
Allergic colitis
For the main page on colitis, please click here
For more information on infectious colitis, please click here
For more information on ischemic colitis, please click here
For more information on chemical colitis, please click here
For more information on drug-induced colitis, please click here
For more information on radiation colitis, please click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Qasim Salau, M.B.B.S., FMCPaed [2]
Synonyms and keywords: Eosinophilic proctocolitis, Eosinophilic colitis, Food protein-induced protocolitis, Food protein-induced colitis, FPIES, Food protein-induced enterocolitis syndrome, FPIAP, Food protein-induced allergic proctocolitis
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Qasim Salau, M.B.B.S., FMCPaed [2]
Overview
Allergic colitis is a non IgE immunological reaction against food protein antigens, particularly cow-milk and soy proteins. The exact mechanism is not known. It usually develops insidiously, and is believed to be T-cell mediated. Allergic colitis is most commonly caused by allergy to cow’s milk protein. Symptoms and signs of allergic colitis are non-specific and observed in other causes of colitis and some systemic diseases. Detailed history and physical examination is needed to make the diagnosis. In addition, endoscopy with biopsy may be required to confirm the diagnosis. The exact prevalence of allergic colitis is unknown. Allergic colitis typically develops in early infancy. Allergic colitis is benign, resolving completely in most children without any sequelae. The most common symptoms of allergic colitis is passage of blood streaked stool in an otherwise healthy young infant. There are no specific laboratory findings that are pathognomonic of allergic colitis. Laboratory studies should therefore be correlated with a carefully taken history and a detailed physical examination. Presence of eosinophils in the stool is suggestive of allergic colitis in the presence of typical clinical findings. The mainstay of treatment of allergic colitis is dietary management. Medical therapy includes allergen avoidance, treatment of severe manifestations of the allergy, and eventual reintroduction of the allergy into the diet.
Historical Perspective
Allergic colitis was first described by Kaijser in 1937. Allergic proctocolitis was described by Rubin in 1940. In the 1960s, Gryboski subsequently described proctocolitis and enterocolitis.
Classification
Allergic colitis can be classified into two subtypes based on the anatomical site involved, proctocolitis and enterocolitis. Allergic colitis manifests more commonly as proctocolitis. It is also more common among infants.
Pathophysiology
Allergic colitis is a non IgE immunological reaction against food protein antigens, particularly cow-milk and soy proteins. The exact mechanism is not known. It usually develops insidiously, and is believed to be T-cell mediated. The activated T-cells lead to recruitment of eosinophils and other polymorphonuclear cells into the intestinal tract, which then cause intestinal inflammation and damage. Some of these children may later develop specific IgE. Genetic influence may also play a role, since disease is sometimes present within families. On gross pathology, there is evidence of inflammation with ulcers and friable, erythematous mucosa. On microscopy, the mucosa architecture is preserved with eosinophil infiltrates.
Causes
Allergic colitis is most commonly caused by allergy to cow’s milk protein. 20-40% of patients with allergic colitis have allergies to both cow’s milk protein and soy protein.
Differential Diagnosis
Symptoms and signs of allergic colitis are non-specific and observed in other causes of colitis and some systemic diseases. Detailed history and physical examination is needed to make the diagnosis. In addition, endoscopy with biopsy may be required to confirm the diagnosis. In infancy, allergic colitis must particularly be differentiated from necrotizing enterocolitis, infectious colitis, anal fissure, intussusception, and volvulus. In adolescent and adults, allergic colitis must be differentiated from inflammatory bowel disease, infectious colitis, and colorectal malignancy.
Epidemiology and Demographics
The exact prevalence of allergic colitis is unknown. Prevalence of food protein-induced allergic proctocolitis (FPIAP) has been reported to range from a low of 16% to a high of 64% among infants with rectal bleeding. FPIAP is the most common cause of non-infectious colitis in infancy. Allergic colitis is mainly a disease of infants, with onset usually in the first two to three months of life. There is a slight male predominance (50–61.6%) for allergic colitis.
Risk Factors
Risk factors for allergic colitis include family history of atopy and previous sibling with IgE mediated food allergy.
Screening
Screening is not recommended for allergic colitis.
Natural History, Complications, and Prognosis
Allergic colitis typically develops in early infancy. Allergic colitis is benign, resolving completely in most children without any sequelae. The infants with food protein-induced allergic proctocolitis are usually on exclusive breastfeeding while those with food protein-induced enterocolitis syndrome are often on infant formula. If left untreated, spontaneous resolution may occur in 20% of the children with allergic colitis without elimination of the triggering food. Most infants with allergic colitis will tolerate the offending food by 1 to 3 years of age.
Diagnosis
History and Symptoms
The most common symptoms of allergic colitis is passage of blood streaked stool in an otherwise healthy young infant especially in FPIAP. History of failure to thrive may also be gotten in the infant with FPIES. There may be a family history of allergy.
Physical Examination
Patients with allergic colitis may appear well in the case of FPIAP or may appear lethargic when they have FPIES. Physical examination of patients with FPIES is usually remarkable for signs of dehydration, pallor, and poor weight.
Laboratory Findings
There are no specific laboratory findings that are pathognomonic of allergic colitis. Laboratory studies should therefore be correlated with a carefully taken history and a detailed physical examination. Presence of eosinophils in the stool is suggestive of allergic colitis in the presence of typical clinical findings.
Imaging Findings
X Ray
There are no diagnostic x ray findings associated with allergic colitis.
CT
There are no diagnostic CT findings associated with allergic colitis.
MRI
There are no diagnostic MRI findings associated with allergic colitis.
Ultrasound
There are no diagnostic ultrasound findings associated with allergic colitis.
Other Imaging Findings
Other imaging studies for allergic colitis include endoscopy. Endoscopy is not recommended in the routine diagnosis of allergic colitis. Endoscopy is usually required for atypical presentation in addition to detailed clinical assessment. The lesions in allergic colitis are most often observed in the the rectosigmoid area. Gross endoscopic findings associated with allergic colitis include; focal or diffuse erythema, edematous and friable mucosa, with nodular hyperplasia and/ or ulcerations. Characteristic circumscribed central pit-like erosions may also be observed.
Other Diagnostic Studies
There are no additional diagnostic studies associated with allergic colitis.
Treatment
Medical Therapy
The mainstay of treatment of allergic colitis is dietary management. Medical therapy includes allergen avoidance, treatment of severe manifestations of the allergy, and eventual reintroduction of the allergy into the diet.
Surgery
There is no indication for surgical intervention in allergic colitis.
Primary Prevention
There are presently no established methods to prevent allergic colitis.
Secondary Prevention
There are presently no secondary preventive measures for allergic colitis. However, it is important to avoid food allergens identified in the individual until tolerance has been demonstrated.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Qasim Salau, M.B.B.S., FMCPaed [2]
Overview
Allergic colitis was first described by Kaijser in 1937. Allergic proctocolitis was described by Rubin in 1940. In the 1960s, Gryboski subsequently described proctocolitis and enterocolitis.
Historical Perspective
- Allergic colitis was first described by Kaijser in 1937.[1][2]
- In 1940, Rubin also described allergic proctocolitis.[2][3]
- In 1966 and 1967, Gryboski published the first case series of cow milk induced colitis in neonates.[4][5][6]
- In the 1970s, Powell described food induced enterocolitis following cow milk and soy milk introduction in young infants.[4][7][8]
- Gryboski and Powell described acute severe symptoms following re-exposure to cow milk formula after an initial period of avoidance.[4]
- In 1982, McDonald et al. first used the term food induced enterocolitis (FIE) to describe cow milk/soy protein induced enterocolitis and subsequently modified the nomenclature in 1984 to food protein-induced enterocolitis (FPIE).[4][9]
- In 1998, Sicherer et al. suggested food protein-induced enterocolitis be called a syndrome, recognizing the disease was characterized by a constellation of shared clinical and laboratory features.[4][10]
References
- ↑ Behjati S, Zilbauer M, Heuschkel R, Phillips A, Salvestrini C, Torrente F; et al. (2009). “Defining eosinophilic colitis in children: insights from a retrospective case series”. J Pediatr Gastroenterol Nutr. 49 (2): 208–15. doi:10.1097/MPG.0b013e31818de373. PMID 19525875.
- ↑ 2.0 2.1 Lozinsky AC, Morais MB (2014). “Eosinophilic colitis in infants”. J Pediatr (Rio J). 90 (1): 16–21. doi:10.1016/j.jped.2013.03.024. PMID 24131740.
- ↑ Katz Y, Goldberg MR (2014). “Natural history of food protein-induced enterocolitis syndrome”. Curr Opin Allergy Clin Immunol. 14 (3): 229–39. doi:10.1097/ACI.0000000000000053. PMC 4011630. PMID 24686278.
- ↑ 4.0 4.1 4.2 4.3 4.4 Mehr S, Frith K, Campbell DE (2014). “Epidemiology of food protein-induced enterocolitis syndrome”. Curr Opin Allergy Clin Immunol. 14 (3): 208–16. doi:10.1097/ACI.0000000000000056. PMC 4011623. PMID 24686277.
- ↑ Gryboski JD, Burkle F, Hillman R (1966). “Milk induced colitis in an infant”. Pediatrics. 38 (2): 299–302. PMID 5952833.
- ↑ Gryboski JD (1967). “Gastrointestinal milk allergy in infants”. Pediatrics. 40 (3): 354–62. PMID 6071957.
- ↑ Powell GK (1976). “Enterocolitis in low-birth-weight infants associated with milk and soy protein intolerance”. J Pediatr. 88 (5): 840–4. PMID 944766.
- ↑ Powell GK (1978). “Milk- and soy-induced enterocolitis of infancy. Clinical features and standardization of challenge”. J Pediatr. 93 (4): 553–60. PMID 568171.
- ↑ McDonald PJ, Goldblum RM, Van Sickle GJ, Powell GK (1984). “Food protein-induced enterocolitis: altered antibody response to ingested antigen”. Pediatr Res. 18 (8): 751–5. PMID 6540862.
- ↑ Sicherer SH, Eigenmann PA, Sampson HA (1998). “Clinical features of food protein-induced enterocolitis syndrome”. J Pediatr. 133 (2): 214–9. PMID 9709708.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Qasim Salau, M.B.B.S., FMCPaed [2]
Overview
Allergic colitis can be classified into two subtypes based on the anatomical site involved, proctocolitis and enterocolitis. Allergic colitis manifests more commonly as proctocolitis. It is also more common among infants.
Classification
Based on the anatomical area involved, allergic colitis may be classified into:[1][2][3]
- Food protein-induced allergic proctocolitis (FPIAP)
- Food protein-induced enterocolitis syndrome (FPIES)
Based on age, allergic colitis can be classified into:[2]
- Infantile
- Adolescent/Adult
Based on immune mechanism, it can be classified into:[2][4]
- Atopic (IgE mediated)
- Non atopic (non-IgE mediated)
Based on the duration of symptoms and presentation, allergic colitis may be classified into:[1]
- Acute: Minutes to few hours after coming in ingesting the offending protein.
- Chronic: Weeks after ingesting the offending protein. Presentation is due to accumulative effect of the protein.
References
- ↑ 1.0 1.1 Nowak-Węgrzyn A (2015). “Food protein-induced enterocolitis syndrome and allergic proctocolitis”. Allergy Asthma Proc. 36 (3): 172–84. doi:10.2500/aap.2015.36.3811. PMC 4405595. PMID 25976434.
- ↑ 2.0 2.1 2.2 Alfadda AA, Storr MA, Shaffer EA (2011). “Eosinophilic colitis: epidemiology, clinical features, and current management”. Therap Adv Gastroenterol. 4 (5): 301–9. doi:10.1177/1756283X10392443. PMC 3165205. PMID 21922029.
- ↑ Boyce JA, Assa’ad A, Burks AW, Jones SM, Sampson HA, Wood RA; et al. (2010). “Guidelines for the Diagnosis and Management of Food Allergy in the United States: Summary of the NIAID-Sponsored Expert Panel Report”. J Allergy Clin Immunol. 126 (6): 1105–18. doi:10.1016/j.jaci.2010.10.008. PMC 4241958. PMID 21134568.
- ↑ Rothenberg ME (2004). “Eosinophilic gastrointestinal disorders (EGID)”. J Allergy Clin Immunol. 113 (1): 11–28, quiz 29. doi:10.1016/j.jaci.2003.10.047. PMID 14713902.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Qasim Salau, M.B.B.S., FMCPaed [2]
Overview
Allergic colitis is a non IgE immunological reaction against food protein antigens, particularly cow-milk and soy proteins. The exact mechanism is not known. It usually develops insidiously, and is thought to be T cell mediated. The activated T cells lead to recruitment of eosinophils and other polymorphonuclear cells into the intestinal tract, which then cause intestinal inflammation and damage. Some of these children may later develop specific IgE. Genetic influence may also play a role, since disease is sometimes present within families. On gross pathology, there is evidence of inflammation, with ulcers and friable, erythematous mucosa. On microscopy, the mucosa architecture is preserved with eosinophil infiltrates.
Pathophysiology
The exact pathophysiologic mechanism by which allergic colitis develops is not fully understood.
Pathogenesis
- It is a non-IgE immunological reaction against food protein antigens, which is thought to be T cell mediated.[1][2][3][4][5]
- Activation of T cells (CD8 and Th2) results in release of inflammatory cytokines TNF-α, and decreased expression of TGF-β in the intestinal mucosa, attracting polymorphonuclear cells (PMN) including eosinophils to the intestinal tract, subsequently causing intestinal inflammation and damage.[6]
- Autoimmunity may play a role in the pathogenesis. Atypical perinuclear antineutrophil cytoplasmic antibodies (a-pANCA) have been found in some of the infants, with intestinal infiltration by neutrophils.[7]
- Specific IgE antibodies against food proteins have been demonstrated in 4 to 24% the children suggesting a role in the pathogenesis of allergic colitis. These antibodies developed over time.[8][9]
Genetics
Allergic colitis is sometimes observed within families, suggesting genetic predisposition may play a role in the pathogenesis.[7]
Gross Pathology
- Gross pathological findings are predominantly in the rectosigmoid region in patients with allergic colitis. The lesions are diffuse or patchy with or without necrosis, ulcers, abscesses within the crypts and hemorrhage. The mucosa is erythematous and friable. Nodular hyperplasia with characteristic circumscribed central pit-like erosions and ulcers may also be observed.[10][11][12]
Microscopic Pathology
- Allergic colitis is characterized by marked eosinophil infiltrates (≥ 60/10 HPF) in the mucosa (especially the lamina propria) of the involved area.[10][11][13]
- Typically, the mucosa architecture is preserved on microscopy.[10][11]
-
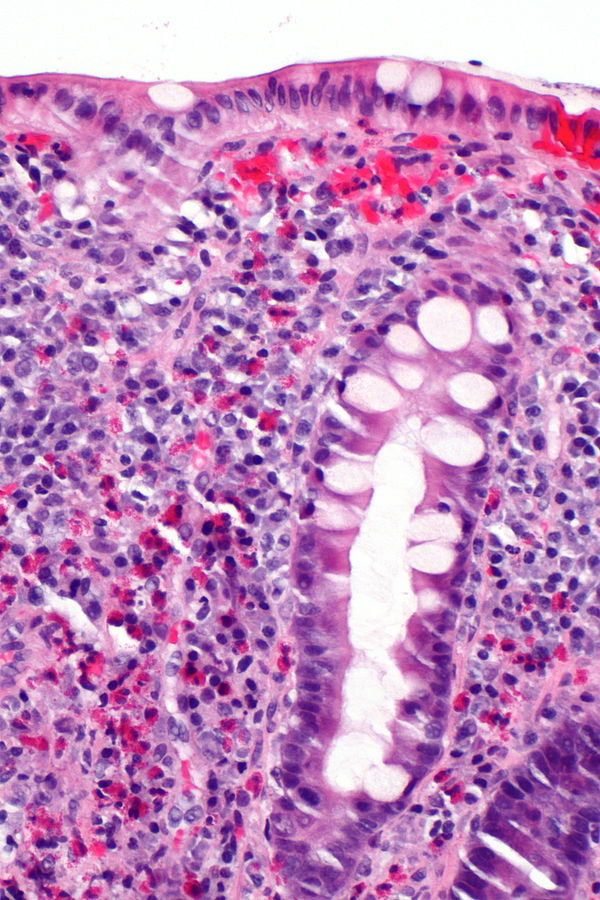 Allergic colitis. H and E stain showing abundant eosinophils – By Nephron – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=30671091
Allergic colitis. H and E stain showing abundant eosinophils – By Nephron – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=30671091

References
- ↑ Pumberger W, Pomberger G, Geissler W (2001). “Proctocolitis in breast fed infants: a contribution to differential diagnosis of haematochezia in early childhood”. Postgrad Med J. 77 (906): 252–4. PMC 1741985. PMID 11264489.
- ↑ Lucarelli S, Di Nardo G, Lastrucci G, D’Alfonso Y, Marcheggiano A, Federici T; et al. (2011). “Allergic proctocolitis refractory to maternal hypoallergenic diet in exclusively breast-fed infants: a clinical observation”. BMC Gastroenterol. 11: 82. doi:10.1186/1471-230X-11-82. PMC 3224143. PMID 21762530.
- ↑ Chesworth BM, Hamilton CB, Walton DM, Benoit M, Blake TA, Bredy H; et al. (2014). “Reliability and validity of two versions of the upper extremity functional index”. Physiother Can. 66 (3): 243–53. doi:10.3138/ptc.2013-45. PMC 4130402. PMID 25125777.
- ↑ Academy of Breastfeeding Medicine (2011). “ABM Clinical Protocol #24: Allergic Proctocolitis in the Exclusively Breastfed Infant”. Breastfeed Med. 6 (6): 435–40. doi:10.1089/bfm.2011.9977. PMID 22050274.
- ↑ Fagundes-Neto U, Ganc AJ (2013). “Allergic proctocolitis: the clinical evolution of a transitory disease with a familial trend. Case reports”. Einstein (Sao Paulo). 11 (2): 229–33. PMC 4872900. PMID 23843067.
- ↑ Feuille E, Nowak-Węgrzyn A (2014). “Definition, etiology, and diagnosis of food protein-induced enterocolitis syndrome”. Curr Opin Allergy Clin Immunol. 14 (3): 222–8. doi:10.1097/ACI.0000000000000055. PMC 4011631. PMID 24686276.
- ↑ 7.0 7.1 Sekerkova A, Fuchs M, Cecrdlova E, Svachova V, Kralova Lesna I, Striz I; et al. (2015). “High Prevalence of Neutrophil Cytoplasmic Autoantibodies in Infants with Food Protein-Induced Proctitis/Proctocolitis: Autoimmunity Involvement?”. J Immunol Res. 2015: 902863. doi:10.1155/2015/902863. PMC 4592904. PMID 26484355.
- ↑ Nowak-Węgrzyn A (2015). “Food protein-induced enterocolitis syndrome and allergic proctocolitis”. Allergy Asthma Proc. 36 (3): 172–84. doi:10.2500/aap.2015.36.3811. PMC 4405595. PMID 25976434.
- ↑ Caubet JC, Ford LS, Sickles L, Järvinen KM, Sicherer SH, Sampson HA; et al. (2014). “Clinical features and resolution of food protein-induced enterocolitis syndrome: 10-year experience”. J Allergy Clin Immunol. 134 (2): 382–9. doi:10.1016/j.jaci.2014.04.008. PMID 24880634.
- ↑ 10.0 10.1 10.2 Odze RD, Wershil BK, Leichtner AM, Antonioli DA (1995). “Allergic colitis in infants”. J Pediatr. 126 (2): 163–70. PMID 7844660.
- ↑ 11.0 11.1 11.2 Hwang JB, Hong J (2013). “Food protein-induced proctocolitis: Is this allergic disorder a reality or a phantom in neonates?”. Korean J Pediatr. 56 (12): 514–8. doi:10.3345/kjp.2013.56.12.514. PMC 3885785. PMID 24416045.
- ↑ Hwang JB, Park MH, Kang YN, Kim SP, Suh SI, Kam S (2007). “Advanced criteria for clinicopathological diagnosis of food protein-induced proctocolitis”. J Korean Med Sci. 22 (2): 213–7. doi:10.3346/jkms.2007.22.2.213. PMC 2693584. PMID 17449926.
- ↑ Schmoldt A, Benthe HF, Haberland G (1975). “Digitoxin metabolism by rat liver microsomes”. Biochem Pharmacol. 24 (17): 1639–41. PMID http://dx.doi.org/10.1016/S0022-3476(95)70540-6 Check
|pmid=value (help).
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Qasim Salau, M.B.B.S., FMCPaed [2]
Overview
Allergic colitis is most commonly caused by allergy to cow’s milk protein. 20-40% of patients with allergic colitis have allergies to both cow’s milk protein and soy protein.
Causes
The most common cause of allergic colitis is cow’s milk protein allergy, which accounts for 50% to 65% of reports. Cow’s milk protein and soy protein together account for about 75% of the causes.[1][2] Other causes include:
References
- ↑ Lake AM (2000). “Food-induced eosinophilic proctocolitis”. J Pediatr Gastroenterol Nutr. 30 Suppl: S58–60. PMID 10634300.
- ↑ Lucarelli S, Di Nardo G, Lastrucci G, D’Alfonso Y, Marcheggiano A, Federici T; et al. (2011). “Allergic proctocolitis refractory to maternal hypoallergenic diet in exclusively breast-fed infants: a clinical observation”. BMC Gastroenterol. 11: 82. doi:10.1186/1471-230X-11-82. PMC 3224143. PMID 21762530.
Differentiating Allergic proctocolitis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Qasim Salau, M.B.B.S., FMCPaed [2]
Overview
Symptoms and signs of allergic colitis are non-specific and observed in other causes of colitis and some systemic diseases. Detailed history and physical examination is needed to make the diagnosis. In addition, endoscopy with biopsy may be required to confirm the diagnosis. In infancy, allergic colitis must particularly be differentiated from necrotizing enterocolitis, infectious colitis, anal fissure, intussusception, and volvulus. In adolescent and adults, allergic colitis must be differentiated from inflammatory bowel disease, infectious colitis, and colorectal malignancy.
Differentiating Allergic Colitis from Other Diseases
The differential diagnosis of allergic colitis can be classified into two according to age group.
Differential Diagnosis in Infants
- Swallowed maternal blood syndrome
- Anorectal fissure
- Necrotizing enterocolitis especially in preterm babies
- Vitamin K deficiency hemorrhage
- Other coagulopathies (hereditary such as coagulation factor deficiency or acquired such as liver disease with clotting factor deficiency)
- Intussusception
- Infectious colitis
- Hirschsprung disease complicated by enterocolitis
- Volvulus
- Inflammatory bowel disease (early onset)
- Meckel diverticulum
- Dermatitis
- Gastrointestinal duplication cyst
- Vascular malformations
- Gastro-duodenal ulcers
- Lymphonodular hyperplasia
Differential Ddiagnosis in Adolescent/Adult
- Inflammatory bowel disease
- Behcet’s disease
- Arteriovenous malformation
- Diverticulosis
- Infectious colitis
- Coagulopathy
- Henoch-Schonlein purpura
- Systemic lupus erythematosus (SLE)
- Colorectal malignancy
- The symptoms of colitis, such as diarrhea (especially bloody diarrhea and abdominal pain)) are observed in all forms of colitis. The table below lists the differential diagnosis of common causes of colitis:[1][2]
| Diseases | History and Symptoms | Physical Examination | Laboratory findings | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Diarrhea | Rectal bleeding | Abdominal pain | Atopy | Dehydration | Fever | Hypotension | Malnutrition | Blood in stool (frank or occult) | Microorganism in stool | Pseudomembranes on endoscopy | Lab Test 4 | |
| Allergic Colitis | + | ++ | + | ++ | ++ | |||||||
| Chemical colitis | + | ++ | ++ | + | + | ++ | + | |||||
| Infectious colitis | ++ | ++ | ++ | +++ | +++ | ++ | + | ++ | ++ | + | ||
| Radiation colitis | + | ++ | + | + | + | ++ | ||||||
| Ischemic colitis | + | + | ++ | + | + | + | + | ++ | ||||
| Drug-induced colitis | + | + | ++ | + | ++ | + | ||||||
References
- ↑ Thielman NM, Guerrant RL (2004). “Clinical practice. Acute infectious diarrhea”. N Engl J Med. 350 (1): 38–47. doi:10.1056/NEJMcp031534. PMID 14702426.
- ↑ Khan AM, Faruque AS, Hossain MS, Sattar S, Fuchs GJ, Salam MA (2004). “Plesiomonas shigelloides-associated diarrhoea in Bangladeshi children: a hospital-based surveillance study”. J Trop Pediatr. 50 (6): 354–6. doi:10.1093/tropej/50.6.354. PMID 15537721.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Qasim Salau, M.B.B.S., FMCPaed [2]
Overview
The exact prevalence of allergic colitis is unknown. Prevalence of food protein-induced allergic proctocolitis (FPIAP) has been reported to range from a low of 16% to a high of 64% among infants with rectal bleeding. FPIAP is the most common cause of non-infectious colitis in infancy. Allergic colitis is mainly a disease of infants, with onset usually in the first two to three months of life. There is a slight male predominance (50–61.6%) for allergic colitis.
Epidemiology and Demographics
Prevalence and Incidence
The exact prevalence and incidence of allergic colitis is unknown.
- Prevalence of food protein-induced allergic proctocolitis (FPIAP) has been reported to range from a low of 16% to a high of 64% among infants with rectal bleeding[1][2][3]
- A population based study reported a prevalence of 1.6 in 1000 children under 1 year had cow’s-milk protein induced rectal bleeding[4]
- The incidence of milk FPIES was estimated as 0.34% of the newborn population in a population based study[4]
- 60% of infants with FPIAP are babies on exclusive breastfeeding[1][5]
- FPIAP is the most common cause of non-infectious colitis in infancy[6]
Age
Allergic colitis is mainly a disease of infants, with onset usually in the first 2-3 months of life. An adolescent form may develop in adolescence or early adulthood.[1][2][3][7]
Gender
There is a slight male predominance (50–61.6%) for allergic colitis.[8][9]
Race
There is no racial predilection for allergic colitis.
References
- ↑ 1.0 1.1 1.2 Nowak-Węgrzyn A (2015). “Food protein-induced enterocolitis syndrome and allergic proctocolitis”. Allergy Asthma Proc. 36 (3): 172–84. doi:10.2500/aap.2015.36.3811. PMC 4405595. PMID 25976434.
- ↑ 2.0 2.1 Arvola T, Ruuska T, Keränen J, Hyöty H, Salminen S, Isolauri E (2006). “Rectal bleeding in infancy: clinical, allergological, and microbiological examination”. Pediatrics. 117 (4): e760–8. doi:10.1542/peds.2005-1069. PMID 16585287.
- ↑ 3.0 3.1 Xanthakos SA, Schwimmer JB, Melin-Aldana H, Rothenberg ME, Witte DP, Cohen MB (2005). “Prevalence and outcome of allergic colitis in healthy infants with rectal bleeding: a prospective cohort study”. J Pediatr Gastroenterol Nutr. 41 (1): 16–22. PMID 15990624.
- ↑ 4.0 4.1 Elizur A, Cohen M, Goldberg MR, Rajuan N, Cohen A, Leshno M; et al. (2012). “Cow’s milk associated rectal bleeding: a population based prospective study”. Pediatr Allergy Immunol. 23 (8): 766–70. doi:10.1111/pai.12009. PMID 23050491.
- ↑ Lake AM (2000). “Food-induced eosinophilic proctocolitis”. J Pediatr Gastroenterol Nutr. 30 Suppl: S58–60. PMID 10634300.
- ↑ Sekerkova A, Fuchs M, Cecrdlova E, Svachova V, Kralova Lesna I, Striz I; et al. (2015). “High Prevalence of Neutrophil Cytoplasmic Autoantibodies in Infants with Food Protein-Induced Proctitis/Proctocolitis: Autoimmunity Involvement?”. J Immunol Res. 2015: 902863. doi:10.1155/2015/902863. PMC 4592904. PMID 26484355.
- ↑ Alfadda AA, Storr MA, Shaffer EA (2011). “Eosinophilic colitis: epidemiology, clinical features, and current management”. Therap Adv Gastroenterol. 4 (5): 301–9. doi:10.1177/1756283X10392443. PMC 3165205. PMID 21922029.
- ↑ Lozinsky AC, Morais MB (2014). “Eosinophilic colitis in infants”. J Pediatr (Rio J). 90 (1): 16–21. doi:10.1016/j.jped.2013.03.024. PMID 24131740.
- ↑ Mehr S, Frith K, Campbell DE (2014). “Epidemiology of food protein-induced enterocolitis syndrome”. Curr Opin Allergy Clin Immunol. 14 (3): 208–16. doi:10.1097/ACI.0000000000000056. PMC 4011623. PMID 24686277.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Qasim Salau, M.B.B.S., FMCPaed [2]
Overview
Risk factors for allergic colitis include family history of atopy and previous sibling with IgE mediated food allergy.
Risk Factors
Risk factors for allergic colitis include:[1]
- Family history of atopy, asthma, environmental allergies
- Previous sibling with IgE mediated food allergy
- IgA deficiency
- Use of formula feeds
- Gastroenteritis
References
- ↑ Allergic Colitis Symptoms and Causes. Boston Children’s Hospital. http://www.childrenshospital.org/conditions-and-treatments/conditions/allergic-colitis/symptoms-and-causes Accessed on April 18, 2017.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Qasim Salau, M.B.B.S., FMCPaed [2]
Overview
Screening is not recommended for allergic colitis.
Screening
Screening is not recommended for allergic colitis.[1][2]
References
- ↑ Boyce JA, Assa’ad A, Burks AW, Jones SM, Sampson HA, Wood RA; et al. (2010). “Guidelines for the Diagnosis and Management of Food Allergy in the United States: Summary of the NIAID-Sponsored Expert Panel Report”. J Allergy Clin Immunol. 126 (6): 1105–18. doi:10.1016/j.jaci.2010.10.008. PMC 4241958. PMID 21134568.
- ↑ U.S. Preventive Services Task Force http://www.uspreventiveservicestaskforce.org/BrowseRec/Search?s=allergic colitis Accessed on September 16, 2016
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Qasim Salau, M.B.B.S., FMCPaed [2]
Overview
Allergic colitis typically develops in early infancy. Allergic colitis is benign, resolving completely in most children without any sequelae. The infants with food protein-induced allergic proctocolitis are usually on exclusive breastfeeding while those with food protein-induced enterocolitis syndrome are often on infant formula. If left untreated, spontaneous resolution may occur in 20% of the children with allergic colitis without elimination of the triggering food. Most infants with allergic colitis will tolerate the offending food by 1 to 3 years of age.
Natural History, Complications, and Prognosis
Natural History
- The symptoms of allergic colitis typically develops in early infancy (within the first two or three months of life). The infants with food protein-induced allergic proctocolitis are usually on exclusive breastfeeding while those with food protein-induced enterocolitis syndrome are often on infant formula. Typically, the episodes resolve within 48 to 96 hours following avoidance of the trigger protein. Spontaneous resolution of symptoms may occur in 20% of the children without elimination of the offending protein. Most infants with food protein-induced allergic proctocolitis will be able to tolerate the offending protein by 1 to 3 years of age, while those with food protein-induced enterocolitis syndrome tolerate the offending protein later usually by 2 to 5 years of age.[1][2][3][4]
- The natural history of allergic colitis that develops in adolescence or early adulthood especially if due to solid food is poorly characterized with the resolution of symptoms often prolonged.[5]
Complications
Complications of allergic colitis are more common with food protein-induced enterocolitis syndrome (FPIES) than food protein-induced allergic proctocolitis (FPIAP). The complications include:[6][7]
- Dehydration
- Electrolyte imbalance
- Iron deficiency anemia
- Hypoalbuminemia (from protein-losing enteropathy)
- Failure to thrive (especially in infants with FPIES)
Prognosis
- The prognosis of allergic colitis is excellent when it presents in infancy.
- The disease is benign, self-limiting, and resolves completely, with the child outgrowing the allergy with age.
- The prognosis for allergic colitis that presents in adolescence or adulthood is not fully understood.[1][3][6]
References
- ↑ 1.0 1.1 Boyce JA, Assa’ad A, Burks AW, Jones SM, Sampson HA, Wood RA; et al. (2010). “Guidelines for the Diagnosis and Management of Food Allergy in the United States: Summary of the NIAID-Sponsored Expert Panel Report”. J Allergy Clin Immunol. 126 (6): 1105–18. doi:10.1016/j.jaci.2010.10.008. PMC 4241958. PMID 21134568.
- ↑ Nowak-Węgrzyn A (2015). “Food protein-induced enterocolitis syndrome and allergic proctocolitis”. Allergy Asthma Proc. 36 (3): 172–84. doi:10.2500/aap.2015.36.3811. PMC 4405595. PMID 25976434.
- ↑ 3.0 3.1 Koletzko S, Niggemann B, Arato A, Dias JA, Heuschkel R, Husby S; et al. (2012). “Diagnostic approach and management of cow’s-milk protein allergy in infants and children: ESPGHAN GI Committee practical guidelines”. J Pediatr Gastroenterol Nutr. 55 (2): 221–9. doi:10.1097/MPG.0b013e31825c9482. PMID 22569527.
- ↑ Lucarelli S, Di Nardo G, Lastrucci G, D’Alfonso Y, Marcheggiano A, Federici T; et al. (2011). “Allergic proctocolitis refractory to maternal hypoallergenic diet in exclusively breast-fed infants: a clinical observation”. BMC Gastroenterol. 11: 82. doi:10.1186/1471-230X-11-82. PMC 3224143. PMID 21762530.
- ↑ Alfadda AA, Storr MA, Shaffer EA (2011). “Eosinophilic colitis: epidemiology, clinical features, and current management”. Therap Adv Gastroenterol. 4 (5): 301–9. doi:10.1177/1756283X10392443. PMC 3165205. PMID 21922029.
- ↑ 6.0 6.1 Pumberger W, Pomberger G, Geissler W (2001). “Proctocolitis in breast fed infants: a contribution to differential diagnosis of haematochezia in early childhood”. Postgrad Med J. 77 (906): 252–4. PMC 1741985. PMID 11264489.
- ↑ Jenkins HR, Pincott JR, Soothill JF, Milla PJ, Harries JT (1984). “Food allergy: the major cause of infantile colitis”. Arch Dis Child. 59 (4): 326–9. PMC 1628682. PMID 6721558.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | X Ray | CT | MRI | Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
References
References
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH