
Primary amoebic meningoencephalitis
For patient information, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Synonyms and keywords: PAM; PAME; Naegleria fowleri infection; N. fowleri infection; primary amebic meningoencephalitis
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Primary amoebic meningoencephalitis is a disease of the central nervous system caused by infection from Naegleria fowleri.[1] Naegleria fowleri is a free-living ameboflagellate that invades the brain and meninges via the nasal mucosa and olfactory nerve to cause acute, fulminant hemorrhagic meningoencephalitis (primary amebic meningoencephalitis – PAM), primarily in healthy children and young adults with a recent history of exposure to warm fresh water. Initial signs and symptoms of PAM begin 1 to 14 days after infection and include sudden onset of headache, fever, nausea, vomiting, and stiff neck accompanied by positive Kernig’s sign and Brudzinski’s sign. In some cases, abnormalities in taste or smell, nasal obstruction and nasal discharge might be seen. Other symptoms might include photophobia, mental-state abnormalities, lethargy, dizziness, loss of balance, other visual disturbances, hallucinations, delirium, seizures, and coma. After the onset of symptoms, the disease progresses rapidly and usually results in death within 3 to 7 days. Although a variety of treatments have been shown to be active against amoebae in vitro and have been used to treat infected persons, most infections have still been fatal.
Historical Perspective
Primary amoebic meningoencephalitis was first documented in Australia in 1965.[2][3] In 1966, four cases were reported in the USA.
Pathophysiology
Naegleria fowleri is a heat-loving (thermophilic), free-living ameba (single-celled microbe), commonly found around the world in warm fresh water (like lakes, rivers, and hot springs) and soil that causes acute, fulminant hemorrhagic meningoencephalitis (primary amebic meningoencephalitis – PAM). Naegleria fowleri is the only species of Naegleria known to infect people. Most of the time, Naegleria fowleri lives in freshwater habitats by feeding on bacteria. However, in rare instances, the ameba can infect humans by entering the nose during water-related activities. Once in the nose, the ameba travels to the brain and causes a severe brain infection, primary amoebic meningoencephalitis (PAM), which is usually fatal.
Causes
Naegleria fowleri is the causative agent for primary amoebic meningoencephalitis, which is normally found in the natural environment and is well adapted to surviving in various habitats, particularly warm-water environments.
Differentiating Primary Amoebic Meningoencephalitis from other Diseases
Primary amoebic meningoencephalitis resembles acute bacterial meningitis and needs to be differentiated from that.
Epidemiology and Demographics
Primary amoebic meningoencephalitis is both exceptionally rare and highly lethal. In the 10 years from 2002 to 2011, 32 infections were reported in the U.S. Of those cases, 28 people were infected by contaminated recreational water, two people were infected by water from a contaminated, geothermal (naturally hot), untreated drinking water supply, and two people were infected after performing nasal irrigation using contaminated tap water.
Risk Factors
Swimming behaviors associated with the increased risk of primary amoebic meningoencephalitis include diving or jumping into the water, submerging the head under water, or engaging in other water-related activities that cause water to go up the nose.
Diagnosis
History and Symptoms
Patients with primary amoebic meningoencephalitis may have a history of swimming, diving, jumping, bathing, or playing in warm, generally stagnant, fresh water or irrigating sinuses (nose) using contaminated tap water during the previous few days to 2 weeks. Symptoms start 1-7 days (median 5 days) after swimming exposure and usually include high fever, headache, nuchal rigidity, photophobia, nausea, and vomiting.
Physical Examination
Initial signs of primary amoebic meningoencephalitis begin 1 to 14 days after infection and include nuchal rigidity, positive Kernig’s sign and Brudzinski’s sign, cerebellar ataxia, palsies of the third, fourth and sixth cranial nerves, and increased intracranial pressure.
Laboratory Findings
Primary amoebic meningoencephalitis is diagnosed using specific laboratory tests available in only a few laboratories in the United States. Because of the rarity of the infection and difficulty in initial detection, about 75% of diagnoses are made after the death of the patient. It can be diagnosed in the laboratory by detecting Naegleria fowleri organisms, nucleic acid, or antigen in cerebrospinal fluid (CSF), biopsy, or tissue specimens.
Treatment
Medical Therapy
Considering the the high mortality rate of primary amoebic meningoencephalitis, unusually non-suggestive symptomology of the early-stage disease, and necessity of microbial culture of the cerebrospinal fluid to effect a positive diagnosis, it has been suggested that physicians should give an array of antimicrobial drugs, including the drugs used to treat amoebic encephalitis, before the disease is actually confirmed in order to increase the number of survivors. However, administering several of those drugs at once (or even some of them known to treat the condition) is often very dangerous and unpleasant for the patient.
Primary Prevention
Personal actions to reduce the risk of primary amoebic meningoencephalitis should focus on limiting the amount of water going up the nose and lowering the chances that Naegleria fowleri may be in the water. Routine, enhanced education of the public in advance of the summer swim season might be helpful.
Future or Investigational Therapies
Recently, an investigational drug, miltefosine,[4] a breast cancer and anti-leishmania drug, has shown some promise against the free-living amoebae in combination with some other drugs. Miltefosine has shown in vitro and mouse model amebicidal activity against Balamuthia, Naegleria fowleri, and Acanthamoeba.
References
- ↑ Cabanes PA, Wallet F, Pringuez E, Pernin P (2001). “Assessing the risk of primary amoebic meningoencephalitis from swimming in the presence of environmental Naegleria fowleri”. Appl. Environ. Microbiol. 67 (7): 2927–31. doi:10.1128/AEM.67.7.2927-2931.2001. PMC 92963. PMID 11425704. Unknown parameter
|month=ignored (help) - ↑ Fowler M, Carter RF (1965). “Acute pyogenic meningitis probably due to Acanthamoeba sp.: a preliminary report”. Br Med J. 2 (5464): 740–2. PMC 1846173. PMID 5825411. Unknown parameter
|month=ignored (help) - ↑ Symmers WC (1969). “Primary amoebic meningoencephalitis in Britain”. Br Med J. 4 (5681): 449–54. doi:10.1136/bmj.4.5681.449. PMC 1630535. PMID 5354833. Unknown parameter
|month=ignored (help) - ↑ Kaminsky R (2002). “Miltefosine Zentaris”. Curr Opin Investig Drugs. 3 (4): 550–4. PMID 12090722.
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Primary amoebic meningoencephalitis was first documented in Australia in 1965.[1][2] In the United States, there have been 128 PAM infections from 1962 through 2012 with only one survivor. These infections have primarily occurred in 15 southern-tier states, with more than half of all infections occurring in Texas and Florida.
Historical Perspective
- Primary amoebic meningoencephalitis was first documented in Australia in 1965.[1][2] In 1966, four cases were reported in the USA. By 1968 the causative organism, previously thought to be a species of Acanthamoeba or Hartmanella, was identified as Naegleria. This same year, occurrence of 16 cases over period of two years (1963–1965) was reported in Ústí nad Labem.[3] In 1970, the species of amoeba was named N. fowleri.[4]
- In 2010, a 7-year-old girl in Stillwater, Minnesota died of the disease.[5]
- In August 2010, 7-year-old Kyle Lewis died after contracting the protist from swimming in Lake Granbury and warm water near Glen Rose, Texas. Texas authorities say this is the tenth case since 2000.[6]
- In August 2011, a 16-year-old girl in Mims, Florida died after swimming in the St. John’s River a week earlier. Doctors found N. fowleri in her cerebral spinal fluid.[7]
- As of December 2011, two individuals in Louisiana died after inhaling infected tap water while using a neti pot.[8][9]
- In July 2012, an 8 year old boy from Sumter, SC died after swimming in Lake Marion (South Carolina).[10]
- In southern part of Pakistan, 8 people died within a week of July 2012.[11]
- In August 2012, Jack Ariola Erenberg, a 9 year old boy from Stillwater, Minnesota, died after swimming in Lily Lake near his home.[12]
- In August 2012, Waylon Abel, 30, of Loogootee IN died after swimming in West Boggs Lake near his home.[13]
References
- ↑ 1.0 1.1 Fowler M, Carter RF (1965). “Acute pyogenic meningitis probably due to Acanthamoeba sp.: a preliminary report”. Br Med J. 2 (5464): 740–2. PMC 1846173. PMID 5825411. Unknown parameter
|month=ignored (help) - ↑ 2.0 2.1 Symmers WC (1969). “Primary amoebic meningoencephalitis in Britain”. Br Med J. 4 (5681): 449–54. doi:10.1136/bmj.4.5681.449. PMC 1630535. PMID 5354833. Unknown parameter
|month=ignored (help) - ↑ Červa L. (5 April 1968). “Ameobic meningoencephalitis: sixteen fatalities”. Science. 160 (3823): 92. doi:10.1126/science.160.3823.92. PMID 5642317. Unknown parameter
|coauthors=ignored (help); Check date values in:|year= / |date= mismatch(help) - ↑ Gutierrez, Yezid (15). “Chapter 6: Free Living Amebae”. Diagnostic Pathology of Parasitic Infections with Clinical Correlations (2 ed.). USA: Oxford University Press. pp. 114–115. ISBN 0-19-512143-0. Unknown parameter
|month=ignored (help); Check date values in:|date=, |year= / |date= mismatch(help) - ↑ “Stillwater girl dies of very rare form of meningitis”. Minneapolis Star Tribune. Retrieved 26 August 2010.
- ↑ “Tarrant County resident dies from amoeba infection”. Pegasus News. August 31, 2010. Retrieved 2011-08-17.
- ↑ “Florida teen, Courtney Nash, dies from rare brain parasite”. NY Daily News. Retrieved 15 August 2011.
- ↑ Stobbe, Mike. “Two die of rare brain infection from amoeba in water in neti pot”. Retrieved 19 December 2011.
- ↑ “Neti Pot Deaths Linked to Brain-Eating Amoeba in Tap Water”. Yahoo!. Associated Press. Retrieved 19 December 2011.
- ↑ “Sumter boy dies of rare brain infection”. The State. Text “accessdate 19 July 2012” ignored (help)
- ↑ “8 dies in Karachi due to Naegleria”. Retrieved 2012-7-19. Check date values in:
|accessdate=(help) - ↑ http://www.dailymail.co.uk/news/article-2186295/Jack-Ariola-9-killed-contracting-brain-eating-amoeba-Lily-Lake-Minnesota.html
- ↑ http://washtimesherald.com/local/x620788801/Beach-closed-Autopsy-confirms-rare-parasite
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hardik Patel, M.D.
Overview
Naegleria fowleri is a heat-loving (thermophilic), free-living ameba (single-celled microbe), commonly found around the world in warm fresh water (like lakes, rivers, and hot springs) and soil that causes acute, fulminant hemorrhagic meningoencephalitis (primary amebic meningoencephalitis – PAM). Naegleria fowleri is the only species of Naegleria known to infect people. Most of the time, Naegleria fowleri lives in freshwater habitats by feeding on bacteria. However, in rare instances, the ameba can infect humans by entering the nose during water-related activities. Once in the nose, the ameba travels to the brain and causes a severe brain infection, primary amoebic meningoencephalitis (PAM), which is usually fatal.
Pathophysiology
Naegleria fowleri propagates in warm, stagnant bodies of freshwater (typically during the summer months), and enters the central nervous system after insufflation of infected water by attaching itself to the olfactory nerve.[1] It then migrates through the cribiform plate and into the olfactory bulbs of the forebrain,[2] where it multiplies itself greatly by feeding on nerve tissue. During this stage, occurring approximately 3–7 days post-infection, the typical symptoms are parosmia, rapidly progressing to anosmia (with resultant ageusia) as the nerve cells of the olfactory bulbs are consumed and replaced with necrotic lesions. After the organisms have multiplied and largely consumed the olfactory bulbs, the infection rapidly spreads through the mitral cell axons to the rest of the cerebrum, resulting in onset of symptoms.
Life Cycle

Naegleria fowleri has 3 stages in its life cycle: ameboid trophozoites, flagellates, and cysts. The only infective stage of the ameba is the ameboid trophozoite. Trophozoites are 10-35 µm long with a granular appearance and a single nucleus. The trophozoites replicate by binary division during which the nuclear membrane remains intact (a process called promitosis). Trophozoites infect humans or animals by penetrating the nasal tissue and migrating to the brain via the olfactory nerves causing primary amebic meningoencephalitis (PAM). Trophozoites can turn into a temporary, non-feeding, flagellated stage (10-16 µm in length) when stimulated by adverse environmental changes such as a reduced food source. They revert back to the trophozoite stage when favorable conditions return. Naegleria fowleri trophozoites are found in cerebrospinal fluid (CSF) and tissue, while flagellated forms are occasionally found in CSF. Cysts are not seen in brain tissue. If the environment is not conducive to continued feeding and growth (like cold temperatures, food becomes scarce) the ameba or flagellate will form a cyst. The cyst form is spherical and about 7-15 µm in diameter. It has a smooth, single-layered wall with a single nucleus. Cysts are environmentally resistant in order to increase the chances of survival until better environmental conditions occur.
 |
 |
 |
Copyleft images obtained courtesy of http://www.cdc.gov/parasites/naegleria/pathogen.html
Gross Pathology Images




Copyleft images obtained courtesy of http://www.cdc.gov/parasites/naegleria/naegleria-fowleri-images.html
Microscopic Pathology Images
-
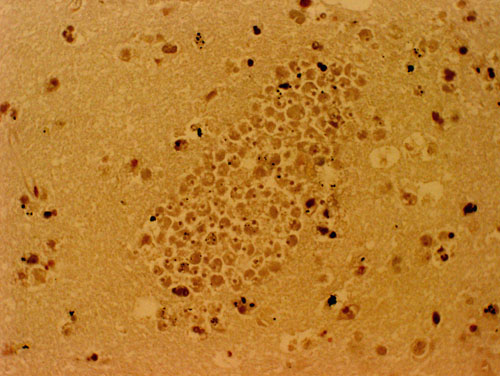 A section of the brain stained with hematoxylin and eosin, of a PAM patient showing a large cluster of Naegleria fowleri trophozoites. Cysts are not seen.
A section of the brain stained with hematoxylin and eosin, of a PAM patient showing a large cluster of Naegleria fowleri trophozoites. Cysts are not seen. -
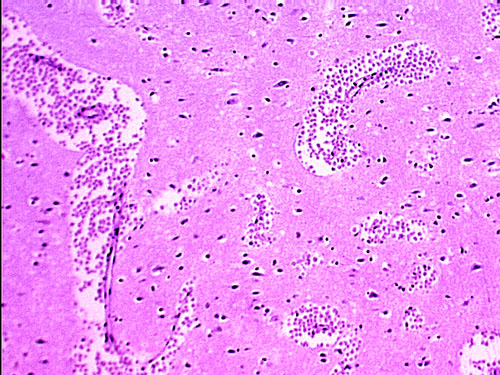 A section of the brain, stained with hematoxylin and eosin, of a PAM patient showing large clusters of Naegleria fowleri trophozoites. Cysts are not seen.
A section of the brain, stained with hematoxylin and eosin, of a PAM patient showing large clusters of Naegleria fowleri trophozoites. Cysts are not seen.


Copyleft images obtained courtesy of http://www.cdc.gov/parasites/naegleria/naegleria-fowleri-images.html
References
- ↑ Centers for Disease Control and Prevention (CDC) (2008). “Primary amebic meningoencephalitis—Arizona, Florida, and Texas, 2007”. MMWR Morb. Mortal. Wkly. Rep. 57 (21): 573–7. PMID 18509301. Unknown parameter
|month=ignored (help) - ↑ Cervantes-Sandoval I, Serrano-Luna Jde J, García-Latorre E, Tsutsumi V, Shibayama M (2008). “Characterization of brain inflammation during primary amoebic meningoencephalitis”. Parasitol. Int. 57 (3): 307–13. doi:10.1016/j.parint.2008.01.006. PMID 18374627. Unknown parameter
|month=ignored (help)
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Naegleria fowleri (also known as the brain eating amoeba) is a ubiquitous, free living amoeba typically grows contaminated, warm (25–35 °C / 77–95 °F), fresh water (e.g. lakes or hot springs). It belongs to a group called the Percolozoa or Heterolobosea. N. fowleri is transmitted to the humans through the nose when individuals swim/dive in lakes. Drinking contaminated water, however, does not result in transmission. N. fowleri causes primary amebic meningoencephalitis (PAM), a rare disease whereby N. fowleri invades the human central nervous system through the cibriform plate and causes fulminant fatal meningoencephalitis in the majority of cases.[1][2]
Taxonomy
- Phylum = Percolozoa
- Class = Heterolobosea
- Order = Schizopyrenida
- Family = Vahlkampfiidae
- Genus = Naegleria
- Species = N. fowleri
- Binomial = Naegleria fowleri
Biology
Shown below is an the life cycle of N. fowleri:

- N. fowleri grows ideally at 42 °C (108 °F), but it can tolerate temperatures as high as 45 °C (113 °F).[3]
- There are 3 morphological stages in the life cycle of Naegleria fowleri:[3]
- Trophozoite: 10-30 mu – Infective stage characterized by the presence of contractile vacuoles. It reproduces by binary fission. It uses pseudopods structure to ingest other organisms, red blood cells, and white blood cells.
- Flagellate: A temporary stage when the organism is exposed to changes in pH (e.g. from culture to distilled water).
- Cyst: 7-14 μm – A resistant stage whereby the organism is protected by a dense cell wall that can tolerate harsh environments, such as cold weather or states of low nutrition. Cysts may be transmitted to the human host and transformed into trophozoites.
Structure
- N. fowleri is a facultatively aerobic, heterotrophic organism.[4]
- In its trophozoite form, it may appear either ameboid or flagellated.
- It contains the following structures for survival and growth:
- Mitochondria
- Pseudopods
- Flagella
- Contractile vacuoles
Tropism
- N. fowleri invades the central nervous system (highly oxygenated environment) and causes meningoencephalitis.[3]
- N. fowleri is transmitted to humans via the nasal cavity into the cribriform plate.
- It invades the subarachnoid spaces by migrating along the mesaxonal of unmyelinated olfactory nerves.
- When it reaches the subarachnoid space, it may then disseminate to other tissues of the central nervous system.
- It migrates along the mesaxonal spaces of unmyelinated
Natural Reservoir
- The natural reservoir of N. fowleri are typically fresh water lakes and hot springs.
- N. fowleri has also been isolated from:[4]
- Soil
- Swimming pools
- Home showers
- Sewers
- Cooling towers
References
- ↑ “The Centers for Disease Control and Prevention, Division of Parasitic Diseases – Naegleria Infection Fact Sheet”. Retrieved 2007-10-09.
- ↑ “6 Die From Brain-Eating Amoeba in Lakes”. Retrieved 2007-10-03.
- ↑ 3.0 3.1 3.2 John DT (1982). “Primary amebic meningoencephalitis and the biology of Naegleria fowleri”. Annu Rev Microbiol. 36: 101–23. doi:10.1146/annurev.mi.36.100182.000533. PMID 6756287.
- ↑ 4.0 4.1 Park JS, Simpson AG, Lee WJ, Cho BC (2007). “Ultrastructure and phylogenetic placement within Heterolobosea of the previously unclassified, extremely halophilic heterotrophic flagellate Pleurostomum flabellatum (Ruinen 1938)”. Protist. 158 (3): 397–413. doi:10.1016/j.protis.2007.03.004. PMID 17576098.
External links
- Naegleria Infection fact sheet from the website of the Centers for Disease Control and Prevention
Differentiating Primary Amoebic Meningoencephalitis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Primary amebic meningoencephalitis must be differentiated from other causes of headache, fever, and confusion., such as bacterial/viral/fungal meningoencephalitis, other protozoal diseases, brain tumors, and vasculitides.
Differential Diagnosis
Primary amebic meningoencephalitis must be differentiated from other causes of headache, fever, and confusion. The following is a list of the differential diagnosis of primary amebic meningoencephalitis:
- Bacterial meningitis or encephalitis
- Viral meningitis or encephalitis
- Angiostrongylus spp. infection
- Baylisascaris spp. infection
- Brain abscess
- Brain tumors
- Cat scratch disease
- Coccidioidomycosis
- Cryptococcosis
- Echinococcosis
- Gnathostomiasis
- Histoplasmosis
- Intracranial or ventricular/periventricular hemorrhage
- Malaria
- Mucormycosis
- Neurocysticercosis
- Rabies
- Sappinia spp. infection
- Toxoplasmosis
- Tuberculosis
- Vasculitis and mixed connective tissue disease
References
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hardik Patel, M.D.
Overview
Primary amoebic meningoencephalitis is both exceptionally rare and highly lethal. In the 10 years from 2002 to 2011, 32 infections were reported in the U.S. Of those cases, 28 people were infected by contaminated recreational water, two people were infected by water from a contaminated, geothermal (naturally hot), untreated drinking water supply, and two people were infected after performing nasal irrigation using contaminated tap water.
Epidemiology and Demographics
Primary amoebic meningoencephalitis is both exceptionally rare and highly lethal. There had been fewer than 200 confirmed cases recorded in medical history as of 2004,[1] 300 cases as of 2008,[2] with an in-hospital case fatality rate of ~97% (3% patient survival rate).[3]
Age
Primary amoebic meningoencephalitis have occurred in all age groups, but 107 cases have occurred in children under 18 years of age (median age of 12 years; range 8 months to 66 years) out of 123 infections documented in the U.S. from 1962 through 2011.
Gender
Over three-quarters (>75%) of infections have been in males.

Number of case-reports of primary amebic meningoencephalitis by age group and gender: United States, 1962-2011.
Copyleft image obtained courtesy of http://www.cdc.gov/parasites/naegleria/graphs.html#gender
Developed Countries
Although most cases of primary amebic meningoencephalitis (PAM) caused by Naegleria fowleri infection in the United States have been fatal (122/123 in the U.S.,[4]), there have been two well-documented survivors in North America: one in California[5] and one in Mexico.[6] It has been suggested that the survivor’s strain of Naegleria fowleri was less virulent, which contributed to the patient’s recovery. In laboratory experiments, the California PAM survivor’s strain did not cause damage to cells as rapidly, suggesting that it was less virulent than strains recovered from other fatal infections.[7] Multiple other patients have received treatments similar to the California PAM survivor, including amphotericin B, miconazole/fluconazole/ketoconazole, and/or rifampin. They did not survive, making it difficult to determine the efficacy of the treatment regimen. Infections are more likely to occur in southern-tier states, but can also occur in other locations. Over half of all reported infections have occurred in Florida and Texas.

Number of case-reports of primary amebic meningoencephalitis by state of exposure: United States, 1962-2011.
Copyleft image obtained courtesy of http://www.cdc.gov/parasites/naegleria/state-map.html
Season
While infections with Naegleria fowleri are very rare, they occur mainly during the summer months of July, August, and September. Infections usually occur when it is hot for prolonged periods of time, which results in higher water temperatures and lower water levels. Infections can increase during heat wave years as water temperatures increase.

Number of case-reports of primary amebic meningoencephalitis by month of illness onset and probable water exposure: United States, 1962-2011.
Copyleft image obtained courtesy of http://www.cdc.gov/parasites/naegleria/graphs.html#exposure
References
- ↑ Wiwanitkit V (2004). “Review of clinical presentations in Thai patients with primary amoebic meningoencephalitis”. MedGenMed. 6 (1): 2. PMC 1140726. PMID 15208515.
- ↑ Caruzo G, Cardozo J (2008). “Primary amoebic meningoencephalitis: a new case from Venezuela”. Trop Doct. 38 (4): 256–7. doi:10.1258/td.2008.070426. PMID 18820207. Unknown parameter
|month=ignored (help) - ↑ “Amebic Meningoencephalitis”. Retrieved 16 July 2010.
- ↑ Yoder JS, Eddy BA, Visvesvara GS, Capewell L, Beach MJ (2010). “The epidemiology of primary amoebic meningoencephalitis in the USA, 1962-2008”. Epidemiol Infect. 138 (7): 968–75. doi:10.1017/S0950268809991014. PMID 19845995.
- ↑ Seidel JS, Harmatz P, Visvesvara GS, Cohen A, Edwards J, Turner J (1982). “Successful treatment of primary amebic meningoencephalitis”. N Engl J Med. 306 (6): 346–8. doi:10.1056/NEJM198202113060607. PMID 7054710.
- ↑ Vargas-Zepeda J, Gómez-Alcalá AV, Vásquez-Morales JA, Licea-Amaya L, De Jonckheere JF, Lares-Villa F (2005). “Successful treatment of Naegleria fowleri meningoencephalitis by using intravenous amphotericin B, fluconazole and rifampicin”. Arch Med Res. 36 (1): 83–6. PMID 15900627.
- ↑ John DT, John RA (1989). “Cytopathogenicity of Naegleria fowleri in mammalian cell cultures”. Parasitol Res. 76 (1): 20–5. PMID 2622894.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Swimming behaviors associated with the increased risk of primary amoebic meningoencephalitis include diving or jumping into the water, submerging the head under water, or engaging in other water-related activities that cause water to go up the nose.
Risk Factors
- Diving or jumping into the warm, usually stagnant, fresh water during periods of high water temperature and low water levels.
- Submerging the head under water during religious practices.
- Putting head under the water in hot springs and other untreated thermal waters.
- Digging in, or stirring up, the sediment while taking part in water-related activities in shallow, warm freshwater areas.
- Irrigating sinuses (nose) using contaminated tap water.
References
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Natural History
Naegleria fowleri enters the nose and then migrates to the brain through the cribiform plate along the olfactory nerve. People do not become infected from drinking contaminated water. After the organisms have multiplied and largely consumed the olfactory bulbs, the infection rapidly spreads through the mitral cell axons to the rest of the cerebrum, resulting in onset of frank encephalitic symptoms, including cephalgia (headache), nausea, and rigidity of the neck muscles, progressing to vomiting, delirium, seizures, and eventually irreversible coma. Symptoms start 1-7 days (median 5 days) after swimming exposure and people die 1-12 days (median 5.3 days) after symptoms begin.
Complications
Complications may vary among the rare survivors of these infections and depend on the extent of CNS involvement. Respiratory failure occurs when the infection spreads to the brain stem, destroying the autonomic nerve cells of the medulla oblongata.
Prognosis
The disease is both exceptionally rare and highly lethal. The high mortality rate of this disease is largely blamed on the unusually non-suggestive symptomology of the early-stage disease compounded by the necessity of microbial culture of the cerebrospinal fluid to effect a positive diagnosis. The parasite also demonstrates a particularly rapid late-stage propagation through the nerves of the olfactory system to many parts of the brain simultaneously (including the vulnerable medulla). For those reasons, it has been suggested that physicians should give an array of antimicrobial drugs, including the drugs used to treat amoebic encephalitis, before the disease is actually confirmed in order to increase the number of survivors. However, administering several of those drugs at once (or even some of them known to treat the condition) is often very dangerous and unpleasant for the patient and people usually die 1-12 days after symptoms begin.
References
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Related Chapters
Related Chapters
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH