
De Quervain's thyroiditis
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Synonyms and keywords: Subacute granulomatous thyroiditis; Subacute thyroiditis; Subacute painful thyroiditis; Subacute nonsuppurative thyroiditis; Giant cell thyroiditis; Pseudogranulomatous thyroiditis; Pseudotuberculous thyroiditis; Struma granulomatosa.
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
De Quervain’s thyroiditis is also known as subacute thyroiditis. In 1895, Mygind first described de Quervain’s thyroiditis. In 1904, Fritz de Quervain differentiated this disease from other forms of thyroiditis on the basis of the pathological findings. De Quervain’s thyroiditis can be classified according to the development of symptoms into the prodromal stage, hyperthyroid stage, euthyroid stage, and hypothyroid stage. The exact pathogenesis of de Quervain’s thyroiditis is unclear. It is proposed that cytotoxic T cell recognition of viral and cell antigens, presented in a complex, leads to the thyroid follicular cell damage; which is responsible for the pathogenesis of de Quervain’s thyroiditis. De Quervain’s thyroiditis is usually preceded by a viral prodrome and also have a genetic predisposition. Human leukocyte antigen B35 and B15/62 are associated with de Quervain’s thyroiditis. De Quervain’s thyroiditis may be caused by viruses such as mumps, adenovirus, Epstein–Barr virus, coxsackievirus, cytomegalovirus, influenza, echovirus, and enterovirus. De Quervain’s thyroiditis must be differentiated from other causes of thyroiditis, such as Hashimoto’s thyroiditis, Riedel’s thyroiditis, and suppurative thyroiditis. Common risk factors in the development of de Quervain’s thyroiditis are viral illness, family history, and female gender. De Quervain’s thyroiditis develops after a viral prodrome and presents as painful thyroid gland with symptoms of thyrotoxicosis. It further leads to a euthyroid phase and eventually hypothyroid phase before the complete resolution of the disease. Complications include hypothyroidism and rarely, esophageal or tracheal compression. The hallmark of de Quervain’s thyroiditis is hyperthyroidism with the neck pain. A positive history of viral illness and family history of de Quervain’s thyroiditis are suggestive of de Quervain’s thyroiditis. The most common symptoms of de Quervain’s thyroiditis are neck pain, palpitations, tachycardia, nervousness, and tremors. Patients with de Quervain’s thyroiditis usually appear fatigued and restless. Physical examination of patients with de Quervain’s thyroiditis is usually remarkable for neck tenderness, tachycardia, and palpitations. In the recovery phase of de Quervain’s thyroiditis patient may develop hypothyroidism. Laboratory findings consistent with the diagnosis of de Quervain’s thyroiditis usually include increased ESR, free T3, and free T4 and decreased thyroid stimulating hormone. Anti-thyroid peroxidase antibody is usually low or absent. The most common EKG finding associated with the thyrotoxicosis in de Quervain’s thyroiditis is sinus tachycardia. Rarely signs of myocardial damage including ST-segment elevation and arrhythmias can also be seen in thyrotoxicosis. Chest X-ray findings in de Quervain’s thyroiditis are usually not significant, but if there is concomitant myocarditis or heart failure, cardiomegaly and pulmonary edema are probable. Non-contrast CT may be used in de Quervain’s thyroiditis to assess the esophageal or tracheal compression. In de Quervain’s thyroiditis, T1-weighted MRI shows mild and T2-weighted image shows a more pronounced hyperintensity in the thyroid gland. Ultrasound findings associated with de Quervain’s thyroiditis are hypoechoic areas, glandular irregularities, and nonhomogeneous echotexture. The histological analysis in de Quervain’s thyroiditis may show the destruction of the follicular epithelium, loss of the follicular integrity and infiltration of inflammatory cells. Fine needle aspiration cytology helps to differentiate between the benign and malignant nodules. The mainstay of therapy for de Quervain’s thyroiditis is aspirin or non-steroidal anti-inflammatory drugs for pain control. Beta-adrenergic blockers are recommended for the patients who develop thyrotoxic symptoms. Corticosteroids are usually used in severely ill patients. Surgical intervention is not usually recommended for the management of de Quervain’s thyroiditis. Thyroidectomy is considered only when there are repeated relapses despite appropriate treatment.
Historical Perspective
In 1895, Mygind first described de Quervain’s thyroiditis. In 1904, Fritz de Quervain differentiated this disease from other forms of thyroiditis on the basis of the pathological findings.
Classification
De Quervain’s thyroiditis can be classified according to the development of symptoms into the prodromal stage, hyperthyroid stage, euthyroid stage, and hypothyroid stage.
Pathophysiology
The exact pathogenesis of de Quervain’s thyroiditis is unclear. It is proposed that cytotoxic T cell recognition of viral and cell antigens, presented in a complex, leads to the thyroid follicular cell damage which is responsible for the pathogenesis of de Quervain’s thyroiditis. De Quervain’s thyroiditis is usually preceded by a viral prodrome and also have a genetic predisposition. HLA B35 and HLA B15/62 are associated with de Quervain’s thyroiditis.
Causes
De Quervain’s thyroiditis may be caused by viruses such as mumps, adenovirus, Epstein–Barr virus, coxsackievirus, cytomegalovirus, influenza, echovirus, and enterovirus. Genetic factors also predispose an individual towards de Quervain’s thyroiditis.
Differentiating De Quervain’s thyroiditis from other Conditions
De Quervain’s thyroiditis must be differentiated from other causes of thyroiditis, such as Hashimoto’s thyroiditis, Riedel’s thyroiditis, and suppurative thyroiditis. De Quervain’s thyroiditis must be differentiated from other causes of thyroiditis, such as De Quervain’s thyroiditis, Riedel’s thyroiditis, and suppurative thyroiditis. De Quervain’s thyroiditis must also be differentiated from other diseases which cause hypothyroidism. As de Quervain’s thyroiditis may cause transient thyrotoxic symptoms, the diseases causing thyrotoxicosis must also be considered in the differential diagnosis.
Epidemiology and Demographics
De Quervain’s thyroiditis is particularly common in middle-aged women, Asians, and Whites. Annually, there are around 22 per 100,000 individuals worldwide.
Risk Factors
Common risk factors in the development of de Quervain’s thyroiditis are viral illness, family history, and female gender.
Screening
There is insufficient evidence to recommend routine screening for de Quervain’s thyroiditis.
Natural History, Complications, and Prognosis
De Quervain’s thyroiditis develops after a viral prodrome and presents as painful thyroid gland with symptoms of thyrotoxicosis. It further leads to a euthyroid phase and eventually hypothyroid phase before the complete resolution of the disease. Complications include hypothyroidism and rarely, esophageal or tracheal compression.
Diagnosis
Diagnostic Criteria
There are no established criteria for the diagnosis of de Quervain’s thyroiditis but painful thyroid mass, decreased radioactive iodine uptake, elevated ESR, serum T3, and T4 are helpful in diagnosing de Quervain’s thyroiditis.
History and Symptoms
The hallmark of de Quervain’s thyroiditis is hyperthyroidism with the neck pain. A positive history of viral illness and a positive family history are suggestive of de Quervain’s thyroiditis. The most common symptoms of de Quervain’s thyroiditis are neck pain, palpitations, tachycardia, nervousness, and tremors.
Physical Examination
Patients with de Quervain’s thyroiditis usually appear fatigued and restless. Physical examination of patients with de Quervain’s thyroiditis is usually remarkable for neck tenderness, tachycardia, and palpitations. In the recovery phase of de Quervain’s thyroiditis patient may develop hypothyroidism.
Laboratory Findings
Laboratory findings consistent with the diagnosis of de Quervain’s thyroiditis usually include increased ESR, CRP, free T3, and free T4 and decreased thyroid stimulating hormone. Anti-thyroid peroxidase antibody is usually low or absent.
Electrocardiogram
The most common EKG finding associated with the thyrotoxicosis in de Quervain’s thyroiditis is sinus tachycardia. Rarely signs of myocardial damage, including ST-segment elevation and arrhythmias, can also be seen in thyrotoxicosis.
Chest X-Ray
Chest X-ray findings in de Quervain’s thyroiditis are usually not significant but may show cardiomegaly and pulmonary edema, if there is concomitant myocarditis or heart failure.
CT
Non-contrast CT may be used in de Quervain’s thyroiditis to assess the tracheal or esophageal compression.
MRI
In de Quervain’s thyroiditis, T1-weighted MRI shows mild and T2-weighted image shows a more pronounced hyperintensity in the thyroid gland.
Echocardiography or Ultrasound
There are no echocardiographic findings related to de Quervain’s thyroiditis. Ultrasound findings associated with de Quervain’s thyroiditis are hypoechoic areas, glandular irregularities, and non-homogeneous echo-texture.
Other Imaging Findings
24-hour iodine-123 uptake is decreased in de Quervain’s thyroiditis.
Other Diagnostic Studies
The histological analysis in de Quervain’s thyroiditis may show the destruction of the follicular epithelium, loss of the follicular integrity and infiltration of inflammatory cells. Fine needle aspiration cytology helps to differentiate between the benign and malignant nodules.
Treatment
Medical Therapy
The mainstay of therapy for de Quervain’s thyroiditis is aspirin or non-steroidal anti-inflammatory drugs for pain control. Beta-adrenergic blockers are recommended for the patients who develop thyrotoxic symptoms. Corticosteroids are usually used in severely ill patients. Levothyroxine is required if the patient develops hypothyroidism following the resolution of the hyperthyroid state.
Surgery
Surgical intervention is not usually recommended for the management of de Quervain’s thyroiditis. Thyroidectomy is considered only when there are repeated relapses despite appropriate treatment.
Primary prevention
There are no primary preventive measures available for de Quervain’s thyroiditis.
Secondary Prevention
There are no secondary preventive measures available for de Quervain’s thyroiditis.
References
Template:WS Template:WikiDoc Sources
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
In 1895, Mygind first described de Quervain’s thyroiditis. In 1904, Fritz de Quervain differentiated this disease from other forms of thyroiditis on the basis of the pathological findings.
Historical Perspective
De Quervain’s thyroiditis is named after Fritz de Quervain who differentiated de Quervain’s thyroiditis clearly from other forms of thyroiditis. The most prominent historical events related to de Quervain’s thyroiditis include:[1][2][3]
- In 1895, Mygind first described de Quervain’s thyroiditis. Mygind presented 18 cases of thyroiditis akuta simplex (the thyroiditis which affected the previously normal gland without abscess formation).
- In 1904, Fritz de Quervain differentiated de Quervain’s thyroiditis clearly from other forms of thyroiditis based on pathological findings.
- In 1936, de Quervain’s thyroiditis was reaffirmed by de Quervain and Giordanengo.
References
- ↑ Mygind H. “[Thyroiditis akuta simplex. ]”. J Laryngol Rhinol Otol. 9 (4): 181–193.
- ↑ de Quervain F, Giordanengo G. “[Die akute und subakute nicht eiterige Thyreoiditis.]”. Mitt Grenzgeb Med Chir. 44: 538–590.
- ↑ de Quervain F. “[Die acute, nicht eiterige Thyreoiditis und die Beteiligung der Schilddruse an akuten Intoxikationen und Infektionen uberhaupt.]”. Mitt Grenzgeb Med Chir Suppl. 2: 1–165.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
De Quervain’s thyroiditis can be classified according to the development of symptoms into the prodromal stage, hyperthyroid stage, euthyroid stage, and hypothyroid stage.
Classification
De Quervain’s thyroiditis can be classified according to the development of symptoms into the following stages:[1][2][3]
Prodromal stage
The prodromal stage includes low-grade fever and viral flu-like symptoms, such as sore throat, myalgia, arthralgia, and malaise.
Hyperthyroid stage
It follows the prodromal stage and includes the symptoms of thyrotoxicosis.
Euthyroid stage
Thyroid hormones are within the normal range and there are no specific symptoms.
Hypothyroid stage
Thyroid hormones are decreased as a result of glandular damage.
References
- ↑ “Thyroiditis — NEJM”.
- ↑ Engkakul P, Mahachoklertwattana P, Poomthavorn P (2011). “Eponym : de Quervain thyroiditis”. Eur. J. Pediatr. 170 (4): 427–31. doi:10.1007/s00431-010-1306-4. PMID 20886353.
- ↑ Leibovitch G, Maaravi Y, Shalev O (1989). “Severe facial oedema and glossitis associated with mianserin”. Lancet. 2 (8667): 871–2. PMID 2571803.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
The exact pathogenesis of de Quervain’s thyroiditis is unclear. It is proposed that cytotoxic T cell recognition of complex viral and cell antigens presentation leads to the thyroid follicular cell damage which is responsible for the pathogenesis of de Quervain’s thyroiditis. De Quervain’s thyroiditis is usually preceded by a viral prodrome and also have a genetic predisposition. HLA B35 and HLA B15/62 are associated with de Quervain’s thyroiditis.
Pathophysiology
The control, synthesis, and release of the thyroid hormone is usually controlled by hypothalamus and pituitary gland.[1][2]
|
 |
Pathogenesis
The exact pathogenesis of de Quervain’s thyroiditis is unclear, but autoimmunity mechanism is proposed.[3][4][5]
- De Quervain’s thyroiditis is usually preceded by a viral prodrome. Various viral infections are associated with the de Quervain’s thyroiditis including mumps, adenovirus, Epstein–Barr virus, coxsackievirus, cytomegalovirus, influenza, echovirus, and enterovirus.
- De Quervain’s thyroiditis is associated with HLA BB35. It is postulated that the antigen triggers the activation of HLA B35 positive inflammatory cells which in turn activates the cytotoxic T-lymphocytes.
- Cytotoxic T cell recognition of viral and cell antigens presented in a complex leads to the thyroid follicular cell damage.
- The autoimmune process leads to inflammatory cells infiltration of the gland. The changes may lead to granulomatous or non-granulomatous lesions.
- Granulomatous lesion
- Granulomatous lesion comprises of colloid, small lymphocytes, neutrophils, macrophages with or without epithelioid features, and multinucleated giant cells of foreign body type. In the granulomatous lesion, the giant cells are usually CD68+, thyroglobulin– and cytokeratin–. Small lymphocytes in the granulomas are CD3+, CD8+, CD45RO+ cytotoxic T-cells. Numerous plasmacytoid monocytes were also closely associated with the granulomas.
- Non-granulomatous lesion
- Follicles in the non-granulomatous lesion are infiltrated by CD8+ T-lymphocytes, plasmacytoid monocytes, and histiocytes, resulting in disrupted basement membrane and rupture of the follicles.
- Granulomatous lesion
Genetics
- De Quervain’s thyroiditis is associated with:[6][7]
- The human leukocyte antigen (HLA B35
- HLA B15/62 (in rare cases)
Associated conditions
The following conditions may be associated with De Quervain’s thyroiditis:[8]
Gross Pathology
On gross pathology, subacute thyroiditis frequently resembles thyroid malignancy. Subacute thyroiditis usually has the following features:[9]
- Firm to dense consistency
- Pale white color
- Poorly defined margins
- Involvement of adjacent normal thyroid
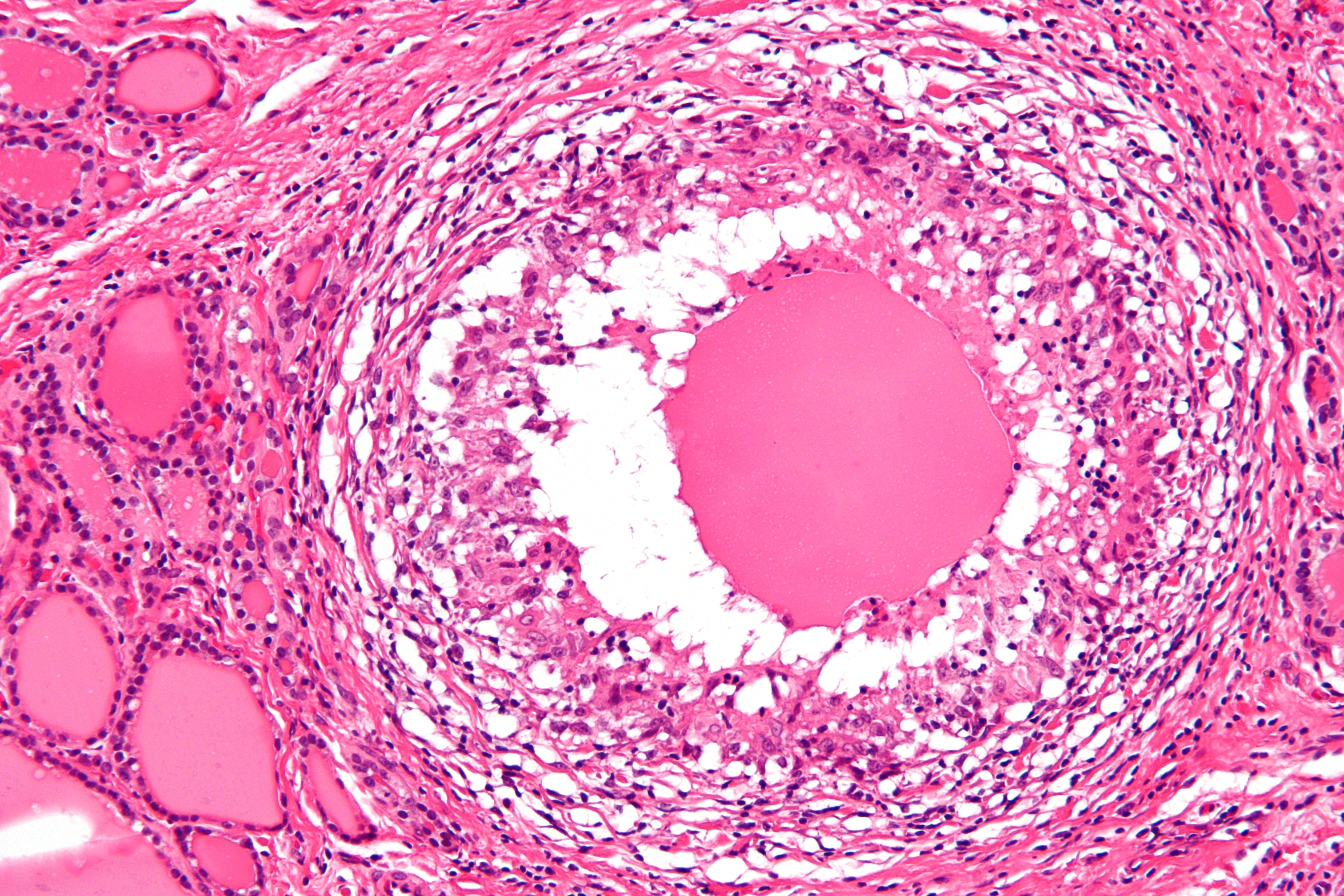
Microscopic pathology
The primary pathology of de Quervain’s thyroiditis is:[3][9]
- Infiltration with polymorphonuclear leukocytes initially
- Predominance of lymphocytes and macrophages in advanced form
- Destruction of the follicular epithelium
- Parenchymal destruction and scar tissue
- Loss of the follicular integrity
Gallery
-
 De Quervain’s thyroiditis (By Nephron – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=18491382)
De Quervain’s thyroiditis (By Nephron – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=18491382) -
 De Quervain’s thyroiditis (By Nephron – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=18491421)
De Quervain’s thyroiditis (By Nephron – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=18491421) -
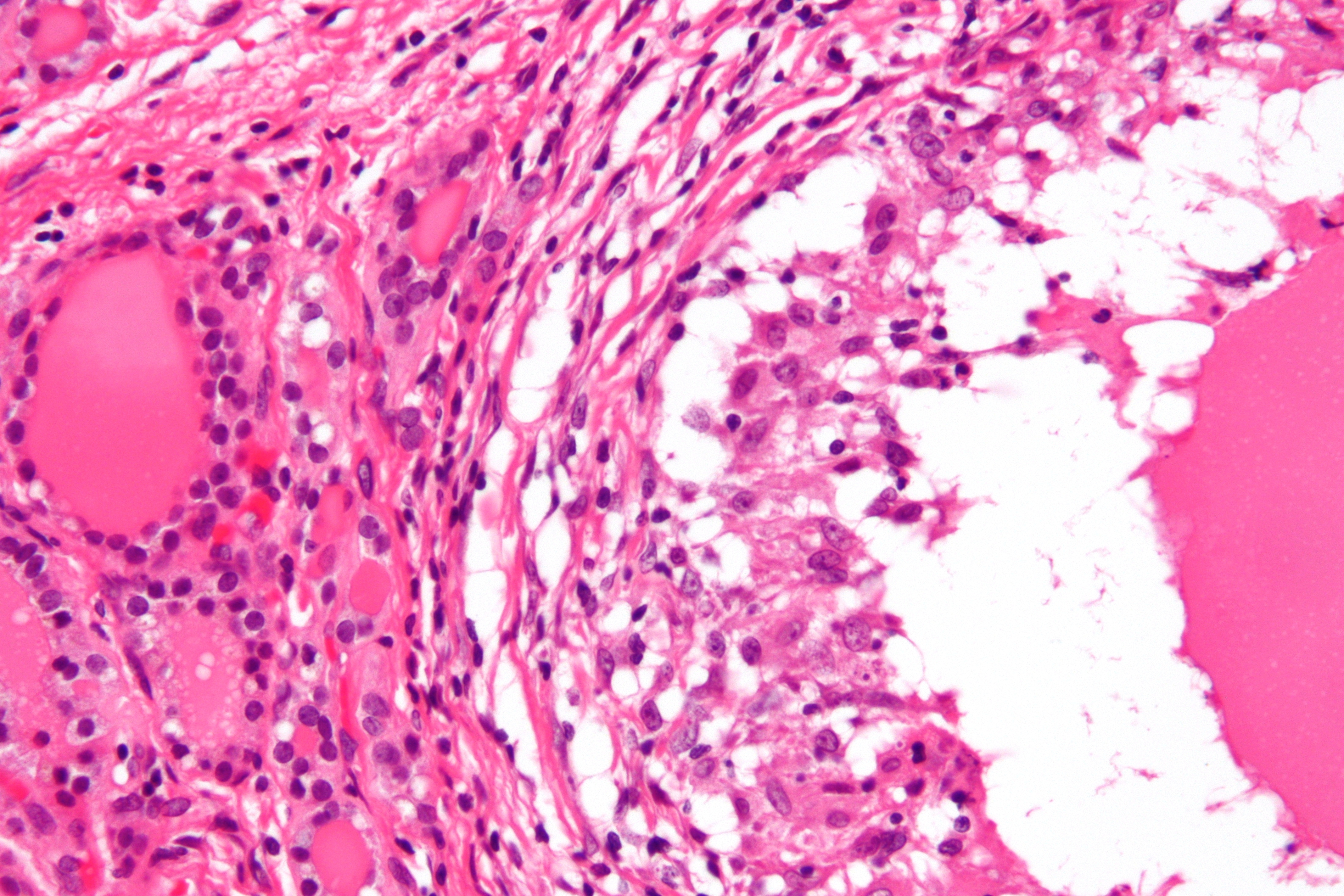 De Quervain’s thyroiditis (By Nephron – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=18491421)
De Quervain’s thyroiditis (By Nephron – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=18491421)



References
- ↑ De Groot LJ, Chrousos G, Dungan K, Feingold KR, Grossman A, Hershman JM, Koch C, Korbonits M, McLachlan R, New M, Purnell J, Rebar R, Singer F, Vinik A, Rousset B, Dupuy C, Miot F, Dumont J. “Thyroid Hormone Synthesis And Secretion”. PMID 25905405.
- ↑ Kirsten D (2000). “The thyroid gland: physiology and pathophysiology”. Neonatal Netw. 19 (8): 11–26. doi:10.1891/0730-0832.19.8.11. PMID 11949270.
- ↑ 3.0 3.1 Kojima M, Nakamura S, Oyama T, Sugihara S, Sakata N, Masawa N (2002). “Cellular composition of subacute thyroiditis. an immunohistochemical study of six cases”. Pathol. Res. Pract. 198 (12): 833–7. doi:10.1078/0344-0338-00344. PMID 12608662.
- ↑ Erdem N, Erdogan M, Ozbek M, Karadeniz M, Cetinkalp S, Ozgen AG, Saygili F, Yilmaz C, Tuzun M, Kabalak T (2007). “Demographic and clinical features of patients with subacute thyroiditis: results of 169 patients from a single university center in Turkey”. J. Endocrinol. Invest. 30 (7): 546–50. PMID 17848836.
- ↑ Desailloud R, Hober D (2009). “Viruses and thyroiditis: an update”. Virol. J. 6: 5. doi:10.1186/1743-422X-6-5. PMC 2654877. PMID 19138419.
- ↑ Nyulassy S, Hnilica P, Buc M, Guman M, Hirschová V, Stefanovic J (1977). “Subacute (de Quervain’s) thyroiditis: association with HLA-Bw35 antigen and abnormalities of the complement system, immunoglobulins and other serum proteins”. J. Clin. Endocrinol. Metab. 45 (2): 270–4. doi:10.1210/jcem-45-2-270. PMID 885992.
- ↑ de Bruin TW, Riekhoff FP, de Boer JJ (1990). “An outbreak of thyrotoxicosis due to atypical subacute thyroiditis”. J. Clin. Endocrinol. Metab. 70 (2): 396–402. doi:10.1210/jcem-70-2-396. PMID 2298855.
- ↑ Fatourechi V, Aniszewski JP, Fatourechi GZ, Atkinson EJ, Jacobsen SJ (2003). “Clinical features and outcome of subacute thyroiditis in an incidence cohort: Olmsted County, Minnesota, study”. J. Clin. Endocrinol. Metab. 88 (5): 2100–5. doi:10.1210/jc.2002-021799. PMID 12727961.
- ↑ 9.0 9.1 Shrestha RT, Hennessey J. Acute and Subacute, and Riedel’s Thyroiditis.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
De Quervain’s thyroiditis may be caused by viruses such as mumps, adenovirus, Epstein–Barr virus, coxsackievirus, cytomegalovirus, influenza, echovirus, and enterovirus. Genetic factors also predispose an individual towards de Quervain’s thyroiditis.
Causes
De Quervain’s thyroiditis is caused by:[1][2][3][4]
References
- ↑ Kojima M, Nakamura S, Oyama T, Sugihara S, Sakata N, Masawa N (2002). “Cellular composition of subacute thyroiditis. an immunohistochemical study of six cases”. Pathol. Res. Pract. 198 (12): 833–7. doi:10.1078/0344-0338-00344. PMID 12608662.
- ↑ Erdem N, Erdogan M, Ozbek M, Karadeniz M, Cetinkalp S, Ozgen AG, Saygili F, Yilmaz C, Tuzun M, Kabalak T (2007). “Demographic and clinical features of patients with subacute thyroiditis: results of 169 patients from a single university center in Turkey”. J. Endocrinol. Invest. 30 (7): 546–50. PMID 17848836.
- ↑ Nyulassy S, Hnilica P, Buc M, Guman M, Hirschová V, Stefanovic J (1977). “Subacute (de Quervain’s) thyroiditis: association with HLA-Bw35 antigen and abnormalities of the complement system, immunoglobulins and other serum proteins”. J. Clin. Endocrinol. Metab. 45 (2): 270–4. doi:10.1210/jcem-45-2-270. PMID 885992.
- ↑ de Bruin TW, Riekhoff FP, de Boer JJ (1990). “An outbreak of thyrotoxicosis due to atypical subacute thyroiditis”. J. Clin. Endocrinol. Metab. 70 (2): 396–402. doi:10.1210/jcem-70-2-396. PMID 2298855.
Differentiating De Quervain’s Thyroiditis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
De Quervain’s thyroiditis must be differentiated from other causes of thyroiditis, such as Hashimoto’s thyroiditis, Riedel’s thyroiditis, and suppurative thyroiditis. De Quervain’s thyroiditis must be differentiated from other causes of thyroiditis, such as De Quervain’s thyroiditis, Riedel’s thyroiditis, and suppurative thyroiditis. De Quervain’s thyroiditis must also be differentiated from other diseases which cause hypothyroidism. As de Quervain’s thyroiditis may cause transient thyrotoxic symptoms, the diseases causing thyrotoxicosis must also be considered in the differential diagnosis.
Differentiating De Quervain’s thyroiditis from other diseases
- De Quervain’s thyroiditis must be differentiated from other causes of thyroiditis, such as Hashimoto’s thyroiditis, Riedel’s thyroiditis, and suppurative thyroiditis.[1]
| Conditions | Causes | Age at onset | Pathological findings | Diagnostic approach |
|---|---|---|---|---|
| Painful subacute (De Quervain’s) thyroiditis |
|
|
| |
| Hashimoto’s thyroiditis |
|
|
|
|
| Silent thyroiditis |
|
|
|
|
| Postpartum thyroiditis |
|
|
|
|
| Riedel’s thyroiditis |
|
|
|
|
| Suppurative thyroiditis (Infectious Thyroiditis) |
|
|
|
|
- De Quervain’s thyroiditis must be differentiated from other causes of hypothyroidism on the basis of history and symptoms and laboratory findings:[2][3][1][4][5][6]
| Disease | History and symptoms | Laboratory findings | Additional findings | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Fever | Pain | TSH | Free T4 | T3 | T3RU† | Thyroglobin | TRH | TPOAb^ | |||
| Transient hypothyroidism | Subacute (de Quervain’s) thyroiditis | +/- | +/- | ↑/↓ | ↓/↑ | Normal | ↓ | ↑ | Normal | Low/absent |
|
| Postpartum thyroiditis | +/- | +/- | ↑/↓ | ↓/↑ | Normal | ↓ | ↑ | Normal/↑ | Present (high titer) |
| |
| Silent thyroiditis | – | – | ↑/↓ | ↓/↑ | Normal | ↓ | ↑ | Normal | Present (high titer) |
| |
| Primary hypothyroidism | Autoimmune (Hashimoto’s thyroiditis) | – | – | ↑* | ↓ | Normal/↓ | Normal/↓ | Normal/↑ | Normal | Present (high titer) |
|
| Riedel’s thyroiditis | – | – | Normal/↑ | Normal/↓ | Normal/↓ | Normal/↓ | Normal | Normal | Usually present |
| |
| Suppurative thyroiditis (Infectious Thyroiditis) | + | + | Normal | Normal | Normal | Normal | Normal | Normal | Absent |
| |
| Others | Drug-induced | – | – | ↑/↓ | ↓/↑ | Normal | ↓ | Normal/↑ | Normal | Absent** |
|
| Radiation-induced | |||||||||||
| Trauma induced | |||||||||||
| Radioiodine induced | |||||||||||
| Thyroidectomy | |||||||||||
| Subclinical hypothyroidism | – | – | ↑ | Normal | Normal | Normal | Normal | Normal | Normal/↑ |
| |
(†)T3RU; Triiodothyronine Resin uptake. (^)TPOAb; Thyroid peroxidase antibodies. (*)TSH may be decreased transiently in the thyrotoxicosis. (**)TPOAb may be present in drug-induced hypo/hyperthyroidism such as Interferon-alpha, interleukin-2, and lithium.
Differentiating de Quervain’s thyroiditis from other causes of thyrotoxicosis
- De Quervain’s thyroiditis can initially present with thyrotoxicosis which must be differentiated from other causes of thyrotoxicosis.[2][3][1][4][5][6][7][8][9]
| Disease | History and symptoms | Laboratory findings | Additional findings | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fever | Pain | TSH | Free T4 | T3 | T3RU† | Thyroglobin | TRH | TSH Receptor Antibody | TPOAb^ | |||
| Thyroiditis | Subacute (de Quervain’s) thyroiditis | +/- | +/- | ↑/↓ | ↓/↑ | Normal | ↓ | ↑ | Normal | Absent | Low/absent |
|
| Hashimoto’s thyroiditis (Hashitoxicosis) | – | – | ↑* | ↓ | Normal/↓ | Normal/↓ | Normal/↑ | Normal | Absent | Present (high titer) |
| |
| Postpartum thyroiditis | +/- | +/- | ↑/↓ | ↓/↑ | Normal | ↓ | ↑ | Normal/↑ | Absent | Present (high titer) |
| |
| Silent thyroiditis | – | – | ↑/↓ | ↓/↑ | Normal | ↓ | ↑ | Normal | Absent | Present (high titer) |
| |
| Primary hyperthyroidism | Grave’s disease | – | – | ↓ | ↑ | Normal/↑ | ↑ | ↑ | Normal | Present | Absent |
|
| Toxic thyroid nodule | – | – | ↓ | ↑ | Normal/↑ | ↑(hot nodule) | Normal/↑ | Normal | Absent | Absent |
– | |
| Secondary hyperthyroidism | Pituitary adenoma | – | – | ↑ | ↑ | Normal/↑ | ↑ | Normal/↑ | Normal | Absent | Absent |
|
| Tertiary hyperthyroidism | Tertiary hyperthyroidism | – | – | ↑ | ↑ | ↑ | ↑ | Normal/↑ | ↑ | Absent | Absent |
|
| Drug induced | Amiodarone type 1 | – | – | ↓ | ↑ | Normal/↑ | ↓ | Normal/↑ | Normal | Absent | Absent |
|
| Amiodarone type 2 | – | – | ↓ | ↑ | Normal/↑ | Absent/↓ | Normal/↑ | Normal | Absent | Absent |
| |
| Others | Factitious thyrotoxicosis | – | – | ↓ | ↑ | Normal/↑ | ↓ | ↓ | Normal | Absent | Absent |
|
| Trophoblastic disease | – | – | ↓ | ↑ | Normal/↑ | ↑ | – | Normal | Absent | Absent |
– | |
| Struma ovarii | – | – | ↓ | ↑ | Normal/↑ | ↓ | – | Normal | Absent | Absent |
– | |
(†)T3RU; Triiodothyronine Resin uptake. (^)TPOAb; Thyroid peroxidase antibodies.
References
- ↑ 1.0 1.1 1.2 “Thyroiditis — NEJM”.
- ↑ 2.0 2.1 Bindra A, Braunstein GD (2006). “Thyroiditis”. Am Fam Physician. 73 (10): 1769–76. PMID 16734054.
- ↑ 3.0 3.1 McDermott MT (2009). “In the clinic. Hypothyroidism”. Ann. Intern. Med. 151 (11): ITC61. doi:10.7326/0003-4819-151-11-200912010-01006. PMID 19949140.
- ↑ 4.0 4.1 Aoki Y, Belin RM, Clickner R, Jeffries R, Phillips L, Mahaffey KR (2007). “Serum TSH and total T4 in the United States population and their association with participant characteristics: National Health and Nutrition Examination Survey (NHANES 1999-2002)”. Thyroid. 17 (12): 1211–23. doi:10.1089/thy.2006.0235. PMID 18177256.
- ↑ 5.0 5.1 Lania A, Persani L, Beck-Peccoz P (2008). “Central hypothyroidism”. Pituitary. 11 (2): 181–6. doi:10.1007/s11102-008-0122-6. PMID 18415684.
- ↑ 6.0 6.1 De Groot LJ, Chrousos G, Dungan K, Feingold KR, Grossman A, Hershman JM, Koch C, Korbonits M, McLachlan R, New M, Purnell J, Rebar R, Singer F, Vinik A, Stockigt J. “Clinical Strategies in the Testing of Thyroid Function”. PMID 25905413.
- ↑ “Clinical Finding and Thyroid Function in Women with Struma Ovarii”.
- ↑ Vaidya B, Pearce SH (2014). “Diagnosis and management of thyrotoxicosis”. BMJ. 349: g5128. PMID 25146390.
- ↑ “Think thyrotoxicosis factitia – measure thyroglobulin | The BMJ”.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
De Quervain’s thyroiditis is particularly common in middle-aged women, Asians, and Whites. Annually, there are around 22 per 100,000 individuals worldwide.
Epidemiology and Demographics
De Quervain’s thyroiditis is the most common cause of painful thyroid disease in adults which may account for up to 0.027 per 6496 of adult thyroid diseases. The prevalence is estimated to be 0.41 per 100,000 adult population.[1][2]
Prevalence
The prevalence is estimated to be 0.41 per 100,000 adult population.[1]
Incidence
The overall incidence of endogenous de Quervain’s thyroiditis is approximately 4.9 cases per 100,000 per year.[3]
Age
De Quervain’s thyroiditis is more common in fourth and fifth decades of life.[1][3]
Gender
De Quervain’s thyroiditis is more common in females.The female to male ratio ranges between 2:1 to 6:1.[1][4]
Race
There is no evidence of racial predilection in de Quervain’s thyroiditis.
Developed and Developing Countries
There is no regional predilection reported towards de Quervain’s thyroiditis but it was the cause in 1.8% of hypothyroid cases in a study done in Denmark.[5]
References
- ↑ 1.0 1.1 1.2 1.3 Erdem N, Erdogan M, Ozbek M, Karadeniz M, Cetinkalp S, Ozgen AG, Saygili F, Yilmaz C, Tuzun M, Kabalak T (2007). “Demographic and clinical features of patients with subacute thyroiditis: results of 169 patients from a single university center in Turkey”. J. Endocrinol. Invest. 30 (7): 546–50. PMID 17848836.
- ↑ De Groot LJ, Chrousos G, Dungan K, Feingold KR, Grossman A, Hershman JM, Koch C, Korbonits M, McLachlan R, New M, Purnell J, Rebar R, Singer F, Vinik A, Shrestha RT, Hennessey J. PMID 25905408. Missing or empty
|title=(help) - ↑ 3.0 3.1 Fatourechi V, Aniszewski JP, Fatourechi GZ, Atkinson EJ, Jacobsen SJ (2003). “Clinical features and outcome of subacute thyroiditis in an incidence cohort: Olmsted County, Minnesota, study”. J. Clin. Endocrinol. Metab. 88 (5): 2100–5. doi:10.1210/jc.2002-021799. PMID 12727961.
- ↑ Bindra A, Braunstein GD (2006). “Thyroiditis”. Am Fam Physician. 73 (10): 1769–76. PMID 16734054.
- ↑ Groot, Leslie (2010). Endocrinology adult and pediatric : the thyroid gland. Philadelphia, Pennsylvania: Saunders. ISBN 9780323240642.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
Common risk factors in the development of de Quervain’s thyroiditis are viral illness, family history, and female gender.
Risk Factors
The risk factors for de Quervain’s thyroiditis are:[1][2][3][4][5][6]
Common Risk factors
- Viral illness
- Family history
- Female gender
- Human leukocyte antigen (HLA) B35
Less common risk factors
- HLA-B15/62
References
- ↑ Erdem N, Erdogan M, Ozbek M, Karadeniz M, Cetinkalp S, Ozgen AG, Saygili F, Yilmaz C, Tuzun M, Kabalak T (2007). “Demographic and clinical features of patients with subacute thyroiditis: results of 169 patients from a single university center in Turkey”. J. Endocrinol. Invest. 30 (7): 546–50. PMID 17848836.
- ↑ Bindra A, Braunstein GD (2006). “Thyroiditis”. Am Fam Physician. 73 (10): 1769–76. PMID 16734054.
- ↑ Nyulassy S, Hnilica P, Buc M, Guman M, Hirschová V, Stefanovic J (1977). “Subacute (de Quervain’s) thyroiditis: association with HLA-Bw35 antigen and abnormalities of the complement system, immunoglobulins and other serum proteins”. J. Clin. Endocrinol. Metab. 45 (2): 270–4. doi:10.1210/jcem-45-2-270. PMID 885992.
- ↑ de Bruin TW, Riekhoff FP, de Boer JJ (1990). “An outbreak of thyrotoxicosis due to atypical subacute thyroiditis”. J. Clin. Endocrinol. Metab. 70 (2): 396–402. doi:10.1210/jcem-70-2-396. PMID 2298855.
- ↑ Kojima M, Nakamura S, Oyama T, Sugihara S, Sakata N, Masawa N (2002). “Cellular composition of subacute thyroiditis. an immunohistochemical study of six cases”. Pathol. Res. Pract. 198 (12): 833–7. doi:10.1078/0344-0338-00344. PMID 12608662.
- ↑ Desailloud R, Hober D (2009). “Viruses and thyroiditis: an update”. Virol. J. 6: 5. doi:10.1186/1743-422X-6-5. PMC 2654877. PMID 19138419.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
There is insufficient evidence to recommend routine screening for de Quervain’s thyroiditis.
Screening
There is insufficient evidence to recommend routine screening for de Quervain’s thyroiditis.
References
Natural History, Complications, and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
De Quervain’s thyroiditis develops after a viral prodrome and presents as painful thyroid gland with symptoms of thyrotoxicosis. It further leads to a euthyroid phase and eventually hypothyroid phase before the complete resolution of the disease. Complications include hypothyroidism and rarely, esophageal or tracheal compression.
Natural history, complications, and prognosis
Natural history
De Quervain’s thyroiditis develops after a viral prodrome and presents as painful thyroid gland with symptoms of thyrotoxicosis. It further leads to a euthyroid phase and eventually hypothyroid phase before the complete resolution of the disease.[1][2][3]
1. Prodromal stage
It includes:
- Low-grade fever and viral flu-like symptoms, such as sore throat, myalgia, arthralgia, and malaise.
- High-grade fever and neck pain with a tender and diffuse thyroid gland enlargement follow flu-like symptoms.
2. Hyperthyroid stage
It follows the prodromal stage and includes the symptoms of thyrotoxicosis such as:
- Tachycardia and tremors
- Irritability and nervousness
3. Euthyroid stage
Thyrotoxic stage is followed by a 1–3-week period of euthyroid phase.
4. Hypothyroid stage
The transient hypothyroid stage lasts for 6-12 months.
- Rarely, the hypothyroid stage may persist for a longer duration.
Complications
Complications that can develop as a result of de Quervain’s thyroiditis are:[1][2][3]
- Hypothyroidism
- Tracheal compression
- Esophageal compression
Prognosis
Prognosis of de Quervain’s thyroiditis is usually good.
References
- ↑ 1.0 1.1 “Thyroiditis — NEJM”.
- ↑ 2.0 2.1 Engkakul P, Mahachoklertwattana P, Poomthavorn P (2011). “Eponym : de Quervain thyroiditis”. Eur. J. Pediatr. 170 (4): 427–31. doi:10.1007/s00431-010-1306-4. PMID 20886353.
- ↑ 3.0 3.1 Leibovitch G, Maaravi Y, Shalev O (1989). “Severe facial oedema and glossitis associated with mianserin”. Lancet. 2 (8667): 871–2. PMID 2571803.
Diagnosis
Diagnosis
Diagnostic Criteria |History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | CT | MRI | Echocardiography or Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary prevention |Secondary prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH