
Cleft lip and palate
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Cleft lip and cleft palate, which can also occur together as cleft lip and palate are variations of a type of clefting congenital deformity caused by abnormal facial development during gestation. This type of deformity is sometimes referred to as a cleft. A cleft is a sub-division in the body’s natural structure, regularly formed before birth. A cleft lip or palate can be successfully treated with surgery soon after birth. Cleft lips or palates occur in somewhere between one in 600-800 births.
The term hare lip is sometimes used colloquially to describe the condition because of the resemblance of a hare’s lip. The Chinese word for cleft lip is tuchun (兔唇), literally “harelip.”
References
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Pathophysiology
Cleft lip
If only skin tissue is affected one speaks of cleft lip. Cleft lip is formed in the top of the lip as either a small gap or an indentation in the lip (partial or incomplete cleft) or continues into the nose (complete cleft). Lip cleft can occur as one sided (unilateral) or two sided (bilateral). It is due to the failure of fusion of the maxillary and medial nasal processes (formation of the primary palate).
-
Unilateral incomplete
-
 Unilateral complete
Unilateral complete -
 Bilateral complete
Bilateral complete


A mild form of a cleft lip is a microform cleft. A microform cleft can appear as small as a little dent in the red part of the lip or look like a scar from the lip up to the nostril. In some cases muscle tissue in the lip underneath the scar is affected and might require reconstructive surgery. It is advised to have newborn infants with a microform cleft checked with a craniofacial team as soon as possible to determine the severeness of the cleft. The actor Joaquin Phoenix is an example of a person with a microform cleft that did not require surgery.
Cleft palate
Cleft palate is a condition in which the two plates of the skull that form the hard palate (roof of the mouth) are not completely joined. The soft palate is in these cases cleft as well. In most cases, cleft lip is also present. Cleft palate occurs in about one in 700 live births worldwide.[1]
Palate cleft can occur as complete (soft and hard palate, possibly including a gap in the jaw) or incomplete (a ‘hole’ in the roof of the mouth, usually as a cleft soft palate). When cleft palate occurs, the uvula is usually split.It occurs due to the failure of fusion of the lateral palatine processes, the nasal septum, and/or the median palatine processes (formation of the secondary palate).
The hole in the roof of the mouth caused by a cleft connects the mouth directly to the nasal cavity.
Note: the next images show the roof of the mouth. The top shows the nose, the lips are colored pink. For clarity the images depict a toothless infant.
-
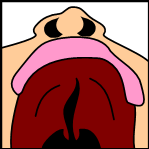 Incomplete cleft palate
Incomplete cleft palate -
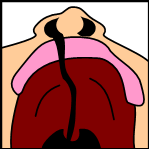 Unilateral complete lip and palate
Unilateral complete lip and palate -
 Bilateral complete lip and palate
Bilateral complete lip and palate



A direct result of an open connection between the oral cavity and nasal cavity is velopharyngeal insufficiency (VPI).
During the first six to eight weeks of pregnancy, the shape of the embryo’s head is formed. Five primitive tissue lobes grow:
- a) one from the top of the head down towards the future upper lip;
- b-c) two from the cheeks, which meet the first lobe to form the upper lip;
- d-e) and just below, two additional lobes grow from each side, which form the chin and lower lip;
If these tissues fail to meet, a gap appears where the tissues should have joined (fused). This may happen in any single joining site, or simultaneously in several or all of them. The resulting birth defect reflects the locations and severity of individual fusion failures (e.g., from a small lip or palate fissure up to a completely malformed face).
The upper lip is formed earlier than the palate, from the first three lobes named a to c above. Formation of the palate is the last step in joining the five embryonic facial lobes, and involves the back portions of the lobes b and c. These back portions are called palatal shelves, which grow towards each other until they fuse in the middle.[2] This process is very vulnerable to multiple toxic substances, environmental pollutants, and nutritional imbalance. The biologic mechanisms of mutual recognition of the two shelves, and the way they are glued together, are quite complex and obscure despite intensive scientific research.[3]
References
- ↑ “Statistics by country for cleft palate”. WrongDiagnosis.com. Retrieved 2007-04-24.
- ↑ Dudas et al. (2007): Palatal fusion – Where do the midline cells go? A review on cleft palate, a major human birth defect. Acta Histochemica, Volume 109, Issue 1, 1 March 2007,1-14
- ↑ Dudas M, Li WY, Kim J, Yang A, Kaartinen V (2007). “Palatal fusion -where do the midline cells go? A review on cleft palate, a major human birth defect”. Acta Histochem. 109 (1): 1–14. doi:10.1016/j.acthis.2006.05.009. PMID 16962647.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Causes
During the first six to eight weeks of pregnancy, the shape of the embryo’s head is formed. Five primitive tissue lobes grow:
- a) one from the top of the head down towards the future upper lip;
- b-c) two from the cheeks, which meet the first lobe to form the upper lip;
- d-e) and just below, two additional lobes grow from each side, which form the chin and lower lip;
If these tissues fail to meet, a gap appears where the tissues should have joined (fused). This may happen in any single joining site, or simultaneously in several or all of them. The resulting birth defect reflects the locations and severity of individual fusion failures (e.g., from a small lip or palate fissure up to a completely malformed face).
The upper lip is formed earlier than the palate, from the first three lobes named a to c above. Formation of the palate is the last step in joining the five embryonic facial lobes, and involves the back portions of the lobes b and c. These back portions are called palatal shelves, which grow towards each other until they fuse in the middle.[1] This process is very vulnerable to multiple toxic substances, environmental pollutants, and nutritional imbalance. The biologic mechanisms of mutual recognition of the two shelves, and the way they are glued together, are quite complex and obscure despite intensive scientific research.[2]
The cause of cleft lip and cleft palate formation can be genetic in nature. A specific gene that increases threefold the occurrence of these deformities has been identified in 2004 as reported by the BBC.[3]
Environmental influences may also cause, or interact with genetics to produce, orofacial clefting. Scientists have investigated seasonal causes (such as pesticide exposure); maternal diet and vitamin intake; retinoids- which are members of the vitamin A family; anticonvulsant drugs; alcohol; cigarette use; nitrate compounds; organic solvents; parental exposure to lead; and illegal drugs (cocaine, crack cocaine, heroin, etc.) as teratogens that increase the possibility of clefting.
If a person is born with a cleft, the chances of that person having a child with a cleft, given no other obvious factor, rises to 1 in 14. Research continues to investigate the extent to which Folic acid can reduce the incidence of clefting.
In some cases, cleft palate is caused by syndromes which also cause other problems. Stickler’s Syndrome can cause cleft lip and palate, joint pain, and myopia. Loeys-Dietz syndrome can cause cleft palate or bifid uvula, hypertelorism, and aortic aneurysm. Cleft lip/palate may be present in Patau’s Syndrome (trisomy 13). Many clefts run in families, even though there does not seem to be any identifiable syndrome present.
Maternal drug use – Clomifene
References
- ↑ Dudas et al. (2007): Palatal fusion – Where do the midline cells go? A review on cleft palate, a major human birth defect. Acta Histochemica, Volume 109, Issue 1, 1 March 2007,1-14
- ↑ Dudas M, Li WY, Kim J, Yang A, Kaartinen V (2007). “Palatal fusion -where do the midline cells go? A review on cleft palate, a major human birth defect”. Acta Histochem. 109 (1): 1–14. doi:10.1016/j.acthis.2006.05.009. PMID 16962647.
- ↑ “BBC NEWS”. Retrieved 2007-07-01. Text ” Cleft palate genetic clue found ” ignored (help); Text ” Health ” ignored (help)
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Epidemiology and Demographics
Prevalence rates reported for live births for Cleft lip with or without Cleft Palate (CL +/- P) and Cleft Palate alone (CPO) varies within different racial groups.
Template:Globalize/USA Cleft is present at different frequencies in different cultures and races as well as countries. An estimated 45% of the population is non-Caucasian. The U.S. is becoming more of a “melting pot”, as it was once coined (Strauss, 1990) and within this “melting pot” there are people who present with cleft lip and/or palate.
On average, about 1 in every 500-750 live births result in a cleft (Hardin-Jones, Karnell, & Peterson-Falzone, 2001). Furthermore, in the U.S., the prevalence for cleft lip with or without cleft palate (CL +/- P) is 2.2 to 11.7 per 10,000 births. Cleft palate alone (CP) results in a prevalence rate of 5.5 to 6.6 per 10,000 births (Forrester & Merz, 2004). Cleft of the lip, palate, or both is one of the most common congenital abnormalities and has a birth prevalence rate ranging from 1/1000 to 2.69/1000 amongst different parts of the world (McLeod, Saeed, & Arana- Urioste, 2004).
Africans and African Americans
A look in to the prevalence rates of different cultures in the U.S. when compared to their country of origin begins with Africans and African Americans. 1 per 2,500 African Americans are born with a cleft (Suleiman, Hamzah, Abusalab, & Samaan, 2005). African Americans have a lower prevalence rate of CL +/- P when compared to Caucasians. A prevalence rate of .61 per 1,000 and 1.05 per 1,000 live births respectively was reported by Croen, Shaw, Wasserman and Tolarova (1998). In Malawi there is a reported low prevalence rate for cleft lip and/or palate, .7 per 1,000 live births (Chisi, Igbibi, & Msamati, 2000). Suleiman et al. (2005) found that the prevalence rate of clefting among a group of Sudanese hospital new-borns in the city of Khartoum is .9 per 1,000 live births.
Latino Americans and Native Latinos
Latin Americans come from Mexico, Central America and South America, and the Caribbean (Meyerson, 1990). The prevalence of Latino Americans is lower than that of Caucasians and Native Americans, yet it is still higher than African Americans (Croen et al., 1998). Latinos have a prevalence of clefting of 9.7 per 10,000 live births (Kirby, Petrini & Alter, 2000). In Sucre, Bolivia the prevalence rate of CL +/- P is 1.23 per 1,000 live births (McLeod et al., 2004).
Jordan
Al Omari & Al-Omari (2004) reported that no study exists that has specifically looked at clefting among Jordanians prior to their investigation. Al Omari et al. (2004) examined the prevalence of clefting over an eleven-year period in Jordan and found an overall rate of 1.39 per 1,000 live births for CL +/- P. This was found to be similar with the prior studies that have examined clefting in other Arab populations.
United States of America
Hawaii is a U.S. state which has an extremely diverse population consisting of 73% people of Asianand Pacific Islander descent. Forrester & Merz (2004) found that the prevalence rates of CL +/- P per 10,000 live births in Hawaii were: 10 in Caucasians, 16 in people of Far East Asian descent, 11 in people of Pacific Islander descent, and 14.5 in people of Filipino descent.
When looking at the countries of origin, a higher rate was seen for Asians, specifically in Pakistan, with the prevalence rate being 1.91 per 1,000 live births (Elahi, Jackson, Elahi, Khan, Mubarak, Tariq, & Mitra, 2004). Similarly, C. Oh, S. Kim, W. Kim, & J. Kim (2002) found a similar prevalence rate of 1.81 per 1,000 births in the Republic of Korea. Valid prevalence rates in the native countries of the Philippines and Pacific Islands could not be reported.
The highest prevalence rates for (CL +/- P) are reported for Native Americans andAsians. Africans have the lowest prevalence rates.
- Native Americans: 3.74/1000
- Japanese: 0.82/1000 to 3.36/1000
- Chinese: 1.45/1000 to 4.04/1000
- Caucasians: 1.43/1000 to 1.86/1000
- Latin Americans: 1.04/1000
- Africans: 0.18/1000 to 1.67/1000
Rate of occurrence of CPO is similar for Caucasians, Africans, North American natives and Asians.
Prevalence of “cleft uvula” has varied from .02% to 18.8% with the highest numbers found among Chippewa and Navajo and the lowest generally in Africans.
References
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Risk Factors
- a family history of cleft lip or palate
- other birth defect
References
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Natural History and Prognosis
Please help WikiDoc by adding more content here. It’s easy! Click here to learn about editing.
Complications

Cleft may cause problems with feeding, ear disease, speech and socialization.
Due to lack of suction, an infant with a cleft may have trouble feeding. An infant with a cleft palate will have greater success feeding in a more upright position. Gravity will help prevent milk from coming through the baby’s nose if he/she has cleft palate. Gravity feeding can be accomplished by using specialized equipment, such as the Haberman Feeder, or by using a combination of nipples and bottle inserts commonly used with other infants. A large hole, crosscut, or slit in the nipple, a protruding nipple and pressure applied to the bottle insert by the caregiver’s hand can result in controllable flow to the infant without the stigma caused by specialized equipment.
Individuals with cleft also face many middle ear infections which can eventually lead to total hearing loss. The eustacian tubes and external ear canals may be angled or tortuous, leading to food or other contamination of a part of the body that is normally self cleaning.
Because the lips and palate are both used in pronunciation, individuals with cleft usually need the aid of a speech therapist. Bonding with the infant, socializing with family and community may be interrupted by the unexpected appearance, unusual speech and the surgical interventions necessary. Support for the parents as well as for the child can be pivotal.(see Psychosocial issues.
References
Treatment
Treatment
Surgery | Psychosocial Issues | Primary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
See also
See also
Treatment/aids
Syndromes
Organisations
Template:Congenital malformations and deformations of digestive system
ar:فلح الشفة والحنك da:Hareskår de:Lippen-, Kiefer-, Gaumenspalte dv:ކްލެފްޓް ޕަލޭޓް eo:Fendlipo ko:언청이 it:Labbro leporino he:שפה שסועה nl:Schisis no:Hareskår se:Simple english sv:Läpp-, käk- och gomspalt te:గ్రహణం మొర్రి
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH