
Atrial septal defect
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, M.D. [2]; Kalsang Dolma, M.B.B.S.[3] Assistant Editor(s)-In-Chief: Kristin Feeney, B.S. [4]
Synonyms and keywords: ASD
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, M.B.B.S. [2]; Cafer Zorkun, M.D., Ph.D. [3] Assistant Editor(s)-In-Chief: Kristin Feeney, B.S. [4]
Overview
Atrial septal defects refer to a group of congenital heart diseases that involve the inter-atrial septum. The inter-atrial septum is the tissue that separates the right and left atria from each other. This tissue prevents arterial and venous blood from mixing with each other. If there is a defect in this septum, a direct communication between the atria can occur, which allows shunting, resulting in mixing of arterial and venous blood. It is possible for blood to travel from the left side of the heart to the right side of the heart, or vice versa. Shunting can result in cyanosis. The excess flow to the right atrium and the right ventricle causes enlargement of these organs, and the increased flow through the pulmonary artery eventually causes pulmonary hypertension.
Anatomy
The embryological development of human fetal heart takes place as early as 4th week of intrauterine life. The normal septal development requires a proper alignment and fusion of the two interatrial septums i.e. septum primum and septum secundum. Failure to do so may lead to the development of atrial septal defects.
Classification
The normal septal development requires a proper alignment and fusion of the two interatrial septums i.e. septum primum and septum secundum. Failure to do so may lead to a patent fossa ovalis and the development of atrial septal defects (ASDs). Atrial septal defects are classified into various types based on their location and the nature of the embryological defect. The types of atrial septal defects that can occur are: ostium primum, ostium secundum, sinus venosus, common or single atrium and coronary sinus defects. Patent foramen ovale, commonly associated with atrial septal defects, is a sister condition involving communication between the two atria. Patent foramen ovale is not a true atrial septal defect as flap like tissue that functions usually like a one way valve is present in a PFO.
Pathophysiology
In the case of a large ASD (>9 mm), which may result in a clinically significant left-to-right shunt, blood will shunt from the left atrium to the right atrium causing excessive mixing of the blood between the two atria. In a hemodynamically significant ASD, Qp is the pulmonary flow and Qs is the systemic flow. If the Qp:Qs is > 1.5:1, then the patient is often symptomatic, and a repair of the ASD may be indicated. This extra blood from the left atrium may cause a volume overload of both the right atrium and the right ventricle, which if left untreated, can result in enlargement of the right side of the heart and ultimately right-sided heart failure.
If left uncorrected, the pressure in the right side of the heart will be greater than the left side of the heart. This will cause the pressure in the right atrium to be higher than the pressure in the left atrium. This will reverse the pressure gradient across the ASD, and the shunt will reverse; a right-to-left shunt will exist. This phenomenon is known as Eisenmenger’s syndrome. Once right-to-left shunting occurs, a portion of the oxygen-poor blood will get shunted to the left side of the heart and ejected to the peripheral vascular system. This will cause signs of cyanosis. Once Eisenmenger’s syndrome develops, the patient can no longer benefit from surgery to correct the defect.
Causes
Often an ASD occurs sporadically. However, ASD has been associated with genetic disorders such as the Holt-Oram syndrome (heart-hand syndrome) , Down syndrome, Noonan syndrome,Treacher Collins syndrome, and the thrombocytopenia-absent radii (TAR) syndrome.
Epidemiology and Demographics
Atrial septal defects are the most common form of congenital heart disease, accounting for 20-40% of all congenital heart disease cases in adults. Atrial septal defects can be classified into : ostium secundum, ostium primum, sinus venosus, coronary sinus ASDs and common or single atrium defects. Collectively, atrial septal defects account for 10% of all congenital heart disease. Infants and adolescent patients may be asymptomatic until later in life. By 40 years of age, approximately 90% of untreated atrial septal defect patients will experience an onset of symptoms.
Risk Factors
As is common with most congenital heart conditions, the exact cause of atrial septal defect is not known. Research suggests a potential link between genetic conditions such as Down syndrome and the development of an atrial septal defect. Other potential causes include exposure to environmental contaminants such as rubella as well as alcohol consumption. A clinician should encourage families with a history of congenital heart defect to consider genetic counseling to identify potential risks.
Natural History, Complications and Prognosis
The natural history of atrial septal defect depends on the location, the size of the defect, the amount of shunting of blood and the presence of associated congenital anomalies. A small atrial septal defect may remain asymptomatic throughout life and/or may close spontaneously in infants. Patients with isolated atrial septal defects generally survive to adulthood. An ASD can also present in adulthood with the insidious development of symptoms. Complications like pulmonary hypertension, atrial fibrillation, right heart failure and stroke can develop if large sized defects are left uncorrected. The mortality rate associated with surgical repair is less than 1% for patients under the age of 45, who have no history of heart failure or pulmonary artery hypertension. Virtually all ASD patients develop symptoms by the age of 60. An ASD that is repaired early in life is associated with no reduction in life expectancy.
Pregnancy causes an increase in cardiac output and stroke volume. This can cause an increased left-to-right shunting of blood. Despite the increased workload on heart, females with isolated asymptomatic atrial septal defects tolerate the pregnancy well. Pregnant females with an atrial septal defect may have increased frequencies of some complications for instance arrhythmias, thromboembolism, and bleeding. Despite this, there are no studies suggesting that pregnancy requires different indications for closure in pregnant females with atrial septal defect compared to a non-pregnant female with atrial septal defect. The ACC/AHA guidelines, however, do dictate clear deviations in course of treatment in certain special circumstances. Pregnancy in patients with ASD and severe PAH (Eisenmenger syndrome) is not recommended owing to excessive maternal and fetal mortality and should be strongly discouraged.
Diagnosis
History and Symptoms
The development of symptoms associated with atrial septal defect relates to the size and severity of intracardiac shunting of blood across the defect. A large atrial septal defect will result in the presentation of symptoms at a younger age. However, smaller, less severe defects may be asymptomatic until adulthood. Smaller defects cause less hemodynamic disruptions. Symptoms such as difficulty breathing,exercise intolerance, and fatigue may be seen. As a person ages, the potential for the development of symptoms increases. Adults, especially those over the age of 40, will become symptomatic. Nearly all adults with an atrial septal defect will present with symptom onset by the age of 60.
Physical Examination
Volume overload of the right side of heart can lead to right heart failure that may present with symptoms of swelling of the extremities, difficulty breathing and signs such as hepatomegaly and an elevated jugular venous pulse. On cardiovascular examinations there is a fixed splitting of second heart sound. Also, a systolic ejection murmur that is attributed to the increased flow of blood through the pulmonic valve can be heard.
Electrocardiogram
The ECG findings may show a prolonged PR interval (first degree heart block). The prolongation of the PR interval is probably due to the enlargement of the atria that is common in ASD. Other findings include right bundle branch block (RBBB), right axis deviation, right ventricular hypertrophy (RVH), atrial fibrillation and atrial flutter.
Chest X Ray
Chest x rays may detect an atrial septal defect. Chest x rays can be limited in imaging quality and may only supplement other imaging modalities. The chest x-ray may demonstrate cardiomegaly (right ventricular and right atrial enlargement), a prominent pulmonary artery segment, and increased pulmonary vascular markings.
CT
Computed tomography can be helpful as a diagnostic tool in conditions where the echocardiographic findings are inconclusive. It is not the technique of choice as it has limitations in defining shunt volume and pressure differences.
MRI
Magnetic resonance imaging (MRI) can be used as a diagnostic tool in identifying an atrial septal defect. It also helps in visualization of the pulmonary veins, quantifying right ventricular volume and shunt size. Velocity-encoded, phase difference MRI can assess the magnitude of left-to-right shunting as reliably as is done by cardiac catheterization [1]. Also, it has the advantage of being a non-invasive tool compared to the invasive cardiac catheterization. Additionally, phase-contrast cine MRI is more reliable than spin-echo images in determining the size of defect that in turn helps to make a better therapeutics decision i.e. trans-cutaneous or the surgical closure [2].However, its current utility is limited for smaller defects and in inconclusive echocardiography findings.
Echocardiography
Echocardiography along with doppler ultrasound are the preferred imaging modalities to diagnose atrial septal defect. On transthoracic echocardiography, an atrial septal defect may be seen on color flow imaging as a jet of blood from the left atrium to the right atrium. Usually transesophageal echocardiography is a better tool for diagnosing atrial septal defects than transthoracic echo. Trials have demonstrated that transesophageal echocardiography is superior to transthoracic echocardiography in diagnosing sinus venosus ASD[3].
Transcranial Doppler Ultrasound
Trans-cranial doppler ultrasound is a diagnostic tool that involves a simple intravenous injection of saline under minimal sedation. It is primarily utilized to further diagnostically evaluate a patent foramen ovale defect.
Cardiac Catheterization
Cardiac catheterization is a lesser utilized imaging modality. Many of the observations/visualizations made on a cardiac catheterization can be visualized confidently in non-invasive measures such as echocardiography. When echocardiography falls short, cardiac catheterization can be an effective tool in detection of the atrial septal defect. It is especially effective in determining the coronary anatomy of the atrial septal defect and surrounding structures.
Exercise Testing
Exercise testing can be used to document changes in oxygen saturation. However, it is contraindicated in severe pulmonary artery hypertension.
Treatment
Atrial septal defects can remain asymptomatic until the fourth decade of life. The treatment can involve either a medical or surgical approach. Surgical closure further could be divided into percutaneous repair or open heart surgery involving either suture or patch closure.
Medical Therapy
Medical therapy has a limited role in the definitive treatment of ASD. Medical therapy consists rate control of atrial fibrillation and anticoagulation to reduce the risk of embolization among patients with atrial fibrillation.
Surgery
Indications for Surgical Repair in Adults
The decision to surgically close an atrial septal defect depends upon many contributing factors including the type of defect, the size of defect, the amount of left-to-right shunting, the development or worsening of symptoms, the presence of pulmonary hypertension and the presence of any associated anomalies.
Surgical Closure
Surgical closure is the most common treatment method for atrial septal defect patients and has been the gold standard for many years. It is still the most popular method for repair of defects like sinus venosus ASD, coronary sinus ASD, or primum ASD. However, surgery is contraindicated in patients with severe irreversible pulmonary artery hypertension, Eisenmenger’s syndrome and no evidence of a left-to-right shunt.
Minimally Invasive Repair
Minimally invasive repair of atrial septal defect has been shown to be as successful as the conventional sternotomy, with the added advantage of being less invasive, less post-surgical complications and decreased hospital stay.
Robotic Repair
Robotic repair is done through the ‘da Vinci Surgical System’ (Intuitive Surgical) is the most recent and advanced approach for the repair of atrial septal defect [4]. Due to this technique a surgeon can perform operations from a remote distance. The surgeon gets an excellent three dimensional view of the heart through the fiberoptic stereoscopic camera. The surgeon‘s hand motions are relayed to a computer processor, which digitizes and relays them to the fine instrument placed into the chest through small port incisions.
Percutaneous Closure
Percutaneous closure is commonly performed for ostium secundum ASDs. This procedure is still not FDA approved for the treatment of other types of atrial septal defects like sinus venosus ASD, coronary sinus ASD or primum ASD. With appropriate patient selection, percutaneous closure of an ostium secundum ASD has been demonstrated to be as successful, safe and effective as surgical closure. Additionally, percutaneous closure has been associated with fewer complications and a reduced average length of hospital stay compared to surgical care.
Post Surgical Follow Up
Due to the development of new minimally invasive techniques, percutaneous closure and improvement in surgical closure, most patients with atrial septal defect can start eating and ambulating within the first or second postoperative days. Also, most patients with surgical closure are discharged by the third or fourth postoperative days and patients with percutaneous closure, are generally discharged the next day. Surgical follow-up care is mostly for 1-2 months. Ideally, at least 1 follow-up echocardiogram to confirm complete closure of the atrial septal defect should be obtained. A cardiologist with good experience with heart defects should continue patient care. An yearly follow up to monitor development of complications like arrhythmias should be arranged. Six months of aspirin with or without clopidogrel is recommended for prevention of thrombus formation.
References
- ↑ Hundley WG, Li HF, Lange RA, Pfeifer DP, Meshack BM, Willard JE; et al. (1995). “Assessment of left-to-right intracardiac shunting by velocity-encoded, phase-difference magnetic resonance imaging. A comparison with oximetric and indicator dilution techniques”. Circulation. 91 (12): 2955–60. PMID 7796506.
- ↑ Holmvang G, Palacios IF, Vlahakes GJ, Dinsmore RE, Miller SW, Liberthson RR; et al. (1995). “Imaging and sizing of atrial septal defects by magnetic resonance”. Circulation. 92 (12): 3473–80. PMID 8521569.
- ↑ Kronzon I, Tunick PA, Freedberg RS, Trehan N, Rosenzweig BP, Schwinger ME (1991). “Transesophageal echocardiography is superior to transthoracic echocardiography in the diagnosis of sinus venosus atrial septal defect”. J Am Coll Cardiol. 17 (2): 537–42. PMID 1991912.
- ↑ Suematsu Y, Kiaii B, Bainbridge DT, del Nido PJ, Novick RJ (2007). “Robotic-assisted closure of atrial septal defect under real-time three-dimensional echo guide: in vitro study”. Eur J Cardiothorac Surg. 32 (4): 573–6. doi:10.1016/j.ejcts.2007.06.026. PMID 17702588.
Anatomy
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, M.B.B.S. [2]; Assistant Editor(s)-In-Chief: Kristin Feeney, B.S. [3]
Overview
The embryological development of human fetal heart takes place as early as 4th week of intrauterine life. The normal septal development requires a proper alignment and fusion of the two interatrial septums i.e. septum primum and septum secundum. Failure to do so may lead to the development of atrial septal defects.
Anatomy

The development of the fetal heart takes place as early as the 4th week of gestation. An abnormal septal development at this stage may lead to atrial septal defect.
Embryogenesis
Normal septal embryogenesis occurs as follows:
- The developing heart has an orifice called ostium primum or primary interatrial foramen between the atrium that serves as an opening between the free edge of the septum primum and the AV cushions.
- A septum primum arises from the superior portion of the common atrium of the developing heart. It serves to subdivide the cavity of the primitive atrium into right and left chambers.
- An endocardial cushion is located between the atria and ventricles, serving to create the infrastructure to the basis of the four-chambered heart formation.
- Septum primum grows downward to the endocardial cushions. This leads to the closing of the orifice (ostium primum) between the atria.
- A second entity, the septum secundum, develops to the right of the septum primum and the opening between the upper and lower limbs of the septum secundum is known as the foramen ovale of the heart and persists until birth. These two septae fuse later in life to complete the formation of the atrial septum.
- In the fetus this orifice allows shunting of blood from right to left side of the heart. This is so because during the fetal life right side heart pressures are more than the systemic pressure. However, there is a reversal of pressure gradient after birth (systemic pressures becomes more than right sided pressure) and this change of pressure causes the septum primum to be held against the septum secundum and closing the interatrial shunt.
- In approximately 30% of population the septum primum and secundum fails to fuse leading to patent foramen ovale (PFO) in the newborn. In this case, elevation of pressure in the pulmonary circulatory system (ie: pulmonary hypertension due to various causes, or transiently during a cough) can cause the foramen ovale to remain open. The patent foramen ovale can be of two types:
- Completely covered but not completely sealed so that the foramen can be opened with reversal of shunt. This is also sometimes called as a probe patent or patent foramen ovale (PFO)
- An open communication exists between right and left atrium persists is the true definition of what is known as an atrial septal defect (ASD).
References
Classification
Ostium Secundum Atrial Septal Defect | Ostium Primum Atrial Septal Defect | Sinus Venosus Atrial Septal Defect | Coronary Sinus | Patent Foramen Ovale | Common or Single Atrium
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, M.B.B.S. [2]; Assistant Editor(s)-In-Chief: Kristin Feeney, B.S. [3]
Overview
The normal septal development requires a proper alignment and fusion of the two interatrial septums i.e. septum primum and septum secundum. Failure to do so may lead to a patent fossa ovalis and the development of atrial septal defects (ASDs). Atrial septal defects are classified into various types based on their location and the nature of the embryological defect. The types of atrial septal defects that can occur are: ostium primum, ostium secundum, sinus venosus, common or single atrium and coronary sinus defects. Patent foramen ovale, commonly associated with atrial septal defects, is a sister condition involving communication between the two atria. Patent foramen ovale is not a true atrial septal defect as flap like tissue that functions usually like a one way valve is present in a PFO.
Classification
Atrial septal defects are classified into various types based on their location and the nature of the embryological defect [1]. Isolated ASDs occur due to abnormal development of the septal between the right and left atrium of the heart and normally are not associated with other cardiac defects.
Ostium Secundum ASD
Ostium secundum ASD at the fossa ovalis account for 75% of all atrial septal defects.
Ostrium Primum ASD
An ostium primum defect usually occurs due to the failure in fusion of the septum primum with the endocardial cushion. This defect is commonly associated with other cardiac anomalies in the septum such as ventricular septal defect, mitral valve cleft, pulmonary stenosis, subaortic stenosis, left superior vena cava, coarctation and atrioventricular septal defect.
Sinus Venosus ASD
Sinus venosus ASD defects can be of two types depending on their location in comparison to the fossa ovalis. They form 5-10% of all the atrial septal defects.
Superior Sinus Venosus Type ASD (Superior Vena Caval Defect)
The defect is superior to fossa ovalis.
Inferior Sinus Venosus Type ASD (Inferior Vena Caval Defect)
The defect is inferior to the fossa ovalis.
Coronary Sinus Defects
Accounting for less than 1% of all atrial septal defects, this rare atrial septal defect occurs at the site of the coronary sinus drainage.
Patent Foramen Ovale
Patent foramen ovale (PFO): A flap like formation where communication exists between the right and left atria. It is commonly associated with atrial septal defects, however, it is not technically considered a true atrial septal defect as no septal tissue is missing. There is not continuous flow across a PFO as there is with an ASD. There is only flow across a PFO when there is an increase in right atrial pressure such as occurs during the valsalva maneuver.
Common or Single Atrium
Common (or single) atrium is a failure of development of the embryologic components that contribute to the atrial septal complex. It is frequently associated with heterotaxy syndrome. [2]
ASD Associated with other Malformations
ASDs are associated with other malformations in 30% of cases of atrial septal defect.
Associated defects include:
- Ostium primum ASDs /Atrioventricular canal defects: Occur due to malformation of the partitioning of the atrioventricular (AV) canal by the endocardial cushions (accounts for 15% to 20% of all atrial septal defects) and is located inferiorly near the crux of heart. It is most commonly associated with other malformations such as cleft in the anterior mitral valve leaflet. AV canal defects can be classified as: complete, incomplete, and common atrium.
- Ostium primum ASD or Ostium secundum ASD: Aneurysmal formations found in some patients and may have multiple small fenestrations.
References
- ↑ Fuster V, Brandenburg RO, McGoon DC, Giuliani ER (1980). “Clinical approach and management of congenital heart disease in the adolescent and adult”. Cardiovasc Clin. 10 (3): 161–97. PMID 6991111.
- ↑ Valdes-Cruz LM, Cayre RO (1998). Echocardiographic diagnosis of congenital heart disease. Philadelphia.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, M.B.B.S. [2]; Assistant Editor(s)-In-Chief: Kristin Feeney, B.S. [3]
Overview
In a normal heart, the typical path of blood flow is to flow from right-to-left allowing for blood to leave the deoxygenated right system and become oxygenated in the left system. In patients with an atrial septal defect, the typical path of blood flow is disrupted by the septal opening. This results in blood shunting from left-to-right. The severity of circulatory complications depends largely on the size of the defect. The larger the defect between the septal walls, the greater the amount of mixing between deoxygenated and oxygenated blood. Flow from the left atrium into the right atrium increases flow through the pulmonary circuit increasing the load on the right ventricle and slowly injuring the pulmonary vasculature over time.
Pathophysiology
Left-Sided Versus Right-Sided Pressures
In unaffected individuals, the chambers of the left side of the heart make up a higher pressure system than the chambers of the right side of the heart. This is because the left ventricle has to produce enough pressure to pump blood throughout the entire body, while the right ventricle only has to produce enough pressure to pump blood to the lungs.
Calculation of the Pulmonary to Systemic Flow Ratios
In the case of a large ASD (>9 mm), which may result in a clinically significant left-to-right shunt, blood will shunt from the left atrium to the right atrium causing excessive mixing of the blood between the two atria. In a hemodynamically significant ASD, Qp is the pulmonary flow and Qs is the systemic flow and the Qp:Qs > 1.5:1). If the Qp:Qs is > 1.5:1, then the patient is often symptomatic, and a repair of the ASD may be indicated. This extra blood from the left atrium may cause a volume overload of both the right atrium and the right ventricle, which if left untreated, can result in enlargement of the right side of the heart and ultimately right-sided heart failure.
Impact of Changes in Left Ventricular Loading Conditions
Any process that increases the pressure in the left ventricle can cause worsening of the left-to-right shunt. This includes hypertension, which increases the pressure that the left ventricle has to generate in order to open the aortic valve during ventricular systole, and coronary artery disease which increases the stiffness of the left ventricle, thereby increasing the filling pressure of the left ventricle during ventricular diastole.
Right Heart Failure as a Consequence of Left Right Shunting
The right ventricle will have to push out more blood than the left ventricle due to the left-to-right shunt. This constant overload of the right side of the heart will cause an overload of the entire pulmonary vasculature. Eventually the pulmonary vasculature will develop pulmonary hypertension as a result of the extra blood flow through the lungs.
The resulting pulmonary hypertension will cause the right ventricle to face increased pressure or increased afterload in addition to the increased preload (higher volume coming into the right side of the heart) as a result of the shunted blood flowing from the left atrium into the right atrium. The right ventricle will be forced to generate higher pressures to try to overcome the pulmonary hypertension. This may lead to right ventricular failure (dilatation and decreased systolic function of the right ventricle). Eventually the right-sided pressures may exceed left-sided pressures.
Equalization of Left and Right Atrial Pressures
When the pressure in the right atrium rises to the level in the left atrium, there will no longer be a pressure gradient between these heart chambers, and the left-to-right shunt will diminish or cease.
Development of Right-to-Left Shunting or Eisenmenger’s Syndrome
If left uncorrected, the pressure in the right side of the heart will be greater than the left side of the heart. This will cause the pressure in the right atrium to be higher than the pressure in the left atrium. This will reverse the pressure gradient across the ASD, and the shunt will reverse; a right-to-left shunt will exist. This phenomenon is known as Eisenmenger’s syndrome. Once right-to-left shunting occurs, a portion of the oxygen-poor blood will get shunted to the left side of the heart and ejected to the peripheral vascular system. This will cause signs of cyanosis. once Eisenmenger’s syndrome develops, the patient can no longer benefit from surgery to correct the defect.
Gross Pathology
-
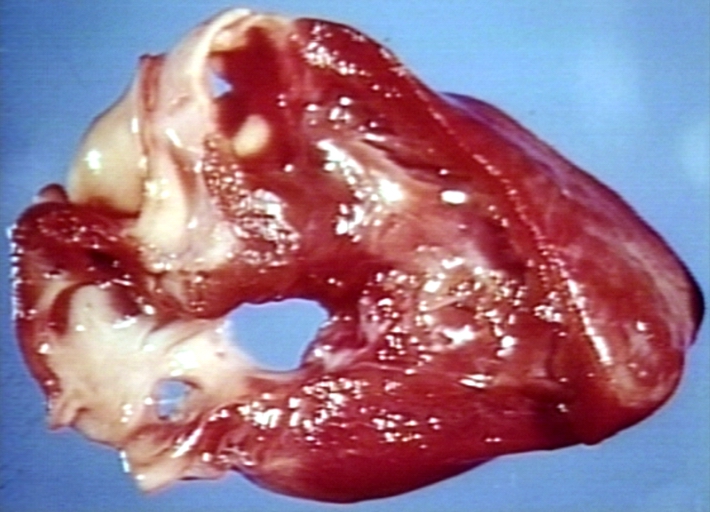 Atrial Septal Defect, Septum Primum; View from Right Atrium (a 4 month old baby)
Atrial Septal Defect, Septum Primum; View from Right Atrium (a 4 month old baby) -
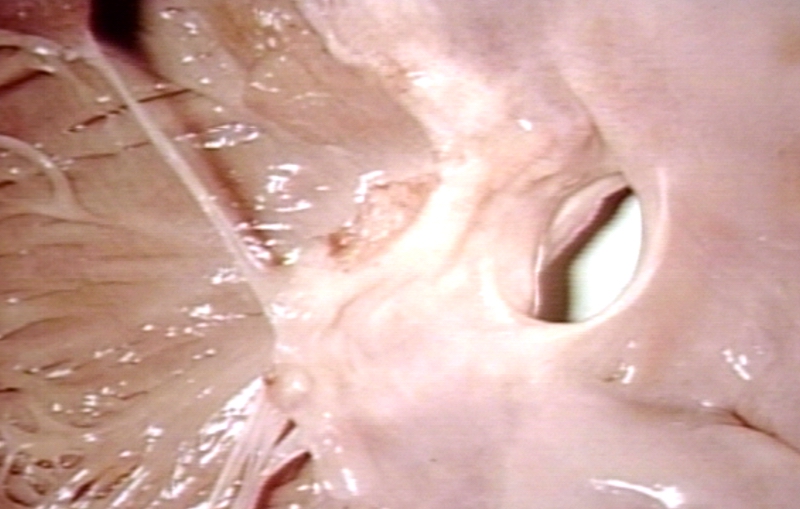 Atrial Septal Defect, Septum Primum; Also Cleft in Anterior Cusp of Mitral Valve
Atrial Septal Defect, Septum Primum; Also Cleft in Anterior Cusp of Mitral Valve


Associated Conditions
Secundum ASD is seen in Holt-Oram Syndrome with obvious limb malformations.
References
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, M.B.B.S. [2]; Assistant Editor(s)-In-Chief: Kristin Feeney, B.S. [3]
Overview
Atrial septal defects are the most common form of congenital heart disease, accounting for 20-40% of all congenital heart disease cases in adults. The Centers for Disease Control and Prevention (CDC) estimated that each year about 1,966 babies in the United States are born with an atrial septal defect.[1]Atrial septal defects can be classified into : ostium secundum, ostium primum, sinus venosus, coronary sinus ASDs and common or single atrium defects. Collectively, atrial septal defects account for 10% of all congenital heart disease. Infants and adolescent patients may be asymptomatic until later in life. By 40 years of age, approximately 90% of untreated atrial septal defect patients will experience an onset of symptoms.
Epidemiology and Demographics
Prevalence
There are four major types of atrial septal defects, ostium secundum, ostium primum, sinus venosus and coronary sinus type [2]
- The ostium secundum defect is the commonest type of atrial septal defect. It constitutes 75% of all types of atrial septal defect. It accounts for 7% of all congenital heart defects and 30-40% of all congenital heart disease in patients aged 40 or older.
- The ostium primum defect is the second most common type of atrial septal defect. It accounts for 15-20% of all atrial septal defects. This particular form of atrial septal defect is also categorized as an atrioventricular septal defect and is associated with mitral valve abnormalities.
- The sinus venosus defect is the third most common form of atrial septal defect. It accounts for 5-10% of all atrial septal defects. It is commonly associated with anomalous connection of the right-sided pulmonary veins and often requires additional imaging tests in diagnosis.
- The coronary sinus ASD is the least common and forms less than 1% of all types of atrial septal defect.
- Another form of inter-atrial communication is patent foramen ovale. A patent foramen ovale is not an atrial septal defect as no septal tissue is missing. (PFOs) are quite common (appearing in 10 – 20% of adults) but are asymptomatic and therefore undiagnosed.
Age
- By 40 years of age, approximately 90% of untreated atrial septal defect patients will experience an onset of symptoms.
- Prior to 40, patients may be entirely asymptomatic and live without complication.
Pediatrics
- As a group, atrial septal defects (ASDs) are detected in 1 child per 1500 live births.
- It accounts for 10% of all congenital heart disease.
Adults
- ASDs make up 20-40% of all congenital heart disease that is seen in adults and are the most common form of congenital heart defect in adults besides bicuspid aortic valve and mitral valve prolapse.[3]
Gender
- In general, atrial septal defect shows a female preponderance, with a female-to-male ratio of 2:1.[4]
References
- ↑ Parker, SE.; Mai, CT.; Canfield, MA.; Rickard, R.; Wang, Y.; Meyer, RE.; Anderson, P.; Mason, CA.; Collins, JS. (2010). “Updated National Birth Prevalence estimates for selected birth defects in the United States, 2004-2006”. Birth Defects Res A Clin Mol Teratol. 88 (12): 1008–16. doi:10.1002/bdra.20735. PMID 20878909. Unknown parameter
|month=ignored (help) - ↑ Fuster V, Brandenburg RO, McGoon DC, Giuliani ER (1980). “Clinical approach and management of congenital heart disease in the adolescent and adult”. Cardiovasc Clin. 10 (3): 161–97. PMID 6991111.
- ↑ Kaplan S (1993). “Congenital heart disease in adolescents and adults. Natural and postoperative history across age groups”. Cardiol Clin. 11 (4): 543–56. PMID 8252558.
- ↑ Feldt R, Avasthey P, Yoshimasu F, Kurland L, Titus J (1971). “Incidence of congenital heart disease in children born to residents of Olmsted County, Minnesota, 1950-1969”. Mayo Clin Proc. 46 (12): 794–9. PMID 5128021.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, M.B.B.S. [2]; Assistant Editor(s)-In-Chief: Kristin Feeney, B.S. [3]
Overview
As is common with most congenital heart conditions, the exact cause of atrial septal defect is not known. Research suggests a potential link between genetic conditions such as Down syndrome and the development of an atrial septal defect. Other potential causes include exposure to environmental contaminants such as rubella as well as alcohol consumption. A clinician should encourage families with a history of congenital heart defect to consider genetic counseling to identify potential risks.
Risk Factors
Although the cause(s) of atrial septal defects are not known, some factors have been found associated with an increased risk of developing an atrial septal defect:
- Increased familial occurrence: Secundum atrial septal defects have been found to occur with an increased frequency among members of a family. In a study done by Whittemore et al. the risk of having congenital heart disease in a child born to a mother with congenital heart disease has been found to somewhere between 8% to 10%.[1][2]
- Genetics: In some studies the genes responsible for atrial septal defects have been shown to be located on chromosome 5. Researchers have observed that an autosomal dominant inheritance with mutations occur within the cardiac transcription factor[3]. These heart defects have been found to be associated with some skeletal abnormalities like Holt-Oram syndrome [4]. Additionally, both secundum and primum ASDs have been found to be associated with trisomy 21 (Down syndrome)
- Maternal health: Some general factors in the mother that may increase the risk of congenital heart diseases include
- Associated conditions: The cause of atrial septal defect is not known. Atrial septal defects are often associated with other malformations such as:
- Partially anomalous pulmonary venous return
- Pulmonary valve stenosis
- Mitral stenosis or mitral valve prolapse
- Ventricular septal defects
- Coarctation of the aorta
References
- ↑ Whittemore R, Wells JA, Castellsague X (1994). “A second-generation study of 427 probands with congenital heart defects and their 837 children”. J Am Coll Cardiol. 23 (6): 1459–67. PMID 8176107.
- ↑ Benson DW, Sharkey A, Fatkin D, Lang P, Basson CT, McDonough B; et al. (1998). “Reduced penetrance, variable expressivity, and genetic heterogeneity of familial atrial septal defects”. Circulation. 97 (20): 2043–8. PMID 9610535.
- ↑ Schott JJ, Benson DW, Basson CT, Pease W, Silberbach GM, Moak JP; et al. (1998). “Congenital heart disease caused by mutations in the transcription factor NKX2-5”. Science. 281 (5373): 108–11. PMID 9651244.
- ↑ HOLT M, ORAM S (1960). “Familial heart disease with skeletal malformations”. Br Heart J. 22: 236–42. PMC 1017650. PMID 14402857.
- ↑ 5.0 5.1 Tikkanen J, Heinonen OP (1992). “Risk factors for atrial septal defect”. Eur J Epidemiol. 8 (4): 509–15. PMID 1397217.
Natural History and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, M.B.B.S. [2]; Assistant Editor(s)-In-Chief: Kristin Feeney, B.S. [3]
Overview
Infants and adolescent patients may be asymptomatic until later in life. By 40 years of age, approximately 90% of untreated atrial septal defect patients will experience an onset of symptoms. Symptom onset and severity is largely dependent upon the size of the defect. Without intervention prior to the development of Eisenmenger’s syndrome, the mortality rate for symptomatic adults is greater than 50%. Possible complications include atrial fibrillation, pulmonary hypertension and stroke.
Natural History
As many atrial septal defect patients are asymptomatic, it is common to survive into adulthood without any need for intervention. Many atrial septal defects smaller than 8 mm in diameter close spontaneously during infancy. Spontaneous closure is uncommon in children and adults. During adulthood there can be the onset of symptoms and an altered life expectancy. Beyond 40-50 years of age, survival without intervention is under 50% with a mortality rate of about 6% per year. Complications occur later in life and include atrial fibrillation, pulmonary hypertension, and stroke.
In a study involving 128 adult (age range 18 to 67 years) atrial septal defect patients, 75% were found to be symptomatic with mild to moderate non-progressive symptoms. Less than 25% of patients had significant pulmonary artery hypertension. Pulmonary artery involvement can be progressive and can lead to shunt reversal, Eisenmenger’s syndrome and ultimately death. The prognosis following medical and / or surgical treatment of pulmonary hypertension can be poor. Heart failure and atrial arrhythmias were other complications found associated with atrial septal defects, mostly in elderly patients.[1]
Complications
Atrial septal defect is associated with complications such as atrial fibrillation, pulmonary hypertension, heart failure, and stroke.
Atrial Septal Defect and Atrial Fibrillation
50-60% of atrial septal defect patients over the age of 40 will develop atrial fibrillation. Late-onset atrial fibrillation is associated with both morbidity and mortality. Anticoagulation may lower the mortality risk. Closing an ASD at this point does not prevent occurrence of atrial fibrillation in these patients. But early closure of ASD lowers the risk of developing atrial fibrillation.
Atrial Septal Defect and Pulmonary Hypertension
15-20% of atrial septal defect patients develop pulmonary hypertension. Although rare in children and adolescents, pulmonary arterial hypertension is observed in approximately 50% of patients over the age of 40. The development of Eisenmenger’s syndrome can result in reversal of the original left-to-right shunt which may switch to become a right-to-left shunt. Right-to-left shunting can in turn lead to deoxygenation (hypoxemia and cyanosis).
Atrial Septal Defect and Right Heart Failure
Atrial septal defect is associated with left-to-right shunting which in turn may be associated with right ventricular volume overload. Patients may experience right heart failure as a result of right ventricular volume overload.
Atrial Septal Defect and Stroke
Even without surgery, as many as 5-10% of all atrial septal defect patients experience thromboembolic events such as stroke and transient ischemic attack. Paradoxical emboli in atrial septal defect patients is not correlated with defect size and can occur in all ASD patients. Early closure of ASD lowers the risk of developing atrial fibrillation.
Prognosis
The prognosis for most atrial septal defect patients, especially prior to the age of 40, is positive. As atrial septal defect patients age, symptoms and complications may advance and influence quality of life. With surgical intervention, the mortality rate is less than 1% for atrial septal defect patients under 45. Surgical intervention in older populations is equally promising and can result in longer longevity and improvements in quality of life. Left untreated, the prognosis for atrial septal defect patients is significantly less favorable and may lead to earlier death.
- Most atrial septal defect patients live to advance in age.
- If an atrial septal defect is detected and diagnosed early in life, surgery is most successful when performed at 2-4 years of age.
- As atrial septal defect patients age, mortality rates of surgical intervention repair increases linearly with age and pulmonary artery pressure.
- The mortality rate for surgical intervention repair is less than 1% for atrial septal defect patients under the age of 45, with no pulmonary artery pressure issues.
- Repair is normally only performed in youth with clinically significant complications. Surgery is still advised for all patients with uncomplicated ASDs with clinically significant shunting from left-to-right. Patients with normal pulmonary artery pressure have comparable age and sex matched 30-year survival rates until the age of 40.
- Patients with pulmonary artery pressure issues may experience a lower survival rate.
- Life expectancy in surgical therapy older patients, though, is better than that of patients with medical therapy. In a small population of patients over the age of 60, presenting without comorbodities, still benefit from surgical intervention.
- In general, surgical intervention of an ASD is associated with an increase in mortality. However, the age of the patient at the time of surgical closure is the single most important predictor of development of potentially serious life-threatening comorbidities.
- Most types of atrial septal defects, when repaired with surgical intervention, are associated with low mortality and low morbidity risks.
- In children, surgical repair can even result in reduction in the right ventricular size from abnormal to closer to normal. Size reduction is not as common in adults with only 20% of all repairs experiencing changes in dimensions. Patients with tricuspid regurgitation and right ventricular failure may experience lifelong symptoms and may have differed long-term outcomes.
- Complications are more common in older atrial septal defect patients after surgical intervention. It is believed that prognosis is influenced by the long-term effect of volume overload on the chambers of the right side. It is also associated with the volume overload as a result of right atrial enlargement and of pulmonary hypertension. These particular strains on the right chamber of the heart lead to increased risk for atrial arrhythmia and stroke. As many as 22% of late deaths can be attributed to cerebrovascular events. Age at repair as well as preoperative status, such as NYHA class III and IV heart failure, are independent predictors of mortality.
References
Complications
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, M.B.B.S. [2]; Cafer Zorkun, M.D., Ph.D. [3] Ayokunle Olubaniyi, M.B,B.S [4]Assistant Editor(s)-In-Chief: Kristin Feeney, B.S. [5]
Overview
Atrial septal defect is associated with complications such as migraine headache with aura, atrial fibrillation, pulmonary hypertension, heart failure, and stroke.
Complications
Atrial Septal Defect and Migraine Headache with Aura (MHA)
A relationship between migraine with aura and right-to-left shunt or patent foramen ovale has been documented in many studies.[1] Patent foramen ovale is more common in patients with migraine headache with aura than in the general population. The prevalence of PFO in migraineurs varies between 40 – 60% as compared to 17 – 30% of people in the general population.[2] In a study, the prevalence of PFO in migraineurs with aura was found to be 47% as compared to 17% among the control subjects. The presence of a large shunt may also increase the odds of having MHA by more than 7-folds.[3] A recent meta-analysis suggests a 3-fold increase in the risk of patients with PFO developing MHA.[4] In a similar manner, migraine with aura is more prevalent in the presence of PFO.
Although the exact causal relationship remains unclear, several pathogenetic mechanisms have been explained, namely:
- Co-inheritance – An autosomal dominant inheritance of atrial shunts was linked to the inheritance of MHA.[5]
- Increased neuronal excitability – Right-to-left shunting of blood exposes neurons to microemboli or vasoactive peptides such as serotonin, which triggers migraine attacks by lowering the neuronal excitability threshold.
- Reduced plasma atrial natriuretic peptide – Atrial natriuretic peptide, which is released by atrial myocytes in response to atrial stretch, is known to play roles in natriuresis, inhibition of platelet aggregation[6] and lowering of vasoreactivity of vascular smooth muscles to vasoconstrictor substances (i.e., it helps in vasodilation). As a result of increased blood volume observed in atrial shunts, patients with ASD have elevated levels of ANP, which subsequently normalizes following closure in majority of patients.[7] As a direct result of this, migraine auras may be facilitated due to the lack of vasodilatory and antiplatelet activities in vulnerable patients.
PFO Closure
Although there is no direct evidence to link migraines and atrial septal defects, some researchers noted that closure of patent foramen ovale resulted in complete resolution or marked reduction in severity and frequency of migraine episodes.[8][9][10][11] A meta-analysis study involving 1,306 patients who underwent PFO closure reported 46% of cases with complete resolution of migraine symptoms and a significant improvement of migraine in 83% of cases.[12] Conversely, there were also reported cases of an increased frequency and severity of migraine attacks with prolonged aura symptoms following closure,[13][14] especially with the closure of secundum ASD.
The MIST (Migraine Intervention with STARFlex Technology) trial which is the only completed randomized trial for PFO closure for migraine headaches was highly critiqued for its failure in reaching its primary and secondary endpoints.[15] The ongoing PREMIUM and the terminated PRIMA randomized controlled trials promises to investigate the role of PFO closure in migraine patients and address the methodological flaws of the MIST trial.[16]
Currently, no conclusion can be drawn from all these studies, but available evidence suggests that PFO is not a risk factor for migraine headaches with aura.
Atrial Septal Defect and Stroke
Even without surgery, as many as 5-10% of all atrial septal defect patients experience thromboembolic events such as stroke and transient ischemic attack. Paradoxical emboli in atrial septal defect patients is not correlated with shunt size and can occur in all ASD patients. Early closure of ASD lowers the risk of developing atrial fibrillation.
Atrial Septal Defect and Atrial Fibrillation
50-60% of atrial septal defect patients over the age of 40 will develop atrial fibrillation. Late-onset atrial fibrillation is associated with bothmorbidity and mortality. Anticoagulation may lower the mortality risk. Closing an ASD at this point does not prevent occurrence of atrial fibrillation in these patients. But early closure of ASD lowers the risk of developing atrial fibrillation.
Atrial Septal Defect and Pulmonary Hypertension
15-20% of atrial septal defect patients develop pulmonary hypertension. Although rare in children and adolescents, pulmonary arterial hypertension is observed in approximately 50% of patients over the age of 40. The development of Eisenmenger’s syndrome can result in reversal of the original left-to-right shunt which may switch to become a right-to-left shunt. Right-to-left shunting can in turn lead to deoxygenation (hypoxemia and cyanosis).
Atrial Septal Defect and Right Heart Failure
Atrial septal defect is associated with left-to-right shunting which in turn may be associated with right ventricular volume overload. Patients may experience right heart failure as a result of right ventricular volume overload.
References
- ↑ Anzola, GP.; Magoni, M.; Guindani, M.; Rozzini, L.; Dalla Volta, G. (1999). “Potential source of cerebral embolism in migraine with aura: a transcranial Doppler study”. Neurology. 52 (8): 1622–5. PMID 10331688. Unknown parameter
|month=ignored (help) - ↑ Del Sette, M.; Angeli, S.; Leandri, M.; Ferriero, G.; Bruzzone, GL.; Finocchi, C.; Gandolfo, C. “Migraine with aura and right-to-left shunt on transcranial Doppler: a case-control study”. Cerebrovasc Dis. 8 (6): 327–30. PMID 9774749.
- ↑ Schwerzmann, M.; Nedeltchev, K.; Lagger, F.; Mattle, HP.; Windecker, S.; Meier, B.; Seiler, C. (2005). “Prevalence and size of directly detected patent foramen ovale in migraine with aura”. Neurology. 65 (9): 1415–8. doi:10.1212/01.wnl.0000179800.73706.20. PMID 16148260. Unknown parameter
|month=ignored (help) - ↑ Schwedt, TJ.; Demaerschalk, BM.; Dodick, DW. (2008). “Patent foramen ovale and migraine: a quantitative systematic review”. Cephalalgia. 28 (5): 531–40. doi:10.1111/j.1468-2982.2008.01554.x. PMID 18355348. Unknown parameter
|month=ignored (help) - ↑ Schwerzmann, M.; Nedeltchev, K.; Meier, B. (2007). “Patent foramen ovale closure: a new therapy for migraine”. Catheter Cardiovasc Interv. 69 (2): 277–84. doi:10.1002/ccd.20966. PMID 17253601. Unknown parameter
|month=ignored (help) - ↑ Ulker, S.; Akgür, S.; Evinç, A.; Soykan, N.; Koşay, S. (1995). “Platelet aggregation and atrial natriuretic peptide”. Gen Pharmacol. 26 (6): 1409–12. PMID 7590139. Unknown parameter
|month=ignored (help) - ↑ Erbay, AR.; Yilmaz, MB.; Balci, M.; Sabah, I. (2004). “Atrial natriuretic peptide levels in adult patients before and after surgery for correction of atrial septal defects: relationship with atrial arrhythmias”. Clin Sci (Lond). 107 (3): 297–302. doi:10.1042/CS20040141. PMID 15142035. Unknown parameter
|month=ignored (help) - ↑ Azarbal B, Tobis J, Suh W, Chan V, Dao C, Gaster R (2005). “Association of interatrial shunts and migraine headaches: impact of transcatheter closure”. J Am Coll Cardiol. 45 (4): 489–92. PMID 15708691.
- ↑ Adams H (2004). “Patent foramen ovale: paradoxical embolism and paradoxical data”. Mayo Clin Proc. 79 (1): 15–20. PMID 14708944.
- ↑ Giardini, A.; Donti, A.; Formigari, R.; Salomone, L.; Palareti, G.; Guidetti, D.; Picchio, FM. (2006). “Long-term efficacy of transcatheter patent foramen ovale closure on migraine headache with aura and recurrent stroke”. Catheter Cardiovasc Interv. 67 (4): 625–9. doi:10.1002/ccd.20699. PMID 16548006. Unknown parameter
|month=ignored (help) - ↑ Reisman, M.; Christofferson, RD.; Jesurum, J.; Olsen, JV.; Spencer, MP.; Krabill, KA.; Diehl, L.; Aurora, S.; Gray, WA. (2005). “Migraine headache relief after transcatheter closure of patent foramen ovale”. J Am Coll Cardiol. 45 (4): 493–5. doi:10.1016/j.jacc.2004.10.055. PMID 15708692. Unknown parameter
|month=ignored (help) - ↑ Butera, G.; Biondi-Zoccai, G.; Sangiorgi, G.; Abella, R.; Giamberti, A.; Bussadori, C.; Sheiban, I.; Saliba, Z.; Santoro, T. (2011). “Percutaneous versus surgical closure of secundum atrial septal defects: a systematic review and meta-analysis of currently available clinical evidence”. EuroIntervention. 7 (3): 377–85. doi:10.4244/EIJV7I3A63. PMID 21729841. Unknown parameter
|month=ignored (help) - ↑ Riederer, F.; Kaya, M.; Christina, P.; Harald, G.; Peter, W. “Migraine with aura related to closure of atrial septal defects”. Headache. 45 (7): 953–6. doi:10.1111/j.1526-4610.2005.05166_2.x. PMID 15985118.
- ↑ Yankovsky, AE.; Kuritzky, A. (2003). “Transformation into daily migraine with aura following transcutaneous atrial septal defect closure”. Headache. 43 (5): 496–8. PMID 12752756. Unknown parameter
|month=ignored (help) - ↑ Dowson, A.; Mullen, MJ.; Peatfield, R.; Muir, K.; Khan, AA.; Wells, C.; Lipscombe, SL.; Rees, T.; De Giovanni, JV. (2008). “Migraine Intervention With STARFlex Technology (MIST) trial: a prospective, multicenter, double-blind, sham-controlled trial to evaluate the effectiveness of patent foramen ovale closure with STARFlex septal repair implant to resolve refractory migraine headache”. Circulation. 117 (11): 1397–404. doi:10.1161/CIRCULATIONAHA.107.727271. PMID 18316488. Unknown parameter
|month=ignored (help) - ↑ Tepper, SJ.; Cleves, C.; Taylor, FR. (2009). “Patent foramen ovale and migraine: association, causation, and implications of clinical trials”. Curr Pain Headache Rep. 13 (3): 221–6. PMID 19457283. Unknown parameter
|month=ignored (help)
Diagnosis
History and Symptoms | Physical Examination | Chest X Ray | Electrocardiogram | Echocardiography | Transcranial Doppler Ultrasound | MRI | CT | Cardiac Catheterization | Exercise Testing | ACC/AHA Guidelines for Evaluation of Unoperated Patients
Treatment
Treatment
Medical Therapy | Indications For Surgical Repair | Surgical Closure | Minimally Invasive Repair | Percutaneous Closure | Robotic ASD Repair | Post Surgical Follow Up
Special Scenarios
Special Scenarios
Pregnancy | Diving and Decompression Sickness | Paradoxical Emboli | Pulmonary Hypertension | Eisenmenger’s Syndrome | Atmospheric Pressure
Related Chapters
Related Chapters
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH