
Necrotizing fasciitis
For patient information on this page, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yamuna Kondapally, M.B.B.S[2], Cafer Zorkun, M.D., Ph.D. [3]
Synonyms and keywords:NF; Phagadena; Phagadena gangrenosum; Meleney’s gangrene; Hemolytic streptococcal gangrene; Flesh eating bacteria; Hospital gangrene; Acute dermal gangrene; Suppurative fasciitis; Synergistic necrotizing cellulitis; Gangrenous ulcer; Malignant ulcer; Putrid ulcer; Necrotizing erysipelas; Nonclostridial gas gangrene; Bacterial synergistic gangrene
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yamuna Kondapally, M.B.B.S[2]
Overview
Necrotizing fasciitis or fasciitis necroticans, commonly known as “flesh-eating bacteria,” is a rare infection of the deeper layers of skin and subcutaneous tissues, easily spreading across the fascial plane within the subcutaneous tissue. Many types of bacteria can cause necrotizing fasciitis (eg. Group A streptococcus, Vibrio vulnificus, Clostridium perfringens, Bacteroides fragilis), of which Group A streptococcus (also known as Streptococcus pyogenes) is the most common cause. It is severe inflammation of the muscle sheath that leads to necrosis of subcutaneous tissue and adjacent fascia.[1][2]
Historical Perspective
Narcotizing fasciitis was first described by Hippocrates in the fifth century B.C. as the complication of erysipelas.[3][4] During the Civil War, necrotizing fasciitis was described as “hospital gangrene” by Confederate Army surgeon Joseph Jones.[5][6] In 1924, Frank L. Meleney reported a series of 20 patients as having hemolytic streptococcal gangrene, later called Meleney’s gangrene.[7] Necrotizing fasciitis of perineum was described in 1883 by the French physician Jean Alfred Fournier.[8]
Classification
Necrotizing fasciitis may be classified according to International Classification of Diseases-10 (ICD-10) into M72.6 Necrotizing fasciitis.[9] Based on microbiological findings, necrotizing fasciitis may be classified into four types: Type I, Type II, Type III, and Type IV. Necrotizing fasciitis is further classified based on anatomic location and severity of symptoms.[10]
Pathophysiology
The pathophysiology of necrotizing fasciitis is common to all types, but the speed of development and associated clinical features differs depending on the causative organisms. Following transmission, the bacteria uses the entry site to invade the fascial planes which causes the wide spread necrosis of superficial fascia, deep fascia, subcutaneous fat, nerves, arteries, and veins. Necrotizing fasciitis can be a serious complication of omphalitis in the neonate. The pathogenesis of necrotizing fasciitis is the result of bacterial and host factors. The exact pathogenesis of type 1 necrotizing fasciitis is not fully understood but polymicrobial species work synergistically to enhance the spread of infection. Group A streptococcus is the most common causative agent of type 2 necrotizing fasciitis. Bacterial virulence factors, exotoxins, superantigens and host immune system plays a major role in the pathogenesis of type II necrotizing fasciitis. Recurrent necrotizing fasciitis is caused by MRSA. On gross pathology, the characteristic findings of necrotizing fasciitis include subcutaneous emphysema, skin sloughing, bulae and necrosis. Inflammatory changes are seen on microscopic histopathology.[1]
Causes
The causative organisms vary depending on the type of necrotizing fasciitis: Type I (polymicrobial), Type II (monomicrobial), Type III (Gram negative monomicrobial, including marine related organisms) and Type IV (fungal).[1]
Differentiating Necrotizing Fasciitis from Other Diseases
Necrotizing fasciitis must be differentiated from other diseases that cause erythema, pain, edema and necrosis of soft tissues such as sunburn, cellulitis, erysipelas, diabetic myonecrosis and vasculitis.[11]
Epidemiology and Demographics
The incidence of necrotizing fasciitis in adults is 0.40 cases per 100,000 people/year and the incidence in children is higher at 0.08 cases per 100,000 people/year.The overall mortality rate in the United states from 2003- 2013 was 4.8/1,000,000 per year. Patients from all age groups can develop necrotizing fasciitis but slightly more common among >50 years age and effects men and women equally.The incidence rate of necrotizing fasciitis is high in black, Hispanic, and American Indian individuals compared to Whites and low in Asian individuals.
Risk Factors
Common risk factors in the development of necrotizing fasciitis include trauma, alcoholism, diabetes, intravenous drug abuse, immunosupression and burns.[1]
Screening
According to the U.S. Preventive Service Task Force (USPSTF), there is insufficient evidence to recommend routine screening for necrotizing fasciitis.
Natural History, Complications, and Prognosis
If left untreated, the acute inflammatory changes spread quickly, accompanied by high fever and extreme weakness leading to necrosis of soft tissue. Common complications of necrotizing fasciitis include limb loss, sepsis, toxic shock syndrome, disseminated intravascular coagulation (DIC). Depending on the extent of the necrotizing fasciitis at the time of diagnosis, the prognosis may vary. The prognostic factors associated with necrotizing fasciitis include diabetes mellitus, acute renal failure, admission serum creatinine >2mg/dl and admission white blood cells >30,000 cells mm3.
Diagnosis
Diagnostic Criteria
LRINEC is a diagnostic scoring system used to distinguish necrotizing fasciitis from other soft tissue infections.
History and Symptoms
During early stages, the symptoms of necrotizing fasciitis are non-specific. Symptoms include fever, nausea, and fatigue.[12][13]
Physical Examination
Physical examination of patients with necrotizing fasciitis is usually remarkable for local soft tissue signs such as warmth, tenderness beyond margins of erythema, swelling, erythema with ill defined margins, blistering/bullae, skin discoloration, foul discharge (greyish or brown discharge), fluctuance, crepitus, skin sloughing or necrosis, absence of lymphangitis or lymphadenopathy (lymphangitis is rarely observed in necrotizing fasciitis patients), sensory and motor deficits (e.g. localized anesthesia).[14][12] Finger probe test is useful in the diagnosis of necrotizing fasciitis.[12]
Laboratory Findings
Laboratory findings consistent with the diagnosis of necrotizing fasciitis include positive blood and tissue culture, elevated inflammatory markers, leukocytosis and elevated serum creatinine.
Imaging Findings
Electrocardiogram
There are no electrocardiogram findings associated with necrotizing fasciitis. Electrocardiogram may be helpful in the diagnosis and management of complications of necrotizing fasciitis.
X Ray
On x ray of affected area, necrotizing fasciitis is characterized by subcutaneous gas or soft tissue swelling (specific x-ray finding) and increased soft tissue thickness and opacity. Chest x-ray findings associated with necrotizing fasciitis include early changes of fluid overload and adult (acute) respiratory distress syndrome (ARDS).
CT
On CT scan, necrotizing fasciitis is characterized by subcutaneous emphysema, asymmetrical fascial thickening associated with fat stranding, edema and abscesses.
MRI
On MRI, necrotizing fasciitis is characterized by features such as loss of muscle texture and high signal intensity compatible with intramuscular hemorrhage in T1 weighted image. On T2-weighted images, subcutaneous and intramuscular edema in a reticulated pattern and subfascial and interfascial crescentic fluid collection are seen.
Ultrasound
Ultrasound is more useful in children (with raising incidence after primary varicella infection). On ultrasound, necrotizing fasciitis is characterized by distorted and thickened fascial planes with turbid fluid accumulation in the fascial layers, subcutaneous edema and soft tissue gas.
Biopsy
On frozen section biopsy, histologic criteria for diagnosis of necrotizing fasciitis include necrosis of superficial fascia, fibrinous thrombi of arteries and veins, polymorphonuclear infiltration of the dermis and fascia, and presence of microorganisms within the destroyed fascia and dermis.
Treatment
Medical Therapy
Necrotizing fasciitis is a medical and surgical emergency. The mainstay of therapy for necrotizing fasciitis includes surgical exploration and debridement along with antimicrobial therapy. Initial pharmacologic therapy often includes a combination of intravenous antibiotics including penicillin, vancomycin, and/or clindamycin.
Surgery
Surgery is the mainstay of treatment for necrotizing fasciitis. Immediate surgical referral remains the only method of reducing mortality and morbidity.
Primary Prevention
Effective measures for the primary prevention of necrotizing fasciitis include prevention of trauma/breaks in skin integrity, treatment of underlying infections, hand washing, proper wound care and proper management of underlying co-morbidities.
Secondary Prevention
Secondary prevention strategies following necrotizing fasciitis include early diagnosis and prompt treatment with either antibiotics or surgery. This strategy prevents or slows the progression and complications of the disease.
References
- ↑ 1.0 1.1 1.2 1.3 Misiakos EP, Bagias G, Patapis P, Sotiropoulos D, Kanavidis P, Machairas A (2014). “Current concepts in the management of necrotizing fasciitis”. Front Surg. 1: 36. doi:10.3389/fsurg.2014.00036. PMC 4286984. PMID 25593960.
- ↑ Hakkarainen TW, Kopari NM, Pham TN, Evans HL (2014). “Necrotizing soft tissue infections: review and current concepts in treatment, systems of care, and outcomes”. Curr Probl Surg. 51 (8): 344–62. doi:10.1067/j.cpsurg.2014.06.001. PMC 4199388. PMID 25069713.
- ↑ Descamps V, Aitken J, Lee MG (1994). “Hippocrates on necrotising fasciitis”. Lancet. 344 (8921): 556. PMID 7914656.
- ↑ Hasham S, Matteucci P, Stanley PR, Hart NB (2005). “Necrotising fasciitis”. BMJ. 330 (7495): 830–3. doi:10.1136/bmj.330.7495.830. PMC 556077. PMID 15817551.
- ↑ WILSON B (1952). “Necrotizing fasciitis”. Am Surg. 18 (4): 416–31. PMID 14915014.
- ↑ Janevicius RV, Hann SE, Batt MD (1982). “Necrotizing fasciitis”. Surg Gynecol Obstet. 154 (1): 97–102. PMID 7031943.
- ↑ Sadasivan J, Maroju NK, Balasubramaniam A (2013). “Necrotizing fasciitis”. Indian J Plast Surg. 46 (3): 472–8. doi:10.4103/0970-0358.121978. PMC 3897089. PMID 24459334.
- ↑ Chennamsetty A, Khourdaji I, Burks F, Killinger KA (2015). “Corary diagnosis and management of Fournier’s gangrene”. Ther Adv Urol. 7 (4): 203–15. doi:10.1177/1756287215584740. PMC 4580094. PMID 26445600.
- ↑ ICD-10 version:2016. http://apps.who.int/classifications/icd10/browse/2016/en#/M72.6 2016 Accessed on August 25,2016
- ↑ Lancerotto L, Tocco I, Salmaso R, Vindigni V, Bassetto F (2012). “Necrotizing fasciitis: classification, diagnosis, and management”. J Trauma Acute Care Surg. 72 (3): 560–6. doi:10.1097/TA.0b013e318232a6b3. PMID 22491537.
- ↑ Wong CH, Wang YS (2005). “The diagnosis of necrotizing fasciitis”. Curr Opin Infect Dis. 18 (2): 101–6. PMID 15735411.
- ↑ 12.0 12.1 12.2 Puvanendran R, Huey JC, Pasupathy S (2009). “Necrotizing fasciitis”. Can Fam Physician. 55 (10): 981–7. PMC 2762295. PMID 19826154.
- ↑ Taviloglu K, Yanar H (2007). “Necrotizing fasciitis: strategies for diagnosis and management”. World J Emerg Surg. 2: 19. doi:10.1186/1749-7922-2-19. PMC 1988793. PMID 17683625.
- ↑ Young MH, Aronoff DM, Engleberg NC (2005). “Necrotizing fasciitis: pathogenesis and treatment”. Expert Rev Anti Infect Ther. 3 (2): 279–94. doi:10.1586/14787210.3.2.279. PMID 15918785.
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yamuna Kondapally, M.B.B.S[2]
Overview
Narcotizing fasciitis was first described by Hippocrates in the fifth century B.C. as the complication of erysipelas.[1][2] During the Civil War, necrotizing fasciitis was described as “hospital gangrene” by Confederate Army surgeon Joseph Jones.[3][4] In 1924, Frank L. Meleney reported a series of 20 patients as having hemolytic streptococcal gangrene, later called Meleney’s gangrene.[5] Necrotizing fasciitis of perineum was described in 1883 by the French physician Jean Alfred Fournier.[6]
Historical Perspective
- Necrotizing fasciitis was first described by Hippocrates in the fifth century B.C. as the complication of erysipelas.[1][2]
- During the Civil War, necrotizing faciitis was described as “hospital gangrene” by Confederate Army surgeon Joseph Jones.[3][4][7]
- In 1924, Frank L. Meleney reported a series of 20 patients as having hemolytic streptococcal gangrene, later called Meleney’s gangrene.[5]
- The association between bacterial infection and necrotizing fasciitis was made in 1918.
- In 1952, the disease was named as necrotizing fasciitis by Wilson.[3]
- Necrotizing fasciitis of perineum was described in 1883 by the French physician, Jean Alfred Fournier.[6]
- Guiliano and colleagues divided the necrotizing fasciitis into type I and type II.[8]
- In 1989, Stevens and colleagues were the first to characterize unique clinical characteristics associated with GASNF.[9]
- The soft tissue infections were first classified as either local or spreading by Smith et al.[10]
References
- ↑ 1.0 1.1 Descamps V, Aitken J, Lee MG (1994). “Hippocrates on necrotising fasciitis”. Lancet. 344 (8921): 556. PMID 7914656.
- ↑ 2.0 2.1 Hasham S, Matteucci P, Stanley PR, Hart NB (2005). “Necrotising fasciitis”. BMJ. 330 (7495): 830–3. doi:10.1136/bmj.330.7495.830. PMC 556077. PMID 15817551.
- ↑ 3.0 3.1 3.2 WILSON B (1952). “Necrotizing fasciitis”. Am Surg. 18 (4): 416–31. PMID 14915014.
- ↑ 4.0 4.1 Janevicius RV, Hann SE, Batt MD (1982). “Necrotizing fasciitis”. Surg Gynecol Obstet. 154 (1): 97–102. PMID 7031943.
- ↑ 5.0 5.1 Sadasivan J, Maroju NK, Balasubramaniam A (2013). “Necrotizing fasciitis”. Indian J Plast Surg. 46 (3): 472–8. doi:10.4103/0970-0358.121978. PMC 3897089. PMID 24459334.
- ↑ 6.0 6.1 Chennamsetty A, Khourdaji I, Burks F, Killinger KA (2015). “Corary diagnosis and management of Fournier’s gangrene”. Ther Adv Urol. 7 (4): 203–15. doi:10.1177/1756287215584740. PMC 4580094. PMID 26445600.
- ↑ Quirk WF, Sternbach G (1996). “Joseph Jones: infection with flesh eating bacteria”. J Emerg Med. 14 (6): 747–53. PMID 8969999.
- ↑ Krieg A, Röhrborn A, Schulte Am Esch J, Schubert D, Poll LW, Ohmann C; et al. (2009). “Necrotizing fasciitis: microbiological characteristics and predictors of postoperative outcome”. Eur J Med Res. 14 (1): 30–6. PMC 3352202. PMID 19258208.
- ↑ Stevens DL (1995). “Streptococcal toxic-shock syndrome: spectrum of disease, pathogenesis, and new concepts in treatment”. Emerg Infect Dis. 1 (3): 69–78. doi:10.3201/eid0103.950301. PMC 2626872. PMID 8903167.
- ↑ Smith AJ, Daniels T, Bohnen JM (1996). “Soft tissue infections and the diabetic foot”. Am J Surg. 172 (6A): 7S–12S. PMID 9003684.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yamuna Kondapally, M.B.B.S[2]
Overview
Necrotizing fasciitis may be classified according to International Classification of Diseases-10 (ICD-10) into M72.6 Necrotizing fasciitis.[1] Based on microbiological findings, necrotizing fasciitis may be classified into four types: Type I, Type II, Type III, and Type IV. Necrotizing fasciitis is further classified based on anatomic location and severity of symptoms.[2]
Classification
Based on microbiological findings, necrotizing fasciitis may be classified into four types.[3][4][5][6][7][8][9]
| Type | Organism |
|---|---|
| Type 1 (70%-80% cases) Polymicrobial/Synergistic |
● Mixed aerobes and anaerobes ● Often bowel flora-derived |
| Type 2 (20% to 30% cases) Monomicrobial |
● Beta-Hemolytic Streptococci group A (Streptococcus pyogenes) ● with/without Staphylococcus aureus ● Skin or throat derived |
| Type 3 (common in Asia) Gram negative monomicrobial NF (including marine related organisms) |
● Vibrio spp mainly |
| Type 4 Fungal |
● Candida (Immunocompromised patients) ● Zygomycetes (Immunocompetent patients) |
- Based on anatomic location, necrotizing fasciitis may be classified into:[2]
- Fournier’s gangrene (necrotizing fasciitis of perineum)
- Craniofascial necrotizing fasciitis
- Cervical fasciitis
- Ludwig’s angina (submandibular and sublingual spaces)[10]
- Based on severity of disease, necrotizing fasciitis is classified into:[11]
- Hyperacute
- Sub-acute
References
- ↑ ICD-10 version:2016. http://apps.who.int/classifications/icd10/browse/2016/en#/M72.6 2016 Accessed on August 25,2016
- ↑ 2.0 2.1 Lancerotto L, Tocco I, Salmaso R, Vindigni V, Bassetto F (2012). “Necrotizing fasciitis: classification, diagnosis, and management”. J Trauma Acute Care Surg. 72 (3): 560–6. doi:10.1097/TA.0b013e318232a6b3. PMID 22491537.
- ↑ Morgan MS (2010). “Diagnosis and management of necrotising fasciitis: a multiparametric approach”. J Hosp Infect. 75 (4): 249–57. doi:10.1016/j.jhin.2010.01.028. PMID 20542593.
- ↑ Giuliano A, Lewis F, Hadley K, Blaisdell FW (1977). “Bacteriology of necrotizing fasciitis”. Am J Surg. 134 (1): 52–7. PMID 327844.
- ↑ Goodell KH, Jordan MR, Graham R, Cassidy C, Nasraway SA (2004). “Rapidly advancing necrotizing fasciitis caused by Photobacterium (Vibrio) damsela: a hyperaggressive variant”. Crit Care Med. 32 (1): 278–81. doi:10.1097/01.CCM.0000104920.01254.82. PMID 14707592.
- ↑ Monaghan SF, Anjaria D, Mohr A, Livingston DH (2008). “Necrotizing fasciitis and sepsis caused by Aeromonas hydrophila after crush injury of the lower extremity”. Surg Infect (Larchmt). 9 (4): 459–67. doi:10.1089/sur.2007.028. PMID 18687029.
- ↑ Jain D, Kumar Y, Vasishta RK, Rajesh L, Pattari SK, Chakrabarti A (2006). “Zygomycotic necrotizing fasciitis in immunocompetent patients: a series of 18 cases”. Mod Pathol. 19 (9): 1221–6. doi:10.1038/modpathol.3800639. PMID 16741524.
- ↑ Quirk WF, Sternbach G (1996). “Joseph Jones: infection with flesh eating bacteria”. J Emerg Med. 14 (6): 747–53. PMID 8969999.
- ↑ Kihiczak GG, Schwartz RA, Kapila R (2006). “Necrotizing fasciitis: a deadly infection”. J Eur Acad Dermatol Venereol. 20 (4): 365–9. doi:10.1111/j.1468-3083.2006.01487.x. PMID 16643131.
- ↑ Wasson J, Hopkins C, Bowdler D (2006). “Did Ludwig’s angina kill Ludwig?”. J Laryngol Otol. 120 (5): 363–5. doi:10.1017/S0022215106000806. PMID 16696873.
- ↑ Wong CH, Wang YS (2005). “The diagnosis of necrotizing fasciitis”. Curr Opin Infect Dis. 18 (2): 101–6. PMID 15735411.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yamuna Kondapally, M.B.B.S[2]
Overview
The pathophysiology of necrotizing fasciitis is common to all types, but the speed of development and associated clinical features differs depending on the causative organisms. Following transmission, the bacteria uses the entry site to invade the fascial planes which causes the wide spread necrosis of superficial fascia, deep fascia, subcutaneous fat, nerves, arteries, and veins. Necrotizing fasciitis can be a serious complication of omphalitis in the neonate. The pathogenesis of necrotizing fasciitis is the result of bacterial and host factors. The exact pathogenesis of type 1 necrotizing fasciitis is not fully understood but polymicrobial species work synergistically to enhance the spread of infection. Group A streptococcus is the most common causative agent of type 2 necrotizing fasciitis. Bacterial virulence factors, exotoxins, superantigens and host immune system plays a major role in the pathogenesis of type II necrotizing fasciitis. Recurrent necrotizing fasciitis is caused by MRSA. On gross pathology, the characteristic findings of necrotizing fasciitis include subcutaneous emphysema, skin sloughing, bulae and necrosis. Inflammatory changes are seen on microscopic histopathology.[1]
Pathophysiology
The pathophysiology of necrotizing fasciitis is common to all types of necrotizing fasciitis, but the speed of development and associated clinical features differs depending on the causative organisms.[1]
- External trauma (e.g., laceration, abrasion, burn, insect bite)
- Direct spread from a perforated viscus (particularly colon, rectum, or anus) or another surgical procedure (e.g., vasectomy, hemorrhoidectomy)
- Urogenital organ
- Perirectal abscess
- Decubitus ulcer
- Following transmission, the bacteria uses the entry site to invade the fascial planes which causes the wide spread necrosis of superficial fascia, deep fascia, subcutaneous fat, nerves, arteries, and veins.
- Superficial skin and deeper muscles are typically spared.
- In late stages, lesions develop liquefactive necrosis at all tissue levels.
Necrotizing fasciitis in neonate
- Necrotizing fasciitis can be a serious complication of omphalitis in the neonate.
- The omphalitis may progress resulting in purplish discoloration and periumbilical necrosis.
- The necrosis may extend to the flanks and even onto the chest wall.
Pathogenesis
The pathogenesis of necrotizing fasciitis is the result of bacterial and host factors.[4][5]
Type 1 NF
- The exact pathogenesis of type 1 necrotizing fasciitis is not fully understood.
- It is thought that type 1 NF is caused by polymicrobial species that work synergistically to enhance the spread of infection.
- Synergistic NF is comparatively slow process evolving over days.
- It usually develops in the area where gut flora breaches the mucosa, entering the tissue planes.
Type 2 NF
- Group A streptococcus is the most common causative agent of type 2 NF.[6][7]
- Type 2 NF is initially insidious in onset but progress more rapidly.[8]
- The disease may appear spontaneously with no obvious focus. Hematogenous infection from many foci such as skin, throat, ascending vaginitis, primary peritonitis reaches the fascial layer or seeds vimentin exposed by muscle damage.
- Direct inoculation of GAS through wounds or associated surgery is less common.
- The pathogenesis of type 2 NF is the result of the following process:
- Inhibition of phagocytosis of bacteria by hyaluronic acid capsule and M protein
- Adherence of bacteria to host cell through adherence factors such as M protein, protein F and lipoteichoic acid[9]
- Release of exotoxins (streptococcal pyogenic exotoxins and superantigen) into blood produce massive proliferation of T cells and cascading release of cytokines activating inflammatory process
- Activation of inflammatory process which begins to kill bacteria
- The streptococci release massive amounts of enzymes, hemolysins, DNAase, proteases and collagenases which destroy the normal skin and surrounding tissue with progressive coagulative necrosis
- The inflamed cells release more cytokines that stimulate more inflammatory cells
- The massive release of cytokines result in systemic inflammatory response syndrome resulting in shock, organ failure, depression of myocardial function and immune suppression
- Stimulation of T-cells by superantigen causes activation of complement pathway, the bradykinin–kallikrein system, and the coagulation cascade, worsening small vessel thrombosis and tissue ischemia. Tissue ischemia impedes oxidative destruction of bacteria by polymorphonuclear cells and prevents adequate delivery of antibiotics.
- The blood flow to local tissue is compromised due to thrombosis of large number of dermal capillaries by the local hypercoaguable state, platelet–neutrophil plugging of vessels and increased interstitial pressure
- Nerves supplying the necrotizing areas of skin die, the central areas become anaesthetic and peripheral areas remain tender
- In later stages, infection from deeper layers ascends, producing edema of epidermal and dermal layers (peau d’orange) and a woody firmness of the tissues
- The fascial and nerve destruction results in sensory and motor deficits, which causes progression of hemorrhagic bulae to cutaneous gangrene
Recurrent necrotizing fasciitis
Recurrent NF is seen in following conditions:[10]
- Methicillin resistant staphylococcus aureus (MRSA)
- Complement C4 deficiency
Gross pathology
On gross pathology the characteristic findings of necrotizing fasciitis include:[11]
- Subcutaneous emphysema
- Edema
- Erythema
- Bulae
- Skin sloughing
- Dull grey discoloration
-
 By Nephron – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=19107063
By Nephron – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=19107063

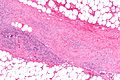
Microscopic Pathology
On microscopic histopathological analysis, the characteristic findings of necrotizing fasciitis are[11]
- Early stages
- Obliterative vasculitis with microangiopathic thrombosis
- Acute inflammation of subcutaneous tissue
- Superficial hyaline necrosis along with edema and inflammation of the dermis and subcutaneous fat
- Dense neutrophil-predominant inflammatory infiltrate
- Late stages
- Noninflammatory intravascular coagulation and hemorrhage
- Myonecrosis
-
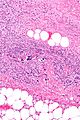 By Piotr Smuszkiewicz, Iwona Trojanowska and Hanna Tomczak – Late diagnosed necrotizing fasciitis as a cause of multiorgan dysfunction syndrome: A case report. Cases Journal 2008, 1:125. doi:10.1186/1757-1626-1-125, CC BY 2.0, https://commons.wikimedia.org/w/index.php?curid=5639655
By Piotr Smuszkiewicz, Iwona Trojanowska and Hanna Tomczak – Late diagnosed necrotizing fasciitis as a cause of multiorgan dysfunction syndrome: A case report. Cases Journal 2008, 1:125. doi:10.1186/1757-1626-1-125, CC BY 2.0, https://commons.wikimedia.org/w/index.php?curid=5639655 -
 By Piotr Smuszkiewicz, Iwona Trojanowska and Hanna Tomczak – Late diagnosed necrotizing fasciitis as a cause of multiorgan dysfunction syndrome: A case report. Cases Journal 2008, 1:125. doi:10.1186/1757-1626-1-125, CC BY 2.0, https://commons.wikimedia.org/w/index.php?curid=5639655
By Piotr Smuszkiewicz, Iwona Trojanowska and Hanna Tomczak – Late diagnosed necrotizing fasciitis as a cause of multiorgan dysfunction syndrome: A case report. Cases Journal 2008, 1:125. doi:10.1186/1757-1626-1-125, CC BY 2.0, https://commons.wikimedia.org/w/index.php?curid=5639655


References
- ↑ 1.0 1.1 Misiakos EP, Bagias G, Patapis P, Sotiropoulos D, Kanavidis P, Machairas A (2014). “Current concepts in the management of necrotizing fasciitis”. Front Surg. 1: 36. doi:10.3389/fsurg.2014.00036. PMC 4286984. PMID 25593960.
- ↑ Lynch CM, Pinelli DM, Cruse CW, Spellacy WN, Sinnott JT, Shashy RG (1997). “Maternal death from postpartum necrotizing fasciitis arising in an episiotomy: a case report”. Infect Dis Obstet Gynecol. 5 (5): 341–4. doi:10.1155/S1064744997000598. PMC 2364577. PMID 18476182.
- ↑ Morgan MS (2010). “Diagnosis and management of necrotising fasciitis: a multiparametric approach”. J Hosp Infect. 75 (4): 249–57. doi:10.1016/j.jhin.2010.01.028. PMID 20542593.
- ↑ Stamenkovic I, Lew PD (1984). “Early recognition of potentially fatal necrotizing fasciitis. The use of frozen-section biopsy”. N Engl J Med. 310 (26): 1689–93. doi:10.1056/NEJM198406283102601. PMID 6727947.
- ↑ Elliott DC, Kufera JA, Myers RA (1996). “Necrotizing soft tissue infections. Risk factors for mortality and strategies for management”. Ann Surg. 224 (5): 672–83. PMC 1235444. PMID 8916882.
- ↑ Leitch HA, Palepu A, Fernandes CM (2000). “Necrotizing fasciitis secondary to group A streptococcus. Morbidity and mortality still high”. Can Fam Physician. 46: 1460–6. PMC 2144855. PMID 10925760.
- ↑ Shiroff AM, Herlitz GN, Gracias VH (2014). “Necrotizing soft tissue infections”. J Intensive Care Med. 29 (3): 138–44. doi:10.1177/0885066612463680. PMID 23753218.
- ↑ McHenry CR, Piotrowski JJ, Petrinic D, Malangoni MA (1995). “Determinants of mortality for necrotizing soft-tissue infections”. Ann Surg. 221 (5): 558–63, discussion 563-5. PMC 1234638. PMID 7748037.
- ↑ Chelsom J, Halstensen A, Haga T, Høiby EA (1994). “Necrotising fasciitis due to group A streptococci in western Norway: incidence and clinical features”. Lancet. 344 (8930): 1111–5. PMID 7934492.
- ↑ Miller LG, Perdreau-Remington F, Rieg G, Mehdi S, Perlroth J, Bayer AS; et al. (2005). “Necrotizing fasciitis caused by community-associated methicillin-resistant Staphylococcus aureus in Los Angeles”. N Engl J Med. 352 (14): 1445–53. doi:10.1056/NEJMoa042683. PMID 15814880.
- ↑ 11.0 11.1 Librae pathology(2015) https://librepathology.org/wiki/Necrotizing_fasciitis Accessed on September 2,2016
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yamuna Kondapally, M.B.B.S[2]
Overview
The causative organisms vary depending on the type of necrotizing fasciitis: Type I (polymicrobial), Type II (monomicrobial), Type III (Gram negative monomicrobial, including marine related organisms) and Type IV (fungal).[1]
Causes
Necrotizing fasciitis may be caused by the following organisms:[2]
| Type | Organism |
|---|---|
| Type 1 (70%-80% cases) Polymicrobial/Synergistic[3][4][5] |
● Mixed aerobes, anaerobes and facultative anerobic bacteria ● Often bowel flora-derived ● Affects immunocomprmised or those with underlying abominal pathology |
| Type 2 (20% to 30% cases) Monomicrobial[6][7] |
● Beta-Hemolytic Streptococci group A (Streptococcus pyogenes) ● With/without Staphylococcus aureus ● Skin or throat derived |
| Type 3 (common in Asia) Gram negative monomicrobial (including marine related organisms)[8][9] |
● Vibrio spp mainly ● Raw oyster ingestion (Vibrio vulnificus) ● Wound contamination with sea water ● Non-vibrio spp (Pasteurella multocida, Haemophilus influenzae, Klebsiella spp. and Aeromonas spp) |
| Type 4 (Fungal)[1] | ● Candida (Immunocompromised patients) ● Zygomycetes such as Mucor and Rhizopus spp (Immunocompetent patients) |
References
- ↑ 1.0 1.1 Misiakos EP, Bagias G, Patapis P, Sotiropoulos D, Kanavidis P, Machairas A (2014). “Current concepts in the management of necrotizing fasciitis”. Front Surg. 1: 36. doi:10.3389/fsurg.2014.00036. PMC 4286984. PMID 25593960.
- ↑ Shimizu T, Tokuda Y (2010). “Necrotizing fasciitis”. Intern Med. 49 (12): 1051–7. PMID 20558917.
- ↑ Salcido RS (2007). “Necrotizing fasciitis: reviewing the causes and treatment strategies”. Adv Skin Wound Care. 20 (5): 288–93, quiz 294-5. doi:10.1097/01.ASW.0000269317.76380.3b. PMID 17473566.
- ↑ Anaya DA, McMahon K, Nathens AB, Sullivan SR, Foy H, Bulger E (2005). “Predictors of mortality and limb loss in necrotizing soft tissue infections”. Arch Surg. 140 (2): 151–7, discussion 158. doi:10.1001/archsurg.140.2.151. PMID 15723996.
- ↑ Miller LG, Perdreau-Remington F, Rieg G, Mehdi S, Perlroth J, Bayer AS; et al. (2005). “Necrotizing fasciitis caused by community-associated methicillin-resistant Staphylococcus aureus in Los Angeles”. N Engl J Med. 352 (14): 1445–53. doi:10.1056/NEJMoa042683. PMID 15814880.
- ↑ Shiroff AM, Herlitz GN, Gracias VH (2014). “Necrotizing soft tissue infections”. J Intensive Care Med. 29 (3): 138–44. doi:10.1177/0885066612463680. PMID 23753218.
- ↑ Umbert IJ, Winkelmann RK, Oliver GF, Peters MS (1989). “Necrotizing fasciitis: a clinical, microbiologic, and histopathologic study of 14 patients”. J Am Acad Dermatol. 20 (5 Pt 1): 774–81. PMID 2654217.
- ↑ Howard RJ, Pessa ME, Brennaman BH, Ramphal R (1985). “Necrotizing soft-tissue infections caused by marine vibrios”. Surgery. 98 (1): 126–30. PMID 4012603.
- ↑ Goodell KH, Jordan MR, Graham R, Cassidy C, Nasraway SA (2004). “Rapidly advancing necrotizing fasciitis caused by Photobacterium (Vibrio) damsela: a hyperaggressive variant”. Crit Care Med. 32 (1): 278–81. doi:10.1097/01.CCM.0000104920.01254.82. PMID 14707592.
Differentiating Necrotizing fasciitis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yamuna Kondapally, M.B.B.S[2]
Overview
Necrotizing fasciitis must be differentiated from other diseases that cause erythema, pain, edema and necrosis of soft tissues such as sunburn, cellulitis, erysipelas, diabetic myonecrosis and vasculitis.[1]
Differential Diagnosis
Necrotizing fasciitis must be differentiated from:[1] [2][3]
Early stage
- Muscle strains
- Viral illness
- Thrombosis
- Sprain or exacerbation of gout
- Sunburn or an allergic rash
Late stage
- Non-necrotizing fasciitis (eosinophilic fasciitis, paraneoplastic fasciitis, nodular fasciitis, and proliferative fasciitis)
- Cellulitis
- Dermatomyositis
- Erysipelas
- Vasculitis (Lupus myofasciitis, Churg-Strauss Vasculitis and others)
- Graft-versus-host disease (GVHD)
- Diabetic myonecrosis
- Compartment syndrome
- Lymphedema
- Phlegmasia cerulea dolens
- Myxedema
- Gastroenteritis
- Necrotizing pyoderma gangrenosum
References
- ↑ 1.0 1.1 Wong CH, Wang YS (2005). “The diagnosis of necrotizing fasciitis”. Curr Opin Infect Dis. 18 (2): 101–6. PMID 15735411.
- ↑ Schmid MR, Kossmann T, Duewell S (1998). “Differentiation of necrotizing fasciitis and cellulitis using MR imaging”. AJR Am J Roentgenol. 170 (3): 615–20. doi:10.2214/ajr.170.3.9490940. PMID 9490940.
- ↑ Ayestaray B, Dudrap E, Chartaux E, Verdier E, Joly P (2010). “Necrotizing pyoderma gangrenosum: an unusual differential diagnosis of necrotizing fasciitis”. J Plast Reconstr Aesthet Surg. 63 (8): e655–8. doi:10.1016/j.bjps.2010.02.008. PMID 20202917.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yamuna Kondapally, M.B.B.S[2]
Overview
The incidence of necrotizing fasciitis in adults is 0.40 cases per 100,000 people/year and the incidence in children is higher at 0.08 cases per 100,000 people/year.The overall mortality rate in the United states from 2003- 2013 was 4.8/1,000,000 per year. Patients from all age groups can develop necrotizing fasciitis but slightly more common among >50 years age and effects men and women equally.The incidence rate of necrotizing fasciitis is high in black, Hispanic, and American Indian individuals compared to Whites and low in Asian individuals.
Epidemiology and Demographics
Incidence
- Since 2010, on average, there are between 700-1100 cases of necrotizing fasciitis caused by group A streptococcus annually in the United States.[1]
- The incidence of necrotizing fasciitis in adults is approximately 0.40 per 100,000 individuals. The incidence of necrotizing fasciitis in children is approximately 0.08 per 100,000 individuals.[2][3]
Mortality Rate
- Early intervention remains the only method of reducing mortality and morbidity in necrotizing fasciitis patients.
- The overall mortality rate of necrotizing fasciitis related deaths in the United States from 2003-2013 was 4.8/1,000,000 per year.[4]
- The mortality rate in necrotizing fasciitis is approximately between 24-34%.[5][6]
- The mortality rate of necrotizing fasciitis increases from 9% to 63% if associated with mysositis and streptococcal toxic shock syndrome.
| Types | Mortality |
|---|---|
| Type 1 | Variable, depends on underlying comorbidities |
| Type 2 | >32% depends on associated myositis or toxic shock |
| Type 3 | 30- 40% |
| Type 4 | >47% (higher if immunocompromised) |
Age
Patients of all age groups may develop necrotizing fasciitis, however, it is slightly more common among patients >50 years age.[7]
Gender
Necrotizing fasciitis effects men and women equally.[8]
Race
- The incidence rate of necrotizing fasciitis is higher in Black, Hispanic, and American Indian individuals compared to Whites.[4]
- The incidence rate is low in Asian populations.
Developing Countries
Necrotizing fasciitis is more common in developing countries because of low socioeconomic status and poor standards of hygiene.[8]
References
- ↑ Centers for Disease Control and Prevention (2016)http://www.cdc.gov/features/necrotizingfasciitis/ Accessed on september 6, 2016
- ↑ File TM, Tan JS, DiPersio JR (1998). “Group A streptococcal necrotizing fasciitis. Diagnosing and treating the “flesh-eating bacteria syndrome““. Cleve Clin J Med. 65 (5): 241–9. PMID 9599907.
- ↑ Chaouat Y, Chaouat D (1988). “[Primary hyperparathyroidism. History]”. Rev Rhum Mal Osteoartic. 55 (7): 475–8. PMID 3051309.
- ↑ 4.0 4.1 Arif N, Yousfi S, Vinnard C (2016). “Deaths from necrotizing fasciitis in the United States, 2003-2013”. Epidemiol Infect. 144 (6): 1338–44. doi:10.1017/S0950268815002745. PMID 26548496.
- ↑ Ryter A, Hirota Y, Jacob F (1968). “DNA-membrane complex and nuclear segregation in bacteria”. Cold Spring Harb Symp Quant Biol. 33: 669–76. PMID 4977757.
- ↑ McHenry CR, Piotrowski JJ, Petrinic D, Malangoni MA (1995). “Determinants of mortality for necrotizing soft-tissue infections”. Ann Surg. 221 (5): 558–63, discussion 563-5. PMC 1234638. PMID 7748037.
- ↑ Machado, Norman Oneil. “Necrotizing fasciitis: The importance of early diagnosis, prompt surgical debridement and adjuvant therapy.” North Am J Med Sci 3 (2011): 107-118.
- ↑ 8.0 8.1 Sadasivan J, Maroju NK, Balasubramaniam A (2013). “Necrotizing fasciitis”. Indian J Plast Surg. 46 (3): 472–8. doi:10.4103/0970-0358.121978. PMC 3897089. PMID 24459334.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yamuna Kondapally, M.B.B.S[2]
Overview
Common risk factors in the development of necrotizing fasciitis include trauma, alcoholism, diabetes, intravenous drug abuse, immunosupression and burns.[1]
Risk Factors
Common risk factors in the development of necrotizing fasciitis include:[1][2][3][4][5][6]
| Type 1 | Type 2 | Type 3 | Type 4 |
|---|---|---|---|
| • Alcoholism • Antecedent trauma • Carcinoma • Cardiopulmonay disease • Diabetes • Iatrogenic procedures • Immunosupression (e.g., HIV and corticosteroid use) • Intravenous drug abuse • Male gender • Peripheral vascular disease • Recent surgery • Smoking • Advanced age |
• Alcoholism • Antecedent trauma • Carcinoma • Cardiopulmonay disease • Diabetes • Immunosupression (e.g., HIV and corticosteroid use) • Intravenous drug abuse • Male gender • Peripheral vascular disease • Recent surgery • Exposure to children with sore throat • HLA class II haplotype • Lack of specific anti-GAS antibodies • Varicella infection • Advanced age |
• Raw oyster ingestion • Wound contamination with sea water • Immunosupression • Advanced age |
• Immunosupression • Antecedent trauma • Burns • Advanced age |
Role of NSAIDS in GASNF
- NSAIDS mask the signs and symptoms leading to delay in diagnosis of existing infection.[1][7][8]
- NSAIDS potentiate the development of renal failure by inhibiting renal prostaglandin synthesis and prevent the respiratory burst necessary for phagocytes to kill intracellular organisms leading to impairment of natural host defense mechanisms.
References
- ↑ 1.0 1.1 1.2 Misiakos EP, Bagias G, Patapis P, Sotiropoulos D, Kanavidis P, Machairas A (2014). “Current concepts in the management of necrotizing fasciitis”. Front Surg. 1: 36. doi:10.3389/fsurg.2014.00036. PMC 4286984. PMID 25593960.
- ↑ Chen JL, Fullerton KE, Flynn NM (2001). “Necrotizing fasciitis associated with injection drug use”. Clin Infect Dis. 33 (1): 6–15. doi:10.1086/320874. PMID 11389488.
- ↑ Elliott DC, Kufera JA, Myers RA (1996). “Necrotizing soft tissue infections. Risk factors for mortality and strategies for management”. Ann Surg. 224 (5): 672–83. PMC 1235444. PMID 8916882.
- ↑ McHenry CR, Piotrowski JJ, Petrinic D, Malangoni MA (1995). “Determinants of mortality for necrotizing soft-tissue infections”. Ann Surg. 221 (5): 558–63, discussion 563-5. PMC 1234638. PMID 7748037.
- ↑ Francis KR, Lamaute HR, Davis JM, Pizzi WF (1993). “Implications of risk factors in necrotizing fasciitis”. Am Surg. 59 (5): 304–8. PMID 8489099.
- ↑ Goh T, Goh LG, Ang CH, Wong CH (2014). “Early diagnosis of necrotizing fasciitis”. Br J Surg. 101 (1): e119–25. doi:10.1002/bjs.9371. PMID 24338771.
- ↑ Holder EP, Moore PT, Browne BA (1997). “Nonsteroidal anti-inflammatory drugs and necrotising fasciitis. An update”. Drug Saf. 17 (6): 369–73. PMID 9429836.
- ↑ NSAIDS and NF http://www.medsafe.govt.nz/Profs/puarticles/necf.htm (2000) Accessed on September 11, 2016
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: ; Yamuna Kondapally, M.B.B.S[2]
Overview
According to the U.S. Preventive Service Task Force (USPSTF), there is insufficient evidence to recommend routine screening for necrotizing fasciitis.
Screening
According to the U.S. Preventive Service Task Force (USPSTF), there is insufficient evidence to recommend routine screening for necrotizing fasciitis.
References
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Yamuna Kondapally, M.B.B.S[2]
Overview
If left untreated, the acute inflammatory changes spread quickly, accompanied by high fever and extreme weakness leading to necrosis of soft tissue. Common complications of necrotizing fasciitis include limb loss, sepsis, toxic shock syndrome, disseminated intravascular coagulation (DIC). Depending on the extent of the necrotizing fasciitis at the time of diagnosis, the prognosis may vary. The prognostic factors associated with necrotizing fasciitis include diabetes mellitus, acute renal failure, admission serum creatinine >2mg/dl and admission white blood cells >30,000 cells mm3.
Natural History
- If left untreated, the acute inflammatory changes spread quickly, accompanied by high fever,extreme weakness and may progress to death.[1]
- The overlying skin becomes smooth, tense and shiny. Diffuse erythema without distinct borders is seen.
- First 1 or 2 days, the lesions develop with progressive color changes from red to purple to blue and then becomes frankly gangrenous, first turning black, then greenish-yellow.
- If the patient has survived, a line of demarcation between viable and necrotic tissue would become sharply defined from days 7 to 10.
- Sloughing of necrotic skin would reveal the underlying pus and extensive liquefactive necrosis of subcutaneous tissues, which will be significantly more extensive than would be suspected with the overlying area of necrotic skin.
- Metastatic abscesses and pulmonary distress may develop as well.
Complications
Common complications of necrotizing fasciitis include:[2]
- Limb loss
- Sepsis
- Kidney failure
- Compartment syndrome
- Extensive scarring and disfigurement
- Toxic shock syndrome
- Rapid advancement of disease resulting in death
- Disseminated intravascular coagulation
Type 2 NF and Streptococcal Toxic Shock Syndrome
- Most of Type 2 NF cases are associated with streptococcal toxic shock syndrome which increases the mortality of streptococcal NF alone from <40% to 67% with up to half of patients needing amputation.
- The superantigens cause massive activation of T-cell, cytokine release, tissue damage, and toxic shock-like syndrome
Prognosis
Depending on the extent of the necrotizing fasciitis at the time of diagnosis, the prognosis may vary.[3]
- The prognostic factors associated with necrotizing fasciitis include:
- Timing to operative intervention (most important prognositic factor)
- Age older than 60 years
- Female gender
- Number of comorbidities
- Acute renal failure
- Underlying malignancy
- Coagulopathy or acidosis on admission
- Clostridial or group A streptococcal infection
- Vibrio vulnificus infection
- Admission white blood cells >30,000 cells/mm3
- Diabetes mellitus
- Shock on admission
- Admission serum creatinine >2mg/dl
- Associated streptococcal toxic shock syndrome
- Over expression of cytokines in host
- Immunodeficiency
- High APACHE (Acute physiology, Age, and chronic health evaluation) II scores (>13)
- Use of NSAIDs
| Types | Prognosis |
|---|---|
| Type 1 | Better prognosis, more indolent, easier to recognize clinically |
| Type 2 | Aggressive, easily missed, very variable |
| Type 3 | Seafood ingestion or wound contamination with seawater |
| Type 4 | Aggressive with rapid extension especially if immunocompromised |
References
- ↑ Morgan MS (2010). “Diagnosis and management of necrotising fasciitis: a multiparametric approach”. J Hosp Infect. 75 (4): 249–57. doi:10.1016/j.jhin.2010.01.028. PMID 20542593.
- ↑ Necrotizing soft tissue infection https://medlineplus.gov/ency/article/001443.htm (2016) Accessed on september 6, 2016
- ↑ Khamnuan P, Chongruksut W, Jearwattanakanok K, Patumanond J, Yodluangfun S, Tantraworasin A (2015). “Necrotizing fasciitis: risk factors of mortality”. Risk Manag Healthc Policy. 8: 1–7. doi:10.2147/RMHP.S77691. PMC 4337692. PMID 25733938.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | X Ray | CT | MRI | Ultrasound | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Future or Investigational Therapies
See also
See also
- Mucormycosis, a rare fungal infection which can present like necrotizing fasciitis
- Toxic shock syndrome
Template:Diseases of the musculoskeletal system and connective tissue
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH