
ST elevation myocardial infarction
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Arzu Kalayci, M.D. [2]
Synonyms and keywords: AMI, STEMI, heart attack, MI, myocardial infarct, acute MI, coronary, coronary thrombosis
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
Acute myocardial infarction, more commonly known as a heart attack, is a medical condition that occurs when the blood supply to a part of the heart muscle or myocardium is interrupted. The resulting ischemia or oxygen shortage causes damage and / or irreversible death (necrosis) of the myocardium (heart muscle). It is a medical emergency, and the leading cause of death for both men and women worldwide, particularly in developed countries.[1] The termmyocardial infarction is derived from myocardium (the heart muscle) and infarction (tissue death due to oxygen starvation). The phrase “heart attack” is sometimes used incorrectly to describe sudden cardiac death, which may or may not be the result of acute myocardial infarction.
There are two types of acute MI: ST elevation myocardial infarction (STEMI), the topic of this chapter and non ST elevation MI (NSTEMI) which is discussed in another chapter of WikiDoc. ST elevation myocardial infarction refers to an electrocardiographic pattern in which the ST segments are elevated reflecting complete epicardial vessel occlusion. Once the vessel is opened by percutaneous coronary angioplasty, the ST segments can remain elevated due to absence of perfusion or flow into the myocardium itself. At this point in the evolution of the ST elevation MI, the epicardial artery is open, but the capillary network is occluded due to swelling, embolization, and / or vasospasm.
Non ST elevation myocardial infarction refers to a disease state in which the epicardial artery is open, but there is inadequate blood flow to the myocardium which results in an electrocardiographic pattern of ST segment depression. While ST elevation reflects transmural injury, ST depression may reflect ongoing subendocardial ischemia. Inadequate blood flow to the muscle may be due to embolization of material downstream into the myocardium or a restriction of blood flow due to severe narrowing of the epicardial artery. [2] [3] [4]
Epidemiology and Demographics
Myocardial infarction is a common presentation of ischemic heart disease. The World Heart Organization (WHO) estimated in 2002 that, 12.6 percent of deaths worldwide were from ischemic heart disease. Ischemic heart disease is the leading cause of death in developed countries, but third to AIDS and lower respiratory infections in developing countries.[5] Although it is difficult to ascertain the true incidence of ST elevation myocardial infarction (STEMI), according to the ACC/AHA guidelines, a conservative estimate is that approximately 500,000 patients suffer STEMI each year [6]. The incidence of STEMI has decreased over time. In an observational study of 5,832 metropolitan patients spanning from 1975 to 1997, the incidence of STEMI decreased from 171/100,000 to 101/100,000 [7].
Risk Factors
Important ST elevation myocardial infarction risk factors are a previous history of vascular disease such as atherosclerotic coronary heart disease and/or angina, a previous heart attack or stroke, advanced age, smoking, the abuse of certain illicit drugs such as cocaine, high LDL (Low-density lipoprotein) and low HDL (High density lipoprotein), diabetes, high blood pressure, obesity and family history of coronary artery disease.[8] [9]
Risk Stratification
Two main risk-stratification scores are used when assessing a patient with ST elevation MI and acute coronary syndromes; the TIMI Risk Score (for MI), and the GRACE risk score (for acute coronary syndrome.
Triggers
A trigger is an activity or environmental condition that produces short-term physiological changes that may lead directly to onset of STEMI. ST elevation myocardial infarction triggers include physical exertion, psychological stress, sexual activity, diurnal (daily) variations in cortisol and platelet aggregation and circannual (yearly) variations in lipids and infectious etiologies, exposure to pollution and or particulate matter, cocaine and ingestion of a recent fatty meal. [10]
Natural History, Complications and Prognosis
The natural progression of ST elevation myocardial infarction depends on epicardial artery patency and the risk for early vessel reocclusion. Without treatment, ST elevation myocardial infarction can prove deadly.
Prognosis
Despite advances in modern pharmacotherapy and device-based therapy, the short term mortality remains high in modern registry series (15%-20%). The prognosis for patients with myocardial infarction varies greatly depending upon simple demographic variables like age, the presence of signs and symptoms of heart failure, the duration of symptoms, and comorbidities that are present. Several risk stratification tools have been developed to predict a patient’s mortality. Most of these risk scores are based upon clinical data obtained at the time of admission rather than at the time of discharge.
While we as physicians often labor under the impression that we can dramatically change a patient’s prognosis, it is noteworthy that 90% of the predictive information regarding 30 day mortality is contained in the following 5 baseline variables that can be modified to only a limited degree: [11]
- Advanced age
- Sinus tachycardia
- Reduced systolic blood pressure
- Heart failure or Killip class of two or greater
- Anterior myocardial infarction location
Sinus tachycardia, hypotension, Killip class, and anterior MI are all essentially markers of poor pump function on admission. These risk factors for 30 day mortality have been well validated in a multivariate analysis of 41,020 patients in the GUSTO-I trial. Advanced age was the most significant factor associated with higher 30-day mortality. The rate was only 1.1% in the youngest decile (< 45 years) and climbed to 20.5% in patients > 75 (adjusted chi 2 = 717, P < .0001). Other variables most closely associated with an increased risk of mortality were lower systolic blood pressure at randomizaiton (chi 2 = 550, P < .0001), higher Killip class (chi 2 = 350, P < .0001), elevated heart rate (chi 2 = 275, P < .0001), and the presence of an anterior infarction (chi 2 = 143, P < .0001). When taken together, these five baseline characteristics contained 90% of the prognostic information. Other significant though less important factors included previous myocardial infarction, height, time to treatment, diabetes, weight, smoking status, type of thrombolytic, previous bypass surgery,hypertension, and prior cerebrovascular disease. When these variables were combined, a validated model was created which stratified patients according to their mortality risk and accurately estimated the likelihood of death.
Various risk tools such as the GRACE risk score have been developed to risk stratify patients.
Pregnancy
Physiological changes during pregnancy may increase the woman’s risk of developing a myocardial infarction (MI). MI during the antepartum period is usually caused by an atherosclotic plaque rupture, whereas MI during the peripartum and postpartum period is usually caused by coronary artery dissection (commonly in the LAD). Diagnosis of MI among pregnant women is similar to that in the general population and requires clinical suspiccion, as well as ECG changes and troponin elevation. In contrast, elevated CK-MB concentration is unreliable, since CK-MB may normally increase during labor and post-delivery due to non-cardiac causes, namely placental and uterine leaks. During an MI, echocardiography is safe and may be performed to evaluate wall motion abnormalities, and fetal monitoring is recommended. Treatment is usually by percutaneous coronary intervention. If spontaneous coronary artery dissection occurs, a more thorough investigation for connective tissue diseases and vasculitis is warranted.
Diagnosis
Diagnostic Criteria
The diagnosis of acute MI is based upon the occurence of clinical symptoms such as substernal chest pain, EKG changes such as ST elevation and a rise in the release of very specific biomarkers into the bloodstream that are normally only found in side the heart muscle cell (the myocyte).
The diagnosis can be confirmed at the time of autopsy or at the time of angiography if a closed artery is seen. A new clinical evidence based diagnostic and classification system has been introduced by Thygesen K, Alpert JS, White HD, et al. and jointly sponsored by the American College of Cardiology (ACC), American Heart Association (AHA), European Society of Cardiology (ESC), and the World Heart Federation (WHF).[12]
History and Symptoms
One third of patients who experience ST Segment Elevation Myocardial Infarction (STEMI) will die within 24 hours of the onset of ischemia, and many of the survivors will suffer significant morbidity. Morbidity and mortality from STEMI can be reduced significantly if patients and bystanders recognize symptoms early, activate the EMS, and thereby shorten the time to definitive treatment.
Classical symptoms of acute myocardial infarction include chest pain (which in some patients may radiate to the left arm), shortness of breath, nausea, vomiting, palpitations, sweating, and anxiety or a feeling of impending doom.
Many patients will state that there was no chest pain, but rather a sense of chest discomfort that they may describe as a squeezing sensation or a sense of chest heaviness or fullness.
Patients frequently feel suddenly ill. Women may experience different symptoms from men. Common associated symptoms of MI in women includeshortness of breath, weakness, and fatigue.
Serial electrocardiographic studies from the Framingham study have shown that approximately one quarter of all myocardial infarctions (the appearance of new pathologic q waves) are silent, without chest pain or other symptoms.[13] The prognosis of patients with a silent MI was as bad as those with a symptomatic MI.
Physical Examination
The physical examination in patients who have suspected acute myocardial infarction may reveal arrhythmia, evidence of heart failure, a new murmur, or cardiovascular compromise and shock. A systems focused examination is probably most appropriate at the time of presentation so as to not delay decisions regarding and implementation of reperfusion therapy. Following these initial stages of management, a more through examination is then warranted. Throughout the patient’s course, detailed serial examinations should be performed in an effort to remain vigilant for the development of mechanical complications of acute MI. The approach to the physical examination in the patient with ST elevation MI is divided into two phases: The initial physical examination and then the more thorough examination of the patient after the initial assessment and treatment of the patient.
Laboratory Findings
A new clinical evidence based classification system has been jointly introduced by the American College of Cardiology (ACC), American Heart Association (AHA), European Society of Cardiology (ESC), and the World Heart Federation (WHF)[14]. The primary diagnostic tests include the electrocardiogram (ECG, EKG) and blood tests to detect elevated creatine kinase or troponin levels (these are chemical markers released by damaged tissues, especially the myocardium).
Electrocardiogram
A primary purpose of the electrocardiogram is to detect ischemia or acute coronary injury in broad, symptomatic emergency department populations. Common EKG findings in STEMI include ST segment elevation, new LBBB pattern and hyperacute T waves.
Imaging
Coronary Angiography
The goal of coronary angiography in STEMI patients is to identify the obstructed culprit artery and to open it as quickly as possible. The goal is to achieve a door to balloon time in under 90 minutes. This is the time from when a patient arrives at the door of the emergency room until the time that the first device is activated in the coronary artery.
Treatment
Medical Therapy
Immediate treatment for suspected acute myocardial infarction includes oxygen, full dose non-enteric coated aspirin, nitroglycerin (also known as glyceryl trinitrate) and pain relief, using an analgesic agent such morphine sulfate. Among patients who do not have signs or symptoms of cardiogenic shock, beta blocker administration has been associated with improved clinical outcomes among patients with ST elevation myocardial infarction[15]. These agents exert their benefit via several mechanisms: They reduce myocardial oxygen demands; they reduce contractility which in turn reduces the risk of mechanical complications; they reduce the risk of lethal ventricular arrhythmias.
A cornerstone in the management of STEMI is reperfusion or opening of the closed epicardial coronary artery. This can be achieved with either drugs such as a fibrinolytic agent, or mechanically with inflation of a balloon to puch the clot aside (percutaneous coronary intervention or PCI). A decade of expereince has shown that if it can be accomplished in a timely manner (a door-to-balloon time < 90 minutes), then PCI offers superior outcomes to fibrinolytic administration. In under 5% of patients, bypass surgery may be required given the extent of disease. A common practice is to perform urgent conventional balloon angioplasty of the culprit vessel as a bridge to a more definitive CABG operation.
Antiplatelet therapy is a mainstay of STEMI management. Aspirin is a cornerstone of STEMI management. Given that the majority of patients undergoing primary PCI are treated with an intracoronary stent, thienopyridine therapy is also essential. Depending upon a variety of factors, glycoprotein IIbIIIa inhibition is administered in approximately 70% of STEMI patients undergoing primary PCI.
Likewise, antithrombin therapy is also a mainstay of STEMI management. Frequent choices among patients treated with fibrinolytic agents include unfractionated heparin in the United States, and enoxaparin and fondaparinux in other countries. Among patients undergoing primary PCI, frequent choices include bivalirudin and unfractionated heparin.
Monitoring of the Patient to Reduce post MI Complications
Admission of patients to the modern coronary care unit has been associated with rapid treatment of and reduced complications from fatal arrhythmias such as ventricular tachycardia or ventricular fibrillation.
Other complications of STEMI include reinfarction, infarct extension, postinfarction angina, rupture of the ventricular septum causing a ventricular septal defect, acute mitral regurgitation, myocardial rupture, development of a pseudoaneurysm, development of cardiogenic shock, development of a ventricular aneurysm, embolic complications, and pericarditis.
References
- ↑ The World Health Report 2004 – Changing History (PDF). World Health Organization. 2004. pp. 120–4. ISBN 92-4-156265-X.
- ↑ Hurst’s The Heart, Fuster V, 12th edition, 2008
- ↑ Topol’s Textbook of Cardiovascular Medicine, Topol E, 3rd edition, 2007
- ↑ Mayo Textbook of Cardiology, 2007
- ↑ “Cause of Death – UC Atlas of Global Inequality”. Center for Global, International and Regional Studies (CGIRS) at the University of California Santa Cruz. Unknown parameter
|accessyear=ignored (|access-date=suggested) (help); Unknown parameter|accessmonthday=ignored (help) - ↑ Antman EM, Anbe DT, Armstrong PW; et al. (2004). “ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction; A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of patients with acute myocardial infarction)”. J. Am. Coll. Cardiol. 44 (3): E1–E211. doi:10.1016/j.jacc.2004.07.014. PMID 15358047. Unknown parameter
|month=ignored (help) - ↑ Furman MI, Dauerman HL, Goldberg RJ, Yarzebski J, Lessard D, Gore JM (2001). “Twenty-two year (1975 to 1997) trends in the incidence, in-hospital and long-term case fatality rates from initial Q-wave and non-Q-wave myocardial infarction: a multi-hospital, community-wide perspective”. J. Am. Coll. Cardiol. 37 (6): 1571–80. PMID 11345367. Unknown parameter
|month=ignored (help) - ↑ Antman EM, Anbe DT, Armstrong PW; et al. (2004). “ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction–executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1999 Guidelines for the Management of Patients With Acute Myocardial Infarction)”. Circulation. 110 (5): 588–636. doi:10.1161/01.CIR.0000134791.68010.FA. PMID 15289388. Unknown parameter
|month=ignored (help) - ↑ Antman EM, Hand M, Armstrong PW; et al. (2008). “2007 focused update of the ACC/AHA 2004 guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines”. J. Am. Coll. Cardiol. 51 (2): 210–47. doi:10.1016/j.jacc.2007.10.001. PMID 18191746. Unknown parameter
|month=ignored (help) - ↑ Muller JE, Abela GS, Nesto RW, Tofler GH (1994). “Triggers, acute risk factors and vulnerable plaques: the lexicon of a new frontier”. J. Am. Coll. Cardiol. 23 (3): 809–13. PMID 8113568. Unknown parameter
|month=ignored (help) - ↑ Lee KL, Woodlief LH, Topol EJ; et al. (1995). “Predictors of 30-day mortality in the era of reperfusion for acute myocardial infarction. Results from an international trial of 41,021 patients. GUSTO-I Investigators”. Circulation. 91 (6): 1659–68. PMID 7882472. Unknown parameter
|month=ignored (help) - ↑ Thygesen K, Alpert JS, White HD; et al. (2007). “Universal definition of myocardial infarction”. Circulation. 116 (22): 2634–53. doi:10.1161/CIRCULATIONAHA.107.187397. PMID 17951284. Unknown parameter
|month=ignored (help) - ↑ Kannel WB (1986). “Silent myocardial ischemia and infarction: insights from the Framingham Study”. Cardiol Clin. 4 (4): 583–91. PMID 3779719. Unknown parameter
|month=ignored (help) - ↑ Thygesen K, Alpert JS, White HD (2007). “Task Force for the Redefinition of Myocardial Infarction. Universal definition of myocardial infarction Joint ESC/ACCF/AHA/WHF”. Circulation. 2007: 2634–2653. PMID 17951284.
- ↑ Dargie HJ (2001). “Effect of carvedilol on outcome after myocardial infarction in patients with left-ventricular dysfunction: the CAPRICORN randomised trial”. Lancet. 357 (9266): 1385–90. PMID 11356434. Unknown parameter
|month=ignored (help)
Classification
Anterior myocardial infarction | Inferior myocardial infarction | Right ventricular myocardial infarction | Posterior myocardial infarction | Lateral myocardial infarction
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editors-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Classification
Acute myocardial infarction is a type of acute coronary syndrome, which is most frequently (but not always) a manifestation of coronary artery disease. The acute coronary syndromes include ST segment elevation myocardial infarction (STEMI), non-ST segment elevation myocardial infarction (NSTEMI), and unstable angina (UA).
Depending on the location of the obstruction in the coronary circulation, different zones of the heart can become injured. Using the anatomical terms of location, one can describe anterior, inferior, lateral, apical and septal infarctions (and combinations, such as anteroinferior, anterolateral, and so on).[1] For example, an occlusion of the left anterior descending coronary artery will result in an anterior wall myocardial infarct.[2]
Another distinction is whether a MI is subendocardial, affecting only the inner third to one half of the heart muscle, or transmural, damaging (almost) the entire wall of the heart.[3] The inner part of the heart muscle is more vulnerable to oxygen shortage, because the coronary arteries run inward from the epicardium to the endocardium, and because the blood flow through the heart muscle is hindered by the heart contraction.[2]
The phrases transmural and subendocardial infarction used to be considered synonymous with Q-wave and non-Q-wave myocardial infarction respectively, based on the presence or absence of Q waves on the ECG. It has since been shown that there is no clear correlation between the presence of Q waves with a transmural infarction and the absence of Q waves with a subendocardial infarction,[4] but Q waves are associated with larger infarctions, while the lack of Q waves is associated with smaller infarctions. The presence or absence of Q-waves also has clinical importance,[5] with improved outcomes associated with a lack of Q waves.[6]
The phrase “massive heart attack” is not a recognized medical term.
See also
- acute coronary syndrome
- angina
- Cardiac arrest
- coronary thrombosis
- Hibernating myocardium
- Stunned myocardium
- Ventricular remodeling
References
- ↑ “Dorland’s Illustrated Medical Dictionary”. WB Saunders, an Elsevier imprint. Unknown parameter
|accessyear=ignored (|access-date=suggested) (help); Unknown parameter|accessmonthday=ignored (help) - ↑ 2.0 2.1 Rubin’s Pathology – Clinicopathological Foundations of Medicine. Maryland: Lippincott Williams & Wilkins. 2001. p. 525. ISBN 0-7817-4733-3. Unknown parameter
|coauthors=ignored (help) - ↑ Rubin’s Pathology – Clinicopathological Foundations of Medicine. Maryland: Lippincott Williams & Wilkins. 2001. pp. p. 545. ISBN 0-7817-4733-3. Unknown parameter
|coauthors=ignored (help) - ↑ Moon JC, De Arenaza DP, Elkington AG, Taneja AK, John AS, Wang D, Janardhanan R, Senior R, Lahiri A, Poole-Wilson PA, Pennell DJ. (2004). “The pathologic basis of Q-wave and non-Q-wave myocardial infarction: a cardiovascular magnetic resonance study”. J Am Coll Cardiol. 44 (3): 554–60. PMID 15358019.
- ↑ Yang H, Pu M, Rodriguez D, Underwood D, Griffin BP, Kalahasti V, Thomas JD, Brunken RC (2004). “Ischemic and viable myocardium in patients with non-Q-wave or Q-wave myocardial infarction and left ventricular dysfunction: a clinical study using positron emission tomography, echocardiography, and electrocardiography”. J Am Coll Cardiol. 43 (4): 592–8. PMID 14975469.
- ↑ Goodman SG, Langer A, Ross AM, Wildermann NM, Barbagelata A, Sgarbossa EB, Wagner GS, Granger CB, Califf RM, Topol EJ, Simoons ML, Armstrong PW. (1998). “Non-Q-wave versus Q-wave myocardial infarction after thrombolytic therapy: angiographic and prognostic insights from the global utilization of streptokinase and tissue plasminogen activator for occluded coronary arteries-I angiographic substudy. GUSTO-I Angiographic Investigators”. Circulation. 97 (5): 444–50. PMID 9490238.
External links
- The MD TV: Comments on Hot Topics, State of the Art Presentations in Cardiovascular Medicine, Expert Reviews on Cardiovascular Research
- Clinical Trial Results: An up to dated resource of Cardiovascular Research
- Risk Assessment Tool for Estimating Your 10-year Risk of Having a Heart Attack – based on information of the Framingham Heart Study, from the United States National Heart, Lung and Blood Institute
- Heart Attack – overview of resources from MedlinePlus.
- Heart Attack Warning Signals from the Heart and Stroke Foundation of Canada
- Regional PCI for STEMI Resource Center – Evidence based online resource center for the development of regional PCI networks for acute STEMI
- STEMI Systems – Articles, profiles, and reviews of the latest publications involved in STEMI care. Quarterly newsletter.
- American College of Cardiology (ACC) Door to Balloon (D2B) Initiative.
- American Heart Association’s Heart Attack web site – Information and resources for preventing, recognizing and treating heart attack.
Pathophysiology
Pathophysiology of Vessel Occlusion | Pathophysiology of Reperfusion | Gross Pathology | Histopathology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
ST elevation myocardial infarction is largely influenced by the role of plaque rupture.
The Role of Plaque Rupture in ST Elevation Myocardial Infarction
Atherosclerosis, or hardening of the arteries, is the gradual buildup of cholesterol and fibrous tissue (collagen and smooth muscle cells) throughout the vascular tree. When there is localized accumulation of lipids and scar tissue, this is called a “plaque”. Somewhat paradoxically, it is not the most severe plaque narrowing that leads to ST elevation MI. Pathological studies indicate that it is often mild-to-moderate, lipid-laden, inflamed plaques that are the ones most likely to rupture and cause an ST elevation MI (STEMI) or a non ST elevation MI (NSTEMI). [1] The role of plaque rupture in STEMI and NSTEMI is supported by studies demonstrating that plaque rupture is present in about 70% and superficial erosion is present in 30% of patients who die suddenly in whom there is documented coronary artery disease. [2] Exposure of the blood stream to the thrombogenic components of the plaque leads to activation of the coagulation cascade and thrombus formation. In STEMI, the clot completely occludes the epicardial artery, and there is a complete lack of blood flow to the involved territory. This causes transmural injury and ST elevation. In NSTEMI, there is partial obstruction with embolization. This causes ischemia and subendocardial injury that are manifested by ST depression.


Pathophysiology of and Risk Factors for Plaque Rupture
- Macrophage accumulation has been shown to be present to a greater degree in patients with acute coronary syndromes than in those patients with chronic stable angina [3] [4] These activated macrophages can release enzymes such as metalloproteinases, interstitial collagenase, gelatinase, and stromelysin that degrade collagen, elastin, and proteoglycans. [5] This enzymatic degradation in turn leads to breakdown of the fibrous cap. The thin shoulders or edges of the fibrous cap appear to be particularly vulnerable to erosion and breakdown.
- Neovascularization of the plaque Moreno et have shown that microvessel density was increased in ruptured plaques when compared with nonruptured plaques (P=0.0001). Furthermore, among lesions with severe macrophage infiltration at the fibrous cap, microvessel density was increased (P=0.0001) was well as at the edges or shoulders of the plaque (P=0.0001). Intraplaque hemorrhage was also associated with an increase in microvessel density (P=0.04) as was the presence of thin-cap fibroatheromas (P=0.038). Microvessel density at the base of the plaque was identified as an independent (P=0.003) correlate of plaque rupture. [6]
- High oscillatory shear stress
- Vasoconstriction
- Spontaneous coronary dissection
Pathophysiology of and Risk Factors for Thrombosis Following Plaque Rupture
There are numerous systemic risk factors associated with thrombus formation following plaque rupture:
- Smoking: Smoking increases platelet aggregation and plasma epinephrine levels [7]
- Fibrinogen: Elevated levels of fibrinogen have been associated with thrombosis including abnormal levels of fibrinogen [8]
- Von Willebrand factor antigen [8]
- Tissue plasminogen activator [8]
- Anticardiolipin antibodies [9]
- Cross-linked fibrin-degradation products [10]
- Polymorphisms of a platelet glycoprotein receptor [11]
Gross Pathology Findings in Plaque Rupture
-
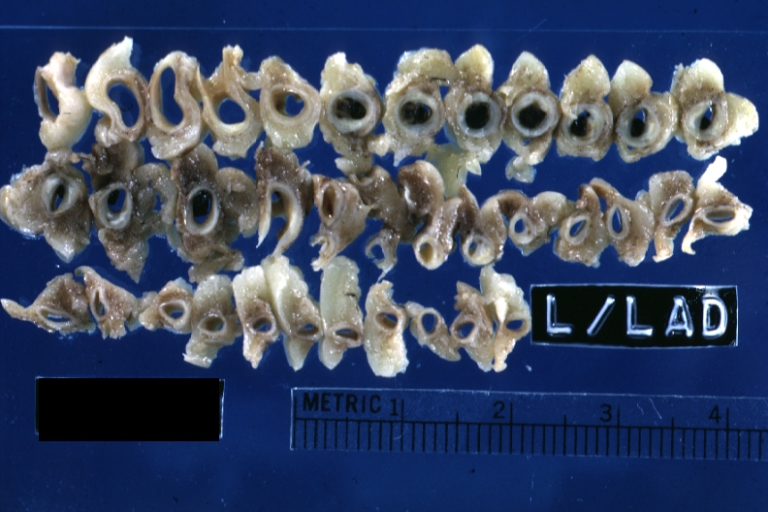
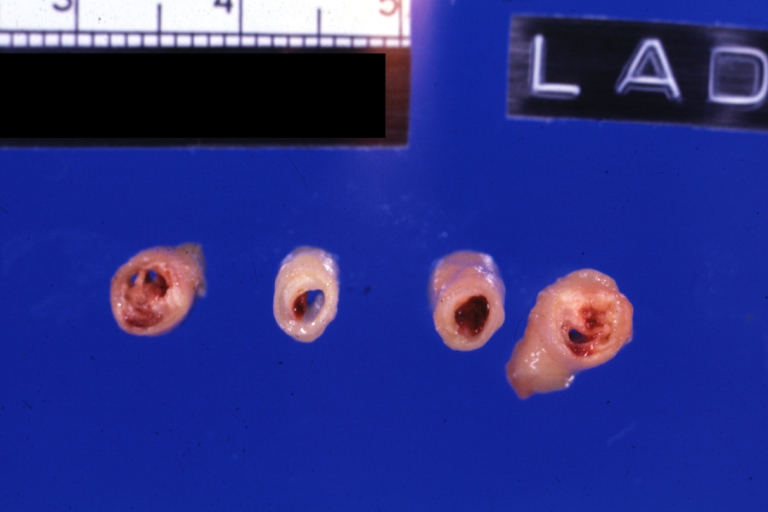 Left anterior descending coronary artery: Atherosclerosis Plaque Ruptured with Thrombosis: Gross; natural color; four cross sections, close-up view (acute anterior myocardial infarction with rupture)
Left anterior descending coronary artery: Atherosclerosis Plaque Ruptured with Thrombosis: Gross; natural color; four cross sections, close-up view (acute anterior myocardial infarction with rupture) -
 Coronary artery: Atherosclerotic Plaque: Gross natural color close-up view of a typical plaque
Coronary artery: Atherosclerotic Plaque: Gross natural color close-up view of a typical plaque


-
 Coronary Atherosclerosis: Gross, natural color, close-up view of large atherosclerotic plaque with soft atheroma (a quite good example in 54yo male. Smoker with hypertension). This slide shows the left main artery
Coronary Atherosclerosis: Gross, natural color, close-up view of large atherosclerotic plaque with soft atheroma (a quite good example in 54yo male. Smoker with hypertension). This slide shows the left main artery -
 Coronary artery: Atherosclerotic Plaque: Gross, natural color, close-up view of plaque with atheroma core causing more than 90% lumen occlusion (an excellent example)
Coronary artery: Atherosclerotic Plaque: Gross, natural color, close-up view of plaque with atheroma core causing more than 90% lumen occlusion (an excellent example)


-
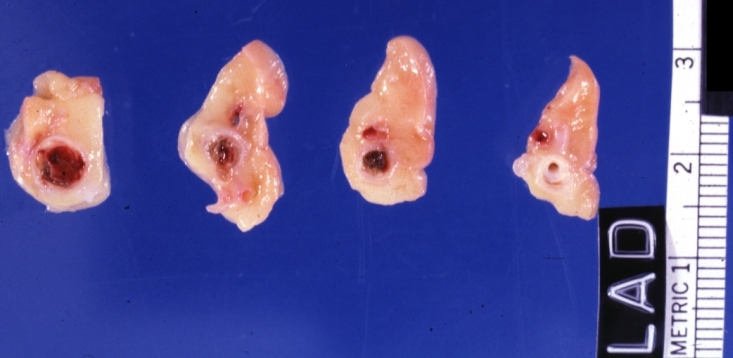
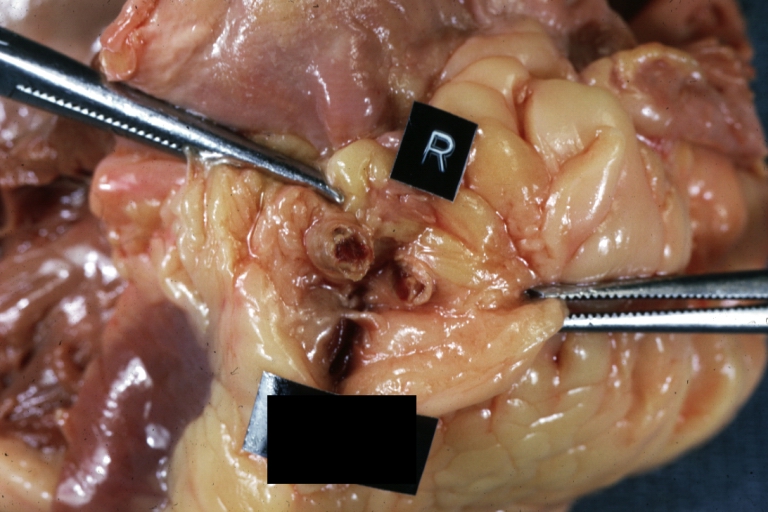
 Coronary artery: Atherosclerotic Plaque with Hemorrhage and Thrombosis: Gross, natural color, cross section, close-up, an excellent example of right coronary artery in 71yo female.
Coronary artery: Atherosclerotic Plaque with Hemorrhage and Thrombosis: Gross, natural color, cross section, close-up, an excellent example of right coronary artery in 71yo female. -
 Coronary artery: Atherosclerotic Plaque with Hemorrhage and Thrombosis: Gross, natural color, cross sections; there is excellent example of hemorrhagic plaque and thrombus at and just below the origin of first diagonal artery. Another one (a more acute one) was in the right coronary artery.
Coronary artery: Atherosclerotic Plaque with Hemorrhage and Thrombosis: Gross, natural color, cross sections; there is excellent example of hemorrhagic plaque and thrombus at and just below the origin of first diagonal artery. Another one (a more acute one) was in the right coronary artery.


-
 Coronary artery: Atherosclerotic Plaque with Thrombus: Gross natural color, close-up of cross section.
Coronary artery: Atherosclerotic Plaque with Thrombus: Gross natural color, close-up of cross section. -
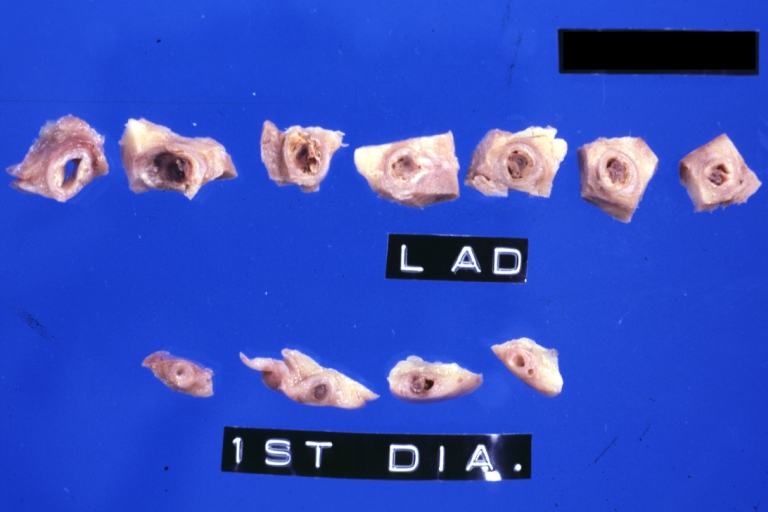 Coronary artery: Atherosclerotic Plaque with Hemorrhage: Gross fixed tissue, cross sections. LAD and 1st diagonal with large plaques and several apparent areas of hemorrhage.
Coronary artery: Atherosclerotic Plaque with Hemorrhage: Gross fixed tissue, cross sections. LAD and 1st diagonal with large plaques and several apparent areas of hemorrhage.


-
 Coronary artery: Atherosclerosis: Gross, an excellent close-up atherosclerosis with hemorrhage into plaque.
Coronary artery: Atherosclerosis: Gross, an excellent close-up atherosclerosis with hemorrhage into plaque. -
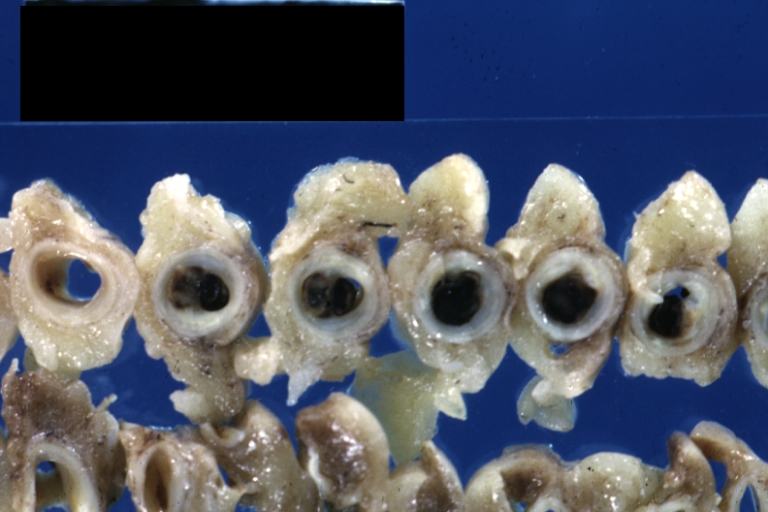
 Coronary artery: Atherosclerosis: Gross, cross sections coronary artery with hemorrhage into plaque (image shows full length of the artery).
Coronary artery: Atherosclerosis: Gross, cross sections coronary artery with hemorrhage into plaque (image shows full length of the artery).


-
 Coronary artery: Atherosclerosis: Gross, cross sections of artery showing plaques (an excellent example)
Coronary artery: Atherosclerosis: Gross, cross sections of artery showing plaques (an excellent example) -
 Coronary artery: Atherosclerosis: Gross natural color in situ cross section with large fibrocalcific plaque with hemorrhage (an excellent example)
Coronary artery: Atherosclerosis: Gross natural color in situ cross section with large fibrocalcific plaque with hemorrhage (an excellent example)


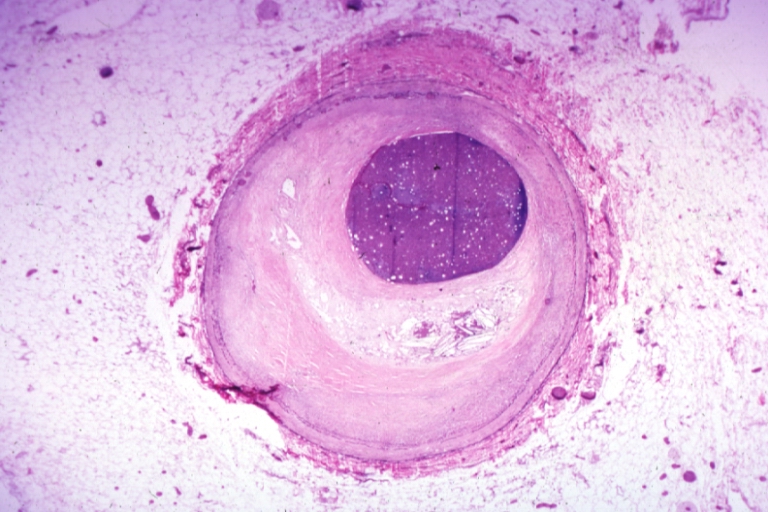
Plaque Rupture Histopathological Findings
-
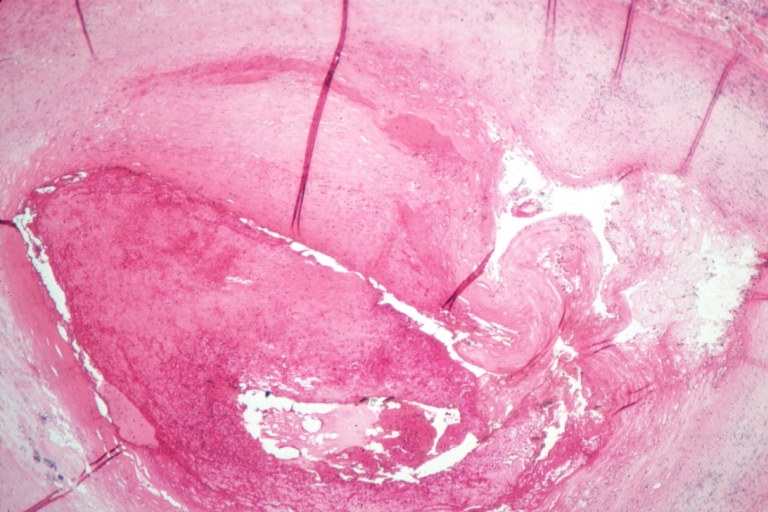
 Coronary artery: Atherosclerosis: Micro H&E med mag; A good example of plaque rupture with thrombosis.
Coronary artery: Atherosclerosis: Micro H&E med mag; A good example of plaque rupture with thrombosis. -
 Right coronary artery: Ruptured Plaque: Micro low mag H&E; Ruptured plaque with foam cell lesion (near rupture site).
Right coronary artery: Ruptured Plaque: Micro low mag H&E; Ruptured plaque with foam cell lesion (near rupture site).


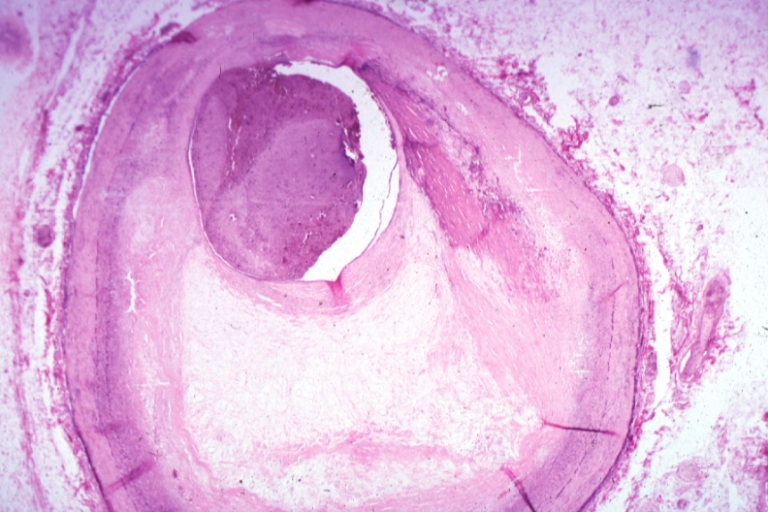
-
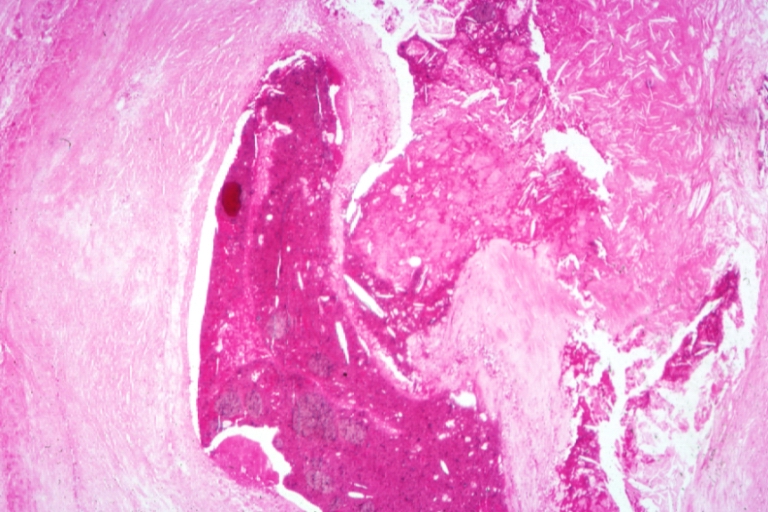
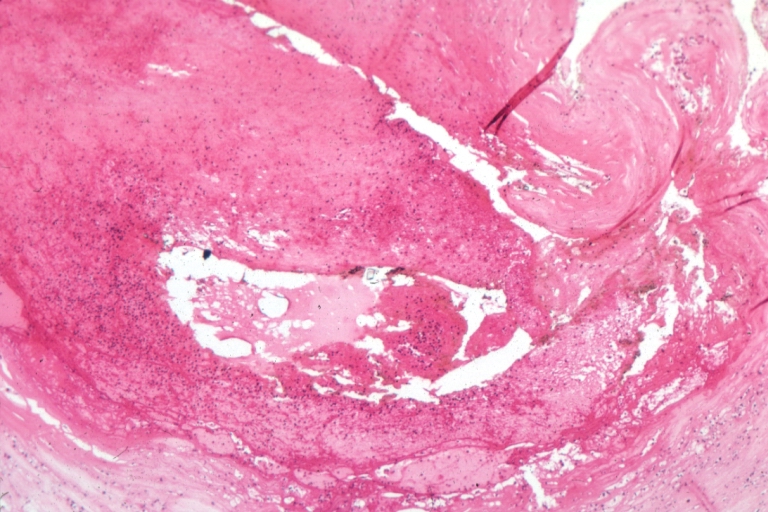
 Right coronary artery: Atherosclerosis Plaque Ruptured with Thrombus: Micro low mag H&E; an excellent view of ruptured plaque with thrombus and some old fibrin in it.
Right coronary artery: Atherosclerosis Plaque Ruptured with Thrombus: Micro low mag H&E; an excellent view of ruptured plaque with thrombus and some old fibrin in it. -
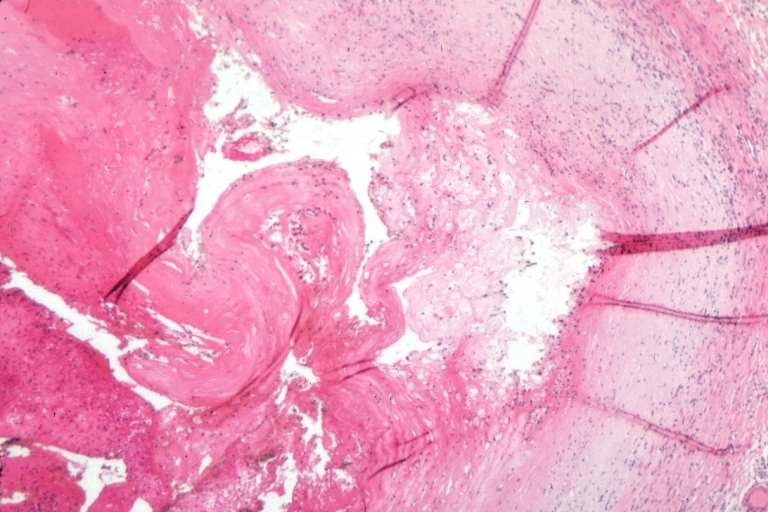
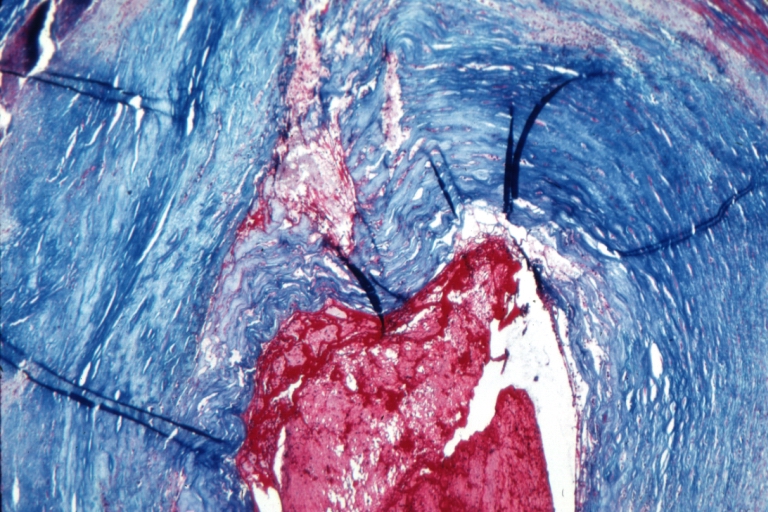 Right coronary artery: Atherosclerosis Plaque Ruptured with Thrombus: Micro low mag trichrome.
Right coronary artery: Atherosclerosis Plaque Ruptured with Thrombus: Micro low mag trichrome.


-
 Right coronary artery: Atherosclerosis Plaque Ruptured: Micro low mag H&E; large plaque with hemorrhage; (an excellent example of hemorrhage).
Right coronary artery: Atherosclerosis Plaque Ruptured: Micro low mag H&E; large plaque with hemorrhage; (an excellent example of hemorrhage). -
 Coronary artery: Atherosclerosis: Micro H&E low mag injected artery fairly typical uncomplicated atheromatous plaque
Coronary artery: Atherosclerosis: Micro H&E low mag injected artery fairly typical uncomplicated atheromatous plaque


-
 Coronary artery: Atherosclerosis: Micro H&E low mag, injected artery has typical fibrous plaque with small hemorrhage in atheroma.
Coronary artery: Atherosclerosis: Micro H&E low mag, injected artery has typical fibrous plaque with small hemorrhage in atheroma. -
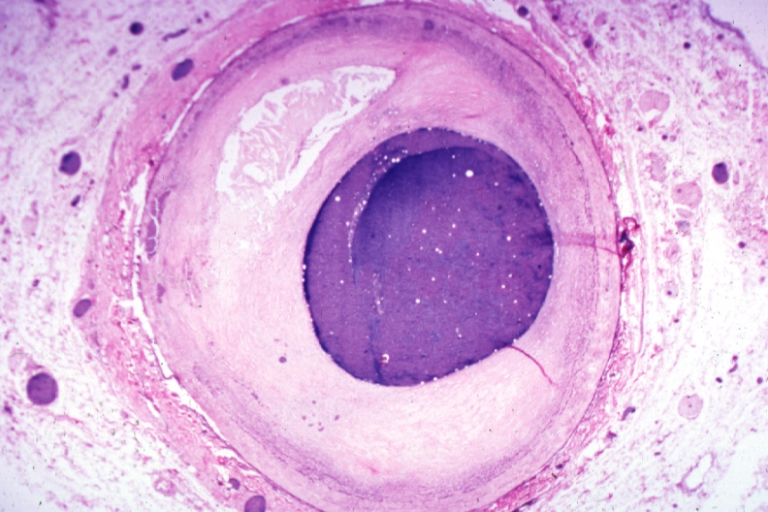
 Coronary artery: Atherosclerosis: Micro H&E low mag, injected artery is a very good example of marked lumen stenosis due to typical fibrous plaque with calcification
Coronary artery: Atherosclerosis: Micro H&E low mag, injected artery is a very good example of marked lumen stenosis due to typical fibrous plaque with calcification


The Consequence of Plaque Rupture and Vessel Occlusion: The Time Dependent Wavefront of Necrosis

In 1940, Blumgart ligated or tied off the coronary artery in dogs and cats and for the first time demonstrated a wavefront of cell death folllowing vessel occlusion [12] [13] [14] [15] [16]
Irreversible injury of ischemic myocytes occurs first in the subendocardial zone. With more extended ischemia, a wavefront of cell death moves through the myocardium to involve progressively more of the transmural thickness of the ischemic zone. The precise location, size, and specific morphologic features of an acute myocardial infarction depend on:
- The location, severity, and rate of development of coronary atherosclerotic obstructions,
- The size of the vascular bed perfused by the obstructed vessels
- The duration of the coronary artery occlusion
- The metabolic / oxygen needs of the myocardium at risk,
- The extent of collateral blood vessels
Decrease of ATP levels in myocytes in reaction to ischemia starts within seconds and causes loss of contractility in first two minutes. If ischemia persists, ATP levels reduced to its half level within 10 minutes and to 1/10 within 40 minutes. Irreversible cell injury occurs between 20-40 minutes and microvascular level injury starts if ischemia lasts more than an hour.[17]
If impaired blood flow to the heart lasts long enough, it triggers a process called the ischemic cascade; the heart cells die (chiefly through necrosis) and do not grow back. A collagen scar forms in its place. Recent studies indicate that another form of cell death called apoptosis also plays a role in the process of tissue damage subsequent to myocardial infarction.[18] As a result, the patient’s heart can be permanently damaged. This scar tissue also puts the patient at risk for potentially life threatening arrhythmias.
Pathophysiology of ST segment elevation on the electrocardiogram
In ST segment myocaridal infarction (STEMI), the ST segments on the ECG are by definition elevated and there is myonecrosis (death of myocytes) as reflected by elevation of biomarkers such as creatine kinase MB fraction (CK-MB) or troponin T or I (tn). The ST segments are elevated due to full thickness injury of the myocardium.
Videos of STEMI pathophysiology
The following are excellent videos demonstrating the underlying pathophysiology. {{#ev:youtube|L6EiPLli5x8}} {{#ev:youtube|cOMzh2hf_Vw}} {{#ev:youtube|a8Idk4EUYTs}}
References
- ↑ Falk E, Shah PK, Fuster V (1995). “Coronary plaque disruption”. Circulation. 92 (3): 657–71. PMID 7634481. Unknown parameter
|month=ignored (help) - ↑ Burke AP, Farb A, Malcom GT, Liang YH, Smialek J, Virmani R (1997). “Coronary risk factors and plaque morphology in men with coronary disease who died suddenly”. N. Engl. J. Med. 336 (18): 1276–82. PMID 9113930. Unknown parameter
|month=ignored (help) - ↑ Moreno PR, Falk E, Palacios IF, Newell JB, Fuster V, Fallon JT (1994). “Macrophage infiltration in acute coronary syndromes. Implications for plaque rupture”. Circulation. 90 (2): 775–8. PMID 8044947. Unknown parameter
|month=ignored (help) - ↑ van der Wal AC, Becker AE, van der Loos CM, Das PK (1994). “Site of intimal rupture or erosion of thrombosed coronary atherosclerotic plaques is characterized by an inflammatory process irrespective of the dominant plaque morphology”. Circulation. 89 (1): 36–44. PMID 8281670. Unknown parameter
|month=ignored (help) - ↑ Shah PK, Falk E, Badimon JJ; et al. (1995). “Human monocyte-derived macrophages induce collagen breakdown in fibrous caps of atherosclerotic plaques. Potential role of matrix-degrading metalloproteinases and implications for plaque rupture”. Circulation. 92 (6): 1565–9. PMID 7664441. Unknown parameter
|month=ignored (help) - ↑ Moreno PR, Purushothaman KR, Fuster V; et al. (2004). “Plaque neovascularization is increased in ruptured atherosclerotic lesions of human aorta: implications for plaque vulnerability”. Circulation. 110 (14): 2032–8. doi:10.1161/01.CIR.0000143233.87854.23. PMID 15451780. Unknown parameter
|month=ignored (help) - ↑ Hung J, Lam JY, Lacoste L, Letchacovski G (1995). “Cigarette smoking acutely increases platelet thrombus formation in patients with coronary artery disease taking aspirin”. Circulation. 92 (9): 2432–6. PMID 7586342. Unknown parameter
|month=ignored (help) - ↑ 8.0 8.1 8.2 Thompson SG, Kienast J, Pyke SD, Haverkate F, van de Loo JC (1995). “Hemostatic factors and the risk of myocardial infarction or sudden death in patients with angina pectoris. European Concerted Action on Thrombosis and Disabilities Angina Pectoris Study Group”. N. Engl. J. Med. 332 (10): 635–41. PMID 7845427. Unknown parameter
|month=ignored (help) - ↑ Vaarala O, Mänttäri M, Manninen V; et al. (1995). “Anti-cardiolipin antibodies and risk of myocardial infarction in a prospective cohort of middle-aged men”. Circulation. 91 (1): 23–7. PMID 7805207. Unknown parameter
|month=ignored (help) - ↑ Ridker PM, Hennekens CH, Cerskus A, Stampfer MJ (1994). “Plasma concentration of cross-linked fibrin degradation product (D-dimer) and the risk of future myocardial infarction among apparently healthy men”. Circulation. 90 (5): 2236–40. PMID 7955179. Unknown parameter
|month=ignored (help) - ↑ Weiss EJ, Bray PF, Tayback M; et al. (1996). “A polymorphism of a platelet glycoprotein receptor as an inherited risk factor for coronary thrombosis”. N. Engl. J. Med. 334 (17): 1090–4. PMID 8598867. Unknown parameter
|month=ignored (help) - ↑ Blumgart HL, Schlesinge MJ, Davis D: Studies on the relation of the clinical manifestations of angina pectoris, coronary thrombosis, and myocardial infarction to the pathologic findings, with particular reference to the significance of collateral circulation. Amer Heart J 19: 1, 1940
- ↑ Blumgart HL, Zoll PM, Freedberg AS, Gilligan DR: The experimental production of intercoronary arterial anastomoses and their functional significance. Circulation 1: 10, 1950 PMID 15401193
- ↑ Blumgart HL, Zoll PM, Kurland CS: Discussion of direct relief of coronary occlusion. Arch Intern Med (Chicago) 104: 862, 1959 PMID 13801751
- ↑ Blumgart HL, Zoll PM. Pathologic physiology of angina pectoris and acute myocardial infarction. Circulation. 1960 Aug;22:301-7. PMID 13801752
- ↑ Blumgart HL, Zoll PM, Clinical Pathologic Correlations in Coronary Artery Disease, Circulation, Volume XLVII, No 6, June 1973, 1139-43 PMID 4575525
- ↑ Robbins Pathologic Basis of Disease, Kumar V, 7th ed
- ↑ Krijnen PA, Nijmeijer R, Meijer CJ, Visser CA, Hack CE, Niessen HW. (2002). “Apoptosis in myocardial ischaemia and infarction”. J Clin Pathol. 55 (11): 801–11. PMID 12401816.
Additional Resources
- Reimer KA, Jennings RB. The “wavefront phenomenon” of myocardial ischemic cell death. II. Transmural progression of necrosis within the framework of ischemic bed size (myocardium at risk) and collateral flow. Lab Invest. 1979 Jun 40(6): 633-44. PMID 449273
- Hasche ET, Fernandes C, Freedman SB, Jeremy RW. Relation between ischemia time, infarct size, and left ventricular function in humans. Circulation. 1995 Aug 15; 92(4): 710-9. PMID 7641348
- Gibson CM, Kirtane AJ, Morrow DA, Palabrica TM, Murphy SA, Stone PH, Scirica BM, Jennings LK, Herrmann HC, Cohen DJ, McCabe CH, Braunwald E; TIMI Study Group. Association between thrombolysis in myocardial infarction myocardial perfusion grade, biomarkers, and clinical outcomes among patients with moderate- to high-risk acute coronary syndromes: observations from the randomized trial to evaluate the relative PROTECTion against post-PCI microvascular dysfunction and post-PCI ischemia among antiplatelet and antithrombotic agents-Thrombolysis In Myocardial Infarction 30 (PROTECT-TIMI 30). Am Heart J. 2006 Oct; 152 (4): 756-61. PMID 16996854
- Christian TF, Schwartz RS, Gibbons RJ. Determinants of infarct size in reperfusion therapy for acute myocardial infarction. Circulation. 1992 Jul; 86(1): 81-90. PMID 1617793
- Gibson CM, Cannon CP, Murphy SA, Marble SJ, Barron HV, Braunwald E; TIMI Study Group. Relationship of the TIMI myocardial perfusion grades, flow grades, frame count, and percutaneous coronary intervention to long-term outcomes after thrombolytic administration in acute myocardial infarction. Circulation 2002 Apr 23; 105 (16): 1909-13. PMID 11997276
- Kandzari DE, Tcheng JE, Gersh BJ, Cox DA, Stuckey T, Turco M, Mehran R, Garcia E, Zimetbaum P, McGlaughlin MG, Lansky AJ, Costantini CO, Grines CL, Stone GW; CADILLAC Investigators. Relationship between infarct artery location, epicardial flow, and myocardial perfusion after primary percutaneous revascularization in acute myocardial infarction. Am Heart J. 2006 Jun; 151(6): 1288-95. PMID 16781238
- Elsman P, van ‘t Hof AW, de Boer MJ, Hoorntje JC, Suryapranata H, Dambrink JH, Zijlstra F; Zwolle Myocardial Infarction Study Group. Role of collateral circulation in the acute phase of ST-segment-elevation myocardial infarction treated with primary coronary intervention. Eur Heart J. 2004 May; 25(10): 854-8. PMID 15140533
- Ortiz-Pérez JT, Meyers SN, Lee DC, Kansal P, Klocke FJ, Holly TA, Davidson CJ, Bonow RO, Wu E. Angiographic estimates of myocardium at risk during acute myocardial infarction: validation study using cardiac magnetic resonance imaging. Eur Heart J. 2007 Jul;28(14):1670-2. Epub 2007 Jun 22 PMID 17586811
- Maehara A, Mintz GS, Bui AB, Walter OR, Castagna MT, Canos D, Pichard AD, Satler LF, Waksman R, Suddath WO, Laird JR Jr, Kent KM, Weissman NJ. Morphologic and angiographic features of coronary plaque rupture detected by intravascular ultrasound. J Am Coll Cardiol. 2002 Sep 4;40 (5): 904-10. PMID 12225714
- Gibson CM, Murphy SA, Kirtane AJ, Giugliano RP, Cannon CP, Antman EM, Braunwald E; TIMI Study Group. Association of duration of symptoms at presentation with angiographic and clinical outcomes after fibrinolytic therapy in patients with ST-segment elevation myocardial infarction. J Am Coll Cardiol. 2004 Sep 1; 44 (5): 980-7. PMID 15337207
- D. Garcia-Dorado, P. Theroux, M. Desco, J. Solares, J. Elizaga, F. Fernandez-Aviles, J. Alonso and J. Soriano, Cell-to-cell interaction: a mechanism to explain wave-front progression of myocardial necrosis. Am J Physiol Heart Circ Physiol 256: H1266-H1273, 1989; 0363-6135/89 $5.00 PMID 2719127
- Sorajja P, Gersh BJ, Cox DA, McLaughlin MG, Zimetbaum P, Costantini C, Stuckey T, Tcheng JE, Mehran R, Lansky AJ, Grines CL, Stone GW. Impact of multivessel disease on reperfusion success and clinical outcomes in patients undergoing primary percutaneous coronary intervention for acute myocardial infarction. Eur Heart J. 2007 Jul; 28(14): 1709-16. Epub 2007 Jun 7. PMID 17556348
- Brener S. Insights into the pathophysiology of ST-elevation myocardial infarction. American Heart Journal, Volume 151, Issue 6, Pages S4 – S10, 2006 PMID 16777509
- Biasucci LM, Leo M, De Maria GL. Local and Systemic Mechanisms of Plaque Rupture. Angiology. 2008 Jun 10. [Epub ahead of print] PMID 1854458
- El-Menyar AA. Cytokines and coronary artery disease: the state of the art. Crit Pathw Cardiol. 2008 Jun; 7(2): 139-51. PMID 18520532
- Kaneda H. Coronary plaque rupture and vessel remodeling. Am J Cardiol 2008 May 15; 101 (10): 1519; PMID 18471472
- Sorajja P, Gersh BJ, Mehran R, Lansky AJ, Krucoff MW, Webb J, Cox DA, Brodie BR, Stone GW. Impact of collateral flow on myocardial reperfusion and infarct size in patients undergoing primary angioplasty for acute myocardial infarction. Am Heart J. 2007 Aug;154(2):379-84. PMID 17643592
- Kitabata H, Kubo T, Akasaka T.Identification of multiple plaque ruptures by optical coherence tomography in a patient with acute myocardial infarction: a three-vessel study. Heart 2008; 94: 544; doi:10.1136/hrt.2007.124339 PMID 18411345
- Hong MK, Mintz GS, Lee CW, Park KM, Lee BK, Kim YH, Kang DH, Cheong SS, Song JK, Kim JJ, Park SW, Park SJ. Plaque ruptures in stable angina pectoris compared with acute coronary syndrome. Int J Cardiol. 2007 Jan 2; 114(1): 78-82. Epub 2006 May 18. PMID 1671298
- Kubo T, Imanishi T, Takarada S, Kuroi A, Ueno S, Yamano T, Tanimoto T, Matsuo Y, Masho T, Kitabata H, Tsuda K, Tomobuchi Y, Akasaka T. Assessment of culprit lesion morphology in acute myocardial infarction: ability of optical coherence tomography compared with intravascular ultrasound and coronary angioscopy. J Am Coll Cardiol. 2007 Sep 4;50(10):933-9. Epub 2007 Aug 20. PMID 17765119
- Rioufol G, Finet G, Ginon I, André-Fouët X, Rossi R, Vialle E, Desjoyaux E, Convert G, Huret JF, Tabib A. Multiple atherosclerotic plaque rupture in acute coronary syndrome: a three-vessel intravascular ultrasound study. Circulation. 2002 Aug 13; 106(7): 804-8. PMID 12176951
- Hong MK, Mintz GS, Lee CW, Lee BK, Yang TH, Kim YH, Song JM, Han KH, Kang DH, Cheong SS, Song JK, Kim JJ, Park SW, Park SJ. The site of plaque rupture in native coronary arteries: a three-vessel intravascular ultrasound analysis. J Am Coll Cardiol. 2005 Jul 19; 46 (2): 261-5. PMID 16022952
- Kusama I, Hibi K, Kosuge M, Nozawa N, Ozaki H, Yano H, Sumita S, Tsukahara K, Okuda J, Ebina T, Umemura S, Kimura K. Impact of plaque rupture on infarct size in ST-segment elevation anterior acute myocardial infarction. J Am Coll Cardiol. 2007 Sep 25;50(13):1230-7. Epub 2007 Sep 10. PMID 17888839
- Tanaka N, Ehara M, Surmely JF, Matsubara T, Terashima M, Tsuchikane E, Katoh O, Suzuki T. Images in cardiovascular medicine. Sixty-four-multislice computed tomography image of a ruptured coronary plaque. Circulation. 2006 Oct 3; 114 (14): e519-20. PMID 17015797
- Fujii K, Mintz GS, Carlier SG, Costa JR Jr, Kimura M, Sano K, Tanaka K, Costa RA, Lui J, Stone GW, Moses JW, Leon MB. Intravascular ultrasound profile analysis of ruptured coronary plaques. Am J Cardiol. 2006 Aug 15;98(4):429-35. Epub 2006 Jun 19. PMID 16893692
- Gilard M, Rioufol G, Zeller M, Cottin Y, Rochette L, Finet G. Reliability and limitations of angiography in the diagnosis of coronary plaque rupture: an intravascular ultrasound study Arch Cardiovasc Dis. 2008 Feb;101(2):114-20. PMID 18398396
- Appelbaum E, Kirtane AJ, Clark A, Pride YB, Gelfand EV, Harrigan CJ, Kissinger KV, Manning WJ, Gibson CM. Association of TIMI Myocardial Perfusion Grade and ST-segment resolution with cardiovascular magnetic resonance measures of microvascular obstruction and infarct size following ST-segment elevation myocardial infarction. J Thromb Thrombolysis. 2008 Feb 2. [Epub ahead of print] PMID 18246410
- Leshnower BG, Sakamoto H, Hamamoto H, Zeeshan A, Gorman JH 3rd, Gorman RC. Progression of myocardial injury during coronary occlusion in the collateral-deficient heart: a non-wavefront phenomenon. Am J Physiol Heart Circ Physiol. 2007 Sep;293(3):H1799-804. Epub 2007 Jul 20. PMID 17644569
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ogheneochuko Ajari, MB.BS, MS [2]
Overview
The most common proximate cause of ST elevation myocardial infarction is plaque rupture. There are risk factors for plaque rupture and triggers of plaque rupture. A full discussion regarding the chronic risk factors and acute triggers of ST elevation MI can be found in other chapters. While plaque rupture is the most common cause of ST segment elevation MI, other conditions can cause ST elevation and myocardial necrosis. In order to expeditiously treat an alternate underlying cause of myonecrosis, it is important to rapidly identify conditions other than plaque rupture that may also cause ST elevation and myonecrosis. Indeed, the management of some of these conditions might differ substantially from that of plaque rupture: cocaine induced STEMI would not be treated with beta-blockers, and myocardial contusion would not be treated with an antithrombin.
Causes
Life Threatening Causes
Life-threatening causes include conditions which may result in death or permanent disability within 24 hours if left untreated.
- Aortic dissection
- Carbon monoxide poisoning
- Disseminated intravascular coagulation
- Infectious endocarditis
Common Causes
Causes by Organ System
Causes in Alphabetical Order
- Acute coronary syndrome
- Air pollution [1][2][3][4] [5]
- Amphetamines
- Amyloidosis
- Anabolic steroids
- Anaphylactic shock
- Anger[6][7][8]
- Anxiety[6]
- Aortic dissection
- Aortic stenosis
- Arrhythmias
- Atherosclerosis
- Bereavement
- Bradyarrhythmias
- Broken heart syndrome
- Carbon monoxide poisoning
- Cocaine [9]
- Combined oral contraceptive pill
- Commotio cordis
- Coronary artery aneurysm
- Coronary artery dissection
- Coronary artery vasospasm
- Coronary heart disease
- Coronary stent thrombosis
- Coronary thrombosis
- Desmopressin
- Desogestrel and Ethinyl Estradiol
- Diabetes mellitus
- Diflunisal
- Disulfiram
- Dissecting aortic aneurysm
- Dyslipidemia
- Earthquakes [10][11][12]
- Electrocution
- Electrolyte imbalance
- Ephedrine
- Epinephrine overdose
- Erythropoietin
- Ethynodiol diacetate and ethinyl estradiol
- Etonogestrel
- Fabry’s disease
- Familial hypercholesterolemia
- Fine particulate matter [13] [14] [15][16]
- Heavy meal [17][18]
- Homocystinuria
- Hurler disease
- Hypercoagulable states
- Hypertension
- Hypotension
- Idarubicin hydrochloride
- Idiopathic hypertrophic subaortic stenosis
- Indinavir
- Infectious endocarditis
- Interferon gamma
- Kawasaki disease
- Malignant hypertension
- Marijuana [19]
- Missile attacks [20][21]
- Medroxyprogesterone
- Meloxicam
- Mucopolysaccharidoses
- Myocardial contusion
- Naratriptan
- Niacin
- Nitroglycerin
- Norgestrel and Ethinyl estradiol
- Nuvaring
- Oxaprozin
- Pergolide
- Pheochromocytoma [22]
- Physical exertion[23][24][25][26][27][28][29][30][25][25][26]
- Piroxicam
- Plaque rupture
- Polyarteritis nodosa
- Polycythemia vera
- Prinzmetal angina
- Pseudoxanthoma elasticum
- Psychological stress
- Ramucirumab
- Respiratory failure
- Sexual activity [31][32]
- Sports injury [33]
- Stress cardiomyopathy
- Sudden withdrawal of beta blockers
- Sudden withdrawal of nitrates
- Sumatriptan
- Tachyarrhythmias
- Takayasu arteritis
- Takotsubo cardiomyopathy[34]
- Testosterone
- Thiamine deficiency [35] [36]
- Thrombocytosis
- Thyrotoxicosis
- Tiagabine
- Transluminal percutaneous coronary angioplasty
- Trauma
- Upper respiratory tract infection [37][38]
- Wartime bombing
References
- ↑ Peters A, Dockery DW, Muller JE, Mittleman MA (2001). “Increased particulate air pollution and the triggering of myocardial infarction”. Circulation. 103 (23): 2810–5. PMID 11401937. Unknown parameter
|month=ignored (help) - ↑ Peters A, Döring A, Wichmann HE, Koenig W (1997). “Increased plasma viscosity during an air pollution episode: a link to mortality?”. Lancet. 349 (9065): 1582–7. doi:10.1016/S0140-6736(97)01211-7. PMID 9174559. Unknown parameter
|month=ignored (help) - ↑ Peters A, Fröhlich M, Döring A; et al. (2001). “Particulate air pollution is associated with an acute phase response in men; results from the MONICA-Augsburg Study”. Eur. Heart J. 22 (14): 1198–204. doi:10.1053/euhj.2000.2483. PMID 11440492. Unknown parameter
|month=ignored (help) - ↑ Pope CA3rd, Dockery DW, Kanner RE, Villegas GM, Schwartz J (1999). “Oxygen saturation, pulse rate, and particulate air pollution: A daily time-series panel study”. Am. J. Respir. Crit. Care Med. 159 (2): 365–72. PMID 9927345. Unknown parameter
|month=ignored (help) - ↑ Peters A, Perz S, Döring A, Stieber J, Koenig W, Wichmann HE (1999). “Increases in heart rate during an air pollution episode”. Am. J. Epidemiol. 150 (10): 1094–8. PMID 10568625. Unknown parameter
|month=ignored (help) - ↑ 6.0 6.1 Mittleman MA, Maclure M, Sherwood JB; et al. (1995). “Triggering of acute myocardial infarction onset by episodes of anger. Determinants of Myocardial Infarction Onset Study Investigators”. Circulation. 92 (7): 1720–5. PMID 7671353. Unknown parameter
|month=ignored (help) - ↑ Möller J, Hallqvist J, Diderichsen F, Theorell T, Reuterwall C, Ahlbom A (1999). “Do episodes of anger trigger myocardial infarction? A case-crossover analysis in the Stockholm Heart Epidemiology Program (SHEEP)”. Psychosom Med. 61 (6): 842–9. PMID 10593637.
- ↑ Koton S, Tanne D, Bornstein NM, Green MS (2004). “Triggering risk factors for ischemic stroke: a case-crossover study”. Neurology. 63 (11): 2006–10. PMID 15596741. Unknown parameter
|month=ignored (help) - ↑ Mittleman MA, Mintzer D, Maclure M, Tofler GH, Sherwood JB, Muller JE (1999). “Triggering of myocardial infarction by cocaine”. Circulation. 99 (21): 2737–41. PMID 10351966. Unknown parameter
|month=ignored (help) - ↑ Leor J, Kloner RA (1996). “The Northridge earthquake as a trigger for acute myocardial infarction”. Am. J. Cardiol. 77 (14): 1230–2. PMID 8651102. Unknown parameter
|month=ignored (help) - ↑ Leor J, Poole WK, Kloner RA (1996). “Sudden cardiac death triggered by an earthquake”. N. Engl. J. Med. 334 (7): 413–9. PMID 8552142. Unknown parameter
|month=ignored (help) - ↑ Brown DL (1999). “Disparate effects of the 1989 Loma Prieta and 1994 Northridge earthquakes on hospital admissions for acute myocardial infarction: importance of superimposition of triggers”. Am. Heart J. 137 (5): 830–6. PMID 10220631. Unknown parameter
|month=ignored (help) - ↑ Liao D, Creason J, Shy C, Williams R, Watts R, Zweidinger R (1999). “Daily variation of particulate air pollution and poor cardiac autonomic control in the elderly”. Environ. Health Perspect. 107 (7): 521–5. PMC 1566669. PMID 10378998. Unknown parameter
|month=ignored (help) - ↑ Pope CA, Verrier RL, Lovett EG; et al. (1999). “Heart rate variability associated with particulate air pollution”. Am. Heart J. 138 (5 Pt 1): 890–9. PMID 10539820. Unknown parameter
|month=ignored (help) - ↑ Gold DR, Litonjua A, Schwartz J; et al. (2000). “Ambient pollution and heart rate variability”. Circulation. 101 (11): 1267–73. PMID 10725286. Unknown parameter
|month=ignored (help) - ↑ Peters A, Liu E, Verrier RL; et al. (2000). “Air pollution and incidence of cardiac arrhythmia”. Epidemiology. 11 (1): 11–7. PMID 10615837. Unknown parameter
|month=ignored (help) - ↑ Lipovetzky N, Hod H, Roth A, Kishon Y, Sclarovsky S, Green MS (2004). “Heavy meals as a trigger for a first event of the acute coronary syndrome: a case-crossover study”. Isr. Med. Assoc. J. 6 (12): 728–31. PMID 15609883. Unknown parameter
|month=ignored (help) - ↑ Vogel RA, Corretti MC, Plotnick GD (1997). “Effect of a single high-fat meal on endothelial function in healthy subjects”. Am. J. Cardiol. 79 (3): 350–4. PMID 9036757. Unknown parameter
|month=ignored (help) - ↑ Mittleman MA, Lewis RA, Maclure M, Sherwood JB, Muller JE (2001). “Triggering myocardial infarction by marijuana”. Circulation. 103 (23): 2805–9. PMID 11401936. Unknown parameter
|month=ignored (help) - ↑ Allegra JR, Mostashari F, Rothman J, Milano P, Cochrane DG (2005). “Cardiac events in New Jersey after the September 11, 2001, terrorist attack”. J Urban Health. 82 (3): 358–63. doi:10.1093/jurban/jti087. PMID 16000653. Unknown parameter
|month=ignored (help) - ↑ Meisel SR, Kutz I, Dayan KI; et al. (1991). “Effect of Iraqi missile war on incidence of acute myocardial infarction and sudden death in Israeli civilians”. Lancet. 338 (8768): 660–1. PMID 1679475. Unknown parameter
|month=ignored (help) - ↑ Subramanyam S, Kreisberg RA (2012). “Pheochromocytoma: a cause of ST-segment elevation myocardial infarction, transient left ventricular dysfunction, and takotsubo cardiomyopathy”. Endocr Pract. 18 (4): e77–80. doi:10.4158/EP11346.CR. PMID 22441003.
- ↑ Willich SN, Lewis M, Löwel H, Arntz HR, Schubert F, Schröder R (1993). “Physical exertion as a trigger of acute myocardial infarction. Triggers and Mechanisms of Myocardial Infarction Study Group”. N. Engl. J. Med. 329 (23): 1684–90. PMID 8232457. Unknown parameter
|month=ignored (help) - ↑ Wilson PW, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB (1998). “Prediction of coronary heart disease using risk factor categories”. Circulation. 97 (18): 1837–47. PMID 9603539. Unknown parameter
|month=ignored (help) - ↑ 25.0 25.1 25.2 Mittleman MA, Maclure M, Tofler GH, Sherwood JB, Goldberg RJ, Muller JE (1993). “Triggering of acute myocardial infarction by heavy physical exertion. Protection against triggering by regular exertion. Determinants of Myocardial Infarction Onset Study Investigators”. N. Engl. J. Med. 329 (23): 1677–83. PMID 8232456. Unknown parameter
|month=ignored (help) - ↑ 26.0 26.1 Hallqvist J, Möller J, Ahlbom A, Diderichsen F, Reuterwall C, de Faire U (2000). “Does heavy physical exertion trigger myocardial infarction? A case-crossover analysis nested in a population-based case-referent study”. Am. J. Epidemiol. 151 (5): 459–67. PMID 10707914. Unknown parameter
|month=ignored (help) - ↑ Giri S, Thompson PD, Kiernan FJ; et al. (1999). “Clinical and angiographic characteristics of exertion-related acute myocardial infarction”. JAMA. 282 (18): 1731–6. PMID 10568645. Unknown parameter
|month=ignored (help) - ↑ Albert CM, Mittleman MA, Chae CU, Lee IM, Hennekens CH, Manson JE (2000). “Triggering of sudden death from cardiac causes by vigorous exertion”. N. Engl. J. Med. 343 (19): 1355–61. PMID 11070099. Unknown parameter
|month=ignored (help) - ↑ Whang W, Manson JE, Hu FB; et al. (2006). “Physical exertion, exercise, and sudden cardiac death in women”. JAMA. 295 (12): 1399–403. doi:10.1001/jama.295.12.1399. PMID 16551711. Unknown parameter
|month=ignored (help) - ↑ Siscovick DS, Weiss NS, Fletcher RH, Lasky T (1984). “The incidence of primary cardiac arrest during vigorous exercise”. N. Engl. J. Med. 311 (14): 874–7. PMID 6472399. Unknown parameter
|month=ignored (help) - ↑ Muller JE, Mittleman MA, Maclure M, Sherwood JB, Tofler GH (1996). “Triggering myocardial infarction by sexual activity. Low absolute risk and prevention by regular physical exertion. Determinants of Myocardial Infarction Onset Study Investigators”. JAMA. 275 (18): 1405–9. PMID 8618365. Unknown parameter
|month=ignored (help) - ↑ Möller J, Ahlbom A, Hulting J; et al. (2001). “Sexual activity as a trigger of myocardial infarction. A case-crossover analysis in the Stockholm Heart Epidemiology Programme (SHEEP)”. Heart. 86 (4): 387–90. PMC 1729949. PMID 11559674. Unknown parameter
|month=ignored (help) - ↑ Witte DR, Bots ML, Hoes AW, Grobbee DE (2000). “Cardiovascular mortality in Dutch men during 1996 European football championship: longitudinal population study”. BMJ. 321 (7276): 1552–4. PMC 27557. PMID 11124170.
- ↑ Akashi YJ, Barbaro G, Sakurai T, Nakazawa K, Miyake F (2007). “Cardiac autonomic imbalance in patients with reversible ventricular dysfunction takotsubo cardiomyopathy”. QJM. 100 (6): 335–43. doi:10.1093/qjmed/hcm028. PMID 17483198.
- ↑ Kawano H, Koide Y, Toda G, Yano K (2005). “ST-segment elevation of electrocardiogram in a patient with Shoshin beriberi”. Intern. Med. 44 (6): 578–85. PMID 16020883. Unknown parameter
|month=ignored (help) - ↑ Hundley JM, Ashburn LL, Sebrell WH. The electrocardiogram in chronic thiamine deficiency in rats. Am J Physiol 144: 404–414, 1954.
- ↑ Smeeth L, Thomas SL, Hall AJ, Hubbard R, Farrington P, Vallance P (2004). “Risk of myocardial infarction and stroke after acute infection or vaccination”. N. Engl. J. Med. 351 (25): 2611–8. doi:10.1056/NEJMoa041747. PMID 15602021. Unknown parameter
|month=ignored (help) - ↑ Saikku P, Leinonen M, Tenkanen L, Linnanmaki E, Ekman MR, Manninen V, Manttari M, Frick MH, Huttunen JK. (1992). “Chronic Chlamydia pneumoniae infection as a risk factor for coronary heart disease in the Helsinki Heart Study”. Ann Intern Med. 116 (4): 273–8. PMID 1733381.
Differentiating ST Elevation Myocardial Infarction from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
ST segment myocardial infarction must be differentiated from other conditions that cause ST elevation and chest pain.
Differential Diagnosis of Causes of ST Segment Elevation in the Absence of Myonecrosis
Acute epicardial artery occlusion by thrombus is certainly one cause of ST segment elevation, but other causes of ST segment elevation which are not associated with myonecrosis include the following:[1][2][3]
In Alphabetical Order
- Aneurysm of the ventricle can result in persistent ST segment elevation that can be exacerbated with tachycardia
- Arrhythmogenic right ventricular cardiomyopathy
- Balloon inflation in a coronary artery during percutaneous coronary intervention
- Brugada syndrome
- Transthoracic cardioversion
- Coronary artery rupture during percutaneous coronary intervention
- Early repolarization is a normal variant that can result in ST segment elevation. It is more common in males of younger age. The ST elevation is exacerbated by bradycardia.
- Hyperkalemia known as the “dialyzable current of njury” hyperkalemia may cause hyperacute ECG changes due to changes in membrane polarity
- Left bundle branch block is associated with ST segment elevation in those leads that are discordant to the QRS. Stated differently, if the QRS is predominantly of a negative deflection, it is normal to observe ST segment elevation in the same leads. The presence of ST elevation in leads where the QRS deflection is upright (concordance) may be a marker of myocardial injury.
- Myopericarditis can cause injury to the subepicardial myocytes and ST segment elevation.
- Myocarditis can cause injury to the subepicardial myocytes and ST segment elevation.
- Pericardiocentesis when the needle comes into contact with the myocardium, there can be ST segment elevation reflecting local injury of the myocardium.
- Pericarditis can cause injury to the subepicardial myocytes and ST elevation.
- Pulmonary Embolism
- Prinzmetal’s angina is associated with ST segment elevation due to transient epicardial coronary artery spasm either in the absence or presence of atherosclerosis. If the condition persists long enough, myonecrosis can be observed.
- Intracranial hemorrhage (stroke) can in some cases cause ST segment elevation due to direct myocyte injury from a hyper-adrenergic stimulation emanating from the central nervous system.
Differential Diagnosis of Causes of ST Segment Elevation in the Presence of Myonecrosis (STEMI)
While plaque rupture is the most common cause of ST segment elevation MI, other conditions can cause ST elevation and myocardial necrosis. In order to expeditiously treat an alternate underlying cause of myonecrosis, it is important to rapidly identify conditions other than plaque rupture that may also cause ST elevation and myonecrosis. Indeed, the management of some of these conditions might be differ substantially from that of plaque rupture: cocaine induced STEMI would not be treated with beta-blockers, and myocardial contusion would not be treated with an antithrombin. These conditions include the following:
By Organ System
| Cardiovascular | Aortic dissection more often extends to occlude the ostium of the right coronary artery
Aortic stenosis can cause subendocardial ischemia and infarction if demand grossly exceeds supply |
| Chemical / poisoning | Carbon monoxide poisoning |
| Dermatologic | No underlying causes |
| Drug Side Effect | Oral contraceptive pills, particularly among women who smoke |
| Ear Nose Throat | A recent upper respiratory tract infections has been associated with a 4.9 fold rise in the risk of MI |
| Endocrine | Thyrotoxicosis |
| Environmental | Blizzards and snow shoveling, and inhalation of fine particulate matter in areas with air pollution and high traffic have been identified as triggers of MI. |
| Gastroenterologic | A heavy meal has been associated with a 4 fold rise in the risk of MI, and it is not clear if this is mediated by hyper-adrenergic tone[4]; |
| Genetic | Familial hypercholesterolemia |
| Hematologic | Disseminated intravascular coagulation (DIC) |
| Iatrogenic | Epinephrine overdose
Sudden withdrawal of Beta blockers or nitrates |
| Infectious Disease | A recent upper respiratory tract infections has been associated with a 4.9 fold rise in the risk of MI
Infectious endocarditis may STEMI as a result of embolization |
| Musculoskeletal / Ortho | No underlying causes |
| Neurologic | No underlying causes |
| Nutritional / Metabolic | A heavy meal has been associated with a 4 fold rise in the risk of MI and it is not clear if this is mediated by hyper-adrenergic tone[4];
Mucopolysaccharidoses or Hurler disease Thiamine deficiency has been associated with ST elevation and myonecrosis [5][6][7] |
| Obstetric/Gynecologic | Spontaneous coronary dissection in the setting of pregnancy |
| Oncologic | Radiation therapy can accelerate atherosclerosis particularly in the distribution of the left anterior descending artery; |
| Opthalmologic | No underlying causes |
| Overdose / Toxicity | Cocaine ingestion which may result in direct myocyte injury due to an adrendergic surge, vasoconstriction of the microvasculature or plaque rupture and thrombus formation;
Marijuana ingestion has been identified as a trigger of MI. |
| Psychiatric | Anger, anxiety, bereavement, work-related stress, earthquakes, bombings and other psychosocial stressors have been identified as triggers of MI, and it is not clear if the mechanism is plaque rupture or hyper-adrenergic tone;
Stress cardiomyopathy or Broken heart syndrome causes ST segment elevation most often in the anterior precordium and is thought to be due to direct myocyte injury from a hyper-adrenergic stimulation emanating from the central nervous system. |
| Pulmonary | A recent upper respiratory tract infections has been associated with a 4.9 fold rise in the risk of MI |
| Renal / Electrolyte | Homocystinuria |
| Rheum / Immune / Allergy | Takayasus |
| Sexual | Sexual activity has been identified as a trigger of MI |
| Trauma | Both penetrating and non-penetrating trauma to the heart or myocardial contusion, commotio cordis can be associated with ST elevation and myonecrosis. |
| Urologic | No underlying causes |
| Miscellaneous | Hypotension particularly if it is prolonged |
Complete Differential Diagnosis of Chest Pain
ST elevation MI is one of several life threatening causes of chest pain that must be distinguished from each other.
5 Life Threatening Diseases to Exclude Immediately
The frequency of conditions exclusive of acute myocardial infarction in a decreasing order is:[8]
- Gastroesophageal disease
- Ischemic heart disease (angina, not myocardial infarction)
- Chest wall syndromes
Differentiating the life threatening and ischemic causes of chest pain from other disorders
Thorough history including: onset, duration, type of pain, location, exacerbating factors, alleviating factors, and radiation. Risk factors for coronary artery disease: family history, smoking, hyperlipidemia, and diabetes.
Clinical Features of Different Conditions Presenting with Acute Chest Discomfort
CARDIOVASCULAR
| Condition | Onset | Duration | Type of pain | Location | Exacerbating factors | Alleviating factors | Radiation | Associated features |
|---|---|---|---|---|---|---|---|---|
| Stable Angina | Sudden (acute) | 2-10 minutes | Heaviness, pressure, tightness, squeezing, burning (Levine’s sign) | Retrosternal | Exertion, emotions, cold | Rest, sublingual nitroglycerine (within minutes) | Radiation to neck, jaw, shoulders, or arms (commonly on left) | Sweating, nausea, palpitations, dizziness, shortness of breath, sense of impending doom |
| Unstable Angina | Acute | 10-20 minutes | Same as stable angina but often more severe | Same as stable angina | Same as stable angina but occurs with lower levels of exertion & rest | Same as stable angina | Same as stable angina | Same as stable angina |
| Myocardial Infarction | Acute | Commonly > 20 minutes | Same as stable angina but often more severe | Same as stable angina | Same as stable angina but occurs with lower levels of exertion & rest | Usually unrelieved by nitroglycerine and rest | Same as stable angina | Same as stable angina |
| Aortic Stenosis | Acute, recurrent episodes of angina | Same as stable angina | Same as stable angina | Same as stable angina | Same as stable angina | Same as stable angina | Same as stable angina | Not specific |
| Aortic Dissection | Sudden severe progressive pain (common) or chronic (rare) | Variable | Tearing, ripping sensation, knife like | Depends on area of dissection | Variable | Unrelenting pain, unrelieved by nitroglycerine and rest | Radiating to back, between shoulder blades (dissection in ascending aorta) | Trauma, surgical manipulation, pregnancy, hypertension, connective tissue disease like marfan’s syndrome (cystic medial degeneration) |
| Pericarditis | Acute or subacute | May last for hours to days | Sharp, localized | Retrosternal | Increases with coughing, deep breathing, supine position | Relieved by sitting up and leaning forward | Radiation to shoulder, neck, back abdomen | Not specific |
PULMONARY
| Condition | Onset | Duration | Type of pain | Location | Exacerbating factors | Alleviating factors | Radiation | Associated features |
|---|---|---|---|---|---|---|---|---|
| Pulmonary Embolism | Acute | May last minutes to hours | Sharp, or knifelike pleuritic pain | Localized to side of lesion | Increased on respiratory movements, deep breathing or cough | Not specific | Not specific | Dyspnea, tachypnea, palpitation, and light headedness, hemoptysis, or a history of venous thromboembolism or coagulation abnormalities. |
| Spontaneous Pneumothorax | Acute | May last minutes to hours | Sharp, localized pleuritic | Localized to side of lesion | Not specific | Not specific | Not specific | Dyspnea, decreased breath sounds on involved side |
| Pleuritis | Acute, subacute, chronic | May last minutes to hours | Sharp, localized pleuritic | Localized to side of lesion | Increased on respiratory movements, deep breathing or cough | Not specific | Not specific | Dyspnea, cough, fever |
| Pulmonary Hypertension | Acute, subacute, chronic | Variable | Pressure like | Substernal | Not specific | Not specific | Not specific | Dyspnea, symptoms of right heart failure (edema |
GASTROINTESTINAL
| Condition | Onset | Duration | Type of pain | Location | Exacerbating factors | Alleviating factors | Radiation | Associated features |
|---|---|---|---|---|---|---|---|---|
| GERD, Peptic Ulcer | Acute | Minutes to hours (gastroesophageal reflux), prolonged (peptic ulcer) | Burning | Substernal, epigastric | Increases on alcohol, aspirin, post meal lying down, morning, empty stomach | Relieves on antacid, food | Not specific | Not specific |
| Esophageal Spasm | Acute | Minutes to hours | Burning, pressure | Retrosternal | Not specific | Relieved by sublingual nitroglycerine | Not specific | Not specific (closely mimic angina) |
| Cholelithiasis | Acute, subacute | Minutes to hours | Burning, colicky | Right upper abdomen, substernal, epigastric | Increases post meal, fatty food, 1-2 hours post meal | Analgesics | Not specific | Not specific |
MISCELLANEOUS
| Condition | Onset | Duration | Type of pain | Location | Exacerbating factors | Alleviating factors | Radiation | Associated features |
|---|---|---|---|---|---|---|---|---|
| Musculo-skeletal Pain | Acute, subacute | Variable | Pressure, aching | Localized to involved area | Increases by movement and pressure on involved area | Analgesics | Not specific | Not specific |
| Psychotic Conditions | Acute, subacute, chronic | Variable | Variable | Variable | Variable | Not specific | Not specific | History of depression, panic attacks, agrophobia |
By Organ System
By Alphabetical Order
- Actinomycosis
- Acute intermittent porphyria
- Adenosine
- Amonafide
- Anemia
- Ankylosing spondylitis
- Aortic valve stenosis
- Arsenic trioxide
- Arsenicals
- Blood transfusion and complications
- Bornholm disease
- Bronchogenic cyst
- Carbon monoxide toxicity
- Cardiomyopathy
- Familial hypertrophic cardiomyopathy
- Cardiopulmonary resuscitation
- Coronary artery dissection
- Diffuse esophageal spasm
- Dissecting aortic aneurysm
- Dressler syndrome
- Pleural empyema
- Esophageal achalasia
- Esophageal cyst
- Fabry disease
- Functional disorders
- Gastric ulcer
- Gastroesophageal reflux
- Gemeprost
- Glatiramer acetate
- Glycogenosis type 7
- Ischaemic heart disease
- Kawasaki disease
- Left ventricular hypertrophy
- Lymphangiomyomatosis
- Mediastinitis
- Mesothelioma
- Mitral valve prolapse
- Myocardial infarction
- Myocarditis
- Naratriptan
- Nylidrin
- Esophageal foreign body
- Esophageal rupture
- Esophagitis
- Pericarditis
- Pleural effusion
- Pleural fibroma
- Pleuritis
- Pneumonia
- Pneumothorax
- Porfimer
- Prinzmetal angina
- Pulmonary embolism
- Pulmonary infarction
- Quaternary syphilis
- Recurrent hereditary polyserositis
- Regadenoson
- Respiratory alkalosis
- Rib fracture
- Rib pain
- Rizatriptan
- Rumination disorder
- SAPHO syndrome
- Shingles
- Sickle cell crisis (thrombotic)
- Sickle cell disease
- Acute spinal cord injury
- Subdiaphragmatic abscess
- Sumatriptan
- Syndrome X
- Tabes dorsalis
- Takotsubo cardiomyopathy
- Tension pneumothorax
- Thallium
- Thyroiditis
- Tietze costochondritis
- Trichinella spiralis
- Unstable angina
- Varicella-zoster virus
- Wegener granulomatosis
- Zolmitriptan
References
- ↑ Tamis-Holland JE, Jneid H, Reynolds HR, Agewall S, Brilakis ES, Brown TM; et al. (2019). “Contemporary Diagnosis and Management of Patients With Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease: A Scientific Statement From the American Heart Association”. Circulation: CIR0000000000000670. doi:10.1161/CIR.0000000000000670. PMID 30913893.
- ↑ Wang K, Asinger RW, Marriott HJ (2003). “ST-segment elevation in conditions other than acute myocardial infarction”. N. Engl. J. Med. 349 (22): 2128–35. doi:10.1056/NEJMra022580. PMID 14645641. Unknown parameter
|month=ignored (help) - ↑ Ako J, Honda Y, Fitzgerald PJ (2004). “Conditions associated with ST-segment elevation”. N. Engl. J. Med. 350 (11): 1152–5, author reply 1152–5. doi:10.1056/NEJM200403113501118. PMID 15014192. Unknown parameter
|month=ignored (help) - ↑ 4.0 4.1 Lipovetzky N, Hod H, Roth A, Kishon Y, Sclarovsky S, Green MS (2004). “Heavy meals as a trigger for a first event of the acute coronary syndrome: a case-crossover study”. Isr. Med. Assoc. J. 6 (12): 728–31. PMID 15609883. Unknown parameter
|month=ignored (help) - ↑ Kawano H, Koide Y, Toda G, Yano K (2005). “ST-segment elevation of electrocardiogram in a patient with Shoshin beriberi”. Intern. Med. 44 (6): 578–85. PMID 16020883. Unknown parameter
|month=ignored (help) - ↑ Hundley JM, Ashburn LL, Sebrell WH. The electrocardiogram in chronic thiamine deficiency in rats. Am J Physiol 144: 404–414, 1954.
- ↑ Read DH, Harrington DD (1981). “Experimentally induced thiamine deficiency in beagle dogs: clinical observations”. Am. J. Vet. Res. 42 (6): 984–91. PMID 7197132. Unknown parameter
|month=ignored (help) - ↑ Fruergaard P, Launbjerg J, Hesse B, Jørgensen F, Petri A, Eiken P, Aggestrup S, Elsborg L, Mellemgaard K (1996). “The diagnoses of patients admitted with acute chest pain but without myocardial infarction”. European Heart Journal. 17 (7): 1028–34. PMID 8809520. Retrieved 2012-05-02. Unknown parameter
|month=ignored (help)
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-In-Chief: Yuri B. Pride, M.D. [2] ; Cafer Zorkun, M.D., Ph.D. [3]
Overview
Myocardial infarction is a common presentation of ischemic heart disease. The World Heart Organization (WHO) estimated in 2002 that, 12.6 percent of deaths worldwide were from ischemic heart disease.
Ischemic heart disease is the leading cause of death in developed countries, but third to AIDS and lower respiratory infections in developing countries.[1]
Epidemiology
Over 9 million patients in the United States alone have angina. An estimated 80,700,000 American adults (one in three) have one or more types of cardiovascular disease (CVD), of whom 38,200,000 are estimated to be age 60 or older. Except as noted, the estimates were extrapolated to the U.S. population in 2005 from NHANES 1999–2004. (Total CVD includes diseases in the bullet points below except for congenital heart disease). Due to overlap, it is not possible to add these conditions to arrive at a total. [2] [3][4]
- Hypertension: 73,000,000
- Coronary heart disease: 16,000,000
- Myocardial infarction: 8,100,000
- Angina pectoris: 9,100,000
- Heart failure: 5,300,000
- Stroke: 5,800,000
- Congenital heart disease: 650,000 – 1,300,000
This means that roughly every 65 seconds, an American dies of a coronary event.
Incidence
Although it is difficult to ascertain the true incidence of ST elevation myocardial infarction (STEMI), according to the ACC/AHA guidelines, a conservative estimate is that approximately 500,000 patients suffer STEMI each year [5]. The incidence of STEMI has decreased over time. In an observational study of 5,832 metropolitan patients spanning from 1975 to 1997, the incidence of STEMI decreased from 171/100,000 to 101/100,000 [6]
Prevalence
The following prevalence estimates are for people age 18 and older from NCHS/NHIS, 2005: [7]
- Among whites only, 12.0% have heart disease, 6.6% have CHD, 21.0% have hypertension and 2.3% have had a stroke.
- Among blacks, 10.2% have heart disease, 6.2% have CHD, 31.2% have hypertension and 3.4% have had a stroke.
- Among Hispanics or Latinos, 8.3% have heart disease, 5.9% have CHD, 20.3% have hypertension and 2.2% have had a stroke.
- Among Asians, 6.7% have heart disease, 3.8% have CHD, 19.4% have hypertension and 2.0% have had a stroke.
- Among Native Hawaiians or other Pacific Islanders, 22.4% have hypertension (other prevalence estimates considered unreliable).
The mortality among patients who suffer STEMI has progressively declined in recent years. From 1975 to 1997, one observational study reported that the in-hospital mortality decreased from 24% to 14% [6]. In the Global Registry of Acute Coronary Events (GRACE), a multinational cohort study that includes 16,814 patients with STEMI were enrolled and followed up in 113 hospitals in 14 countries between 1999 and 2006, in-hospital mortality declined from 8.4% in 1999 to 4.6% in 2005 [8].
The reason for this decline in mortality is likely multifactorial and includes, but is certainly not limited to, decline in symptom onset-to-presentation time, more widespread use of primary PCI [9], improvements in time to reperfusion (door-to-needle and door-to-balloon times) [10][11] and improved medical therapy, including increases in the use of evidence-based therapies such as aspirin [12], beta blockers[13] [14], clopidogrel [15], statins [16] and angiotension converting enzyme inhibitors or angiotensin receptor blockers [17].
References
- ↑ “Cause of Death – UC Atlas of Global Inequality”. Center for Global, International and Regional Studies (CGIRS) at the University of California Santa Cruz. Unknown parameter
|accessyear=ignored (|access-date=suggested) (help); Unknown parameter|accessmonthday=ignored (help) - ↑ 2008 Heart Disease and Stroke Statistics
- ↑ Anderson JL, Adams CD, Antman EM; et al. (2007). “ACC/AHA 2007 guidelines for the management of patients with unstable angina/non ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non ST-Elevation Myocardial Infarction): developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons: endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine”. Circulation. 116 (7): e148–304. doi:10.1161/CIRCULATIONAHA.107.181940. PMID 17679616. Unknown parameter
|month=ignored (help) - ↑ Anderson JL, Adams CD, Antman EM; et al. (2007). “ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine”. J. Am. Coll. Cardiol. 50 (7): e1–e157. doi:10.1016/j.jacc.2007.02.013. PMID 17692738. Unknown parameter
|month=ignored (help) - ↑ Antman EM, Anbe DT, Armstrong PW; et al. (2004). “ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction; A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of patients with acute myocardial infarction)”. J. Am. Coll. Cardiol. 44 (3): E1–E211. doi:10.1016/j.jacc.2004.07.014. PMID 15358047. Unknown parameter
|month=ignored (help) - ↑ 6.0 6.1 Furman MI, Dauerman HL, Goldberg RJ, Yarzebski J, Lessard D, Gore JM (2001). “Twenty-two year (1975 to 1997) trends in the incidence, in-hospital and long-term case fatality rates from initial Q-wave and non-Q-wave myocardial infarction: a multi-hospital, community-wide perspective”. J. Am. Coll. Cardiol. 37 (6): 1571–80. PMID 11345367. Unknown parameter
|month=ignored (help) - ↑ Vital Health Stat 10.2006 [232]: 1–153
- ↑ Fox KA, Steg PG, Eagle KA; et al. (2007). “Decline in rates of death and heart failure in acute coronary syndromes, 1999-2006”. JAMA. 297 (17): 1892–900. doi:10.1001/jama.297.17.1892. PMID 17473299. Unknown parameter
|month=ignored (help) - ↑ Rogers WJ, Canto JG, Lambrew CT; et al. (2000). “Temporal trends in the treatment of over 1.5 million patients with myocardial infarction in the US from 1990 through 1999: the National Registry of Myocardial Infarction 1, 2 and 3”. J. Am. Coll. Cardiol. 36 (7): 2056–63. PMID 11127441. Unknown parameter
|month=ignored (help) - ↑ McNamara RL, Wang Y, Herrin J; et al. (2006). “Effect of door-to-balloon time on mortality in patients with ST-segment elevation myocardial infarction”. J. Am. Coll. Cardiol. 47 (11): 2180–6. doi:10.1016/j.jacc.2005.12.072. PMID 16750682. Unknown parameter
|month=ignored (help) - ↑ Nallamothu B, Fox KA, Kennelly BM; et al. (2007). “Relationship of treatment delays and mortality in patients undergoing fibrinolysis and primary percutaneous coronary intervention. The Global Registry of Acute Coronary Events”. Heart. 93 (12): 1552–5. doi:10.1136/hrt.2006.112847. PMID 17591643. Unknown parameter
|month=ignored (help) - ↑ “Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarction: ISIS-2. ISIS-2 (Second International Study of Infarct Survival) Collaborative Group”. Lancet. 2 (8607): 349–60. 1988. PMID 2899772. Unknown parameter
|month=ignored (help) - ↑ “Metoprolol in acute myocardial infarction. Mortality. The MIAMI Trial Research Group”. Am. J. Cardiol. 56 (14): 15G–22G. 1985. PMID 3904389. Unknown parameter
|month=ignored (help) - ↑ “Randomised trial of intravenous atenolol among 16 027 cases of suspected acute myocardial infarction: ISIS-1. First International Study of Infarct Survival Collaborative Group”. Lancet. 2 (8498): 57–66. 1986. PMID 2873379. Unknown parameter
|month=ignored (help) - ↑ Sabatine MS, Cannon CP, Gibson CM; et al. (2005). “Addition of clopidogrel to aspirin and fibrinolytic therapy for myocardial infarction with ST-segment elevation”. N. Engl. J. Med. 352 (12): 1179–89. doi:10.1056/NEJMoa050522. PMID 15758000. Unknown parameter
|month=ignored (help) - ↑ Cannon CP, Braunwald E, McCabe CH; et al. (2004). “Intensive versus moderate lipid lowering with statins after acute coronary syndromes”. N. Engl. J. Med. 350 (15): 1495–504. doi:10.1056/NEJMoa040583. PMID 15007110. Unknown parameter
|month=ignored (help) - ↑ Latini R, Maggioni AP, Flather M, Sleight P, Tognoni G (1995). “ACE inhibitor use in patients with myocardial infarction. Summary of evidence from clinical trials”. Circulation. 92 (10): 3132–7. PMID 7586285. Unknown parameter
|month=ignored (help)
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
In these chapters on ST elevation, the word risk factors refers to those epidemiologic and genetic variables that expose someone to a higher risk of developing atherosclerotic plaque. The word triggers refer to those factors in the patients immediate history or environment that may have lead to rupture of the atherosclerotic plaque.
Nomenclature
Muller et al have developed the following nomenclature to categorize and analyze data pertaining to triggers of MI [1]:
- (1) Trigger: An activity that produces short-term physiological changes that may lead directly to onset of acute CVD.
- (2) Acute risk factor: A short-term physiological change, such as a surge in arterial pressure or heart rate, an increase in coagulability, or vasoconstriction, that follows a trigger and may result in disease onset.
- (3) Hazard period: The time interval after trigger initiation associated with an increased risk of disease onset because of the trigger. The onset and offset times of the hazard period, which could also be designated a “vulnerable period,” may be sharply defined, as in heavy exertion, or less well defined, as with respiratory infection. The duration of the hazard period may also vary, eg from < 1 hour during heavy physical exertion to weeks or months with bereavement.
- (4) Triggered acute risk prevention (TARP): Cardiovascular risk reduction that focuses on the short-term increase in risk associated with a trigger.
Risk Factors
Traditional Risk Factors for Atherosclerosis[2]
Risk factors for atherosclerosis are generally risk factors for myocardial infarction:
- Advancing age
- Male gender[3]
- Cigarette smoking
- Hypercholesterolemia (more accurately hyperlipoproteinemia, especially high low density lipoprotein and low high density lipoprotein)
- Diabetes (with or without insulin resistance)
- High blood pressure
- Obesity[4] (defined by a body mass index of more than 30 kg/m², or alternatively by waist circumference or waist-hip ratio).
- Elevated homocysteine
Genetic Disorders
- Mendelian inherited conditions
- Autosomal dominant conditions
- Pseudoxanthoma elasticum dominant type 1
- Autosomal recessive conditions
- Cystathionine beta-synthase deficiency
- Sitosterolemia
Family History and Heart Disease
According to present trends in the United States, half of healthy 40-year-old males and 1 in 3 healthy 40-year-old women will develop coronary artery disease (CAD) in the future.[5] This chance is greater when a family history of heart disease is involved.
Studies have reported that the risk of CAD increases two- to sevenfold when there is a genetic link. [6] The studies by Nora and Nora (1978a) evaluated a large number of patients with congenital heart disease.[7] Results show that about 8% of the defects were primarily genetics-related, 2% were environmental (caused by drugs, viruses, maternal nutrition, maternal metabolism, or fetal hemodynamics) and 90% were multifactorial (due to a combination of environmental and genetic factors). The study also noted that there is a two- to threefold increase in the recurrence risk for congenital heart disease when two of the family members are affected. This is particularly the case when the parent is severely affected or when the affected members are child and parent. The risk for a myocardial infarction is two to three times greater in a first-degree relative than in a person with no family history of heart disease. This fact speaks in particular to the early presentation of CAD in patients with no other risk factors. Second cousins have a 1 in 23 chance of sharing a particular gene and third cousins have a 1 in 128 likelihood.
Genetic hypertension and hyperlipidemia are strong predictors of familial heart disease.[8] Hypertensive people are twice as likely to have a family history of the condition than are normotensives. Genetic hypertension is an example of a polygenic mode of inheritance that reflects cellular sodium transport defects and an abnormal response to psychogenic stress. There is indication that Pheochromocytoma, a rare cause of hypertension, may be familial as well.
Endocrine Conditions
- Diabetes mellitus type 2 (NIDDM)
- Primary hyperparathyroidism
Rheumatologic and Autoimmune Conditions
Socioeconomic Factors
Socioeconomic factors such as a shorter education and lower income (particularly in women), and living with a partner may also contribute to the risk of MI.[9] To understand epidemiological study results, it’s important to note that many factors associated with MI mediate their risk via other factors. For example, the effect of education is partially based on its effect on income and marital status.[9]
Women who use combined oral contraceptive pills have a modestly increased risk of myocardial infarction, especially in the presence of other risk factors, such as smoking.[10]
Inflammation is known to be an important step in the process of atherosclerotic plaque formation.[11] C-reactive protein (CRP) is a sensitive but non-specific marker for inflammation. Elevated CRP blood levels, especially measured with high sensitivity assays, can predict the risk of MI, as well as stroke and development of diabetes.[11] Moreover, some drugs for MI might also reduce CRP levels.[11] The use of high sensitivity CRP assays as a means of screening the general population is advised against, but it may be used optionally at the physician’s discretion, in patients who already present with other risk factors or known coronary artery disease.[12] Whether CRP plays a direct role in atherosclerosis remains uncertain.[11]
Inflammation in periodontal disease may be linked coronary heart disease, and since periodontitis is very common, this could have great consequences for public health.[13] Serological studies measuring antibody levels against typical periodontitis-causing bacteria found that such antibodies were more present in subjects with coronary heart disease.[14] Periodontitis tends to increase blood levels of CRP, fibrinogen and cytokines;[15] thus, periodontitis may mediate its effect on MI risk via other risk factors.[16] Preclinical research suggests that periodontal bacteria can promote aggregation of platelets and promote the formation of foam cells.[17][18] A role for specific periodontal bacteria has been suggested but remains to be established.[19]
Controversial Risk Factors
Baldness, hair greying, a diagonal earlobe crease[20] and possibly other skin features are independent risk factors for MI. Their role remains controversial; a common denominator of these signs and the risk of MI is supposed, possibly genetic.[21]
Risk Factor Modification
While family history, along with age and sex, is uncontrollable[3], many of the risk factors for heart disease can be eliminated by maintaining a healthy lifestyle. In fact, a person’s daily habits significantly affect the risk of heart disease due to genetic predisposition. Studies have shown that deaths can be avoided by attending to the controllable risk factors. Such risk factors include: obesity, blood pressure, cigarette smoking and plasma cholesterol.[22]
A study published in Circulation shines some light on the importance of eliminating these controllable risk factors in people with a family history of heart disease. Data demonstrated that in men with a genetic link to heart disease, an estimated 68% of the excess deaths were due to the addition of smoking, a modifiable risk factor; concluding that the risk of heart disease in men with a family history of the condition is significantly related to the additional risk factors he accumulates.
References
- ↑ Muller JE, Abela GS, Nesto RW, Tofler GH (1994). “Triggers, acute risk factors and vulnerable plaques: the lexicon of a new frontier”. J. Am. Coll. Cardiol. 23 (3): 809–13. PMID 8113568. Unknown parameter
|month=ignored (help) - ↑ “Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III)”. JAMA. 285 (19): 2486–97. 2001. PMID 11368702. Unknown parameter
|month=ignored (help) - ↑ 3.0 3.1 Wilson PW, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. (1998). “Prediction of coronary heart disease using risk factor categories” (PDF). Circulation. 97 (18): 1837–47. PMID 9603539.
- ↑ Yusuf S, Hawken S, Ounpuu S, Bautista L, Franzosi MG, Commerford P, Lang CC, Rumboldt Z, Onen CL, Lisheng L, Tanomsup S, Wangai P Jr, Razak F, Sharma AM, Anand SS; INTERHEART Study Investigators. (2005). “Obesity and the risk of myocardial infarction in 27,000 participants from 52 countries: a case-control study”. Lancet. 366 (9497): 1640–9. PMID 16271645.
- ↑ Rosamond W, Flegal K, Friday G (2007). “Heart disease and stroke statistics–2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee”. Circulation. 115 (5): e69–171. doi:10.1161/CIRCULATIONAHA.106.179918. PMID 17194875. Unknown parameter
|month=ignored (help) - ↑ Khaw KT, Barrett-Connor E (1986). “Family history of heart attack: a modifiable risk factor?”. Circulation. 74 (2): 239–44. PMID 3731415. Unknown parameter
|month=ignored (help) - ↑ http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=cm&part=A540#A556
- ↑ http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=cm&part=A540#A556
- ↑ 9.0 9.1 Nyboe J, Jensen G, Appleyard M, Schnohr P. (1989). “Risk factors for acute myocardial infarction in Copenhagen. I: Hereditary, educational and socioeconomic factors. Copenhagen City Heart Study”. Eur Heart J. 10 (10): 910–6. PMID 2598948.
- ↑ Khader YS, Rice J, John L, Abueita O. (2003). “Oral contraceptives use and the risk of myocardial infarction: a meta-analysis”. Contraception. 68 (1): 11–7. PMID 12878281.
- ↑ 11.0 11.1 11.2 11.3 Wilson AM, Ryan MC, Boyle AJ. (2006). “The novel role of C-reactive protein in cardiovascular disease: risk marker or pathogen”. Int J Cardiol. 106 (3): 291–7. PMID 16337036.
- ↑ Pearson TA, Mensah GA, Alexander RW, Anderson JL, Cannon RO 3rd, Criqui M, Fadl YY, Fortmann SP, Hong Y, Myers GL, Rifai N, Smith SC Jr, Taubert K, Tracy RP, Vinicor F; Centers for Disease Control and Prevention; American Heart Association. (2003). “Markers of inflammation and cardiovascular disease: application to clinical and public health practice: A statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association” (PDF). Circulation. 107 (3): 499–511. PMID 12551878.
- ↑ Janket SJ, Baird AE, Chuang SK, Jones JA. (2003). “Meta-analysis of periodontal disease and risk of coronary heart disease and stroke”. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 95 (5): 559–69. PMID 12738947.
- ↑ Pihlstrom BL, Michalowicz BS, Johnson NW. (2005). “Periodontal diseases”. Lancet. 366 (9499): 1809–20. PMID 16298220.
- ↑ Scannapieco FA, Bush RB, Paju S. (2003). “Associations between periodontal disease and risk for atherosclerosis, cardiovascular disease, and stroke. A systematic review”. Ann Periodontol. 8 (1): 38–53. PMID 14971247.
- ↑ D’Aiuto F, Parkar M, Nibali L, Suvan J, Lessem J, Tonetti MS. (2006). “Periodontal infections cause changes in traditional and novel cardiovascular risk factors: results from a randomized controlled clinical trial”. Am Heart J. 151 (5): 977–84. PMID 16644317.
- ↑ Lourbakos A, Yuan YP, Jenkins AL, Travis J, Andrade-Gordon P, Santulli R, Potempa J, Pike RN. (2001). “Activation of protease-activated receptors by gingipains from Porphyromonas gingivalis leads to platelet aggregation: a new trait in microbial pathogenicity” (PDF). Blood. 97 (12): 3790–7. PMID 11389018.
- ↑ Qi M, Miyakawa H, Kuramitsu HK. (2003). “Porphyromonas gingivalis induces murine macrophage foam cell formation”. Microb Pathog. 35 (6): 259–67. PMID 14580389.
- ↑ Spahr A, Klein E, Khuseyinova N, Boeckh C, Muche R, Kunze M, Rothenbacher D, Pezeshki G, Hoffmeister A, Koenig W. (2006). “Periodontal infections and coronary heart disease: role of periodontal bacteria and importance of total pathogen burden in the Coronary Event and Periodontal Disease (CORODONT) study”. Arch Intern Med. 166 (5): 554–9. PMID 16534043.
- ↑ Lichstein E, Chadda KD, Naik D, Gupta PK. (1974). “Diagonal ear-lobe crease: prevalence and implications as a coronary risk factor”. N Engl J Med. 290 (11): 615–6. PMID 4812503.
- ↑ Miric D, Fabijanic D, Giunio L, Eterovic D, Culic V, Bozic I, Hozo I. (1998). “Dermatological indicators of coronary risk: a case-control study”. Int J Cardiol. 67 (3): 251–5. PMID 9894707.
- ↑ Khaw KT, Barrett-Connor E (1986). “Family history of heart attack: a modifiable risk factor?”. Circulation. 74 (2): 239–44. PMID 3731415. Unknown parameter
|month=ignored (help)
Triggers
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Several factors have been associated with an increased risk of developing ST elevation myocardial infarction (STEMI). These factors include physical exertion, psychological stress, sexual activity, diurnal (daily) variations in cortisol and platelet aggregation and circannual (yearly) variations in lipids and infectious etiologies, exposure to pollution and or particulate matter, cocaine and ingestion of a recent fatty meal.
Nomenclature
Muller et al have developed the following nomenclature to categorize and analyze data pertaining to triggers of MI [1]:
(1) Trigger: An activity that produces short-term physiological changes that may lead directly to onset of acute CVD.
(2) Acute risk factor: A short-term physiological change, such as a surge in arterial pressure or heart rate, an increase in coagulability, or vasoconstriction, that follows a trigger and may result in disease onset.
(3) Hazard period: The time interval after trigger initiation associated with an increased risk of disease onset because of the trigger. The onset and offset times of the hazard period, which could also be designated a “vulnerable period,” may be sharply defined, as in heavy exertion, or less well defined, as with respiratory infection. The duration of the hazard period may also vary, eg from < 1 hour during heavy physical exertion to weeks or months with bereavement.
(4) Triggered acute risk prevention (TARP): Cardiovascular risk reduction that focuses on the short-term increase in risk associated with a trigger.
Putting Relative Risk of MI and Absolute Risk of MI Into Clinical Context
In the following sections, you will read that certain triggers are associated with a dramatic rise in the relative risk of having an MI (e.g. heavy exertion among patients with a sedentary lifestyle increases their risk of an MI 107 fold). These dramatic increases in relative risk, must, however, be placed in the appropriate clinical context.
It must be born in mind that while triggers are frequent events, MI or sudden death are relatively infrequent events. The risk of sudden death with exercise provides a nice example. The relative risk of sudden death within 30 minutes after >/= 6 METS of exercise goes up 16.9 fold. However, because sudden death is so infrequent, this translates into 1 sudden cardiac death for every 1.51 million episodes of heavy exertion. [2] The number of absolute events is even lower among nurses in the Nurses Health Study undertaking mild to meoderate exertion: 1 sudden death for every 36.5 hours of exertion. [3]
While the presence of triggers increases the relative risk of MI dramatically, the absolute number of MIs attributable to the trigger may be quite low.
A dramatic rise in the relative risk of a very, very, very infrequent event therefore translates clinically into a very small rise in the absolute number of events attributable to the trigger.
Physical Exertion and MI
Physical exertion, especially if the exertion is much more intense than the individual usually performs has been associated with the onset of STEMI. [4][5][6] [7] [8][2][3][9] The ONSET study demonstrated that intense exertion (defined as >/= 6 metabolic equivalents of METS) within the previous hour was associated with a 5.9 fold rise in the risk of MI [6].
Studies linking physical exertion to MI:
- The ONSET Study: Relative risk = 5.9 [6]
- The Stockholm Heart Epidemiology Program (SHEEP): Relative risk = 6.1 [7]
- The Triggers and Mechanisms of Myocardial Infarction (TRIMM) study: Relative risk = 2.1 [4]
Blizzards have often been cited as a trigger of MI, and the physical exertion of snow shoveling has frequently been cited as a contributor. [10] [11]
Impact of a sedentary lifestyle: The relative risk of MI quoted above increases dramatically among those individuals who lead a sedentary lifestyle. For those in poor physical condition, the relative risk was 107 fold higher in the ONSET study. In contrast, among those individuals who reported that they engaged in physical activity 5 days a week or more, the risk was only doubled.
Mechanism: It has been hypothesized that exertion increases blood pressure, pulse and oscillatory shear which in turn may increase the risk of plaque rupture.
Physical Exertion and Sudden Death
While the above discussion pertains to documented nonfatal MI, approximately a quarter of MI patients may die of sudden death or fatal MI before reaching the hospital. In a cohort of 21,481 male physicians in the United States who by self report who had no prior history of coronary artery disease, there was a 16.9 fold rise in the risk of sudden cardiac death within 30 minutes of intense exertion (>/= 6 METS) [2]. Similar to what has been reported with respect to the onset of MI, there was no increase in the risk of sudden death with heavy exertion among those nurses who exercised more than 2 hours per week.
Psychological Stress
Psychological stress associated with anger [12], work related stressful events [13], wartime bombing [14] [15] , earthquakes [16] and other natural disasters has been associated with an increased risk of onset of myocardial infarction.
Anger
Intense anger (fist / teeth clenched) has been associated with a risk in the risk of MI in the 2 hours following the episode in the following studies:
The psychosocial stressors that precipitated the anger were as follows:
- Argument with family members (25%)
- Conflicts at work (22%)
- Legal problems (8%)
Anxiety
If a patient is in the >75th percentile for anxiety, this increases the relative risk of MI 1.6 fold for the 2 hours following the period of anxiety.[12]
Bereavement and the Broken Heart Syndrome
Stress cardiomyopathy which is also known as Left Ventricular Apical Ballooning Syndrome, Takotsubo cardiomyopathy, or Ampulla-shaped cardiomyopathy is a cardiac syndrome characterized by a reversible transient apical ventricular dysfunction. Since the cardiomyopathy is often triggered by emotional stress, such as the death of a loved one, the condition is sometimes also referred to as the Broken Heart Syndrome. In 2006, the syndrome was renamed Stress Cardiomyopathy, and was classified as an acquired cardiomyopathy. [19]
The typical presentation of someone with takotsubo cardiomyopathy is a sudden onset of congestive heart failure or chest pain associated with EKG changes suggestive of an anterior wall acute MI. During the course of evaluation of the patient, a bulging out of the left ventricular apex with a hypercontractile base of the left ventricle is often noted. It is the hallmark bulging out of the apex of the heart with preserved function of the base that earned the syndrome its name “tako tsubo”, or octopus trap in Japan, where it was first described. Evaluation of individuals with takotsubo cardiomyopathy typically include a coronary angiogram, which does not reveal any significant blockages that would cause the left ventricular dysfunction. Provided that the individual survives their initial presentation, the left ventricular function improves within days to weeks[20]. Takotsubo cardiomyopathy is more commonly seen in post-menopausal women[21]. Often there is a history of a recent severe emotional or physical stress.[21]
Work Related Stress
Deadlines
An aggressive timeline or deadline at work has been associated with a rise in the risk of MI:
- The SHEEP study: 6 fold rise
- The ONSET study: 2.3 fold rise
Firing an Employee
The stress of firing an employee has been associated with a rise in the risk of MI:
- The ONSET study: 2.2 fold rise
Natural Disasters
Natural disasters have been associated with an increased risk of MI. The best documented association has been with earthquakes. For instance the 1994 earthquake in Los Angeles was associated with a 4 fold rise in the risk of sudden death and a 35% rise in the relative risk of a non-fatal MI. [22] [23] It is notable that the association of earthquakes with MI is variable depending upon the time of day that the earthquake occurs. The LA earthquake occurred just after 4 A.M., just when platelet aggregation may be at a peak (see below). However, the earthquake that struck San Francisco Bay in 1989 at 5 P.M. was not associated with an increased risk of MI. [24]
Wartime Stress and Missile Attacks
9/11/2001
Within 50 miles of the world trade center, there was a 49% increase in the relative risk of an MI in the 60 days following the 9/11 attack: There were 118 MIs in the 60 days after the attack versus 79 MIs in the 60 days before (p=0.01). How much of this is attributable to particulate matter versus psychological stress is not clear. [25]
Missile Attacks
The stress of missile attacks has been associated with a doubling in the risk of non fatal MI and sudden death. [26]
Sporting Events
The stress of sporting events has been associated with an increased risk of MI in a population. An example that has been cited is the 50% increase in the risk of MI or stroke among Dutch men associated with the loss of Holland to France in the 1996 European football finals. It is notable that no such rise in risk was observed among Dutch women or the French. [27] [28] The World Cup of soccer has been associated with a doubling of MI incidence. [29]
Sexual Activity
The association of sexual activity with the onset of MI may represent components of physical exertion as well as psychologic stress. In both the SHEEP and the ONSET studies, recent sexual activity increased the risk of MI by 2.5 fold [30][31]. Again, to place this relative risk into clinical context, it should be noted that only 3% of MI patients had had sexual intercourse within the past 2 hours prior to the onset of MI. It should also be noted that the increase in risk of MI with sexual activity did not differ between patients with and without a history of coronary artery disease.
The risk of MI with sexual intercourse is a frequent concern among patients who have coronary artery disease. Again, the data above indicates that recent sexual activity doubles the risk of an MI, and this may on the surface appear to be disconcerting to both a patient and healthcare professional. But again, to place this relative risk into context, the absolute risk must be taken into account. The average risk of an MI in a patient at average risk has been estimated to be about 1 chance in a million during any given hour during middle age. Sexual activity increases that risk to 2 in a million per hour for the 2 hours after sexual intercourse. If the annual risk of MI is about 1%, weekly sexual intercourse will increase this annual risk to just 1.01%. [32] As is the case with physical exertion, regular exercise (6 METS >/= 3 times per week) reduced the relative risk of MI with sexual intercourse from 3.0 to 1.2 in the ONSET study.[30]
Thus, because the risk is small, because the frequency of sexual activity is relatively small, and because the period of increased risk is short (approximately 2 hours) the absolute risk of MI associated with sexual intercourse is quite small.
Air Pollution / Fine Particulate Matter
Exposure to high levels of ambeint air pollution (exposure to fine particulate matter in the past 2 – 24 hours) has been associated with a transient elevation in the risk of myocardial infarction [33]. There is a rise in CRP and plasma viscosity following exposure to fine particulate matter and it has been speculated that the pulmonary inflammation that follows such exposure may trigger a systemic state of hypercoagulability [34][35]. Exposure to fine particulate matter has also been associated with changes in autonomic tone manifested by sinus tachycardia [36] [37], as well as a reduction in heart rate variability [38] [39] [40]. Finally, ventricular arrhythmias as manifested by firing of AICDs has been associated with exposure to fine particulate matter [41].
Antecedent Infection
Acute severe infection, such as pneumonia, can trigger myocardial infarction [42]. A more controversial link is that between Chlamydophila pneumoniae infection and atherosclerosis[43]. While this intracellular organism has been demonstrated in atherosclerotic plaques, evidence is inconclusive as to whether it can be considered a causative factor[43].Treatment with antibiotics in patients with proven atherosclerosis has not demonstrated a decreased risk of heart attacks or other coronary vascular diseases.[44]
A Heavy Meal
There have been reports of a 4 fold rise in the risk of MI following a heavy meal. [45]
This rise in risk may account for a second peak in the circadian variation in the onset of MI around 8 P.M. in the evening. The mechanism underlying the association is not clear. It has been speculated that ingestion of a heavy fatty meal may be associated with a rise in prothrombotic factors and heart rate, and a reduction in vascular reactivity. [46] [47]
Cocaine
Ingestion of cocaine has been associated with STEMI [48].
Marijuana
Marijuana use has been associated with a 4.8 fold rise in the risk of MI. [49]
Circadian Variation in the Onset of STEMI
Most MIs occur in the early morning hours when cortisol and adrenaline rise and platelets are more activated. This diurnal variation is obliterated with aspirin therapy, pointing to the putative role of platelets in the initiation of MI. [50] [51] [52] [53] [54] [55] [56]
Relative Frequency of Triggers in Association with MI
When a creful history is obtained, approximately half (48%) of MI patients will report a trigger [57]. It is notable that 13% of patients will report that there were of 2 or more triggers. The following triggers were most commonly associated with the onset of MI in the Multicenter Investigation of Limitation of Infarct Size (MILIS) study [57]:
- Emotional upset (18%)
- Moderate physical activity (14%)
- Heavy physical activity (9%)
- Lack of sleep (8%)
- Overeating (7%)
STEMI Triggers in Popular Culture

Following the sudden death of Tim Russert of NBC’s Meet the Press on June 13th 2008, many laypeople and physicians alike have asked “what are the triggers of a sudden heart attack”? Barbara Walters speculated that Tim Russert may have died from “the stress of the job”. Others were concerned about a recent weight gain and lack of sleep. This chapter reviews the literature pertaining to triggers of acute MI.
References
- ↑ Muller JE, Abela GS, Nesto RW, Tofler GH (1994). “Triggers, acute risk factors and vulnerable plaques: the lexicon of a new frontier”. J. Am. Coll. Cardiol. 23 (3): 809–13. PMID 8113568. Unknown parameter
|month=ignored (help) - ↑ 2.0 2.1 2.2 Albert CM, Mittleman MA, Chae CU, Lee IM, Hennekens CH, Manson JE (2000). “Triggering of sudden death from cardiac causes by vigorous exertion”. N. Engl. J. Med. 343 (19): 1355–61. PMID 11070099. Unknown parameter
|month=ignored (help) - ↑ 3.0 3.1 Whang W, Manson JE, Hu FB; et al. (2006). “Physical exertion, exercise, and sudden cardiac death in women”. JAMA. 295 (12): 1399–403. doi:10.1001/jama.295.12.1399. PMID 16551711. Unknown parameter
|month=ignored (help) - ↑ 4.0 4.1 Willich SN, Lewis M, Löwel H, Arntz HR, Schubert F, Schröder R (1993). “Physical exertion as a trigger of acute myocardial infarction. Triggers and Mechanisms of Myocardial Infarction Study Group”. N. Engl. J. Med. 329 (23): 1684–90. PMID 8232457. Unknown parameter
|month=ignored (help) - ↑ Wilson PW, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB (1998). “Prediction of coronary heart disease using risk factor categories”. Circulation. 97 (18): 1837–47. PMID 9603539. Unknown parameter
|month=ignored (help) - ↑ 6.0 6.1 6.2 Mittleman MA, Maclure M, Tofler GH, Sherwood JB, Goldberg RJ, Muller JE (1993). “Triggering of acute myocardial infarction by heavy physical exertion. Protection against triggering by regular exertion. Determinants of Myocardial Infarction Onset Study Investigators”. N. Engl. J. Med. 329 (23): 1677–83. PMID 8232456. Unknown parameter
|month=ignored (help) - ↑ 7.0 7.1 Hallqvist J, Möller J, Ahlbom A, Diderichsen F, Reuterwall C, de Faire U (2000). “Does heavy physical exertion trigger myocardial infarction? A case-crossover analysis nested in a population-based case-referent study”. Am. J. Epidemiol. 151 (5): 459–67. PMID 10707914. Unknown parameter
|month=ignored (help) - ↑ Giri S, Thompson PD, Kiernan FJ; et al. (1999). “Clinical and angiographic characteristics of exertion-related acute myocardial infarction”. JAMA. 282 (18): 1731–6. PMID 10568645. Unknown parameter
|month=ignored (help) - ↑ Siscovick DS, Weiss NS, Fletcher RH, Lasky T (1984). “The incidence of primary cardiac arrest during vigorous exercise”. N. Engl. J. Med. 311 (14): 874–7. PMID 6472399. Unknown parameter
|month=ignored (help) - ↑ Glass RI, Zack MM (1979). “Increase in deaths from ischaemic heart-disease after blizzards”. Lancet. 1 (8114): 485–7. PMID 85066. Unknown parameter
|month=ignored (help) - ↑ Franklin BA, Bonzheim K, Gordon S, Timmis GC (1996). “Snow shoveling: a trigger for acute myocardial infarction and sudden coronary death”. Am. J. Cardiol. 77 (10): 855–8. doi:10.1016/S0002-9149(97)89181-3. PMID 8623739. Unknown parameter
|month=ignored (help) - ↑ 12.0 12.1 12.2 Mittleman MA, Maclure M, Sherwood JB; et al. (1995). “Triggering of acute myocardial infarction onset by episodes of anger. Determinants of Myocardial Infarction Onset Study Investigators”. Circulation. 92 (7): 1720–5. PMID 7671353. Unknown parameter
|month=ignored (help) - ↑ Möller J, Theorell T, de Faire U, Ahlbom A, Hallqvist J (2005). “Work related stressful life events and the risk of myocardial infarction. Case-control and case-crossover analyses within the Stockholm heart epidemiology programme (SHEEP)”. J Epidemiol Community Health. 59 (1): 23–30. doi:10.1136/jech.2003.019349. PMC 1763356. PMID 15598722. Unknown parameter
|month=ignored (help) - ↑ Johnston SC, Sorel ME, Sidney S (2002). “Effects of the September 11th attacks on urgent and emergent medical evaluations in a Northern California managed care plan”. Am. J. Med. 113 (7): 556–62. PMID 12459401. Unknown parameter
|month=ignored (help) - ↑ Vukovic DS, Krotin ME, Babic MM, Zivanovic BM (2005). “Anxiety level and responses to stress caused by air raids among patients with ischemic heart disease”. Prehosp Disaster Med. 20 (4): 249–52. PMID 16128473.
- ↑ Trichopoulos D, Katsouyanni K, Zavitsanos X, Tzonou A, Dalla-Vorgia P (1983). “Psychological stress and fatal heart attack: the Athens (1981) earthquake natural experiment”. Lancet. 1 (8322): 441–4. PMID 6131167. Unknown parameter
|month=ignored (help) - ↑ Möller J, Hallqvist J, Diderichsen F, Theorell T, Reuterwall C, Ahlbom A (1999). “Do episodes of anger trigger myocardial infarction? A case-crossover analysis in the Stockholm Heart Epidemiology Program (SHEEP)”. Psychosom Med. 61 (6): 842–9. PMID 10593637.
- ↑ Koton S, Tanne D, Bornstein NM, Green MS (2004). “Triggering risk factors for ischemic stroke: a case-crossover study”. Neurology. 63 (11): 2006–10. PMID 15596741. Unknown parameter
|month=ignored (help) - ↑ Maron BJ, Towbin JA, Thiene G; et al. (2006). “Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention”. Circulation. 113 (14): 1807–16. doi:10.1161/CIRCULATIONAHA.106.174287. PMID 16567565.
- ↑ Akashi YJ, Barbaro G, Sakurai T, Nakazawa K, Miyake F (2007). “Cardiac autonomic imbalance in patients with reversible ventricular dysfunction takotsubo cardiomyopathy”. QJM. 100 (6): 335–43. doi:10.1093/qjmed/hcm028. PMID 17483198.
- ↑ 21.0 21.1 Azzarelli S, Galassi AR, Amico F, Giacoppo M, Argentino V, Tomasello SD, Tamburino C, Fiscella A. (2006). “Clinical features of transient left ventricular apical ballooning”. Am J Cardiol. 98 (9): 1273–6. PMID 17056345.
- ↑ Leor J, Kloner RA (1996). “The Northridge earthquake as a trigger for acute myocardial infarction”. Am. J. Cardiol. 77 (14): 1230–2. PMID 8651102. Unknown parameter
|month=ignored (help) - ↑ Leor J, Poole WK, Kloner RA (1996). “Sudden cardiac death triggered by an earthquake”. N. Engl. J. Med. 334 (7): 413–9. PMID 8552142. Unknown parameter
|month=ignored (help) - ↑ Brown DL (1999). “Disparate effects of the 1989 Loma Prieta and 1994 Northridge earthquakes on hospital admissions for acute myocardial infarction: importance of superimposition of triggers”. Am. Heart J. 137 (5): 830–6. PMID 10220631. Unknown parameter
|month=ignored (help) - ↑ Allegra JR, Mostashari F, Rothman J, Milano P, Cochrane DG (2005). “Cardiac events in New Jersey after the September 11, 2001, terrorist attack”. J Urban Health. 82 (3): 358–63. doi:10.1093/jurban/jti087. PMID 16000653. Unknown parameter
|month=ignored (help) - ↑ Meisel SR, Kutz I, Dayan KI; et al. (1991). “Effect of Iraqi missile war on incidence of acute myocardial infarction and sudden death in Israeli civilians”. Lancet. 338 (8768): 660–1. PMID 1679475. Unknown parameter
|month=ignored (help) - ↑ Witte DR, Bots ML, Hoes AW, Grobbee DE (2000). “Cardiovascular mortality in Dutch men during 1996 European football championship: longitudinal population study”. BMJ. 321 (7276): 1552–4. PMC 27557. PMID 11124170.
- ↑ Toubiana L, Hanslik T, Letrilliart L (2001). “French cardiovascular mortality did not increase during 1996 European football championship”. BMJ. 322 (7297): 1306. PMC 1120392. PMID 11403063. Unknown parameter
|month=ignored (help) - ↑ N Engl J Med 2008; 358:475-483.
- ↑ 30.0 30.1 Muller JE, Mittleman MA, Maclure M, Sherwood JB, Tofler GH (1996). “Triggering myocardial infarction by sexual activity. Low absolute risk and prevention by regular physical exertion. Determinants of Myocardial Infarction Onset Study Investigators”. JAMA. 275 (18): 1405–9. PMID 8618365. Unknown parameter
|month=ignored (help) - ↑ Möller J, Ahlbom A, Hulting J; et al. (2001). “Sexual activity as a trigger of myocardial infarction. A case-crossover analysis in the Stockholm Heart Epidemiology Programme (SHEEP)”. Heart. 86 (4): 387–90. PMC 1729949. PMID 11559674. Unknown parameter
|month=ignored (help) - ↑ Tofler GH, Muller JE (2006). “Triggering of acute cardiovascular disease and potential preventive strategies”. Circulation. 114 (17): 1863–72. doi:10.1161/CIRCULATIONAHA.105.596189. PMID 17060396. Unknown parameter
|month=ignored (help) - ↑ Peters A, Dockery DW, Muller JE, Mittleman MA (2001). “Increased particulate air pollution and the triggering of myocardial infarction”. Circulation. 103 (23): 2810–5. PMID 11401937. Unknown parameter
|month=ignored (help) - ↑ Peters A, Döring A, Wichmann HE, Koenig W (1997). “Increased plasma viscosity during an air pollution episode: a link to mortality?”. Lancet. 349 (9065): 1582–7. doi:10.1016/S0140-6736(97)01211-7. PMID 9174559. Unknown parameter
|month=ignored (help) - ↑ Peters A, Fröhlich M, Döring A; et al. (2001). “Particulate air pollution is associated with an acute phase response in men; results from the MONICA-Augsburg Study”. Eur. Heart J. 22 (14): 1198–204. doi:10.1053/euhj.2000.2483. PMID 11440492. Unknown parameter
|month=ignored (help) - ↑ Pope CA3rd, Dockery DW, Kanner RE, Villegas GM, Schwartz J (1999). “Oxygen saturation, pulse rate, and particulate air pollution: A daily time-series panel study”. Am. J. Respir. Crit. Care Med. 159 (2): 365–72. PMID 9927345. Unknown parameter
|month=ignored (help) - ↑ Peters A, Perz S, Döring A, Stieber J, Koenig W, Wichmann HE (1999). “Increases in heart rate during an air pollution episode”. Am. J. Epidemiol. 150 (10): 1094–8. PMID 10568625. Unknown parameter
|month=ignored (help) - ↑ Liao D, Creason J, Shy C, Williams R, Watts R, Zweidinger R (1999). “Daily variation of particulate air pollution and poor cardiac autonomic control in the elderly”. Environ. Health Perspect. 107 (7): 521–5. PMC 1566669. PMID 10378998. Unknown parameter
|month=ignored (help) - ↑ Pope CA, Verrier RL, Lovett EG; et al. (1999). “Heart rate variability associated with particulate air pollution”. Am. Heart J. 138 (5 Pt 1): 890–9. PMID 10539820. Unknown parameter
|month=ignored (help) - ↑ Gold DR, Litonjua A, Schwartz J; et al. (2000). “Ambient pollution and heart rate variability”. Circulation. 101 (11): 1267–73. PMID 10725286. Unknown parameter
|month=ignored (help) - ↑ Peters A, Liu E, Verrier RL; et al. (2000). “Air pollution and incidence of cardiac arrhythmia”. Epidemiology. 11 (1): 11–7. PMID 10615837. Unknown parameter
|month=ignored (help) - ↑ Smeeth L, Thomas SL, Hall AJ, Hubbard R, Farrington P, Vallance P (2004). “Risk of myocardial infarction and stroke after acute infection or vaccination”. N. Engl. J. Med. 351 (25): 2611–8. doi:10.1056/NEJMoa041747. PMID 15602021. Unknown parameter
|month=ignored (help) - ↑ 43.0 43.1 Saikku P, Leinonen M, Tenkanen L, Linnanmaki E, Ekman MR, Manninen V, Manttari M, Frick MH, Huttunen JK. (1992). “Chronic Chlamydia pneumoniae infection as a risk factor for coronary heart disease in the Helsinki Heart Study”. Ann Intern Med. 116 (4): 273–8. PMID 1733381.
- ↑ Andraws R, Berger JS, Brown DL. (2005). “Effects of antibiotic therapy on outcomes of patients with coronary artery disease: a meta-analysis of randomized controlled trials”. JAMA. 293 (21): 2641–7. PMID 15928286.
- ↑ Lipovetzky N, Hod H, Roth A, Kishon Y, Sclarovsky S, Green MS (2004). “Heavy meals as a trigger for a first event of the acute coronary syndrome: a case-crossover study”. Isr. Med. Assoc. J. 6 (12): 728–31. PMID 15609883. Unknown parameter
|month=ignored (help) - ↑ Miller GJ, Martin JC, Mitropoulos KA; et al. (1991). “Plasma factor VII is activated by postprandial triglyceridaemia, irrespective of dietary fat composition”. Atherosclerosis. 86 (2–3): 163–71. PMID 1872911. Unknown parameter
|month=ignored (help) - ↑ Vogel RA, Corretti MC, Plotnick GD (1997). “Effect of a single high-fat meal on endothelial function in healthy subjects”. Am. J. Cardiol. 79 (3): 350–4. PMID 9036757. Unknown parameter
|month=ignored (help) - ↑ Mittleman MA, Mintzer D, Maclure M, Tofler GH, Sherwood JB, Muller JE (1999). “Triggering of myocardial infarction by cocaine”. Circulation. 99 (21): 2737–41. PMID 10351966. Unknown parameter
|month=ignored (help) - ↑ Mittleman MA, Lewis RA, Maclure M, Sherwood JB, Muller JE (2001). “Triggering myocardial infarction by marijuana”. Circulation. 103 (23): 2805–9. PMID 11401936. Unknown parameter
|month=ignored (help) - ↑ Muller JE, Stone PH, Turi ZG; et al. (1985). “Circadian variation in the frequency of onset of acute myocardial infarction”. N. Engl. J. Med. 313 (21): 1315–22. PMID 2865677. Unknown parameter
|month=ignored (help) - ↑ Willich SN, Levy D, Rocco MB, Tofler GH, Stone PH, Muller JE (1987). “Circadian variation in the incidence of sudden cardiac death in the Framingham Heart Study population”. Am. J. Cardiol. 60 (10): 801–6. PMID 3661393. Unknown parameter
|month=ignored (help) - ↑ Marler JR, Price TR, Clark GL; et al. (1989). “Morning increase in onset of ischemic stroke”. Stroke. 20 (4): 473–6. PMID 2648651. Unknown parameter
|month=ignored (help) - ↑ Behar S, Halabi M, Reicher-Reiss H; et al. (1993). “Circadian variation and possible external triggers of onset of myocardial infarction. SPRINT Study Group”. Am. J. Med. 94 (4): 395–400. PMID 8475932. Unknown parameter
|month=ignored (help) - ↑ Tofler GH, Muller JE, Stone PH; et al. (1992). “Modifiers of timing and possible triggers of acute myocardial infarction in the Thrombolysis in Myocardial Infarction Phase II (TIMI II) Study Group”. J. Am. Coll. Cardiol. 20 (5): 1049–55. PMID 1401601. Unknown parameter
|month=ignored (help) - ↑ Ridker PM, Manson JE, Buring JE, Muller JE, Hennekens CH (1990). “Circadian variation of acute myocardial infarction and the effect of low-dose aspirin in a randomized trial of physicians”. Circulation. 82 (3): 897–902. PMID 2203556. Unknown parameter
|month=ignored (help) - ↑ Parker JD, Testa MA, Jimenez AH; et al. (1994). “Morning increase in ambulatory ischemia in patients with stable coronary artery disease. Importance of physical activity and increased cardiac demand”. Circulation. 89 (2): 604–14. PMID 8313548. Unknown parameter
|month=ignored (help) - ↑ 57.0 57.1 Tofler GH, Stone PH, Maclure M; et al. (1990). “Analysis of possible triggers of acute myocardial infarction (the MILIS study)”. Am. J. Cardiol. 66 (1): 22–7. PMID 2193495. Unknown parameter
|month=ignored (help)
Natural History and Complications
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Without treatment, ST elevation myocardial infarction can prove fatal. Complications of ST elevation MI are divided into the following categories: ischemic, mechanical, arrythmic, embolic, and pericarditis. The prognosis for patients with myocardial infarction varies greatly depending upon simple demographic variables like age, infarct artery location, the presence of signs and symptoms of heart failure on presentation, the symptom to door time, and comorbidities that are present. Several risk stratification tools have been developed to predict a patient’s mortality. Most of these risk scores are based upon clinical data obtained at the time of admission rather than at the time of discharge.
Complications
Ischemic Complications
Reinfarction or reocclusion of the infarct-related artery is associated with a doubling of mortality.[1] Unfortunately, it is difficult to predict who will reinfarct following fibrinolytic therapy. Among patients undergoing primary PCI, bivalirudin monotherapy has been associated with stent thrombosis in the HORIZONS-AMI and EUROMAX trials.[2][3] Aggressive antiplatelet and antithrombotic therapy minimizes the risk of reinfarction.
Mechanical Complications
A new murmur in patients with ST elevation myocardial infarction should raise an immediate concern of mechanical complicaitons such as papillary muscle rupture, septal rupture, and free-wall rupture which portend a dismal prognosis and may be differentiated on the basis of physical and echocardiographic findings or hemodynamic profiles. Other mechanical sequelae include true or false ventricular aneurysm, dynamic left ventricular outflow tract obstruction, cardiogenic shock, and heart failure.
- A true left ventricular aneurysm is an outpouching formed by a stretched, thinned-out myocardial scar. Patients with transmural infarction and patients who do not receive reperfusion therapy are at increased risk. LV aneurysm may manifest acutely as low-output cardiogenic shock or chronically as heart failure or thromboembolism in the presence of mural thrombus. A large, diffuse point of maximal impulse and S3 gallops may be evident on physical examination. A chest radiograph may demonstrate a localized bulging segment in the cardiac silhouette. Dyskinetic or paradoxical motions of the aneurysmal segment may be detected by echocardiography or ventriculography. True aneurysm connects with the LV cavity by a wide neck and is less susceptible to rupture than a false aneurysm. ACE inhibitor and vasodilator are used in the mangement of chronic heart failure associated with ventricular aneurysm. Anticoagulant is indicated in the presence of mural thrombus. Sustained ventricular arrhythmia from an aneurysm may require defibrillator placement. Surgical resection may be considered in selected cases with refractory symptoms.
- In contrast to the true aneurysm which contains viable myocardium in its wall, pseudoaneurysm lacks the myocardial elements and is formed by adherent pericardium and organized hematoma. Unlike true ventricular aneurysm, pseudoaneurysm communicates with the cavity of the left ventricle through a narrow neck and is more prone to rupture. Pseudoaneurysm may partially reduce stroke volume similar to a true aneurysm. Surgery is recommended for all patients regardless of symptoms or the size of pseudoaneurysm in light of a high risk for spontaneous rupture and sudden death.
- Papillary muscle rupture is characterized by symptoms of acute severe mitral regurgitation and pulmonary edema and should be suspected in STEMI patients with a new soft holosystolic murmur at the apex. Posterior papillary muscle rupture, as occurs in inferior MI, is more common than anterior papillary muscle rupture which may be a complication of anterior or lateral MI. Posterior papillary muscle is considered more susceptible to ischemic rupture due to its singular blood supply from the posterior descending artery. In contradistinction to the posterior papillary muscle, the anterior papillary muscle receives a dual blood supply from the left anterior descending artery and the circumflex artery.[4] Urgent transthoracic echocardiography should be obtained to establish a definite diagnosis. Nitroglycerin or nitroprusside may be used to temporize the patient if systolic blood pressure is above 90 mm Hg. If the patient cannot tolerate vasodilator due to rapid hemodynamic deterioration, intra-aortic balloon counterpulsation should be instituted as a bridging therapy until emergency mitral valve replacement can be performed.
- Patients with septal rupture frequently report chest pain, shortness of breath, and symptoms of low-output cardiogenic shock. Key physical findings include a harsh, loud holosystolic murmur best heard at the lower left sternal border, palpable thrill at the right precordium, S3 gallops, and accentuation of pulmonic component of the second heart sound. Color Doppler echocardiography is useful for determining the location and size of the defect and detecting left-to-right shunt and right ventricular overload. Septal rupture should be managed by temporary stabilization with intra-aortic balloon counterpulsation followed by intravenous vasodilator and early surgical closure.
- Free-wall rupture usually leads to hemopericardium and abrupt circulatory collapse. Clinical manifestations range from anginal, pleuritic, or pericardial chest discomfort to catastrophic symptoms of cardiogenic shock, cardiac tamponade, and sudden death. Echocardiography is useful for the diagnosis and emergency pericardiocentesis may be indicated for cardiac tamponade. Survival depends primarily on early recognition and prompt surgical repair.
| Feature | Mechanical Complication of ST Elevation Myocardial Infarction | ||
| Papillary Muscle Rupture | Ventricular Septal Rupture | Free-Wall Rupture | |
| Physical Findings | Soft pansystolic murmur best audible at the apex with radiation to the axilla, ⊖ precordial thrill, variable signs of RV overload | Harsh pansystolic murmur best audible at the lower left sternal border with radiation to the right parastenal area, ⊕ precordial thrill, S3, accentuated second heart sound | Diminished heart sounds, pericardial rub, to-and-fro murmur, jugular venous distention, pulsus paradoxus |
| Echocardiographic Findings | Hypercontractile LV, torn papillary muscle or chordae tendineae, flail leaflet, severe mitral regurgitation | Left-to-right shunt at the ventricular level, pattern of RV overload | Layered high-acoustic echoes within the pericardium, pericardial effusion, RA and RV diastolic collapse, dilated inferior vena cava, marked respiratory variations in mitral and tricuspid inflow |
| Hemodynamic Profiles | No oxygen saturation gradient from the RA to RV, large V waves in pulmonary artery and capillary wedge tracings, high pulmonary-capillary wedge pressure | Step-up in oxygen saturation between the RA and RV (or PA), large V waves | Equalization of diastolic pressures among the cardiac chambers |
Conduction Abnormalities
Atrial Fibrillation
New onset atrial fibrillation in the setting of STEMI is associated with a very poor prognosis [6]. New onset atrial fibrillation is likely a marker for left atrial distension due to impaired left ventricular compliance.
Arrhythmic Complications
Embolic Complications
Pericarditis
2013 Revised ACCF/AHA Guidelines for the Management of ST-Elevation Myocardial Infarction (DO NOT EDIT)[7]
Assessment of Left Ventricular Function (DO NOT EDIT)[7]
| Class I |
| “1. LV ejection fraction should be measured in all patients with STEMI. (Level of Evidence: C)” |
Sources
- 2013 Revised ACCF/AHA Guidelines for the Management of ST-Elevation Myocardial Infarction [7]
References
- ↑ Gibson CM, Karha J, Murphy SA, James D, Morrow DA, Cannon CP; et al. (2003). “Early and long-term clinical outcomes associated with reinfarction following fibrinolytic administration in the Thrombolysis in Myocardial Infarction trials”. J Am Coll Cardiol. 42 (1): 7–16. PMID 12849652.
- ↑ Dangas GD, Caixeta A, Mehran R, Parise H, Lansky AJ, Cristea E; et al. (2011). “Frequency and predictors of stent thrombosis after percutaneous coronary intervention in acute myocardial infarction”. Circulation. 123 (16): 1745–56. doi:10.1161/CIRCULATIONAHA.110.981688. PMID 21482968.
- ↑ Clemmensen, Peter; Hof, Arnoud van’t; Deliargyris, Efthymios N.; Coste, Pierre; ten Berg, Jurrien; Cavallini, Claudio; Hamon, Martial; Dudek, Dariusz; Zeymer, Uwe; Tabone, Xavier; Clayton, Tim; Bernstein, Debra; Prats, Jayne (2014). “PREDICTORS ASSOCIATED WITH ACUTE STENT THROMBOSIS AFTER PRIMARY PCI: THE EUROMAX TRIAL”. Journal of the American College of Cardiology. 63 (12): A27. doi:10.1016/S0735-1097(14)60027-9. ISSN 0735-1097.
- ↑ Voci P, Bilotta F, Caretta Q, Mercanti C, Marino B (1995). “Papillary muscle perfusion pattern. A hypothesis for ischemic papillary muscle dysfunction”. Circulation. 91 (6): 1714–8. PMID 7882478.
- ↑ Birnbaum Y, Fishbein MC, Blanche C, Siegel RJ (2002). “Ventricular septal rupture after acute myocardial infarction”. N Engl J Med. 347 (18): 1426–32. doi:10.1056/NEJMra020228. PMID 12409546.
- ↑ GUSTO 1 trial
- ↑ 7.0 7.1 7.2 O’Gara PT, Kushner FG, Ascheim DD; et al. (2012). “2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction: Executive Summary: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines”. Circulation. doi:10.1161/CIR.0b013e3182742c84. PMID 23247303. Unknown parameter
|month=ignored (help)
Risk Stratification and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Five variables explain 90% of the prognosis in STEMI: Advanced age,sinus tachycardia, reduced systolic blood pressure, heart failure or Killip class of two or greater, and anterior myocardial infarction location. Two main risk-stratification scores are used when assessing a patient with ST elevation MI and acute coronary syndromes; the TIMI Risk Score (for STEMI), and the GRACE risk score (for acute coronary syndrome.
Prognosis
Factors Associated with a Poor Prognosis in STEMI
While we as physicians often labor under the impression that we can dramatically change a patient’s prognosis, it is noteworthy that 90% of the predictive information regarding 30 day mortality is contained in the following 5 baseline variables that can be modified to only a limited degree: [1]
- Advanced age
- Sinus tachycardia
- Reduced systolic blood pressure
- Heart failure or Killip class of two or greater
- Anterior myocardial infarction location
Sinus tachycardia, hypotension, Killip class, and anterior MI are all essentially markers of poor pump function on admission. These risk factors for 30 day mortality have been well validated in a multivariate analysis of 41,020 patients in the GUSTO-I trial. Advanced age was the most significant factor associated with higher 30-day mortality. The rate was only 1.1% in the youngest decile (< 45 years) and climbed to 20.5% in patients > 75 (adjusted chi 2 = 717, P < .0001). Other variables most closely associated with an increased risk of mortality were lower systolic blood pressure at randomization (chi 2 = 550, P < .0001), higher Killip class (chi 2 = 350, P < .0001), elevated heart rate (chi 2 = 275, P < .0001), and the presence of an anterior infarction (chi 2 = 143, P < .0001). When taken together, these five baseline characteristics contained 90% of the prognostic information. Other significant though less important factors included previous myocardial infarction, height, time to treatment, diabetes, weight, smoking status, type of thrombolytic, previous bypass surgery, hypertension, and prior cerebrovascular disease. When these variables were combined, a validated model was created which stratified patients according to their mortality risk and accurately estimated the likelihood of death.
Other Prognostic Variables not Identified in GUSTO I
Other risk factors include, serum creatinine concentration [2], and peripheral vascular disease.[3][4]
Left Ventricular Function as a Risk Stratifier
Assessment of left ventricular ejection fraction may increase the predictive power of some risk stratification models.[5] The prognostic importance of Q-waves is debated.[6] Prognosis is significantly worsened if a mechanical complication (papillary muscle rupture, myocardial free wall rupture, and so on) were to occur.
There is evidence that case fatality of myocardial infarction has been improving over the years in all ethnicities.[7]
The Smokers Paradox
Interestingly, although tobacco abuse is a risk factor for CAD and STEMI, smoking is associated with a lower risk of mortality among patients who present with STEMI [8][9] This is due, at least in part, to the finding that smokers who present with STEMI are, on average, at least a decade younger than non-smokers. Smokers more often have involvement of the right coronary artery rather than the left anterior descending artery as well. Smokers paradoxically have better myocardial perfusion following reperfusion therapy than non smokers [10].
The TIMI Risk Score
The Thrombolysis in Myocardial Infarction TIMI Risk Score [11] and TIMI Risk Index [12] are two prognostic indices that have been validated in clinical trials and epidemiologic studies to predict 30-day mortality among patients with STEMI.
The TIMI risk score for STEMI was created from simple arithmetic sum of independent predictors of mortality weighted according to the adjusted odds ratios from logistic regression analysis. The risk score was derived from 14,114 patients enrolled in the Intravenous nPA for Treatment of Infarcting Myocardium Early II trial (TIME II). The TIMI risk score was subsequently validated in an unselected heterogeneous community population through the National Registry of Myocardial Infarction (NRMI) 3 & 4. The TIMI Risk Score incorporates eight clinical variables (age, systolic blood pressure [SBP], heart rate [HR], Killip class, anterior ST elevation or left bundle branch block on electrocardiogram, diabetes mellitus, history of hypertension or angina, low weight and time to treatment >4 hours) and assigns them a point value based on their odds ratio for mortality.
The TIMI Risk Score was developed and validated in clinical trials of fibrinolytic therapy, but it has also been reported to be prognostic in community-based real-world registries [13] as well as elderly patients [14]. The TIMI risk score for TIMI is calculated by adding the numbers assigned to the different criteria shown below. The total possible score is 14.[11]
| Risk Factor | Points |
| Demographic data and medical history | |
| Age ≥75 years | 3 |
| Age 65–74 years | 2 |
| History of diabetes mellitus or hypertension or angina | 1 |
| Physical examination | |
| Systolic blood pressure <100 | 3 |
| Heart rate >100 | 2 |
| Killip class II–IV | 2 |
| Weight <67 kg | 1 |
| Evaluation at presentation | |
| Anterior ST elevation or left bundle branch block | 1 |
| Time to therapy >4 hours | 1 |
Interpretation of TIMI Risk Score for STEMI
| Score | 30 Day Mortality (%)[11] |
| 0 | 0.8% |
| 1 | 1.6% |
| 2 | 2.2% |
| 3 | 4.4% |
| 4 | 7.3% |
| 5 | 12.4% |
| 6 | 16.1% |
| 7 | 23.4% |
| 8 | 26.8% |
| >8 | 35.9% |
The TIMI Risk Index incorporates age, HR and SBP (HR x [age/10] x 2/SBP), and has been validated in unselected patients [15], registries [16] and population-based cohorts [17]
GRACE Risk Score
- The Global Registry of Acute Coronary Events (GRACE) risk score for ACS:
- The GRACE risk score was created from a multivariable logistic regression model using ACS patients enrolled in the GRACE registry (N=11389).
- The GRACE risk score was validated using subsequent cohort of patients enrolled in GRACE (n=3972) and the Global Use of Strategies to Open Occluded Coronary Arteries IIb (GUSTO-IIb) trial (n=12142).
Calculation of Grace Risk Score for In-Hospital Mortality
The total GRACE risk score is calculated by adding the points assigned to the different variable shown below. The highest total possible score 363.[18]
| Variable | Points |
| Age (years) | |
| <30 | 0 |
| 30–39 | 8 |
| 40–49 | 25 |
| 50–59 | 41 |
| 60–69 | 58 |
| 70–79 | 75 |
| 80–89 | 91 |
| ≥90 | 100 |
| Heart rate (beats/minute) | |
| <50 | 0 |
| 50–69 | 3 |
| 70–89 | 9 |
| 90–109 | 15 |
| 110–149 | 24 |
| 150–199 | 38 |
| ≥200 | 46 |
| Systolic blood pressure (mmHg) | |
| <80 | 58 |
| 80–99 | 53 |
| 100–119 | 43 |
| 120–139 | 34 |
| 140–159 | 24 |
| 160–199 | 10 |
| ≥200 | 0 |
| Initial serum creatinine (mg/dL) | |
| 0.0–0.39 | 1 |
| 0.4–0.79 | 4 |
| 0.8–1.19 | 7 |
| 1.2–1.59 | 10 |
| 1.6–1.99 | 13 |
| 0.2–3.99 | 21 |
| ≥4 | 28 |
| Killip class | |
| I | 0 |
| II | 20 |
| III | 39 |
| IV | 59 |
| Cardiac arrest at admission | 39 |
| Elevated cardiac markers | 14 |
| ST segment deviation | 28 |
Interpretation of Grace Risk Score for In-Hospital Mortality
A nomogram for the probability in-hospital mortality has been developed based on the GRACE score. Shown below is the probability of in-hospital mortality by the corresponding GRACE score value.[18]
| Score | Probability of in-hospital mortality (%) |
| ≤60 | ≤0.2% |
| 70 | 0.3% |
| 80 | 0.4% |
| 90 | 0.6% |
| 100 | 0.8% |
| 110 | 1.1% |
| 120 | 1.6% |
| 130 | 2.1% |
| 140 | 2.9% |
| 150 | 3.9% |
| 160 | 5.4% |
| 170 | 7.3% |
| 180 | 9.8% |
| 190 | 13% |
| 200 | 18% |
| 210 | 23% |
| 220 | 29% |
| 230 | 36% |
| 240 | 44% |
| ≥250 | ≥52% |
Grace Risk Score for All-Cause Mortality From Discharge to 6 Months
Calculation of the GRACE Score for All-Cause Mortality From Discharge to 6 Months
The total GRACE risk score is calculated by adding the points assigned to the different variable shown below.[19] The highest total possible score 263.
| Variable | Points |
| Age (years) | |
| <40 | 0 |
| 40–49 | 18 |
| 50–59 | 36 |
| 60–69 | 55 |
| 70–79 | 73 |
| 80–89 | 91 |
| ≥90 | 100 |
| Heart rate (beats/minute) | |
| ≤49.9 | 0 |
| 50–69.9 | 3 |
| 70–89.9 | 9 |
| 90–109.9 | 14 |
| 110–149.9 | 23 |
| 150–199.9 | 35 |
| ≥200 | 43 |
| Systolic blood pressure (mmHg) | |
| <80 | 24 |
| 80–99.9 | 22 |
| 100–119.9 | 18 |
| 120–139.9 | 14 |
| 140–159.9 | 10 |
| 160–199.9 | 4 |
| ≥200 | 0 |
| Initial serum creatinine (mg/dL) | |
| 0.0–0.39 | 1 |
| 0.4–0.79 | 3 |
| 0.8–1.19 | 5 |
| 1.2–1.59 | 7 |
| 1.6–1.99 | 9 |
| 0.2–3.99 | 15 |
| ≥4 | 20 |
| History of congestive heart failure | 24 |
| History of myocardial infarction | 12 |
| Elevated cardiac markers | 15 |
| ST segment depression | 11 |
| No in-hospital PCI | 14 |
References
- ↑ Lee KL, Woodlief LH, Topol EJ; et al. (1995). “Predictors of 30-day mortality in the era of reperfusion for acute myocardial infarction. Results from an international trial of 41,021 patients. GUSTO-I Investigators”. Circulation. 91 (6): 1659–68. PMID 7882472. Unknown parameter
|month=ignored (help) - ↑ Gibson CM, Pinto DS, Murphy SA; et al. (2003). “Association of creatinine and creatinine clearance on presentation in acute myocardial infarction with subsequent mortality”. J. Am. Coll. Cardiol. 42 (9): 1535–43. PMID 14607434. Unknown parameter
|month=ignored (help) - ↑ Fox KA, Dabbous OH, Goldberg RJ; et al. (2006). “Prediction of risk of death and myocardial infarction in the six months after presentation with acute coronary syndrome: prospective multinational observational study (GRACE)”. BMJ. 333 (7578): 1091. doi:10.1136/bmj.38985.646481.55. PMC 1661748. PMID 17032691. Unknown parameter
|month=ignored (help) - ↑ Weir RA, McMurray JJ, Velazquez EJ. (2006). “Epidemiology of heart failure and left ventricular systolic dysfunction after acute myocardial infarction: prevalence, clinical characteristics, and prognostic importance”. Am J Cardiol. 97 (10A): 13F–25F. PMID 16698331.
- ↑ Bosch X, Theroux P. (2005). “Left ventricular ejection fraction to predict early mortality in patients with non-ST-segment elevation acute coronary syndromes”. Am Heart J. 150 (2): 215–20. PMID 16086920.
- ↑ Nicod P, Gilpin E, Dittrich H, Polikar R, Hjalmarson A, Blacky A, Henning H, Ross J (1989). “Short- and long-term clinical outcome after Q wave and non-Q wave myocardial infarction in a large patient population”. Circulation. 79 (3): 528–36. PMID 2645061.
- ↑ Liew R, Sulfi S, Ranjadayalan K, Cooper J, Timmis AD. (2006). “Declining case fatality rates for acute myocardial infarction in South Asian and white patients in the past 15 years”. Heart. 92 (8): 1030–4. PMID 16387823.
- ↑ Gourlay SG, Rundle AC, Barron HV (2002). “Smoking and mortality following acute myocardial infarction: results from the National Registry of Myocardial Infarction 2 (NRMI 2)”. Nicotine Tob. Res. 4 (1): 101–7. doi:10.1080/14622200110103205. PMID 11906686. Unknown parameter
|month=ignored (help) - ↑ Weisz G, Cox DA, Garcia E; et al. (2005). “Impact of smoking status on outcomes of primary coronary intervention for acute myocardial infarction–the smoker’s paradox revisited”. Am. Heart J. 150 (2): 358–64. doi:10.1016/j.ahj.2004.01.032. PMID 16086943. Unknown parameter
|month=ignored (help) - ↑ Kirtane AJ, Martinezclark P, Rahman AM; et al. (2005). “Association of smoking with improved myocardial perfusion and the angiographic characterization of myocardial tissue perfusion after fibrinolytic therapy for ST-segment elevation myocardial infarction”. J. Am. Coll. Cardiol. 45 (2): 321–3. doi:10.1016/j.jacc.2004.10.018. PMID 15653037. Unknown parameter
|month=ignored (help) - ↑ 11.0 11.1 11.2 Morrow DA, Antman EM, Charlesworth A; et al. (2000). “TIMI risk score for ST-elevation myocardial infarction: A convenient, bedside, clinical score for risk assessment at presentation: An intravenous nPA for treatment of infarcting myocardium early II trial substudy”. Circulation. 102 (17): 2031–7. PMID 11044416. Unknown parameter
|month=ignored (help) - ↑ Morrow DA, Antman EM, Giugliano RP; et al. (2001). “A simple risk index for rapid initial triage of patients with ST-elevation myocardial infarction: an InTIME II substudy”. Lancet. 358 (9293): 1571–5. doi:10.1016/S0140-6736(01)06649-1. PMID 11716882. Unknown parameter
|month=ignored (help) - ↑ Morrow DA, Antman EM, Parsons L; et al. (2001). “Application of the TIMI risk score for ST-elevation MI in the National Registry of Myocardial Infarction 3”. JAMA. 286 (11): 1356–9. PMID 11560541. Unknown parameter
|month=ignored (help) - ↑ Rathore SS, Weinfurt KP, Foody JM, Krumholz HM (2005). “Performance of the Thrombolysis in Myocardial Infarction (TIMI) ST-elevation myocardial infarction risk score in a national cohort of elderly patients”. Am. Heart J. 150 (3): 402–10. doi:10.1016/j.ahj.2005.03.069. PMID 16169316. Unknown parameter
|month=ignored (help) - ↑ Ilkhanoff L, O’Donnell CJ, Camargo CA, O’Halloran TD, Giugliano RP, Lloyd-Jones DM (2005). “Usefulness of the TIMI Risk Index in predicting short- and long-term mortality in patients with acute coronary syndromes”. Am. J. Cardiol. 96 (6): 773–7. doi:10.1016/j.amjcard.2005.04.059. PMID 16169358. Unknown parameter
|month=ignored (help) - ↑ Wiviott SD, Morrow DA, Frederick PD; et al. (2004). “Performance of the thrombolysis in myocardial infarction risk index in the National Registry of Myocardial Infarction-3 and -4: a simple index that predicts mortality in ST-segment elevation myocardial infarction”. J. Am. Coll. Cardiol. 44 (4): 783–9. doi:10.1016/j.jacc.2004.05.045. PMID 15312859. Unknown parameter
|month=ignored (help) - ↑ Bradshaw PJ, Ko DT, Newman AM, Donovan LR, Tu JV (2007). “Validation of the Thrombolysis In Myocardial Infarction (TIMI) risk index for predicting early mortality in a population-based cohort of STEMI and non-STEMI patients”. Can J Cardiol. 23 (1): 51–6. PMID 17245483. Unknown parameter
|month=ignored (help) - ↑ 18.0 18.1 Granger CB, Goldberg RJ, Dabbous O, Pieper KS, Eagle KA, Cannon CP; et al. (2003). “Predictors of hospital mortality in the global registry of acute coronary events”. Arch Intern Med. 163 (19): 2345–53. doi:10.1001/archinte.163.19.2345. PMID 14581255.
- ↑ Eagle KA, Lim MJ, Dabbous OH, Pieper KS, Goldberg RJ, Van de Werf F; et al. (2004). “A validated prediction model for all forms of acute coronary syndrome: estimating the risk of 6-month postdischarge death in an international registry”. JAMA. 291 (22): 2727–33. doi:10.1001/jama.291.22.2727. PMID 15187054. Review in: ACP J Club. 2004 Nov-Dec;141(3):80
STEMI in Pregnancy
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Physiological changes during pregnancy may increase the woman’s risk of developing a myocardial infarction (MI). MI during the antepartum period is usually caused by an atherosclotic plaque rupture, whereas MI during the peripartum and postpartum period is usually caused by coronary artery dissection (commonly in the LAD). Diagnosis of MI among pregnant women is similar to that in the general population and requires clinical suspiccion, as well as ECG changes and troponin elevation. In contrast, elevated CK-MB concentration is unreliable, since CK-MB may normally increase during labor and post-delivery due to non-cardiac causes, namely placental and uterine leaks. During an MI, echocardiography is safe and may be performed to evaluate wall motion abnormalities, and fetal monitoring is recommended. Treatment is usually by percutaneous coronary intervention. If spontaneous coronary artery dissection occurs, a more thorough investigation for connective tissue diseases and vasculitis is warranted.
Acute MI in Pregnancy
- Incidence: 1 per 35,000 deliveries
- Maternal mortality rate: 5% to 18%, fetal mortality rate: 9%
- Common in third trimester until 1-2 months post-delivery
- Antepartum: Atherosclotic plaque rupture is the most common cause
- Perpartum or postpartum: Coronary artery dissection (LAD > RCA > LC > LM)
Risk Factors
- It is unknown if pregnancy itself is a risk factor in development of acute MI.
- The most important risk factors in the development of AMI in pregnancy are generally similar to those in the general population. Risk factors include:
- Age > 35 years
- Diabetes mellitus
- Hypertension
- Smoking
- Connective tissue diseases (e.g. Ehler Danlos syndrome)
- Vasculitis (e.g. Takayasu arteritis)
- Thrombophilia (e.g. antiphospholipid syndrome)
- Acute post-partum stress:
- Severe post-partum hemorrhage
- Post-partum infection
Pathophysiology
- During pregnancy, progesterone release results in structural changes in the vascular intima and media.
- Physiologically, cardiac output and blood volume increase during pregnancy, both of which may increase the risk of cardiovascular events.
Diagnosis
- Diagnosis similar to the general population by: Symptoms, ECG changes, and troponin.
- CK-MB concentrations may markedly increase during labor and post-delivery due to non-cardiac causes, namely placental and uterine leaks.
- Echocardiography is safe and may be performed to evaluate wall motion abnormalities.
- Fetal monitoring is recommended.
Treatment
- Percutaneous coronary intervention
- If spontaneous coronary artery dissection occurs, a more thorough investigation for connective tissue diseases and vasculitis is warranted.
Diagnosis
Diagnosis
Diagnostic Criteria | History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | EKG Examples | Chest X Ray | Cardiac MRI | Echocardiography | Coronary Angiography
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
The diagnosis of acute MI is based upon the occurence of clinical symptoms such as substernal chest pain, ECG changes such as ST elevation and a rise in the release of very specific biomarkers into the bloodstream that are normally only found in side the heart muscle cell (the myocyte).
The diagnosis can be confirmed at the time of autopsy or at the time of angiography if a closed artery is seen. A new clinical evidence based diagnostic and classification system has been introduced by Thygesen K, Alpert JS, White HD, et al. and jointly sponsored by the American College of Cardiology (ACC), American Heart Association (AHA), European Society of Cardiology (ESC), and the World Heart Federation (WHF).[1]
Criteria for Diagnosis of Acute Myocardial Infarction
The term myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting consistent with myocardial ischemia. Under these conditions any one of the following criteria meets the diagnosis for acute myocardial infarction. [1]
Below are the criteria quoted from the Thygesen article:
- Detection of rise and/or fall of cardiac biomarkers (preferably Troponin) with at least one of the following
- a. Symptoms of ischemia
- b. EKG changes indicative of ischemia as ST segment elevation of >_ 0.1 mV in at least 2 contiguous leads, or new left bundle branch block LBBB). If initial ECG is non-diagnostic, repeat at 5 to 10 min intervals.
- c. Development of pathological Q waves
- d. Imaging evidence of new viable myocardium or wall motion abnormality
- Sudden unexpected cardiac death, including cardiac arrest, often with symptoms suggestive of myocardial ischemia, accompanied by presumably new ST segment elevation, or new LBBB, and/or evidence of fresh thrombus in a coronary artery by angiography and/or at autopsy, if death has occurred before blood samples could be obtained, or at a time before the appearance of cardiac biomarkers in the blood
- In patients with normal baseline troponin values, a greater than 3 times increase above the 99th percentile of the upper limit of normal of cardiac biomarkers has been designated as the definition of PCI related myocardial infarction. A subtype related to documented stent thrombosis is recognized.
- For patients with CABG surgery; (In patients with normal baseline troponin values) increases of cardiac biomarkers greater than 5 times, (> 5 times the 99th percentile upper limit of normal) and either new pathological Q waves or new LBBB or angiographically evidence of new graft or native vessel occlusion have been designated as defining CABG surgery related myocardial infarction.
- Pathological findings of acute myocardial infarction.
Criteria for the Diagnosis of a Prior Myocardial Infarction
If any of the following are present, then a diagnosis of prior myocardial infarction is established:[1]
- Development of new pathological Q waves with or without symptoms
- Imaging evidence of a region of loss of viable myocardium that is thinned and fails to contract in the absence of a non ischemic cause.
- Pathological findings of healed or healing myocardial infarction.
Modern Classification as to the Type of MI
Five types of MI are now recognized and classified as follows: [1]
- Type 1: Spontaneous myocardial infarction related to ischemia due to a primary coronary event, such as plaque erosion and/or rupture, fissuring, or dissection.
- Type 2: Myocardial infarction secondary to ischemia due to an imbalance of O2 supply and demand, as from coronary spasm or embolism, anemia, arrhythmias, hypertension, or hypotension
- Type 3: Sudden unexpected cardiac death, including cardiac arrest, often with symptoms suggesting ischemia with new ST segment elevation; new left bundle branch block; or pathologic or angiographic evidence of fresh coronary thrombus (in the absence of reliable biomarker findings)
- Type 4:
- a. Myocardial infarction associated with Percutaneous Coronary Interventions (PCI)
- b. Myocardial infarction associated with documented stent thrombosis.
- Type 5: Myocardial infarction associated with Coronary Artery Bypass Graft surgery
For the main article on cardiac markers see the chapter on cardiac markers. For the main article on the diagnosis of STEMI, see the chapter on Clinical classification of acute myocardial infarction.
Older Classification Schemes as to the Type of MI
There have been several prior classification schemes for characterizing MI:
1. Transmural (necrosis of full thickness of ventricle) vs. non-transmural (necrosis of partial thickness of ventricle)
2. Q wave vs. non Q wave: Based upon the development of electrocardiographic Q waves representing electrically inert tissue.
3. ST elevation MI (STEMI) and Non ST elevation myocardial infarction (NSTEMI)
At one time it was thought that Transmural MI and Q wave MI were synonymous. However, not all Q wave MIs are transmural, and not all transmural MIs are associated with Q waves.
Likewise, not all ST elevation MIs go on to cause q waves. Non ST elevation MIs can result in q waves.
Thus, ST elevation MI should not be equated with transmural MI or q wave MI. Likewise, Non ST elevation MI should not be equated with non transmural MI or non q wave MI. These 3 designations reflect three separate but overlapping characterization schemes.
Biomarkers in the Diagnosis of MI
Cardiac markers or cardiac enzymes are proteins that are present in cardiac myocytes that should not be in the bloodstream. When cardiac injury occurs (such as in acute MI), these intracellular proteins are then released into the bloodstream. Along with the patient’s history and the electrocardiogram, the release of these enzymes forms the basis of the diagnosis of ST elevation myocardial infarction.
Until the 1980s, the enzymes SGOT and LDH were used to assess cardiac injury. In the early 1980s it was found that disproportional elevation of the MB subtype of the enzyme creatine kinase (CK) was very specific for myocardial injury. More recently, troponin has been used as an even more specific marker of myonecrosis. Current guidelines are generally in favor of troponin sub-units I or T, which are very specific for damage to myocytes.[2] [3][4]
It is important to note that it may take hours for cardiac enzymes to rise following injury to the myocardium, and that cardiac biomarkers may not be elevated on presentation. For this reason, cardiac enzymes and ECGs are checked every 6 to 8 hours over the course of the first 24 hours to “rule out” acute MI. These enzyme measures over the first 24 hours are used to gauge the size of an MI: higer peak levels and a greater area under the curve of enzyme release are associated with larger MIs and poorer prognosis.
The 2007 Joint ESC/ACCF/AHA/WHF Task Force Guidelines[5]
| “ |
Criteria for acute myocardial infarction: 1. Detection of rise and/or fall in cardiac biomarkers (preferably troponin) with at least one value above 99th percentile of the upper reference limit (URL) together with the evidence of myocardial ischemia with at least one of the following:
|
” |
False Positive Diagnosis of MI: Troponin Elevations That Are Not Due to Thrombotic Coronary Occlusion
It is important to note that cardiac troponins are a marker of all heart muscle damage, not just myocardial infarction. There are other “false positive” causes of troponin elevation that directly or indirectly lead to heart muscle damage can also therefore increase troponin levels:[6][7][8][9]
- Cardiac:
- Acute aortic dissection
- Aortic valve disease
- Cardiac amyloidosis and other cardiac infiltrative disorders
- Cardiac contusion
- Cardiac surgery and heart transplant
- Closure of atrial septal defects
- Coronary artery vasospasm
- Defibrillation
- Dilated cardiomyopathy
- Endocarditis
- Endomyocardial biopsy
- Heart failure
- Hypertrophic cardiomyopathy
- Hypotension
- Myocarditis
- Percutaneous coronary intervention
- Pericarditis
- Pulmonary hypertension
- Radiofrequency ablation
- Supraventricular tachycardia including atrial fibrillation
- Takotsubo cardiomyopathy
- Non-cardiac:
- ARDS
- Critical illness, e.g. sepsis
- Extensive burn
- High-dose chemotherapy
- Hypovolemia
- Intracranial hemorrhage
- Primary pulmonary hypertension
- Pulmonary embolism
- Pulmonary emphysema
- Renal failure
- Scorpion venom
- Shock
- Strenuous exercise (e.g. marathon)
- Stroke
- Subarachnoid hemorrhage
- Sympathomimetic ingestion
References
- ↑ 1.0 1.1 1.2 1.3 Thygesen K, Alpert JS, White HD; et al. (2007). “Universal definition of myocardial infarction”. Circulation. 116 (22): 2634–53. doi:10.1161/CIRCULATIONAHA.107.187397. PMID 17951284. Unknown parameter
|month=ignored (help) - ↑ Eisenman A (2006). “Troponin assays for the diagnosis of myocardial infarction and acute coronary syndrome: where do we stand?”. Expert Rev Cardiovasc Ther. 4 (4): 509–14. doi:10.1586/14779072.4.4.509. PMID 16918269. Unknown parameter
|month=ignored (help) - ↑ Aviles RJ, Askari AT, Lindahl B; et al. (2002). “Troponin T levels in patients with acute coronary syndromes, with or without renal dysfunction”. N. Engl. J. Med. 346 (26): 2047–52. doi:10.1056/NEJMoa013456. PMID 12087140. Unknown parameter
|month=ignored (help) - ↑ Summary of “Troponin T levels in patients…” for laymen
- ↑ Thygesen K, Alpert JS, White HD, Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial Infarction (2007) Universal definition of myocardial infarction. Eur Heart J 28 (20):2525-38. DOI:10.1093/eurheartj/ehm355 PMID: 17951287
- ↑ Jeremias A, Gibson CM (2005). “Narrative review: alternative causes for elevated cardiac troponin levels when acute coronary syndromes are excluded”. Ann. Intern. Med. 142 (9): 786–91. PMID 15867411. Unknown parameter
|month=ignored (help) - ↑ Ammann P, Pfisterer M, Fehr T, Rickli H. Raised cardiac troponins. BMJ 2004;328:1028-9. PMID 15117768.
- ↑ Agewall S, Giannitsis E, Jernberg T, Katus H (2011). “Troponin elevation in coronary vs. non-coronary disease”. Eur Heart J. 32 (4): 404–11. doi:10.1093/eurheartj/ehq456. PMID 21169615.
- ↑ Mahajan VS, Jarolim P (2011). “How to interpret elevated cardiac troponin levels”. Circulation. 124 (21): 2350–4. doi:10.1161/CIRCULATIONAHA.111.023697. PMID 22105197.
Treatment
Treatment
Oxygen | Nitrates | Analgesics | Aspirin | Beta Blockers | Antithrombins | The coronary care unit | The step down unit | STEMI and Out-of-Hospital Cardiac Arrest
Pharmacologic Reperfusion | Reperfusion Therapy (Overview of Fibrinolysis and Primary PCI) | Fibrinolysis
Mechanical Reperfusion | The importance of reducing Door-to-Balloon times | Primary PCI | Adjunctive and Rescue PCI | Rescue PCI | Facilitated PCI | Adjunctive PCI | CABG | Management of Patients Who Were Not Reperfused | Assessing Success of Reperfusion
Antithrombin Therapy | Antithrombin therapy | Unfractionated heparin | Low Molecular Weight Heparinoid Therapy | Direct Thrombin Inhibitor Therapy | Factor Xa Inhibition | DVT prophylaxis | Long term anticoagulation
Antiplatelet Agents | Aspirin | Thienopyridine Therapy | Glycoprotein IIbIIIa Inhibition
Other Initial Therapy | Inhibition of the Renin-Angiotensin-Aldosterone System | Magnesium Therapy | Glucose Control | Calcium Channel Blocker Therapy | Lipid Management
Long-Term Medical Therapy and Secondary Prevention
Long-Term Medical Therapy and Secondary Prevention
Overview | Inhibition of the Renin-Angiotensin-Aldosterone System | Cardiac Rehabilitation | Pacemaker Implantation | Long Term Anticoagulation | Implantable Cardioverter Defibrillator
Disclaimer
Disclaimer
Any recommendations found on these pages are for education use only. WikiDoc is not a substitute for a licensed healthcare provider. Please see the disclaimers page for important information regarding limitations of the information found here.
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH