
Cardiovascular physiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Assistant Editor(s)-in-Chief: Rim Halaby
Anatomy of the heart
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Assistant Editor(s)-in-Chief: Rim Halaby, Yazan Daaboul
Synonyms and keywords: Heart anatomy
Sources
- Kishore, K. (2003). The Heart of Structural Development: The Functional Basis of the Location and Morphology of the Human Vascular Pump. J Postgrad Med, 49:282-4.
- Moore, K. L., Agur, A. M., & Dalley, A. F. (2011). Essential Clinical Anatomy – Fourth Edition. Lippincott Williams & Wilkins.
- Tank, P. W. (2009). Grant’s Dissector – Fourteenth Edition. Lippincott Williams & Wilkins.
Coronary circulation
Template:Infobox Anatomy Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Rim Halaby, M.D. [3]
Overview
The coronary circulation is the circulation of blood in the blood vessels that supply blood to and from the heart muscle itself. Although blood fills the chambers of the heart, the muscle tissue of the heart, the myocardium, is so thick that it requires coronary blood vessels to deliver blood deep into it. The coronary arteries are the vessels that deliver oxygen-rich blood to the myocardium. Cardiac veins are the vessels that remove the deoxygenated blood from the heart muscle. Epicardial coronary arteries are the coronary arteries that run on the surface of the heart. These arteries, when healthy, are capable of autoregulation to maintain coronary blood flow at levels appropriate to the needs of the heart muscle. These relatively narrow vessels are commonly affected by atherosclerosis and can become blocked, causing angina or a heart attack. Subendocardial coronary arteries run deep within the myocardium. The coronary arteries are classified as end circulation, since they represent the only source of blood supply to the myocardium: there is very little redundant blood supply, which is why blockage of these vessels can be so critical.
Coronary Arteries and Veins
Coronary Arteries
he coronary arteries supply oxygenated blood to the heart muscle itself. Although blood fills the chambers of the heart, the muscle tissue of the heart, or myocardium, is so thick that it requires coronary blood vessels to deliver blood deep into it. There are two primary arteries supplying the heart, the left coronary artery and the right coronary artery. These two epicardial coronary arteries course along the surface of the heart and this is why they are called “epicardial” (on top of the heart) arteries. Smaller arteries dive deep into the heart muscle and are called subendocardial coronary arteries.
Click here for details about coronary arteries.
Cardiac Veins
The cardiac veins are the vessels that remove the deoxygenated blood from the heart muscle and return it to the right atrium.
Click here for details about cardiac veins.
Shown below is an image depicting the coronary arteries and cardiac veins.

Blood Supply to the Papillary Muscles
- The papillary muscles tether the mitral valve (the valve between the left atrium and the left ventricle) and the tricuspid valve (the valve between the right atrium and the right ventricle) to the wall of the heart.
- If the papillary muscles are not functioning properly, the mitral valve leaks during contraction of the left ventricle and causes some of the blood to travel “in reverse”, from the left ventricle to the left atrium, instead of forward to the aorta and the rest of the body.
- This leaking of blood to the left atrium is known as mitral regurgitation.
- The anterolateral papillary muscle:
- It receives two blood supplies: the LAD and LCX.
- It is therefore somewhat resistant to coronary ischemia (insufficiency of oxygen-rich blood).
- The posteromedial papillary muscle:
- It is supplied only by the PDA.
- This makes the posteromedial papillary muscle significantly more susceptible to ischemia.
- The clinical significance of the nature of blood supply to the papillary muscles is that a myocardial infarction involving the PDA is more likely to cause mitral regurgitation.
Coronary flow
- During contraction of the ventricular myocardium (systole), the subendocardial coronary vessels (the vessels that enter the myocardium) are compressed due to the high intraventricular pressures. However the epicardial coronary vessels (the vessels that run along the outer surface of the heart) remain patent. Because of this, blood flow in the subendocardium stops.
- As a result most myocardial perfusion occurs during heart relaxation (diastole) when the subendocardial coronary vessels are patent and under low pressure. This contributes to the filling difficulties of the coronary arteries.
- Failure of oxygen delivery via increases in blood flow to meet the increased oxygen demand of the heart results in tissue ischemia, a condition of oxygen debt.
- Brief ischemia is associated with intense chest pain, known as angina.
- Severe ischemia can cause the heart muscle to die of oxygen starvation, called a myocardial infarction.
- Chronic moderate ischemia causes contraction of the heart to weaken, known as myocardial hibernation.
- In addition to metabolism, the coronary circulation possesses unique pharmacologic characteristics. Prominent among these is its reactivity to adrenergic stimulation. The majority of vasculature in the body constricts to norepinephrine, a sympathetic neurotransmitter the body uses to increase blood pressure.
- In the coronary circulation, norepinephrine elicits vasodilation, due to the predominance of beta-adrenergic receptors in the coronary circulation.
- Agonists of alpha-receptors, such as phenylephrine, elicit very little constriction in the coronary circulation.
References
Microcirculation

Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Assistant Editor(s)-in-Chief: Rim Halaby
Overview
- The microcirculation is the blood flow through blood vessels smaller than 100 µm (i.e. arterioles, capillaries, and venules), this contrasts with macrocirculation, which transports blood to and from the organs.
- The main functions of the microcirculation are transporting blood cells and substances to/from the tissues, and acting as body coolant in thermoregulation processes.
- It also contributes to tissues color and stiffness.
- Diffusion is the capillary exchange of substances across the endothelial cells membranes.
The Components of the Microcirculation
- The vessels on the arterial side of the microcirculation are called the arterioles, which are well innervated, are surrounded by smooth muscle cells, and are 10-100 µm in diameter.
- Arterioles carry the blood to the capillaries, which are not innervated, have no smooth muscle, and are about 5-8 µm in diameter.
- Blood flows out of the capillaries into the venules, which have little smooth muscle and are 10-200 µm. The blood flows from venules into the veins.
- In addition to these blood vessels, the microcirculation also includes lymphatic capillaries and collecting ducts.
Determinants of Capillary Exchange
- 1- Surface area of the capillary bed
- It is dependent on the metabolic activity of the tissue.
- 2- Permeability of the capillary bed
- 3- Free diffusion coefficient of the solutes to be exchanged
- It is dependent on the solutes size, charge and lipid solubility.
- 4- Concentration of the solutes to be exchanged
- The difference in concentration of the solutes in the blood and in the interstitium drives the flow of substances across the capillary bed.[1]
Starling’s Law
- The Starling equation is an equation that illustrates the role of hydrostatic and oncotic forces (the so-called Starling forces) in the movement of fluid across capillary membranes.
- According to Starling’s equation, the movement of fluid depends on six variables:
- Capillary hydrostatic pressure ( Pc )
- Interstitial hydrostatic pressure ( Pi )
- Capillary oncotic pressure ( πc )
- Interstitial oncotic pressure ( πi )
- Filtration coefficient ( Kf )
- Reflection coefficient ( σ )
- Starling’s equation reads as follows:
![]()
Transvascular Exchange of Water
- Water moves across the capillary walls based on the same principles of Starling’s law and thus it depends on the difference of hydrostatic pressures and oncotic pressures in the blood vessels and in the interstitium.
- Filtration is the movement of water out of the vessels
- Reabsorption is the movement of water in the vessels.
References
- ↑ Hoit BD, Walsh RA. Chapter 5. Normal Physiology of the Cardiovascular System. In: Fuster V, Walsh RA, Harrington RA, eds. Hurst’s The Heart. 13th ed. New York: McGraw-Hill; 2011.
Cardiac electrophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Assistant Editor(s)-in-Chief: Rim Halaby; Serge Korjian
Overview
- Cardiac electrophysiology (also referred to as clinical cardiac electrophysiology , or electrophysiology) is the science of the mechanisms, functions, and performance of the electrical activities of specific regions of the heart.
- The normal electrical conduction in the heart allows the impulse that is generated by the sinoatrial node (SA node) of the heart to be propagated to (and stimulate) the myocardium (Cardiac muscle). The myocardium contracts after stimulation. It is the ordered stimulation of the myocardium that allows efficient contraction of the heart, thereby allowing blood to be pumped throughout the body.
Cardiac Conduction System
- Proper cardiac function heavily depends on the ability of the cardiomyocytes to receive and propagate an electrical impulse allowing the heart to contract.
- These impulses, known as action potentials, originate and travel through the cardiac conduction system.
- A time-ordered propagation of the electrical impulse through the myocardium allows efficient contraction of all four chambers of the heart, starting with the atria pumping the blood toward the ventricles, followed by the ventricles which contribute to the pulmonary and systemic circulation.
The Components of the Cardiac Conduction System:
- The sinus (sinoatrial) node
- The internodal tracts
- The atrioventricular (AV) node
- The His/AV bundle
- The right and left bundle branches,
- The Purkinje fibers.
The Direction of Propagation of the Action Potential:
- The initial cardiac impulse, produced by pacemaker cells, originates in the sinoatrial (SA) node at the intersection of the right atrium and the superior vena cava.
- This action potential is the trigger of every cardiac cycle, initiating the atrial then ventricular contractions; it is henceforth responsible for the rhythmic beating of the heart.
- This action potential then propagates as a wave of depolarization through the internodal tracts initiating atrial contraction and then converging at the AV node.
- The convergence occurs because, in a normal heart, the AV node is the only electrical connection between the atria and the ventricles.
- The conduction of this potential is delayed at the AV node mainly due to the slower depolarization in these cells.
- This delay is represented as the PR interval of the ECG.
- The electrical impulse then moves to the ventricles by means of the AV or His bundle located in the superior portion of the interventricular septum.
- It then continues moving apically and propagating through both [[]]ventricles via the right and left bundle branches, and the Purkinje fibers.[1][2][3][4]
-
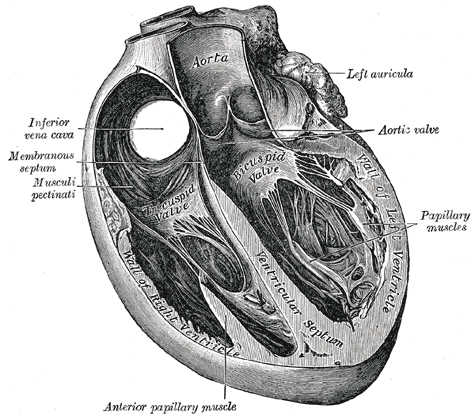 Section of the heart showing the ventricular septum.
Section of the heart showing the ventricular septum. -
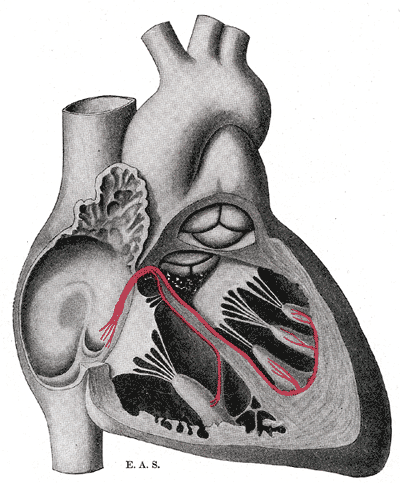 Schematic representation of the atrioventricular bundle of His.
Schematic representation of the atrioventricular bundle of His.


- Similarly to skeletal muscle cells which are also striated muscles, the cardiomyocytes contract in response to a rapid alteration in the cell membrane’s potential.
- However, the cardiomyocytes differ from skeletal muscle cells by three important variations that are essential for cardiac function:
- 1) They can self-generate a change in cell membrane potential.
- 2) The action potential can be transmitted directly from cell to cell.
- 3) The action potentials have a significantly longer duration.
The Resting Membrane Potential
- All cells including cardiomyocytes have a resting membrane potential that is maintained assuming there is no electrical charge crossing the membrane from the intracellular towards the extracellular milieu or vice versa.
- This potential is estimated to be –80 to –90 mV.
- The most crucial ions that determine this resting potential are:
- Sodium (Na+)
- Calcium (Ca2+)
- Potassium (K+)
- Sodium (Na+) and calcium (Ca2+) are most present in the interstitial fluid, while potassium (K+) is more present in intracellularly.
- These ions are lipid insoluble which prevents them from crossing the lipid bilayer or the cell membrane.
- Alternatively, ions cross via specific protein structures in the cell membrane that may be either: ion channels, ion pumps, or ion exchangers.
- These transmembrane proteins are highly specific and allow only one type of ion to pass through which allows good maintenance of the membrane potential.
- Ion channels can be opened, inactivated or closed depending on complex factors that modulate their activity.
The Cardiac Action Potential
- The cardiac contraction action potential is divided into 5 phases.
Phase 0: Depolarization
- The initial rapid increase in the transmembrane potential from -80mV to approximately +30mV constitutes the Phase 0 or the depolarization phase.
- This depolarization results from a rapid increase in the membrane permeability to Na+ ions via opening of voltage-dependent fast Na+ channels allowing Na+ ions to move intracellularly according to their electrochemical gradient.
- Following the conduction of an action potential, a recovery phase is attained where a large number of Na+ channels are inactivated, preventing the conduction of a second action potential.
- When the membrane is fully repolarized, these channels are reactivated and allow the conduction of the following action potential.
Phase I: Initial Repolarization
- The phase I of the action potential, known as the initial rapid repolarization ensues, resulting from K+ and Cl- ion flux across the membrane.
- This forms the notch seen in the action potential following the depolarization.
Phase II: Plateau
- Phase II, almost exclusive to cardiomyocytes, represents a plateau in the membrane potential as an outcome of the equilibrium between Ca2+ influx and K+ outflow.
- The channels responsible for this Ca2+ influx are known as the L-type calcium channels, which are activated rapidly when the membrane potential reaches -50mV, but are slowly inactivated thereafter.
- Throughout this plateau phase, few Na+ channels also remain active.
- These are Na+/Ca2+ exchangers that allow 1 ion of calcium to move outside the cell for every 3 molecules of sodium moving inside the cell.
Phase III: Repolarization
- The third phase, also known as rapid repolarization, depicts the restoration of a resting membrane potential.
- It is initiated by inactivation of the L-type calcium channels and an increase in K+ outflow.
- This change in potassium across the membrane is related to 3 K+ currents:
- 1) Inwardly rectifying K+ current (IK1) à Produces the resting membrane potential
- 2) Transient outward K+ current (ITO) à Accounts for initial part of repolarization
- 3) Delayed outward K+ current (IK) à Responsible for final part of repolarization
- After repolarization has occurred, intracellular Na+ and extracellular K+ are rearranged via the Na+/K+ ATPase pump.
- The ATPase moves 3 sodium ions out for every 2 potassium ions moved intracellularly.
- Equilibrium of ions across the membrane is also achieved via the Na+/Ca2+ exchangers.
Phase IV: Diastolic depolarization
- The phase IV of the action potential is characterized by a diastolic depolarization that is both spontaneous and slow.
- This phase provides cardiac cells with features of automaticity.
- In a normal functioning heart, only the sinoatrial node is able to reach a threshold potential during phase IV making it the pacemaker of the heart.
- Nevertheless other cells including those in the AV node, the His bundle, and the Purkinje fibers are able to reach a threshold and fire automatically if they are not suppressed by the SA node, which is true in some disease entities.
The factors responsible for the initial diastolic depolarization in the SA node are:
- Inward Ca2+ current
- Delayed outward K+ current
- IF Currents – Inward sodium-potassium currents activated if membrane repolarizes below the If threshold
- T-type Ca2+ channel – Releases calcium from internal stores
The rate of impulse generation by the SA node is determined by 3 factors:
- 1) The slope of diastolic depolarization
- 2) The maximal diastolic potential
- 3) The threshold potential
- All these factors are controlled by the autonomic nervous system allowing for the modulation of the rate of SA node firing and subsequently the heart rate.[1][5][3][4]
Electrophysiology Studies and Therapeutic Modalities
Overview
- An electrophysiologic study is a term used to describe a number of invasive (intracardiac) and non-invasive recording of spontaneous electrical activity as well as of cardiac responses to programmed electrical stimulation.
- These studies are performed to assess arrhythmias, elucidate symptoms, evaluate abnormal electrocardiograms, assess risk of developing arrhythmias in the future, and design treatment.
- These procedures increasingly include therapeutic methods (typically radiofrequency ablation) in addition to diagnostic and prognostic procedures.
- Other therapeutic modalities employed in this field include antiarrhythmic drug therapy and implantation of pacemakers and implantable cardioverter-defibrillators.
- A specialist in cardiac electrophysiology is known as a cardiac electrophysiologist, or (more commonly) simply an electrophysiologist. Cardiac electrophysiology is considered a subspecialty of cardiology, and in most countries requires two or more years of fellowship training beyond a general cardiology fellowship. They are trained to perform interventional cardiac EP procedures as well as surgical device implantations.
Diagnostic Testing
- Ambulatory electrocardiographic monitoring (Holter recording and interpretation; loop recording and interpretation)
- Tilt table testing
- Signal-averaged electrocardiogram (SAECG) interpretation, also referred to as “late potentials” reading
- Electrophysiologic study (EPS)
- Pacing and recording electrodes are inserted either in the esophagus (intra-esophageal EPS) or, through blood vessels, directly into the heart chambers (intra-cardiac EPS) in order to measure electrical properties of the heart. In addition, intra-cardiac EPS electrically stimulates the heart and induces arrhythmias for diagnostic purposes (“programmed electrical stimulation”).
Medical Treatment
Electrophysiologists play a role in:
- The initial administration and monitoring of the effect of drugs for treatment of heart rhythm disorders
- The management of severe or life threatening arrhythmias
- The management of arrythmias requiring multiple drugs use
Catheter Ablation
- Ablation therapy is the catheter based creation of lesions in the heart with radiofrequency energy, cryotherapy (destructive freezing), or ultrasound energy in order to cure or control arrhythmias (see radiofrequency ablation). Ablation is usually performed during the same procedure as the electrophysiology study which induces and confirms the diagnosis of the arrhythmia for which ablation therapy is sought.
Non-complex ablation
- It includes ablation for arrhythmias such as: AV nodal reentrant tachycardia, accessory pathway mediated tachycardia and atrial flutter.
- This procedure is usually performed using intracardiac catheters , fluoroscopy (a real-time X-ray camera), and electrical recordings from the inside of the heart.
Complex ablation
- It includes ablation for arrhythmias such as: multifocal atrial tachycardia, atrial fibrillation, and ventricular tachycardia.
- In addition to the apparatus used for a “non-complex” ablation, these procedures often make use of sophisticated computer mapping systems to localize the source of the abnormal rhythm and to direct delivery of ablation lesions.
Surgical Procedures: Pacemaker and Defibrillator Implantation and Follow Up
- Implantation of single and dual chamber pacemakers and defibrillators
- Implantation of “biventricular” pacemakers and defibrillators for patients with congestive heart failure
- Implantation of loop recorders (implanted ECG recorders for long term monitoring of ECG to allow for diagnosis of an arrhythmia)
- Clinical follow up and reprogramming of implanted devices
Abnormalities in Cardiac Electrophysiology
- Mechanism of Arrhythmias
- Diseases of the Conduction System and Bradyarrhythmias
- Narrow Complex Tachycardias
- Wide Complex Tachycardias
- Ventricular Tachyarrhythmias, Cardiac Arrest and Sudden Cardiac Death
- Arrhythmias in Pregnancy
Treatment Modalities for Arrhythmia
- Antiarrhythmic Medications
- Indications for Pacemakers
- Indications for an ICD
- Cardiac Resynchronization Therapy
- Catheter ablation
See also
- Clinical cardiac electrophysiology
- Electrical conduction system of the heart
- Electrocardiogram (EKG)
- Basic Principles of ECG Interpretation
- Electrophysiologic study
- Cardiology
- Cardiac arrhythmia
External links
References
- ↑ 1.0 1.1 David E. Mohrman, L. J. (2010). Cardiovascular Physiology, 7e. The McGraw-Hill Companies, Inc.
- ↑ Kim E. Barrett, S. B. (2012). Ganong’s Review of Medical Physiology, 24e . The McGraw-Hill Companies, Inc.
- ↑ 3.0 3.1 Olson, E. N. (2004). A decade of discoveries in cardiac biology. Nature Medicine, 467 – 474.
- ↑ 4.0 4.1 Valentin Fuster, R. A. (2011). Hurst’s The Heart, 13e. The McGraw-Hill Companies, Inc.
- ↑ Kim E. Barrett, S. B. (2012). Ganong’s Review of Medical Physiology, 24e . The McGraw-Hill Companies, Inc.
Cardiac muscle
Template:Infobox Anatomy Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Assistant Editor(s)-in-Chief: Rim Halaby
Overview
- Cardiac muscle is a type of involuntary striated muscle found in the walls of the myocardium.
- Cardiac muscle is one of three major types of muscle, the others being skeletal and smooth muscle.
- Coordinated contractions of cardiac muscle cells during systole propel blood out of the atria and ventricles to the blood vessels of the systemic and pulmonary circulatory systems.
- The inherent contractile activity of the heart is extensively regulated by the autonomic nervous system.
Metabolism
- Cardiac muscle is adapted to be highly resistant to fatigue:
- It has a large number of mitochondria enabling continuous aerobic respiration.
- The heart is so tuned to aerobic metabolism that it is unable to pump sufficiently in ischaemic conditions. At basal metabolic rates, about 1% of energy is derived from anaerobic metabolism. This can increase to 10% under moderately hypoxic conditions, but under more severe hypoxic conditions, not enough energy can be liberated by lactate production to sustain ventricular contractions. [1]
- It has numerous myoglobins (oxygen storing pigment).
- It has good blood supply throught the coronary arteries, which provides metabolic substrate and oxygen.
- It has a large number of mitochondria enabling continuous aerobic respiration.
- The sources of energy under basal aerobic conditions:
- 60% of energy comes from fat (free fatty acids and triacylglycerides)
- 35% of energy comes from carbohydrates
- 5% of energy comes from amino acids and ketone bodies
- However, these proportions vary widely according to nutritional state. For example, in starvation, lactate can be recycled by the heart. There is a cost to lactate recycling, since one NAD+ is reduced to get pyruvate from lacate, but the pyruvate can then be burnt aerobically in the TCA cycle, liberating much more energy.
- In diabetes, more fat and less carbohydrate is used, due to the reduced induction of GLUT4 glucose transporters to the cell surfaces. However, contraction itself plays a part in bringing GLUT4 transporters to the surface[2].
Contraction of the Cardiac Muscle
Characteristics of the Contraction of the Cardiac Muscle
Self Excitability:
- Unlike skeletal muscle, which contracts in response to nerve stimulation, and like single unit smooth muscle, cardiac muscle is myogenic, meaning that it is self-excitable stimulating contraction without a requisite electrical impulse coming from the central nervous system.
Synchrony:
- A single cardiac muscle cell, if left without input, will contract rhythmically at a steady rate; if two cardiac muscle cells are in contact, whichever one contracts first will stimulate the other to contract, and so on.
- This transmission of impulses makes cardiac muscle tissue similar to nerve tissue, although cardiac muscle cells are notably connected to each other by intercalated discs.
- Intercalated discs support synchronized contraction of cardiac tissue.
- Intercalated discs conduct electrochemical potentials directly between the cytoplasms of adjacent cells via gap junctions.
- In contrast to the chemical synapses used by neurons, electrical synapses, in the case of cardiac muscle, are created by ions flowing from cell to cell, known as an action potential.
- If synchronization of cardiac muscle contraction is disrupted for some reason (for example, in a heart attack), uncoordinated contraction known as fibrillation can result.
Regulation:
- Specialized pacemaker cells in the sinoatrial node normally determine the overall rate of contractions, with an average resting pulse of 72 beats per minute.
- The central nervous system does not directly create the impulses to contract the heart, but only sends signals to speed up or slow down the heart rate through the autonomic nervous system using two opposing kinds of modulation:
- 1- Sympathetic nervous system (fight or flight response)
- 2- Parasympathetic nervous system (rest and repose)
- Since cardiac muscle is myogenic, the pacemaker serves only to modulate and coordinate contractions. The cardiac muscle cells would still fire in the absence of a functioning SA node pacemaker, albeit in a chaotic and ineffective manner. This condition is known as fibrillation. Note that the heart can still beat properly even if its connections to the central nervous system are completely severed.
Excitation Contraction Coupling
- In contrast to skeletal muscle, cardiac muscle cannot contract in the absence of extracellular calcium ions as well as extracellular potassium ions.
- In this sense, it is intermediate between smooth muscle, which has a poorly developed sarcoplasmic reticulum and derives its calcium across the sarcolemma; and skeletal muscle which is activated by calcium stored in the sarcoplasmic reticulum (SR).
- Change in the voltage of the sarcolemma causes the dihydropyridine receptors to open and allows an initial calcium flow to the sarcoplasm.
- The small concentration of calcium that entered binds to ryanodine receptors on the sarcoplasmic reticulum and causes the release of larger stores of calcium from the sarcoplasmic reticulum. This is referred to as calcium-induced calcium release.
- Ryanodine receptors are blocked by plant alkaloid ryanodine.
- Ryanodine receptors are activated by methyl xanthine caffeine.
- The high concentration of calcium promotes actin-myosin bridging and subsequent cardiac muscle contraction.
- At the end of cardiac contraction, the concentration of calcium inside of the sarcoplasm declines:
- 80% of calcium is reabsorbed into the sarcoplasmic reticulum via an ATP dependent pump:
- The ATP dependent pump is regulated by phospholamban.
- Phosphorylated phospholamban is the active form. For example, norepinephrine causes the phosphoryllation of phospholamban and thus promotes calcium re-uptake and cardiac muscle relaxation.
- 20% of calcium is taken out of the cell by one of two mechanisms:
- 1- Calcium ATPase pump
- 2- Na+/Ca++ exchanger
- 80% of calcium is reabsorbed into the sarcoplasmic reticulum via an ATP dependent pump:
- Na+/Ca++ exchanger allows the entry of 3 molecules of sodium in exchange with one molecule of calcium.
- Digitalis blocks Na+/K+ ATPase which is usually present on the sarcolemma and leads to the following sequence of events:
- The intracellular sodium concentration increases.
- The gradient of sodium concentration across the sarcolemma decreases.
- This decrease in sodium gradient will decrease the activity of the Na+/Ca++ exchanger.
- The intracellular concentration of calcium increases.
- Cardiac muscle contractility increases.
- Digitalis blocks Na+/K+ ATPase which is usually present on the sarcolemma and leads to the following sequence of events:
- The excitation contraction coupling in the cardiac muscle, unlike that in the skeletal muscle, is modulated in such a way that different calcium levels can cause different degree of contractility.[3]
- Shown below is a scheme summarizing the different steps in the excitation-contraction coupling in the cardiac muscle cell:

Histological Appearance
Multinucleated Cardiac Muscle Cells
- The cells that comprise cardiac muscle, called cardiomyocytes or myocardiocyteal muscle cells,can contain one, two, or very rarely three or four cell nuclei.[4][5]
Striation
- Cardiac muscle exhibits cross striations formed by alternation segments of thick and thin protein filaments which are anchored by segments called Z-lines.
- The primary structural proteins of cardiac muscle are actin and myosin.
- The actin filaments are thin causing the lighter appearance of the I bands in muscle
- The myosin is thicker and darker lending a darker appearance to the alternating A bands in cardiac muscle as observed by a light enhanced microscope.
T-Tubules
- Another histological difference between cardiac muscle and skeletal muscle is that the T-tubules in cardiac muscle are shorter, broader and run along the Z-Discs.
- There are fewer T-tubules in comparison with Skeletal muscle.
Intercalated Discs
- An intercalated disc is an undulating double membrane separating adjacent cells in cardiac muscle fibers.
- Intercalated discs support synchronized contraction of cardiac tissue.
- Three types of membrane junctions exist within an intercalated disc:
- 1- Fascia adherens are anchoring sites for actin, and connects to the closest sarcomere.
- 2- Macula adherens stop separation during contraction by binding intermediate filaments joining the cells together, also called a desmosome.
- 3- Gap junctions allow action potentials to spread between cardiac cells by permitting the passage of ions between cells, producing depolarization of the heart muscle.
- Under light microscopy, intercalated discs appear as thin, typically dark-staining lines dividing adjacent cardiac muscle cells.
- The intercalated discs run perpendicular to the direction of muscle fibers.
- Under electron microscopy, an intercalated disc’s path appears more complex.
- At low magnification, this may appear as a convoluted electron dense structure overlying the location of the obscured Z-line.
- At high magnification, the intercalated disc’s path appears even more convoluted, with both longitudinal and transverse areas appearing in longitudinal section.[6] Gap junctions (or nexus junctions) fascia adherens (resembling the zonula adherens), and desmosomes are visible.
- In transverse section, the intercalated disk’s appearance is labyrinthine and may include isolated interdigitations.
References
- ↑ Ganong, Review of Medical Physiology, 22nd Edition. p81
- ↑ S Lund, GD Holman, O Schmitz, and O Pedersen. Contraction Stimulates Translocation of Glucose Transporter GLUT4 in Skeletal Muscle Through a Mechanism Distinct from that of Insulin. PNAS 92: 5817-5821.
- ↑ Mohrman DE, Heller LJ. Chapter 2. Characteristics of Cardiac Muscle Cells. In: Mohrman DE, Heller LJ, eds. Cardiovascular Physiology. 7th ed. New York: McGraw-Hill; 2010.
- ↑ Pollard, Thomas D. and Earnshaw, William. C., “Cell Biology”. Philadelphia: Saunders. 2007.
- ↑ Olivetti G, Cigola E, Maestri R; et al. (1996). “Aging, cardiac hypertrophy and ischemic cardiomyopathy do not affect the proportion of mononucleated and multinucleated myocytes in the human heart”. J. Mol. Cell. Cardiol. 28 (7): 1463–77. doi:10.1006/jmcc.1996.0137. PMID 8841934. Unknown parameter
|month=ignored (help) - ↑ Histology image: 22501loa – Histology Learning System at Boston University
External links
- Essentials of Human Physiology by Thomas M. Nosek. Section 2/2ch7/2ch7line.
See also
Cardiac cycle

Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Assistant Editor(s)-in-Chief: Rim Halaby
Overview
Cardiac cycle is the term referring to all or any of the events related to the flow of blood that occur from the beginning of one heartbeat to the beginning of the next[1]. The frequency of the cardiac cycle is the heart rate. Throughout the cardiac cycle, the blood pressure increases and decreases.
Every single ‘beat’ of the heart involves three major stages that together form one cardiac cycle:
1- Atrial systole
2- Ventricular systole
3- Complete cardiac diastole
While the term systole is synonymous with contraction (movement or stretching) of a muscle, the term diastole is synonymous with relaxation of a muscle.
Atrial Systole
- Atrial systole is the contraction of the heart muscle (myocardia) of the left and right atria. Normally, both atria contract at the same time. The term systole is synonymous with contraction (movement or stretching) of a muscle.
- Electrical systole is the electrical activity that stimulates the myocardium of the chambers of the heart to make them contract.
- This is soon followed by Mechanical systole, which is the mechanical contraction of the heart.
- As the atria contract, the blood pressure in each atrium increases, forcing additional blood into the ventricles. The additional flow of blood is called atrial kick.
- Atrial kick is absent if there is loss of normal electrical conduction in the heart, such as during atrial fibrillation, atrial flutter, and complete heart block.
- Atrial kick is different in character when the condition of the heart is altered such as in the case of increased cardiac stiffness found in patients with diastolic dysfunction.

Detection of atrial systole
Ventricular Systole
- Ventricular systole is the contraction of the muscles (myocardia) of the left and right ventricles.
- Ventricular systole can be divided into two phases:
- Isovolumetric ventricular contraction:
- Ventricles contract and push the atrioventricular valves (mitral and tricuspid valves) to close.
- The pressure inside the ventricles rises but not enough to open the semilunar valves (aortic and pulmonary valves).
- The volume of blood inside the ventricles remain unchanged during this phase, hence the term “isovolmetric”.
- Ventricular ejection:
- As the ventricles further contracts, the pressure inside the ventricle increases to a level that surpasses the pressure in the arteries.
- As the pressure in the ventricles is larger than that in the arteries, the aortic and pulmonary valves open and the blood is ejected outside the ventricles.
- During this phase, the pressure inside the ventricles is high and the volume of the blood in the ventricles decrease as it is ejected.
- Isovolumetric ventricular contraction:

Detection of ventricular systole
Heart sounds
- The first heart tone:
- The closing of the mitral and tricuspid valves (known together as the atrioventricular valves) at the beginning of ventricular systole cause the first part of the “lub-dub” sound made by the heart as it beats.
- Formally, this sound is known as the First Heart Tone, or S1.
- This first heart tone is created by the closure of mitral and tricuspid valve and is actually a two component sound, M1, T1.
- The second heart tone:
- The second part of the “lub-dub” (the Second Heart Tone, or S2), is caused by the closure of the aortic and pulmonic valves at the end of ventricular systole.
- As the left ventricle empties, its pressure falls below the pressure in the aorta, and the aortic valve closes. Similarly, as the pressure in the right ventricle falls below the pressure in the pulmonary artery, the pulmonic valve closes.
- The second heart sound is also two components, A2, P2: the aortic valve closes earlier than the pulmonic valve and they are audibly separated from each other in the second heart sound.
Electrocardiogram
- In an electrocardiogram, electrical systole of the ventricles begins at the beginning of the QRS complex.
Complete Cardiac Diastole
- Cardiac Diastole is the period of time when the heart relaxes after contraction in preparation for refilling with circulating blood.
- Ventricular diastole is when the ventricles are relaxing, while atrial diastole is when the atria are relaxing. Together they are known as complete cardiac diastole.
- During ventricular diastole, the pressure in the (left and right) ventricles drops from the peak that it reaches in systole.
- When the pressure in the left ventricle drops to below the pressure in the left atrium, the mitral valve opens, and the left ventricle fills with blood that was accumulating in the left atrium.
- Likewise, when the pressure in the right ventricle drops below that in the right atrium, the tricuspid valve opens, and the right ventricle fills with blood that was accumulating in the right atrium.
Regulation of the Cardiac Cycle
- Cardiac muscle is myogenic, which means that it is self-exciting. This is in contrast with skeletal muscle, which requires either conscious or reflex nervous stimuli for excitation.
- The heart’s rhythmic contractions occur spontaneously, although the frequency or heart rate can be changed by nervous or hormonal influences such as exercise or the perception of danger. For example, the phrenic nerve accelerates heart rate and the vagus nerve decelerates heart rate.
- The rhythmic sequence of contractions is coordinated by the sinoatrial (SA) and atrioventricular (AV) nodes.
- The sinoatrial node, often known as the cardiac pacemaker, is located in the upper wall of the right atrium and is responsible for the wave of electrical stimulation that initiates atrial contraction by creating an action potential.
- Once the wave reaches the AV node, situated in the lower right atrium, it is delayed there before being conducted through the bundles of His and back up the Purkinje fibers, leading to a contraction of the ventricles. The delay at the AV node allows enough time for all of the blood in the atria to fill their respective ventricles.
- In the event of severe pathology, the AV node can also act as a pacemaker; this is usually not the case because their rate of spontaneous firing is considerably lower than that of the pacemaker cells in the SA node and hence is overridden.
Related Chapters
- Apex beat
- Blood pressure
- Cardiac action potential
- Cardiac muscle
- Cardiac output
- Electrocardiogram
- Heart
- Systolic array (computer architecture)
- Ventricle
Cardiac Cycle Video
{{#ev:youtube|rguztY8aqpk}}
References
- ↑ Guyton, A.C. & Hall, J.E. (2006) Textbook of Medical Physiology (11th ed.) Philadelphia: Elsevier Saunder ISBN 0-7216-0240-1
External Links
- Interactive cardiac cycle. Interactivephysiology.com
- Cardiac cycle. University of Utah School of Medicine
- Heart sounds. ULCA School of Medicine
da:Hjertecyklus de:Diastole nl:Diastole nn:Diastole sv:Diastole
Pressure-volume loop
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Assistant Editor(s)-in-Chief: Rim Halaby
Synonyms and keywords: Pressure-volume loop; P-V diagram; volume-pressure loop
Overview
- A plot of a system’s pressure versus volume has long been used to measure the work done by the system and its efficiency. This analysis can be applied to heat engines and pumps, including the heart.
- Real time left ventricular (LV) pressure-volume loops provide a framework for understanding cardiac mechanics; in fact, a considerable amount of information on cardiac performance can be determined from the pressure versus volume plot (also known as pressure volume diagram).
- Several physiologically relevant hemodynamic parameters such as stroke volume, cardiac output, ejection fraction, myocardial contractility can be determined from these loops.
- To generate a pressure volume loop for the left ventricle, the left ventricular pressure is plotted against left ventricular volume at multiple time points during a single cardiac cycle.
Cardiac Pressure-Volume Loop
- The left ventricular pressure-volume loop (PV loop) represents the different events of the cardiac cycle.
- To generate a PV loop for the left ventricle, the left ventricular pressure is plotted against the left ventricular volume at multiple time points during a single cardiac cycle.
- The left ventricular pressure-volume illustrates the four phases of the cardiac cycle with respect to pressure and volume changes:
- Phase I: Diastolic ventricular filling
- The mitral valve is open while the aortic valve is closed.
- The volume increases to reach the maximal ventricular capacity known as end diastolic volume EDV.
- The pressure slightly increases.
- Phase II: Isovolumetric contraction
- The mitral and aortic valves are both closed.
- The volume of the blood is unchanged as the ventricles are contracting.
- The pressure inside the ventricles significantly increases.
- Phase III: Ventricular ejection
- The aortic valve opens as the pressure inside the ventricles exceeds that of the aorta.
- The blood volume inside the left ventricle decreases because it is pumped into the systemic circulation.
- Phase IV: Isovolumetric relaxation
- The aortic and mitral valves are closed.
- The volume inside the left ventricle is unchanged and it corresponds to the volume remaining in the ventricle after systole, known as end systolic volume ESV.
- The pressure inside the ventricle tremendously decreases as the ventricles are relaxing.
- Phase I: Diastolic ventricular filling
- Below is an image showing idealized pressure-volume diagram featuring cardiac cycle events.

Pressure-Volume Parameters
Stroke Volume
- Stroke volume (SV) is the amount of blood pumped by the left ventricle in a single cardiac cycle.
- The stroke volume is an indicator the left ventricular function which is mainly affected by the preload, afterload and contractility of the heart.
Stroke Work
- Ventricular stroke work (SW) is defined as the work performed by the left or right ventricle to eject the stroke volume into the aorta or pulmonary artery, respectively.
- The area enclosed by the PV loop is a measure of the ventricular stroke work, which is a product of the stroke volume and the mean aortic or pulmonary artery pressure (afterload), depending on whether one is considering the left or the right ventricle.
Cardiac Output
- Cardiac output (CO) is defined as the amount of blood pumped by the left ventricle in unit time.
- CO = Stroke Volume x Heart Rate
- The normal cardiac output is 5-6L/min and it can increase up to 5 times during exercise.
- CO is an indicator of the left ventricular function.
Ejection Fraction
- Ejection fraction (EF) is defined as the fraction of end diastolic volume that is ejected out of the ventricle during each contraction.
- Ejection Fraction = Stroke volume/end diastolic volume
- Healthy ventricles typically have ejection fractions greater than 0.55.
- Myocardial infarction or cardiomyopathy causes damage to the myocardium, which impairs the heart’s ability to eject blood and therefore reduces ejection fraction. This reduction in the ejection fraction can manifest itself as heart failure.
- Low EF usually indicates systolic dysfunction and severe heart failure can result in EF lower than 0.2.
dP/dtmin and dP/dtmax
- These represent the minimum and maximum rate of pressure change in the ventricle. Peak dP/dt has historically been used as an index of ventricular performance. However, it is known to be load dependent and inferior to hemodynamic parameters defined by the PV plane.
- An increase in contractility is manifested as an increase in dP/dtmax during isovolumic contraction. However, dP/dtmax is also influenced by preload, afterload, heart rate and myocardial hypertrophy. Hence the relationship between ventricular end-diastolic volume and dP/dt is a more accurate index of contractility than dP/dt alone.
- Similarly, an increase in diastolic function or an increase in relaxation (lusitropy) causes increased dP/dtmin during isovolumic relaxation. Hence, dP/dtmin has been used as a valuable tool in the analysis of isovolumic relaxation. However, studies have shown that this parameter may not be a valid measure of LV relaxation rate, especially during acute alterations in contractility or afterload.
Isovolumic Relaxation Constant (Τau)
- Tau represents the exponential decay of the ventricular pressure during isovolumic relaxation. Several studies have shown that Tau is a preload independent measure of isovolumic relaxation.
- Calculation of Tau (Glantz method)
P(t)= P0e-t⁄τE +Pα
where
- P = pressure at time t
- P0 = amplitude constant
- τE = Glantz relaxation constant
- Pα = non zero asymptote due to pleural and pericardial pressure
- Below is an image showing the calculation of Tau using Glantz Method.

Determinants of Left Ventricular Function
- 1- Preload:
- The preload is the volume that fills in the heart during diastole, and it is referred to as the end diastolic volume (EDV).
- According to Frank Starling’s law, the larger the blood volume filling the heart is, the larger the degree of cardiac stretching is and consequently more blood is pumped.
- The Frank–Starling mechanism can be explained on the basis of preload. As the heart fills with more blood than usual, there is an increase in the load experienced by each myocyte. This stretches the muscle fibers, increasing the affinity of troponin C to Ca2+ ions causing a greater number of cross-bridges to form within the muscle fibers. This increases the contractile force of the cardiac muscle, resulting in increased stroke volume.
- Below is an image showing Frank Starling’s law according to which the left ventricular function increases as the preload increases.

- 2- Afterload:
- The afterload is the pressure corresponding to the mean arterial pressure that the heart needs to overcome when pumping blood.
- When the afterload increases, it makes it harder for the heart to pump the blood, and thus the volume remaining in the ventricles after ventricular contraction (end systolic volume) will increase and the stroke volume will be low.
- 3- Contractility:
- The contractility of the heart is defined as the intrinsic force with which the heart contracts.
- Factors that increase the contractility of the heart (positive ionotropy) are: catecholamines, xanthines (caffeine), medications (Digitalis).
- Factors that decrease the contractlity of the heart (negative ionotropy) are: hypercapnea, hypoxia, acidosis, medications (quinidine, procainamide, barbiturates), heart failure.[1]
- Below is an image showing various curves illustrating different states of contractlity of the heart.

Pressure-Volume Loop Analysis
End Systolic Pressure Volume Relationship ESPVR
- End systolic pressure volume relationship (ESPVR) describes the maximal pressure that can be developed by the ventricle at any given LV volume. This implies that the PV loop cannot cross over the line defining ESPVR for any given contractile state.
- The slope of ESPVR represents the end-systolic elastance, which provides an index of myocardial contractility.
- The ESPVR is relatively insensitive to changes in preload, afterload and heart rate. This makes it an improved index of systolic function over other hemodynamic parameters like ejection fraction, cardiac output and stroke volume.
- The ESPVR becomes steeper and shifts to the left as inotropy (contractility) increases.
- The ESPVR becomes flatter and shifts to the right as inotropy decreases.
- Below is an image showing a pressure-volume loop with a steeper ESPVR that shifts to the left in the case of increased inotropy or contractility.

End Diastolic Pressure Volume Relationship EDPVR
- End diastolic pressure volume relationship (EDPVR) describes the passive filling curve for the ventricle and thus the passive properties of the myocardium.
- The slope of the EDPVR at any point along this curve is the reciprocal of ventricular compliance (or ventricular stiffness).
- If ventricular compliance is decreased (such as in ventricular hypertrophy):
- The ventricle is stiffer.
- This results in higher ventricular end-diastolic pressures (EDP) at any given end-diastolic volume (EDV).
- Alternatively, for a given EDP, a less compliant ventricle would have a smaller EDV due to impaired filling.
- If ventricular compliance increases (such as in dilated cardiomyopathy):
- The EDV may be very high but the EDP may not be greatly elevated.
- If ventricular compliance is decreased (such as in ventricular hypertrophy):
- Below is an image showing a pressure volume loop with changes in the EDPVR’s part resulting from variations in the ventricular compliance.

Pressure Volume Area
- The Pressure-volume area (PVA) represents the total mechanical energy generated by ventricular contraction.
- This is equal to the sum of the stroke work (SW), encompassed within the PV loop, and the elastic potential energy (PE).
- PVA = PE + SW
Pressure- Volume Loop Changes in Cardiac Abnormalities
Variation in Preload and Afterload
- When preload increases the following changes are observed:
- Increased end diastolic volume
- Increased stroke volume
- No changes in pressure
- When afterload increases the following changes are observed:
- Increased end systolic volume
- Decreased stroke volume
- Increased ventricular pressure because the ventricles need to contract more in order to overcome the afterload
- Below is an image showing the pressure volume graph in case of changes in preload and afterload.

Dilated Cardiomyopathy
- In dilated cardiomyopathy, the ventricle becomes dilated without compensatory thickening of the wall and consequently the following changes are observed:
- Decreased contractility of the left ventricle that is illustrated by a shift to the right of the ESPVR curve
- Decreased ventricular compliance illustrated by the shift to the right of the EDPVR curve
- Decreased stroke volume leading to an increase in the end systolic volume
- Increased end diastolic volume due to the dilatation of the ventricles
- Decreased cardiac output
- No change in the ventricular pressures accompanies the changes in the volume.
- Below is an image showing the pressure volume graph in case of dilated cardiomyopathy.

Left Ventricular Hypertrophy
- Left ventricular hypertrophy (LVH) is an increase in the thickness and mass of the myocardium.
- The thickening of the ventricular muscle results in decreased chamber compliance and consequently the following changes are observed:
- Elevated left ventricular pressures
- Increased ESV
- Decreased EDV
- Decreased cardiac output
- Below is an image showing the pressure volume curve in case of left ventricular hypertrophy (LVH) with associated reduced stroke volume (SV), end diastolic volume (EDV) and increased left ventricular pressure (LVP).

- There are two exceptions to these changes, where moderate hypertrophy allows for a lower heart rate, increased diastolic volume, and thus higher stroke volume:
- Increased left ventricular hypertrophy with increased EDV and SV seen with athletes[2]
- Increased left ventricular hypertrophy in healthy normal elderly individuals.
Restrictive Cardiomyopathy
- Restrictive cardiomyopathy includes a group of heart disorders in which the walls of the ventricles become stiff (but not necessarily thickened) and resist normal filling with blood between heartbeats.
- This condition occurs when heart muscle is gradually infiltrated or replaced by scar tissue or when abnormal substances accumulate in the heart muscle and consequently the following changes are observed:
- Normal ventricular systolic pressure
- Elevated diastolic pressure
- Reduced cardiac output
- Below is an image showing the pressure volume curve in case of restrictive cardiomyopathy with associated reduced stroke volume.

Valvular Diseases
Aortic Stenosis
- Aortic valve stenosis is the abnormal narrowing of the aortic valve.
- This results in the left ventricle pressures being much greater than the aortic pressures during left ventricular ejection. The magnitude of the pressure gradient is determined by the severity of the stenosis and the flow rate across the valve.
- The following changes are observed in severe aortic stenosis:
- Reduced ventricular stroke volume due to increased afterload (which decreases ejection velocity)
- Increased end-systolic volume
- Compensatory increase in end-diastolic volume and pressure
- Below is an image showing a pressure volume diagram in case of aortic stenosis depicting increased end systolic pressure and reduced stroke volume.

Mitral Stenosis
- Mitral stenosis is the abnormal narrowing of the mitral valve orifice.
- The following changes are observed inmitral stenosis:
- Decreased end-diastolic volume (preload) due to impaired left ventricular filling
- Decreased stroke volume resulting from the decreased preload according to the Frank–Starling mechanism
- Decreased cardiac output and aortic pressure (afterload) as the stroke volume is decreased
- Slightly decreased end-systolic volume due to the decrease in the afterload
- Below is an image showing a pressure volume curve in case of mitral stenosis depicting reduced end diastolic volume and reduced stroke volume.

Aortic Regurgitation
- Aortic insufficiency (AI) or regurgitation is the failure of the valve to close completely at the end of systolic ejection, causing leakage of blood back through the valve during LV diastole.
- The following changes are observed in aortic regurgitation:
- Increased end diastolic volume (preload) because the LV volume is greatly increased due to the enhanced ventricular filling from the constant backflow of blood through the leaky valve
- Increased systolic pressure and stroke volume due to the elevated preload according to the Frank–Starling mechanism
- Not that when the LV begins to contract and develop pressure, blood is still entering the LV from the aorta (since aortic pressure is higher than LV pressure), implying that there is no true isovolumic contraction. Once the LV pressure exceeds the aortic diastolic pressure, the LV begins to eject blood into the aorta.
- Below is an image showing the pressure volume curve in case of aortic regurgitation depicting increased end diastolic volume, increased stroke volume and increased LV systolic pressure.

Mitral Regurgitation
- Mitral regurgitation (MR) is the failure of the mitral valve to close completely, causing blood to flow back into the left atrium during ventricular systole.
- The increased ventricular
- The following changes are observed in mitral regurgitation:
- Decreased end systolic volume due to the constant back flow of blood through the leaky valve
- Increased left ventricular end diastolic volume as the volume and pressure of atria are higher than normal
- Increased stroke volume in such a way that the ejection into the aorta (forward flow) is reduced as the stroke volume in this case includes the volume of blood ejected into the aorta as well as the volume ejected back into the left atrium
- Below is an image showing the pressure volume curve in case of mitral regurgitation depicting increased end diastolic volume and increased stroke voume.

References
- ↑ Barrett KE, Barman SM, Boitano S, Brooks HL. Chapter 30. The Heart as a Pump. In: Barrett KE, Barman SM, Boitano S, Brooks HL, eds. Ganong’s Review of Medical Physiology. 24th ed. New York: McGraw-Hill; 2012.
- ↑ Scharhag, J.ürgen. “Athlete’s heart”. Athlete’s heart.
Related Chapters
Hemodynamics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Assistant Editor(s)-in-Chief: Rim Halaby
Overview
- The circulatory system transports blood and helps in delivering oxygen, nutrients and chemicals to the cells of the body and in removing cell wastes.
- Hemodynamics, meaning literally “blood movement”, is the study of blood flow or the circulation and it includes studying the following concepts:
- The factors influencing hemodynamics are extensive and include circulating fluid volume, respiration, vascular diameter and resistance, and blood viscosity. Each of these may in turn be influenced by physiological factors, such as diet, exercise, disease, drugs or alcohol, obesity and excess weight.
The Circulatory System
- The circulatory system is a connected series of tubes, which includes the heart, the arteries, the micro-circulation, and the veins. The “beating” of the heart generates pulsatile blood flow which is conducted into the arteries, across the micro-circulation and eventually, back via the venous system to the heart.
- The heart, vessels and lungs are all actively involved in maintaining healthy cells and organs, and all influence hemodynamics.
The Components of the Circulatory System
- The Heart
- The heart is the driver of the circulatory system generating cardiac output (CO) by rhythmically contracting and relaxing. This creates changes in regional pressures, and, combined with a complex valvular system in the heart and the veins, ensures that the blood moves around the circulatory system in one direction.
- The Arterial System
- The aorta, the main artery, leaves the left heart and proceeds to divide into smaller and smaller arteries until they become arterioles, and eventually capillaries, where oxygen transfer occurs.
- The microcirculation
- The micro-circulation, formed by the arterioles, capillaries and venules, constitutes most of the area of the vascular system and is the site of the transfer of, O2, glucose and substrates into the cells.
- The Venous System
- The venous system returns the deoxygenated blood to the right heart where it is pumped into the lungs to become oxygenated and CO2 and other gaseous wastes exchanged and expelled during breathing. Blood then returns to the left side of the heart where it begins the process again.
Cardiac Output
- Cardiac output (CO) is defined as the amount of blood pumped by the left ventricle in unit time.
- CO = Stroke Volume x Heart Rate
- The normal cardiac output is 5-6L/min and it can increase up to 5 times during exercise.
- CO is an indicator of the left ventricular function.
- Cardiac index (CI) is the output of the heart per minute per body surface area.
- CI = CO / Body Surface Area
- The normal cardiac index is 3.2 L/min/m2.[1]
- Stroke volume (SV) is the amount of blood pumped by the left ventricle in a single cardiac cycle.
Factors affecting the cardiac output
- CO = Stroke volume x Heart rate
- The cardiac output changes when there is any change in the stroke volume, the heart rate or both.
Factors affecting the heart rate:
- The electrical activity of the heart is generated spontaneously in the sinoatrial node. However, the autonomic nervous system affects the speed at which the electrical activity of the heart is generated and hence affects the heart rate.
- The sympathetic nervous system increases the heart rate (positive chronotropy).
- The parasympathetic nervous system decreases the heart rate (negative chronotropy).[2]
Factors affecting the stroke volume
- 1- Preload:
- 2- Afterload:
- The afterload is the pressure corresponding to the mean arterial pressure that the heart needs to overcome when pumping blood.
- When the afterload increases, it makes it harder for the heart to pump the blood, and thus the volume remaining in the ventricles after ventricular contraction (end systolic volume) will increase and the stroke volume will be low.
- 3- The contractility of the heart:
- The contractility of the heart is defined as the intrinsic force with which the heart contracts.
- Factors that increase the contractility of the heart (positive ionotropy) are: catecholamines, xanthines (caffeine), medications (Digitalis).
- Factors that decrease the contractlity of the heart (negative ionotropy) are: hypercapnea, hypoxia, acidosis, medications (quinidine, procainamide, barbiturates), heart failure.[3]
Clinical Correlation
- Diseases of the cardiovascular system are often associated with changes in CO.
- Cardiomyopathy and heart failure cause a reduction in cardiac output.
- Hypertension, infection and sepsis are known to increase cardiac output.
Blood Flow
- Blood flows from one site to another proportionally to the difference of pressures between these sites and inversely proportionally to the resistance of conduits (which are the vessels) in which blood is circulating.
- This is the same concept of Ohm’s law and it can be illustrated in the following formula:
- Flow = Difference in Pressure/Resistance
- Difference in pressure= Pressure at the first site – Pressure at the second site
- Resistance= 8 x viscosity of blood x length of vessels/ Pi x radius of vessels^4
- Circulation is influenced by the resistance of the vascular bed against which the heart is pumping.
- Pulmonary Vascular Resistance (PVR) is created by the pulmonary bed on the right side of the heart.
- Systemic Vascular Resistance (SVR) is created by the systemic vascular bed on the left side of the heart.
- The vessels actively change diameter under the influence of physiology or therapy:
- Vasoconstrictors decrease vessel diameter and increase resistance and hence decrease the blood flow.
- Vasodilators increase vessel diameter and decrease resistance and hence increase the blood flow.
Blood Pressure
- Blood pressure (BP) is the pressure exerted by the circulating blood on the walls of the blood vessels.
- The blood pressure can be clinically measured using a plethysmograph or cuff connected to a pressure sensor (mercury or aneroid manometer).
- Blood pressure varies during each cardiac cycle:
- Systolic blood pressure:
- It is the maximal blood pressure during each cycle.
- It is normally around 120 mmHg.
- It corresponds to the pressure exerted by the circulating blood on the walls of the vessels as the left ventricle is contracting and pushing blood into the aorta.
- Diastolic blood pressure:
- It is the minimal blood pressure during each cycle.
- It is normally around 70 mmHg.
- It corresponds to the pressure exerted by the circulating blood on the walls of the vessels as the left ventricle is relaxing.
- Systolic blood pressure:
- The average pressure throughout the cardiac cycle is referred to as mean arterial pressure (MAP).
- MAP = diastolic BP + (systolic BP – diastolic BP)/3= (systolic BP + 2x diastolic pressure)/3 [4]
Factors Influencing Blood Pressure
- Blood Pressure = Cardiac Output x Peripheral vascular resistance
- Any factor that affects the cardiac output, peripheral resistance or both will alter the blood pressure.

Regulation of Blood Pressure
- The regulation of the blood pressure is complex as it involves the interaction between the cardiovascular, renal and neurological systems among others.
1- Short term regulation of the blood pressure:
- Arterial baroreceptor reflex is the most important factor in the short term regulation of the blood pressure.
- Other cardiovascular reflexes:

2- Long term regulation of the blood pressure:
- Fluid balance by the renin-angiotensin system(RAAS) is the main contributor of the long term regulation of the blood pressure.[6]

See also
External links
Sources
1. Berne RM, Levy MN. Cardiovascular physiology. 7th Ed Mosby 1997
2. Rowell LB. Human Cardiovascular Control. Oxford University press 1993
3. Braunwald E (Editor). Heart Disease: A Textbook of Cardiovascular Medicine. 5th Ed. W.B.Saunders 1997
4. Siderman S, Beyar R, Kleber AG. Cardiac Electrophysiology, Circulation and Transport. Kluwer Academic Publishers 1991
6. Otto CM, Stoddard M, Waggoner A, Zoghbi WA. Recommendations for Quantification of Doppler Echocardiography: A Report from the Doppler Quantification Task Force of the Nomenclature and Standards Committee of the American Society of Echocardiography. J Am Soc Echocardiogr 2002;15:167-184
References
- ↑ Barrett KE, Barman SM, Boitano S, Brooks HL. Chapter 30. The Heart as a Pump. In: Barrett KE, Barman SM, Boitano S, Brooks HL, eds. Ganong’s Review of Medical Physiology. 24th ed. New York: McGraw-Hill; 2012.
- ↑ Barrett KE, Barman SM, Boitano S, Brooks HL. Chapter 30. The Heart as a Pump. In: Barrett KE, Barman SM, Boitano S, Brooks HL, eds. Ganong’s Review of Medical Physiology. 24th ed. New York: McGraw-Hill; 2012.
- ↑ Barrett KE, Barman SM, Boitano S, Brooks HL. Chapter 30. The Heart as a Pump. In: Barrett KE, Barman SM, Boitano S, Brooks HL, eds. Ganong’s Review of Medical Physiology. 24th ed. New York: McGraw-Hill; 2012.
- ↑ Mohrman DE, Heller LJ. Chapter 9. Regulation of Arterial Pressure. In: Mohrman DE, Heller LJ, eds. Cardiovascular Physiology. 7th ed. New York: McGraw-Hill; 2010.
- ↑ Mohrman DE, Heller LJ. Chapter 9. Regulation of Arterial Pressure. In: Mohrman DE, Heller LJ, eds. Cardiovascular Physiology. 7th ed. New York: McGraw-Hill; 2010.
- ↑ Mohrman DE, Heller LJ. Chapter 9. Regulation of Arterial Pressure. In: Mohrman DE, Heller LJ, eds. Cardiovascular Physiology. 7th ed. New York: McGraw-Hill; 2010.
Key Words
Key Words
Listed in alphabetical order:
- Angiotensin
- Aortic body
- Autoregulation
- Baroreceptor
- Baroreflex
- Blood pressure
- Blood vessel
- Cardiac action potential
- Cardiac output
- Cardiac pacemaker
- Carotid body
- Central venous pressure
- Chronotropic
- Compliance
- Diastolic pressure
- Dromotropic
- Ejection fraction
- Electrical conduction system of the heart
- Electrocardiogram
- End-diastolic volume
- End-systolic volume
- Fick’s law of diffusion
- Frank-Starling law of the heart
- Heart
- Heart rate
- Inotropic
- Juxtaglomerular apparatus
- Mean arterial pressure
- Microcirculation
- Poiseuille’s law
- Pressure volume diagram
- Pulse pressure
- Renin
- Renin-angiotensin system
- Skeletal-muscle pump
- Starling equation
- Stroke volume
- Systolic pressure
- Total peripheral resistance
- Wiggers diagram
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH