
Left ventricular aneurysm
For patient information, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Left ventricular (LV) aneurysm forms when intraventricular tension stretches the injured heart muscle during each cardiac cycle. It is a complication of myocardial infarction (MI) and it is categorized into true and false aneurysms, based on the nature of it’s wall. It is usually asymptomatic but may present as chest pain and dyspnea, and it should be suspected in patients with sustained ST elevation after MI. The diagnosis is based on echocardiographic findings.
Historical perspective
The British vascular surgeons, John and William Hunter, first described the aneurysm in 1880. In 1967, Gorlin and colleagues reported that aneurysms can be strongly suspected in up to 75% of patients with myocardial infarction.[1]
Classification
Based on the nature of the wall and its components, left ventricular aneurysms are classified as true or false aneurysms.[2]
True Left Ventricular Aneurysm
A true left ventricular aneurysm has an aneurysmal sac which contains the endocardium, epicardium, and thinned fibrous tissue (scar) which is a remnant of the left ventricular muscle.
False Left Ventricular Aneurysm or Pseudoaneurysm
Unlike a true aneurysm which contains some myocardial elements in its wall, the walls of a false aneurysm are composed of organized hematoma and pericardium and lack any element of the original myocardial wall.
Pathophysiology
Aneurysms form when intraventricular tension stretches the noncontracting, infarcted heart muscle, producing the expansion of the thin layer of necrotic muscle and fibrous tissue, which bulge with each cardiac contraction. The wall of a mature aneurysm is a white fibrous scar which becomes more densely fibrotic with the passage of time. The outward bulge with each cardiac contraction compromises the left ventricular stroke volume. On histopathological analysis, hyalinized fibrous tissue is the predominant finding. It usually takes 1 month for fibrous tissue to form.[1][3]
Causes
Myocardial infarction is the most common cause of left ventricular (LV) aneurysm formation. Less common causes include HCM, trauma, idiopathic and congenital abnormalities.[4][5][2][6]
Differential diagnosis
True LV aneurysm must be differentiated from false aneurysms.[7] [8]
Epidemiology
It was estimated that LV aneurysm develops in 30%-35% of patients with Q wave MI, but this has decreased significantly due to improvements in the management of patients with acute MI.[9] Currently it is estimated that true left ventricular aneurysms develop in less than 5% of all patients with STEMI.[10] According to this report, the use of thrombolytic agents has decreased the incidence of LV aneurysm from 18.8% to 7.2%.[10]
Risk Factors
The most potent risk factor for the development of LV aneurysm is ST elevation MI. Other risk factors include:[10][2][11][12]
- Hypertrophic cardiomyopathy (HCM)
- Dilated cardiomyopathy (DCM)
- Advanced age
- Hypertension
- Use of corticosteroids
Screening
The clue to the diagnosis of LV aneurysm following MI is a persistent ST elevation without chest pain, and there is no recommendation to screen patients for LV aneurysm.
Natural History
If left untreated, it may lead to heart failure and persistent anginal pain. For false aneurysms, rupture and hemodynamic compromise are the usual outcomes if left untreated. Improvements in STEMI management, control of hypertension and avoidance of corticosteroids in STEMI have led to a better prognosis and decreased mortality.[12]
Complications
Mural thrombosis, heart failure, persistent angina, and arrhythmia, are the major complications.
Symptoms
The symptoms of left ventricular aneurysm depends on the size of the aneurysm. Small and medium sized aneurysms are usually asymptomatic but large sized aneurysms may present as persistent chest pain and dyspnea despite the proper treatment of the underlying cardiac condition.
Physical exam
Physical findings on cardiac examination in patients with LV aneurysm include diffuse and displaced apical impulse, S3 and/or S4 heart sounds and mitral regurgitation murmur.
Electrocardiography
A persistent ST elevation is suggestive of LV aneurysm.[12]
Chest X ray
A bulge of the silhouette of the left ventricle on chest x-ray is the characteristic finding for LV aneurysm. [12]
CT scan
Chest CT scan with or without contrast may reveal the size and the location of LV aneurysm, it can also show the presence of calcifications in it.
MRI
Cardiac MRI is helpful for the diagnosis of LV aneurysm and it may be emerging as the preferred noninvasive technique for the preoperative assessment of LV shape, thinning, and resectability.[13]
Echocardiography
- Echocardiography is the modality of choice for the diagnosis of LV aneurysm. [14][15]
- It can measure the size and location of the aneurysm, and it is helpful for distinguishing true from false aneurysms based on the mouth size.
- Echocardiography is useful to diagnose dyskinesia or akinesia during systole.
- Echocardiography is helpful to diagnose mural thrombosis in aneurysm sac.
- Color flow echocardiography is helpful to establish the diagnosis based on in and out flow in the aneurysm.
Medical Therapy
Medical therapy is indicated for small and medium-sized LV aneurysms. Medical therapy is targeted at decreasing the cardiac work load (afterload reduction), anti ischemic therapy for chest pain and anti coagulation if mural thrombosis exist.[16]
- Afterload reduction:
- ACE inhibitors are the drug of choice for decreasing the afterload.
- Anti ischemic therapy:
- Many medications are used for treating underlying ischemic event and decreasing ischemic burden. The medications include:[16]
- Nitrates | Beta Blockers | Calcium Channel Blockers | Potassium Channel Openers | Newer Anti-anginal Agents
Surgery
- Surgical aneurysmectomy is recommended for large symptomatic aneurysms that cause angina pectoris or heart failure. Appropriate CABG is indicated at the time of aneurysmectomy.[17]
- Another indication for surgical intervention is in patients who can not tolerate long term anticoagulation therapy.[18]
References
- ↑ 1.0 1.1 Gorlin R, Klein MD, Sullivan JM (1967). “Prospective correlative study of ventricular aneurysm. Mechanistic concept and clinical recognition”. Am. J. Med. 42 (4): 512–31. PMID 6024720.
- ↑ 2.0 2.1 2.2 Maron MS, Finley JJ, Bos JM, Hauser TH, Manning WJ, Haas TS, Lesser JR, Udelson JE, Ackerman MJ, Maron BJ (2008). “Prevalence, clinical significance, and natural history of left ventricular apical aneurysms in hypertrophic cardiomyopathy”. Circulation. 118 (15): 1541–9. doi:10.1161/CIRCULATIONAHA.108.781401. PMID 18809796.
- ↑ Dubnow MH, Burchell HB, Titus JL (1965). “Postinfarction ventricular aneurysm. A clinicomorphologic and electrocardiographic study of 80 cases”. Am. Heart J. 70 (6): 753–60. PMID 5842520.
- ↑ Mann, Douglas (2015). Braunwald’s heart disease : a textbook of cardiovascular medicine. Philadelphia, PA: Elsevier/Saunders. ISBN 978-1455751341.
- ↑ Ichida M, Nishimura Y, Kario K (2014). “Clinical significance of left ventricular apical aneurysms in hypertrophic cardiomyopathy patients: the role of diagnostic electrocardiography”. J Cardiol. 64 (4): 265–72. doi:10.1016/j.jjcc.2014.02.011. PMID 24674752.
- ↑ Xia S, Wu B, Zhang X, Hu X (2009). “Left ventricular aneurysm in patients with idiopathic dilated cardiomyopathy: clinical analysis of six cases”. Neth Heart J. 17 (12): 475–80. PMC 2804080. PMID 20087451.
- ↑ Cho MN, Mehta SK, Matulevicius S, Weinstein D, Wait MA, McGuire DK (2006). “Differentiating true versus pseudo left ventricular aneurysm: a case report and review of diagnostic strategies”. Cardiol Rev. 14 (6): e27–30. doi:10.1097/01.crd.0000233756.66532.45. PMID 17053370.
- ↑ Makkuni P, Kotler MN, Figueredo VM (2010). “Diverticular and aneurysmal structures of the left ventricle in adults: report of a case within the context of a literature review”. Tex Heart Inst J. 37 (6): 699–705. PMC 3014120. PMID 21224951.
- ↑ Mills NL, Everson CT, Hockmuth DR (1993). “Technical advances in the treatment of left ventricular aneurysm”. Ann. Thorac. Surg. 55 (3): 792–800. PMID 8452458.
- ↑ 10.0 10.1 10.2 Napodano M, Tarantini G, Ramondo A, Cacciavillani L, Corbetti F, Marra MP, Fraccaro C, Peluso D, Razzolini R, Iliceto S (2009). “Myocardial abnormalities underlying persistent ST-segment elevation after anterior myocardial infarction”. J Cardiovasc Med (Hagerstown). 10 (1): 44–50. doi:10.2459/JCM.0b013e32831967b2. PMID 19145116.
- ↑ Bulkley BH, Roberts WC (1974). “Steroid therapy during acute myocardial infarction. A cause of delayed healing and of ventricular aneurysm”. Am. J. Med. 56 (2): 244–50. PMID 4812079.
- ↑ 12.0 12.1 12.2 12.3 Mourdjinis A, Olsen E, Raphael MJ, Mounsey JP (1968). “Clinical diagnosis and prognosis of ventricular aneurysm”. Br Heart J. 30 (4): 497–513. PMC 487659. PMID 5659397.
- ↑ Hüther J, Doenst T, Nitzsche S, Thiele H, Mohr FW, Gutberlet M (2011). “Cardiac magnetic resonance imaging for the assessment of ventricular function, geometry, and viability before and after surgical ventricular reconstruction”. J. Thorac. Cardiovasc. Surg. 142 (6): 1515–22.e1. doi:10.1016/j.jtcvs.2011.04.040. PMID 21907357.
- ↑ Arvan S, Varat MA (1984). “Persistent ST-segment elevation and left ventricular wall abnormalities: a 2-dimensional echocardiographic study”. Am. J. Cardiol. 53 (11): 1542–6. PMID 6731299.
- ↑ Matsumoto M, Watanabe F, Goto A, Hamano Y, Yasui K, Minamino T, Abe H, Kamada T (1985). “Left ventricular aneurysm and the prediction of left ventricular enlargement studied by two-dimensional echocardiography: quantitative assessment of aneurysm size in relation to clinical course”. Circulation. 72 (2): 280–6. PMID 3159507.
- ↑ 16.0 16.1 Mann, Douglas (2015). Braunwald’s heart disease : a textbook of cardiovascular medicine. Philadelphia, PA: Elsevier/Saunders. ISBN 978-1455751341.
- ↑ Kouchoukos, Nicholas (2013). Kirklin/Barratt-Boyes cardiac surgery : morphology, diagnostic criteria, natural history, techniques, results, and indications. Philadelphia: Elsevier/Saunders. ISBN 978-1416063919.
- ↑ Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA, Hand M, Hochman JS, Krumholz HM, Kushner FG, Lamas GA, Mullany CJ, Ornato JP, Pearle DL, Sloan MA, Smith SC, Alpert JS, Anderson JL, Faxon DP, Fuster V, Gibbons RJ, Gregoratos G, Halperin JL, Hiratzka LF, Hunt SA, Jacobs AK (2004). “ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction–executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1999 Guidelines for the Management of Patients With Acute Myocardial Infarction)”. Circulation. 110 (5): 588–636. doi:10.1161/01.CIR.0000134791.68010.FA. PMID 15289388.
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Aneurysm was first described by John Hunter in 1880.
Historical perspective
- British vascular surgeons, John and William Hunter, first described an aneurysm in 1880.
- In 1967, Gorlin and colleagues reported that a strong suspicion of aneurysm could be obtained in 75% of patients with myocardial infarction.[1]
References
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
The main classification method is based on the components of the wall of the aneurysm, and it classifies LV aneurysms into true and false (pseudo) aneurysms.
Classification
Components
Based on the nature of the wall of the aneurysm and its components, left ventricular aneurysms are classified as true or false aneurysms.[1]
| True Aneurysm | |||||||||||||||||||||||||||||||||||||||||||||||||||
| LV Aneurysm | |||||||||||||||||||||||||||||||||||||||||||||||||||
| Pseudo Aneurysm | |||||||||||||||||||||||||||||||||||||||||||||||||||
True Left Ventricular Aneurysm
A true left ventricular aneurysm has an aneurysmal sac which contains the endocardium, epicardium, and thinned fibrous tissue (scar) that is a remnant of the left ventricular muscle.
False Left Ventricular Aneurysm or Pseudoaneurysm
Unlike a true aneurysm, which contains some myocardial elements in its wall, the walls of a false aneurysm are composed of organized hematoma and pericardium and lack any element of the original myocardial wall.
Location
Left ventricular aneurysm may also be classified by location as anterolateral (apical) or posterior.[1]
References
- ↑ 1.0 1.1 Maron MS, Finley JJ, Bos JM, Hauser TH, Manning WJ, Haas TS, Lesser JR, Udelson JE, Ackerman MJ, Maron BJ (2008). “Prevalence, clinical significance, and natural history of left ventricular apical aneurysms in hypertrophic cardiomyopathy”. Circulation. 118 (15): 1541–9. doi:10.1161/CIRCULATIONAHA.108.781401. PMID 18809796.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Aneurysms form when the intraventricular tension stretches the non contracting, infarcted heart muscle, resulting in an expansion of the thin layer of necrotic muscle and fibrous tissue, which bulges with each cardiac contraction. The wall of a mature aneurysm is a white fibrous scar. It becomes more densely fibrotic as the time passes, and bulges outward with each cardiac contraction, resulting in a reduction of the left ventricular stroke volume. On microscopy, hyalinized fibrous tissue is the predominant finding. It usually takes 1 month for fibrous tissue to form.
Pathophysiology
Microscopic findings
- Hyalinized fibrous tissue is the predominant finding.
- However, a small number of viable muscle cells are also usually present.[1]
- It usually takes 1 month for fibrous tissue to form.
Gross Pathology
- The wall of a mature aneurysm is a white fibrous scar.
- The aneurysmal portion of the LV wall is thin. A mural thrombosis (which can be calcified), may be seen attached to the endocardial surface.[3]
- The endocardium beneath retains its trabeculations; the area of scarring is not clearly demarcated from the rest of the wall.
- The wall of the aneurysm becomes more densely fibrotic as the time passes, it bulges outward with each cardiac contraction and compromises the left ventricular stroke volume.
Images
The gross pathologic features of LV aneurysm are shown below.[4]
-
 Left ventricular aneurysm
Left ventricular aneurysm -
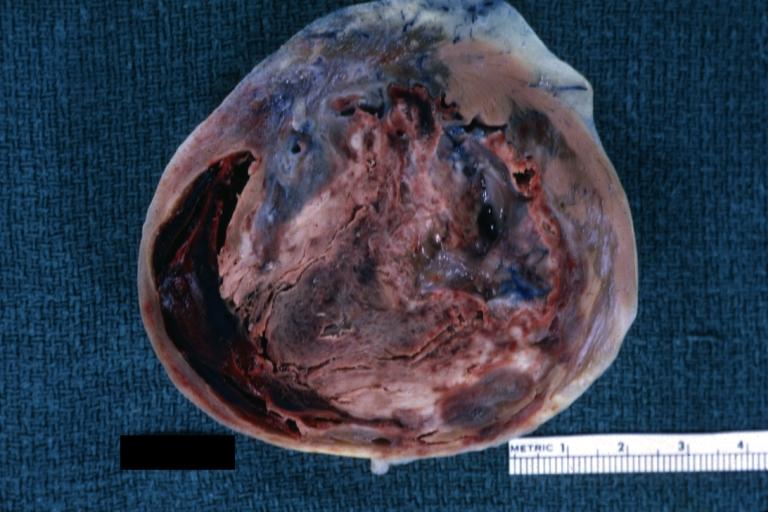 Left Ventricular Aneurysm; Gross pathology: The horizontal section shows the apex of the left ventricle with aneurysmal dilation and mural thrombus. A large scar tissue can be seen in the myocardium.
Left Ventricular Aneurysm; Gross pathology: The horizontal section shows the apex of the left ventricle with aneurysmal dilation and mural thrombus. A large scar tissue can be seen in the myocardium. -
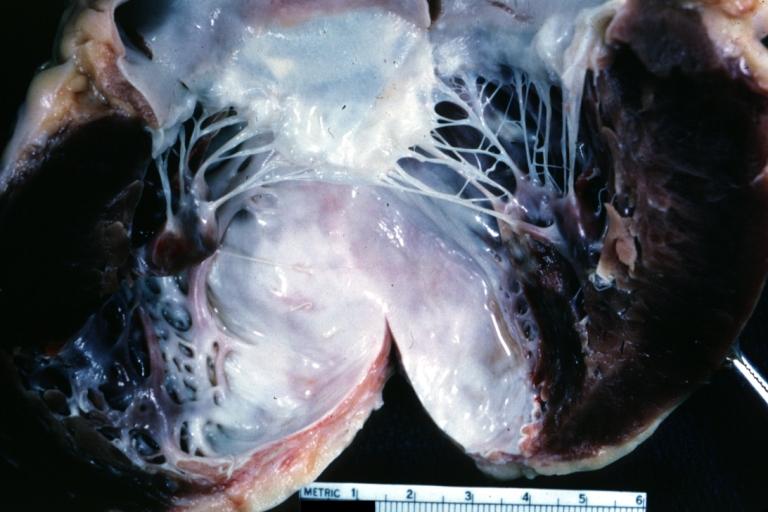 Left ventricular aneurysm.
Left ventricular aneurysm. -
 Heart; old myocardial infarction with aneurysm formation
Heart; old myocardial infarction with aneurysm formation




References
- ↑ Gorlin R, Klein MD, Sullivan JM (1967). “Prospective correlative study of ventricular aneurysm. Mechanistic concept and clinical recognition”. Am. J. Med. 42 (4): 512–31. PMID 6024720.
- ↑ PHARES WS, EDWARDS JE, BURCHELL HB (1953). “Cardiac aneurysms; clinicopathologic studies”. Proc Staff Meet Mayo Clin. 28 (9): 264–71. PMID 13056012.
- ↑ Dubnow MH, Burchell HB, Titus JL (1965). “Postinfarction ventricular aneurysm. A clinicomorphologic and electrocardiographic study of 80 cases”. Am. Heart J. 70 (6): 753–60. PMID 5842520.
- ↑ Images courtesy of Professor Peter Anderson DVM PhD and published with permission. © PEIR, University of Alabama at Birmingham, Department of Pathology
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Myocardial infarction is the most common cause of left ventricular (LV) aneurysm formation. Less common causes include HCM, trauma, idiopathic and congenital abnormalities.
Causes
Common Causes
The most common cause of LV aneurysm is myocardial infarction. It accounts for approximately 90% of apical aneurysms.[1] Other less common causes include:[2][3][4][5][6][7]
- Hypertrophic cardiomyopathy (HCM)
- Dilated cardiomyopathy (DCM)
- Trauma
- Idiopathic
- Congenital
- Iatrogenic
- Sarcoidosis
- Chagas disease
- Endocarditis
Causes by Organ System
| Cardiovascular | Dilated cardiomyopathy, Hypertrophic cardiomyopathy, Myocardial infarction, Endocarditis |
| Chemical/Poisoning | No underlying causes |
| Dental | No underlying causes |
| Dermatologic | No underlying causes |
| Drug Side Effect | No underlying causes |
| Ear Nose Throat | No underlying causes |
| Endocrine | No underlying causes |
| Environmental | No underlying causes |
| Gastroenterologic | No underlying causes |
| Genetic | Congenital |
| Hematologic | No underlying causes |
| Iatrogenic | Iatrogenic |
| Infectious Disease | Chagas disease |
| Musculoskeletal/Orthopedic | No underlying causes |
| Neurologic | No underlying causes |
| Nutritional/Metabolic | No underlying causes |
| Obstetric/Gynecologic | No underlying causes |
| Oncologic | No underlying causes |
| Ophthalmologic | No underlying causes |
| Overdose/Toxicity | No underlying causes |
| Psychiatric | No underlying causes |
| Pulmonary | No underlying causes |
| Renal/Electrolyte | No underlying causes |
| Rheumatology/Immunology/Allergy | Sarcoidosis |
| Sexual | No underlying causes |
| Trauma | Trauma |
| Urologic | No underlying causes |
| Miscellaneous | Idiopathic |
Causes in Alphabetical Order
References
- ↑ Mann, Douglas (2015). Braunwald’s heart disease : a textbook of cardiovascular medicine. Philadelphia, PA: Elsevier/Saunders. ISBN 978-1455751341.
- ↑ Ichida M, Nishimura Y, Kario K (2014). “Clinical significance of left ventricular apical aneurysms in hypertrophic cardiomyopathy patients: the role of diagnostic electrocardiography”. J Cardiol. 64 (4): 265–72. doi:10.1016/j.jjcc.2014.02.011. PMID 24674752.
- ↑ Maron MS, Finley JJ, Bos JM, Hauser TH, Manning WJ, Haas TS, Lesser JR, Udelson JE, Ackerman MJ, Maron BJ (2008). “Prevalence, clinical significance, and natural history of left ventricular apical aneurysms in hypertrophic cardiomyopathy”. Circulation. 118 (15): 1541–9. doi:10.1161/CIRCULATIONAHA.108.781401. PMID 18809796.
- ↑ Xia S, Wu B, Zhang X, Hu X (2009). “Left ventricular aneurysm in patients with idiopathic dilated cardiomyopathy: clinical analysis of six cases”. Neth Heart J. 17 (12): 475–80. PMC 2804080. PMID 20087451.
- ↑ Jmeian A, Thawabi M, Goldfarb I, Shamoon F (2015). “Left ventricular aneurysm and ventricular tachycardia as initial presentation of cardiac sarcoidosis”. N Am J Med Sci. 7 (3): 114–8. doi:10.4103/1947-2714.153923. PMC 4382765. PMID 25839003.
- ↑ Mori M, Sakakura K, Wada H, Ikeda N, Jinnouchi H, Sugawara Y, Kubo N, Momomura S, Ako J (2013). “Left ventricular apical aneurysm following primary percutaneous coronary intervention”. Heart Vessels. 28 (6): 677–83. doi:10.1007/s00380-012-0301-2. PMID 23089891.
- ↑ Kim GB, Kim WH, Min BJ, Lee YO, Park EA, Bae EJ (2011). “Aneurysm of left ventricular apex in a patient with pulmonary atresia, intact ventricular septum”. J. Am. Coll. Cardiol. 57 (13): e201. doi:10.1016/j.jacc.2010.07.064. PMID 21435511.
Differentiating Left ventricular aneurysm from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
True left ventricular (LV) aneurysm must be differentiated from pseudo aneurysm and LV diverticulum.
Differential diagnosis
True LV aneurysm must be differentiated from false aneurysms.[1] [2]
| True LV aneurysm | False LV aneurysm |
|---|---|
| Mostly apical (anterolateral) | Mostly inferoposterior |
| Wide mouth | Narrow mouth |
| Wall composed of LV myocardial remnants and fibrous tissue | Wall made up of parietal pericardium |
| Almost never ruptures | Often ruptures |
| May contain thrombus | Almost always contain thrombus |
Left ventricular diverticulum is another differential diagnosis of LV aneurysm.[3][4]
- It is defined as an outpouching structure that contains endocardium, myocardium, and pericardium.
- It displays normal contraction and is considered to be congenital.
References
- ↑ Cho MN, Mehta SK, Matulevicius S, Weinstein D, Wait MA, McGuire DK (2006). “Differentiating true versus pseudo left ventricular aneurysm: a case report and review of diagnostic strategies”. Cardiol Rev. 14 (6): e27–30. doi:10.1097/01.crd.0000233756.66532.45. PMID 17053370.
- ↑ Makkuni P, Kotler MN, Figueredo VM (2010). “Diverticular and aneurysmal structures of the left ventricle in adults: report of a case within the context of a literature review”. Tex Heart Inst J. 37 (6): 699–705. PMC 3014120. PMID 21224951.
- ↑ Pressoir R, Downing JW (1980). “Congenital diverticula of the right ventricle of the heart: a case report”. J Natl Med Assoc. 72 (3): 262–4. PMC 2552564. PMID 6771415.
- ↑ SKAPINKER S (1951). “Diverticulum of the left ventricle of the heart; review of the literature and report of a successful removal of the diverticulum”. AMA Arch Surg. 63 (5): 629–34. PMID 14868223.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
It is estimated that 5% of all patients with STEMI will develop LV aneurysm.
Epidemiology
It was estimated that LV aneurysm develops in 30%-35% of patients with Q wave MI, but there has been a significant decrease following improvements in the management of patients with acute MI.[1] Currently, it is estimated that true left ventricular aneurysms develop in less than 5% of all patients with STEMI.[2] The use of thrombolytic agents has decreased the incidence of LV aneurysm from 18.8% to 7.2%.[2]
Age
There is no data regarding the age predominance in LV aneurysm formation but it is assumed that elderly patients are more prone to develop it.
Race
There is no data regarding racial predominance in developing LV aneurysm.
References
- ↑ Mills NL, Everson CT, Hockmuth DR (1993). “Technical advances in the treatment of left ventricular aneurysm”. Ann. Thorac. Surg. 55 (3): 792–800. PMID 8452458.
- ↑ 2.0 2.1 Napodano M, Tarantini G, Ramondo A, Cacciavillani L, Corbetti F, Marra MP, Fraccaro C, Peluso D, Razzolini R, Iliceto S (2009). “Myocardial abnormalities underlying persistent ST-segment elevation after anterior myocardial infarction”. J Cardiovasc Med (Hagerstown). 10 (1): 44–50. doi:10.2459/JCM.0b013e32831967b2. PMID 19145116.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
The common risk factors for developing LV aneurysm include ST elevation MI, hypertrophic cardiomyopathy (HCM), dilated cardiomyopathy (DCM), advanced age, and hypertension.
Risk Factors
The most potent risk factor for the development of the LV aneurysm is ST elevation MI. Other risk factors include:[1][2][3][4]
- Hypertrophic cardiomyopathy (HCM)
- Dilated cardiomyopathy (DCM)
- Advanced age
- Hypertension
- Use of corticosteroids
References
- ↑ Napodano M, Tarantini G, Ramondo A, Cacciavillani L, Corbetti F, Marra MP, Fraccaro C, Peluso D, Razzolini R, Iliceto S (2009). “Myocardial abnormalities underlying persistent ST-segment elevation after anterior myocardial infarction”. J Cardiovasc Med (Hagerstown). 10 (1): 44–50. doi:10.2459/JCM.0b013e32831967b2. PMID 19145116.
- ↑ Maron MS, Finley JJ, Bos JM, Hauser TH, Manning WJ, Haas TS, Lesser JR, Udelson JE, Ackerman MJ, Maron BJ (2008). “Prevalence, clinical significance, and natural history of left ventricular apical aneurysms in hypertrophic cardiomyopathy”. Circulation. 118 (15): 1541–9. doi:10.1161/CIRCULATIONAHA.108.781401. PMID 18809796.
- ↑ Bulkley BH, Roberts WC (1974). “Steroid therapy during acute myocardial infarction. A cause of delayed healing and of ventricular aneurysm”. Am. J. Med. 56 (2): 244–50. PMID 4812079.
- ↑ Mourdjinis A, Olsen E, Raphael MJ, Mounsey JP (1968). “Clinical diagnosis and prognosis of ventricular aneurysm”. Br Heart J. 30 (4): 497–513. PMC 487659. PMID 5659397.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
The clue to the diagnosis of LV aneurysm after an MI is a persistent ST elevation without chest pain, and there is no recommendation for screening patients for LV aneurysm.
Screening
According to 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction, screening for LV aneurysm is not recommended.[1]
References
- ↑ O’Gara PT, Kushner FG, Ascheim DD, Casey DE, Chung MK, de Lemos JA, Ettinger SM, Fang JC, Fesmire FM, Franklin BA, Granger CB, Krumholz HM, Linderbaum JA, Morrow DA, Newby LK, Ornato JP, Ou N, Radford MJ, Tamis-Holland JE, Tommaso CL, Tracy CM, Woo YJ, Zhao DX (2013). “2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the American College of Emergency Physicians and Society for Cardiovascular Angiography and Interventions”. Catheter Cardiovasc Interv. 82 (1): E1–27. doi:10.1002/ccd.24776. PMID 23299937.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Heart failure, ventricular arrhythmia, mural thrombosis, and ventricular rupture, are complications of LV aneurysm that may develop despite proper treatment of the underlying myocardial event. The overall prognosis is dependent on the size of the aneurysm, the presence of akinesia, and the extent of the underlying cardiac event.
Natural History
If left untreated, it may lead to heart failure and persistent anginal pain. For false aneurysms, rupture and hemodynamic compromise are the usual outcomes if left untreated. Improvements in STEMI management, control of hypertension, and avoidance of corticosteroids in STEMI have led to a better prognosis and decreased mortality.[1]
Complications
Mural thrombi
It occurs in almost 50% of patients and can be detected by angiography or echocardiography.[1]
Heart failure
Paradoxical movement in the aneurysmal portion of the LV wall reduces the efficiency of the ventricular contraction, and compromises the stroke volume. It may lead to LV dilation and an increase in LV end-diastolic pressure, this may be accompanied by chest pain.[2][3]
Arrhythmia
Approximately 15% have symptomatic ventricular arrhythmias that may be intractable and life-threatening.[4]
Ventricular rupture
Unlike false aneurysms, a mature true LV aneurysm rarely ruptures.[5]
Prognosis
Depending on the size of the aneurysm, the extent of the underlying cardiac event, the presence of complications, and the promptness of medical intervention, the prognosis may vary. However, the overall prognosis is improved by modern treatment and advanced management.
References
- ↑ 1.0 1.1 Mourdjinis A, Olsen E, Raphael MJ, Mounsey JP (1968). “Clinical diagnosis and prognosis of ventricular aneurysm”. Br Heart J. 30 (4): 497–513. PMC 487659. PMID 5659397.
- ↑ Nicolosi AC, Spotnitz HM (1988). “Quantitative analysis of regional systolic function with left ventricular aneurysm”. Circulation. 78 (4): 856–62. PMID 3168193.
- ↑ Klein MD, Herman MV, Gorlin R (1967). “A hemodynamic study of left ventricular aneurysm”. Circulation. 35 (4): 614–30. PMID 6024006.
- ↑ Waldo AL, Arciniegas JG, Klein H (1981). “Surgical treatment of life-threatening ventricular arrhythmias: the role of intraoperative mapping and consideration of the presently available surgical techniques”. Prog Cardiovasc Dis. 23 (4): 247–64. PMID 7008078.
- ↑ Vlodaver Z, Coe JI, Edwards JE (1975). “True and false left ventricular aneurysms. Propensity for the altter to rupture”. Circulation. 51 (3): 567–72. PMID 1132088.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | CT | MRI | Echocardiography or Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH