
Bronchogenic cyst
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor: Joanna Ekabua, M.D. [2]
Synonyms and keywords: Bronchial cyst
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Joanna Ekabua, M.D. [2]
Overview
Bronchogenic cyst is a rare benign congenital malformation of the tracheobronchial tree derived from the ventral aspect of the foregut. It most frequently occurs in the middle mediastinum, in the early stages of gestation or in the lungs, at the later stages of gestation. Atypical locations may be explained by its embryologic origin. Patients with bronchogenic cyst may be asymptomatic or present with respiratory distress, increasing stridor, feeding difficulties, chest pain, cough, progressive dysphagia, odynophagia, purulent sputum, dyspnea, anorexia and/orweight loss. Radiologic findings are useful to differentiate bronchogenic cysts from other cysts but they may not always confirm the diagnosis. Diagnosis is confirmed by surgical excision, which is curative, and histological findings of ciliated columnar epithelial lining of the cyst.
Historical Perspective
There is limited information about the historical perspective of bronchogenic cyst.
Classification
Bronchogenic cyst can be classified based on location; pulmonary and extrapulmonary.
Pathophysiology
It is thought that bronchogenic cyst is the result of abnormal budding of the ventral portion of the primitive foregut between days 26 – 40 of gestation.
Causes
The cause of bronchogenic cysts is undetermined.
Differentiating Bronchogenic cyst from other Diseases
Differentiating bronchogenic cyst from lung abcess, thymic cyst, and esophageal duplication cysts.
Bronchogenic cyst epidemiology and demographics|Epidemiology and Demographics
There is no racial predilection to bronchogenic cyst. Bronchogenic cyst is slightly more prevalent in men and often remain undetected until the third or fourth decade of life.
Risk factors
There are no established risk factors for bronchogenic cyst.
Screening
There is insufficient evidence to recommend routine screening for bronchogenic cyst as it is usually an incidental finding.
Natural history, complications and prognosis
Natural History
The symptoms of bronchogenic cyst usually develop in the third to fourth decade of life and start with symptoms such as
- Dyspnea
- Chronic dry cough
- Rhinitis
- Chest discomfort/pain
- Neck pain
- Flu-like symptoms and Fever
- Purulent sputum
- Abdominal discomfort
- Limb weakness
- Paroxysmal supraventricular tachycardia
- Atrioventricular block
- Memory impairment
- Asthenia
- Seizure and loss of consciousness
- Dizziness
- Lower back pain
- Urinary incontinence
Complication
Common complications of bronchogenic cyst include
- Tracheal compression
- Esophageal compression
- Cough
- Infection/abscess
- Hemoptysis
- Superior vena cava syndrome
- Pneumothorax
- Pleurisy
- Pneumonia
- Lymphangioma
- Haemorrhage
- Neoplasia(adenocarcinoma, mucoepidermoid carcinoma, anaplastic carcinoma, and leiomyosarcoma)
- Rupture
- Air embolism
- Cardiac tamponade
- Ventricular septal defect
- syringomyelia
Prognosis
Prognosis is generally good, a Morbidity & Mortality rate of 20% has been recorded in older patients treated for bronchogenic cyst.
Diagnostic Study of Choice
Excision and Hematoxylin and Eosin staining.
Diagnostic results
Cillated columar epithelia cells is definitive for broncogenic cyst.
Diagnostic criteria
Cystic mass-producing compressive symptoms.
History and symptoms
The majority of patients with bronchogenic cyst are asymptomatic and are diagnosed during investigations for other pathologies.
When symptomatic, the clinical presentation of bronchogenic cyst depends on the age of the patient, size and the location of the cyst.
In infants bronchogenic cyst presents with
- respiratory distress
- Increasing stridor
- Reccurrent croup
- Feeding difficulties.
- Palpable neck mass
- Non-bilious emesis
In children and adults, bronchogenic cyst presents with
- Dull chest pain with radiation to the shoulder in diaphragmatic broncogenic cyst.
- Cough
- Progressive dysphagia
- Odynophagia
- wheezing
- Adobminal bloating
- Fever
- Palpable neck mass
- purulent sputum
- Hemoptysis
- Dyspnea
- Anorexia and/or weight loss
- Dizziness
- Paroxysmal supraventricular tachycardia
- Atrioventricular block
- Atrial and ventricular premature complexes
- Memory impairment
- Asthenia
- Limping
- Seizure and loss of consciousness
- Sciatica
- Back pain
- Neuralgia
- Urinary incontinence
Physical examinaton
Physical examination of patients with bronchogenic cyst is usually normal. On rare occasions, the following signs can be seen
- Cough
- wheezing
- Stridor
- Hemoptysis
- Dyspnea
- Tracheal deviation
- Fluid-thrill
- Anorexia and/or weight loss
- Fever
- Asthenia
- Foot drop
- Atrophy
- Heart murmur
- Tenderness
- Cutanous pigmentation
- Negative knee and ankle reflexes
- Numbness
Laboratory findings
An elevated serum tumor makers CA125 and CA19-9, which is usually suggestive of progression/complication.
CT
CT scan may be helpful in the diagnosis of bronchogenic cyst. The density of bronchogenic cysts is variable from water density to high density due to blood, anthracotic pigment, increased calcium content, or increased protein content of the fluid. Findings on CT scan suggestive of bronchogenic cyst is an
- Cysic mass with air-fluid levels.
- ovoid and well-defined encapsulated low-density cystic mass with no contrast enhancement.
- Thin subtle walls.
MRI
MRI may be helpful in the diagnosis of bronchogenic cyst. After contrast injection, enhancement of the cyst is frequently absent. Findings on MRI suggestive of bronchogenic cyst include
- T1-weighted images show ipointense signal
- T2-weighted images show hyperintense signal.
Ultrasound
ultrasound may be helpful in the diagnosis of bronchogenic cyst. Finding on an ultrasound suggestive of bronchogenic cyst include
- On endobronchial ultrasound, an anechoic or hypoechoic fluid-filled solid mass.
- On transthoracic echocardiography revealing intracardiac cystic mass.
- On endoscopic ultrasonography, which demonstartes abdominal anatomic relations of the cyst.
Other Diagnostic Studies
Other diagnostic studies for bronchogenic cyst include: Excision and Hematoxylin and Eosin staining, which demonstrates ciliated columar epithelia cells is definitive for bronchogenic cyst
- Immunohistochemical staining of bronchogenic cyst of the esophagus , which demonstrates a positive expression of CA199 and CA125.
- Bronchoscopy, which demonstrates pink cystic mass with bronchial attachment
- Gastroendoscopy which demonstartes abdominal anatomic relations of the cyst.
- fluorodeoxyglucose–positron emission tomography to confirm cyst infection.
Treatment
Medical therapy
The mainstay of treatment for bronchogenic cyst is surgery.
Surgery
Surgery is the mainstay of treatment for bronchogenic cyst even when the patients are asymptomatic, a conservative approach is not approved.
Primary prevention
There are no established measures for the primary prevention of bronchogenic cyst.
Secondaryy prevention
There are no established measures for the secondary prevention of bronchogenic cyst.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Joanna Ekabua, M.D. [2]
Overview
Bronchogenic cyst is a rare benign congenital malformation of the tracheobronchial tree derived from the ventral aspect of the foregut.
Historical Perspective
There is limited information about the historical perspective of bronchogenic cyst.
References
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Joanna Ekabua, M.D. [2]
Overview
Classification
Bronchogenic cyst can be classified based on location as follows[1][2]
- Pulmonary
- Extra-pulmonary
| Bronchogenic cyst | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pulmonary | Extra-pulmonary | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Plural | Tracheobronchial tree | Cranial | Cervical | Mediastinal | Abdominal | Perianal | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Visceral | Parietal | Paratracheal | Carinal | Hilar | esophageal | Cardiac | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Intraperitoneal | Retroperitoneal | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Diphragmatic | Gastric | Spinal | Adrenal | Pancreatic | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
References
- ↑ 1.0 1.1 1.2 1.3 Maier HC (1948). “Bronchiogenic Cysts of the Mediastinum”. Ann Surg. 127 (3): 476–502. doi:10.1097/00000658-194803000-00010. PMC 1513836. PMID 17859095.
- ↑ 2.0 2.1 2.2 2.3 Sarper A, Ayten A, Golbasi I, Demircan A, Isin E (2003). “Bronchogenic cyst”. Tex Heart Inst J. 30 (2): 105–8. PMC 161894. PMID 12809250.
- ↑ Nakagawa M, Hara M, Oshima H, Shibamoto Y, Sato Y, Kondo S; et al. (2008). “Pleural bronchogenic cysts: imaging findings”. J Thorac Imaging. 23 (4): 284–8. doi:10.1097/RTI.0b013e318176b935. PMID 19204476.
- ↑ Bian B, Yu M, Liu S, Li S, Wei Y, Zhang B (2019). “A suprasellar bronchogenic cyst: A case report”. Medicine (Baltimore). 98 (30): e16650. doi:10.1097/MD.0000000000016650. PMC 6709100 Check
|pmc=value (help). PMID 31348319. - ↑ Xu Q, Feng Y, Ye K, Zhou Y, Zhan R (2015). “Bronchogenic cyst in left anterior cranial fossa”. Neurology. 84 (11): 1181–2. doi:10.1212/WNL.0000000000001368. PMID 25780019.
- ↑ Teissier N, Elmaleh-Bergès M, Ferkdadji L, François M, Van den Abbeele T (2008). “Cervical bronchogenic cysts: usual and unusual clinical presentations”. Arch Otolaryngol Head Neck Surg. 134 (11): 1165–9. doi:10.1001/archotol.134.11.1165. PMID 19015445.
- ↑ Kün-Darbois JD, Breheret R, Bizon A, Paré A, Laccourreye L (2015). “Bronchogenic cyst of the tip of the tongue: report of two cases”. Eur Ann Otorhinolaryngol Head Neck Dis. 132 (1): 49–51. doi:10.1016/j.anorl.2013.11.007. PMID 24993780.
- ↑ Mega S (2015). “[Anterior Mediastinal Bronchogenic Cyst Associated with paroxysmal supraventricular tachycardia ; Report of a Case]”. Kyobu Geka. 68 (10): 871–3. PMID 26329634.
- ↑ Wang W, Ni Y, Zhang L, Li X, Ke C, Lu Q; et al. (2012). “A case report of para-esophageal bronchogenic cyst with esophageal communication”. J Cardiothorac Surg. 7: 94. doi:10.1186/1749-8090-7-94. PMC 3599576. PMID 23013612.
- ↑ Chuang KH, Huang TW, Cheng YL, Chen JC, Tzao C, Chang H; et al. (2007). “Esophageal bronchogenic cyst: a rare entity”. Z Gastroenterol. 45 (9): 958–60. doi:10.1055/s-2007-963069. PMID 17874358.
- ↑ Yang X, Zong Y, Zhao HY, Wu YD, Ji M (2019). “Complete excision of esophageal bronchogenic cyst by endoscopic submucosal tunnel dissection: a case presentation”. BMC Gastroenterol. 19 (1): 155. doi:10.1186/s12876-019-1072-3. PMC 6714396 Check
|pmc=value (help). PMID 31462259. - ↑ Miwa E, Tani T, Okada Y, Furukawa Y (2017). “A rare cardiac tumor: Bronchogenic cyst of interatrial septum”. Echocardiography. 34 (3): 474–475. doi:10.1111/echo.13445. PMID 28139004.
- ↑ Mesland JB, Gérard L, Van Caenegem O, Castanares-Zapatero D (2018). “Bronchogenic cyst infection presenting as pleuropericarditis”. BMJ Case Rep. 2018. doi:10.1136/bcr-2018-225081. PMC 6011476. PMID 29895549.
- ↑ Olsen M, Mitchell TA, Percival TJ, Helsel BS (2015). “Interatrial Bronchogenic Cyst Resection”. Ann Thorac Surg. 100 (2): 709–11. doi:10.1016/j.athoracsur.2014.10.025. PMID 26234845.
- ↑ Gou Y, Wang Y, Fang H, Xu X, Yu W, Zhang K; et al. (2015). “Bronchogenic cyst in the hepatogastric ligament masquerading as an esophageal mesenchymal tumor: a case report”. Int J Clin Exp Pathol. 8 (11): 15307–11. PMC 4713671. PMID 26823885.
- ↑ Legras A, Mordant P, Gibault L, Hernigou A, Le Pimpec Barthes F, Riquet M (2014). “[Diaphragmatic bronchogenic cyst: an exceptional location]”. Rev Pneumol Clin. 70 (6): 357–61. doi:10.1016/j.pneumo.2014.05.002. PMID 25131363.
- ↑ Ikeda T, Nakano J, Sano T (2019). “[Intraphrenic Bronchogenic Cyst;Report of a Case]”. Kyobu Geka. 72 (6): 477–479. PMID 31268025.
- ↑ Chumakova M, Morris-Stiff G, Khachaturov V, Ibrahim S (2016). “Bronchogenic cyst arising from the crus of the left hemidiaphragm”. BMJ Case Rep. 2016. doi:10.1136/bcr-2015-213658. PMC 4840741. PMID 27068723.
- ↑ Han WG, Xue HD, Pan WD (2019). “[Bronchogenic Cyst of Stomach:Report of One Case]”. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 41 (4): 572–574. doi:10.3881/j.issn.1000-503X.10798. PMID 31484624.
- ↑ Ruiz Molina I, Landauro Comesaña C, Solís García E, Cívico Amat V, Sánchez Quintana F (2019). “[Gastric bronchogenic cysts. An unusual location]”. Rev Esp Patol. 52 (2): 117–119. doi:10.1016/j.patol.2017.12.003. PMID 30902375.
- ↑ Zou MX, Hu JR, Kang YJ, Li J, Lv GH, She XL (2015). “Bronchogenic cyst of the conus medullaris with spinal cord tethering: a case report and review of the literature”. Int J Clin Exp Pathol. 8 (4): 3937–42. PMC 4466965. PMID 26097578.
- ↑ Lee HD, Han SH, Park SB, Ko Y, Lee KH (2017). “An intradural extramedullary bronchogenic cyst in the thoracolumbar spine: A case report”. Medicine (Baltimore). 96 (50): e9263. doi:10.1097/MD.0000000000009263. PMC 5815783. PMID 29390371.
- ↑ Candy N, Young A, Devadass A, Dean A, McMillen J, Trivedi R (2017). “Dual lumbar bronchogenic and arachnoid cyst presenting with sciatica and left foot drop”. Acta Neurochir (Wien). 159 (10): 2029–2032. doi:10.1007/s00701-017-3284-z. PMID 28762109.
- ↑ Haddadin WJ, Reid R, Jindal RM (2001). “A retroperitoneal bronchogenic cyst: a rare cause of a mass in the adrenal region”. J Clin Pathol. 54 (10): 801–2. doi:10.1136/jcp.54.10.801. PMC 1731290. PMID 11577133.
- ↑ Bulut G, Bulut MD, Bahadır I, Kotan Ç (2015). “Bronchogenic cyst mimicking an adrenal mass in the retroperitoneal region: report of a rare case”. Indian J Pathol Microbiol. 58 (1): 96–8. doi:10.4103/0377-4929.151200. PMID 25673605.
- ↑ Cao DH, Zheng S, Lv X, Yin R, Liu LR, Yang L; et al. (2014). “Multilocular bronchogenic cyst of the bilateral adrenal: report of a rare case and review of literature”. Int J Clin Exp Pathol. 7 (6): 3418–22. PMC 4097272. PMID 25031770.
- ↑ Shin SS, Choi YD, Jun CH (2017). “An Incidental Pancreatic Mass in a Young Woman”. Gastroenterology. 153 (1): e16–e17. doi:10.1053/j.gastro.2016.10.044. PMID 28602758.
- ↑ Maly T, Mihal V, Michalkova K, Tichy T, Neoral C, Zonca P (2014). “Retroperitoneal bronchogenic cyst: prenatal diagnosis of cystoid formation, its progression and surgery”. Bratisl Lek Listy. 115 (2): 98–100. doi:10.4149/bll_2014_021. PMID 24601704.
- ↑ Liu L, Zhang Y, Zhang Z, Si L (2013). “Perianal bronchogenic cyst: a report of two cases”. Indian J Pathol Microbiol. 56 (4): 411–2. doi:10.4103/0377-4929.125355. PMID 24441234.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Joanna Ekabua, M.D. [2] Kalsang Dolma, M.B.B.S.[3]
Overview
It is thought that bronchogenic cyst is the result of abnormal budding of the ventral [1] portion of the primitive foregut[2][3][4]destined to become the tracheobronchial tree[5] between days 26 – 40 of gestation. [5] At such, it is often found in relation to the trachea or esophagus.[6] On rare occasions, they may be found in the cranial, cervical, mediastinal, and abdominal regions. If the cell mass maintains its connection with the tracheobronchial tree, the cyst becomes intrapulmonary or in close association with the lungs. If separated, there is no contiunity with the bronchia lumen. Such cyst increases in size gradually due to secretions produced within the cavity, leading to compressive symptoms.[2][7]
Gross pathology
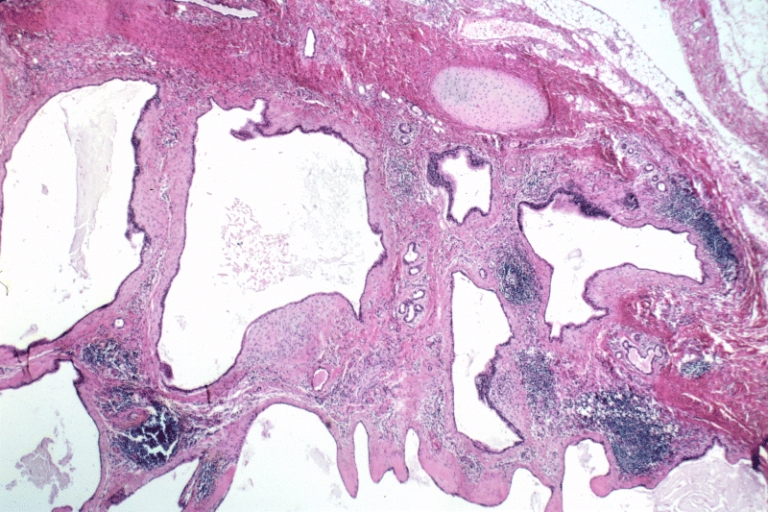
Bronchogenic cyst appear as single or multiple smooth spherical pink masses which may be unlobulated or lobulated. [5][2] The lobules could be of various sizes, communicating or noncommunicating. The wall is relatively thin and frequently trabeculated,[2] even though there may be thicker portions. Cyst often appear to have check valves,[8] leading to their enlargement from secretions by its clilated columnar epithelium. Secretions may be a thick, white mucoid material if uninfected, and a dirty brown mucoid to purulent material if infected.[2] Occassionally, secretions could be hemorrhagic or pneumatic.[3]


Images shown below are courtesy of Professor Peter Anderson DVM PhD and published with permission. © PEIR, University of Alabama at Birmingham, Department of Pathology
-
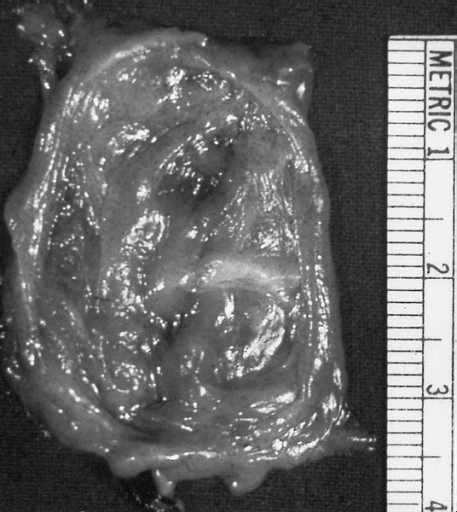 Lower Respiratory Tract: Bronchogenic cysts are grossly nondescript, usually unilocular cavities containing mucus or mucopurulent material with a wall that varies in thickness and may contain cartilage.
Lower Respiratory Tract: Bronchogenic cysts are grossly nondescript, usually unilocular cavities containing mucus or mucopurulent material with a wall that varies in thickness and may contain cartilage. -
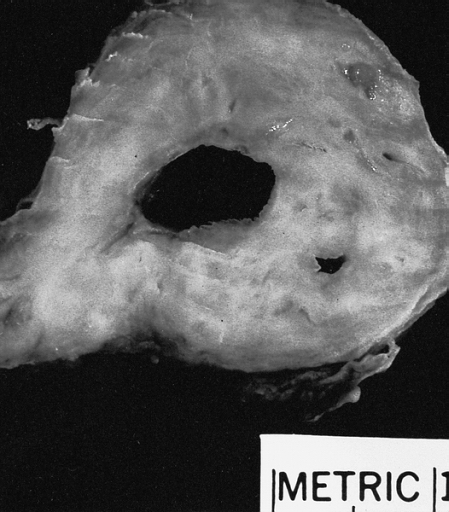 Lower Respiratory Tract: Bronchogenic cysts are grossly nondescript, usually unilocular cavities containing mucus or mucopurulent material with a wall that varies in thickness and may contain cartilage.
Lower Respiratory Tract: Bronchogenic cysts are grossly nondescript, usually unilocular cavities containing mucus or mucopurulent material with a wall that varies in thickness and may contain cartilage.


-
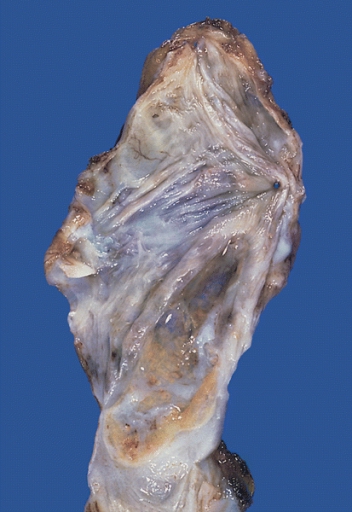
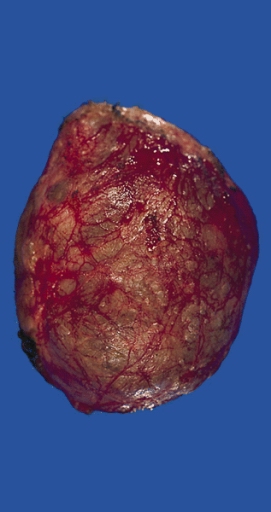 Mediastinum: Bronchogenic cyst; A thin-walled cyst which was present in the posterior mediastinum is distended with slightly cloudy somewhat mucinous fluid.
Mediastinum: Bronchogenic cyst; A thin-walled cyst which was present in the posterior mediastinum is distended with slightly cloudy somewhat mucinous fluid. -
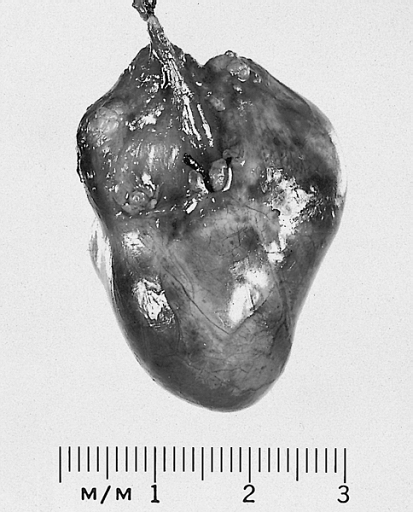 Heart-Great Vessels: Bronchogenic cyst; This example was removed from the epicardial surface of a 13-year-old.
Heart-Great Vessels: Bronchogenic cyst; This example was removed from the epicardial surface of a 13-year-old.


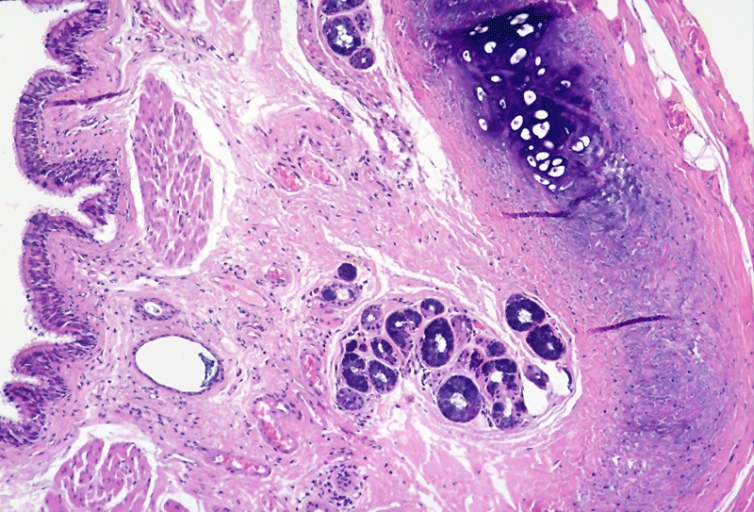
Histopathology
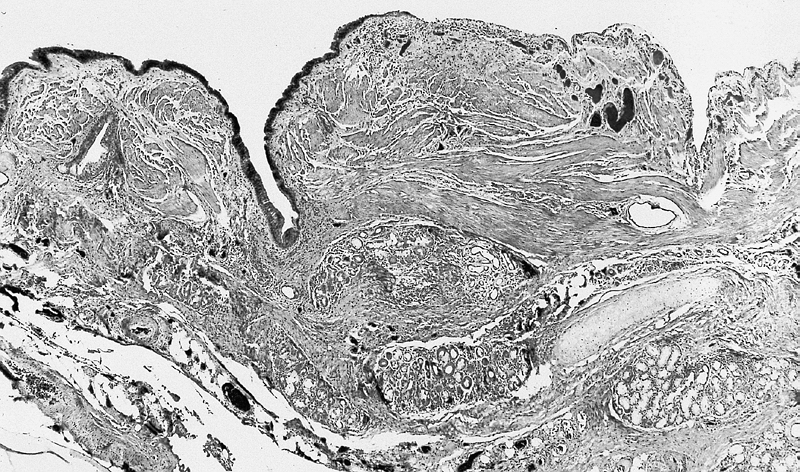
Bronchogenic cysts are usually lined by ciliated columnar epithelium of respiratory type, leading to distention as a result of secretions produced within the cavity. Cyst wall may be composed of cartilage, smooth muscle, fibrous tissue, chronic inflammatory infiltrates, necrotic tissue, focal areas of squamous metaplasia, vascular proliferation, bronchial gland, and mucous glands.[5] [2] [9] [4][10]


Images shown below are courtesy of Professor Peter Anderson DVM PhD and published with permission. © PEIR, University of Alabama at Birmingham, Department of Pathology
-
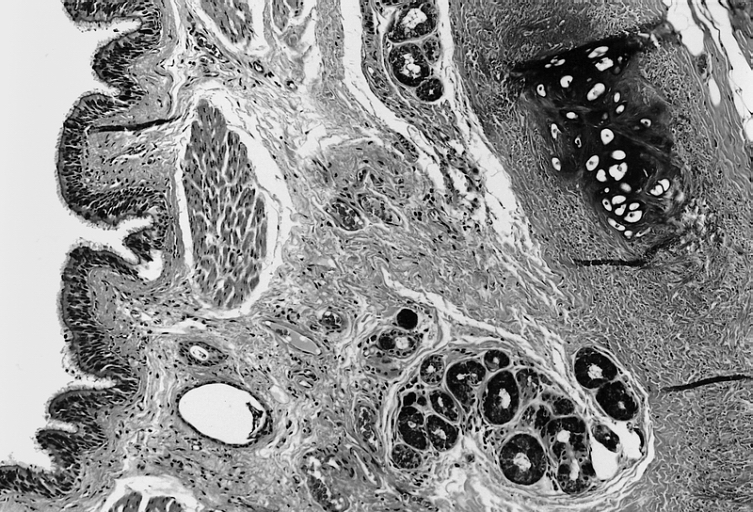
 Lower Respiratory Tract: Intrathoracic bronchogenic cyst; Histologically, smooth muscle bundles, minor salivary gland type tissue, and cartilage can be seen in the wall of the cyst.
Lower Respiratory Tract: Intrathoracic bronchogenic cyst; Histologically, smooth muscle bundles, minor salivary gland type tissue, and cartilage can be seen in the wall of the cyst. -
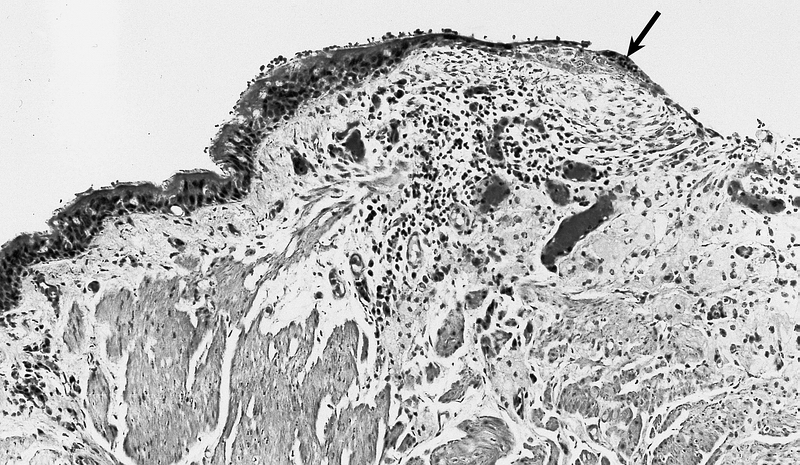 Lower Respiratory Tract: Intrathoracic bronchogenic cyst; The lining is typically pseudostratified ciliated columnar epithelium which may show foci of squamous metaplasia at sites of inflammation (arrow).
Lower Respiratory Tract: Intrathoracic bronchogenic cyst; The lining is typically pseudostratified ciliated columnar epithelium which may show foci of squamous metaplasia at sites of inflammation (arrow).


-
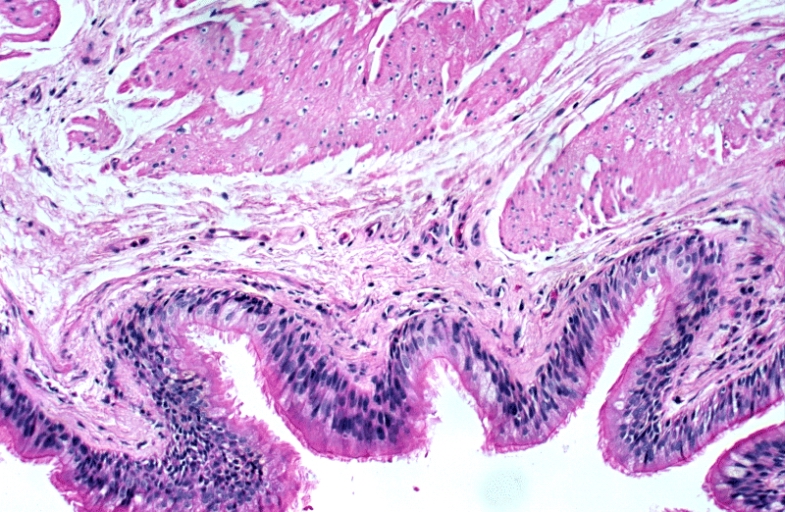
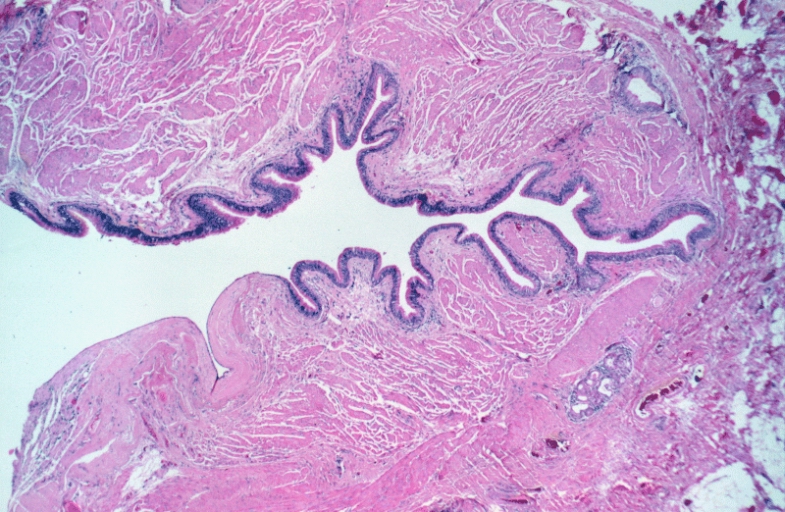 Lower Respiratory Tract: Bronchogenic cyst; There is a cyst lined by bronchiolar epithelium and thick fascicles of smooth muscle in the wall. Islands of cartilage and submucosal salivary glands are lacking and the designation “foregut cyst consistent with bronchogenic cyst” might be more appropriate.
Lower Respiratory Tract: Bronchogenic cyst; There is a cyst lined by bronchiolar epithelium and thick fascicles of smooth muscle in the wall. Islands of cartilage and submucosal salivary glands are lacking and the designation “foregut cyst consistent with bronchogenic cyst” might be more appropriate. -
 Lower Respiratory Tract: Bronchogenic cyst; There is a cyst lined by bronchiolar epithelium and thick fascicles of smooth muscle in the wall. Islands of cartilage and submucosal salivary glands are lacking and the designation “foregut cyst consistent with bronchogenic cyst” might be more appropriate.
Lower Respiratory Tract: Bronchogenic cyst; There is a cyst lined by bronchiolar epithelium and thick fascicles of smooth muscle in the wall. Islands of cartilage and submucosal salivary glands are lacking and the designation “foregut cyst consistent with bronchogenic cyst” might be more appropriate.


-
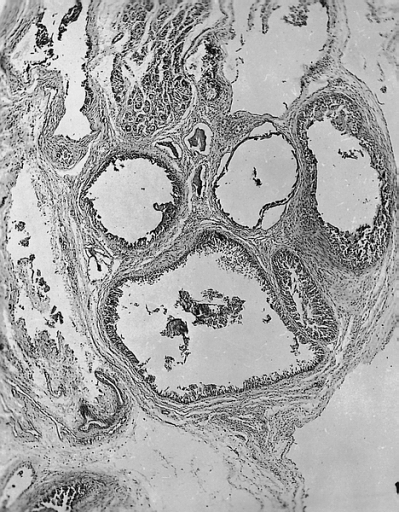
 Lower Respiratory Tract: Bronchogenic cyst; There is a multiloculated cyst lined by bronchiolar epithelium. A small island of cartilage is present at the upper right.
Lower Respiratory Tract: Bronchogenic cyst; There is a multiloculated cyst lined by bronchiolar epithelium. A small island of cartilage is present at the upper right. -
 Heart-Great Vessels: Bronchogenic cyst; The lining cells are cuboidal, and the cysts are surrounded by muscle and may contain underlying seromucous glands.
Heart-Great Vessels: Bronchogenic cyst; The lining cells are cuboidal, and the cysts are surrounded by muscle and may contain underlying seromucous glands.


-
 Mediastinum: Bronchogenic cyst; The inner surface is smooth and trabeculated in areas.
Mediastinum: Bronchogenic cyst; The inner surface is smooth and trabeculated in areas. -
 Mediastinum: Bronchogenic cyst; The cyst is lined by pseudostratified ciliated columnar epithelial cells and the wall contains accessory glands, layers of smooth muscle, and cartilage.
Mediastinum: Bronchogenic cyst; The cyst is lined by pseudostratified ciliated columnar epithelial cells and the wall contains accessory glands, layers of smooth muscle, and cartilage. -
 Mediastinum: Bronchogenic cyst; The cyst is lined by pseudostratified ciliated columnar epithelial cells and the wall contains accessory glands, layers of smooth muscle, and cartilage.
Mediastinum: Bronchogenic cyst; The cyst is lined by pseudostratified ciliated columnar epithelial cells and the wall contains accessory glands, layers of smooth muscle, and cartilage.



References
- ↑ Han C, Lin R, Yu J, Zhang Q, Zhang Y, Liu J; et al. (2016). “A Case Report of Esophageal Bronchogenic Cyst and Review of the Literature With an Emphasis on Endoscopic Ultrasonography Appearance”. Medicine (Baltimore). 95 (11): e3111. doi:10.1097/MD.0000000000003111. PMC 4839937. PMID 26986156.
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 Maier HC (1948). “Bronchiogenic Cysts of the Mediastinum”. Ann Surg. 127 (3): 476–502. doi:10.1097/00000658-194803000-00010. PMC 1513836. PMID 17859095.
- ↑ 3.0 3.1 Sarper A, Ayten A, Golbasi I, Demircan A, Isin E (2003). “Bronchogenic cyst”. Tex Heart Inst J. 30 (2): 105–8. PMC 161894. PMID 12809250.
- ↑ 4.0 4.1 Teissier N, Elmaleh-Bergès M, Ferkdadji L, François M, Van den Abbeele T (2008). “Cervical bronchogenic cysts: usual and unusual clinical presentations”. Arch Otolaryngol Head Neck Surg. 134 (11): 1165–9. doi:10.1001/archotol.134.11.1165. PMID 19015445.
- ↑ 5.0 5.1 5.2 5.3 “StatPearls”. 2020. PMID 30725658.
- ↑ Schmoldt A, Benthe HF, Haberland G (1975). “Digitoxin metabolism by rat liver microsomes”. Biochem Pharmacol. 24 (17): 1639–41. PMID https://doi.org/10.1186/1749-8090-7-94 Check
|pmid=value (help). - ↑ Suda K, Sueyoshi R, Okawada M, Koga H, Lane GJ, Yamataka A; et al. (2015). “Completely intramural bronchogenic cyst of the cervical esophagus in a neonate”. Pediatr Surg Int. 31 (7): 683–7. doi:10.1007/s00383-015-3720-1. PMID 26002606.
- ↑ Ribet ME, Copin MC, Gosselin BH (1996). “Bronchogenic cysts of the lung”. Ann Thorac Surg. 61 (6): 1636–40. doi:10.1016/0003-4975(96)00172-5. PMID 8651761.
- ↑ Mehta RP, Faquin WC, Cunningham MJ (2004). “Cervical bronchogenic cysts: a consideration in the differential diagnosis of pediatric cervical cystic masses”. Int J Pediatr Otorhinolaryngol. 68 (5): 563–8. doi:10.1016/j.ijporl.2003.12.015. PMID 15081229.
- ↑ Aktoğu S, Yuncu G, Halilçolar H, Ermete S, Buduneli T (1996). “Bronchogenic cysts: clinicopathological presentation and treatment”. Eur Respir J. 9 (10): 2017–21. doi:10.1183/09031936.96.09102017. PMID 8902460.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Joanna Ekabua, M.D. [2]
Overview
Bronchogenic cyst is a rare benign congenital malformation of the tracheobronchial tree derived from the ventral aspect of the foregut.
Causes
The cause of bronchogenic cysts is undetermined.
References
Differentiating Bronchogenic cyst from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Joanna Ekabua, M.D. [2]
Overview
Bronchogenic cyst must be differentiated from lung abcess, thymic cyst, and esophageal duplication cysts
Differentiating bronchogenic cyst from lung abcess, thymic cyst, and esophageal duplication cysts
| Diseases | Clinical manifestations | Para-clinical findings | Gold standard | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Symptoms | Physical examination | |||||||||||||
| Lab Findings | Imaging | Histopathology | ||||||||||||
| Symptom 1 | Symptom 2 | Symptom 3 | Physical exam 1 | Physical exam 2 | Physical exam 3 | Lab 1 | Lab 2 | Lab 3 | Imaging 1 | Imaging 2 | Imaging 3 | |||
| Lung abcess[1] | Fever | Chest pain | night sweats | Dullness to percussion | coarse inspiratory crackles | Decreased breath sounds | Leukocytosis | Increased inflamatory markers (ESR, CRP) | Anemia of chronic disease |  |
 |
 |
 |
CT with intravenous contrast |
| Thymic cyst[2] | Cough | Chest pain | Dyspnea | Some patients may present with a soft compressible neck mass | – | – | – | – | – |  |
 |
 |
 |
Biopsy withhistopathology and cytology |
| Esophageal duplication cysts[2][3][2] | Retrosternal and thoracic back pain | Epigastric discomfort | Dysphagia | – | – | – | – | – | – |  |
 |
 |
 |
Endoscopic ultrasound
|
References
- ↑ Kuhajda I, Zarogoulidis K, Tsirgogianni K, Tsavlis D, Kioumis I, Kosmidis C; et al. (2015). “Lung abscess-etiology, diagnostic and treatment options”. Ann Transl Med. 3 (13): 183. doi:10.3978/j.issn.2305-5839.2015.07.08. PMC 4543327. PMID 26366400.
- ↑ 2.0 2.1 2.2 Juanpere S, Cañete N, Ortuño P, Martínez S, Sanchez G, Bernado L (2013). “A diagnostic approach to the mediastinal masses”. Insights Imaging. 4 (1): 29–52. doi:10.1007/s13244-012-0201-0. PMC 3579993. PMID 23225215.
- ↑ Liu R, Adler DG (2014). “Duplication cysts: Diagnosis, management, and the role of endoscopic ultrasound”. Endosc Ultrasound. 3 (3): 152–60. doi:10.4103/2303-9027.138783. PMC 4145475. PMID 25184121.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Joanna Ekabua, M.D. [2]
Overview
Epidemiology and Demographics
Incidence
- Bronchogenic cyst accounts for 10% to 15% of mediastinal tumors and 50 to 60% of all mediastinal cysts.[1]
Prevalences
- The prevalence of bronchogenic cyst is estimated at 1 per 42,000 and 1 per 68,000 admissions in two hospital series.[2]
Case fatality rate/mortality rate
- In 2011, broncogenic cyst was shown to have a case-fatality rate/mortality rate of 20%.[3]
Age
Race
- There is no racial predilection to bronchogenic cyst.
Gender
- Bronchogenic cyst is slightly more prevalent in men and often remain undetected till the third or fourth decade of life.[5][6]
References
- ↑ McAdams HP, Kirejczyk WM, Rosado-de-Christenson ML, Matsumoto S (2000). “Bronchogenic cyst: imaging features with clinical and histopathologic correlation”. Radiology. 217 (2): 441–6. doi:10.1148/radiology.217.2.r00nv19441. PMID 11058643.
- ↑ Limaïem F, Ayadi-Kaddour A, Djilani H, Kilani T, El Mezni F (2008). “Pulmonary and mediastinal bronchogenic cysts: a clinicopathologic study of 33 cases”. Lung. 186 (1): 55–61. doi:10.1007/s00408-007-9056-4. PMID 18064522.
- ↑ Makhija Z, Moir CR, Allen MS, Cassivi SD, Deschamps C, Nichols FC; et al. (2011). “Surgical management of congenital cystic lung malformations in older patients”. Ann Thorac Surg. 91 (5): 1568–73, discussion 1573. doi:10.1016/j.athoracsur.2011.01.080. PMID 21420068.
- ↑ Ribet ME, Copin MC, Gosselin BH (1996). “Bronchogenic cysts of the lung”. Ann Thorac Surg. 61 (6): 1636–40. doi:10.1016/0003-4975(96)00172-5. PMID 8651761.
- ↑ Lardinois D, Gugger M, Ris HB (1999). “Bronchogenic cyst of the left lower lobe associated with severe hemoptysis”. Eur J Cardiothorac Surg. 16 (3): 382–3. doi:10.1016/s1010-7940(99)00226-2. PMID 10554866.
- ↑ Aktoğu S, Yuncu G, Halilçolar H, Ermete S, Buduneli T (1996). “Bronchogenic cysts: clinicopathological presentation and treatment”. Eur Respir J. 9 (10): 2017–21. doi:10.1183/09031936.96.09102017. PMID 8902460.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Joanna Ekabua, M.D. [2]
Overview
There are no established risk factors for bronchogenic cyst.
Risk factors
There are no established risk factors for bronchogenic cyst.
References
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Joanna Ekabua, M.D. [2]
Overview
There is insufficient evidence to recommend routine screening for bronchogenic cyst as it is usually an incidental finding.
Screening
There is insufficient evidence to recommend routine screening for bronchogenic cyst as it is usually an incidental finding.
References
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Joanna Ekabua, M.D. [2]
Overview
The symptoms of bronchogenic cyst usually develop in the third to fourth decade of life.
Natural history, complications and prognosis
Natural History
The symptoms of bronchogenic cyst usually develop in the third to fourth decade of life and start with symptoms such as
- Dyspnea[1][2][3][4]
- Chronic dry cough[1][2][4]
- Rhinitis[5]
- Chest discomfort/pain[1][6][2][3]
- Neck pain[7]
- Flu-like symptoms and Fever[1][2][3]
- Purulent sputum[1]
- Abdominal discomfort
- Limb weakness
- Paroxysmal supraventricular tachycardia[8]
- Atrioventricular block[9]
- Memory impairment[10]
- Asthenia[10][11][12]
- Seizure and loss of consciousness[13]
- Dizziness[14]
- Lower back pain[11]
- Urinary incontinence[11]
Complication
Common complications of bronchogenic cyst include
- Tracheal compression[15][16]
- Esophageal compression[1]
- Cough[15]
- Infection/abscess[15][17][18][5]
- Hemoptysis[1][15]
- Superior vena cava syndrome[16][19][20]
- Pneumothorax[1][16]
- Pleurisy[16]
- Pneumonia[1][16]
- Lymphangioma[17]
- Haemorrhage[17][18]
- Neoplasia(adenocarcinoma, mucoepidermoid carcinoma, anaplastic carcinoma, and leiomyosarcoma)[17][21][22][18]
- Rupture[1][21][18]
- Air embolism[13]
- Cardiac tamponade[3]
- Ventricular septal defect[23]
- syringomyelia[7]
Prognosis
Prognosis is generally good,[17] a Morbidity & Mortality rate of 20% has been recorded in older patients treated for bronchogenic cyst.[24]
References
- ↑ 1.00 1.01 1.02 1.03 1.04 1.05 1.06 1.07 1.08 1.09 Sarper A, Ayten A, Golbasi I, Demircan A, Isin E (2003). “Bronchogenic cyst”. Tex Heart Inst J. 30 (2): 105–8. PMC 161894. PMID 12809250.
- ↑ 2.0 2.1 2.2 2.3 Mesland JB, Gérard L, Van Caenegem O, Castanares-Zapatero D (2018). “Bronchogenic cyst infection presenting as pleuropericarditis”. BMJ Case Rep. 2018. doi:10.1136/bcr-2018-225081. PMC 6011476. PMID 29895549.
- ↑ 3.0 3.1 3.2 3.3 Yildiz H, Reichwein R, Poncelet A, Lacroix V, D’abadie P, Ghaye B; et al. (2019). “An unusual case of cardiac tamponade: Bronchogenic cyst infection due to Salmonella bredeney”. J Infect Chemother. 25 (2): 151–153. doi:10.1016/j.jiac.2018.07.012. PMID 30098916.
- ↑ 4.0 4.1 Olsen M, Mitchell TA, Percival TJ, Helsel BS (2015). “Interatrial Bronchogenic Cyst Resection”. Ann Thorac Surg. 100 (2): 709–11. doi:10.1016/j.athoracsur.2014.10.025. PMID 26234845.
- ↑ 5.0 5.1 DiBardino DM, Brenner K (2017). “Bronchogenic Cyst Abscess”. J Bronchology Interv Pulmonol. 24 (3): 31–32. doi:10.1097/LBR.0000000000000375. PMID 28696968.
- ↑ Chumakova M, Morris-Stiff G, Khachaturov V, Ibrahim S (2016). “Bronchogenic cyst arising from the crus of the left hemidiaphragm”. BMJ Case Rep. 2016. doi:10.1136/bcr-2015-213658. PMC 4840741. PMID 27068723.
- ↑ 7.0 7.1 Chen F, Marx S, Zhang C, Cao J, Yu Y, Chen D (2019). “Intramedullary bronchogenic cyst in the foramen magnum region accompanied with syringomyelia: A case report and literature review”. Medicine (Baltimore). 98 (5): e14353. doi:10.1097/MD.0000000000014353. PMC 6380722. PMID 30702626.
- ↑ Mega S (2015). “[Anterior Mediastinal Bronchogenic Cyst Associated with paroxysmal supraventricular tachycardia ; Report of a Case]”. Kyobu Geka. 68 (10): 871–3. PMID 26329634.
- ↑ Miwa E, Tani T, Okada Y, Furukawa Y (2017). “A rare cardiac tumor: Bronchogenic cyst of interatrial septum”. Echocardiography. 34 (3): 474–475. doi:10.1111/echo.13445. PMID 28139004.
- ↑ 10.0 10.1 Bian B, Yu M, Liu S, Li S, Wei Y, Zhang B (2019). “A suprasellar bronchogenic cyst: A case report”. Medicine (Baltimore). 98 (30): e16650. doi:10.1097/MD.0000000000016650. PMC 6709100 Check
|pmc=value (help). PMID 31348319. - ↑ 11.0 11.1 11.2 Zou MX, Hu JR, Kang YJ, Li J, Lv GH, She XL (2015). “Bronchogenic cyst of the conus medullaris with spinal cord tethering: a case report and review of the literature”. Int J Clin Exp Pathol. 8 (4): 3937–42. PMC 4466965. PMID 26097578.
- ↑ Lee HD, Han SH, Park SB, Ko Y, Lee KH (2017). “An intradural extramedullary bronchogenic cyst in the thoracolumbar spine: A case report”. Medicine (Baltimore). 96 (50): e9263. doi:10.1097/MD.0000000000009263. PMC 5815783. PMID 29390371.
- ↑ 13.0 13.1 Khawar M, Elmahrouk A, Chaikhouni A (2016). “Air embolism during air flight in a passenger with bronchogenic cyst”. J Thorac Cardiovasc Surg. 152 (1): e1–2. doi:10.1016/j.jtcvs.2016.02.014. PMID 26969135.
- ↑ Xu Q, Feng Y, Ye K, Zhou Y, Zhan R (2015). “Bronchogenic cyst in left anterior cranial fossa”. Neurology. 84 (11): 1181–2. doi:10.1212/WNL.0000000000001368. PMID 25780019.
- ↑ 15.0 15.1 15.2 15.3 Ribet ME, Copin MC, Gosselin BH (1996). “Bronchogenic cysts of the lung”. Ann Thorac Surg. 61 (6): 1636–40. doi:10.1016/0003-4975(96)00172-5. PMID 8651761.
- ↑ 16.0 16.1 16.2 16.3 16.4 Aktoğu S, Yuncu G, Halilçolar H, Ermete S, Buduneli T (1996). “Bronchogenic cysts: clinicopathological presentation and treatment”. Eur Respir J. 9 (10): 2017–21. doi:10.1183/09031936.96.09102017. PMID 8902460.
- ↑ 17.0 17.1 17.2 17.3 17.4 Teissier N, Elmaleh-Bergès M, Ferkdadji L, François M, Van den Abbeele T (2008). “Cervical bronchogenic cysts: usual and unusual clinical presentations”. Arch Otolaryngol Head Neck Surg. 134 (11): 1165–9. doi:10.1001/archotol.134.11.1165. PMID 19015445.
- ↑ 18.0 18.1 18.2 18.3 Yang X, Zong Y, Zhao HY, Wu YD, Ji M (2019). “Complete excision of esophageal bronchogenic cyst by endoscopic submucosal tunnel dissection: a case presentation”. BMC Gastroenterol. 19 (1): 155. doi:10.1186/s12876-019-1072-3. PMC 6714396 Check
|pmc=value (help). PMID 31462259. - ↑ Hayabuchi Y, Sakata M, Kagami S (2015). “Bronchogenic cyst compressing the pulmonary artery and the left atrium”. Eur Heart J Cardiovasc Imaging. 16 (7): 746. doi:10.1093/ehjci/jev059. PMID 25750196.
- ↑ Parsons C, Zhao CB, Huang J (2019). “Gigantic Pericardial Bronchogenic Cyst Compressing Superior Vena Cava and Coronary Artery”. Anesthesiology. 131 (3): 667. doi:10.1097/ALN.0000000000002739. PMID 31008767.
- ↑ 21.0 21.1 Chuang KH, Huang TW, Cheng YL, Chen JC, Tzao C, Chang H; et al. (2007). “Esophageal bronchogenic cyst: a rare entity”. Z Gastroenterol. 45 (9): 958–60. doi:10.1055/s-2007-963069. PMID 17874358.
- ↑ Han C, Lin R, Yu J, Zhang Q, Zhang Y, Liu J; et al. (2016). “A Case Report of Esophageal Bronchogenic Cyst and Review of the Literature With an Emphasis on Endoscopic Ultrasonography Appearance”. Medicine (Baltimore). 95 (11): e3111. doi:10.1097/MD.0000000000003111. PMC 4839937. PMID 26986156.
- ↑ Blesneac C, Horvath E, Muntean I, Benedek T, Toganel R (2018). “Intracardiac bronchogenic cyst associated with ventricular septal defect: an extremely rare feature in children”. Eur Heart J Cardiovasc Imaging. 19 (9): 1074. doi:10.1093/ehjci/jey078. PMID 29897508.
- ↑ Makhija Z, Moir CR, Allen MS, Cassivi SD, Deschamps C, Nichols FC; et al. (2011). “Surgical management of congenital cystic lung malformations in older patients”. Ann Thorac Surg. 91 (5): 1568–73, discussion 1573. doi:10.1016/j.athoracsur.2011.01.080. PMID 21420068.
Diagnosis
Diagnosis
Diagnostic Study of Choice | History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | X-ray | Electrocardiography and ultrasound | CT | MRI | Ultrasound | Other imaging findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Intervention | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH