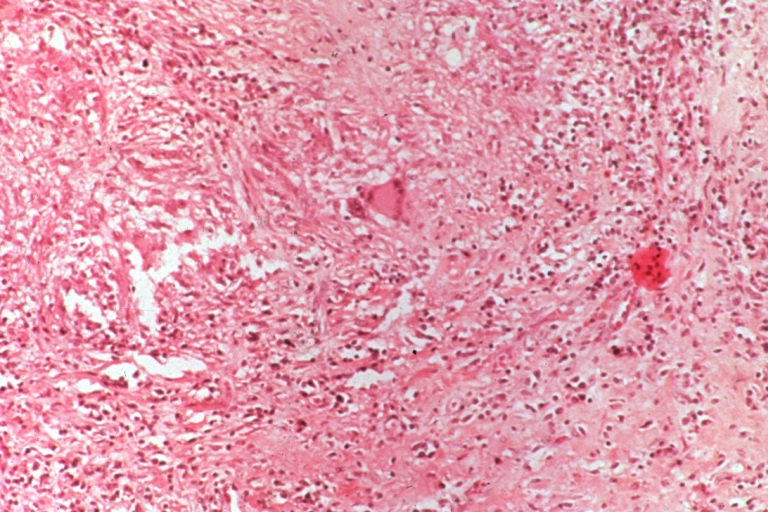 Tuberculous pericarditis.
Tuberculous pericarditis. -
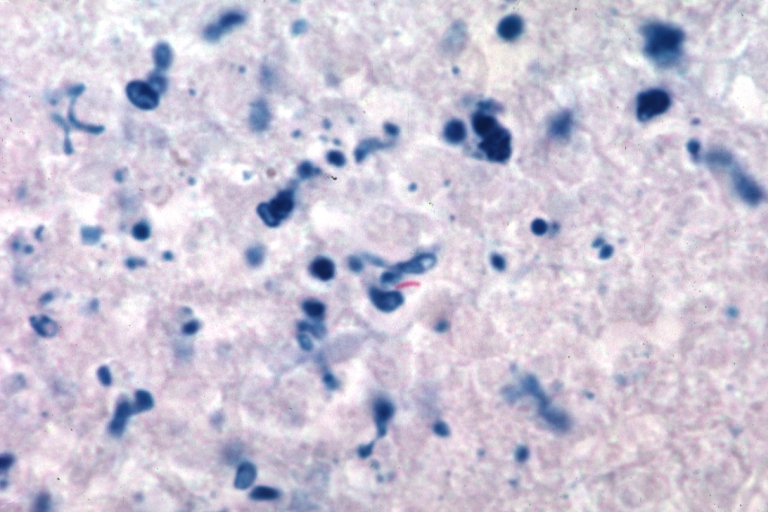 Tuberculous pericarditis: Micro oil acid fast stain. The organism easily seen.
Tuberculous pericarditis: Micro oil acid fast stain. The organism easily seen.



-
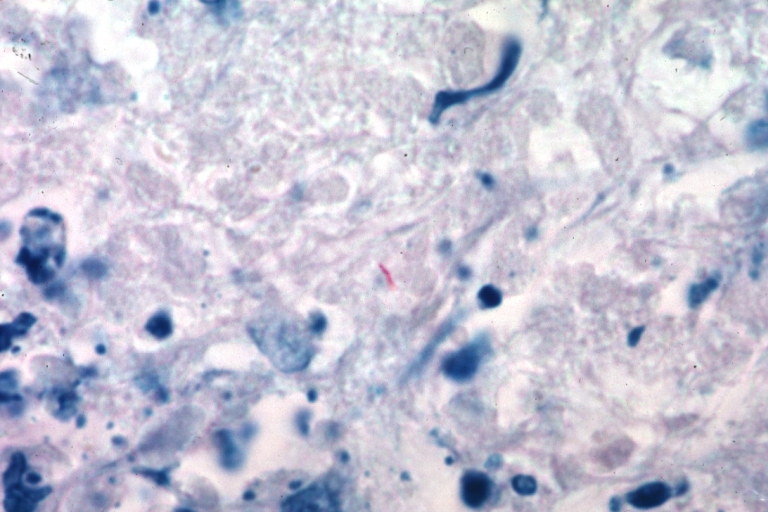 Tuberculous pericarditis: Micro oil acid fast stain. The organism easily seen.
Tuberculous pericarditis: Micro oil acid fast stain. The organism easily seen. -
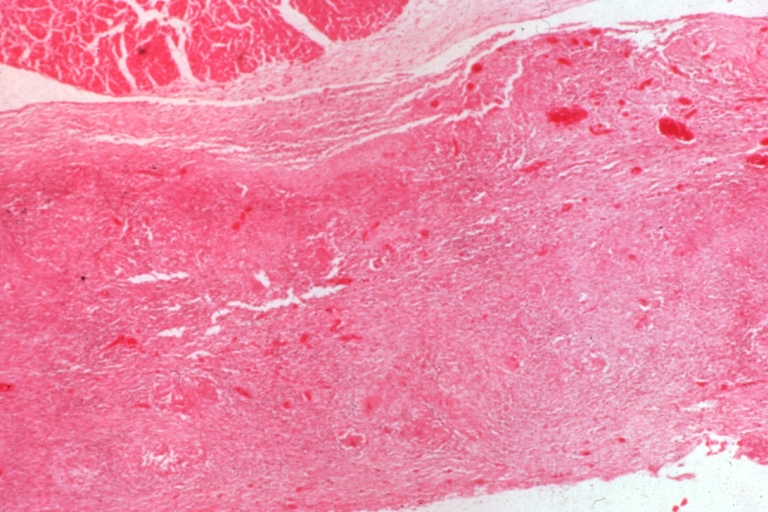
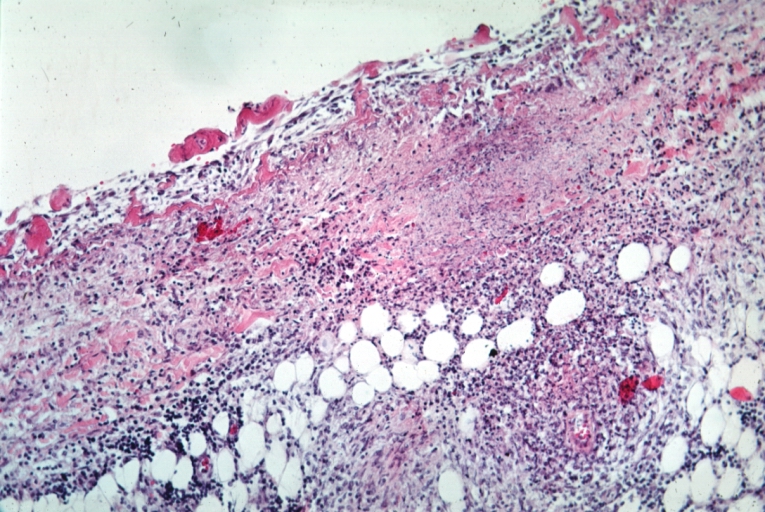
 Uremic pericarditis: Micro med mag, H&E. A good example
Uremic pericarditis: Micro med mag, H&E. A good example -
 Tuberculous pericarditis: Micro med mag, H&E, a typical lesion
Tuberculous pericarditis: Micro med mag, H&E, a typical lesion



-
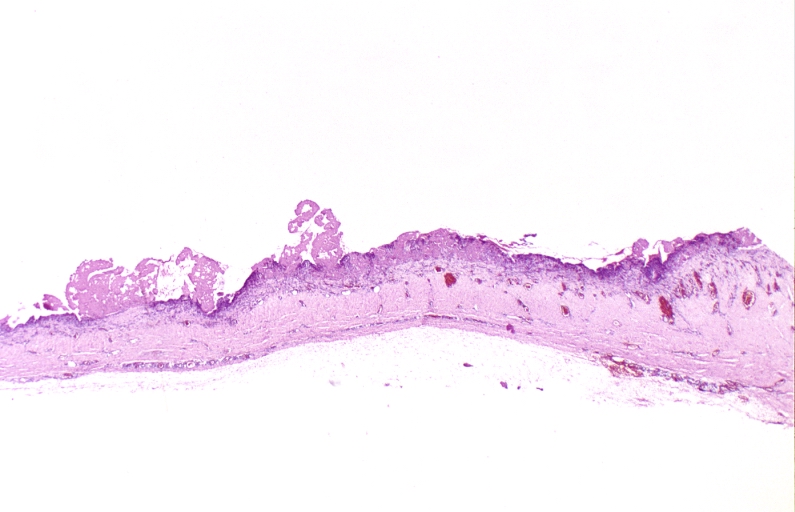 Fibrinous pericarditis.
Fibrinous pericarditis. -
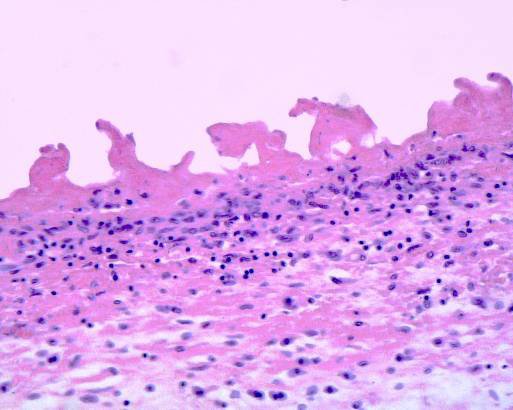 Pericarditis fibrinosa (Fibrinous pericarditis).
Pericarditis fibrinosa (Fibrinous pericarditis). -
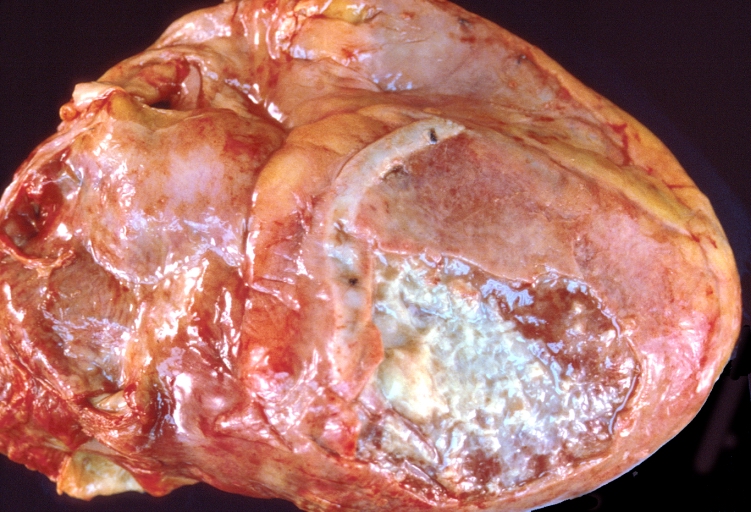
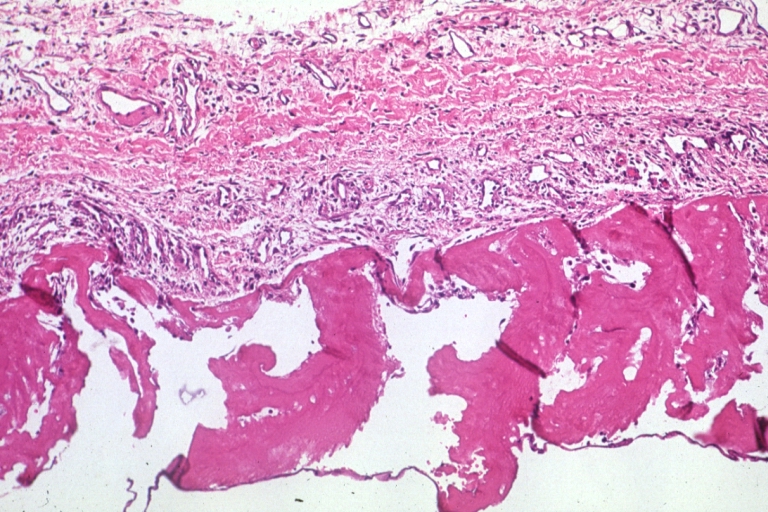
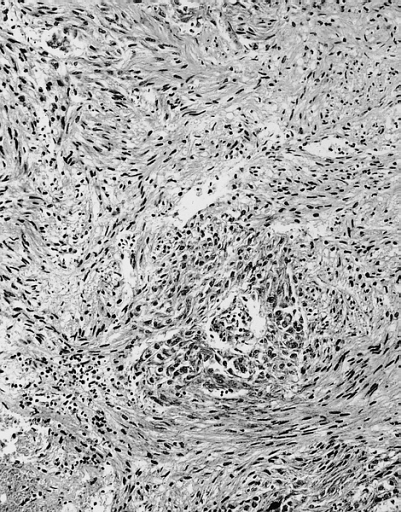 Malignant Mesothelioma, Biphasic Type: Pericardium: This tumor has epithelioid cells (lower half) surrounded by spindled cells. The patient was a 46-year-old woman with constrictive pericarditis; the pericardium was studded with coalescing tumor nodules.
Malignant Mesothelioma, Biphasic Type: Pericardium: This tumor has epithelioid cells (lower half) surrounded by spindled cells. The patient was a 46-year-old woman with constrictive pericarditis; the pericardium was studded with coalescing tumor nodules.



Videos
| AKS7kSl4x5k}} | Acute Fibrinous Pericarditis
{{#ev:youtube|5fz_W1YxbC8}} |
|---|
References
- ↑ Kishore, K. (2003). The Heart of Structural Development: The Functional Basis of the Location and Morphology of the Human Vascular Pump. J Postgrad Med, 49:282-4.
- ↑ Moore, K. L., Agur, A. M., & Dalley, A. F. (2011). Essential Clinical Anatomy – Fourth Edition. Lippincott Williams & Wilkins.
- ↑ Tank, P. W. (2009). Grant’s Dissector – Fourteenth Edition. Lippincott Williams & Wilkins.
- ↑ Kishore, K. (2003). The Heart of Structural Development: The Functional Basis of the Location and Morphology of the Human Vascular Pump. J Postgrad Med, 49:282-4.
- ↑ Moore, K. L., Agur, A. M., & Dalley, A. F. (2011). Essential Clinical Anatomy – Fourth Edition. Lippincott Williams & Wilkins.
- ↑ Tank, P. W. (2009). Grant’s Dissector – Fourteenth Edition. Lippincott Williams & Wilkins.
- ↑ Matthews JD, Cameron SJ, George M (1970). “Constrictive pericarditis following Coxsackie virus infection”. Thorax. 25 (5): 624–6. PMC 472200. PMID 5489188.
- ↑ Ilan Y, Oren R, Ben-Chetrit E (1991). “Acute pericarditis: etiology, treatment and prognosis. A study of 115 patients”. Jpn Heart J. 32 (3): 315–21. PMID 1920818.
- ↑ Shabetai R (1990). “Acute pericarditis”. Cardiol Clin. 8 (4): 639–44. PMID 2249218.
- ↑ Klacsmann PG, Bulkley BH, Hutchins GM (1977). “The changed spectrum of purulent pericarditis: an 86 year autopsy experience in 200 patients”. Am J Med. 63 (5): 666–73. PMID 930941.
- ↑ Kauffman CA, Watanakunakorn C, Phair JP (1973). “Purulent pneumococcal pericarditis. A continuing problem in the antibiotic era”. Am J Med. 54 (6): 743–50. PMID 4200204.
- ↑ Rubin RH, Moellering RC (1975). “Clinical, microbiologic and therapeutic aspects of purulent pericarditis”. Am J Med. 59 (1): 68–78. PMID 1138554.
- ↑ Ribeiro P, Shapiro L, Nihoyannopoulos P, Gonzalez A, Oakley CM (1985). “Pericarditis in infective endocarditis”. Eur Heart J. 6 (11): 975–8. PMID 4076207.
- ↑ Roberts WC, Buchbinder NA (1972). “Right-sided valvular infective endocarditis. A clinicopathologic study of twelve necropsy patients”. Am J Med. 53 (1): 7–19. PMID 4402567.
- ↑ Peel AA (1948). “TUBERCULOUS PERICARDITIS”. Br Heart J. 10 (3): 195–207. PMC 481044. PMID 18610109.
- ↑ Permanyer-Miralda G, Sagristá-Sauleda J, Soler-Soler J (1985). “Primary acute pericardial disease: a prospective series of 231 consecutive patients”. Am J Cardiol. 56 (10): 623–30. PMID 4050698.
- ↑ Mayosi BM, Burgess LJ, Doubell AF (2005). “Tuberculous pericarditis”. Circulation. 112 (23): 3608–16. doi:10.1161/CIRCULATIONAHA.105.543066. PMID 16330703.
Causes
HIV | Post-MI | Post-pericardiotomy | Radiation | Tuberculosis | Uremia | Malignancy
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mugilan Poongkunran M.B.B.S [2] Ahmed Zaghw, M.D. [3] Homa Najafi, M.D.[4]
Overview
The causes of pericarditis can be divided into infectious and non-infectious ones. Infectious causes include bacterial, viral, fungal and, parasitic. While, non-infectious causes include autoimmune, neoplastic, metabolic, traumatic and iatrogenic, and drug-related. Acute myocardial infarction, Addisonian crisis, aortic dissection and rupture, blunt or penetrating chest trauma, esophageal perforation, gastric perforation, and myocardial rupture are life threatening causes of pericarditis. Common causes of pericarditis include viral, bacterial organisms, neoplasms, autoimmune and renal failure.
Causes
Life Threatening Causes
Life-threatening causes include conditions which may result in death or permanent disability within 24 hours if left untreated and include:[1][2][3][4]
- Acute myocardial infarction
- Addisonian crisis
- Aortic dissection
- Aortic rupture
- Blunt or penetrating chest trauma
- Esophogeal perforation
- Gastric perforation
- Myocardial rupture
Common Causes
- Acute myocardial infarction
- Cardiac catheterization
- Staphylococcus aureus (MSSA, MRSA)
- Streptococcus pneumoniae
- Neisseria meningitidis
- Enterobacteriaceae
- Tuberculosis
- Histoplasmosis
- Coxsackie B virus
- Echovirus
- HIV
- Adenovirus
- Influenza
- Neoplasm
- Renal Failure
- Sulfa drugs
- Aminosalicylic acid
- Amiodarone
- Systemic lupus erythematosus
- Rheumatoid arthritis
- Idiopathic
Causes by Organ System
Causes in Alphabetical Order
- 5-Fluorouracil
- Actinomycosis
- Acute myocardial infarction
- Acute rheumatic fever
- Addisonian crisis
- Adenovirus
- Amebiasis
- Aminosalicylic acid
- Amiodarone
- Amyloidosis
- Angioma
- Ankylosing spondylitis
- Anticoagulants
- Aortic dissection
- Aortic rupture
- Asbestosis
- Behcet’s disease
- Benign obstruction of thoracic duct
- Blunt or penetrating chest trauma
- Borrelia
- Breast cancer
- Bromocriptine
- Carcinoid
- Cardiac catheterization
- Cardiopulmonary resuscitation
- Cathether ablation for arrhythmias
- Certolizumab pegol
- Chlamydia psittaci
- Cholesterol pericarditis
- Chylopericardium
- Coccidioidomycosis
- Collagen vascular disease
- Coronary artery bypass grafting
- Coxsackie B virus
- Cromolyn sodium
- Cyclophosphamide
- Cyclosporine
- Cytarabine
- Cytomegalovirus
- Dantrolene
- Daunorubicin
- Dermatomyositis
- Dialysis
- Dissecting aortic aneurysm
- Doxorubicin
- Dressler’s syndrome
- EBV
- Echinococcosis
- ECHO virus
- Endocarditis
- Esophageal rupture
- Esophogeal perforation
- Familial mediterranean fever
- Fibroma
- Francisella
- Gastric perforation
- Gaucher disease
- Heart surgery
- Herpes viruses
- Histoplasmosis
- HIV
- Hydantoin
- Hydralazine
- Hypothyroidism
- Idiopathic
- Infectious mononucleosis
- Inflammatory bowel disease
- Influenza virus
- Isoniazid
- Jacobs arthropathy-camptodactyly syndrome
- Kaposi’s sarcoma
- Kawasaki disease
- Leiomyoma
- Legionella
- Leukemia
- Lipoma
- Lung cancer
- Lymphoma
- Melanoma
- Meningococci
- Mesalazine
- Mesothelioma
- Methyldopa
- Methysergide
- Minoxidil
- Mixed connective tissue disease
- Mulibrey nanism syndrome
- Mumps virus
- Mycoplasma
- Myocardial rupture
- Myocarditis
- Myxedema
- Neisseria gonorrhoeae
- Neoplasia that has spread to the pericardium,
- Ovarian cancer
- Pacemaker syndrome
- Pancreatic-pericardial fistula
- Penicillin
- Percutaneous coronary intervention
- Pergolide
- Phenylbutazone
- Pneumococci
- Pneumonia
- Polyarteritis nodosa
- Polymyositis
- Polytetrafluoroethylene inhalation
- Postpericardiotomy syndrome
- Practolol
- Procainamide
- Radiation therapy
- Recurrent hereditary polyserositis
- Rhabdomyosarcoma
- Reiter’s syndrome
- Renal failure
- Reserpine
- Rheumatoid arthritis
- Rickettsia
- Sarcoidosis
- Sarcoma
- Scleroderma
- Serum sickness
- Silicosis
- Sipple syndrome
- Staphylococci
- Streptococci
- Streptokinase
- Streptomycin
- Sulfa drugs
- Systemic lupus erythematosus
- TAVI
- Temporal arteritis
- Teratoma
- Thiazides
- Thiouracil
- Thoracic surgery
- Thorax trauma
- Thrombolytics
- Tocainide
- Toxoplasmosis
- Treponema pallidum
- Tuberculosis
- Ureaplasma
- Uremia
- Vaccines (smallpox, yellow fever)
- Valvuloplasty
- Varicella virus
- Wegener’s granulomatosis
- Whipple’s Disease
Summery of causes
| Pericarditis classification based on etiology | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Infectious causes | Non-infectious causes | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Viral:
Enteroviruses(coxsackieviruses, echoviruses) Herpes viruses(EBV, CMV, HHV-6) Adenoviruses Parvovirus B19 | Bacterial:
Mycobacterium tuberculosis Coxiella burnetii Borrelia burgdorferi | Fungal:
Histoplasma species Aspergillus species Blastomyces species Candida species | Parasitic:
Echinococcus species Toxoplasma species | Autoimmune:
Systemic autoimmune and auto-inflammatory diseases Systemic vasculitides Sarcoidosis Familial Mediterranean fever IBD Still disease | Neoplastic:
Primary tumours (pericardial mesothelioma) secondary metastatic tumors( lung and breast cancer, lymphoma) | Metabolic:
Uraemia Myxoedema Anorexia nervosa | Traumatic and Iatrogenic | Drug-related | Others:
Amyloidosis Aortic dissection Pulmonary arterial Hypertension Chronic heart failure Congenital absence of the pericardium | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
References
- ↑ Imazio, Massimo (2012). “Contemporary management of pericardial diseases”. Current Opinion in Cardiology. 27 (3): 308–317. doi:10.1097/HCO.0b013e3283524fbe. ISSN 0268-4705.
- ↑ Imazio, Massimo; Spodick, David H.; Brucato, Antonio; Trinchero, Rita; Adler, Yehuda (2010). “Controversial Issues in the Management of Pericardial Diseases”. Circulation. 121 (7): 916–928. doi:10.1161/CIRCULATIONAHA.108.844753. ISSN 0009-7322.
- ↑ Imazio, Massimo; Brucato, Antonio; DeRosa, Francesco Giuseppe; Lestuzzi, Chiara; Bombana, Enrico; Scipione, Federica; Leuzzi, Stefano; Cecchi, Enrico; Trinchero, Rita; Adler, Yehuda (2009). “Aetiological diagnosis in acute and recurrent pericarditis: when and how”. Journal of Cardiovascular Medicine. 10 (3): 217–230. doi:10.2459/JCM.0b013e328322f9b1. ISSN 1558-2027.
- ↑ Sliwa, Karen; Mocumbi, Ana Olga (2009). “Forgotten cardiovascular diseases in Africa”. Clinical Research in Cardiology. 99 (2): 65–74. doi:10.1007/s00392-009-0094-1. ISSN 1861-0684.
Differentiating Pericarditis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [2]; Associate Editor(s)-in-Chief: Syed Hassan A. Kazmi BSc, MD [3] Homa Najafi, M.D.[4]
Overview
Pericarditis must be differentiated from diseases presenting with chest pain, shortness of breath and tachypnea which include myocardial infarction, pulmonary embolism, congestive heart failure, pneumonia, vasculitis, and chronic obstructive pulmonary disease (COPD). Manifestation of the pericarditis can help in differentiation from myocardial infarction. Moreover, other differential diagnosis include aortic stenosis, coronary artery vasospasm, esophageal rupture, esophageal spasm, esophagitis,acute gastritis, gastroesophageal reflux disease, and peptic ulcer disease should be considered.
Differentiating Pericarditis from other Diseases
- Pericarditis must be differentiated from diseases presenting with chest pain, shortness of breath and tachypnea.
- For a full discussion of the differential diagnosis of chest pain click here
- For an expert algorithm that aids in the diagnosis of the cause of chest pain click here
- Pericarditis must be differentiated from myocardial infarction as an important cause of chest pain.The differentiating features include:[1]
| Characteristic/Parameter | Pericarditis | Myocardial infarction |
|---|---|---|
| Pain description | Sharp, pleuritic, retro-sternal (under the sternum) or left precordial (left chest) pain. | Crushing, pressure-like, heavy pain. Described as “elephant on the chest“. |
| Radiation | Pain radiates to the trapezius ridge (to the lowest portion of the scapula on the back) or no radiation. | Pain radiates to the jaw, or the left or arm, or does not radiate. |
| Exertion | Does not change the pain | Can increase the pain |
| Position | Pain is worse supine or upon inspiration (breathing in) | Not positional |
| Onset/duration | Sudden pain, that lasts for hours or sometimes days before a patient comes to the ER | Sudden or chronically worsening pain that can come and go in paroxysms or it can last for hours before the patient decides to come to the ER |
Differentiating pericarditis from other diseases on the basis of chest pain, shortness of breath, and tachypnea
The differentials include the following:[2][3][4][5][6][7][8][9][10][11][12][13][14][15][16][17][18][19][20][21]
| Diseases | Diagnostic tests | Physical Examination | Symptoms | Past medical history | Other Findings | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CT scan and MRI | EKG | Chest X-ray | Tachypnea | Tachycardia | Fever | Chest Pain | Hemoptysis | Dyspnea on Exertion | Wheezing | Chest Tenderness | Nasalopharyngeal Ulceration | Carotid Bruit | |||
| Pulmonary embolism |
|
|
|
✔ | ✔ | ✔ (Low grade) | ✔ | ✔ (In case of massive PE) | ✔ | – | – | – | – |
|
|
| Congestive heart failure |
|
✔ | ✔ | ✔ | – | – | ✔ | – | – | – | – |
|
| ||
| Percarditis |
|
|
|
✔ | ✔ | ✔ (Low grade) | ✔ (Relieved by sitting up and leaning forward) | – | ✔ | – | – | – | – |
|
|
| Pneumonia |
|
|
|
✔ | ✔ | ✔ | ✔ | – | ✔ | ✔ | – | – | – |
|
|
| Vasculitis |
|
|
✔ | ✔ | ✔ | ✔ | ✔ | ✔ | – | ✔ | ✔ | ✔ |
|
||
| Chronic obstructive pulmonary disease (COPD) |
|
|
✔ | ✔ | – | – | – | ✔ | ✔ | – | – | – |
|
| |
Other differentials
Pericarditis also resembles the following disorders and needs to be differentiated from them:
- Angina pectoris
- Aortic stenosis
- Coronary artery vasospasm
- Esophageal rupture
- Esophageal spasm
- Esophagitis
- Gastritis, acute
- Gastroesophageal reflux disease
- Peptic ulcer disease
References
- ↑ American College of Physicians (ACP). Medical Knowledge Self-Assessment Program (MKSAP-15): Cardiovascular Medicine. “Pericardial disease.” p. 64. ISBN 978-934465-28-8 [1]
- ↑ Brenes-Salazar JA (2014). “Westermark’s and Palla’s signs in acute and chronic pulmonary embolism: Still valid in the current computed tomography era”. J Emerg Trauma Shock. 7 (1): 57–8. doi:10.4103/0974-2700.125645. PMC 3912657. PMID 24550636.
- ↑ “CT Angiography of Pulmonary Embolism: Diagnostic Criteria and Causes of Misdiagnosis | RadioGraphics”.
- ↑ Bĕlohlávek J, Dytrych V, Linhart A (2013). “Pulmonary embolism, part I: Epidemiology, risk factors and risk stratification, pathophysiology, clinical presentation, diagnosis and nonthrombotic pulmonary embolism”. Exp Clin Cardiol. 18 (2): 129–38. PMC 3718593. PMID 23940438.
- ↑ “Pulmonary Embolism: Symptoms – National Library of Medicine – PubMed Health”.
- ↑ Ramani GV, Uber PA, Mehra MR (2010). “Chronic heart failure: contemporary diagnosis and management”. Mayo Clin. Proc. 85 (2): 180–95. doi:10.4065/mcp.2009.0494. PMC 2813829. PMID 20118395.
- ↑ Blinderman CD, Homel P, Billings JA, Portenoy RK, Tennstedt SL (2008). “Symptom distress and quality of life in patients with advanced congestive heart failure”. J Pain Symptom Manage. 35 (6): 594–603. doi:10.1016/j.jpainsymman.2007.06.007. PMC 2662445. PMID 18215495.
- ↑ Hawkins NM, Petrie MC, Jhund PS, Chalmers GW, Dunn FG, McMurray JJ (2009). “Heart failure and chronic obstructive pulmonary disease: diagnostic pitfalls and epidemiology”. Eur. J. Heart Fail. 11 (2): 130–9. doi:10.1093/eurjhf/hfn013. PMC 2639415. PMID 19168510.
- ↑ Takasugi JE, Godwin JD (1998). “Radiology of chronic obstructive pulmonary disease”. Radiol. Clin. North Am. 36 (1): 29–55. PMID 9465867.
- ↑ Wedzicha JA, Donaldson GC (2003). “Exacerbations of chronic obstructive pulmonary disease”. Respir Care. 48 (12): 1204–13, discussion 1213–5. PMID 14651761.
- ↑ Nakawah MO, Hawkins C, Barbandi F (2013). “Asthma, chronic obstructive pulmonary disease (COPD), and the overlap syndrome”. J Am Board Fam Med. 26 (4): 470–7. doi:10.3122/jabfm.2013.04.120256. PMID 23833163.
- ↑ Khandaker MH, Espinosa RE, Nishimura RA, Sinak LJ, Hayes SN, Melduni RM, Oh JK (2010). “Pericardial disease: diagnosis and management”. Mayo Clin. Proc. 85 (6): 572–93. doi:10.4065/mcp.2010.0046. PMC 2878263. PMID 20511488.
- ↑ Bogaert J, Francone M (2013). “Pericardial disease: value of CT and MR imaging”. Radiology. 267 (2): 340–56. doi:10.1148/radiol.13121059. PMID 23610095.
- ↑ Gharib AM, Stern EJ (2001). “Radiology of pneumonia”. Med. Clin. North Am. 85 (6): 1461–91, x. PMID 11680112.
- ↑ Schmidt WA (2013). “Imaging in vasculitis”. Best Pract Res Clin Rheumatol. 27 (1): 107–18. doi:10.1016/j.berh.2013.01.001. PMID 23507061.
- ↑ Suresh E (2006). “Diagnostic approach to patients with suspected vasculitis”. Postgrad Med J. 82 (970): 483–8. doi:10.1136/pgmj.2005.042648. PMC 2585712. PMID 16891436.
- ↑ Stein PD, Dalen JE, McIntyre KM, Sasahara AA, Wenger NK, Willis PW (1975). “The electrocardiogram in acute pulmonary embolism”. Prog Cardiovasc Dis. 17 (4): 247–57. PMID 123074.
- ↑ Warnier MJ, Rutten FH, Numans ME, Kors JA, Tan HL, de Boer A, Hoes AW, De Bruin ML (2013). “Electrocardiographic characteristics of patients with chronic obstructive pulmonary disease”. COPD. 10 (1): 62–71. doi:10.3109/15412555.2012.727918. PMID 23413894.
- ↑ Stein PD, Matta F, Ekkah M, Saleh T, Janjua M, Patel YR, Khadra H (2012). “Electrocardiogram in pneumonia”. Am. J. Cardiol. 110 (12): 1836–40. doi:10.1016/j.amjcard.2012.08.019. PMID 23000104.
- ↑ Hazebroek MR, Kemna MJ, Schalla S, Sanders-van Wijk S, Gerretsen SC, Dennert R, Merken J, Kuznetsova T, Staessen JA, Brunner-La Rocca HP, van Paassen P, Cohen Tervaert JW, Heymans S (2015). “Prevalence and prognostic relevance of cardiac involvement in ANCA-associated vasculitis: eosinophilic granulomatosis with polyangiitis and granulomatosis with polyangiitis”. Int. J. Cardiol. 199: 170–9. doi:10.1016/j.ijcard.2015.06.087. PMID 26209947.
- ↑ Dennert RM, van Paassen P, Schalla S, Kuznetsova T, Alzand BS, Staessen JA, Velthuis S, Crijns HJ, Tervaert JW, Heymans S (2010). “Cardiac involvement in Churg-Strauss syndrome”. Arthritis Rheum. 62 (2): 627–34. doi:10.1002/art.27263. PMID 20112390.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Varun Kumar, M.B.B.S. Homa Najafi, M.D.[2]
Overview
The incidence of acute pericarditis is approximately 27.7 per 100,000 individuals annually. The recurrence of disease is seen in almost 30% of patients after first episode. The mortality rate of acute pericarditis is approximately 1.1% in developed countries. Patients of all age groups may develop acute pericarditis. Although it commonly affects men in 20 to 50 years of age. Pericarditis in developed countries is most commonly due to malignancy or viral infection. It usually follows respiratory infections, most commonly echovirus or coxsackie virus. In children, it is most commonly caused by adenovirus or coxsackie virus. In developing countries pericarditis is usually secondary to tuberculosis or HIV infection. Tuberculous pericarditis, caused by Mycobacterium tuberculosis, is found in approximately 1% of all autopsied cases of TB and in 1% to 2% of instances of pulmonary TB.
Epidemiology and Demographics
Incidence
- The incidence of acute pericarditis is approximately 27.7 per 100,000 individuals annually.[1][2][3][4]
- The incidence of hospitalization for acute pericarditis was estimated to be 3.32 cases per 100,000 individuals annually.
- The recurrence of pericarditis is seen in almost 30% of patients after first episode of disease.
Case-fatality rate/Mortality rate
- The mortality rate of acute pericarditis is approximately 1.1% in developed countries.[2]
Age
- Patients of all age groups may develop acute pericarditis. Although it commonly affects people in 20 to 50 years of age.[5]
Race
Gender
Developed Countries
- Pericarditis in developed countries is most commonly due to malignancy or viral infection.[6][7][8]
- It usually follows respiratory infections, most commonly echovirus or coxsackie virus.
- In children, it is most commonly caused by adenovirus or coxsackie virus.
- The incidence and prevalence of viral pericarditis vary with season and region.
Developing Countries
- In developing countries pericarditis is usually secondary to tuberculosis or HIV infection.[9][10][11][12]
- Tuberculous pericarditis, caused by Mycobacterium tuberculosis, is found in approximately 1% of all autopsied cases of TB and in 1% to 2% of instances of pulmonary TB. It accounted for 69.5% (162 of 233) of cases referred for diagnostic pericardiocentesis in a study in Western Cape Province of South Africa, while the same accounts for 4% of cases in developed countries.
References
- ↑ Imazio, M; Cecchi, E; Demichelis, B; Chinaglia, A; Ierna, S; Demarie, D; Ghisio, A; Pomari, F; Belli, R; Trinchero, R (2007). “Myopericarditis versus viral or idiopathic acute pericarditis”. Heart. 94 (4): 498–501. doi:10.1136/hrt.2006.104067. ISSN 1355-6037.
- ↑ 2.0 2.1 Kytö, Ville; Sipilä, Jussi; Rautava, Päivi (2014). “Clinical Profile and Influences on Outcomes in Patients Hospitalized for Acute Pericarditis”. Circulation. 130 (18): 1601–1606. doi:10.1161/CIRCULATIONAHA.114.010376. ISSN 0009-7322.
- ↑ Imazio, Massimo; Bobbio, Marco; Cecchi, Enrico; Demarie, Daniela; Demichelis, Brunella; Pomari, Franco; Moratti, Mauro; Gaschino, Gianni; Giammaria, Massimo; Ghisio, Aldo; Belli, Riccardo; Trinchero, Rita (2005). “Colchicine in Addition to Conventional Therapy for Acute Pericarditis”. Circulation. 112 (13): 2012–2016. doi:10.1161/CIRCULATIONAHA.105.542738. ISSN 0009-7322.
- ↑ Imazio, Massimo; Brucato, Antonio; Cemin, Roberto; Ferrua, Stefania; Maggiolini, Stefano; Beqaraj, Federico; Demarie, Daniela; Forno, Davide; Ferro, Silvia; Maestroni, Silvia; Belli, Riccardo; Trinchero, Rita; Spodick, David H.; Adler, Yehuda (2013). “A Randomized Trial of Colchicine for Acute Pericarditis”. New England Journal of Medicine. 369 (16): 1522–1528. doi:10.1056/NEJMoa1208536. ISSN 0028-4793.
- ↑ Ariyarajah, Vignendra; Spodick, David H. (2007). “Acute Pericarditis”. Cardiology in Review. 15 (1): 24–30. doi:10.1097/01.crd.0000210645.89717.34. ISSN 1061-5377.
- ↑ Troughton RW, Asher CR, Klein AL (2004). “Pericarditis”. Lancet. 363 (9410): 717–27. doi:10.1016/S0140-6736(04)15648-1. PMID 15001332.
- ↑ Little WC, Freeman GL (2006). “Pericardial disease”. Circulation. 113 (12): 1622–32. doi:10.1161/CIRCULATIONAHA.105.561514. PMID 16567581.
- ↑ Imazio M, Brucato A, Adler Y, Brambilla G, Artom G, Cecchi E; et al. (2007). “Prognosis of idiopathic recurrent pericarditis as determined from previously published reports”. Am J Cardiol. 100 (6): 1026–8. doi:10.1016/j.amjcard.2007.04.047. PMID 17826391.
- ↑ Sagristà-Sauleda J, Permanyer-Miralda G, Soler-Soler J (1988). “Tuberculous pericarditis: ten year experience with a prospective protocol for diagnosis and treatment”. J Am Coll Cardiol. 11 (4): 724–8. PMID 3351140.
- ↑ Chen Y, Brennessel D, Walters J, Johnson M, Rosner F, Raza M (1999). “Human immunodeficiency virus-associated pericardial effusion: report of 40 cases and review of the literature”. Am Heart J. 137 (3): 516–21. PMID 10047635.
- ↑ Fowler NO (1991). “Tuberculous pericarditis”. JAMA. 266 (1): 99–103. PMID 2046135.
- ↑ Reuter H, Burgess LJ, Doubell AF (2005). “Epidemiology of pericardial effusions at a large academic hospital in South Africa”. Epidemiol Infect. 133 (3): 393–9. PMC 2870262. PMID 15962545.
Natural History, Complications and Prognosis
Pericardial Effusion | Cardiac Tamponade | Constrictive Pericarditis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Varun Kumar, M.B.B.S. Homa Najafi, M.D.[2]
Overview
Pericarditis can lead to the development of pericardial effusion, cardiac tamponade and constrictive pericarditis. Cardiac tamponade, or compression of the heart by fluid in the pericardial sac, reduces the ability of the heart to pump blood. It is a medical emergency that requires urgent pericardiocentesis or a pericardial window. The prognosis depends on the complications of pericarditis, the underlying etiology, and the associated co-morbidities. Pericarditis secondary to malignancy, MI, autoimmune disease and renal failure carries a poor prognosis.
Natural History, Complications, and Prognosis
Natural History
Pericarditis is inflammation of the pericardium, the double-walled sac that contains the heart and the roots of the great vessels. There can be an accompanying accumulation of fluid that can be either serous (free flowing fluid) or fibrinous (an exudate, which is a thick fluid composed of proteins, fibrin strands, inflammatory cells, cell breakdown products, and sometimes bacteria), which leads to development of pericardial effusion and cardiac tamponade. Vascular congestion of the pericardium is also present. The underlying myocardium may or may not be inflamed as well. If the myocardium is involved in the inflammatory process, it is called myopericarditis, and the CK and troponin levels may be elevated. Subsequent scarring of the pericardium may lead to constrictive pericarditis.
Complications
Common complications of pericarditis include:[1]
- Pericardial Effusion
- Many forms of pericarditis can be complicated by significant fluid buildup around the heart, which is known as a pericardial effusion.
- Pericardial Tamponade
- If the fluid accumulates too rapidly or is too large, then cardiac tamponade, a condition in which the heart is compressed by the fluid and cannot pump enough blood forward, may occur. Cardiac tamponade may require urgent intervention including pericardiocentesis or a pericardial window. This complication is more common in patients with specific underlying etiologies such as malignancy, tuberculosis, or purulent pericarditis. It rarely occurs in idiopathic pericarditis.
- Constrictive Pericarditis
- If scarring of the sac around the heart (pericardium) occurs, then this is called constrictive pericarditis which may require surgical stripping of the scar (pericardiectomy).
Prognosis
The prognosis associated with pericarditis depends on the underlying cause and associated condition(s).[2][3][4][5]
- Idiopathic Pericarditis:
- Idiopathic pericarditis is often self-limited and most patients recover in 2 weeks to 3 months. Idiopathic or viral pericarditis is associated with a favorable long-term prognosis with few developing recurrences. Approximately 15-30% of patients with idiopathic acute pericarditis who are not treated with colchicine will develop recurrent pericarditis.
- Post MI Pericarditis or Dressler’s Syndrome:
- Post MI pericarditis is usually associated with larger infarcts, and therefore these patients have a poorer long term prognosis.
- Tuberculous Pericarditis:
- The mortality rate associated with tuberculous pericarditis in the preantibiotic era was 80-90%. The mortality is 17-34% if the tuberculous pericarditis is associated with HIV.
- Traumatic Pericardial Injury:
- In penetrating injuries, pericardial effusion and tamponade may develop rapidly. Early detection and early treatment of cardiac tamponade is associated with a good prognosis. Minor perforations, isolated right ventricular wounds, and a systolic blood pressure more than 50 mm Hg are all associated with better outcomes.
- Malignant Pericarditis:
- Pericarditis associated with malignancy is associated with poorer outcomes and a more complicated course.
- Autoimmune Disease:
- Pericarditis associated with scleroderma and rheumatic fever is associated with worse outcomes.
- Renal Failure:
- Pericarditis associated with renal failure is associated with significant morbidity and may result in hemorrhagic pericarditis.
References
- ↑ Mayosi BM, Burgess LJ, Doubell AF (2005). “Tuberculous pericarditis”. Circulation. 112 (23): 3608–16. doi:10.1161/CIRCULATIONAHA.105.543066. PMID 16330703.
- ↑ Ilan Y, Oren R, Ben-Chetrit E (1991). “Acute pericarditis: etiology, treatment and prognosis. A study of 115 patients”. Jpn Heart J. 32 (3): 315–21. PMID 1920818.
- ↑ Shabetai R (1990). “Acute pericarditis”. Cardiol Clin. 8 (4): 639–44. PMID 2249218.
- ↑ Harvey AM, Whitehill MR. Tuberculous pericarditis. Medicine. 1937; 16: 45–94<ref name=”pmid10908256″>Hakim JG, Ternouth I, Mushangi E, Siziya S, Robertson V, Malin A (2000). “Double blind randomised placebo controlled trial of adjunctive prednisolone in the treatment of effusive tuberculous pericarditis in HIV seropositive patients”. Heart. 84 (2): 183–8. PMC 1760932. PMID 10908256.
- ↑ Nicholls, AJ. Heart and Circulation. In: Handbook of Dialysis, Daugirdas, JT, Ing, TS (Eds), Little, Brown and Co., New York 1994. p.149.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | EKG Examples | Chest X Ray | MRI | CT | Echocardiography | Other Imaging Findings
Treatment
Treatment
Medical Therapy | Pericardiocentesis | Pericardial Window | Pericardial Stripping | Treatment Related Videos
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2] Ahmed Zaghw, M.D. [3] Homa Najafi, M.D.[4] Hafiz M. Ahmed, M.D.[5]
Overview
The management of pericarditis depends on whether the patient has an uncomplicated or complicated disease course. Uncomplicated pericarditis is treated with an NSAID or aspirin combined with colchicine. Aspirin is preferred when concomitant ischemic heart disease is present. For recurrent or incessant pericarditis failing first-line therapy, treatment is guided by phenotype: anti-IL-1 agents (anakinra, rilonacept, goflikicept) are preferred for the inflammatory phenotype, while low-dose corticosteroids are preferred for the noninflammatory phenotype. Cardiac tamponade requires urgent pericardiocentesis. Purulent pericarditis requires antibiotics and drainage.
Management of Uncomplicated Pericarditis
Patients with uncomplicated acute pericarditis can generally be treated and followed up in an outpatient clinic. First-line therapy consists of dual anti-inflammatory treatment with a non-steroidal anti-inflammatory drug (or aspirin) combined with colchicine. Aspirin is the preferred agent when concomitant ischemic heart disease is present. Patients should be observed for gastrointestinal side effects, and a proton-pump inhibitor should be co-prescribed for gastric protection. If the underlying cause of pericarditis is something other than viral or idiopathic, the specific etiology should be treated.[1]
Non-steroidal Anti-inflammatory Drugs (NSAIDs)
- NSAIDs are a mainstay of therapy for uncomplicated pericarditis (viral or idiopathic pericarditis), used in combination with colchicine as dual first-line therapy. The goal of therapy is to reduce pain and inflammation. The preferred NSAID is ibuprofen, dosed at 600 to 800 mg three times daily for days to weeks as needed. Indomethacin 25 to 50 mg three times daily is another option. In order to minimize recurrence, a slow tapering of the NSAID dose guided by symptom resolution and normalization of C-reactive protein (CRP) is recommended rather than abrupt discontinuation. In patients with relative contraindications to NSAIDs (such as heart failure, chronic kidney disease, peptic ulcer disease, bleeding diathesis, or concurrent use of anticoagulants, ACE inhibitors, ARBs, or calcineurin inhibitors), NSAIDs should be prescribed at the lowest effective dose for the shortest duration, and alternatives such as high-dose aspirin should be considered. A proton-pump inhibitor should be co-prescribed for gastric protection. The gastroprotection recommendation is based on several studies that have evaluated factors placing patients at increased risk of gastroduodenal toxicity from NSAIDs.[1][2][3][4]
- The American College of Gastroenterology identified the five most important risk factors for gastroduodenal toxicity:[5]
- Age 60 years (relative risk [RR] 5.52)
- History of an adverse gastroduodenal event (RR 4.76)
- High-dosage NSAIDs (more than twice normal; RR 10.1)
- Concurrent use of glucocorticoids (RR 4.4)
- Concurrent use of anticoagulants (RR 12.7).
Note: Patients with several risk factors are at the highest risk of NSAID-induced gastroduodenal toxicity.
Aspirin Therapy
Aspirin at 500 to 1,000 mg three times daily is a first-line therapy for acute pericarditis, equivalent to ibuprofen. It is the preferred agent when the patient has concomitant ischemic heart disease or is already receiving aspirin for another clinical indication. As with other NSAIDs, a proton-pump inhibitor should be co-prescribed.[1][6]
Post-MI Pericarditis
In pericarditis following acute myocardial infarction, NSAIDs other than aspirin should be avoided since they can impair scar formation.
Failure to Respond to a Week of Traditional Therapy
Failure to respond to NSAIDs within one week (as indicated by persistence of fever, a worsening of symptoms such as chest pain, the development of a new pericardial effusion), likely indicates that the underlying cause may not be viral or idiopathic in nature. These patients may require re-evaluation, observation, and more aggressive therapy as described in the next section.
Colchicine
Colchicine is recommended as adjunctive first-line therapy alongside an NSAID or aspirin for both acute and recurrent pericarditis. The standard dose is 0.6 mg twice daily. For patients weighing less than 70 kg, or those with severe renal or hepatic impairment or gastrointestinal intolerance, the dose should be reduced to 0.6 mg once daily. The recommended duration is 3 months for a first episode and at least 6 months for recurrent pericarditis. Tapering may be considered at the end of the treatment course.
The rate of recurrence after an initial episode is lowered with colchicine therapy by approximately 50% – from 26% to 14% (see Forest plot).[7]

For example, in a multicenter, double-blind trial, the use of colchicine at a dose of 0.5 mg twice daily for 3 months for patients weighing >70 kg or 0.5 mg once daily for patients weighing ≤70 kg in acute pericarditis, when added to conventional antiinflammatory therapy with aspirin or ibuprofen, significantly reduced the rate of symptom persistence at 72 hours (19.2% vs. 40.0%, P=0.001), the number of recurrences per patient (0.21 vs. 0.52, P = 0.001), the hospitalization rate (5.0% vs. 14.2%, P = 0.02), and the remission rate at 1 week (85.0% vs. 58.3%, P<0.001), as compared with placebo.[8]
Colchicine is generally well tolerated, though gastrointestinal side effects (nausea, vomiting, diarrhea, abdominal pain) may require dose reduction or discontinuation in approximately 10% of patients. Dose reductions to 0.3 to 0.6 mg daily should be considered when co-prescribing colchicine with potent inhibitors of P-glycoprotein (P-gp) and/or cytochrome P450 3A4 (CYP3A4), such as clarithromycin, cyclosporine, or certain antifungals, to reduce the risk of toxicity. Alternatively, substituting the interacting medication may allow the full colchicine dose to be maintained. Colchicine is contraindicated in patients with severe renal impairment (creatinine clearance less than 30 mL/min).[1]
Steroids
Corticosteroids are not recommended as first-line therapy for acute pericarditis. While they provide rapid symptom relief, their use during a first episode has been associated with a higher rate of recurrence in observational studies. When corticosteroids are required (such as in patients who are refractory to or intolerant of NSAIDs and colchicine, or in those with autoimmune disease), they should be prescribed at low to moderate doses (prednisone 0.2 to 0.5 mg/kg/day), maintained until clinical remission, and then slowly tapered over several months. Higher doses (such as prednisone 1.0 mg/kg/day) should be avoided due to increased recurrence risk. For patients with recurrent or incessant pericarditis and evidence of systemic inflammation, anti-IL-1 agents are now preferred over corticosteroids as escalation therapy (see Anti-IL-1 Therapy section). Corticosteroids remain the preferred escalation option for patients with a noninflammatory phenotype (normal or near-normal CRP, often autoimmune-related). Prophylaxis for pneumocystis pneumonia and osteoporosis should be considered for patients requiring glucocorticoid doses equivalent to more than 20 mg of prednisone daily for 1 month or longer.[1]
Inflammatory vs. Noninflammatory Phenotype
The treatment approach for pericarditis that fails first-line therapy is guided by the presence or absence of an inflammatory phenotype. The inflammatory phenotype, which accounts for approximately 80% to 90% of cases, is characterized by elevated CRP (greater than 1 mg/dL or 10 mg/L), fever, neutrophilic leukocytosis, and pericardial or pleural effusions. The noninflammatory phenotype, seen in approximately 10% to 20% of cases, is characterized by low or near-normal CRP and is often associated with underlying autoimmune conditions. This distinction is clinically important because anti-IL-1 agents are the preferred escalation therapy for the inflammatory phenotype, whereas low-dose corticosteroids are preferred for the noninflammatory phenotype.[1]
Anti-IL-1 (Interleukin-1) Therapy
Anti-IL-1 agents represent a major advance in the treatment of recurrent and incessant pericarditis. Multiple randomized trials have demonstrated their efficacy in achieving clinical remission, reducing recurrences, and normalizing inflammatory markers in patients with the inflammatory phenotype (elevated CRP greater than 1 mg/dL or 10 mg/L). These agents are now considered the preferred escalation option over corticosteroids for patients who fail first-line dual therapy with NSAIDs and colchicine and who have evidence of systemic inflammation.
Three anti-IL-1 agents have been studied:
- Anakinra (IL-1 receptor antagonist): 1 to 2 mg/kg/day subcutaneously, up to 100 mg/day in adults, for more than 12 months. In the AIRTRIP trial, recurrence occurred in 18% of patients continuing anakinra compared with 90% of those who discontinued it.
- Rilonacept (IL-1 trap): 320 mg subcutaneous loading dose followed by 160 mg weekly, for more than 12 months. Rilonacept is FDA-approved for the treatment and prevention of recurrent pericarditis. In the RHAPSODY trial, recurrence occurred in 6.7% of patients continuing rilonacept versus 74% of those who discontinued it.
- Goflikicept: 80 mg subcutaneously every 2 weeks, for more than 12 months. This agent is not yet available in the United States.
Before initiating anti-IL-1 therapy, patients should be screened for hepatitis B and C, HIV, and tuberculosis. Once established on an anti-IL-1 agent, other anti-inflammatory medications may be sequentially weaned (typically corticosteroids first, then NSAID, then colchicine), although colchicine may sometimes be continued for potential additive benefit. The optimal duration of anti-IL-1 therapy remains uncertain. Recurrence rates are very low while on treatment, but approximately 50% to 75% of patients experience recurrence upon discontinuation. Long-term extension data support treatment beyond 18 months for sustained disease control.[1]
Exercise Restriction
Exercise restriction is recommended for at least 1 month following a pericarditis diagnosis or flare. During this period, maximal heart rate should be kept below 100 beats per minute regardless of the type of physical activity, until clinical remission is achieved. The rationale is that increased heart rate enhances the frequency of friction between the pericardial layers, which can perpetuate inflammation. Athletes should follow the same restriction, with return to competitive activity guided by symptom resolution and normalization of CRP and imaging findings.
Identification of High Risk or Complicated Pericarditis
Patients at high risk of developing complications of pericarditis may require admission to an inpatient service for careful observation and hemodynamic monitoring. High-risk features include:[1]
- High fever (greater than 38°C / 100.4°F) and leukocytosis
- Subacute onset of symptoms (over days to weeks rather than acute)
- Large pericardial effusion (echo-free space greater than 20 mm) resistant to NSAID treatment
- Development of cardiac tamponade
- Concomitant myocarditis (myopericarditis)
- Immunocompromised status
- History of oral anticoagulation therapy
- Pericarditis secondary to acute trauma
- Failure to respond to seven days of NSAID treatment
Management of Complicated Pericarditis
- Pericardiocentesis may be required to treat cardiac tamponade. Pericardiocentesis is generally not recommended for pericardial effusion in the absence of tamponade physiology.
- Antibiotics are required to manage an underlying bacterial infection or a purulent pericarditis.[9]
|
- † Immediate pericardial fluid removal for hemodynamic compromise
- ‡ Modify regimen and narrow coverage based on results of culture and susceptibility tests.
- Antifungals are required to manage an underlying fungal infection, (Histoplasmosis is the most common fungal cause pericarditis associated with histoplasmosis mediastinitis.[10]
|
- Anti-IL-1 agents (anakinra, rilonacept, or goflikicept) are the preferred escalation therapy for recurrent or incessant pericarditis with an inflammatory phenotype (elevated CRP) that fails first-line dual therapy with NSAIDs and colchicine.
- Corticosteroids may be required in patients with autoimmune disease or those with a noninflammatory phenotype (normal or near-normal CRP) who fail first-line therapy. Anti-IL-1 agents are generally preferred over corticosteroids when systemic inflammation is present.
- Colchicine is a component of first-line dual therapy and should be continued as described above.
- Surgery (radical pericardiectomy on cardiopulmonary bypass) may be required in the presence of refractory recurrent pericarditis or constrictive pericarditis. Partial pericardiectomy is not recommended.[1]
Management of Cardiac Tamponade and Large Pericardial Effusion
Pericardiocentesis is an invasive procedure in which the pericardial fluid is drained through a needle. A pericardial window is a surgical procedure to drain fluid form the pericardium. Indications for a pericardiocentesis or a pericardial window include the following:[3]
- Cardiac tamponade
- Large, persistent, symptomatic pericardial effusion
- For diagnostic purposes, if there is suspected purulent, tuberculosis, or neoplastic pericarditis.
Pericardial effusions are classified by echocardiographic size as follows: trivial (less than 1.0 cm, not visible throughout the cardiac cycle), small (less than 1.0 cm), moderate (1.0 to 1.9 cm), large (2.0 to 2.5 cm), and very large (greater than 2.5 cm). Echocardiographic features suggestive of tamponade physiology include diastolic right ventricular collapse (the most specific finding), right atrial inversion lasting more than one-third of the cardiac cycle, dilated inferior vena cava (greater than 2.1 cm) with minimal respiratory variation (sensitive but not specific), and exaggerated respiratory variation in mitral inflow velocities (greater than 30%) and tricuspid inflow velocities (greater than 60%).
Management of Recurrent Pericarditis
- Recurrent pericarditis is defined as a relapse of symptoms after a symptom-free interval of at least 4 to 6 weeks following the initial episode, with completion of medical therapy. Treatment is guided by the inflammatory phenotype.
- First-line therapy consists of an NSAID (aspirin 500 to 1,000 mg three times daily or ibuprofen 600 to 800 mg three times daily) combined with colchicine 0.6 mg twice daily (or 0.6 mg once daily if less than 70 kg or with severe renal/hepatic impairment) for at least 6 months. NSAIDs are started at high dose and tapered after symptom resolution and CRP normalization.
- For patients who fail first-line dual therapy, the treatment approach depends on the phenotype:
- Inflammatory phenotype (elevated CRP, fever, pericardial inflammation on imaging): Anti-IL-1 agents (anakinra, rilonacept, or goflikicept) are the preferred escalation therapy over corticosteroids.
- Noninflammatory phenotype (normal or near-normal CRP, often autoimmune-related): Low-dose corticosteroids (prednisone 0.2 to 0.5 mg/kg/day) are the preferred escalation therapy, maintained until remission and then slowly tapered over months.
- For patients who fail both anti-IL-1 agents and corticosteroids, azathioprine (starting at 1 mg/kg/day, gradually increased to 2 to 3 mg/kg/day) or intravenous immunoglobulin (IVIG, 400 to 500 mg/kg IV daily for 5 days) may be considered.
- Radical pericardiectomy on cardiopulmonary bypass at a high-volume experienced surgical center is a last-resort option for patients who do not respond to pharmacotherapy, have contraindications to medical therapy, or desire pregnancy. Partial pericardiectomy is not recommended. Anti-inflammatory medications may be continued until surgery and for 3 to 6 months postoperatively if active inflammation persists. Most patients will respond to aggressive medical therapy before surgery is needed.[1]
Referral to a Pericardial Diseases Center
Referral to a multidisciplinary Pericardial Diseases Center (PDC) should be considered for patients with recurrent, incessant, or chronic pericarditis; suspected or confirmed constrictive pericarditis; large or complex pericardial effusions requiring drainage; or when advanced therapies such as anti-IL-1 agents or pericardiectomy are being considered. A PDC ideally includes expertise in multimodality imaging (echocardiography, CMR, CT), rheumatology, infectious diseases, genetics, cardiothoracic surgery, and specialty pharmacy.[1]
Bacterial Pericarditis
Antimicrobial Therapy
1. Bacterial Pericarditis
-
- Preferred regimen: Vancomycin 1 g IV q12h targeting trough levels of 15–20 μg/mL for 28 days AND Ciprofloxacin 400 mg IV q12h for 28 days
- Alternative regimen (1): Vancomycin 1 g IV q12h targeting trough levels of 15–20 μg/mL for 28 days AND Cefepime 2 g IV q12h for 28 days
- Alternative regimen (2): Vancomycin 1 g IV q12h targeting trough levels of 15–20 μg/mL for 14–42 days AND Ceftriaxone 2 g IV q24h for 14–42 days
- Note: Pericardiocentesis must be promptly performed. Pericardial drainage combined with effective systemic antibiotic therapy is mandatory (antistaphylococcal agent plus aminoglycoside, followed by tailored antibiotic therapy according to cultures). Frequent irrigation of the pericardial cavity with urokinase or streptokinase may be considered. Open surgical drainage through subxiphoid pericardiotomy is preferable. Pericardiectomy may be required in patients with dense adhesions, loculated and thick purulent effusion, recurrence of tamponade, persistent infection, and progression to constriction.
-
- 1.2.1. Purulent pericarditis with contiguous pneumonia
- Preferred regimen: Vancomycin 1 g IV q12h targeting trough levels of 15–20 μg/mL AND (Ceftriaxone 1–2 g IV q12h OR Cefotaxime 2 g IV q6–8h) AND (Ciprofloxacin 400 mg IV q12h OR Levofloxacin 500–750 mg IV q24h)
- 1.2.2. Purulent pericarditis with contiguous head and neck infection
- Preferred regimen: Imipenem 500 mg IV q6–8h OR Ampicillin-Sulbactam 3 g IV q6h
- 1.2.3. Purulent pericarditis secondary to infective endocarditis
- Preferred regimen: Vancomycin 15–20 mg/kg IV q8–12h targeting trough levels of 15–20 μg/mL AND Gentamicin 3 mg/kg/day IV q8–12h
- 1.2.4. Purulent pericarditis after cardiac surgery, pediatric
- Preferred regimen: Vancomycin 15 mg/kg IV q6h targeting trough levels of 15–20 μg/mL AND (Ceftriaxone 100 mg/kg/day IV q12–24h OR Cefotaxime 200–300 mg/kg/day IV q6–8h) AND Gentamicin 6–7.5 mg/kg/day IV q8h
- 1.2.5. Purulent pericarditis with genitourinary infection, pediatric
- Preferred regimen: Vancomycin 15 mg/kg IV q6h targeting trough levels of 15–20 μg/mL AND (Ceftriaxone 100 mg/kg/day IV q12–24h OR Cefotaxime 200–300 mg/kg/day IV q6–8h) AND Gentamicin 6–7.5 mg/kg/day IV q8h
- 1.2.6. Purulent pericarditis in immunocompromised host, pediatric
- Preferred regimen: Vancomycin 15 mg/kg IV q6h targeting trough levels of 15–20 μg/mL AND (Ceftriaxone 100 mg/kg/day IV q12–24h OR Cefotaxime 200–300 mg/kg/day IV q6–8h) AND Gentamicin 6–7.5 mg/kg/day IV q8h
- 1.3. Pathogen-directed antimicrobial therapy[17]
- 1.3.1. Anaerobes
- Preferred regimen: Clindamycin 600–900 mg IV q8h for 14–42 days OR Metronidazole 7.5 mg/kg IV q6h for 14–42 days OR Ampicillin-Sulbactam 3 g IV q6h for 14–42 days
- 1.3.2. Gram-negative bacilli
- Preferred regimen: Ciprofloxacin 400 mg IV q12h for 14–42 days OR Levofloxacin 500–750 mg IV q24h for 14–42 days OR Cefepime 2 g IV q12h for 14–42 days
- 1.3.3. Legionella pneumophila
- Preferred regimen: Ciprofloxacin 400 mg IV q12h for 14–42 days OR Levofloxacin 500–750 mg IV q24h for 14–42 days OR Azithromycin 500 mg IV q24h for 14–42 days
- 1.3.4. Mycoplasma pneumoniae
- Preferred regimen: Doxycycline 100 mg IV q12h for 14–42 days OR Azithromycin 500 mg IV q24h for 14–42 days
- 1.3.5. Neisseria meningitidis
- Preferred regimen: Penicillin G 5–24 MU/day IM/IV q4–6h for 14–42 days OR Cefotaxime 2 g IV q6–8h for 14–42 days OR Ceftriaxone 2 g IV q24h for 14–42 days
- 1.3.6. Staphylococcus aureus, methicillin-susceptible
- Preferred regimen: Nafcillin 1–2 g IV q4h for 14–42 days OR Oxacillin 1–2 g IV q4h for 14–42 days OR Cefazolin 1–2 g IV q48h for 14–42 days OR Vancomycin 1 g IV q12h targeting trough levels of 15–20 μg/mL for 14–42 days OR Clindamycin 600–900 mg IV q8h for 14–42 days
- 1.3.7. Staphylococcus aureus, methicillin-resistant
- Preferred regimen: Vancomycin 1 g IV q12h targeting trough levels of 15–20 μg/mL for 14–42 days OR Linezolid 600 mg IV q12h for 14–42 days
- 1.3.8. Streptococcus pneumoniae, penicillin-susceptible
- Preferred regimen: Penicillin G 5–24 MU/day IM/IV q4–6h for 14–42 days OR Cefotaxime 2 g IV q6–8h for 14–42 days OR Ciprofloxacin 400 mg IV q12h for 14–42 days OR Levofloxacin 500–750 mg IV q24h for 14–42 days
- 1.3.9. Streptococcus pneumoniae, penicillin-resistant
- Preferred regimen: Ciprofloxacin 400 mg IV q12h for 14–42 days OR Levofloxacin 500–750 mg IV q24h for 14–42 days OR Vancomycin 1 g IV q12h targeting trough levels of 15–20 μg/mL for 14–42 days
2. Tuberculous Pericarditis[18].
- Preferred regimen: (Isoniazid 5 mg/kg (300 mg) PO qd AND Rifampicin 10 mg/kg (600 mg) PO qd AND Pyrazinamide 1,500 mg PO qd AND Ethambutol 1,200 mg PO qd for 2 months) THEN (Rifampicin 10 mg/kg (600 mg) PO qd AND Pyrazinamide 1,500 mg PO qd for 4 months) AND Prednisolone 1–2 mg/kg/day for 5–7 days with slow taper over 6–8 weeks[19].
- Pediatric doses: Isoniazid 10–15 mg/kg (300 mg); Rifampin 10–20 mg/kg (600 mg); Pyrazinamide 15–30 mg/kg (2.0 g); Ethambutol 15–20 mg/kg daily (1.0 g).
- Note: Intrapericardial drainage is done if needed. If constriction develops inspite of medical therapy, pericardiectomy is indicated.
3. Viral pericarditis[18]
- 3.1. CMV pericarditis
- Preferred regimen: Immunoglobulin 1 time per day 4 ml/kg on day 0, 4, and 8; 2 ml/kg on day 12 and 16.
- Note: Symptomatic treatment is given to the patients with viral pericarditis while in large effusions and cardiac tamponade pericardiocentesis is necessary. The use of corticosteroid therapy is contraindicated except in patients with secondary tuberculous pericarditis, as an adjunct to tuberculosis treatment. Drainage, if needed is done.
- 3.2. Coxsackie B pericarditis
- Preferred regimen: Interferon alpha or beta 2,5 Mio. IU/m2 surface area SC 3 times per week
- Note: Symptomatic treatment is given to the patients with viral pericarditis while in large effusions and cardiac tamponade pericardiocentesis is necessary. The use of corticosteroid therapy is contraindicated except in patients with secondary tuberculous pericarditis, as an adjunct to tuberculosis treatment. Drainage, if needed is done.
- 3.3. Adenovirus and parvovirus B19 perimyocarditis
- Preferred regimen: Immunoglobulin 10 g IV at day 1 and 3 for 6–8 hours
- Note: Symptomatic treatment is given to the patients with viral pericarditis while in large effusions and cardiac tamponade pericardiocentesis is necessary. The use of corticosteroid therapy is contraindicated except in patients with secondary tuberculous pericarditis, as an adjunct to tuberculosis treatment. Drainage, if needed is done.
4. Fungal Pericarditis[18]
- Empiric therapy : Fluconazole, Ketoconazole, Itraconazole, Amphotericin B, Liposomal amphotericin B or Amphotericin B lipid complex is indicated.
- 4.1. Histoplasmosis
- Preferred regimen: Nonsteroidal anti-inflammatory drugs given during 2–12 weeks.
- Note: Corticosteroids and NSAIDs can support the treatment with antifungal drugs. Pericardiocentesis or surgical treatment is indicated for haemodynamic impairment. Pericardiectomy is indicated in fungal constrictive pericarditis.
- 4.2. Nocardiosis
- Preferred regimen: Sulfonamides are the drugs of choice.
- Note: Corticosteroids and NSAIDs can support the treatment with antifungal drugs. Pericardiocentesis or surgical treatment is indicated for haemodynamic impairment. Pericardiectomy is indicated in fungal constrictive pericarditis.
- 4.3. Actinomycosis
- Preferred regimen: Combination of three antibiotics including Penicillin.
- Note: Corticosteroids and NSAIDs can support the treatment with antifungal drugs. Pericardiocentesis or surgical treatment is indicated for haemodynamic impairment. Pericardiectomy is indicated in fungal constrictive pericarditis.
2006 ACC/AHA/ESC Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death (DO NOT EDIT)[20]
Pericardial Diseases (DO NOT EDIT)[20]
| Class I |
| “1. Ventricular arrhythmias that develop in patients with pericardial disease should be treated in the same manner that such arrhythmias are treated in patients with other diseases including ICD and pacemaker implantation as required. Patients receiving ICD implantation should be receiving chronic optimal medical therapy and have reasonable expectation of survival with a good functional status for more than 1 year. (Level of Evidence: C)” |
2015 ESC Guidelines on the Diagnosis and Treatment of Pericarditis (DO NOT EDIT)[21]
Recommendations for the management of acute pericarditis
| Class I |
| 1. Hospital admission is recommended for high-risk patients with acute pericarditis (at least one risk factor).
2. Outpatient management is recommended for low-risk patients with acute pericarditis. 3. Evaluation of response to anti-inflammatory therapy is recommended after 1 week. (Level of Evidence: B)[22][23]
|
Recommendations for the treatment of acute pericarditis
| Class I |
| 1. Aspirin or NSAIDs are recommended as first-line therapy for acute pericarditis with gastroprotection.[24]
2. Colchicine is recommended as first-line therapy for acute pericarditis as an adjunct to aspirin/NSAID therapy. (Level of Evidence: A)[25][26][27][28]
|
| Class IIa |
| 1. Serum CRP should be considered to guide the treatment length and assess the response to therapy.
2. Low-dose corticosteroids should be considered for acute pericarditis in cases of contraindication/failure of aspirin/NSAIDs and colchicine, and when an infectious cause has been excluded, or when there is a specific indication such as autoimmune disease. 3. Exercise restriction should be considered for non-athletes with acute pericarditis until resolution of symptoms and normalization of CRP, ECG, and echocardiogram. 4. For athletes, the duration of exercise restriction should be considered until resolution of symptoms and normalization of CRP, ECG, and echocardiogram—at least 3 months is recommended. (Level of Evidence: C)
|
| Class III |
| Corticosteroids are not recommended as first-line therapy for acute pericarditis. (Level of Evidence: C) |
Recommendations for the management of recurrent pericarditis
| Class I |
| 1. Aspirin and NSAIDs are mainstays of treatment and are recommended at full doses, if tolerated, until complete symptom resolution.[24][27]
2. Colchicine (0.5 mg twice daily or 0.5 mg daily for patients, 70 kg or intolerant to higher doses); use for 6 months is recommended as an adjunct to aspirin/NSAIDs.(Level of Evidence: A)[29][30][25][27][28]
|
| Class IIa |
| 1. Colchicine therapy of longer duration (>6 months) should be considered in some cases, according to clinical response.
2. CRP dosage should be considered to guide the treatment duration and assess the response to therapy. 3. After CRP normalization, a gradual tapering of therapies should be considered, tailored to symptoms and CRP, stopping a single class of drugs at a time. 4. Drugs such as IVIG, anakinra, and azathioprine may be considered in cases of corticosteroid-dependent recurrent pericarditis in patients not responsive to Colchicine. 5. Exercise restriction should be considered for non-athletes with recurrent pericarditis until symptom resolution and CRP normalization, taking into account the previous history and clinical conditions. 6. Exercise restriction for a minimum of 3 months should be considered for athletes with recurrent pericarditis until symptom resolution and normalization of CRP, ECG, and echocardiogram. 7. If ischaemic heart disease is a concern or antiplatelet therapy is required, Aspirin should be considered, at medium-high doses (1–2.4 g/day). 8. If symptoms recur during therapy tapering, the management should consider not increasing the dose of corticosteroids to control symptoms, but increasing to the maximum dose of Aspirin or NSAIDs, well distributed, generally every 8 hours, and intravenously if necessary, adding Colchicine and adding analgesics for pain control. (Level of Evidence: C)
|
| Class III |
| Corticosteroid therapy is not recommended as a first-line approach.(Level of Evidence: B)[29][30][25][24][31][32] |
Recommendations for therapy of constrictive pericarditis
| Class I |
| 1. The mainstay of treatment of chronic permanent constriction is pericardiectomy.
2. Medical therapy of specific pericarditis (i.e.tuberculous pericarditis) is recommended to prevent the progression of constriction. (Level of Evidence: C)
|
| Class IIb |
| Empiric anti-inflammatory therapy may be considered in cases with transient or new diagnosis of constriction with concomitant evidence of pericardial inflammation (i.e. CRP elevation or pericardial enhancement on CT/CMR). (Level of Evidence: C) |
Recommendations for the diagnosis and therapy of viral pericarditis
| Class IIa |
| For the definited diagnosis of viral pericarditis, a comprehensive workup of histological, cytological, immunohistological and molecular investigations in pericardial fluid and peri-/epicardial biopsies should be considered. (Level of Evidence: C) |
| Class III |
| 1. Routine viral serology is not recommended, with the possible exception of HIV and HCV.
2. Corticosteroid therapy is not recommended in viral pericarditis. (Level of Evidence: C)
|
Recommendations for the therapy of purulent pericarditis
| Class I |
| 1. Effective pericardial drainage is recommended for purulent pericarditis.
2. Administration of intravenous antibiotics is indicated to treat purulent pericarditis.(Level of Evidence: C) |
| Class IIa |
| 1. Subxiphoid pericardiotomy and rinsing of the pericardial cavity should be considered.
2. Intrapericardial thrombolysis should be considered. 3. Pericardiectomy for dense adhesions, loculated or thick purulent effusion, recurrence of tamponade, persistent infection and progression to constriction should be considered. (Level of Evidence: C)
|
Recommendations for the management of pericarditis in renal failure
| Class IIa |
| 1. Dialysis should be considered in uraemic pericarditis.
2. When patients with adequate dialysis develop pericarditis, intensifying dialysis should be considered. (Level of Evidence: C)
|
| Class IIb |
| 1. Pericardial aspiration and/or drainage may be considered in non-responsive patients with dialysis.
2. NSAIDs and corticosteroids (systemic or intrapericardial) may be considered when intensive dialysis is ineffective.(Level of Evidence: C)
|
| Class III |
| Colchicine is contraindicated in patients with pericarditis and severe renal impairment. (Level of Evidence: C) |
Recommendations for the diagnosis and management of pericarditis associated with myocarditis
| Class I |
| 1. In cases of pericarditis with suspected associated myocarditis, coronary angiography (according to clinical presentation and risk factor assessment) is recommended in order to rule out acute coronary syndromes.
2. Cardiac magnetic resonance is recommended for the confirmation of myocardial involvement. 3. Hospitalization is recommended for diagnosis and monitoring in patients with myocardial involvement. 4. Rest and avoidance of physical activity beyond normal sedentary activities is recommended in non-athletes and athletes with myopericarditis for a period of 6 months. (Level of Evidence: C)
|
| Class IIa |
| Empirical anti-inflammatory therapies (lowest efficacious doses) should be considered to control chest pain. (Level of Evidence: C) |
Recommendations for the prevention and management of radiation pericarditis
| Class I |
| 1. Radiation therapy methods that reduce both the volume and the dose of cardiac irradiation are recommended whenever
possible.(Level of Evidence: C)
|
| Class IIa |
| 1. Pericardiectomy should be considered for radiation-induced constrictive pericarditis, but with a worse outcome than when performed for constrictive pericarditis of other causes, because of co-existing myopathy. (Level of Evidence: B)[33][34][35][36] |
Recommendations for therapy of acute and recurrent pericarditis in children
| Class I |
| 1. NSAIDs at high doses are recommended as first-line therapy for acute pericarditis in children until complete symptom
resolution. (Level of Evidence: C)
|
| Class IIa |
| Colchicine should be considered as an adjunct to anti-inflammatory therapy for acute recurrent pericarditis in children:
<5 years, 0.5 mg/day; >5 years, 1.0–1.5 mg/day in two to three divided doses.(Level of Evidence: C)
|
| Class IIb |
| Anti-IL-1 drugs may be considered in children with recurrent pericarditis and especially when they are corticosteroid
dependent.(Level of Evidence: C)
|
| Class III |
| 1. Aspirin is not recommended in children due to the associated risk of Reye’s syndrome and hepatotoxicity.
2. Corticosteroids are not recommended due to the severity of their side effects in growing children unless there are specific indications such as autoimmune diseases.(Level of Evidence: C)
|
References
- ↑ 1.00 1.01 1.02 1.03 1.04 1.05 1.06 1.07 1.08 1.09 1.10 Tom Kai Ming Wang, MBChB, MD, FACC, Klein MD CM FACC, A., Cremer MD FACC, P., Imazio, M., Facc, S. K. M., Facc, S. A. L., Mardigyan, V., Facc, M. M. M., Mas, K. O. M., Facc, S. V. M., & George F. Wohlford, P. (2025). 2025 Concise Clinical Guidance: An ACC Expert Consensus Statement on the Diagnosis and Management of Pericarditis: A Report of the American College of Cardiology Solution Set Oversight Committee. Journal of the American College of Cardiology. https://doi.org/10.1016/j.jacc.2025.05.023
- ↑ Gabriel, SE.; Jaakkimainen, L.; Bombardier, C. (1991). “Risk for serious gastrointestinal complications related to use of nonsteroidal anti-inflammatory drugs. A meta-analysis”. Ann Intern Med. 115 (10): 787–96. PMID 1834002. Unknown parameter
|month=ignored (help) - ↑ 3.0 3.1 Maisch B, Seferovic PM, Ristic AD, Erbel R, Rienmuller R, Adler Y, Tomkowski WZ, Thiene G, Yacoub MH (2004). “Guidelines on the diagnosis and management of pericardial diseases executive summary; The Task force on the diagnosis and management of pericardial diseases of the European Society of Cardiology”. Eur Heart J. 25 (7): 587–10. doi:10.1016/j.ehj.2004.02.002. PMID 15120056.
- ↑ Imazio, M.; Demichelis, B.; Parrini, I.; Giuggia, M.; Cecchi, E.; Gaschino, G.; Demarie, D.; Ghisio, A.; Trinchero, R. (2004). “Day-hospital treatment of acute pericarditis: a management program for outpatient therapy”. J Am Coll Cardiol. 43 (6): 1042–6. doi:10.1016/j.jacc.2003.09.055. PMID 15028364. Unknown parameter
|month=ignored (help) - ↑ Lanza, FL. (1998). “A guideline for the treatment and prevention of NSAID-induced ulcers. Members of the Ad Hoc Committee on Practice Parameters of the American College of Gastroenterology”. Am J Gastroenterol. 93 (11): 2037–46. doi:10.1111/j.1572-0241.1998.00588.x. PMID 9820370. Unknown parameter
|month=ignored (help) - ↑ Imazio M, Demichelis B, Parrini I, Giuggia M, Cecchi E, Gaschino G, Demarie D, Ghisio A, Trinchero R (2004). “Day-hospital treatment of acute pericarditis: a management program for outpatient therapy”. J Am Coll Cardiol. 43 (6): 1042–6. doi:10.1016/j.jacc.2003.09.055. PMID 15028364.
- ↑ Colchicine for pericarditis: a living systematic review. GitHub. Available at http://openmetaanalysis.github.io/Colchicine-for-Pericarditis/. Accessed November 16, 2014.
- ↑ Imazio, M.; Brucato, A.; Cemin, R.; Ferrua, S.; Maggiolini, S.; Beqaraj, F.; Demarie, D.; Forno, D.; Ferro, S. (2013). “A Randomized Trial of Colchicine for Acute Pericarditis”. N Engl J Med. doi:10.1056/NEJMoa1208536. PMID 23992557. Unknown parameter
|month=ignored (help) - ↑ Parikh, SV.; Memon, N.; Echols, M.; Shah, J.; McGuire, DK.; Keeley, EC. (2009). “Purulent pericarditis: report of 2 cases and review of the literature”. Medicine (Baltimore). 88 (1): 52–65. doi:10.1097/MD.0b013e318194432b. PMID 19352300. Unknown parameter
|month=ignored (help) - ↑ Wheat, LJ.; Freifeld, AG.; Kleiman, MB.; Baddley, JW.; McKinsey, DS.; Loyd, JE.; Kauffman, CA. (2007). “Clinical practice guidelines for the management of patients with histoplasmosis: 2007 update by the Infectious Diseases Society of America”. Clin Infect Dis. 45 (7): 807–25. doi:10.1086/521259. PMID 17806045. Unknown parameter
|month=ignored (help) - ↑ Gilbert, David (2015). The Sanford guide to antimicrobial therapy. Sperryville, Va: Antimicrobial Therapy. ISBN 978-1930808843.
- ↑ Bartlett, John (2012). Johns Hopkins ABX guide : diagnosis and treatment of infectious diseases. Burlington, MA: Jones and Bartlett Learning. ISBN 978-1449625580.
- ↑ Maisch, Bernhard; Seferović, Petar M.; Ristić, Arsen D.; Erbel, Raimund; Rienmüller, Reiner; Adler, Yehuda; Tomkowski, Witold Z.; Thiene, Gaetano; Yacoub, Magdi H.; Task Force on the Diagnosis and Management of Pricardial Diseases of the European Society of Cardiology (2004-04). “Guidelines on the diagnosis and management of pericardial diseases executive summary; The Task force on the diagnosis and management of pericardial diseases of the European society of cardiology”. European Heart Journal. 25 (7): 587–610. doi:10.1016/j.ehj.2004.02.002. ISSN 0195-668X. PMID 15120056. Check date values in:
|date=(help) - ↑ Pankuweit, Sabine; Ristić, Arsen D.; Seferović, Petar M.; Maisch, Bernhard (2005). “Bacterial pericarditis: diagnosis and management”. American Journal of Cardiovascular Drugs: Drugs, Devices, and Other Interventions. 5 (2): 103–112. ISSN 1175-3277. PMID 15725041.
- ↑ Goodman, null (2000-08). “Purulent Pericarditis”. Current Treatment Options in Cardiovascular Medicine. 2 (4): 343–350. ISSN 1092-8464. PMID 11096539. Check date values in:
|date=(help) - ↑ Cherry, James (2014). Feigin and Cherry’s textbook of pediatric infectious diseases. Philadelphia, PA: Elsevier/Saunders. ISBN 978-1455711772.
- ↑ Bartlett, John (2012). Johns Hopkins ABX guide : diagnosis and treatment of infectious diseases. Burlington, MA: Jones and Bartlett Learning. ISBN 978-1449625580.
- ↑ 18.0 18.1 18.2 Maisch B, Seferović PM, Ristić AD, Erbel R, Rienmüller R, Adler Y; et al. (2004). “Guidelines on the diagnosis and management of pericardial diseases executive summary; The Task force on the diagnosis and management of pericardial diseases of the European society of cardiology”. Eur Heart J. 25 (7): 587–610. doi:10.1016/j.ehj.2004.02.002. PMID 15120056.
- ↑ Blumberg HM, Burman WJ, Chaisson RE, Daley CL, Etkind SC, Friedman LN; et al. (2003). “American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America: treatment of tuberculosis”. Am J Respir Crit Care Med. 167 (4): 603–62. doi:10.1164/rccm.167.4.603. PMID 12588714.
- ↑ 20.0 20.1 Zipes DP, Camm AJ, Borggrefe M, Buxton AE, Chaitman B, Fromer M; et al. (2006). “ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: a report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (writing committee to develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society”. Circulation. 114 (10): e385–484. doi:10.1161/CIRCULATIONAHA.106.178233. PMID 16935995.
- ↑ Adler, Yehuda; Charron, Philippe; Imazio, Massimo; Badano, Luigi; Barón-Esquivias, Gonzalo; Bogaert, Jan; Brucato, Antonio; Gueret, Pascal; Klingel, Karin; Lionis, Christos; Maisch, Bernhard; Mayosi, Bongani; Pavie, Alain; Ristić, Arsen D.; Sabaté Tenas, Manel; Seferovic, Petar; Swedberg, Karl; Tomkowski, Witold (2015). “2015 ESC Guidelines for the diagnosis and management of pericardial diseases”. European Heart Journal. 36 (42): 2921–2964. doi:10.1093/eurheartj/ehv318. ISSN 0195-668X.
- ↑ Imazio, Massimo; Demichelis, Brunella; Parrini, Iris; Giuggia, Marco; Cecchi, Enrico; Gaschino, Gianni; Demarie, Daniela; Ghisio, Aldo; Trinchero, Rita (2004). “Day-hospital treatment of acute pericarditis”. Journal of the American College of Cardiology. 43 (6): 1042–1046. doi:10.1016/j.jacc.2003.09.055. ISSN 0735-1097.
- ↑ Imazio, Massimo; Cecchi, Enrico; Demichelis, Brunella; Ierna, Salvatore; Demarie, Daniela; Ghisio, Aldo; Pomari, Franco; Coda, Luisella; Belli, Riccardo; Trinchero, Rita (2007). “Indicators of Poor Prognosis of Acute Pericarditis”. Circulation. 115 (21): 2739–2744. doi:10.1161/CIRCULATIONAHA.106.662114. ISSN 0009-7322.
- ↑ 24.0 24.1 24.2 Lotrionte, Marzia; Biondi-Zoccai, Giuseppe; Imazio, Massimo; Castagno, Davide; Moretti, Claudio; Abbate, Antonio; Agostoni, Pierfrancesco; Brucato, Antonio L.; Di Pasquale, Pietro; Raatikka, Marja; Sangiorgi, Giuseppe; Laudito, Antonio; Sheiban, Imad; Gaita, Fiorenzo (2010). “International collaborative systematic review of controlled clinical trials on pharmacologic treatments for acute pericarditis and its recurrences”. American Heart Journal. 160 (4): 662–670. doi:10.1016/j.ahj.2010.06.015. ISSN 0002-8703.
- ↑ 25.0 25.1 25.2 Imazio, Massimo; Bobbio, Marco; Cecchi, Enrico; Demarie, Daniela; Demichelis, Brunella; Pomari, Franco; Moratti, Mauro; Gaschino, Gianni; Giammaria, Massimo; Ghisio, Aldo; Belli, Riccardo; Trinchero, Rita (2005). “Colchicine in Addition to Conventional Therapy for Acute Pericarditis”. Circulation. 112 (13): 2012–2016. doi:10.1161/CIRCULATIONAHA.105.542738. ISSN 0009-7322.
- ↑ Imazio, Massimo; Brucato, Antonio; Cemin, Roberto; Ferrua, Stefania; Maggiolini, Stefano; Beqaraj, Federico; Demarie, Daniela; Forno, Davide; Ferro, Silvia; Maestroni, Silvia; Belli, Riccardo; Trinchero, Rita; Spodick, David H.; Adler, Yehuda (2013). “A Randomized Trial of Colchicine for Acute Pericarditis”. New England Journal of Medicine. 369 (16): 1522–1528. doi:10.1056/NEJMoa1208536. ISSN 0028-4793.
- ↑ 27.0 27.1 27.2 Imazio, Massimo; Brucato, Antonio; Belli, Riccardo; Forno, Davide; Ferro, Silvia; Trinchero, Rita; Adler, Yehuda (2014). “Colchicine for the prevention of pericarditis”. Journal of Cardiovascular Medicine. 15 (12): 840–846. doi:10.2459/JCM.0000000000000103. ISSN 1558-2027.
- ↑ 28.0 28.1 Alabed, Samer; Cabello, Juan B; Irving, Greg J; Qintar, Mohammed; Burls, Amanda (2014). “Colchicine for pericarditis”. Cochrane Database of Systematic Reviews. doi:10.1002/14651858.CD010652.pub2. ISSN 1465-1858.
- ↑ 29.0 29.1 Imazio, Massimo (2011). “Colchicine for Recurrent Pericarditis (CORP)”. Annals of Internal Medicine. 155 (7): 409. doi:10.7326/0003-4819-155-7-201110040-00359. ISSN 0003-4819.
- ↑ 30.0 30.1 Imazio, Massimo; Belli, Riccardo; Brucato, Antonio; Cemin, Roberto; Ferrua, Stefania; Beqaraj, Federico; Demarie, Daniela; Ferro, Silvia; Forno, Davide; Maestroni, Silvia; Cumetti, Davide; Varbella, Ferdinando; Trinchero, Rita; Spodick, David H; Adler, Yehuda (2014). “Efficacy and safety of colchicine for treatment of multiple recurrences of pericarditis (CORP-2): a multicentre, double-blind, placebo-controlled, randomised trial”. The Lancet. 383 (9936): 2232–2237. doi:10.1016/S0140-6736(13)62709-9. ISSN 0140-6736.
- ↑ Imazio, Massimo; Brucato, Antonio; Cumetti, Davide; Brambilla, Giovanni; Demichelis, Brunella; Ferro, Silvia; Maestroni, Silvia; Cecchi, Enrico; Belli, Riccardo; Palmieri, Giancarlo; Trinchero, Rita (2008). “Corticosteroids for Recurrent Pericarditis”. Circulation. 118 (6): 667–671. doi:10.1161/CIRCULATIONAHA.107.761064. ISSN 0009-7322.
- ↑ Imazio, Massimo; Brucato, Antonio; Adler, Yehuda; Brambilla, Giovanni; Artom, Galit; Cecchi, Enrico; Palmieri, Giancarlo; Trinchero, Rita (2007). “Prognosis of Idiopathic Recurrent Pericarditis as Determined from Previously Published Reports”. The American Journal of Cardiology. 100 (6): 1026–1028. doi:10.1016/j.amjcard.2007.04.047. ISSN 0002-9149.
- ↑ Bertog, Stefan C.; Thambidorai, Senthil K.; Parakh, Kapil; Schoenhagen, Paul; Ozduran, Volkan; Houghtaling, Penny L.; Lytle, Bruce W.; Blackstone, Eugene H.; Lauer, Michael S.; Klein, Allan L. (2004). “Constrictive pericarditis: etiology and cause-specific survival after pericardiectomy”. Journal of the American College of Cardiology. 43 (8): 1445–1452. doi:10.1016/j.jacc.2003.11.048. ISSN 0735-1097.
- ↑ DeValeria, Patrick A.; Baumgartner, William A.; Casale, Alfred S.; Greene, Peter S.; Cameron, Duke E.; Gardner, Timothy J.; Gott, Vincent L.; Watkins, Levi; Reitz, Bruce A. (1991). “Current indications, risks, and outcome after pericardiectomy”. The Annals of Thoracic Surgery. 52 (2): 219–224. doi:10.1016/0003-4975(91)91339-W. ISSN 0003-4975.
- ↑ Komoda, Takeshi; Frumkin, Alexander; Knosalla, Christoph; Hetzer, Roland (2013). “Child-Pugh Score Predicts Survival After Radical Pericardiectomy for Constrictive Pericarditis”. The Annals of Thoracic Surgery. 96 (5): 1679–1685. doi:10.1016/j.athoracsur.2013.06.016. ISSN 0003-4975.
- ↑ Ling, Lieng H.; Oh, Jae K.; Schaff, Hartzell V.; Danielson, Gordon K.; Mahoney, Douglas W.; Seward, James B.; Tajik, A. Jamil (1999). “Constrictive Pericarditis in the Modern Era”. Circulation. 100 (13): 1380–1386. doi:10.1161/01.CIR.100.13.1380. ISSN 0009-7322.
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH