
Bicuspid aortic stenosis
For patient information, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Varun Kumar, M.B.B.S. [2]; Usama Talib, BSc, MD [3]
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Varun Kumar, M.B.B.S. [2]; Usama Talib, BSc, MD [3]
Overview
A normal aortic valve has three leafs (it is a tricuspid valve), but some patients are born with a congenital abnormality in which the aortic valve has two leaflets (a bicuspid aortic valve)[1].
Pathophysiology
A congenital bicuspid aortic valve may be associated with the development of either progressive clacific stenosis or regurgitation. What differentiates the pathophysiology of bicuspid aortic stenosis from other forms of aortic stenosis such as the degenerative aortic stenosis is the presence of concomitant valve disease, aortic root disease, and an increased incidence of coarctation of the aorta.[2]
Epidemiology and Demographics
In this condition, instead of three valve cusps, the aortic valve has two cusps which results from the fusing of one of the commissures. Bicuspid aortic stenosis is the most common congenital abnormality of the heart accounting for 5% of congenital heart defects and it occurs in 1-2% of the population. It can be manifested as a murmur and usually has no long term health consequences, but if it does, the manifestation of aortic stenosis occurs 10 years earlier.
Risk Factors
Risk factors of bicuspid aortic valve to progress to stenosis are hypercholesterolaemia, hypertension and asymmetrical leaflets.[3]
Screening
First degree relatives of patients with bicuspid aortic valves should be screened using echocardiogram for its presence as there are evidence of familial clustering with autosomal dominant inheritance pattern.[4]
Natural History
Typically, aortic stenosis due to calcification of a bicuspid valve appears earlier, at 40 to 50 years of age, whereas that due to calcification and degeneration of a tricuspid aortic valve appears later, at 70 to 80 years of age.
Videos
Below is the video of Dr. Lars Svensson, Cardiothoracic Surgeon and Director of the Aorta Center, at the Cleveland Clinic giving an overview of bicuspid aortic valve and its management. {{#ev:youtube|n5V6ISV3VuA}}
References
- ↑ “Yale Atlas of Echo- Bicuspid aortic valve”. Retrieved 2007-08-08.
- ↑ Girdauskas E, Rouman M, Disha K, Dubslaff G, Fey B, Theis B; et al. (2016). “Aortopathy in Bicuspid Aortic Valve Stenosis with Fusion of Right-Left versus Right-Non-Coronary Cusps: Are These Different Diseases?”. J Heart Valve Dis. 25 (3): 262–269. PMID 27989035.
- ↑ Valdis M, DeRose G, Guo L, Chu MW (2016). “Ross, Hybrid Arch, and Frozen Elephant Trunk Reconstruction for Late Complications of Bicuspid Aortic Valve and Aortopathy”. Can J Cardiol. 32 (12): 1576.e11–1576.e14. doi:10.1016/j.cjca.2016.07.004. PMID 27884484.
- ↑ Gago-Díaz M, Brion M, Gallego P, Calvo F, Robledo-Carmona J, Saura D; et al. (2016). “The genetic component of bicuspid aortic valve and aortic dilation. An exome-wide association study”. J Mol Cell Cardiol. 102: 3–9. doi:10.1016/j.yjmcc.2016.11.012. PMID 27894865.
Anatomy
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Varun Kumar, M.B.B.S. [2]; Usama Talib, BSc, MD [3]
Overview
The Bicuspid Aortic Valve has two cusps: one larger than the other. It is considered unobstructive if the edges of the cusps are free. If the edges are fused or no free the aortic valve is considered obstructive developing a dome during systole.[1]
Anatomy
Bicuspid aortic valve have two distinct anatomical configurations:[2]
- Antero-posterior orientation of the commissures resulting in right and left cusps. This occurs in approximately 53 percent of cases. The right coronary artery originates from the right cusp and the left coronary from the left cusp. The false raphe is present in right cusp.
- 47 percent of patients have commissures on right and left sides of annulus resulting in anterior and posterior cusps. The ostia of both coronary arteries and the false raphe are present in anterior cusp.
There are five varieties of congenitally abnormal aortic valves based on the number and types of cusps and commisures:[3][4][5]
- Unicuspid:
- Acommissural
- Unicommissural
- Bicuspid
- Tricuspid:
- Miniature (small aortic ring)
- Dysplastic
- Cuspal inequality
- Quadricuspid
- Six-cuspid
| Here is a bicuspid aortic valve compared with a normal aortic valve: | |
|---|---|
 |
 |
References
- ↑ Gago-Díaz M, Brion M, Gallego P, Calvo F, Robledo-Carmona J, Saura D; et al. (2016). “The genetic component of bicuspid aortic valve and aortic dilation. An exome-wide association study”. J Mol Cell Cardiol. 102: 3–9. doi:10.1016/j.yjmcc.2016.11.012. PMID 27894865.
- ↑ Roberts WC (1970). “The congenitally bicuspid aortic valve. A study of 85 autopsy cases”. The American Journal of Cardiology. 26 (1): 72–83. PMID 5427836. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Hamatani Y, Ishibashi-Ueda H, Nagai T, Sugano Y, Kanzaki H, Yasuda S; et al. (2016). “Pathological Investigation of Congenital Bicuspid Aortic Valve Stenosis, Compared with Atherosclerotic Tricuspid Aortic Valve Stenosis and Congenital Bicuspid Aortic Valve Regurgitation”. PLoS One. 11 (8): e0160208. doi:10.1371/journal.pone.0160208. PMC 4968844. PMID 27479126.
- ↑ Kwon HJ, Park JH, Kim SS, Sun BJ, Jin SA, Kim JH; et al. (2016). “Severe Aortic Stenosis Associated with Unicommissural Unicuspid Aortic Valve in a Middle Aged Male”. J Cardiovasc Ultrasound. 24 (3): 247–250. doi:10.4250/jcu.2016.24.3.247. PMC 5050315. PMID 27721957.
- ↑ Sangalli F, Formica F, Avalli L, Paolini G (2005). “Quadricuspid aortic valve as a cause of severe aortic regurgitation”. Ital Heart J. 6 (2): 157–9. PMID 15819511.
Historical perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Usama Talib, BSc, MD [2]
Overview
In 1513, Leonardo da Vinci was the first artist who first sketched the bicuspid aortic valve and termed it “cuspal inquelity”. [1]
References
- ↑ Ratib O, Perloff JK, Child JS (2004). “Images in cardiovascular medicine. Bicuspid aortic valve aneurysm”. Circulation. 109 (5): 671. doi:10.1161/01.CIR.0000115643.50179.6E. PMID 14769689.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Usama Talib, BSc, MD [3]
Overview
A congenital bicuspid aortic valve may be associated with the development of either progressive clacific stenosis or regurgitation. What differentiates the pathophysiology of bicuspid aortic stenosis from other forms of aortic stenosis such as the degenerative aortic stenosis is the presence of concomitant valve disease, aortic root disease, and an increased incidence of coarctation of the aorta.[1]
Pathophysiology of Aortic Stenosis
The pathophysiology of aortic stenosis is described in the main chapter on the pathophysiology of aortic stenosis here. What differentiates the pathophysiology of bicuspid aortic stenosis from other forms of aortic stenosis such as the degenerative aortic stenosis is the presence of concomitant valve disease, aortic root disease, and an increased incidence of coarctation of the aorta.[2]
Incidence of Concomitant Valve Disease
- Only 25% of patients with congenital aortic stenosis (AS) have aortic insufficiency (AI) compared with 75% of cases with acquired AS.
- In 75% of those with acquired AS, there is associated mitral valve disease. This association is rare in congenital AS.
Concomitant Disease of the Aorta
The aorta of patients with bicuspid aortic valve does not have the same histological characteristics of a normal aorta. The tensile strength is reduced. These patients are at a higher risk for aortic dissection and aneurysm formation of the ascending aorta. The size of the proximal aorta should be evaluated carefully during the evaluation of the patient for aortic stenosis surgery. The initial diameter of the aorta should be noted and periodic evaluation with CT scan (every year or sooner if there is a change in aortic diameter) should be recommended. Therefore, if the patient needs surgery, the size of the aorta will determine what type of surgery should be offered to the patient.[3]
Associated Congenital Heart Disease
Patients with bicuspid aortic valve are also at higher risk of aortic coarctation, an abnormal narrowing of the thoracic aorta [4].
Gross Pathology
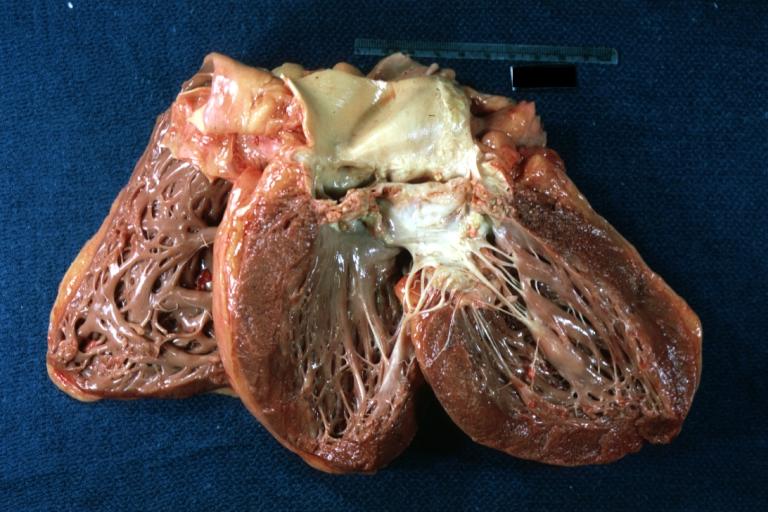
Gross pathologic evaluation in patients with bicuspid aortic stenosis demonstrates fusion of one of the three commisures which results in two functional leaflets instead of the usual three aortic leaflets. Left ventricular hypertrophy is present in bicuspid aortic stenosis.[5]
Pathological Findings
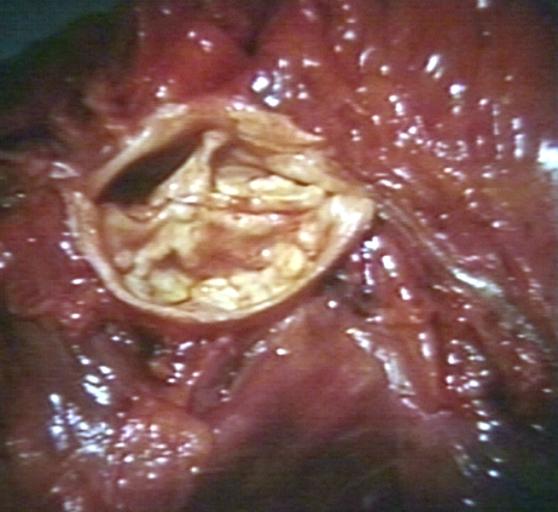
Images shown below are courtesy of Professor Peter Anderson DVM PhD[6] and published with permission.
-
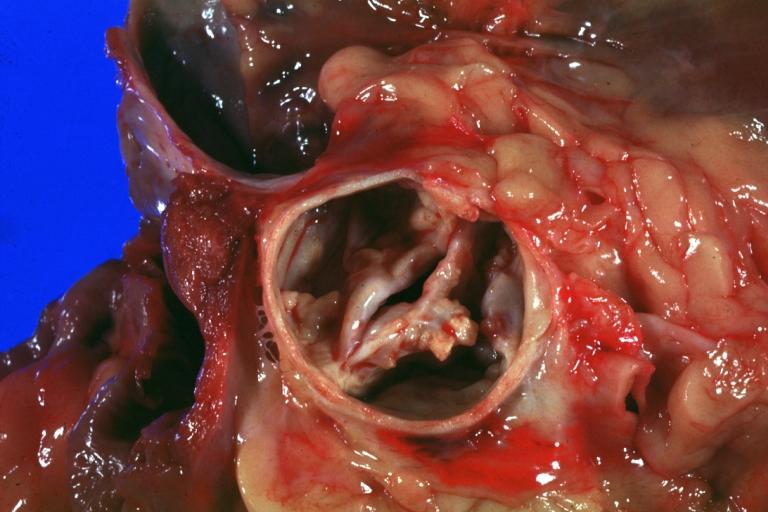
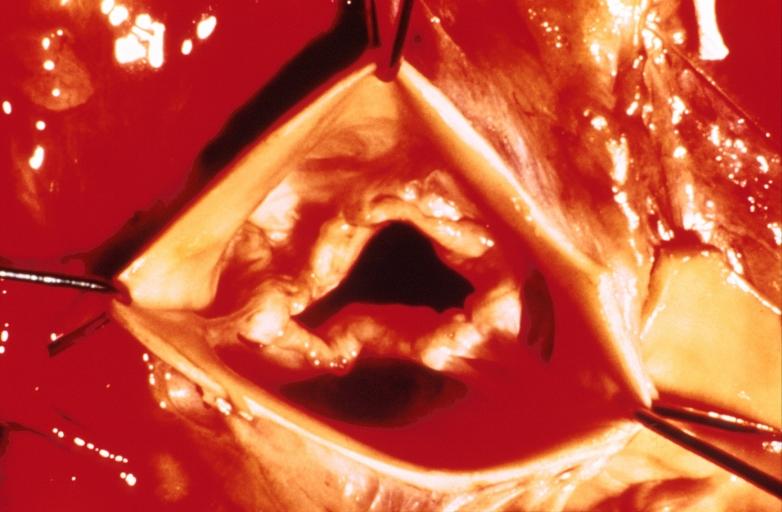
 Aortic Stenosis, Bicuspid valve: Gross; excellent image of bicuspid and calcific valve showing a false raphe.
Aortic Stenosis, Bicuspid valve: Gross; excellent image of bicuspid and calcific valve showing a false raphe. -
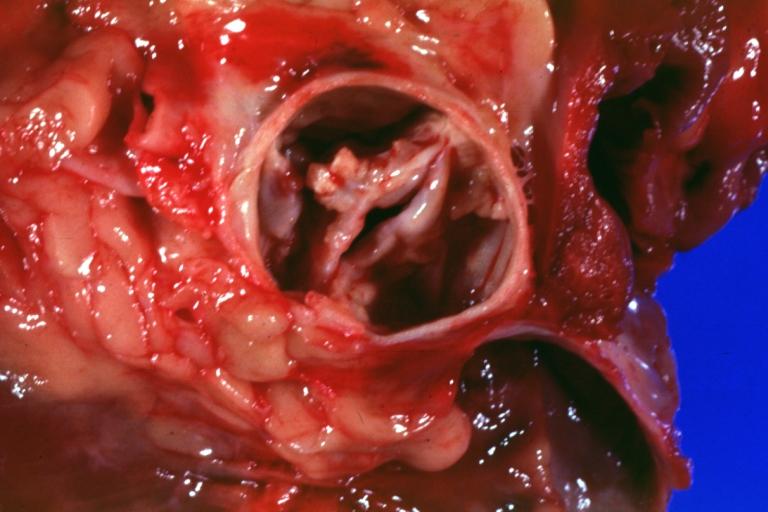
 Aortic Stenosis, Bicuspid valve: Gross; good example of bicuspid valve
Aortic Stenosis, Bicuspid valve: Gross; good example of bicuspid valve


-
 Aortic Stenosis, Bicuspid valve: Gross; image of bicuspid aortic valve, an excellent example
Aortic Stenosis, Bicuspid valve: Gross; image of bicuspid aortic valve, an excellent example -
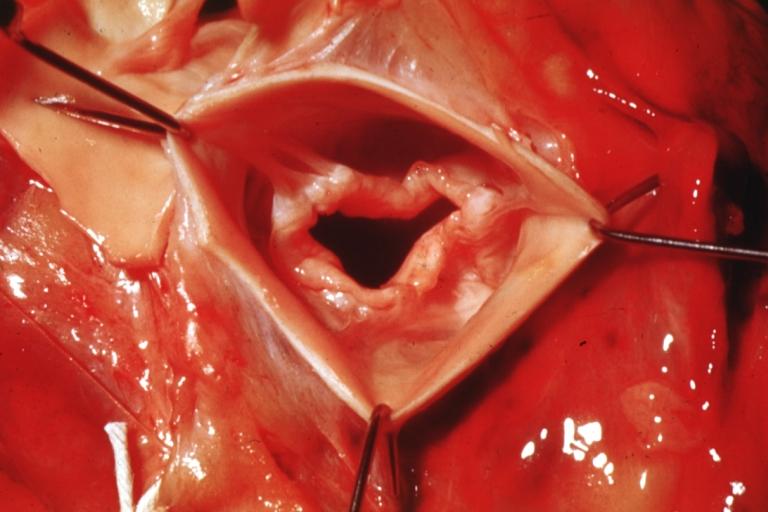
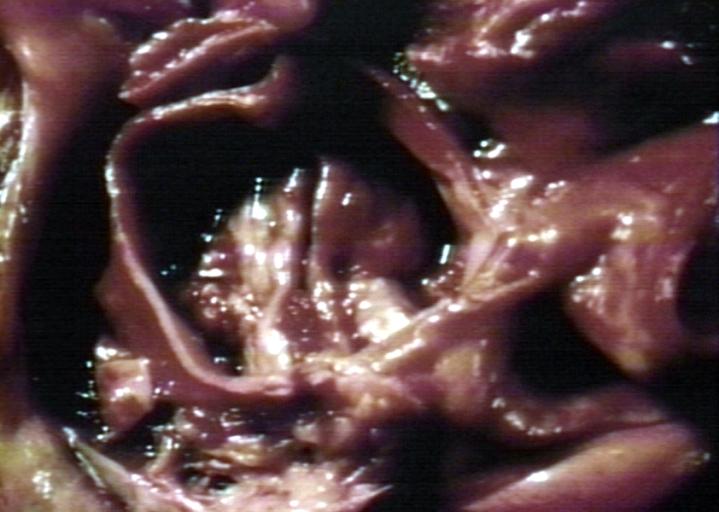
 Aortic Stenosis, Bicuspid valve: Gross; close-up image of bicuspid aortic valve.
Aortic Stenosis, Bicuspid valve: Gross; close-up image of bicuspid aortic valve.


-
 Aortic Stenosis, Bicuspid valve: Gross; close-up image of bicuspid aortic valve.
Aortic Stenosis, Bicuspid valve: Gross; close-up image of bicuspid aortic valve. -
 Bicuspid aortic valve
Bicuspid aortic valve


-
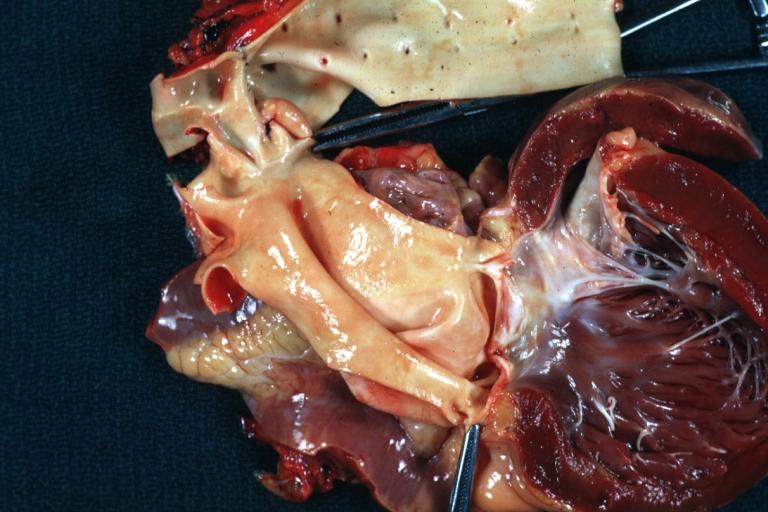
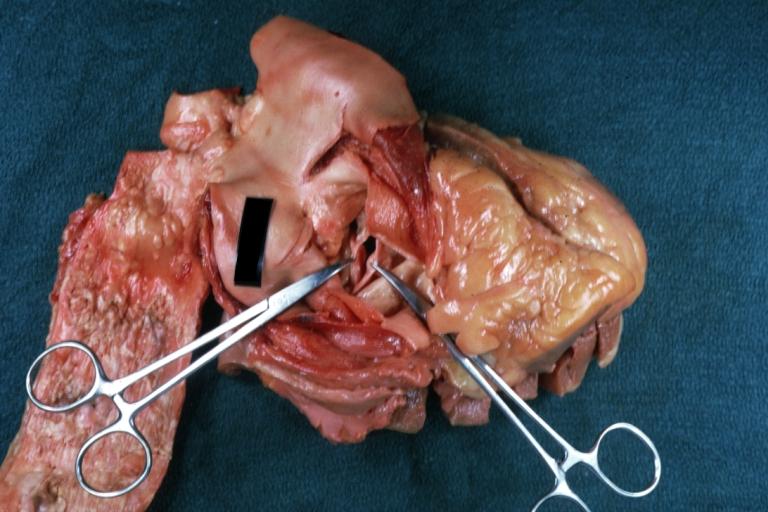 Gross natural color opened first portion aortic arch with bicuspid aortic valve shows stenosis and aortic root is dilated
Gross natural color opened first portion aortic arch with bicuspid aortic valve shows stenosis and aortic root is dilated -
 Aortic Stenosis Bicuspid: Gross; natural color opened left ventricular outflow tract with calcific masses on valve as well as anterior leaflet mitral valve probably did not cause significant stenosis
Aortic Stenosis Bicuspid: Gross; natural color opened left ventricular outflow tract with calcific masses on valve as well as anterior leaflet mitral valve probably did not cause significant stenosis


-
 Bicuspid Aortic Valve with Repaired Aorta Coarctation: Gross natural color opened left ventricular outflow tract with uncomplicated bicuspid aortic valve repaired coarctation barely visible ruptured postoperative young female with ovaries Turner mosaic not ruled out
Bicuspid Aortic Valve with Repaired Aorta Coarctation: Gross natural color opened left ventricular outflow tract with uncomplicated bicuspid aortic valve repaired coarctation barely visible ruptured postoperative young female with ovaries Turner mosaic not ruled out -
 Bicuspid Aortic Stenosis: Gross; fixed tissue
Bicuspid Aortic Stenosis: Gross; fixed tissue


-
 Aortic Stenosis, Bicuspid: Gross; fixed tissue view of stenotic valve through ventricular outlet track
Aortic Stenosis, Bicuspid: Gross; fixed tissue view of stenotic valve through ventricular outlet track -
 Aortic Stenosis Bicuspid: Gross; fixed tissue. Bicuspid valve and false raphe classical
Aortic Stenosis Bicuspid: Gross; fixed tissue. Bicuspid valve and false raphe classical


-
 Bicuspid aortic valve
Bicuspid aortic valve -
 Bicuspid aortic valve
Bicuspid aortic valve


-
 Bicuspid aortic valve
Bicuspid aortic valve -
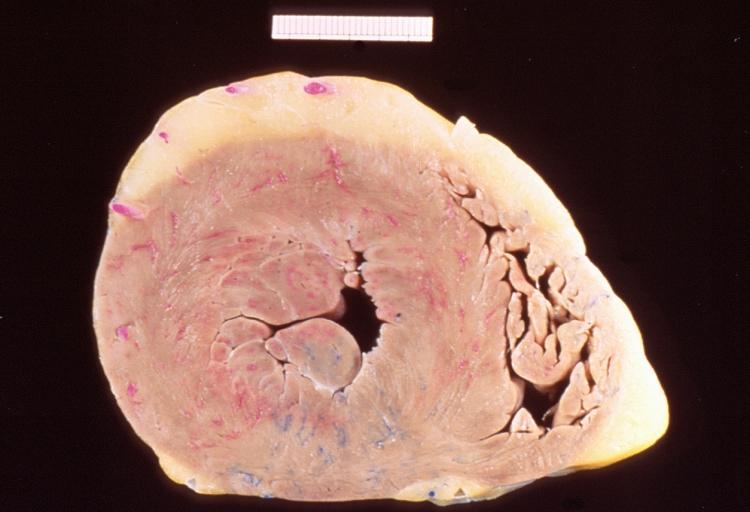 Left ventricular hypertrophy due to bicuspid aortic valve
Left ventricular hypertrophy due to bicuspid aortic valve


References
- ↑ Bonow RO, Carabello BA, Chatterjee K, de Leon AC, Faxon DP, Freed MD; et al. (2008). “2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients with valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons”. J Am Coll Cardiol. 52 (13): e1–142. doi:10.1016/j.jacc.2008.05.007. PMID 18848134.
- ↑ Dweck MR, Boon NA, Newby DE (2012). “Calcific aortic stenosis: a disease of the valve and the myocardium”. J Am Coll Cardiol. 60 (19): 1854–63. doi:10.1016/j.jacc.2012.02.093. PMID 23062541.
- ↑ Zilberszac R, Gabriel H, Schemper M, Laufer G, Maurer G, Rosenhek R (2016). “Asymptomatic Severe Aortic Stenosis in the Elderly”. JACC Cardiovasc Imaging. doi:10.1016/j.jcmg.2016.05.015. PMID 27639763.
- ↑ Cohn LH, Edmunds LH Jr. Cardiac Surgery in the Adult. McGraw-Hill, 2003.
- ↑ Jang JY, Seo JS, Sun BJ, Kim DH, Song JM, Kang DH; et al. (2016). “Impact of Valvuloarterial Impedance on Concentric Remodeling in Aortic Stenosis and Its Regression after Valve Replacement”. J Cardiovasc Ultrasound. 24 (3): 201–207. doi:10.4250/jcu.2016.24.3.201. PMC 5050308. PMID 27721950.
- ↑ http://www.peir.net © PEIR, University of Alabama at Birmingham, Department of Pathology
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Usama Talib, BSc, MD [2]
Overview
In this condition, instead of three valve cusps, the aortic valve has two cusps which results from the fusing of one of the commissures. Bicuspid aortic stenosis is the most common congenital abnormality of the heart accounting for 5% of congenital heart defects and it occurs in 1-2% of the population. It can be manifested as a murmur and usually has no long term health consequences, but if it does, the manifestation of aortic stenosis occurs 10 years earlier.
Genetics
Bicuspid aortic valve has been found to be an inheritable condition, with a demonstrated association with Notch 1.[1] Familial clustering as well as isolated valve defects have been documented. The incidence of bicuspid aortic valve can be as high as 10% to 20% in families affected with the valve problem[2]. Other congential heart defects are associated with bicuspid aortic valve at various frequencies.
Timing of Diagnosis
This condition is often undiagnosed until later in life when the person develops symptomatic aortic stenosis. Aortic stenosis occurs in this condition usually in patients in their 40s or 50s, an average of 10 years earlier than can occur in people with congenitally normal aortic valves. 30% of cases are diagnosed in adolescence.
Incidence of Bicuspid Aortic Valve Disease Versus Degenerative Disease Among Patients with Surgical AS
The congenital bicuspid aortic valve may become calcified, which may lead to half the cases of surgically important pure aortic stenosis in adults, with varying degrees of severity of aortic stenosis and aortic regurgitation.
Male Predominance
Bicuspid aortic stenosis is more common in men than women (3:1 to 5:1).[3]
References
- ↑ Garg V, Muth AN, Ransom JF; et al. (2005). “Mutations in NOTCH1 cause aortic valve disease”. Nature. 437 (7056): 270–4. doi:10.1038/nature03940. PMID 16025100.
- ↑ Kerstjens-Frederikse WS, Du Marchie Sarvaas GJ, et al. Left ventricular outflow tract obstruction: should cardiac screening be offered to first-degree relatives?. Heart. Aug 2011;97(15):1228-32.
- ↑ Simard L, Côté N, Dagenais F, Mathieu P, Couture C, Trahan S; et al. (2016). “Sex-Related Discordance Between Aortic Valve Calcification and Hemodynamic Severity of Aortic Stenosis: Is Valvular Fibrosis the Explanation?”. Circ Res. doi:10.1161/CIRCRESAHA.116.309306. PMID 27879282.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Varun Kumar, M.B.B.S. [2]; Usama Talib, BSc, MD [3]
Overview
Risk factors of bicuspid aortic valve to progress to stenosis are hypercholesterolaemia, hypertension and asymmetrical leaflets.
Risk Factors
Factors affecting the rate of stenosis of bicuspid valves are not clearly defined.
- The rate of calcification of the bicuspid aortic valve depends on:[1]
- Total cholesterol
- Hypertension
- Asymmetrical leaflet sizes as there is more pronounced hemodynamic stress, resulting from straightening and stretching of the leaflets when they are open and close[2]
- Sclerotic changes resulting in stenosis tend to occur at faster rate in patients with:[3]
- Anteroposteriorly located cusps than in those with right-left located cusps
- Asymmetrical leaflet sizes
There are increasing evidences of heritability of bicuspid aortic valves which follows autosomal dominant inheritance pattern.[4][5]
References
- ↑ Chan KL, Ghani M, Woodend K, Burwash IG (2001). “Case-controlled study to assess risk factors for aortic stenosis in congenitally bicuspid aortic valve”. The American Journal of Cardiology. 88 (6): 690–3. PMID 11564401. Retrieved 2012-04-10. Unknown parameter
|month=ignored (help) - ↑ EDWARDS JE (1961). “The congenital bicuspid aortic valve”. Circulation. 23: 485–8. PMID 13725804. Retrieved 2012-04-10. Unknown parameter
|month=ignored (help) - ↑ Beppu S, Suzuki S, Matsuda H, Ohmori F, Nagata S, Miyatake K (1993). “Rapidity of progression of aortic stenosis in patients with congenital bicuspid aortic valves”. The American Journal of Cardiology. 71 (4): 322–7. PMID 8427176. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Huntington K, Hunter AG, Chan KL (1997). “A prospective study to assess the frequency of familial clustering of congenital bicuspid aortic valve”. Journal of the American College of Cardiology. 30 (7): 1809–12. PMID 9385911. Retrieved 2012-04-10. Unknown parameter
|month=ignored (help) - ↑ Cripe L, Andelfinger G, Martin LJ, Shooner K, Benson DW (2004). “Bicuspid aortic valve is heritable”. Journal of the American College of Cardiology. 44 (1): 138–43. doi:10.1016/j.jacc.2004.03.050. PMID 15234422. Retrieved 2012-04-10. Unknown parameter
|month=ignored (help)
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Varun Kumar, M.B.B.S. [2]; Usama Talib, BSc, MD [3]
Overview
First degree relatives of patients with bicuspid aortic valves should be screened using echocardiogram for its presence as there are evidence of familial clustering with autosomal dominant inheritance pattern.[1]
2008 ACC/AHA Guidelines for Screening of Bicuspid Aortic Valve[2]
| “ |
1. Patient referral to a pediatric cardiologist experienced in fetal echocardiography is indicated in the second trimester of pregnancy to search for cardiac defects in the fetus. (Level of Evidence: C) 2. Echocardiographic screening for the presence of bicuspid aortic valve is recommended for first-degree relatives of patients with bicuspid aortic valve. (Level of Evidence: B) |
” |
References
- ↑ Gago-Díaz M, Brion M, Gallego P, Calvo F, Robledo-Carmona J, Saura D; et al. (2016). “The genetic component of bicuspid aortic valve and aortic dilation. An exome-wide association study”. J Mol Cell Cardiol. 102: 3–9. doi:10.1016/j.yjmcc.2016.11.012. PMID 27894865.
- ↑ Warnes CA, Williams RG, Bashore TM, Child JS, Connolly HM, Dearani JA, del Nido P, Fasules JW, Graham TP, Hijazi ZM, Hunt SA, King ME, Landzberg MJ, Miner PD, Radford MJ, Walsh EP, Webb GD (2008). “ACC/AHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to develop guidelines on the management of adults with congenital heart disease)”. Circulation. 118 (23): e714–833. doi:10.1161/CIRCULATIONAHA.108.190690. PMID 18997169. Retrieved 2012-04-10. Unknown parameter
|month=ignored (help)
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Varun Kumar, M.B.B.S. [2]; Usama Talib, BSc, MD [3]
Causes for Bicuspid Aortic Stenosis
- There is increasing evidence that occurrence of bicuspid aortic valve is heriditary with incidence as high as 10-17% in first-degree relatives of probands.[1]
- Hypercholesterolemia accelerates the stenotic process via calcification.
- Other conditions associated with occurrence of bicuspid aortic valves include:
References
- ↑ Cripe L, Andelfinger G, Martin LJ, Shooner K, Benson DW (2004). “Bicuspid aortic valve is heritable”. Journal of the American College of Cardiology. 44 (1): 138–43. doi:10.1016/j.jacc.2004.03.050. PMID 15234422. Retrieved 2012-04-11. Unknown parameter
|month=ignored (help) - ↑ Sachdev V, Matura LA, Sidenko S, Ho VB, Arai AE, Rosing DR, Bondy CA (2008). “Aortic valve disease in Turner syndrome”. Journal of the American College of Cardiology. 51 (19): 1904–9. doi:10.1016/j.jacc.2008.02.035. PMID 18466808. Retrieved 2012-04-11. Unknown parameter
|month=ignored (help) - ↑ Hallidie-Smith KA, Karas S (1988). “Cardiac anomalies in Williams-Beuren syndrome”. Archives of Disease in Childhood. 63 (7): 809–13. PMC 1779091. PMID 3415298. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Duran AC, Frescura C, Sans-Coma V, Angelini A, Basso C, Thiene G (1995). “Bicuspid aortic valves in hearts with other congenital heart disease”. The Journal of Heart Valve Disease. 4 (6): 581–90. PMID 8611973. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Gelb BD, Zhang J, Sommer RJ, Wasserman JM, Reitman MJ, Willner JP (1999). <175::AID-AJMG9>3.0.CO;2-%23 “Familial patent ductus arteriosus and bicuspid aortic valve with hand anomalies: a novel heart-hand syndrome”. American Journal of Medical Genetics. 87 (2): 175–9. PMID 10533032. Retrieved 2012-04-11. Unknown parameter
|month=ignored (help)
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Varun Kumar, M.B.B.S. [2]; Usama Talib, BSc, MD [3]
Natural History
Bicuspid aortic valve, during childhood functions without any significant pressure gradient. However, the thickening and calcification of the valves may be detectable pathologically and on echocardiography by second decade[1]. This progresses to aortic stenosis requiring operative correction in approximately 75% of cases.[2][3]
Bicuspid aortic stenosis progressively leads to heart failure, arrythmias, angina and other symptoms which generally manifests between 40 to 60 years of age which is relatively younger to manifestation of aortic stenosis otherwise.[2] However, children who develop early pathologic changes in bicuspid aortic valve are more likely to develop aortic insufficiency than stenosis.
Complications
Bicuspid aortic valve disease is associated with the following complications:
- Aortic stenosis in the majority (75%) of patients.[2]
- Aortic insufficiency[4][5]
- Endocarditis[6]
- Aortic aneurysm[3]
- Aortic dissection[3]
- Sudden death can occur in children during and immediately after exertion especially among those with pressure gradient > 50 mmHg across the aortic valve.[7]
For complications of aortic stenosis, click here
References
- ↑ Beppu S, Suzuki S, Matsuda H, Ohmori F, Nagata S, Miyatake K (1993). “Rapidity of progression of aortic stenosis in patients with congenital bicuspid aortic valves”. The American Journal of Cardiology. 71 (4): 322–7. PMID 8427176. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ 2.0 2.1 2.2 Fenoglio JJ, McAllister HA, DeCastro CM, Davia JE, Cheitlin MD (1977). “Congenital bicuspid aortic valve after age 20”. The American Journal of Cardiology. 39 (2): 164–9. PMID 835475. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ 3.0 3.1 3.2 Lewin MB, Otto CM (2005). “The bicuspid aortic valve: adverse outcomes from infancy to old age”. Circulation. 111 (7): 832–4. doi:10.1161/01.CIR.0000157137.59691.0B. PMID 15723989. Retrieved 2012-04-10. Unknown parameter
|month=ignored (help) - ↑ Keane MG, Wiegers SE, Plappert T, Pochettino A, Bavaria JE, Sutton MG (2000). “Bicuspid aortic valves are associated with aortic dilatation out of proportion to coexistent valvular lesions”. Circulation. 102 (19 Suppl 3): III35–9. PMID 11082359. Retrieved 2012-04-10. Unknown parameter
|month=ignored (help) - ↑ Roberts WC, Morrow AG, McIntosh CL, Jones M, Epstein SE (1981). “Congenitally bicuspid aortic valve causing severe, pure aortic regurgitation without superimposed infective endocarditis. Analysis of 13 patients requiring aortic valve replacement”. The American Journal of Cardiology. 47 (2): 206–9. PMID 7468467. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Gersony WM, Hayes CJ, Driscoll DJ, Keane JF, Kidd L, O’Fallon WM, Pieroni DR, Wolfe RR, Weidman WH (1993). “Bacterial endocarditis in patients with aortic stenosis, pulmonary stenosis, or ventricular septal defect”. Circulation. 87 (2 Suppl): I121–6. PMID 8425318. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Keane JF, Driscoll DJ, Gersony WM, Hayes CJ, Kidd L, O’Fallon WM, Pieroni DR, Wolfe RR, Weidman WH (1993). “Second natural history study of congenital heart defects. Results of treatment of patients with aortic valvar stenosis”. Circulation. 87 (2 Suppl): I16–27. PMID 8425319. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help)
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Lab Tests | Electrocardiogram | Chest X Ray | CT | MRI | Echocardiography | Cardiac Catheterization
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH