
Sprained ankle
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Javaria Anwer M.D.[2]
Synonyms and keywords: Ankle sprain; ankle injury; ankle ligament injury
Overview
Overview
A sprained ankle is a common medical condition where one or more of the ligaments of the ankle is/are stretched, partially or completely torn. Ankle sprains are more common among physically active individuals. The anterior talofibular ligament is one of the most commonly involved ligaments. Sprains to the lateral aspect of the ankle account for 85% of ankle sprains. Females are more commonly affected with an ankle sprain than males. The diagnosis of most ankle sprains is made in the light of history of acute ankle trauma and examination findings.
Classification
Classification
| Grading for functional loss of Ankle sprain | ||
| Grade | Degree of ligament damage | Symptoms and signs |
| Grade I | Mild stretching |
|
| Grade II | Incomplete tear |
|
| Grade III | Complete tear |
|
Pathophysiology
Pathophysiology
- The pathogenesis of ankle sprain is characterized by ankle movement beyond the elastic limits of its supporting structures causing acute ankle pathology.
- Lateral ankle sprain injury is usually caused by forefoot adduction, hindfoot inversion, and tibial external rotation with ankle in plantar flexion. Depending on the amount and direction of the force, one or more of the lateral ligaments can be involved.[2]
- The ATFL is the most commonly injured structure with the lowest load to failure when compared to the other lateral ligaments. The anterior tallofibular ligament (ATFL) is the most commonly injured ligament and is most susceptible to injury during ankle plantarflexion with the ankle‘s bony anatomy providing less stability. In this position, ATFL acts as a collateral ligament to the ankle. The ATFL prevents talar internal rotation, anterior translation and is a restraint to plantarflexion. The most common mechanism of injury to the ATFL is inversion injury where a plantarflexed ankle undergoes supination and adduction.[3]
- An ankle sprain can involve any of the following injuries:[4]
- Anterior (and/or posterior) talofibular ligament injury
- Calcaneofibular ligament injury
- Possible peroneal and flexor tendon injuries
- Syndesmotic injury
- On microscopic histopathological analysis, microscopic failure of the collagen fibers characterize ankle sprain when the load and velocity applied to outweigh the mechanical strength of the ligament and speed of a corrective muscle reflex.[5]
Causes
Causes
A lateral ankle sprain occurs when the ankle is inverted beyond the elastic limits of its supporting structures causing acute ankle pathology.
Differentiating ankle sprain from other Diseases
- Ankle sprain should be differentiated from (click on the disease name to read more):[6]
- Tendon pathologies: Tendon rupture, ITiFi ligament tear.
- Joint pathologies: Joint effusion, and chronic osteoarthritis.
- Fractures: of the low fibula, Diaphyseal fibula, medial malleolus, postmedial talar process, anterior calcaneal process, os peronei, fifth metatarsal,
- Microfractures: of the cuboid, calcaneum, and tibia.
- Stress fracture
- Subluxation
- Impingement syndrome, sinus tarsi syndrome, tarsal tunnel syndrome, Talar neck avulsion, peroneal groove pathology, peroneal tenosynovitis.
- Muscle pathologies: Split peroneus brevis, peroneus longus, tibialis anterior tear, tibialis posterior dislocation, and flexor digitorum brevis tear.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
In human anatomy, the ankle joint is formed where the foot and the leg meet. The ankle, or talocrural joint, is a synovial hinge joint that connects the distal ends of the tibia and fibula in the lower limb with the proximal end of the talus bone in the foot.[1] The articulation between the tibia and the talus bears more weight than between the smaller fibula and the talus.
The term “ankle” is used to describe structures in the region of the ankle joint proper.[2]
Movement
The ankle joint is responsible for dorsiflexion (moving the toes up as when standing only on the heels) and plantar flexion of the foot (moving the toes down, as when standing on the toes), and allows for the greatest movement of all the joints in the foot. The ankle does not allow rotation.
In plantar flexion, the anterior ligaments of the joint become longer while the posterior ligaments become shorter. The reverse is true for dorsiflexion.
Articulation
The lateral malleolus of the fibula and the medial malleolus of the tibia along with the inferior surface of the distal tibia articulate with three facets of the talus. These surfaces are covered by cartilage.
The anterior talus is wider than the posterior talus. When the foot is dorsiflexed , the wider part of the superior talus moves into the articulating surfaces of the tibia and fibula, creating a more stable joint than when the foot is plantar flexed.
Ligaments
The ankle joint is bound by the strong deltoid ligament and three lateral ligaments: the anterior talofibular ligament, the posterior talofibular ligament, and the calcaneofibular ligament.
- The deltoid ligament supports the medial side of the joint, and is attached at the medial malleolus of the tibia and connect in four places to the sustentaculum tali of the calcaneus, calcaneonavicular ligament, the navicular tuberosity, and to the medial surface of the talus.
- The anterior and posterior talofibular ligaments support the lateral side of the joint from the lateral malleolus of the fibula to the dorsal and ventral ends of the talus.
- The calcaneofibular ligament is attached at the lateral malleolus and to the lateral surface of the calcaneus.
The joint is most stable in dorsiflexion and a sprained ankle is more likely to occur when the foot is plantar flexed. This type of injury more frequently occurs at the anterior talofibular ligament.
Name derivation
The word ankle or ancle is common, in various forms, to Germanic languages, probably connected in origin with the Latin “angulus”, or Greek “αγκυλος”, meaning bent.
Related terms
A common variant of the word “ankle” is “cankle“, which is commonly used derogatorily to describe the ankles of obese individuals where the ankle and calf may be indistinguishable. This insult can be taken further (often jokingly) using the term “thankle”, which implies a person’s thighs and ankles are indistinguishable.
Fractures

Most traumatic incidents involving the ankle result in ankle sprains. Symptoms of an ankle fracture can be similar than for sprains (pain, hematoma) or there may be an abnormal position, abnormal movement or lack of movement (if there is an accompanying dislocation), or the patient may have heard a crack.
On clinical examination, it is important to evaluate the exact location of the pain, the range of motion and the condition of the nerves and vessels. It is important to palpate the calf bone (fibula) because there may be an associated fracture, and to palpate the sole of the foot to look for a Jones fracture.
Evaluation of ankle injuries for fracture is done with the Ottawa ankle rules, a set of rules that were developed to minimize unnecessary X-rays. On X-rays, there can be a fracture of the medial malleolus, the lateral malleolus, or the anterior or posterior margin. If both malleoli are broken, this is called a bimalleolar fracture (some of them are called Pott’s fractures). If three of these are broken at the same time, this is called a trimalleolar fracture (although there are only two malleoli). Ankle fractures are classified according to Weber, depending on their position relative to the anterior ligament of the lateral malleolus (type A = below the ligament, type B = at its level, type C = above the ligament). A special form of type C fracture is the Maisonneuve fracture, which involves a spiral fracture of the fibula with a tear of the distal tibiofibular syndesmosis and the interosseous membrane.
Only type A fractures of the lateral malleolus can be treated like sprains; all other types require surgery (most often an open reduction and internal fixation). A cast may be required to immobilize the ankle following surgery. Trimalleolar fractures or those with dislocation have a high risk of developing arthrosis.
Additional images
-
The bones in the foot.
-
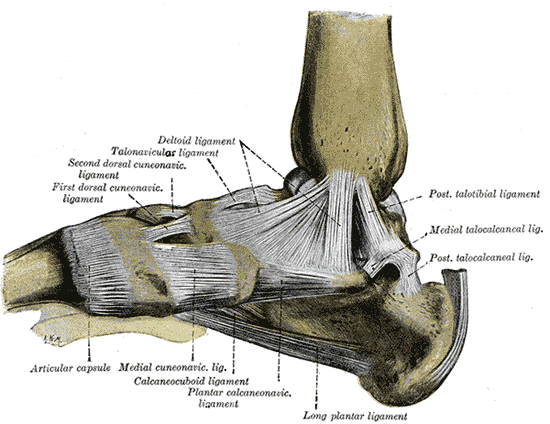 Ligaments of the medial aspect of the foot.
Ligaments of the medial aspect of the foot. -
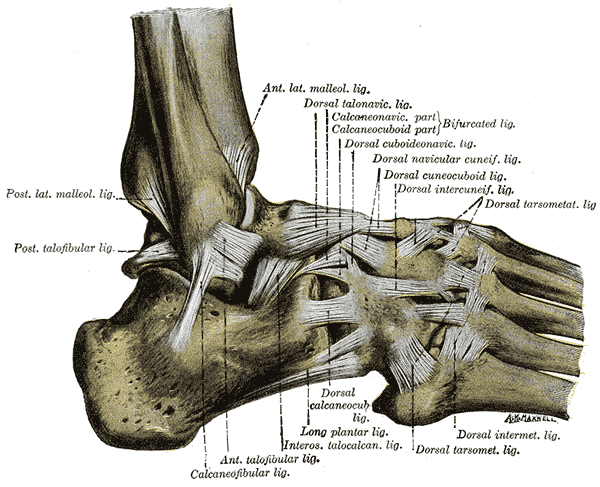 The ligaments of the foot from the lateral aspect.
The ligaments of the foot from the lateral aspect. -
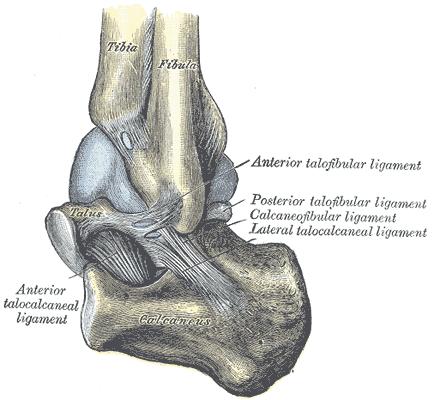 Capsule of left talocrura articulation (distended). Lateral aspect.
Capsule of left talocrura articulation (distended). Lateral aspect. -
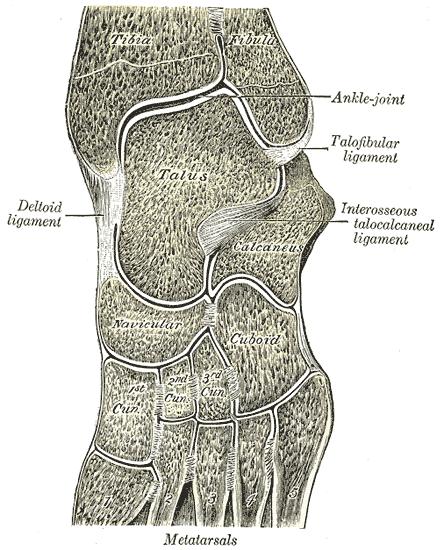 Oblique section of left intertarsal and tarsometatarsal articulations, showing the synovial cavities.
Oblique section of left intertarsal and tarsometatarsal articulations, showing the synovial cavities.




References
- ↑ “eMedicine/Stedman Medical Dictionary Lookup!”. Retrieved 2008-01-14.
- ↑ “eMedicine/Stedman Medical Dictionary Lookup!”. Retrieved 2008-01-14.
- Calais-Germain, Blandine. “Anatomy of Movement”, Eastland Press, 1993. ISBN 0-939616-17-3
- Martini, Frederic; Timmons, Michael; McKinnley, Michael. “Human Anatomy”, 3rd Edition, Prentice-Hall, 2000. ISBN 0-13-010011-0
- Marieb, Elaine. “Essentials of Human Anatomy and Physiology”, 6th Edition. Addison Wesley Longman, 2000. ISBN 0-8053-4940-5
See also
| File:Wiktionary-logo-en-v2.svg | Look up ankle in Wiktionary, the free dictionary. |
External links
| Wikimedia Commons has media related to Ankle. |
- The Ankle from the University of Glasgow
- How to Diagnose Lateral Ankle Injuries from Podiatry Today
- American Academy of Orthopedic Surgeons website about Foot & Ankle
Template:Joints of lower limbs Template:Human anatomical features
Epidemiology and Demographics
Epidemiology and Demographics
- The prevalence of ankle sprain is approximately [number or range] per 100,000 individuals worldwide. The most common injuries suffered from during athletic/recreational activities is lateral ankle sprains.[7][8][9]
- The indoor/court sports has a “cumulative incidence rate of 7 per 1,000 exposures or 1.37 per 1,000 athlete exposures and 4.9 per 1,000 h”.[10]
Age
- A systematic review and meta-analyses of prospective studies reported that children compared with adolescents and adults are more likely to sustain an ankle sprain.[10]
Gender
- A systematic review and meta-analyses of prospective studies reported that females are more commonly affected with ankle sprain than males.[10]
Race
- There is no racial predilection for ankle sprain.
Risk Factors
Risk Factors
Natural History, Complications and Prognosis
Natural History, Complications and Prognosis
- The majority of patients with ankle sprain may remain asymptomatic.
- Early clinical features include tenderness, swelling, and ecchymosis over the anterior talofibuar and calcaneofibular ligaments. Although the patient may be asymptomatic depending upon the extent of injury.
- If left untreated patients with ankle sprain may progress to develop balance problems due to proprioception deficits. [12].
- Common complications of ankle sprain include chronic pain, joint instability, arthritis.[13]
- Prognosis is generally good but acute ankle sprains have been reported to have a high recurrence rate and may also lead to chronic ankle instability.[14]
Diagnosis
Diagnosis
Diagnostic Criteria
- The diagnosis of most ankle sprains is made in the light of history of acute ankle trauma and examination findings. Diagnostic imaging is unnecessary although ultrasound may help assess the extent of tendon injury.[15][2]
Symptoms
- Acute injuries may not demonstrate any signs and symptoms. Ask the patient to describe injury mechanism. Most sprains involve ankle inversion with some plantar flexion and suggest lateral ligament injury. Another mechanism, such as dorsiflexion, eversion suggest some other ligament involvement.[1]
Physical Examination
- Patients with ankle sprain usually appear fine. But, the patient may be in distress depending upon the intensity of pain.
- Physical examination of a typical lateral ankle sprain may be remarkable for:
- Tenderness, swelling, and ecchymosis over anterior talofibuar and calcaneofibular ligaments. Swelling and bruising of the whole foot and toe may be demonstrated if no proper treatment has been applied and the patient has been ambulating.[1]
- The patient should be assessed for the degree of instability, site, pain intensity, and an evaluation of neurovascular status.[16]
Laboratory Findings
- There are no specific laboratory findings associated with ankle sprain.
Electrocardiogram
- There are no ECG findings associated with ankle sprain.
X-ray
- An x-ray may be helpful in the diagnosis of ankle sprain. The Ottawa criteria (100% sensitivity) helps indicate of the radiography is indicated. According to the criteria, in case of pain in the malleolar or midfoot region, or tenderness of the bone over the potential fracture region, or weight bearing inability for four steps right after the injury warrants radiography.[17][18]
- Lateral, anteroposterior, and mortise views of the ankle help visualize the lesion.
Ultrasound
- Ultrasound findings include thickening and hypoechogenicity of the affected ligament demonstrate a sprain.[4]
CT scan
- CT scan may be helpful in the diagnosis of ankle sprain. Findings on CT scan suggestive of sprain include thickening, thinning, irregularity, discontinuity, or an absent ligament. Sometimes bony avulsions can be visible.[4]
MRI
Treatment
Treatment
- Although treatment decisions must be made on an individual basis, functional support for most ankle sprains is the first step.[21] Brace, tape, elastic bandage, or soft cast are preferred over immobilization.[22] It gives the leg an exercise and yet keeps the damaged part from moving. Crutches and air-braces while conventionally used, are currently out of vogue.
- Immediately following the injury it is important the follow the PRICE protocol – Protection, Rest, Ice, Compression, and Elevation (also known as RICE: Rest, Ice, Compress, and Elevate).[23]
- Cold therapy for 12 to 20 minutes together with compression until the swelling settles or 48 hours, is found to be helpful.[24][25][23]
- Severe ankle sprains should be assessed by an orthopedic specialist, although physical therapy is extremely effective for most sprained ankles.
- The evidence of use of ultrasound, LASER, and manual therapy (such as anteroposterior glide of the talus, Mulligan’s mobilization with movement, chiropractic mortise adjustment technique) for reducing swelling and pain is at various levels.[26][27][28][21]
Medical Therapy
Surgery
- Surgical repair can be performed for patients with ruptured ankle ligaments. Operative treatment has been shown to have a better long-term outcome for residual pain, recurrent sprains and stability in a randomised clinical trial.[31]
Prevention
References
References
- ↑ 1.0 1.1 1.2 Tiemstra JD (June 2012). “Update on acute ankle sprains”. Am Fam Physician. 85 (12): 1170–6. PMID 22962897.
- ↑ 2.0 2.1 McGovern RP, Martin RL (2016). “Managing ankle ligament sprains and tears: current opinion”. Open Access J Sports Med. 7: 33–42. doi:10.2147/OAJSM.S72334. PMC 4780668. PMID 27042147.
- ↑ Hur ES, Bohl DD, Lee S (August 2020). “Lateral Ligament Instability: Review of Pathology and Diagnosis”. Curr Rev Musculoskelet Med. 13 (4): 494–500. doi:10.1007/s12178-020-09641-z. PMC 7340720 Check
|pmc=value (help). PMID 32495041 Check|pmid=value (help). - ↑ 4.0 4.1 4.2 “Lateral ankle sprain | Radiology Reference Article | Radiopaedia.org”.
- ↑ Dubin JC, Comeau D, McClelland RI, Dubin RA, Ferrel E (September 2011). “Lateral and syndesmotic ankle sprain injuries: a narrative literature review”. J Chiropr Med. 10 (3): 204–19. doi:10.1016/j.jcm.2011.02.001. PMC 3259913. PMID 22014912.
- ↑ Meyr, Andrew (2008). Pain management. Philadelphia, Pa: Elsevier Saunders. ISBN 1416063412.
- ↑ Fernandez WG, Yard EE, Comstock RD (July 2007). “Epidemiology of lower extremity injuries among U.S. high school athletes”. Acad Emerg Med. 14 (7): 641–5. doi:10.1197/j.aem.2007.03.1354. PMID 17513688.
- ↑ Hootman JM, Dick R, Agel J (2007). “Epidemiology of collegiate injuries for 15 sports: summary and recommendations for injury prevention initiatives”. J Athl Train. 42 (2): 311–9. PMC 1941297. PMID 17710181.
- ↑ Hubbard TJ, Wikstrom EA (July 2010). “Ankle sprain: pathophysiology, predisposing factors, and management strategies”. Open Access J Sports Med. 1: 115–22. doi:10.2147/oajsm.s9060. PMC 3781861. PMID 24198549.
- ↑ 10.0 10.1 10.2 Doherty C, Delahunt E, Caulfield B, Hertel J, Ryan J, Bleakley C (January 2014). “The incidence and prevalence of ankle sprain injury: a systematic review and meta-analysis of prospective epidemiological studies”. Sports Med. 44 (1): 123–40. doi:10.1007/s40279-013-0102-5. PMID 24105612.
- ↑ McKay GD, Goldie PA, Payne WR, Oakes BW (April 2001). “Ankle injuries in basketball: injury rate and risk factors”. Br J Sports Med. 35 (2): 103–8. doi:10.1136/bjsm.35.2.103. PMC 1724316. PMID 11273971.
- ↑ Akbari M, Karimi H, Farahini H, Faghihzadeh S (2006). “Balance problems after unilateral lateral ankle sprains”. J Rehabil Res Dev. 43 (7): 819–24. doi:10.1682/jrrd.2006.01.0001. PMID 17436168.
- ↑ Martin B (April 2008). “Ankle sprain complications: MRI evaluation”. Clin Podiatr Med Surg. 25 (2): 203–47, vi. doi:10.1016/j.cpm.2007.12.004. PMID 18346591.
- ↑ Herzog MM, Kerr ZY, Marshall SW, Wikstrom EA (June 2019). “Epidemiology of Ankle Sprains and Chronic Ankle Instability”. J Athl Train. 54 (6): 603–610. doi:10.4085/1062-6050-447-17. PMC 6602402 Check
|pmc=value (help). PMID 31135209. - ↑ 15.0 15.1 Vuurberg G, Hoorntje A, Wink LM, van der Doelen B, van den Bekerom MP, Dekker R, van Dijk CN, Krips R, Loogman M, Ridderikhof ML, Smithuis FF, Stufkens S, Verhagen E, de Bie RA, Kerkhoffs G (August 2018). “Diagnosis, treatment and prevention of ankle sprains: update of an evidence-based clinical guideline”. Br J Sports Med. 52 (15): 956. doi:10.1136/bjsports-2017-098106. PMID 29514819. Vancouver style error: initials (help)
- ↑ Meyr, Andrew (2008). Pain management. Philadelphia, Pa: Elsevier Saunders. ISBN 1416063412.
- ↑ Bachmann LM, Kolb E, Koller MT, Steurer J, ter Riet G (February 2003). “Accuracy of Ottawa ankle rules to exclude fractures of the ankle and mid-foot: systematic review”. BMJ. 326 (7386): 417. doi:10.1136/bmj.326.7386.417. PMC 149439. PMID 12595378.
- ↑ Dowling S, Spooner CH, Liang Y, Dryden DM, Friesen C, Klassen TP, Wright RB (April 2009). “Accuracy of Ottawa Ankle Rules to exclude fractures of the ankle and midfoot in children: a meta-analysis”. Acad Emerg Med. 16 (4): 277–87. doi:10.1111/j.1553-2712.2008.00333.x. PMID 19187397.
- ↑ Wolfe MW, Uhl TL, Mattacola CG, McCluskey LC (January 2001). “Management of ankle sprains”. Am Fam Physician. 63 (1): 93–104. PMID 11195774.
- ↑ Lazarus ML (July 1999). “Imaging of the foot and ankle in the injured athlete”. Med Sci Sports Exerc. 31 (7 Suppl): S412–20. doi:10.1097/00005768-199907001-00002. PMID 10416542.
- ↑ 21.0 21.1 Lin CW, Hiller CE, de Bie RA (March 2010). “Evidence-based treatment for ankle injuries: a clinical perspective”. J Man Manip Ther. 18 (1): 22–8. doi:10.1179/106698110X12595770849524. PMC 3103112. PMID 21655420.
- ↑ Kerkhoffs GM, Rowe BH, Assendelft WJ, Kelly K, Struijs PA, van Dijk CN (2002). “Immobilisation and functional treatment for acute lateral ankle ligament injuries in adults”. Cochrane Database Syst Rev (3): CD003762. doi:10.1002/14651858.CD003762. PMID 12137710.
- ↑ 23.0 23.1 van den Bekerom MP, Struijs PA, Blankevoort L, Welling L, van Dijk CN, Kerkhoffs GM (2012). “What is the evidence for rest, ice, compression, and elevation therapy in the treatment of ankle sprains in adults?”. J Athl Train. 47 (4): 435–43. doi:10.4085/1062-6050-47.4.14. PMC 3396304. PMID 22889660.
- ↑ Sloan JP, Hain R, Pownall R (March 1989). “Clinical benefits of early cold therapy in accident and emergency following ankle sprain”. Arch Emerg Med. 6 (1): 1–6. doi:10.1136/emj.6.1.1. PMC 1285549. PMID 2712981.
- ↑ Airaksinen O, Kolari PJ, Miettinen H (May 1990). “Elastic bandages and intermittent pneumatic compression for treatment of acute ankle sprains”. Arch Phys Med Rehabil. 71 (6): 380–3. PMID 2334279.
- ↑ Eisenhart AW, Gaeta TJ, Yens DP (September 2003). “Osteopathic manipulative treatment in the emergency department for patients with acute ankle injuries”. J Am Osteopath Assoc. 103 (9): 417–21. PMID 14527076.
- ↑ Green T, Refshauge K, Crosbie J, Adams R (April 2001). “A randomized controlled trial of a passive accessory joint mobilization on acute ankle inversion sprains”. Phys Ther. 81 (4): 984–94. PMID 11276181.
- ↑ Collins N, Teys P, Vicenzino B (May 2004). “The initial effects of a Mulligan’s mobilization with movement technique on dorsiflexion and pain in subacute ankle sprains”. Man Ther. 9 (2): 77–82. doi:10.1016/S1356-689X(03)00101-2. PMID 15040966.
- ↑ Massey T, Derry S, Moore RA, McQuay HJ (June 2010). “Topical NSAIDs for acute pain in adults”. Cochrane Database Syst Rev (6): CD007402. doi:10.1002/14651858.CD007402.pub2. PMC 4163964. PMID 20556778.
- ↑ Morán M (1991). “Double-blind comparison of diclofenac potassium, ibuprofen and placebo in the treatment of ankle sprains”. J Int Med Res. 19 (2): 121–30. doi:10.1177/030006059101900205. PMID 1864448.
- ↑ Pijnenburg AC, Bogaard K, Krips R, Marti RK, Bossuyt PM, van Dijk CN (May 2003). “Operative and functional treatment of rupture of the lateral ligament of the ankle. A randomised, prospective trial”. J Bone Joint Surg Br. 85 (4): 525–30. doi:10.1302/0301-620x.85b4.13928. PMID 12793557.
Template:Dislocations, sprains and strains Template:WH Template:WS
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH