
Cardiac tamponade
For patient information click here
For the main page on pericarditis, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Varun Kumar, M.B.B.S. Ramyar Ghandriz MD[3]
Synonyms and keywords: Pericardial tamponade; tamponade
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Varun Kumar, M.B.B.S Ramyar Ghandriz MD[3]
Overview
Cardiac tamponade is a medical emergency condition in which fluid/blood accumulates in the pericardium (the sac in which the heart is enclosed). The elevated pericardial pressure puts significant pressure on the heart, causing a decrease in the diastolic filling of the ventricles, and hence in stroke volume. The end result is ineffective pumping of blood, shock, and potentially death. It is caused mainly by the accumulation of a large or uncontrolled pericardial effusion. The effusion can occur rapidly (as in the case of trauma or myocardial rupture), or over a more gradual period of time (as in cancer). The fluid involved is often blood, but pus is also found in some circumstances. Common causes of increased pericardial effusion include hypothyroidism, trauma (either penetrating trauma involving the pericardium or blunt chest trauma), pericarditis (inflammation of the pericardium), iatrogenic trauma (during an invasive procedure), and ventricular rupture. It should be differentiated from tension pneumothorax, hypovolemia and acute congestive heart failure. Patients with cardiac tamponade may present with sudden onset of chest pain, palpitations, breathlessness and lightheadedness. Physical examination may show the classic Beck’s triad (hypotension, muffled heart sound, and elevated jugular venous distension), tachycardia, pulsus paradoxus, and pericardial rub depending on the type, and severity of tamponade. The electrocardiogram in cardiac tamponade usually demonstrates sinus tachycardia, and may sometimes show reduced QRS voltage and electrical alternans. Chest X ray will demonstrate pneumopericardium and cardiac silhouette changes. Echocardiography findings include pericardial effusion, diastolic compression of the RV, diastolic compression of the right atrium (RA), plethora of the inferior vena cava and paradoxical septal motion. Pericardiocentesis can provide a diagnostic sampling of pericardial fluid and can be used as a therapeutic maneuver to evacuate pericardial fluid and lower the pericardial pressure.
Historical Perspective
Cardiac tamponade is a very common emergent manifestation, which can be caused by traumatic injuries, since the emulation of the disease tracks back to centuries ago. Acknowledgment of existing pericardial is first done by hippocrates, which was continued by Galen to describing what is now known as pericardial effusion.
Classification
Cardiac tamponade is an emergency form of cardiac effusion. it is more over classified by the pathological causes. The management of emergent situation is not very differed by the basic cause.
Pathophysiology
Cardiac tamponade occurs when the pericardial space fills up with fluid faster than the pericardial sac can stretch. If the amount of fluid increases slowly (such as in hypothyroidism) the pericardial sac can expand to contain a liter or more of fluid prior to tamponade occurring. If the fluid occurs rapidly (as may occur after trauma or myocardial rupture) as little as 100 ml can cause tamponade. However, if the volume of the fluid accumulation is too rapid and or large, then the hemodynamic compromise can occur with a rise in pericardial pressure. This in turn reduces stroke volume, and eventually, cardiac output. If fluid continues to accumulate, then with each successive diastole, less and less blood enters the ventricles, as the increasing pressure presses on the heart and forces the septum to bend into the left ventricle, leading to a decreased stroke volume.
Causes
Cardiac tamponade is caused by the accumulation of a large or uncontrolled pericardial effusion. The effusion can occur rapidly (as in the case of trauma or myocardial rupture), or over a more gradual period of time (as in cancer). The fluid involved is often blood, but pus is also found in some circumstances. Common causes of increased pericardial effusion include hypothyroidism, trauma (either penetrating trauma involving the pericardium or blunt chest trauma), pericarditis (inflammation of the pericardium), iatrogenic trauma (during an invasive procedure), and ventricular rupture.
Differentiating cardiac tamponade from Other Diseases
The initial diagnosis of cardiac tamponade can be challenging, as there are a number of differential diagnoses, including tension pneumothorax, hypovolemia and acute congestive heart failure. The differential diagnosis of cardiac tamponade differs based on the type of cardiac tamponade (either acute or subacute).
Epidemiology and Demographics
The cardiac tamponade is most often attributed to the rupture of an acute myocardial infarction or an intrapericardial rupture of a dissecting ascending aortic aneurysm. In developed countries malignancy is the leading cause of cardiac tamponade secondary to pericardial effusion. The incidence of cardiac tamponade based on a giant sample size of about 216 million emergency admissions was about 115,638(0.05%). The incidence of cardiac tamponade increases with age; the mean age was around 61.9. Cardiac temponade mortality rate is significantly different due to its underlying cause.
Risk Factors
Most potent risk factors for cardiac tamponade include heart surgeries, cardiac myxomas, myocardial infarction and traumas.
Screening
Cardiac tamponade is more of a clinical diagnosis. If the patient clinical manifestation was raising suspicious toward tamponade, CT scan and echocardiogram are diagnostic gold standards for the disease.
Natural History, Complications, and Prognosis
Cardiac tamponade is a life-threatening condition requiring urgent intervention to remove the pericardial fluid. Complications include pulmonary edema, cardiac failure, cardiogenic shock and ultimately death.
Cardiac tamponade has a good prognosis if detected early and treated immediately. Short-term survival is mostly dependent on early diagnosis and relief of tamponade. Long-term survival depends upon the prognosis of the underlying cause, irrespective of the mode of treatment.
Diagnosis
Diagnostic Study of Choice
Cardiac tamponade is more of a clinical diagnosis, but still some diagnostic studies may be helpful.
History and Symptoms
Patients with cardiac tamponade may present with sudden onset of chest pain, palpitations, breathlessness and lightheadedness. Presentation vary with the cause and acuteness of development of tamponade. An acute cardiac tamponade follows trauma to the chest or rupture of the aorta or heart. A subacute cardiac tamponade occurs in the setting of a neoplasm or renal failure. A low pressure cardiac tamponade occurs in patients who are hypovolemic secondary to hemorrhage or over diuresis.
Physical Examination
Physical examination may vary depending on the type of cardiac tamponade. Physical examination may show the classic Beck’s triad (hypotension, muffled heart sound, and elevated jugular venous distension), tachycardia, pulsus paradoxus, and pericardial rub depending on the type, and severity of tamponade. Initial diagnosis can be challenging, as there are a number of differential diagnoses, including tension pneumothorax, and acute heart failure.
Laboratory Findings
Non-specific markers of inflammation are generally elevated in pericarditis. This include the CBC, elevated C-reactive protein, ESR. The cardiac troponin is elevated if there is injury to the underlying myocardium, a condition termed myopericarditis. Diagnostic pericardiocentesis and biopsy help in identifying an underlying infectious or malignant process.
Electrocardiogram
The electrocardiogram in cardiac tamponade usually demonstrates sinus tachycardia, and may sometimes show reduced QRS voltage and electrical alternans.
X-ray
Cardiac tamponade is a clinical diagnosis, however chest X ray can be helpful sometimes. It will demonstrate pneumopericardium and cardiac silhouette changes.
Echocardiography and Ultrasound
The role of echocardiography in the evaluation of the patient with pericarditis is to characterize the presence, size, location and hemodynamic impact of a pericardial effusion. Tamponade is characterized by pericardial effusion, diastolic compression of the RV, diastolic compression of the right atrium (RA), plethora of the inferior vena cava and paradoxical septal motion.
CT scan
A CT scan is not commonly used for the diagnosis of cardiac tamponade as it is effectively diagnosed based on clinical features and echocardiography. Findings on CT include [Superior vena cava]] andInferior vena cava enlargement, Hepatic and renal vein enlargment, periportal edema, reflux of contrast material, collapse of the right atrium, Pericardial thickening.
MRI
Cardiovascular MRI is not commonly used for the diagnosis of cardiac tamponade as it is effectively diagnosed based on clinical features and echocardiography. Findings include Pericardial effusion, distension of the vena cavae and hepatic vein, collapse of the right sided cardiac chambers, interventricular septum shifts towards the left, paradoxical septal motion.
Other Imaging Findings
There are no other imaging findings associated with cardiac tamponade.
Other Diagnostic Studies
There are no other diagnostic studies associated with cardiac tampnoade.
Treatment
Medical Therapy
If the patient is symptomatic, and if there are signs of cardiac tamponade, urgent pericardiocentesis should be performed. Additional supportive therapy includes the administration of oxygen, fluid repletion, echocardiographic monitoring, treatment of underlying pathology, reversal of anticoagulation and monitoring.
Surgery
Percutaneous pericardiocentesis is a procedure where fluid is aspirated from the pericardium (the sac enveloping the heart) using a needle via a percutaneous approach. Pericardiocentesis can provide a diagnostic sampling of pericardial fluid and can be used as a therapeutic maneuver to evacuate pericardial fluid and lower the pericardial pressure.
Primary Prevention
There are no established measures for the primary prevention of cardiac tamponade.
Secondary Prevention
There are no established measures for the secondary prevention of cardiac tamponade.
References
Anatomy
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
The pericardium is a double-walled sac that contains the heart and the roots of the great vessels.
Overview
Layers
There are two layers to the pericardial sac: the fibrous pericardium and the serous pericardium. The serous pericardium, in turn, is divided into two layers, the parietal pericardium, which is fused to and inseparable from the fibrous pericardium, and the visceral pericardium, which is in fact the epicardium, or the outer surface of the heart.
In between the parietal and visceral pericardial layers there is a potential space called the pericardial cavity. It is normally lubricated by a film of pericardial fluid. Too much fluid in the cavity (such as in a pericardial effusion) can result in pericardial tamponade, which refers to compression of the heart within the pericardial sac.
Pericardial Sinuses
There are two small chambers or sinuses are located where the visceral and parietal pericardia are continuous with one another within the pericardial cavity.
The pericardial sinuses are:
- Oblique pericardial sinus
- Transverse pericardial sinus


Additional Images
-
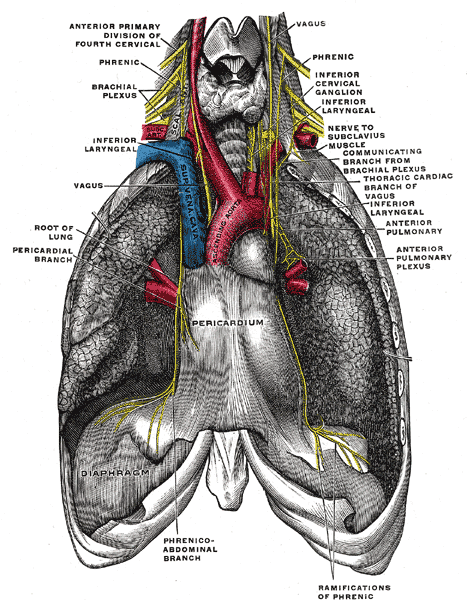 The phrenic nerve and its relations with the vagus nerve.
The phrenic nerve and its relations with the vagus nerve. -
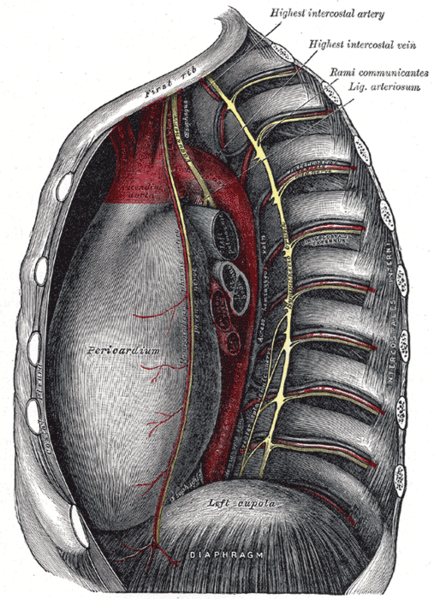 Thoracic portion of the sympathetic trunk.
Thoracic portion of the sympathetic trunk. -
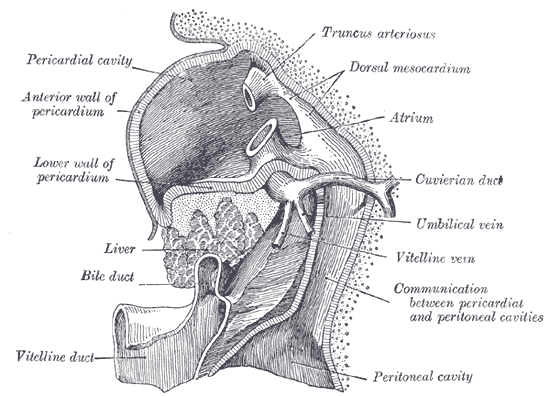 Liver with the septum transversum. Human embryo 3 mm long.
Liver with the septum transversum. Human embryo 3 mm long. -
 The thymus of a full-time fetus, exposed in situ.
The thymus of a full-time fetus, exposed in situ.




Diseases of the Pericardium
- Pericarditis is an inflammatory condition of the pericardium.
- Pericardial effusion is fluid accumulation in the pericardial sac.
- Constrictive pericarditis occurs when there is a scar encasing the heart that chronically constricts the filling of the heart.
- Cardiac tamponade is a medical emergency in which fluid in the pericardial sac acutely restricts the filling of the heart. This requires surgical drainage or pericardiocentesis.
References
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Varun Kumar, M.B.B.S. Ramyar Ghandriz MD[3]
Overview
Cardiac tamponade occurs when the pericardial space fills up with fluid faster than the pericardial sac can stretch. If the amount of fluid increases slowly (such as in hypothyroidism) the pericardial sac can expand to contain a liter or more of fluid prior to tamponade occurring. If the fluid occurs rapidly (as may occur after trauma or myocardial rupture) as little as 100 ml can cause tamponade. However, if the volume of the fluid accumulation is too rapid and or large, then the hemodynamic compromise can occur with a rise in pericardial pressure. This in turn reduces stroke volume, and eventually, cardiac output. If fluid continues to accumulate, then with each successive diastole, less and less blood enters the ventricles, as the increasing pressure presses on the heart and forces the septum to bend into the left ventricle, leading to a decreased stroke volume.
Pathophysiology
Anatomy and Physiology of Pericardium
Layers of the Pericardium
- The pericardium is made up of two layers[1][2][3][4]
- Fibrous pericardium
- Serous pericardium
- Smooth internal layer made up of 2 components:
- Parietal: reflects onto fibrous pericardium
- Visceral: reflects onto heart and great vessels and forms the epicardium, the external layer of the heart wall
- Smooth internal layer made up of 2 components:
- Pericardial cavity: Potential space between parietal and visceral layers. It contains a serous fluid film that occupies the cavity and functions as lubricant against friction by all chest movements.
Pericardial Sinuses
- There are two small chambers or sinuses located where the visceral and parietal pericardia are continuous with one another within the pericardial cavity.[5][6][7]
- Transverse sinus:
- Located posterior to the pulmonary trunk and ascending aorta at the level between the superior vena cava and aortic arch
- Formed after dorsal mesocardium rupture embryonically
- Functional role is to allow the unhindered expansion of great arteries posteriorly during cardiac systole
- Utilized surgically to pass surgical clamps or place ligatures around great arteries.
- Oblique sinus:
- A blind recess (cul-de-sac) posterior to the left atrium between superior vena cava, right and left pulmonary veins inferior to the transverse sinus
- Formed embryonically by the incorporation of the pulmonary vein tributaries into the left atrium
- Functional role believed to be the expansion of the left atrium upon the normal collapse of the thorax
Pathogenesis
- The outer pericardium is made of fibrous tissue which does not easily stretch, and so once fluid begins to enter the pericardial space, pressure starts to increase. This causes obstructive shock to develop, and if left untreated, cardiac arrest may occur (in which case the presenting rhythm is likely to be Pulseless electrical activity). [8][9][10].
- Ordinarily, drainage from the pericardium occurs via the thoracic duct and the right lymphatic duct into the right pleural space. In the absence of disease, the normal pericardium contains only 20-50 cc of serous fluid due to ultrafiltration from the blood. Up to about 75 cc can accumulate acutely in the pericardium without hemodynamic compromise. Much greater amounts of fluid can accumulate chronically over a prolonged period of time as the pericardial sac stretches slowly to accommodate the fluid without hemodynamic compromise. However, if the volume of the fluid accumulation is too rapid and or large, then the hemodynamic compromise can occur with a rise in pericardial pressure. This in turn reduces stroke volume, and eventually, cardiac output.
- If fluid continues to accumulate, then with each successive diastole, less and less blood enters the ventricles, as the increasing pressure presses on the heart and forces the septum to bend into the left ventricle, leading to a decreased stroke volume.
Below is a video demonstrating hemorrhagic effusion leading to cardiac tamponade. {{#ev:youtube|QwgfuDegC5Y}}
Gross Pathology
-
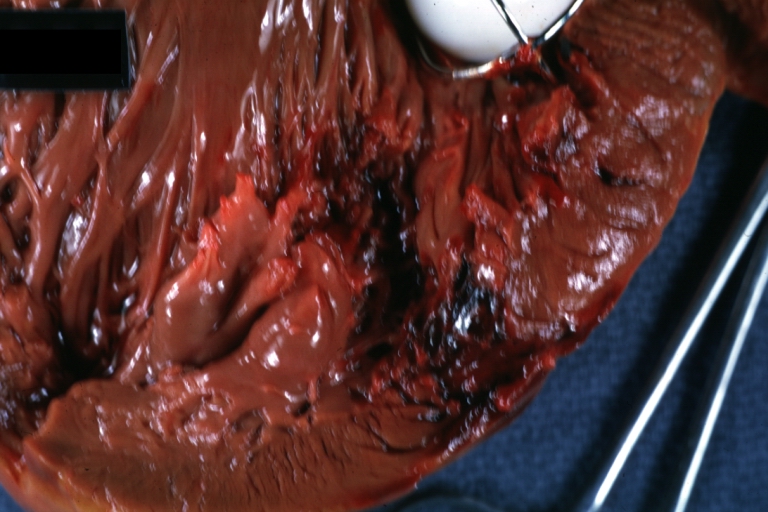
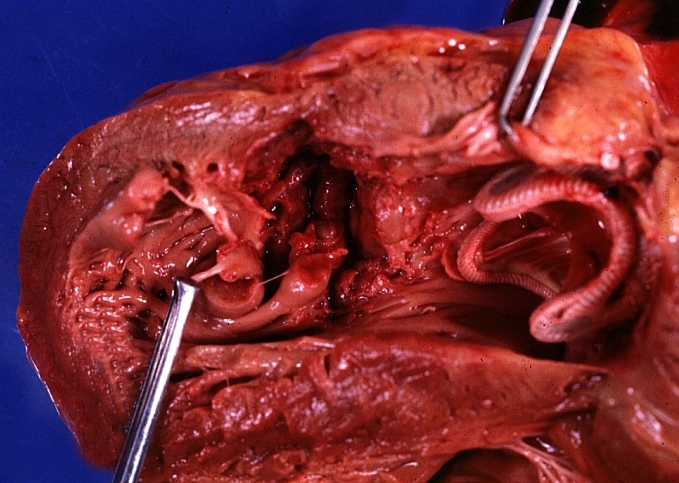 HEART: Myocardial Rupture Following Mitral Valve Replacement: Gross, an excellent example with valve and obviously ruptured heart wall.
HEART: Myocardial Rupture Following Mitral Valve Replacement: Gross, an excellent example with valve and obviously ruptured heart wall. -
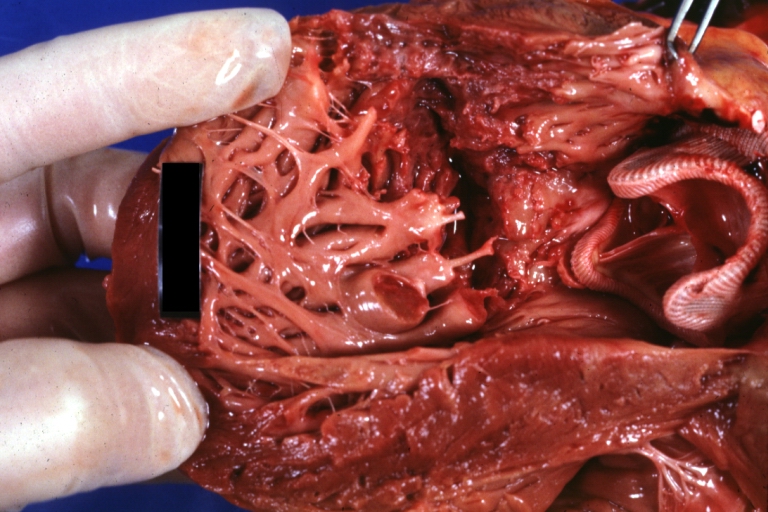
![HEART: Myocardial Rupture Following Mitral Valve Replacement: Gross, natural color view from within left ventricle caged plastic ball with steel complete struts [11]](https://www.wikidoc.org/images/a/a2/Myocardial_rupture_2.jpg) HEART: Myocardial Rupture Following Mitral Valve Replacement: Gross, natural color view from within left ventricle caged plastic ball with steel complete struts [11]
HEART: Myocardial Rupture Following Mitral Valve Replacement: Gross, natural color view from within left ventricle caged plastic ball with steel complete struts [11]

![HEART: Myocardial Rupture Following Mitral Valve Replacement: Gross, natural color view from within left ventricle caged plastic ball with steel complete struts [11]](https://www.wikidoc.org/index.php/File%3AMyocardial_rupture_2.jpg)
-
 HEART: Myocardial Rupture Following Mitral Valve Replacement: Gross, natural color portion of caged plastic ball prosthesis shown with close-up of ruptured left ventricular wall
HEART: Myocardial Rupture Following Mitral Valve Replacement: Gross, natural color portion of caged plastic ball prosthesis shown with close-up of ruptured left ventricular wall -
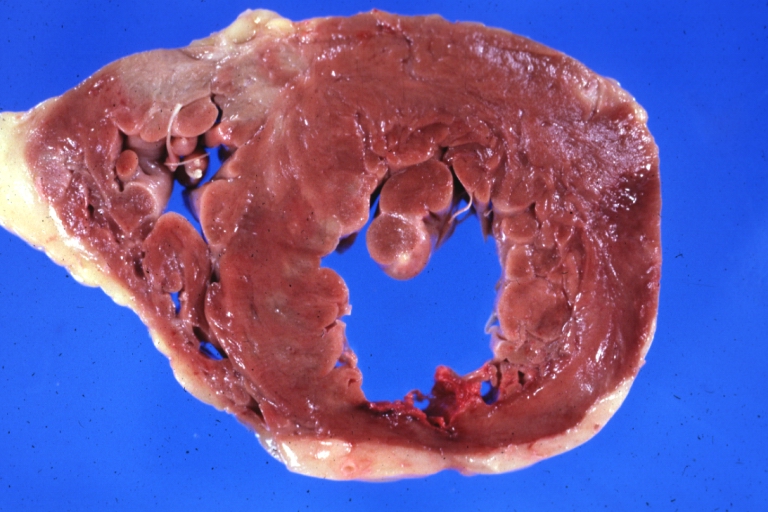
 HEART: Myocardial Rupture Following Mitral Valve Replacement: Gross, natural color close-up view of torn myocardium and bottom of hetero or homograft valve
HEART: Myocardial Rupture Following Mitral Valve Replacement: Gross, natural color close-up view of torn myocardium and bottom of hetero or homograft valve


-
 HEART: Infarct; Acute, Ruptured: Gross, natural color horizontal section ventricle anterior infarct not easily appreciated with thinning of myocardium
HEART: Infarct; Acute, Ruptured: Gross, natural color horizontal section ventricle anterior infarct not easily appreciated with thinning of myocardium -
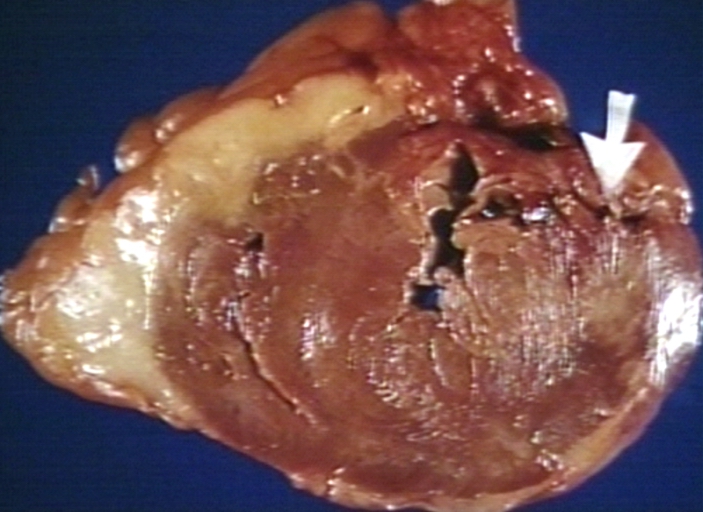 HEART: Rupture after myocardial infarction.
HEART: Rupture after myocardial infarction.


References
- ↑ *Fornauer, Andrew (2003). “Pericardial Tamponade Complicating Central Venous Interventions”. Journal of Vascular and Interventional Radiology. PMID 12582195. Unknown parameter
|coauthors=ignored (help); Unknown parameter|month=ignored (help) - ↑ Kishore, K. (2003). The Heart of Structural Development: The Functional Basis of the Location and Morphology of the Human Vascular Pump. J Postgrad Med, 49:282-4.
- ↑ Moore, K. L., Agur, A. M., & Dalley, A. F. (2011). Essential Clinical Anatomy – Fourth Edition. Lippincott Williams & Wilkins.
- ↑ Tank, P. W. (2009). Grant’s Dissector – Fourteenth Edition. Lippincott Williams & Wilkins.
- ↑ Kishore, K. (2003). The Heart of Structural Development: The Functional Basis of the Location and Morphology of the Human Vascular Pump. J Postgrad Med, 49:282-4.
- ↑ Moore, K. L., Agur, A. M., & Dalley, A. F. (2011). Essential Clinical Anatomy – Fourth Edition. Lippincott Williams & Wilkins.
- ↑ Tank, P. W. (2009). Grant’s Dissector – Fourteenth Edition. Lippincott Williams & Wilkins.
- ↑ Mattson Porth, C. (Ed.) (2005) (7th Ed.) Pathophysiology: Concepts of Altered Health States. Philadelphia : Lippincott Williams & Wilkins ISBN 978-0781749886
- ↑ Mattson Porth, C. (Ed.) (2005) (7th Ed.) Pathophysiology: Concepts of Altered Health States. Philadelphia : Lippincott Williams & Wilkins ISBN 978-0781749886
- ↑ Thibodeau, G.A., Patton, K.T. (2000). Anatomy & Physiology. Missouri: Mosby ISBN 9780323010962
- ↑ Habibi R, Faramarzi N, Altamirano AJ, Dadkhah S (2018). “A Patient Presenting with Cardiac Tamponade and the Challenges of Finding Its Cause: A Cardiac Angiosarcoma”. Case Rep Cardiol. 2018: 2084390. doi:10.1155/2018/2084390. PMC 5851018. PMID 29682355.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Varun Kumar, M.B.B.S.
Overview
Cardiac tamponade is caused by the accumulation of a large or uncontrolled pericardial effusion. The effusion can occur rapidly (as in the case of trauma or myocardial rupture), or over a more gradual period of time (as in cancer). The fluid involved is often blood, but pus is also found in some circumstances. Common causes of increased pericardial effusion include hypothyroidism, trauma (either penetrating trauma involving the pericardium or blunt chest trauma), pericarditis (inflammation of the pericardium), iatrogenic trauma (during an invasive procedure), and ventricular rupture.
Causes
Life Threatening Causes
Life-threatening causes include conditions which may result in death or permanent disability within 24 hours if left untreated. Any cause of pericardial effusion capable of compromising the hemodynamic status of a patient is potentially life threatening.[1][2]
Common Causes
The most common cause of cardiac tamponade include the following[3][4][5][6][7][8][9]
- Ascending aortic dissection
- Collagen vascular diseases
- Iatrogenic – central line insertion, pacemaker insertion, coronary interventions, myocardial biopsy
- Idiopathic
- Malignancy – breast cancer, Kaposi’s sarcoma, lung cancer, lymphomas
- Penetrating trauma
- Pericarditis
- Bacteria – pneumococcus, streptococcus, staphylococcus
- Fungus – blastomyces, cryptococcus, histoplasma, pneumocystis carinii
- Tuberculous
- Virus – coxsackie virus, echovirus, CMV
Causes by Organ System
Causes in Alphabetical Order
References
- ↑ Mattson Porth, C. (Ed.) (2005) (7th Ed.) Pathophysiology: Concepts of Altered Health States. Philadelphia : Lippincott Williams & Wilkins ISBN 978-0781749886
- ↑ Mattson Porth, C. (Ed.) (2005) (7th Ed.) Pathophysiology: Concepts of Altered Health States. Philadelphia : Lippincott Williams & Wilkins ISBN 978-0781749886
- ↑ Mittal A, Ray A, Talupula RM, Sood R (February 2018). “Sheehan’s syndrome presenting as cardiac tamponade”. BMJ Case Rep. 2018. doi:10.1136/bcr-2017-223129. PMC 5812377. PMID 29431100.
- ↑ Kurth BJ, Wagler V, Keith M (September 2016). “Cardiac tamponade as a manifestation of severe dermatomyositis”. BMJ Case Rep. 2016. doi:10.1136/bcr-2016-216860. PMC 5051378. PMID 27664227.
- ↑ Fadel R, El-Menyar A, ElKafrawy S, Gad MG (2019). “Traumatic blunt cardiac injuries: An updated narrative review”. Int J Crit Illn Inj Sci. 9 (3): 113–119. doi:10.4103/IJCIIS.IJCIIS_29_19. PMC 6792398 Check
|pmc=value (help). PMID 31620349. - ↑ Almehmadi F, Chandy M, Connelly KA, Edwards J (2016). “Delayed Tamponade after Traumatic Wound with Left Ventricular Compression”. Case Rep Cardiol. 2016: 2154748. doi:10.1155/2016/2154748. PMC 5019924. PMID 27651957.
- ↑ Zadra AR, Ripellino P, Barzaghi N (April 2015). “Cardiac tamponade as presenting symptom of tuberculosis”. BMJ Case Rep. 2015. doi:10.1136/bcr-2014-208787. PMC 4422911. PMID 25926581.
- ↑ Chiu MH, Sharma NC (July 2018). “A case of hypertensive emergency, primary hypothyroidism and large pericardial effusion with early tamponade”. J Cardiol Cases. 18 (1): 29–32. doi:10.1016/j.jccase.2018.03.005. PMC 6149587. PMID 30279905.
- ↑ Sinha A, Yeruva SL, Kumar R, Curry BH (2015). “Early Cardiac Tamponade in a Patient with Postsurgical Hypothyroidism”. Case Rep Cardiol. 2015: 310350. doi:10.1155/2015/310350. PMC 4534597. PMID 26294982.
Differentiating Cardiac Tamponade from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Priyamvada Singh, M.D. [2]Ramyar Ghandriz MD[3]
Overview
The initial diagnosis of cardiac tamponade can be challenging, as there are a number of differential diagnoses, including tension pneumothorax, hypovolemia and acute congestive heart failure. The differential diagnosis of cardiac tamponade differs based on the type of cardiac tamponade (either acute or subacute).
Differentiating Cardiac Tamponade from Other Diseases
Differential Diagnosis of Acute Cardiac Tamponade
In a trauma patient presenting with PEA (pulseless electrical activity) in the absence of hypovolemia and tension pneumothorax, the most likely diagnosis is cardiac tamponade.[1] Other acute disorders that cardiac tamponade must be distinguished from include:
- Aortic dissection
- Congestive heart failure
- Hypovolemia
- Pulmonary embolus
- Right ventricular myocardial infarction
- Tension pneumothorax
Differential Diagnosis of Subacute Cardiac Tamponade
Signs of classical cardiac tamponade include three signs, known as Beck’s triad. Hypotension occurs because of decreased stroke volume, jugular-venous distension due to impaired venous return to the heart, and muffled heart sounds due to fluid inside the pericardium.[2]
Other signs of tamponade include pulsus paradoxus (a drop of at least 10mmHg in arterial blood pressure on inspiration), and ST segment changes on the electrocardiogram, which may also show low voltage QRS complexes, as well as general signs & symptoms of shock (such as tachycardia, breathlessness and decreasing level of consciousness).
Echocardiography, which is the diagnostic test of choice, often demonstrates an enlarged pericardium or collapsed ventricles. Tamponade can often be diagnosed radiographically, if time allows and the chest x-ray may show a large, globular heart if the pericardial effusion is large.
Differential table
| Type of Shock | Etiology | CO | SVR | PCWP | CVP | SVO2 | RVS | RVD | PAS | PAD |
| Cardiogenic | Acute Ventricular Septal Defect | ↓↓ | ↑ | N — ↑ | ↑↑ | ↑ — ↑↑ | N — ↑ | ↑ | N — ↑ | N — ↑ |
| Acute Mitral Regurgitation | ↓↓ | ↑ | ↑↑ | ↑ — ↑↑ | ↓ | ↑ | N — ↑ | ↑ | ↑ | |
| Myocardial Dysfunction | ↓↓ | ↑ | ↑↑ | ↑↑ | ↓ | N — ↑ | N — ↑ | N — ↑ | ↑ | |
| Right Ventricular Infarction | ↓↓ | ↑ | N — ↓ | ↑↑ | ↓ | ↓ — ↑ | ↑ | ↓ — ↑ | ↓ — ↑ | |
| Obstructive | Pulmonary Embolism | ↓↓ | ↑ | N — ↓ | ↑↑ | ↓ | ↓ — ↑ | ↑ | ↓ — ↑ | ↓ — ↑ |
| Cardiac Tamponade | ↓ — ↓↓ | ↑ | ↑↑ | ↑↑ | ↓ | N — ↑ | ↑ | N — ↑ | N — ↑ | |
| Distributive | Septic Shock | N — ↑↑ | ↓ — ↓↓ | N — ↓ | N — ↓ | ↑ — ↑↑ | N — ↓ | N — ↓ | ↓ | ↓ |
| Anaphylactic Shock | N — ↑↑ | ↓ — ↓↓ | N — ↓ | N — ↓ | ↑ — ↑↑ | N — ↓ | N — ↓ | ↓ | ↓ | |
| Hypovolemic | Volume Depletion | ↓↓ | ↑ | ↓↓ | ↓↓ | ↓ | N — ↓ | N — ↓ | ↓ | ↓ |
- Note that that in Obstructive shock PCWP (left atrial pressure) which is an indicator of left circulation preload , decreases, but in tamponade it increases paradoxically due to pericardial effusion pressure on left atrium.
The following table outlines the major differential diagnoses of Shock on the basis of clinical manifestations..[5][6][7][8][9][10][11][12][13][14][15][16][17][18][19][20][21][22][23][24][25][26][27][28][29][30][31][32][33][34][35][36][37][38][39][40]
Abbreviations: ABG (arterial blood gas); ACE (angiotensin converting enzyme); BMI (body mass index); CBC (complete blood count); CSF (cerebrospinal fluid); CXR (chest X-ray); ECG (electrocardiogram); FEF (forced expiratory flow rate); FEV1 (forced expiratory volume); FVC (forced vital capacity); JVD (jugular vein distention); MCV (mean corpuscular volume); Plt (platelet); RV (residual volume); SIADH (syndrome of inappropriate antidiuretic hormone); TSH (thyroid stimulating hormone); Vt (tidal volume); WBC (white blood cell); Coronary CT angiography (CCTA); multidetector row scanners (MDCT); Cardiovascular magnetic resonance — CMRI; Myocardial perfusion imaging (MPI); single-photon emission CT (SPECT); Positron emission tomography (PET) scanning; Magnetic resonance (MR) angiography, Computed tomographic (CT) angiography, and Transesophageal echocardiography (TEE), late gadolinium enhancement (LGE); right ventricular hypertrophy (RVH), right atrial enlargement (RAE), functional tricuspid regurgitation (TR), Pulmonary artery systolic pressure (PASP; adenosine deaminase (ADA); Serum amyloid A (SAA), soluble interleukin-2 receptor (sIL2R); High-resolution CT (HRCT) scanning
| Differentials on the basis of Etiology | Disease | Clinical manifestations | Diagnosis | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Symptoms | Risk factors | Physical exam | Lab Findings | EKG | Imaging | Gold standard | |||||||||
| Onset | Duration | Quality of Pain | Cough | Fever | Dyspnea | Weight loss | Associated Features | ||||||||
| Pericardial Tamponade[41][42] | Acute or subacute | May last for hours to days |
|
+/- | + | + | – |
|
EKG findings:
|
|
|||||
| Myocardial Infarction[5][6][7][8] | Acute | Commonly > 20 minutes |
|
– | – | + | – |
|
|
|
|
| |||
| Cardiac | |||||||||||||||
| Aortic Dissection[43][44] | Sudden severe progressive pain (common) or chronic (rare) | Variable |
|
– | – | + | – |
|
|
|
|
|
| ||
| Aortic intramural hematoma | Sudden severe progressive pain (common) or chronic (rare) | Variable |
|
– | – | + | – |
|
|
|
|
|
| ||
| Penetrating atherosclerotic aortic ulcer[45][46][47] | Sudden severe pain | Variable |
|
– | – | + | – |
|
_ |
_ |
|
| |||
| Myocarditis[48][49][50] | Acute or subacute | Variable |
|
+/- | + | + | – |
|
|
|
|
||||
| Hypertrophic cardiomyopathy[51][52][53] | Acute or subacute | Variable | Typical or atypical chest pain | – | – | + | – |
|
|
|
Non-specific |
|
|
Genetic testing for HCM | |
| Stress (takotsubo) | Acute | Commonly > 20 minutes |
|
– | – | + | – |
|
Stress |
|
|
|
|||
| Aortic Stenosis[58][59][60] | Acute, recurrent episodes of angina | 2-10 minutes |
|
– | – | + | – |
|
|
|
|
|
|||
| Heart Failure[61][62][63] | Subacute or chronic | Variable |
|
+ | +/- | + | + | Dyslipidemia, hypertension, smoking, family history of premature disease, and diabetes |
|
|
|
||||
| Differentials on the basis of Etiology | Disease | Clinical manifestations | Diagnosis | ||||||||||||
| Symptoms | Risk factors | Physical exam | Lab Findings | EKG | Imaging | Gold standard | |||||||||
| Onset | Duration | Quality of Pain | Cough | Fever | Dyspnea | Weight loss | Associated Features | ||||||||
| Pulmonary | Pulmonary Embolism[64][65] | Acute | May last minutes to hours |
|
+ | +/- | + | – |
|
Hormone replacement therapy
Cancer Oral contraceptive pills Stroke Pregnancy Postpartum Prior history of VTE Thrombophilia |
|
|
|
||
| Spontaneous Pneumothorax[66][67] | Acute | May last minutes to hours |
|
– | – | + | – |
|
|
|
|
|
| ||
| Tension Pneumothorax[68][69] | Acute | May last minutes to hours |
|
– | – | + | – |
|
|
|
|
||||
| Pleural Effusion[70][71][72] | Acute or subacute or chronic | Variable |
|
+ | +/- | + | +/- |
|
|
|
|
||||
| Acute chest syndrome (Sickle cell anemia)[73][74][75] | Acute | May last minutes to hours |
|
+ | +/- | + | – |
|
|
|
|
|
— | ||
| Differentials on the basis of Etiology | Disease | Clinical manifestations | Diagnosis | ||||||||||||
| Symptoms | Risk factors | Physical exam | Lab Findings | EKG | Imaging | Gold standard | |||||||||
| Onset | Duration | Quality of Pain | Cough | Fever | Dyspnea | Weight loss | Associated Features | ||||||||
| Gastrointestinal | Perforated Peptic Ulcer[76][77][78] | Acute |
|
|
+/- | – | – | +/- |
|
|
|
|
|
| |
| Esophagitis[79][80][81] | Acute | Variable |
|
+ | + | – | +/- |
|
|
|
|||||
| Esophageal Perforation[10] | Acute | Minutes to hours |
|
– | +/- | + | – |
|
|
|
|
|
| ||
| Mediastinitis[82][83][84][85] | Acute, Chronic | Variable |
|
+/- | + | + | – |
|
|
|
|
|
|
CT scan | |
| Pancreatitis[86][87][88][89][90] | Acute, Chronic | Variable |
|
– | + | + | +/- |
|
|
|
|
| |||
| IBD[91] | Acute, Chronic | Variable |
|
– | + | + | + |
|
|
|
|
|
|
| |
References
- ↑ American College of Surgeons Committee on Trauma (2007). Advanced Trauma Life Support for Doctors, 7th Edition. Chicago: American College of Surgeons
- ↑ Holt L, Dolan B (2000). Accident and emergency: theory into practice. London: Baillière Tindall. ISBN 0-7020-2239-X.
- ↑ Parrillo, Joseph E.; Ayres, Stephen M. (1984). Major issues in critical care medicine. Baltimore: William Wilkins. ISBN 0-683-06754-0.
- ↑ Judith S. Hochman, E. Magnus Ohman (2009). Cardiogenic Shock. Wiley-Blackwell. ISBN 9781405179263.
- ↑ 5.0 5.1 Svavarsdóttir AE, Jónasson MR, Gudmundsson GH, Fjeldsted K (June 1996). “Chest pain in family practice. Diagnosis and long-term outcome in a community setting”. Can Fam Physician. 42: 1122–8. PMC 2146490. PMID 8704488.
- ↑ 6.0 6.1 Klinkman MS, Stevens D, Gorenflo DW (April 1994). “Episodes of care for chest pain: a preliminary report from MIRNET. Michigan Research Network”. J Fam Pract. 38 (4): 345–52. PMID 8163958.
- ↑ 7.0 7.1 Bösner S, Becker A, Haasenritter J, Abu Hani M, Keller H, Sönnichsen AC, Karatolios K, Schaefer JR, Seitz G, Baum E, Donner-Banzhoff N (2009). “Chest pain in primary care: epidemiology and pre-work-up probabilities”. Eur J Gen Pract. 15 (3): 141–6. doi:10.3109/13814780903329528. PMID 19883149.
- ↑ 8.0 8.1 Ebell MH (March 2011). “Evaluation of chest pain in primary care patients”. Am Fam Physician. 83 (5): 603–5. PMID 21391528.
- ↑ von Kodolitsch Y, Schwartz AG, Nienaber CA (October 2000). “Clinical prediction of acute aortic dissection”. Arch. Intern. Med. 160 (19): 2977–82. PMID 11041906.
- ↑ 10.0 10.1 Pate JW, Walker WA, Cole FH, Owen EW, Johnson WH (May 1989). “Spontaneous rupture of the esophagus: a 30-year experience”. Ann. Thorac. Surg. 47 (5): 689–92. PMID 2730190.
- ↑ Fleet RP, Dupuis G, Marchand A, Burelle D, Beitman BD (October 1994). “Panic disorder, chest pain and coronary artery disease: literature review”. Can J Cardiol. 10 (8): 827–34. PMID 7954018.
- ↑ Bass C, Chambers JB, Kiff P, Cooper D, Gardner WN (December 1988). “Panic anxiety and hyperventilation in patients with chest pain: a controlled study”. Q. J. Med. 69 (260): 949–59. PMID 3270082.
- ↑ Evans DW, Lum LC (January 1977). “Hyperventilation: An important cause of pseudoangina”. Lancet. 1 (8004): 155–7. PMID 64694.
- ↑ Ros E, Armengol X, Grande L, Toledo-Pimentel V, Lacima G, Sanz G (July 1997). “Chest pain at rest in patients with coronary artery disease. Myocardial ischemia, esophageal dysfunction, or panic disorder?”. Dig. Dis. Sci. 42 (7): 1344–53. PMID 9246027.
- ↑ Ben Freedman S, Tennant CC (April 1998). “Panic disorder and coronary artery spasm”. Med. J. Aust. 168 (8): 376–7. PMID 9594945.
- ↑ Smoller JW, Pollack MH, Wassertheil-Smoller S, Jackson RD, Oberman A, Wong ND, Sheps D (October 2007). “Panic attacks and risk of incident cardiovascular events among postmenopausal women in the Women’s Health Initiative Observational Study”. Arch. Gen. Psychiatry. 64 (10): 1153–60. doi:10.1001/archpsyc.64.10.1153. PMID 17909127.
- ↑ Mehta NJ, Khan IA (November 2002). “Cardiac Munchausen syndrome”. Chest. 122 (5): 1649–53. PMID 12426266.
- ↑ Swap CJ, Nagurney JT (November 2005). “Value and limitations of chest pain history in the evaluation of patients with suspected acute coronary syndromes”. JAMA. 294 (20): 2623–9. doi:10.1001/jama.294.20.2623. PMID 16304077.
- ↑ Marcus GM, Cohen J, Varosy PD, Vessey J, Rose E, Massie BM, Chatterjee K, Waters D (January 2007). “The utility of gestures in patients with chest discomfort”. Am. J. Med. 120 (1): 83–9. doi:10.1016/j.amjmed.2006.05.045. PMID 17208083.
- ↑ Verdon F, Burnand B, Herzig L, Junod M, Pécoud A, Favrat B (September 2007). “Chest wall syndrome among primary care patients: a cohort study”. BMC Fam Pract. 8: 51. doi:10.1186/1471-2296-8-51. PMC 2072948. PMID 17850647.
- ↑ Davies HA, Jones DB, Rhodes J, Newcombe RG (December 1985). “Angina-like esophageal pain: differentiation from cardiac pain by history”. J. Clin. Gastroenterol. 7 (6): 477–81. PMID 4086742.
- ↑ Panju AA, Hemmelgarn BR, Guyatt GH, Simel DL (October 1998). “The rational clinical examination. Is this patient having a myocardial infarction?”. JAMA. 280 (14): 1256–63. PMID 9786377.
- ↑ Berger JP, Buclin T, Haller E, Van Melle G, Yersin B (March 1990). “Right arm involvement and pain extension can help to differentiate coronary diseases from chest pain of other origin: a prospective emergency ward study of 278 consecutive patients admitted for chest pain”. J. Intern. Med. 227 (3): 165–72. PMID 2313224.
- ↑ Yelland MJ (September 2001). “Back, chest and abdominal pain. How good are spinal signs at identifying musculoskeletal causes of back, chest or abdominal pain?”. Aust Fam Physician. 30 (9): 908–12. PMID 11676323.
- ↑ Chan S, Maurice AP, Davies SR, Walters DL (October 2014). “The use of gastrointestinal cocktail for differentiating gastro-oesophageal reflux disease and acute coronary syndrome in the emergency setting: a systematic review”. Heart Lung Circ. 23 (10): 913–23. doi:10.1016/j.hlc.2014.03.030. PMID 24791662.
- ↑ Henrikson CA, Howell EE, Bush DE, Miles JS, Meininger GR, Friedlander T, Bushnell AC, Chandra-Strobos N (December 2003). “Chest pain relief by nitroglycerin does not predict active coronary artery disease”. Ann. Intern. Med. 139 (12): 979–86. PMID 14678917.
- ↑ Pryor DB, Harrell FE, Lee KL, Califf RM, Rosati RA (November 1983). “Estimating the likelihood of significant coronary artery disease”. Am. J. Med. 75 (5): 771–80. PMID 6638047.
- ↑ Buntinx F, Knockaert D, Bruyninckx R, de Blaey N, Aerts M, Knottnerus JA, Delooz H (December 2001). “Chest pain in general practice or in the hospital emergency department: is it the same?”. Fam Pract. 18 (6): 586–9. PMID 11739341.
- ↑ Tierney WM, Roth BJ, Psaty B, McHenry R, Fitzgerald J, Stump DL, Anderson FK, Ryder KW, McDonald CJ, Smith DM (July 1985). “Predictors of myocardial infarction in emergency room patients”. Crit. Care Med. 13 (7): 526–31. PMID 4006491.
- ↑ Sequist TD, Marshall R, Lampert S, Buechler EJ, Lee TH (November 2006). “Missed opportunities in the primary care management of early acute ischemic heart disease”. Arch. Intern. Med. 166 (20): 2237–43. doi:10.1001/archinte.166.20.2237. PMID 17101942.
- ↑ Norell M, Lythall D, Coghlan G, Cheng A, Kushwaha S, Swan J, Ilsley C, Mitchell A (January 1992). “Limited value of the resting electrocardiogram in assessing patients with recent onset chest pain: lessons from a chest pain clinic”. Br Heart J. 67 (1): 53–6. PMC 1024701. PMID 1739527.
- ↑ Law K, Elley R, Tietjens J, Mann S (July 2006). “Troponin testing for chest pain in primary healthcare: a survey of its use by general practitioners in New Zealand”. N. Z. Med. J. 119 (1238): U2082. PMID 16868579.
- ↑ Wilhelmsen L, Rosengren A, Hagman M, Lappas G (July 1998). ““Nonspecific” chest pain associated with high long-term mortality: results from the primary prevention study in Göteborg, Sweden”. Clin Cardiol. 21 (7): 477–82. PMID 9669056.
- ↑ Ruigómez A, Rodríguez LA, Wallander MA, Johansson S, Jones R (April 2006). “Chest pain in general practice: incidence, comorbidity and mortality”. Fam Pract. 23 (2): 167–74. doi:10.1093/fampra/cmi124. PMID 16461444.
- ↑ Robinson JG, Wallace R, Limacher M, Sato A, Cochrane B, Wassertheil-Smoller S, Ockene JK, Blanchette PL, Ko MG (December 2006). “Elderly women diagnosed with nonspecific chest pain may be at increased cardiovascular risk”. J Womens Health (Larchmt). 15 (10): 1151–60. doi:10.1089/jwh.2006.15.1151. PMID 17199456.
- ↑ Geraldine McMahon C, Yates DW, Hollis S (February 2008). “Unexpected mortality in patients discharged from the emergency department following an episode of nontraumatic chest pain”. Eur J Emerg Med. 15 (1): 3–8. doi:10.1097/MEJ.0b013e32827b14cd. PMID 18180659.
- ↑ Yelland M, Cayley WE, Vach W (March 2010). “An algorithm for the diagnosis and management of chest pain in primary care”. Med. Clin. North Am. 94 (2): 349–74. doi:10.1016/j.mcna.2010.01.011. PMID 20380960.
- ↑ Wang WH, Huang JQ, Zheng GF, Wong WM, Lam SK, Karlberg J, Xia HH, Fass R, Wong BC (June 2005). “Is proton pump inhibitor testing an effective approach to diagnose gastroesophageal reflux disease in patients with noncardiac chest pain?: a meta-analysis”. Arch. Intern. Med. 165 (11): 1222–8. doi:10.1001/archinte.165.11.1222. PMID 15956000.
- ↑ Borzecki AM, Pedrosa MC, Prashker MJ (March 2000). “Should noncardiac chest pain be treated empirically? A cost-effectiveness analysis”. Arch. Intern. Med. 160 (6): 844–52. PMID 10737285.
- ↑ Wertli MM, Ruchti KB, Steurer J, Held U (November 2013). “Diagnostic indicators of non-cardiovascular chest pain: a systematic review and meta-analysis”. BMC Med. 11: 239. doi:10.1186/1741-7015-11-239. PMC 4226211. PMID 24207111.
- ↑ Ewart W (March 1896). “Practical Aids in the Diagnosis of Pericardial Effusion, in Connection with the Question as to Surgical Treatment”. Br Med J. 1 (1838): 717–21. PMC 2406464. PMID 20756103.
- ↑ Adler Y, Charron P, Imazio M, Badano L, Barón-Esquivias G, Bogaert J, Brucato A, Gueret P, Klingel K, Lionis C, Maisch B, Mayosi B, Pavie A, Ristić AD, Sabaté Tenas M, Seferovic P, Swedberg K, Tomkowski W, Achenbach S, Agewall S, Al-Attar N, Angel Ferrer J, Arad M, Asteggiano R, Bueno H, Caforio AL, Carerj S, Ceconi C, Evangelista A, Flachskampf F, Giannakoulas G, Gielen S, Habib G, Kolh P, Lambrinou E, Lancellotti P, Lazaros G, Linhart A, Meurin P, Nieman K, Piepoli MF, Price S, Roos-Hesselink J, Roubille F, Ruschitzka F, Sagristà Sauleda J, Sousa-Uva M, Uwe Voigt J, Luis Zamorano J (November 2015). “2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS)”. Eur. Heart J. 36 (42): 2921–64. doi:10.1093/eurheartj/ehv318. PMID 26320112.
- ↑ Takagi H, Ando T, Umemoto T (November 2017). “Meta-Analysis of Circadian Variation in the Onset of Acute Aortic Dissection”. Am. J. Cardiol. 120 (9): 1662–1666. doi:10.1016/j.amjcard.2017.07.067. PMID 28847596.
- ↑ Kojima S, Sumiyoshi M, Nakata Y, Daida H (March 2002). “Triggers and circadian distribution of the onset of acute aortic dissection”. Circ. J. 66 (3): 232–5. PMID 11922269.
- ↑ Eggebrecht, Holger; Baumgart, Dietrich; Schmermund, Axel; Herold, Ulf; Hunold, Peter; Jakob, Heinz; Erbel, Raimund (2003). “Penetrating atherosclerotic ulcer of the aorta: treatment by endovascular stent-graft placement”. Current Opinion in Cardiology. 18 (6): 431–435. doi:10.1097/00001573-200311000-00002. ISSN 0268-4705.
- ↑ Bossone, Eduardo; LaBounty, Troy M; Eagle, Kim A (2018). “Acute aortic syndromes: diagnosis and management, an update”. European Heart Journal. 39 (9): 739–749d. doi:10.1093/eurheartj/ehx319. ISSN 0195-668X.
- ↑ DeMartino, Randall R.; Sen, Indrani; Huang, Ying; Bower, Thomas C.; Oderich, Gustavo S.; Pochettino, Alberto; Greason, Kevin; Kalra, Manju; Johnstone, Jill; Shuja, Fahad; Harmsen, W. Scott; Macedo, Thanila; Mandrekar, Jay; Chamberlain, Alanna M.; Weiss, Salome; Goodney, Philip P.; Roger, Veronique (2018). “Population-Based Assessment of the Incidence of Aortic Dissection, Intramural Hematoma, and Penetrating Ulcer, and Its Associated Mortality From 1995 to 2015”. Circulation: Cardiovascular Quality and Outcomes. 11 (8). doi:10.1161/CIRCOUTCOMES.118.004689. ISSN 1941-7713.
- ↑ Dec GW, Palacios IF, Fallon JT, Aretz HT, Mills J, Lee DC, Johnson RA (April 1985). “Active myocarditis in the spectrum of acute dilated cardiomyopathies. Clinical features, histologic correlates, and clinical outcome”. N. Engl. J. Med. 312 (14): 885–90. doi:10.1056/NEJM198504043121404. PMID 3974674.
- ↑ Caforio AL, Calabrese F, Angelini A, Tona F, Vinci A, Bottaro S, Ramondo A, Carturan E, Iliceto S, Thiene G, Daliento L (June 2007). “A prospective study of biopsy-proven myocarditis: prognostic relevance of clinical and aetiopathogenetic features at diagnosis”. Eur. Heart J. 28 (11): 1326–33. doi:10.1093/eurheartj/ehm076. PMID 17493945.
- ↑ Ukena C, Mahfoud F, Kindermann I, Kandolf R, Kindermann M, Böhm M (April 2011). “Prognostic electrocardiographic parameters in patients with suspected myocarditis”. Eur. J. Heart Fail. 13 (4): 398–405. doi:10.1093/eurjhf/hfq229. PMID 21239404.
- ↑ Elliott PM, Kaski JC, Prasad K, Seo H, Slade AK, Goldman JH, McKenna WJ (July 1996). “Chest pain during daily life in patients with hypertrophic cardiomyopathy: an ambulatory electrocardiographic study”. Eur. Heart J. 17 (7): 1056–64. PMID 8809524.
- ↑ Pasternac A, Noble J, Streulens Y, Elie R, Henschke C, Bourassa MG (April 1982). “Pathophysiology of chest pain in patients with cardiomyopathies and normal coronary arteries”. Circulation. 65 (4): 778–89. PMID 7199403.
- ↑ Webb JG, Sasson Z, Rakowski H, Liu P, Wigle ED (January 1990). “Apical hypertrophic cardiomyopathy: clinical follow-up and diagnostic correlates”. J. Am. Coll. Cardiol. 15 (1): 83–90. PMID 2295747.
- ↑ Sharkey SW, Lesser JR, Zenovich AG, Maron MS, Lindberg J, Longe TF, Maron BJ (February 2005). “Acute and reversible cardiomyopathy provoked by stress in women from the United States”. Circulation. 111 (4): 472–9. doi:10.1161/01.CIR.0000153801.51470.EB. PMID 15687136.
- ↑ Krishnamoorthy P, Garg J, Sharma A, Palaniswamy C, Shah N, Lanier G, Patel NC, Lavie CJ, Ahmad H (July 2015). “Gender Differences and Predictors of Mortality in Takotsubo Cardiomyopathy: Analysis from the National Inpatient Sample 2009-2010 Database”. Cardiology. 132 (2): 131–136. doi:10.1159/000430782. PMID 26159108.
- ↑ Templin C, Ghadri JR, Diekmann J, Napp LC, Bataiosu DR, Jaguszewski M, Cammann VL, Sarcon A, Geyer V, Neumann CA, Seifert B, Hellermann J, Schwyzer M, Eisenhardt K, Jenewein J, Franke J, Katus HA, Burgdorf C, Schunkert H, Moeller C, Thiele H, Bauersachs J, Tschöpe C, Schultheiss HP, Laney CA, Rajan L, Michels G, Pfister R, Ukena C, Böhm M, Erbel R, Cuneo A, Kuck KH, Jacobshagen C, Hasenfuss G, Karakas M, Koenig W, Rottbauer W, Said SM, Braun-Dullaeus RC, Cuculi F, Banning A, Fischer TA, Vasankari T, Airaksinen KE, Fijalkowski M, Rynkiewicz A, Pawlak M, Opolski G, Dworakowski R, MacCarthy P, Kaiser C, Osswald S, Galiuto L, Crea F, Dichtl W, Franz WM, Empen K, Felix SB, Delmas C, Lairez O, Erne P, Bax JJ, Ford I, Ruschitzka F, Prasad A, Lüscher TF (September 2015). “Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy”. N. Engl. J. Med. 373 (10): 929–38. doi:10.1056/NEJMoa1406761. PMID 26332547.
- ↑ Bybee KA, Kara T, Prasad A, Lerman A, Barsness GW, Wright RS, Rihal CS (December 2004). “Systematic review: transient left ventricular apical ballooning: a syndrome that mimics ST-segment elevation myocardial infarction”. Ann. Intern. Med. 141 (11): 858–65. PMID 15583228.
- ↑ Green SJ, Pizzarello RA, Padmanabhan VT, Ong LY, Hall MH, Tortolani AJ (April 1985). “Relation of angina pectoris to coronary artery disease in aortic valve stenosis”. Am. J. Cardiol. 55 (8): 1063–5. PMID 3984868.
- ↑ Silaruks S, Clark D, Thinkhamrop B, Sia B, Buxton B, Tonkin A (2001). “Angina pectoris and coronary artery disease in severe isolated valvular aortic stenosis”. Heart Lung Circ. 10 (1): 14–23. doi:10.1046/j.1444-2892.2001.00060.x. PMID 16352020.
- ↑ Munt B, Legget ME, Kraft CD, Miyake-Hull CY, Fujioka M, Otto CM (February 1999). “Physical examination in valvular aortic stenosis: correlation with stenosis severity and prediction of clinical outcome”. Am. Heart J. 137 (2): 298–306. doi:10.1053/hj.1999.v137.95496. PMID 9924164.
- ↑ Anker SD, Sharma R (September 2002). “The syndrome of cardiac cachexia”. Int. J. Cardiol. 85 (1): 51–66. PMID 12163209.
- ↑ Horwich TB, Kalantar-Zadeh K, MacLellan RW, Fonarow GC (May 2008). “Albumin levels predict survival in patients with systolic heart failure”. Am. Heart J. 155 (5): 883–9. doi:10.1016/j.ahj.2007.11.043. PMID 18440336.
- ↑ Breathett K, Allen LA, Udelson J, Davis G, Bristow M (October 2016). “Changes in Left Ventricular Ejection Fraction Predict Survival and Hospitalization in Heart Failure With Reduced Ejection Fraction”. Circ Heart Fail. 9 (10). doi:10.1161/CIRCHEARTFAILURE.115.002962. PMC 5082710. PMID 27656000.
- ↑ Stein PD, Beemath A, Matta F, Weg JG, Yusen RD, Hales CA, Hull RD, Leeper KV, Sostman HD, Tapson VF, Buckley JD, Gottschalk A, Goodman LR, Wakefied TW, Woodard PK (October 2007). “Clinical characteristics of patients with acute pulmonary embolism: data from PIOPED II”. Am. J. Med. 120 (10): 871–9. doi:10.1016/j.amjmed.2007.03.024. PMC 2071924. PMID 17904458.
- ↑ “Value of the ventilation/perfusion scan in acute pulmonary embolism. Results of the prospective investigation of pulmonary embolism diagnosis (PIOPED)”. JAMA. 263 (20): 2753–9. 1990. PMID 2332918.
- ↑ Bense L, Wiman LG, Hedenstierna G (September 1987). “Onset of symptoms in spontaneous pneumothorax: correlations to physical activity”. Eur J Respir Dis. 71 (3): 181–6. PMID 3678419.
- ↑ Seow A, Kazerooni EA, Pernicano PG, Neary M (February 1996). “Comparison of upright inspiratory and expiratory chest radiographs for detecting pneumothoraces”. AJR Am J Roentgenol. 166 (2): 313–6. doi:10.2214/ajr.166.2.8553937. PMID 8553937.
- ↑ Stark P, Leung A (1996). “Effects of lobar atelectasis on the distribution of pleural effusion and pneumothorax”. J Thorac Imaging. 11 (2): 145–9. PMID 8820023.
- ↑ Jalli R, Sefidbakht S, Jafari SH (April 2013). “Value of ultrasound in diagnosis of pneumothorax: a prospective study”. Emerg Radiol. 20 (2): 131–4. doi:10.1007/s10140-012-1091-7. PMID 23179505.
- ↑ Feinsilver SH, Barrows AA, Braman SS (October 1986). “Fiberoptic bronchoscopy and pleural effusion of unknown origin”. Chest. 90 (4): 516–9. PMID 3757561.
- ↑ Collins TR, Sahn SA (June 1987). “Thoracocentesis. Clinical value, complications, technical problems, and patient experience”. Chest. 91 (6): 817–22. PMID 3581930.
- ↑ Venekamp LN, Velkeniers B, Noppen M (2005). “Does ‘idiopathic pleuritis’ exist? Natural history of non-specific pleuritis diagnosed after thoracoscopy”. Respiration. 72 (1): 74–8. doi:10.1159/000083404. PMID 15753638.
- ↑ Vichinsky EP, Styles LA, Colangelo LH, Wright EC, Castro O, Nickerson B (March 1997). “Acute chest syndrome in sickle cell disease: clinical presentation and course. Cooperative Study of Sickle Cell Disease”. Blood. 89 (5): 1787–92. PMID 9057664.
- ↑ Castro O, Brambilla DJ, Thorington B, Reindorf CA, Scott RB, Gillette P, Vera JC, Levy PS (July 1994). “The acute chest syndrome in sickle cell disease: incidence and risk factors. The Cooperative Study of Sickle Cell Disease”. Blood. 84 (2): 643–9. PMID 7517723.
- ↑ Vichinsky EP, Neumayr LD, Earles AN, Williams R, Lennette ET, Dean D, Nickerson B, Orringer E, McKie V, Bellevue R, Daeschner C, Manci EA (June 2000). “Causes and outcomes of the acute chest syndrome in sickle cell disease. National Acute Chest Syndrome Study Group”. N. Engl. J. Med. 342 (25): 1855–65. doi:10.1056/NEJM200006223422502. PMID 10861320.
- ↑ Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R (August 2006). “The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus”. Am. J. Gastroenterol. 101 (8): 1900–20, quiz 1943. doi:10.1111/j.1572-0241.2006.00630.x. PMID 16928254.
- ↑ Vakil NB, Traxler B, Levine D (August 2004). “Dysphagia in patients with erosive esophagitis: prevalence, severity, and response to proton pump inhibitor treatment”. Clin. Gastroenterol. Hepatol. 2 (8): 665–8. PMID 15290658.
- ↑ Giannini EG, Zentilin P, Dulbecco P, Vigneri S, Scarlata P, Savarino V (February 2008). “Management strategy for patients with gastroesophageal reflux disease: a comparison between empirical treatment with esomeprazole and endoscopy-oriented treatment”. Am. J. Gastroenterol. 103 (2): 267–75. doi:10.1111/j.1572-0241.2007.01659.x. PMID 18289194.
- ↑ Bott S, Prakash C, McCallum RW (August 1987). “Medication-induced esophageal injury: survey of the literature”. Am. J. Gastroenterol. 82 (8): 758–63. PMID 3605035.
- ↑ Parfitt JR, Jayakumar S, Driman DK (September 2008). “Mycophenolate mofetil-related gastrointestinal mucosal injury: variable injury patterns, including graft-versus-host disease-like changes”. Am. J. Surg. Pathol. 32 (9): 1367–72. PMID 18763324.
- ↑ Jaspersen D (March 2000). “Drug-induced oesophageal disorders: pathogenesis, incidence, prevention and management”. Drug Saf. 22 (3): 237–49. PMID 10738847.
- ↑ Loyd JE, Tillman BF, Atkinson JB, Des Prez RM (September 1988). “Mediastinal fibrosis complicating histoplasmosis”. Medicine (Baltimore). 67 (5): 295–310. PMID 3045478.
- ↑ Feigin DS, Eggleston JC, Siegelman SS (January 1979). “The multiple roentgen manifestations of sclerosing mediastinitis”. Johns Hopkins Med J. 144 (1): 1–8. PMID 762913.
- ↑ Garrett HE, Roper CL (December 1986). “Surgical intervention in histoplasmosis”. Ann. Thorac. Surg. 42 (6): 711–22. PMID 3539049.
- ↑ Sherrick AD, Brown LR, Harms GF, Myers JL (August 1994). “The radiographic findings of fibrosing mediastinitis”. Chest. 106 (2): 484–9. PMID 7774324.
- ↑ Dickson AP, Imrie CW (October 1984). “The incidence and prognosis of body wall ecchymosis in acute pancreatitis”. Surg Gynecol Obstet. 159 (4): 343–7. PMID 6237447.
- ↑ Yadav D, Agarwal N, Pitchumoni CS (June 2002). “A critical evaluation of laboratory tests in acute pancreatitis”. Am. J. Gastroenterol. 97 (6): 1309–18. doi:10.1111/j.1572-0241.2002.05766.x. PMID 12094843.
- ↑ Fortson MR, Freedman SN, Webster PD (December 1995). “Clinical assessment of hyperlipidemic pancreatitis”. Am. J. Gastroenterol. 90 (12): 2134–9. PMID 8540502.
- ↑ Lecesne R, Taourel P, Bret PM, Atri M, Reinhold C (June 1999). “Acute pancreatitis: interobserver agreement and correlation of CT and MR cholangiopancreatography with outcome”. Radiology. 211 (3): 727–35. doi:10.1148/radiology.211.3.r99jn08727. PMID 10352598.
- ↑ Stimac D, Miletić D, Radić M, Krznarić I, Mazur-Grbac M, Perković D, Milić S, Golubović V (May 2007). “The role of nonenhanced magnetic resonance imaging in the early assessment of acute pancreatitis”. Am. J. Gastroenterol. 102 (5): 997–1004. doi:10.1111/j.1572-0241.2007.01164.x. PMID 17378903.
- ↑ Colbert, James F.; Schmidt, Eric P.; Faubel, Sarah; Ginde, Adit A. (2017). “Severe Sepsis Outcomes Among Hospitalizations With Inflammatory Bowel Disease”. SHOCK. 47 (2): 128–131. doi:10.1097/SHK.0000000000000742. ISSN 1073-2322.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] ; Associate Editor(s)-in-Chief: Ramyar Ghandriz MD[2]
Overview
The cardiac tamponade is most often attributed to the rupture of an acute myocardial infarction or an intrapericardial rupture of a dissecting ascending aortic aneurysm. In developed countries malignancy is the leading cause of cardiac tamponade secondary to pericardial effusion.The incidence of cardiac tamponade based on a giant sample size of about 216 million emergency admissions was about 115,638(0.05%). The incidence of cardiac tamponade increases with age; the mean age was around 61.9. Cardiac temponade mortality rate is significantly different due to its underlying cause.
Epidemiology and Demographics
Incidence
- The incidence of cardiac tamponade based on a giant sample size of about 216 million emergency admissions was about 115,638(0.05%)[1][2][3][4]
Case-fatality rate/Mortality rate
- Cardiac temponade mortality rate is significantly different due to its underlying cause.[5][1][6]
- Overall, hospitalized mortality rate is around 14.3% and sub groups with higher mortality are :
- Sepsis (odds ratio:3.17)
- Chest trauma (odds ratio:2.15)
- Metastatic cancer:(odds ratio:1.90)
- Acute kidney injury(odds ratio:1.91)
- Idiopathic pericarditis (odds ratio: 0.21, least cause of mortality)
Age
Race
- There is no racial predilection to cardiac tamponade.
Gender
- Cardiac tamponade affects men and women equally.
- There is no study suggesting a meaningful sex difference among diagnosed patients.
Approximate Health Care cost In US
- It needs around 12 days of hospitalization and a mean cost of $160,397.
Developed Countries
- The leading cause of developing tamponade in developed countries is cancer.[7]
References
- ↑ 1.0 1.1 1.2 “CARDIAC TAMPONADE INCIDENCE, DEMOGRAPHICS AND IN-HOSPITAL OUTCOMES: ANALYSIS OF THE NATIONAL INPATIENT SAMPLE DATABASE | JACC: Journal of the American College of Cardiology”.
- ↑ Yerdel MA, Şen O, Zor U, Kara S, Acunaş B (September 2018). “Cardiac Tamponade as a Life-Threatening Complication of Laparoscopic Antireflux Surgery: The Real Incidence and 3D Anatomy of a Heart Injury by Helical Tacks”. J Laparoendosc Adv Surg Tech A. 28 (9): 1041–1046. doi:10.1089/lap.2017.0713. PMC 6157358. PMID 29493372.
- ↑ Ariyarajah V, Spodick DH (2007). “Cardiac tamponade revisited: a postmortem look at a cautionary case”. Tex Heart Inst J. 34 (3): 347–51. PMC 1995065. PMID 17948086.
- ↑ Spodick DH (August 2003). “Acute cardiac tamponade”. N. Engl. J. Med. 349 (7): 684–90. doi:10.1056/NEJMra022643. PMID 12917306.
- ↑ Porte HL, Janecki-Delebecq TJ, Finzi L, Métois DG, Millaire A, Wurtz AJ (1999). “Pericardoscopy for primary management of pericardial effusion in cancer patients”. Eur J Cardiothorac Surg. 16 (3): 287–91. PMID 10554845.
- ↑ You SC, Shim CY, Hong GR, Kim D, Cho IJ, Lee S, Chang HJ, Ha JW, Chang BC, Chung N (2016). “Incidence, Predictors, and Clinical Outcomes of Postoperative Cardiac Tamponade in Patients Undergoing Heart Valve Surgery”. PLoS ONE. 11 (11): e0165754. doi:10.1371/journal.pone.0165754. PMC 5113894. PMID 27855225.
- ↑ 7.0 7.1 Gornik HL, Gerhard-Herman M, Beckman JA (2005). “Abnormal cytology predicts poor prognosis in cancer patients with pericardial effusion”. J Clin Oncol. 23 (22): 5211–6. doi:10.1200/JCO.2005.00.745. PMID 16051963.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] ;Associate Editor(s)-in-Chief: Ramyar Ghandriz MD[2]
Overview
Cardiac tamponade is a life-threatening condition requiring urgent intervention to remove the pericardial fluid. Complications include pulmonary edema, cardiac failure, cardiogenic shock and ultimately death.
Cardiac tamponade has a good prognosis if detected early and treated immediately. Short-term survival is mostly dependent on early diagnosis and relief of tamponade. Long-term survival depends upon the prognosis of the underlying cause, irrespective of the mode of treatment.
Natural History, Complications, and Prognosis
Natural History
- Because of restrictive manners of cardiac tamponade , it causes acute heart failure and increase in blood hydro-static pressure.[1]
- In severe forms, increase in hydro-static pressure and decompensated left and right heart failure causes pulmonary edema, low blood pressure,low brain blood supply and eventually death.
Complications
Cardiac tamponade is a life-threatening condition requiring urgent intervention to remove the fluid from the pericardial cavity. If untreated, the patient may develop the following complications[2]:
- Pulmonary edema due to decreased forward flow of blood from the left ventricle and increased pressures within the pulmonary vasculature.
- Cardiac failure secondary to inadequate ventricular filling and cardiac output.
- Cardiogenic shock
- Pulseless electrical activity
- Death
Complications
Prognosis
- The prognosis of cardiac tamponade depends upon tow factors:
- The underlying condition
- duration of diagnosis and treatment
- The prognosis of a cardiac tamponade is typically good with early recognition and management of the condition and the underlying causes of the tamponade. 3.2% of the total deaths over a 10-year period were attributable to cardiac tamponade in a postmortem study of 14,368 patients in County of Cornwall, UK between 1995 and 2004.[3]
- Cardiac tamponade caused by central venous catheters had a mortality rate of 77% before 1980 and 47% between 1980-1989[4].
- Patients with underlying malignancy has the highest rate of mortality[5]. Short-term survival is mostly dependent on early diagnosis and relief of tamponade. Long-term survival depends upon the prognosis of the underlying cause, irrespective of the mode of treatment[2].
- Tamponade secondary to idiopathic effusion and penetrating chest wounds has been shown to be associated with better outcomes with emergent removal of pericardial fluid.
References
- ↑ Weitzman, L B; Tinker, W P; Kronzon, I; Cohen, M L; Glassman, E; Spencer, F C (1984). “The incidence and natural history of pericardial effusion after cardiac surgery–an echocardiographic study”. Circulation. 69 (3): 506–511. doi:10.1161/01.CIR.69.3.506. ISSN 0009-7322.
- ↑ 2.0 2.1 Markiewicz W, Borovik R, Ecker S (1986). “Cardiac tamponade in medical patients: treatment and prognosis in the echocardiographic era”. Am Heart J. 111 (6): 1138–42. PMID 3716989.
- ↑ Swaminathan A, Kandaswamy K, Powari M, Mathew J (2007). “Dying from cardiac tamponade”. World J Emerg Surg. 2: 22. doi:10.1186/1749-7922-2-22. PMC 2042492. PMID 17822563.
- ↑ Nasim A, Cooper GG, Ah-See AK (1992). “Cardiac tamponade due to central venous catheterization”. J R Coll Surg Edinb. 37 (5): 337–9. PMID 1282555.
- ↑ Soler-Soler J, Sagristà-Sauleda J, Permanyer-Miralda G (2001). “Management of pericardial effusion”. Heart. 86 (2): 235–40. PMC 1729838. PMID 11454853.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | CT | MRI | Echocardiography | Cardiac Catheterization
Treatment
Treatment
Treatment | Pericardiocentesis | Pericardial Window
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Varun Kumar, M.B.B.S.
Overview
If the patient is symptomatic, and if there are signs of cardiac tamponade, urgent pericardiocentesis should be performed. Additional supportive therapy includes the administration of oxygen, fluid repletion, echocardiographic monitoring, treatment of underlying pathology, reversal of anticoagulation and monitoring.
Treatment
Pre-Hospital Care
- There is not much pre-hospital care that can be provided other than general treatment for shock which includes intravenous fluids.
- Some pre-hospital providers will have facilities to provide pericardiocentesis, but this is generally futile if the patient has already suffered a cardiac arrest before arrival of the healthcare professional. [1]Rapid evacuation to a hospital equiped to perform invasive procedures is usually the more appropriate course of action.
Supportive Care
Tamponade presents as a spectrum of illness. There is not much debate about the course of management in the treatment of the very sick or the asymptomatic patient with a large effusion who has no signs or symptoms of cardiac tamponade. The course of treatment is often debated in those patients with echocardiographic evidence of tamponade but no clinical findings. A prudent strategy in these cases is to observe the progression of the disease process and intervene at the onset of any evidence of compromise. Volume repletion, serial echocardiographic and clinical assessment is warranted in these cases.
- Watchful monitoring of a patient’s clinical status
- Serial echocardiography
- Volume repletion (saline, plasma, or blood)
- Treatment of underlying etiology and reversal of anticoagulation
- The role of ionotropic agents is unclear
Hospital Management
If the patient is symptomatic and has signs of cardiac tamponade the initial management in the hospital setting is by urgent pericardiocentesis. [2] This involves aspirating the fluid by inserting a needle through the skin and into the pericardium. Often, a cannula is left in place during resuscitation following initial drainage so that additional fluid can continue to drain. If there is distortion of anatomy, a small effusion, or if the effusion is loculated or located posteriorly, an emergency pericardial window may be performed instead. [3] This procedure involves cutting the pericardium open to allow the fluid to drain. Following stabilization of the patient, surgery is provided to seal the source of the bleed and mend the pericardium.
Drug Contraindication
References
- ↑ Greaves, I., Porter, K. (2007). Oxford handbook of pre-hospital care. Oxford: Oxford University Press ISBN 9780198515845
- ↑ Gwinnutt, C., Driscoll, P. (Eds) (2003) (2nd Ed.) Trauma Resuscitation: The Team Approach. Oxford: BIOS Scientific Publishers Ltd. ISBN 978-1859960097
- ↑ Gwinnutt, C., Driscoll, P. (Eds) (2003) (2nd Ed.) Trauma Resuscitation: The Team Approach. Oxford: BIOS Scientific Publishers Ltd. ISBN 978-1859960097
Related Chapters
Related Chapters
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH