
Riedel's thyroiditis
For patient information, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Synonyms and keywords: Riedel’s struma; Invasive fibrous thyroiditis; Fibrous thyroiditis
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
Riedel’s thyroiditis was first described by Semple, in 1864 and Bolby in 1888. Riedel’s thyroiditis was reported to the International Congress of Surgery by Bernhard Riedel in 1894 and 1896. It was initially considered to be the fibrous variant of Hashimoto’s thyroiditis but was later recognized as a separate disease. The exact pathogenesis of Riedel’s thyroiditis is not fully understood. The presence of thyroid autoantibodies and lymphoid infiltration of the thyroid gland resembling that of Hashimoto’s thyroiditis might indicate an autoimmune etiology. It is considered that the infiltrating lymphocytes release cytokines which are responsible for the activation of fibroblasts responsible for the fibrosis. Riedel’s thyroiditis is characterized by a replacement of the normal thyroid parenchyma by a dense fibrosis that invades adjacent structures of the neck and extends beyond the thyroid capsule. This makes the thyroid gland stone-hard and fixed to adjacent structures. A shared mechanism with retroperitoneal fibrosis and sclerosing cholangitis has been suggested. Riedel’s thyroiditis is considered to have autoimmune etiology and may be caused by the eosinophilia and the proliferation fibroblast as a result of cytokines released by inflammatory cells. Riedel’s thyroiditis must be differentiated from other causes of thyroiditis, such as De Quervain’s thyroiditis, Hashimoto’s thyroiditis, and suppurative thyroiditis. Riedel’s thyroiditis is a rare disease with an approximate incidence of 1.06 cases per 100,000 individuals worldwide. Riedel’s thyroiditis commonly affects individuals between 30-50 years of age. Females are more commonly affected by Riedel’s thyroiditis. Common risk factors in the development of Riedel’s thyroiditis include genetic factors, medications such as lysergic acid, ergotamine, serotonin, and other autoimmune diseases such as Graves’ disease and Hashimoto’s thyroiditis. If left untreated, patients with Riedel’s thyroiditis may progress to develop complications such as painless neck pressure, hoarseness, stridor, dysphagia, hypothyroidism, hypoparathyroidism, Horner’s syndrome, and occlusive phlebitis. Prognosis is generally good and the disease-specific death rate ranges from 6 to 10%. Diagnostic criteria of Riedel’s thyroiditis is based on the histopathological findings and includes infiltration of inflammatory cells in the thyroid gland, extension beyond the capsule, evidence of occlusive phlebitis and absence of giant cells, lymphoid follicles, or granulomas. The hallmark of Riedel’s thyroiditis is hard and fixed thyroid mass. A positive history of other autoimmune diseases and the use of certain medications is suggestive of Riedel’s thyroiditis. The most common symptoms of Riedel’s thyroiditis include hard and fixed neck mass, painless goiter, dysphagia, dyspnea, and hoarseness. Less common symptoms of Riedel’s thyroiditis include muscular cramps, paresthesias, fatigue, and dry skin. Patients may have the clinical signs of hypocalcemia such as positive Chvostek sign and positive Trousseau sign. Laboratory findings consistent with the diagnosis of Riedel’s thyroiditis include elevated ESR, mild elevation of thyroid peroxidase antibodies and occasionally elevated TSH levels. X-ray is helpful to identify esophageal or tracheal compression. CT scan findings suggestive of Riedel’s thyroiditis include hypodense infiltrative mass, invasion of nearby soft tissues, compression of the trachea, and esophageal compression. MRI findings suggestive of Riedel’s thyroiditis include focal, homogeneous hypointensity in T1 and T2. Ultrasound findings suggestive of Riedel’s thyroiditis include hypoechogenicity, thyroid nodule infiltrating adjacent structures, and absence of blood flow on Doppler ultrasound. 24-hour iodine-123 uptake is absent or decreased in Riedel’s thyroiditis. Other diagnostic studies for Riedel’s thyroiditis include pathological analysis, which demonstrates inflammatory cells infiltration, fibrosis with hyalinization, and extension of fibrosis outside the capsule, and immunohistochemical analysis, which demonstrates the predominance of T lymphocytes, strong positive stain to thyroglobulin, the presence of CD8+, CD4+ and plasma cells. Pharmacologic medical therapies for Riedel’s thyroiditis include corticosteroids, tamoxifen, and mycophenolate mofetil. Surgery is usually reserved for patients with esophageal or tracheal compressive symptoms.
Historical Perspective
Riedel’s thyroiditis was first described by Semple, in 1864 and Bolby in 1888. Riedel’s thyroiditis was reported to the International Congress of Surgery by Bernhard Riedel in 1894 and 1896. It was initially considered to be the fibrous variant of Hashimoto’s thyroiditis but was later recognized as a separate disease.
Classification
There is no established system for the classification of Riedel’s thyroiditis.
Pathophysiology
The exact pathogenesis of Riedel’s thyroiditis is not fully understood. The presence of thyroid autoantibodies and lymphoid infiltration of the thyroid gland resembling that of Hashimoto’s thyroiditis might indicate an autoimmune etiology. It is considered that the infiltrating lymphocytes release cytokines which are responsible for the activation of fibroblasts responsible for the fibrosis. Riedel’s thyroiditis is characterized by a replacement of the normal thyroid parenchyma by a dense fibrosis that invades adjacent structures of the neck and extends beyond the thyroid capsule. This makes the thyroid gland stone-hard and fixed to adjacent structures. A shared mechanism with retroperitoneal fibrosis and sclerosing cholangitis has been suggested.
Causes
Riedel’s thyroiditis is considered to have autoimmune etiology and may be caused by the eosinophilia and the proliferation fibroblast as a result of cytokines released by inflammatory cells. Although some drugs such as methysergide, serotonin, lysergic acid, and ergotamine have also been identified as the cause of retroperitoneal fibrosis, there are no reports of the direct association with Riedel’s thyroiditis.
Differentiating Riedel’s thyroiditis from Other Diseases
Riedel’s thyroiditis must be differentiated from other causes of thyroiditis, such as De Quervain’s thyroiditis, Hashimoto’s thyroiditis, and suppurative thyroiditis.
Epidemiology and Demographics
Riedel’s thyroiditis is a rare disease with an approximate incidence of 1.06 cases per 100,000 individuals worldwide. Riedel’s thyroiditis commonly affects individuals between 30-50 years of age. Females are more commonly affected by Riedel’s thyroiditis.
Risk Factors
Common risk factors in the development of Riedel’s thyroiditis include genetic factors, medications such as lysergic acid, ergotamine, serotonin, and other autoimmune diseases such as Graves’ disease and Hashimoto’s thyroiditis.
Screening
There is insufficient evidence to recommend routine screening for Riedel’s thyroiditis.
Natural History, Complications, and Prognosis
If left untreated, patients with Riedel’s thyroiditis may progress to develop complications such as painless neck pressure out of proportion to the size of the goiter, hoarseness, stridor, dysphagia, hypothyroidism, hypoparathyroidism, Horner’s syndrome, and occlusive phlebitis. Prognosis is generally good and the disease-specific death rate ranges in frequency from 6-10% in the patients with Riedel’s thyroiditis.
Diagnosis
Diagnostic Criteria
Diagnostic criteria of Riedel’s thyroiditis is based on the histopathological findings and includes infiltration of inflammatory cells in the thyroid gland, extension beyond the capsule, evidence of occlusive phlebitis and absence of giant cells, lymphoid follicles, or granulomas.
History and Symptoms
The hallmark of Riedel’s thyroiditis is hard and fixed thyroid mass. A positive history of other autoimmune diseases and the use of certain medications is suggestive of Riedel’s thyroiditis. The most common symptoms of Riedel’s thyroiditis include hard and fixed neck mass, painless goiter, dysphagia, dyspnea, and hoarseness. Less common symptoms of Riedel’s thyroiditis include muscular cramps, paresthesias, fatigue, and dry skin.
Physical Examination
Physical examination of patients with Riedel’s thyroiditis is usually remarkable for hard thyroid mass and clinical signs of hypothyroidism such as fatigue, bradycardia, bradypnea. Patients may have the clinical signs of hypocalcemia such as positive Chvostek sign and positive Trousseau sign.
Laboratory Findings
Laboratory findings consistent with the diagnosis of Riedel’s thyroiditis include elevated ESR, mild elevation of thyroid peroxidase antibodies and occasionally elevated TSH levels.
Electrocardiogram
There are no ECG findings associated with Riedel’s thyroiditis.
X-ray
X-ray findings in Riedel’s thyroiditis are helpful to identify esophageal or tracheal compression.
CT scan
CT scan may be helpful in the diagnosis of Riedel’s thyroiditis. Findings on CT scan suggestive of Riedel’s thyroiditis include hypodense infiltrative mass, invasion of nearby soft tissues, compression of the trachea, and esophageal compression.
MRI
MRI may be helpful in the diagnosis of Riedel’s thyroiditis. Findings on MRI suggestive of Riedel’s thyroiditis include focal, homogeneous hypointensity in T1 and T2.
Ultrasound
Ultrasound may be helpful in the diagnosis of Riedel’s thyroiditis. Findings on an ultrasound suggestive of Riedel’s thyroiditis include hypoechogenicity, thyroid nodule infiltrating adjacent structures, and absence of blood flow on Doppler ultrasound.
Other Imaging Findings
24-hour iodine-123 uptake is absent or decreased in Riedel’s thyroiditis.
Other Diagnostic Studies
Other diagnostic studies for Riedel’s thyroiditis include pathological analysis, which demonstrates inflammatory cells infiltration, fibrosis with hyalinization, and extension of fibrosis outside the capsule, and immunohistochemical analysis, which demonstrates the predominance of T lymphocytes, strong positive stain to thyroglobulin, the presence of CD8+, CD4+ and plasma cells.
Treatment
Medical Therapy
Pharmacologic medical therapies for Riedel’s thyroiditis include corticosteroids, tamoxifen, and mycophenolate mofetil.
Surgery
Surgery is usually reserved for patients with esophageal or tracheal compressive symptoms.
Primary Prevention
There are no established measures for the primary prevention of Riedel’s thyroiditis.
Secondary Prevention
There are no established measures for the secondary prevention of Riedel’s thyroiditis.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
Riedel’s thyroiditis was first described by Semple, in 1864 and Bolby in 1888. Riedel’s thyroiditis was reported to the International Congress of Surgery by Bernhard Riedel in 1894 and 1896. It was initially considered to be the fibrous variant of Hashimoto’s thyroiditis but was later recognized as a separate disease.
Historical Perspective
Riedel’s thyroiditis was initially thought to be the fibrous variant of Hashimoto’s thyroiditis and was later differentiated from Hashimoto’s thyroiditis.[1][2][3]
Discovery
- Riedel’s thyroiditis was first described by Semple, in 1864 and Bolby in 1888 even before the description of Bernhard Riedel.
- Riedel’s thyroiditis was reported to the International Congress of Surgery by Bernhard Riedel in 1894 and 1896. He gave a complete description of the disease.
- Riedel described 2 patients with a hard goiter and tracheal compressive symptoms. Initially, it was considered to be a fibrous variant of Hashimoto’s thyroiditis.
References
- ↑ “Redirecting”.
- ↑ B. M. C. L. Riedel. Die chronische, zur Bildung eisenharter Tumoren führende Entzündung der Schilddrüse. Verhandlungen der deutschen Gesellschaft für Chirurgie, 1896, 25: 101-105.
- ↑ Papi G, LiVolsi VA (2004). “Current concepts on Riedel thyroiditis”. Am. J. Clin. Pathol. 121 Suppl: S50–63. PMID 15298150.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
There is no established system for the classification of Riedel’s thyroiditis.
Classification
There is no established system for the classification of Riedel’s thyroiditis.
References
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
The exact pathogenesis of Riedel’s thyroiditis is not fully understood. The presence of thyroid autoantibodies and lymphoid infiltration of the thyroid gland resembling that of Hashimoto’s thyroiditis might indicate an autoimmune etiology. It is considered that the infiltrating lymphocytes release cytokines which are responsible for the activation of fibroblasts responsible for the fibrosis. Riedel’s thyroiditis is characterized by a replacement of the normal thyroid parenchyma by a dense fibrosis that invades adjacent structures of the neck and extends beyond the thyroid capsule. This makes the thyroid gland stone-hard and fixed to adjacent structures. A shared mechanism with retroperitoneal fibrosis and sclerosing cholangitis has been suggested.
Pathophysiology
The control, synthesis, and release of the thyroid hormone is usually controlled by hypothalamus and pituitary gland.[1][2]
|
 |
Pathogenesis
The exact pathogenesis of Riedel’s thyroiditis is not fully understood. The presence of thyroid autoantibodies and lymphoid infiltration of the thyroid gland resembling that of Hashimoto’s thyroiditis might indicate an autoimmune etiology.[3]
- It is considered that the infiltrating lymphocytes (CD4+ and CD8+) release cytokines which are responsible for the activation of fibroblasts responsible for the fibrosis.[4]
- Riedel’s thyroiditis is characterized by a replacement of the normal thyroid parenchyma by a dense fibrosis that invades adjacent structures of the neck and extends beyond the thyroid capsule.This makes the thyroid gland stone-hard and fixed to adjacent structures.[5]
- Tissue eosinophilia and Major basic protein (MBP) identified in the thyroid gland on the histopathological analysis are also thought to play a role in the proliferation of fibroblasts.[6]
- A shared mechanism with retroperitoneal fibrosis and sclerosing cholangitis is also suggested.[7]
Hypotheses
The following hypotheses regarding the pathogenesis of Riedel’s thyroiditis have been proposed:[8]
The Systemic Autoimmune Hypothesis
According to this theory, Riedel’s thyroiditis (RT) might be a primary disease of fibroblasts triggered by autoimmune stimuli.[8][9][10][11][12][13]
- It is proposed that the endothelial cells release oxidized low-density lipoprotein from atheromatous plaques following the injury resulting in an allergic hypersensitivity reaction.
- The natural consequence of this hypothesis is that the antigen initiating fibrosis is not localized within the thyroid but is affected secondarily by a systemic fibroinflammatory process.
- Thyroid follicular cells, peri-thyroid muscular cells, or intrathyroidal endothelial cells express antigens, cytokines, or adhesion molecules that might contribute to local activation of the disease. The evidence of a perivascular concentration of inflammatory cells in RT (occlusive phlebitis) might support the theory that the allergic process first involves blood vessels.
- Once the allergic reaction has started, a heavy inflammatory cell population such as B and T lymphocytes, plasma cells, monocytes, and eosinophils infiltrate tissues and produce several cytokines.
- The role of eosinophils in this context probably is central. When eosinophils migrate into the tissues involved by the disease, they degranulate and release cationic toxins into connective tissue including Major basic protein (MBP), eosinophil cationic protein, eosinophil peroxidase, and eosinophil-derived neurotoxin.
- Eosinophils also release cytokines, the most important of which are transforming growth factor β, transforming growth factor α, and granulocyte-macrophage colony-stimulating factor. This stimulates fibroblast proliferation that finally causes fibrosis.
The Genetic Hypothesis
This hypothesis was proposed for the multifocal fibrosclerosis which is associated with Riedel’s thyroiditis.[14]
- The basis of this hypothesis was a report of multifocal fibrosclerotic disease in two brothers, whose parents were first cousins. They developed different combinations of the multifocal fibrosclerotic disease and a familial multifocal fibrosclerosis was hypothesized.
- It was thought that genetic factors might have played a partial role in an enzymatic defect in the tryptophan → serotonin → 5-hydroxyindolacetic acid pathway. However, such a relationship has never been proven, and the siblings described remain the only case of familial multifocal fibrosclerosis reported in the literature.
The Intrathyroidal hypothesis
Riedel’s thyroiditis is associated with Hashimoto’s thyroiditis and de Quervain’s thyroiditis.[15]
- It is proposed that Riedel’s thyroiditis might represent a late fibrotic stage of subacute or chronic thyroiditis. The fundamental concept of this theory is that the fibrosing process of RT is specific to the thyroid gland.
The Pharmacologic Hypothesis
This hypothesis is also proposed primarily for multifocal fibrosclerosis. As Riedel’s thyroiditis is associated with multifocal fibrosclerosis this theory might explain the indirect association of Riedel’s thyroiditis with drugs.[8][16]
- The production of fibrosis by the drugs might be determined by an increased serum serotonin concentration through competitive inhibition at the serotonin receptor level and a reaction of hypersensitivity causing vasculitis and plasma exudation resulting in fibrosis.
- Although drugs have been found to cause multi organ fibrosis, there are no reports regarding medication induced Riedel’s thyroiditis. This theory might explain the indirect association of Riedel’s thyroiditis with drugs as Riedel’s thyroiditis is associated with multifocal fibrosclerosis.
Associated Conditions
Riedel’s thyroiditis is associated various other autoimmune conditions including:[4][17][18][19][20][16]
- Graves’ disease
- Hashimoto’s thyroiditis
- Multifocal idiopathic fibrosclerosis
- Addison’s disease
- Pernicious anemia
- Type 1 diabetes
Gross Pathology
On gross pathology the following findings are characteristic of Riedel’s thyroiditis:[21]
Microscopic Pathology
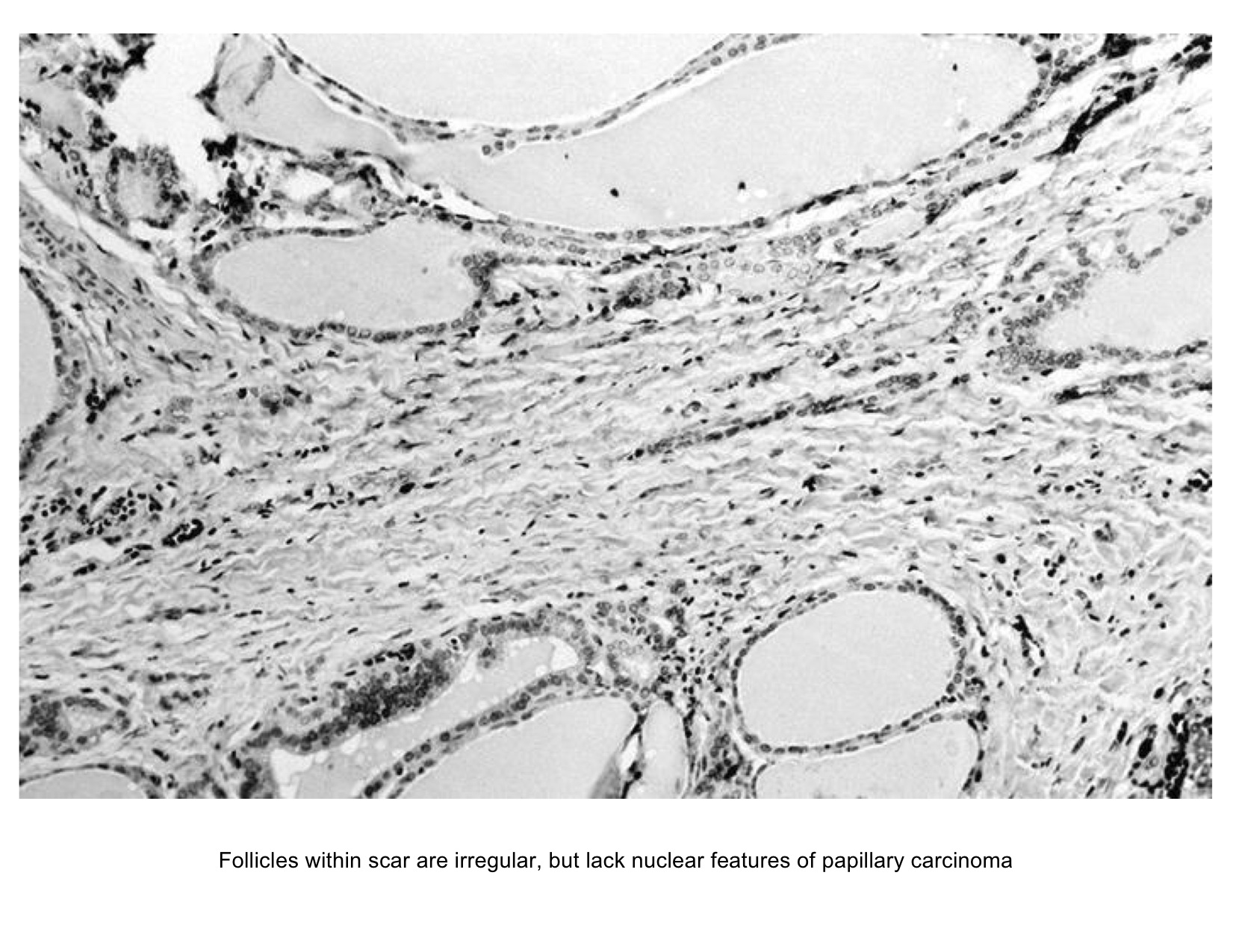
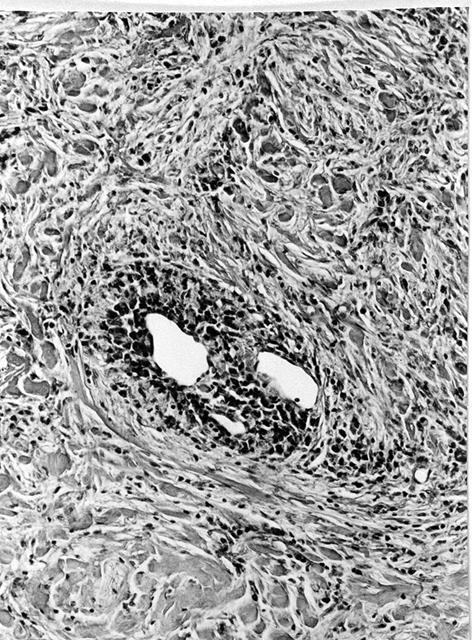
On microscopic histopathological analysis the following findings are usually seen:[22][8]
- Destruction of thyroid follicle by inflammatory cells
- Inflammatory cells including lymphocytes, plasma cells, and eosinophils in a dense matrix of hyalinized connective tissue
- Fibrous tissues and invasion of surrounding structures
Gallery
-
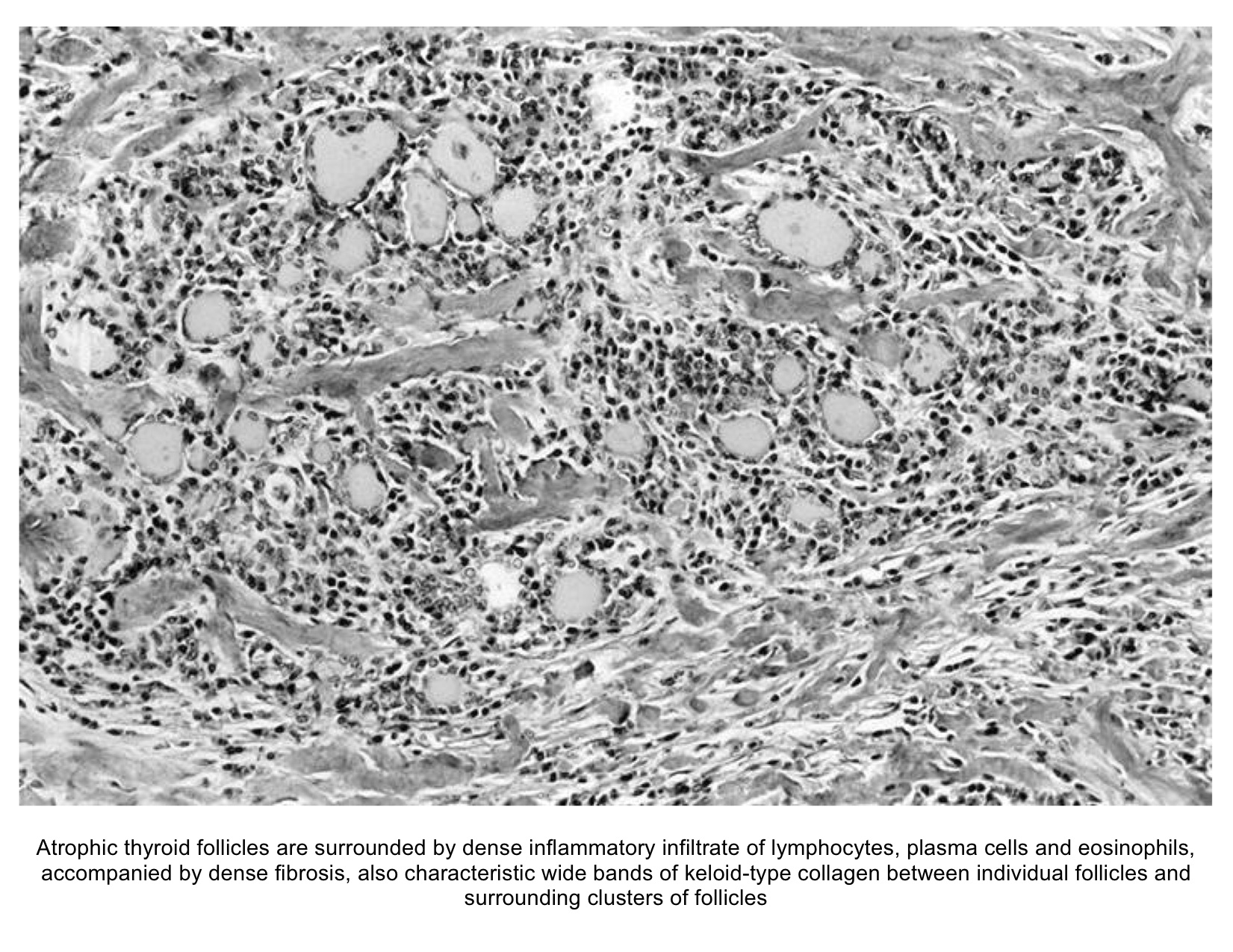 Histology of Riedel’s thyroiditis (Image courtesy of AFIP and PathologyOutlines.com; http://www.pathologyoutlines.com/topic/thyroidriedel.html )
Histology of Riedel’s thyroiditis (Image courtesy of AFIP and PathologyOutlines.com; http://www.pathologyoutlines.com/topic/thyroidriedel.html ) -
 Histology of Riedel’s thyroiditis (Image courtesy of AFIP and PathologyOutlines.com; http://www.pathologyoutlines.com/topic/thyroidriedel.html )
Histology of Riedel’s thyroiditis (Image courtesy of AFIP and PathologyOutlines.com; http://www.pathologyoutlines.com/topic/thyroidriedel.html ) -
 Histology of Riedel’s thyroiditis (Image courtesy of AFIP and PathologyOutlines.com; http://www.pathologyoutlines.com/topic/thyroidriedel.html )
Histology of Riedel’s thyroiditis (Image courtesy of AFIP and PathologyOutlines.com; http://www.pathologyoutlines.com/topic/thyroidriedel.html )



References
- ↑ De Groot LJ, Chrousos G, Dungan K, Feingold KR, Grossman A, Hershman JM, Koch C, Korbonits M, McLachlan R, New M, Purnell J, Rebar R, Singer F, Vinik A, Rousset B, Dupuy C, Miot F, Dumont J. “Thyroid Hormone Synthesis And Secretion”. PMID 25905405.
- ↑ Kirsten D (2000). “The thyroid gland: physiology and pathophysiology”. Neonatal Netw. 19 (8): 11–26. doi:10.1891/0730-0832.19.8.11. PMID 11949270.
- ↑ Schwaegerle SM, Bauer TW, Esselstyn CB (1988). “Riedel’s thyroiditis”. Am. J. Clin. Pathol. 90 (6): 715–22. PMID 3057862.
- ↑ 4.0 4.1 Zimmermann-Belsing T, Feldt-Rasmussen U (1994). “Riedel’s thyroiditis: an autoimmune or primary fibrotic disease?”. J. Intern. Med. 235 (3): 271–4. PMID 8120524.
- ↑ Cho MH, Kim CS, Park JS; et al. (2007). “Riedel’s thyroiditis in a patient with recurrent subacute thyroiditis: a case report and review of the literature”. Endocr. J. 54 (4): 559–62. PMID 17603227.
- ↑ “Tissue eosinophilia and eosinophil degranulation in Riedel’s invasive fibrous thyroiditis | The Journal of Clinical Endocrinology & Metabolism | Oxford Academic”.
- ↑ De Boer WA (1993). “Riedel’s thyroiditis, retroperitoneal fibrosis, and sclerosing cholangitis: diseases with one pathogenesis?”. Gut. 34 (5): 714. PMC 1374200. PMID 8504980.
- ↑ 8.0 8.1 8.2 8.3 Papi G, LiVolsi VA (2004). “Current concepts on Riedel thyroiditis”. Am. J. Clin. Pathol. 121 Suppl: S50–63. PMID 15298150.
- ↑ Heufelder AE, Goellner JR, Bahn RS, Gleich GJ, Hay ID (1996). “Tissue eosinophilia and eosinophil degranulation in Riedel’s invasive fibrous thyroiditis”. J. Clin. Endocrinol. Metab. 81 (3): 977–84. doi:10.1210/jcem.81.3.8772560. PMID 8772560.
- ↑ Noguchi H, Kephart GM, Colby TV, Gleich GJ (1992). “Tissue eosinophilia and eosinophil degranulation in syndromes associated with fibrosis”. Am. J. Pathol. 140 (2): 521–8. PMC 1886427. PMID 1739138.
- ↑ Gleich GJ, Adolphson CR (1986). “The eosinophilic leukocyte: structure and function”. Adv. Immunol. 39: 177–253. PMID 3538819.
- ↑ Gleich GJ, Frigas E, Loegering DA, Wassom DL, Steinmuller D (1979). “Cytotoxic properties of the eosinophil major basic protein”. J. Immunol. 123 (6): 2925–7. PMID 501097.
- ↑ Seibold JR, Giorno RC, Claman HN (1990). “Dermal mast cell degranulation in systemic sclerosis”. Arthritis Rheum. 33 (11): 1702–9. PMID 2242067.
- ↑ Comings DE, Skubi KB, Van Eyes J, Motulsky AG (1967). “Familial multifocal fibrosclerosis. Findings suggesting that retroperitoneal fibrosis, mediastinal fibrosis, sclerosing cholangitis, Riedel’s thyroiditis, and pseudotumor of the orbit may be different manifestations of a single disease”. Ann. Intern. Med. 66 (5): 884–92. PMID 6025229.
- ↑ Ewing J (1919). Neoplastic Diseases 2nd edition. Saunders; 1922:908.
- ↑ 16.0 16.1 Drieskens O, Blockmans D, Van den Bruel A, Mortelmans L (2002). “Riedel’s thyroiditis and retroperitoneal fibrosis in multifocal fibrosclerosis: positron emission tomographic findings”. Clin Nucl Med. 27 (6): 413–5. PMID 12045432.
- ↑ Drury MI, Sweeney EC, Heffernan SJ (1974). “Invasive fibrous (Riedel’s) thyroiditis”. Ir Med J. 67 (14): 388–90. PMID 4413980.
- ↑ “Chronic thyroiditis: A case showing features of both riedel’s and hashimoto’s thyroiditis – Merrington – 1948 – British Journal of Surgery – Wiley Online Library”.
- ↑ Hines RC, Scheuermann HA, Royster HP (1970). “Invasive Fibrous (Riedel’s) Thyroiditis With Bilateral Fibrous Parotitis”. JAMA: 869–871. doi:10.1001/jama.1970.03170310147054.
- ↑ “Riedel’s Thyroiditis: A Clinical Review | The Journal of Clinical Endocrinology & Metabolism | Oxford Academic”.
- ↑ “Riedel’s Thyroiditis | American Journal of Clinical Pathology | Oxford Academic”.
- ↑ “Redirecting”.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
Riedel’s thyroiditis is considered to have autoimmune etiology and may be caused by the eosinophilia and the proliferation fibroblast as a result of cytokines released by inflammatory cells. Although some drugs such as methysergide, serotonin, lysergic acid, and ergotamine have also been identified as the cause of retroperitoneal fibrosis, there are no reports of the direct association with Riedel’s thyroiditis.
Causes
Causes of Riedel’s thyroiditis may include:[1][2][3][4]
Common Causes
- Autoimmunity
- T and B Lymphocyte and macrophage infiltration
- Eosinophilic infiltration
Less common causes
- Drugs
- There are no reports of the direct association with Riedel’s thyroiditis with drugs. Some drugs have been identified as the cause of retroperitoneal fibrosis. As Riedels’ thyroiditis can develop as a manifestation of multi organ fibrosis these drugs are still relevant even though the direct link is not established. Some of the drugs which can cause retroperitoneal fibrosis are:
References
- ↑ Guimaraes VC, Ajjan RA, Weetman AP. “Subacute and Reidel’s thyroiditis”.
- ↑ “Tissue eosinophilia and eosinophil degranulation in Riedel’s invasive fibrous thyroiditis | The Journal of Clinical Endocrinology & Metabolism | Oxford Academic”.
- ↑ Ormond JK (1965). “Idiopathic retroperitoneal fibrosis: a discussion of the etiology”. J. Urol. 94 (4): 385–90. PMID 5839568.
- ↑ Iversen BM, Johannesen JW, Nordahl E, Ofstad J, Thunold S, Willassen Y (1975). “Retroperitoneal fibrosis during treatment with methydopa”. Lancet. 2 (7929): 302–4. PMID 50510.
Differentiating Riedel’s thyroiditis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
Riedel’s thyroiditis must be differentiated from other causes of thyroiditis, such as De Quervain’s thyroiditis, Hashimoto’s thyroiditis, Riedel’s thyroiditis, and suppurative thyroiditis.
Differentiating Riedel’s Thyroiditis from other Diseases
- Riedel’s thyroiditis must be differentiated from other causes of thyroiditis, such as De Quervain’s thyroiditis, Hashimoto’s thyroiditis, Riedel’s thyroiditis, and suppurative thyroiditis.[1]
| Conditions | Causes | Age at onset | Pathological findings | Diagnostic findings |
|---|---|---|---|---|
| Riedel’s thyroiditis |
|
|
|
|
| Hashimoto’s thyroiditis |
|
|
| |
| Painful subacute (De Quervain’s) thyroiditis |
|
|
|
|
| Silent thyroiditis |
|
|
| |
| Postpartum thyroiditis |
|
|
| |
| Suppurative thyroiditis |
|
|
|
|
- Riedel’s thyroiditis must be differentiated from other causes of hypothyroidism on the basis of history and symptoms and laboratory findings:[2][3][1][4][5][6]
| Disease | History and symptoms | Laboratory findings | Additional findings | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Fever | Pain | TSH | Free T4 | T3 | T3RU† | Thyroglobin | TRH | TPOAb^ | |||
| Primary hypothyroidism | Riedel’s thyroiditis | – | – | Normal/↑ | Normal/↓ | Normal/↓ | Normal/↓ | Normal | Normal | Usually present |
|
| Autoimmune (Hashimoto’s thyroiditis) | – | – | ↑* | ↓ | Normal/↓ | Normal/↓ | Normal/↑ | Normal | Present (high titer) |
| |
| Infectious thyroiditis | + | + | Normal | Normal | Normal | Normal | Normal | Normal | Absent |
| |
| Transient hypothyroidism | Subacute (de Quervain’s) thyroiditis | +/- | +/- | ↑/↓ | ↓/↑ | Normal | ↓ | ↑ | Normal | Low/absent |
|
| Postpartum thyroiditis | +/- | +/- | ↑/↓ | ↓/↑ | Normal | ↓ | ↑ | Normal/↑ | Present (high titer) |
| |
| Silent thyroiditis | – | – | ↑/↓ | ↓/↑ | Normal | ↓ | ↑ | Normal | Present (high titer) |
| |
| Others | Drug-induced | – | – | ↑/↓ | ↓/↑ | Normal | ↓ | Normal/↑ | Normal | Absent** |
|
| Radiation-induced | |||||||||||
| Trauma induced | |||||||||||
| Radioiodine induced | |||||||||||
| Thyroidectomy | |||||||||||
| Subclinical hypothyroidism | – | – | ↑ | Normal | Normal | Normal | Normal | Normal | Normal/↑ |
| |
†: T3RU; Triiodothyronine Resin uptake
^: TPOAb; Thyroid peroxidase antibodies
*: TSH may be decreased transiently in the thyrotoxicosis
**: TPOAb may be present in drug-induced hypo/hyperthyroidism such as Interferon-alpha, interleukin-2, and lithium.
References
- ↑ 1.0 1.1 “Thyroiditis — NEJM”.
- ↑ Bindra A, Braunstein GD (2006). “Thyroiditis”. Am Fam Physician. 73 (10): 1769–76. PMID 16734054.
- ↑ McDermott MT (2009). “In the clinic. Hypothyroidism”. Ann. Intern. Med. 151 (11): ITC61. doi:10.7326/0003-4819-151-11-200912010-01006. PMID 19949140.
- ↑ Aoki Y, Belin RM, Clickner R, Jeffries R, Phillips L, Mahaffey KR (2007). “Serum TSH and total T4 in the United States population and their association with participant characteristics: National Health and Nutrition Examination Survey (NHANES 1999-2002)”. Thyroid. 17 (12): 1211–23. doi:10.1089/thy.2006.0235. PMID 18177256.
- ↑ Lania A, Persani L, Beck-Peccoz P (2008). “Central hypothyroidism”. Pituitary. 11 (2): 181–6. doi:10.1007/s11102-008-0122-6. PMID 18415684.
- ↑ De Groot LJ, Chrousos G, Dungan K, Feingold KR, Grossman A, Hershman JM, Koch C, Korbonits M, McLachlan R, New M, Purnell J, Rebar R, Singer F, Vinik A, Stockigt J. “Clinical Strategies in the Testing of Thyroid Function”. PMID 25905413.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
Riedel’s thyroiditis is a rare disease with an approximate incidence of 1.06 cases per 100,000 individuals worldwide. Riedel’s thyroiditis commonly affects individuals between 30-50 years of age. Females are more commonly affected by Riedel’s thyroiditis.
Epidemiology and Demographics
Incidence
- The incidence of Riedel’s thyroiditis is estimated to be approximately 1.06 cases per 100,000 individuals worldwide.[1]
Prevalence
- Riedel’s thyroiditis is rare. In 1985, 37 patients reported were identified with Riedel’s thyroiditis over a 64 years period during which more than 56,000 thyroidectomies were performed in a study.[1]
Case-fatality rate
- There are no reports of reduced life expectancy in subjects with Riedel’s thyroiditis (RT). One lethal case of RT has been described up until now.[2]
Age
Race
- There is no racial predilection to Riedel’s thyroiditis.
Gender
- Females are more commonly affected by Riedel’s thyroiditis than men. Women have been noted to be affected 3-fold more frequently than men.[3][4]
References
- ↑ 1.0 1.1 Hay ID (1985). “Thyroiditis: a clinical update”. Mayo Clin. Proc. 60 (12): 836–43. PMID 3906289.
- ↑ Girod DA, Bigler SA, Coltrera MD (1992). “Riedel’s thyroiditis: report of a lethal case and review of the literature”. Otolaryngol Head Neck Surg. 107 (4): 591–5. doi:10.1177/019459989210700413. PMID 1437192.
- ↑ 3.0 3.1 Fatourechi MM, Hay ID, McIver B, Sebo TJ, Fatourechi V (2011). “Invasive fibrous thyroiditis (Riedel thyroiditis): the Mayo Clinic experience, 1976-2008”. Thyroid. 21 (7): 765–72. doi:10.1089/thy.2010.0453. PMID 21568724.
- ↑ 4.0 4.1 Singer PA (1991). “Thyroiditis. Acute, subacute, and chronic”. Med. Clin. North Am. 75 (1): 61–77. PMID 1987447.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
Common risk factors in the development of Riedel’s thyroiditis include genetic factors, medications such as lysergic acid, ergotamine, serotonin, and other autoimmune diseases such as Graves’ disease and Hashimoto’s thyroiditis.
Risk Factors
Common Risk Factors
Common risk factors in the development of Riedel’s thyroiditis include:[1][2][3][4][5][6][7]
- Genetic factors
- Medications
- Other autoimmune diseases
- Graves’ disease
- Hashimoto’s thyroiditis
- Multifocal idiopathic fibrosclerosis
- Addison’s disease
- Pernicious anemia
- Smoking
References
- ↑ “Current Concepts on Riedel Thyroiditis | Pathology Patterns Reviews | Oxford Academic”.
- ↑ Zimmermann-Belsing T, Feldt-Rasmussen U (1994). “Riedel’s thyroiditis: an autoimmune or primary fibrotic disease?”. J. Intern. Med. 235 (3): 271–4. PMID 8120524.
- ↑ Drury MI, Sweeney EC, Heffernan SJ (1974). “Invasive fibrous (Riedel’s) thyroiditis”. Ir Med J. 67 (14): 388–90. PMID 4413980.
- ↑ “Chronic thyroiditis: A case showing features of both riedel’s and hashimoto’s thyroiditis – Merrington – 1948 – British Journal of Surgery – Wiley Online Library”.
- ↑ Hines RC, Scheuermann HA, Royster HP (1970). “Invasive Fibrous (Riedel’s) Thyroiditis With Bilateral Fibrous Parotitis”. JAMA: 869–871. doi:10.1001/jama.1970.03170310147054.
- ↑ “Riedel’s Thyroiditis: A Clinical Review | The Journal of Clinical Endocrinology & Metabolism | Oxford Academic”.
- ↑ Fatourechi MM, Hay ID, McIver B, Sebo TJ, Fatourechi V (2011). “Invasive fibrous thyroiditis (Riedel thyroiditis): the Mayo Clinic experience, 1976-2008”. Thyroid. 21 (7): 765–72. doi:10.1089/thy.2010.0453. PMID 21568724.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
There is insufficient evidence to recommend routine screening for Riedel’s thyroiditis.
Screening
There is insufficient evidence to recommend routine screening for Riedel’s thyroiditis.
References
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
If left untreated, patients with Riedel’s thyroiditis may progress to develop complications such as painless neck pressure out of proportion to the size of the goiter, hoarseness, stridor, dysphagia, hypothyroidism, hypoparathyroidism, Horner’s syndrome, and occlusive phlebitis. Prognosis is generally good and the disease-specific death rate ranges in frequency from 6-10% in the patients with Riedel’s thyroiditis.
Natural History, Complications, and Prognosis
Natural History
The symptoms of Riedel’s thyroiditis usually develop in the third to fifth decade of life and progresses slowly.[1][2][3][4][5][6]
- Diagnosis of is often delayed for a variable period of time after the onset of clinical symptoms.
- After the initial presentation, it has been observed that the process may stabilize or even regress.
- If left untreated, patients with Riedel’s thyroiditis may progress to develop dysphagia, stridor, painless neck pressure out of proportion to the size of the goiter, and hypothyroidism.
Complications
Prognosis
- Prognosis is generally good and the disease-specific death rate ranges in frequency from 6-10% in patients with Riedel’s thyroiditis.[13][14][8]
References
- ↑ Singer PA (1991). “Thyroiditis. Acute, subacute, and chronic”. Med. Clin. North Am. 75 (1): 61–77. PMID 1987447.
- ↑ Groot, Leslie (2010). Endocrinology adult and pediatric : the thyroid gland. Philadelphia, Pennsylvania: Saunders. ISBN 9780323240642.
- ↑ Heufelder AE, Hay ID (1995). “Further evidence for autoimmune mechanisms in the pathogenesis of Riedel’s invasive fibrous thyroiditis”. J. Intern. Med. 238 (1): 85–6. PMID 7608652.
- ↑ 4.0 4.1 Sheu SY, Schmid KW (2003). “[Inflammatory diseases of the thyroid gland. Epidemiology, symptoms and morphology]”. Pathologe (in German). 24 (5): 339–47. doi:10.1007/s00292-003-0628-7. PMID 12961022.
- ↑ Chopra D, Wool MS, Crosson A, Sawin CT (1978). “Riedel’s struma associated with subacute thyroiditis, hypothyroidism, and hypoparathyroidism”. J. Clin. Endocrinol. Metab. 46 (6): 869–71. doi:10.1210/jcem-46-6-869. PMID 263470.
- ↑ “Riedel’s thyroiditis associated with Hashimoto’s thyroiditis, hypoparathyroidism, and retroperitoneal fibrosis | SpringerLink”.
- ↑ Kabalak T, Ozgen AG (2002). “Familial occurrence of subacute thyroiditis”. Endocr. J. 49 (2): 207–9. PMID 12081240.
- ↑ 8.0 8.1 Fatourechi MM, Hay ID, McIver B, Sebo TJ, Fatourechi V (2011). “Invasive fibrous thyroiditis (Riedel thyroiditis): the Mayo Clinic experience, 1976-2008”. Thyroid. 21 (7): 765–72. doi:10.1089/thy.2010.0453. PMID 21568724.
- ↑ Yasmeen T, Khan S, Patel SG, Reeves WA, Gonsch FA, de Bustros A, Kaplan EL (2002). “Clinical case seminar: Riedel’s thyroiditis: report of a case complicated by spontaneous hypoparathyroidism, recurrent laryngeal nerve injury, and Horner’s syndrome”. J. Clin. Endocrinol. Metab. 87 (8): 3543–7. doi:10.1210/jcem.87.8.8752. PMID 12161472.
- ↑ Meijer S, Hoitsma HF, Scholtmeijer R (1976). “Idiopathic retroperitoneal fibrosis in multifocal fibrosclerosis”. Eur. Urol. 2 (5): 258–60. PMID 1009988.
- ↑ Meyer S, Hausman R (1976). “Occlusive phlebitis in multifocal fibrosclerosis”. Am. J. Clin. Pathol. 65 (3): 274–83. PMID 943929.
- ↑ Geissler B, Wagner T, Dorn R, Lindemann F (2001). “Extensive sterile abscess in an invasive fibrous thyroiditis (Riedel’s thyroiditis) caused by an occlusive vasculitis”. J. Endocrinol. Invest. 24 (2): 111–5. doi:10.1007/BF03343824. PMID 11263468.
- ↑ “Riedel’s Thyroiditis: A Clinical Review | The Journal of Clinical Endocrinology & Metabolism | Oxford Academic”.
- ↑ Schwaegerle SM, Bauer TW, Esselstyn CB (1988). “Riedel’s thyroiditis”. Am. J. Clin. Pathol. 90 (6): 715–22. PMID 3057862.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | X-Ray Findings | Echocardiography and Ultrasound | CT-Scan Findings | MRI Findings | Other Diagnostic Studies | Other Imaging Findings
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH