
Ventricular septal defect
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-In-Chief: Priyamvada Singh, MBBS [2]; Cafer Zorkun, M.D., Ph.D. [3];Kalsang Dolma, M.B.B.S.[4] Assistant Editor-In-Chief: Kristin Feeney, B.S. [5]
Synonyms and keywords: VSD
This chapter deals with congenital ventricular septal defect. The chapter on ventricular septal rupture can be found here
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, MBBS [2]; Cafer Zorkun, M.D., Ph.D. [3]; Assistant Editor(s)-In-Chief: Kristin Feeney, B.S. [4]
Overview
A ventricular septal defect (or VSD) is a defect in the ventricular septum (the wall dividing the left and right ventricles of the heart). The ventricular septum consists of a muscular (inferior) and membranous portion (superior). The membranous portion (which is close to the atrioventricular node) is most commonly affected.[1]
Congential VSDs are collectively the most common congenital heart defect. The incidence of VSD in adulthood has decreased over past decades due to successful surgical closure of large defects.[2]
Epidemiology and Demographics
The ventricular septal defect is the most common congenital cardiac malformation with an incidence of 300 to 350 per 100,000 live births,[3] corresponding to 30% of all newborns with a congenital heart defect. There is no predilection based on sex. Incidence rates are similar in different races and seasons and are unrelated to maternal age, birth order, sex, and socioeconomic status. Congential VSDs are frequently associated with other congenital conditions, such as Down syndrome. [4]
Diagnosis
Physical Examination
The physical examination findings of a ventricular septal defect depend upon the size of the defect, the location of the defect, the magnitude and directionality of the intracardiac shunt, and the age of the patient (the duration of the VSD).
CT
Computed tomography can be helpful as a diagnostic tool in conditions where the echocardiographic findings are inconclusive.
MRI
Magnetic resonance imaging can be helpful as a diagnostic tool in conditions where the echocardiographic findings are inconclusive.
References
- ↑ Anderson RH, Ho SY, Becker AE. Anatomy of the human atrioventricular junctions revisited. Anatomical Record 2000;260:81-91
- ↑ Allwork SP, Anderson RH. Developmental anatomy of the membranous part of the ventricular septum in the human heart. Br Heart J 1979; 41:275-280
- ↑ Hoffman JI, Kaplan S (2002). “The incidence of congenital heart disease”. J Am Coll Cardiol. 39 (12): 1890–900. PMID 12084585.
- ↑ Giuliani et al, Cardiology: Fundamentals and Practice, Second Edition, Mosby Year Book, Boston, 1991.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Based on the size of the defect, VSD can be classified into small, medium, and large ventricular septal defects.
Classification
VSDs can be classified into small, medium, and large based on the size of the defect[1]
Small VSDs
There is a small left-to-right shunt (Qp/Qs < 1.5) and a normal ratio of PA to systemic pressures.
Medium-Sized VSDs
There is a moderate shunt left-to-right present (Qp/Qs = 1.5-2.0) that still has some resistance to flow across the defect.
Large VSDs
There is a large defect on the ventricular septum, > 1 cm2/m2 of BSA, with a large shunt left-to-right (Qp/Qs is > 2), causing volume overload of the LV, which may result in its failure. The defect may approximate the size of the aortic orifice.

References
- ↑ Soto B, Becker AE, Moulaert AJ, Lie JT, Anderson RH (1980). “Classification of ventricular septal defects”. Br Heart J. 43 (3): 332–43. doi:10.1136/hrt.43.3.332. PMC 482284. PMID 7437181.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] and Leida Perez, M.D.; Associate Editor(s)-in-Chief: Keri Shafer, M.D. [2]; Priyamvada Singh, M.B.B.S; Omar Toubat
Overview
In ventricular septal defect, a persistent opening in the upper interventricular septum resulting from failure of fusion with the aortic septum allows blood to flow from the high pressure left ventricle into the low pressure chamber or right ventricle. Disruption of the septation process, from inherited perturbations during embryological development or acquired cardiac injury, may result in ventricular septal defects (VSDs).
Pathophysiology
Embryology of VSD
The goal of ventricular septation is to permanently divide a single ventricular cavity into unique right and left chambers. Successful division of the ventricles necessitates a continuous barrier to ensure pulmonary and systemic flow separation in the developed heart. The true interventricular septum is a heterogenous structure composed of a muscular segment and a membranous segment. Disruption of the septation process, from inherited perturbations during embryological development or acquired cardiac injury, may result in ventricular septal defects (VSDs). The most commonly surgically corrected VSDs arise in the fibrous membranous ventricular septum.[1]
Septation of the primitive ventricle into distinct right and left ventricular chambers begins shortly after cardiac looping. In the early stages of bilateral ventricular formation there is a large interventricular communication known as the primary interventricular foramen.[2] However, this defect is temporary and begins to narrow as ventricular ballooning creates an upward muscular growth from the floor of the ventricle.[3] The growth of the primitive muscular septum from its apical origin towards the endocardial cushion arrests before closure of the defect is complete, leaving a secondary interventricular foramen.[4] Eventually the secondary interventricular foramen in sealed, accomplishing the bilateral division of the right and left ventricular chambers. Closure of the secondary interventricular foramen requires the proper convergence of three different tissues:[5]
- The muscular interventricular septum
- The endocardial cushion
- The bulbar septum
Together, the endocardial cushion and the bulbar septum contribute to the formation of the membranous septum, which will intersect the muscular septum and complete the process of ventricular septation.[5]
VSDs develop in the membranous or muscular portions of the ventricular septum. Congenital muscular septal defects can emerge because of non-compaction of the muscular septum, leaving one of many interventricular communications in the postnatal heart.[4] Likewise, improper positioning or growth of any component of the membranous septum also results in abnormal septation.[4] Appropriate ventricular septation is a coordinated effort involving the spatiotemporal placement of several different tissue components. Morphological defects in this complex process are varied and can occur at any point during septation, accounting for the phenotypic dynamism in VSDs.
Anatomy of Ventricular Septum
Click here to learn more about the anatomy of the ventricular septum.
Diagram of VSD

Please click here to learn more about the normal ventricular septum anatomy.
Factors Affecting the Pathophysiology of VSD
- The subsequent natural history and pathophysiology depends on
- The size of the defect
- The magnitude of left-to-right shunting.
- Small defects (QP/QS less than 1.5) maybe asymptomatic, but with the high risk for bacterial endocarditis.
- Large defects are associated with left ventricular failure.
- Chronic but more moderate left-to-right shunts may lead to pulmonary vascular disease and right sided failure.
The primary variable is the size of the defect. As a child grows, the relative size of the defect may decrease and the defect may even close spontaneously in early childhood.
During the first few months of life the PVR decreases, and the magnitude of left-to-right shunt increases. After the first few months the degree of shunting is dependent on the size of the defect.
Presentations in the Adult or Adolescent
a) Small defect without significant left-to-right shunting
b) Large defect with severe pulmonary hypertension and cyanosis due to right-to-left shunt.
c) Large defect with a large left-to-right shunt that has induced secondary infundibular stenosis (tough to differentiate from tetralogy of Fallot).
Small VSDs
A high resistance to flow across the VSD due to the large pressure difference between the two ventricles. There is a small left-to-right shunt (Qp/Qs < 1.5) and a normal ratio of PA to systemic pressures.
There is little or no increase in the pulmonary vascular resistance. A holosystolic murmur is present due to the pressure gradient across the defect. The majority of these defects close during the first three years of life.
Medium-Sized VSDs
There is a moderate left-to-right shunt present (Qp/Qs = 1.5-2.0) that still has some resistance to flow across the defect. There is also volume overload of the LA and the LV and LVH. There may therefore be a mid diastolic mitral murmur and a third heart sound (S3). The ratio of the PA systolic pressure to the systemic pressure is < 5.
The area of the defect is usually less than 1 cm2/m2 of body surface area and is unusual for this group to have a marked increase in PVR. In some cases and depending on the type of VSD, as the child becomes older, the relative size of the defect will decrease.
Large VSDs
There is a large defect on the ventricular septum, > 1 cm2/m2 of BSA, with a large shunt left-to-right (Qp/Qs is > 2), causing volume overload of the LV, which may result in its failure. The defect may approximate the size of the aortic orifice.
The ratio of the PA pressure to the systemic pressure is > 5. Produce the same clinical findings as moderate sized VSD but also pulmonary hypertension.
There is rarely spontaneously closure of the defect, and these patients either die, or progress to adolescence or adulthood with severe pulmonary hypertension or with secondary protective infundibular pulmonary stenosis.
In the group with severe pulmonary hypertension, the left-to-right shunt decreases and the degree of right-to-left shunting increases with accompanying cyanosis (i.e. they develop Eisenmenger’s syndrome).
Protective infundibular stenosis may also result in reversal of the shunt, and may be indistinguishable clinically from tetralogy of Fallot.
Gross Pathology
-
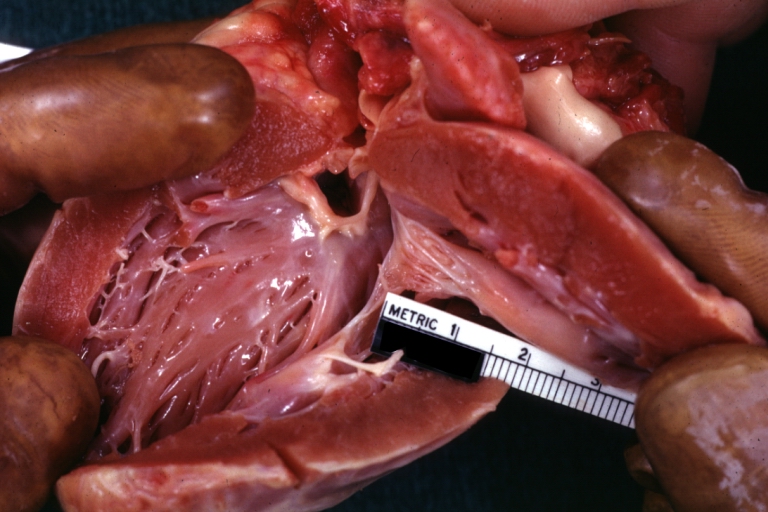
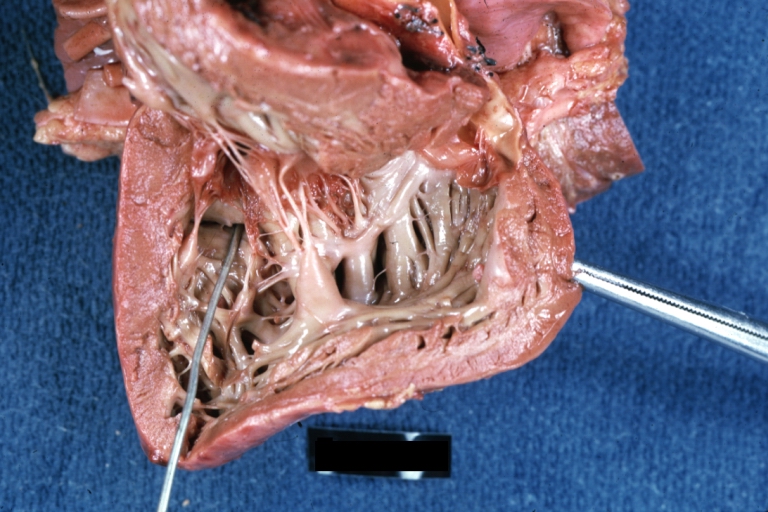
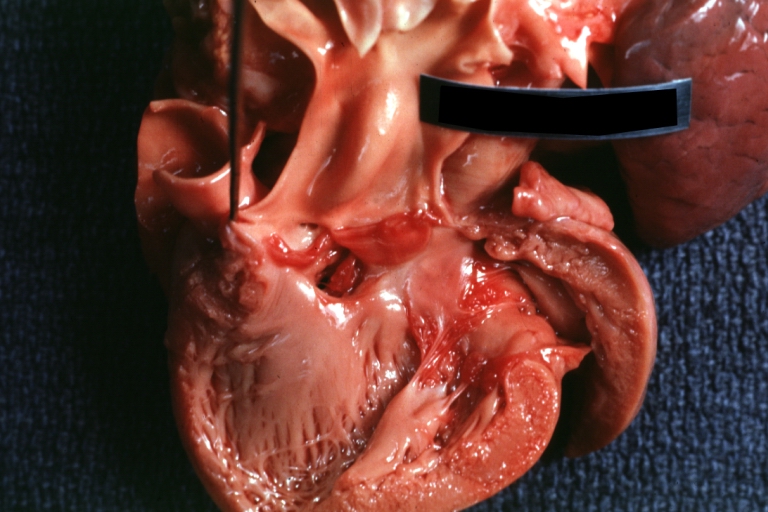
 Ventricular septal defect, view from left ventricle
Ventricular septal defect, view from left ventricle -
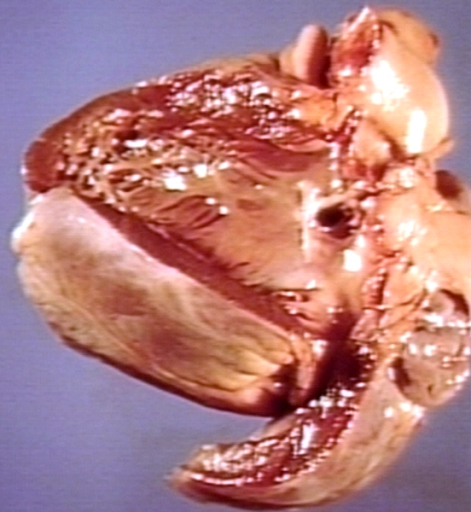
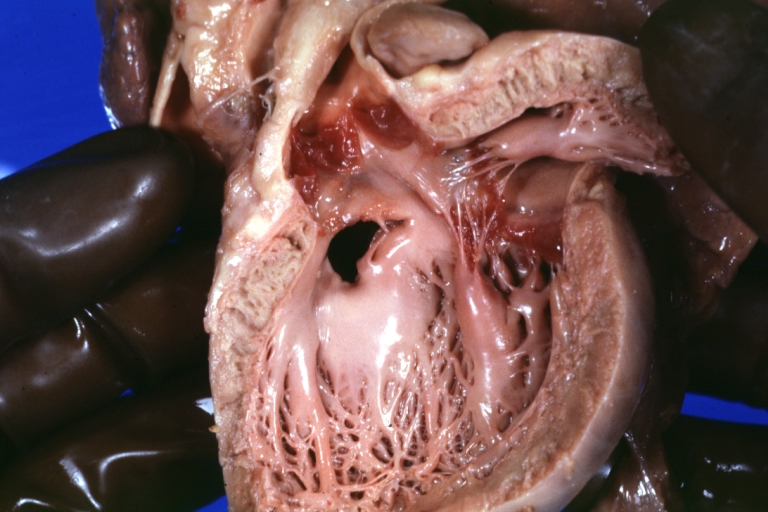
 Interventricular Septal Defect (Muscular Septum): Gross, natural color, muscular septal defect in newborn
Interventricular Septal Defect (Muscular Septum): Gross, natural color, muscular septal defect in newborn -
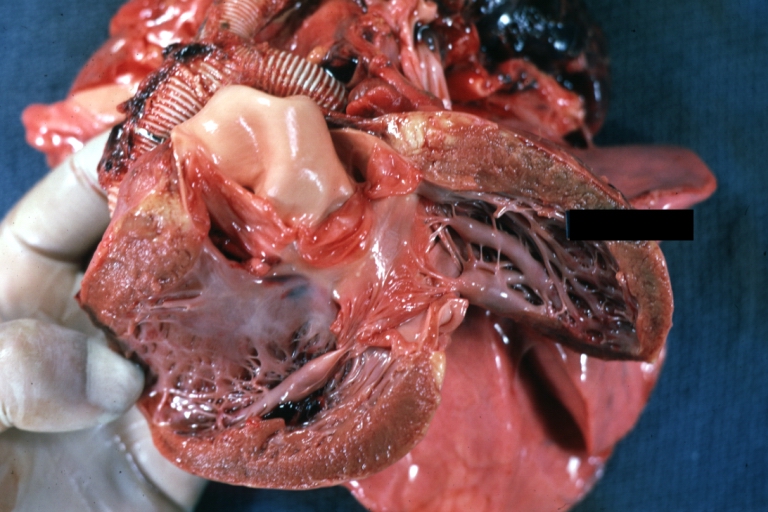
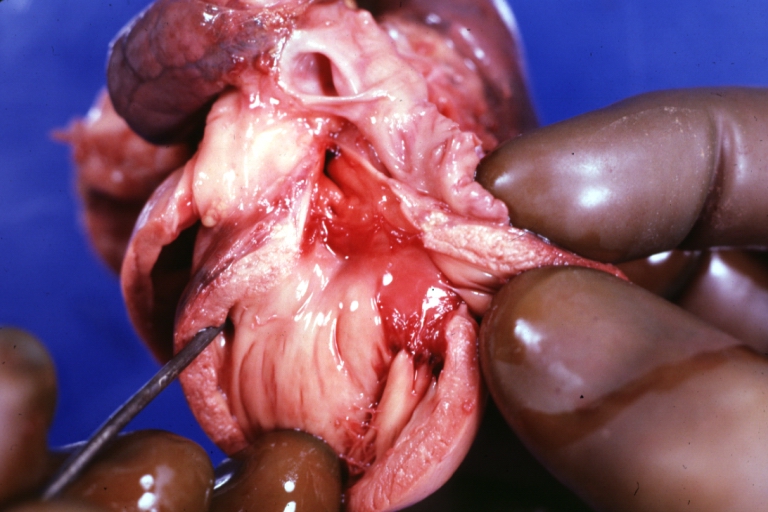
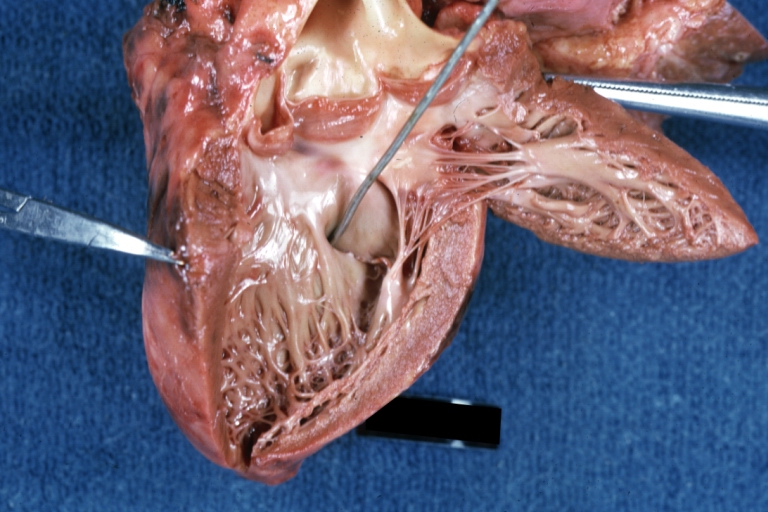
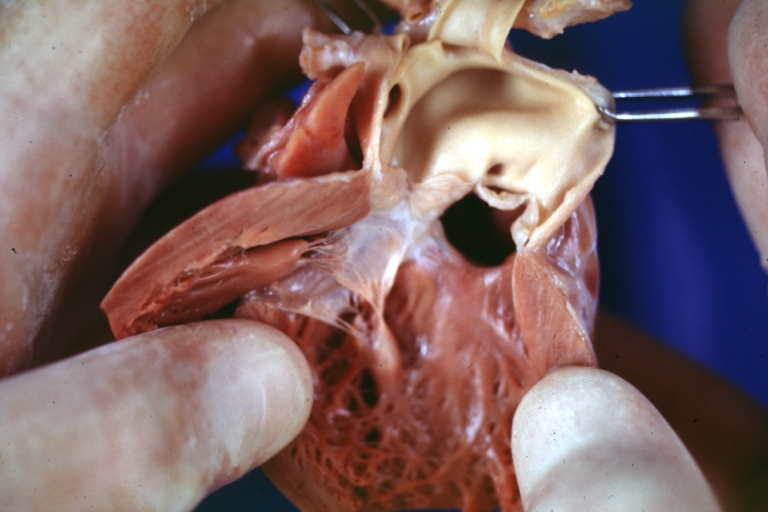
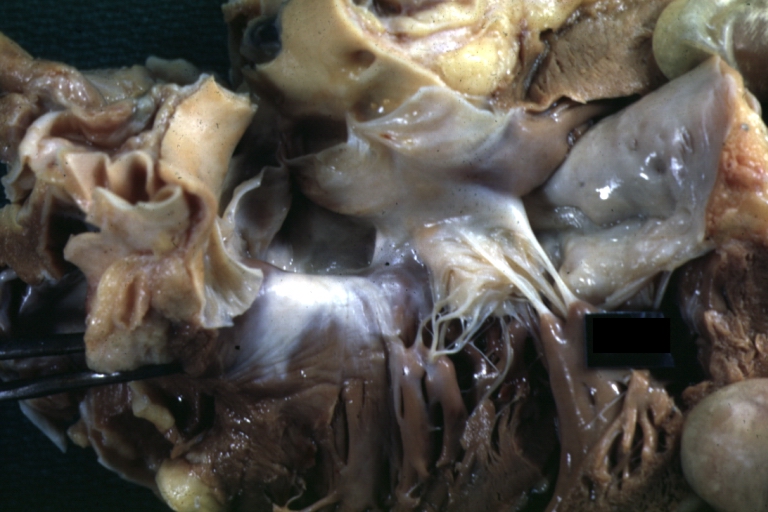
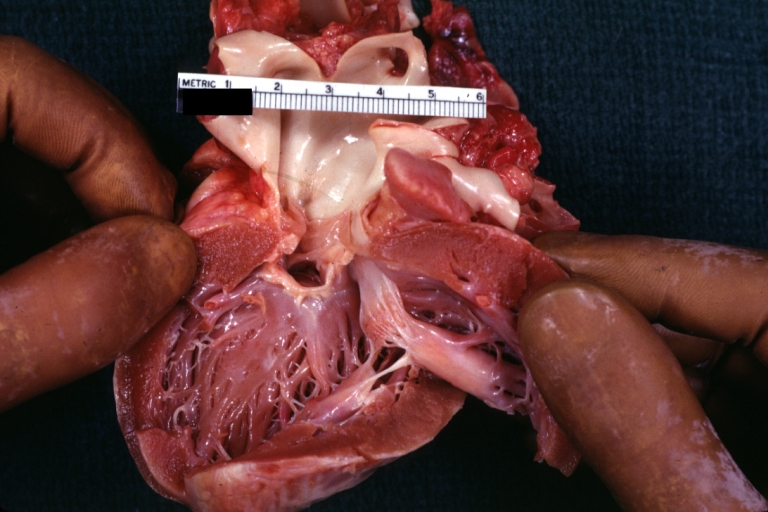 Subvalvular Ventricular Septal Defect: Gross, good view of defect with overriding aorta
Subvalvular Ventricular Septal Defect: Gross, good view of defect with overriding aorta



-
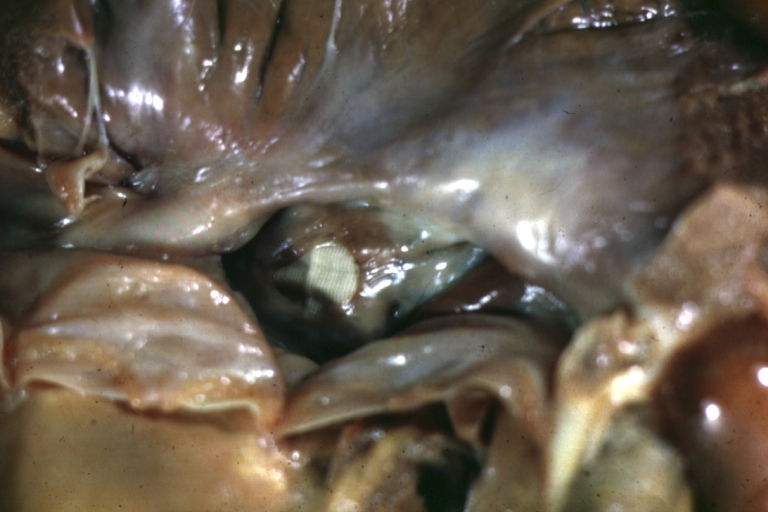
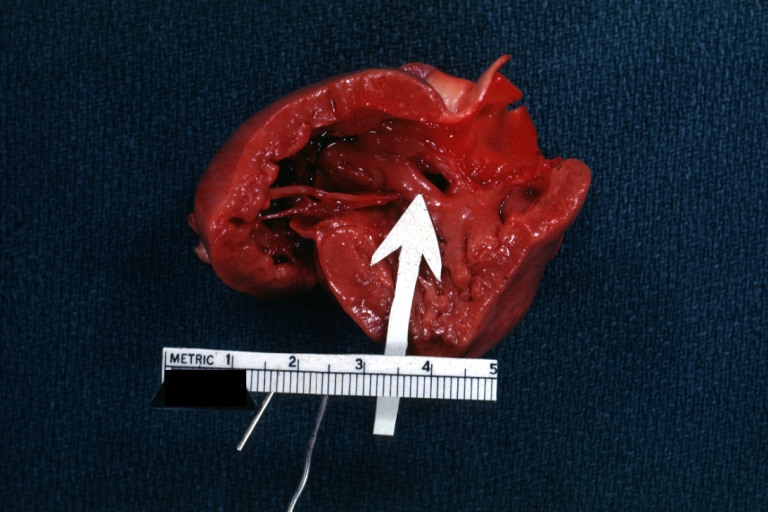 Ventricular Septal Defect: Gross, infant heart, pulmonary outlet, muscular septal defect
Ventricular Septal Defect: Gross, infant heart, pulmonary outlet, muscular septal defect -
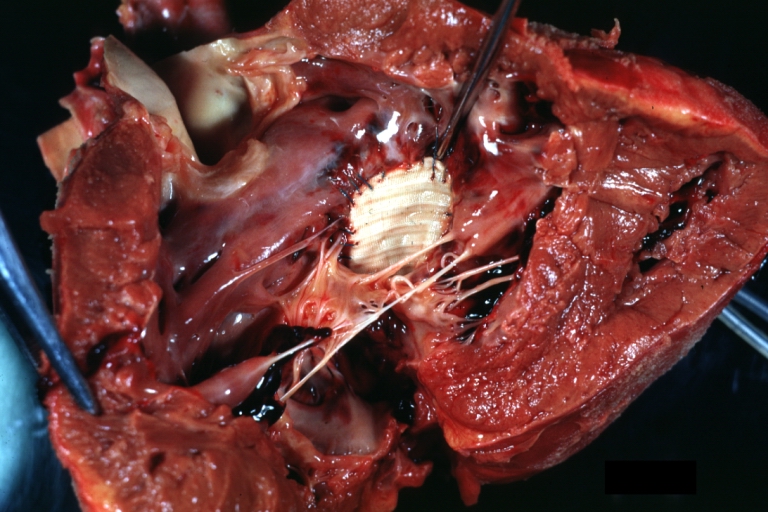
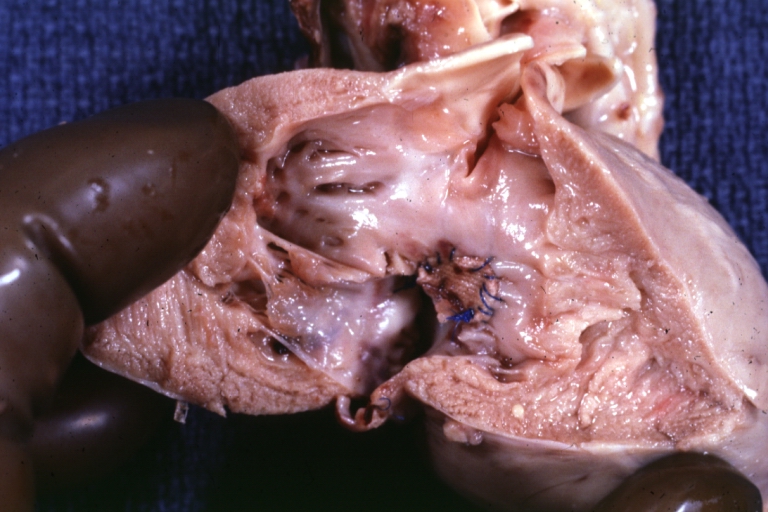 Perimembranous Ventricular Septal Defect: Gross, fixed tissue, lesion seen from right ventricle (with patch)
Perimembranous Ventricular Septal Defect: Gross, fixed tissue, lesion seen from right ventricle (with patch) -
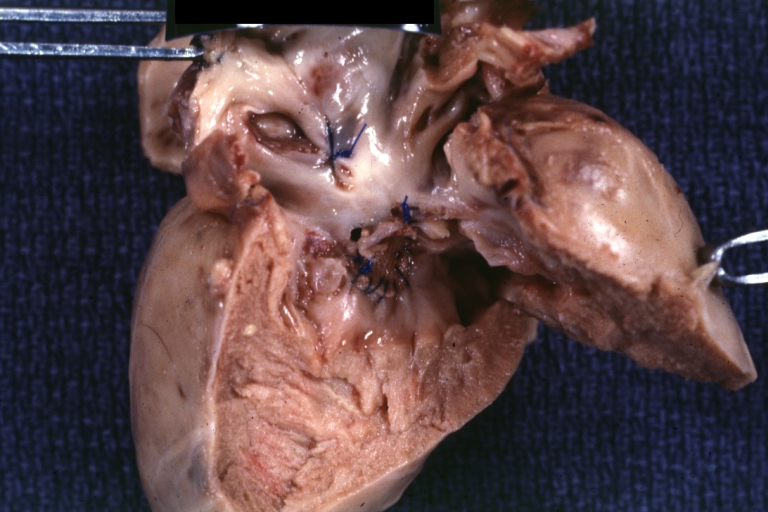 Perimembranous Interventricular Septal Defect: Gross, fixed tissue, view from right atrium and ventricle with patch placed three days prior to death.
Perimembranous Interventricular Septal Defect: Gross, fixed tissue, view from right atrium and ventricle with patch placed three days prior to death.



-
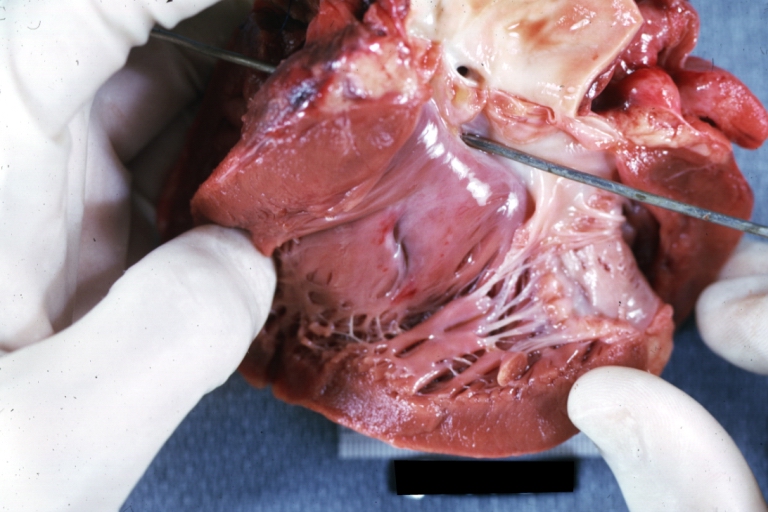
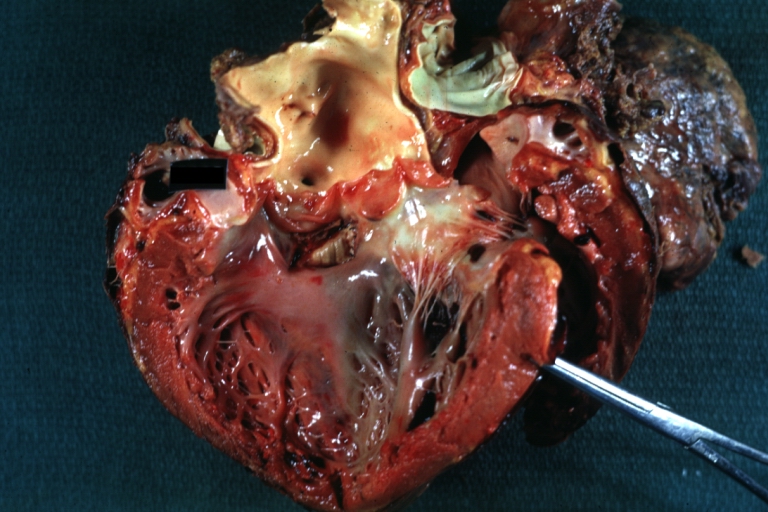
 Perimembranous Ventricular Septal Defect: Gross, an excellent example
Perimembranous Ventricular Septal Defect: Gross, an excellent example -
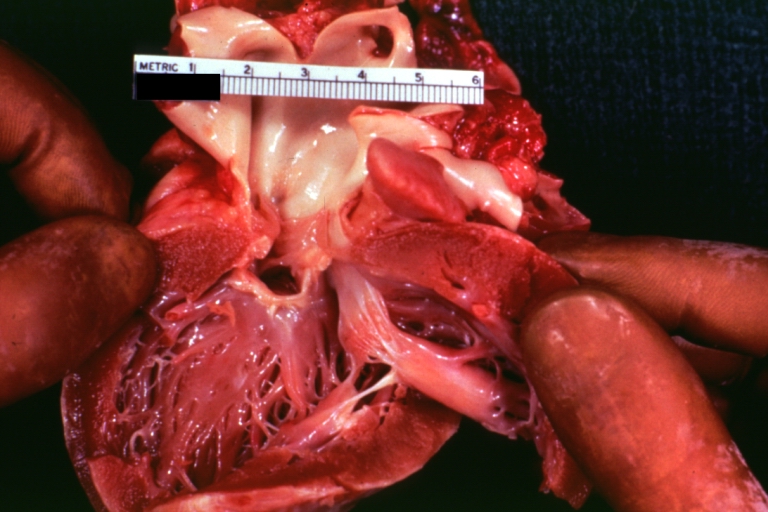
 Ventricular Septal Defect: Gross, subvalvular defect, left ventricle view of tetralogy of Fallot (very good example)
Ventricular Septal Defect: Gross, subvalvular defect, left ventricle view of tetralogy of Fallot (very good example) -
 Ventricular septal defect
Ventricular septal defect



-
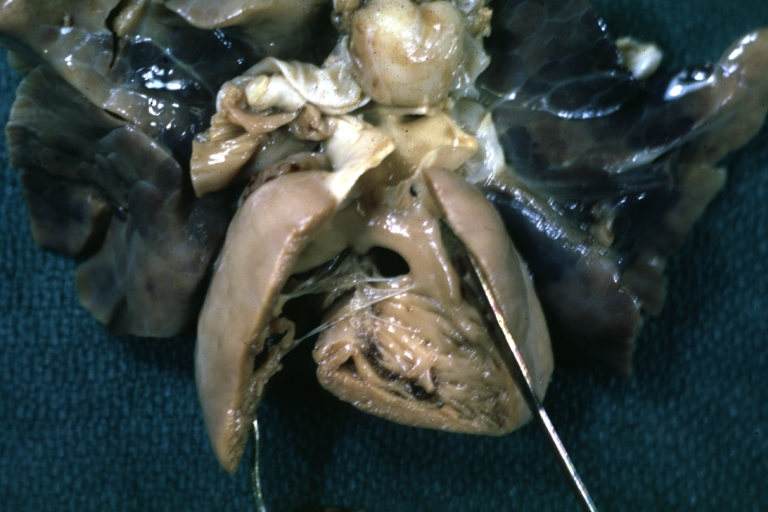
 Subpulmonic Ventricular Septal Defect: Gross, a well shown lesion.
Subpulmonic Ventricular Septal Defect: Gross, a well shown lesion. -
 Subvalvular Ventricular Septal Defect
Subvalvular Ventricular Septal Defect -
 Subvalvular Ventricular Septal Defect
Subvalvular Ventricular Septal Defect



-
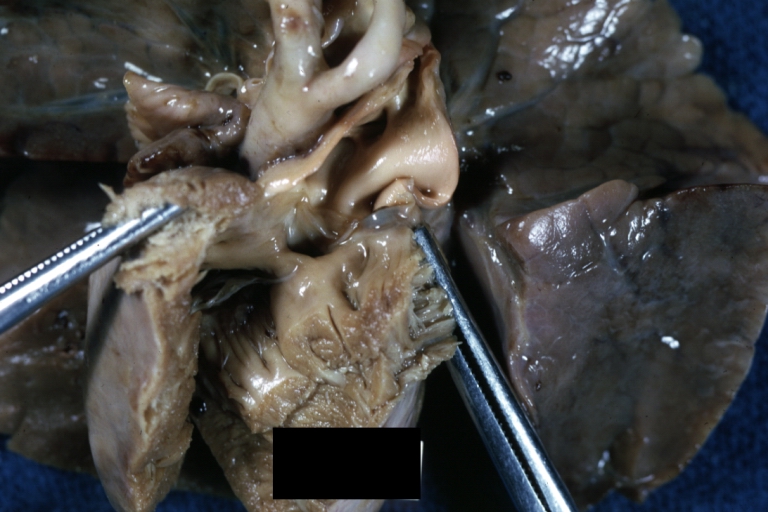
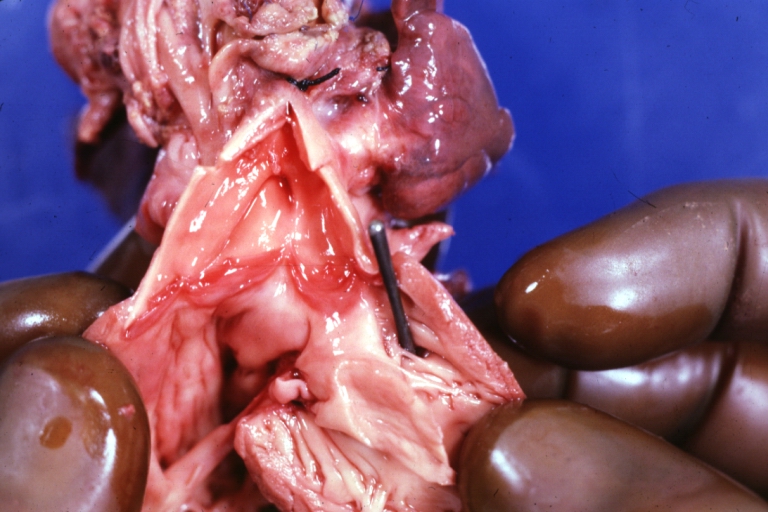
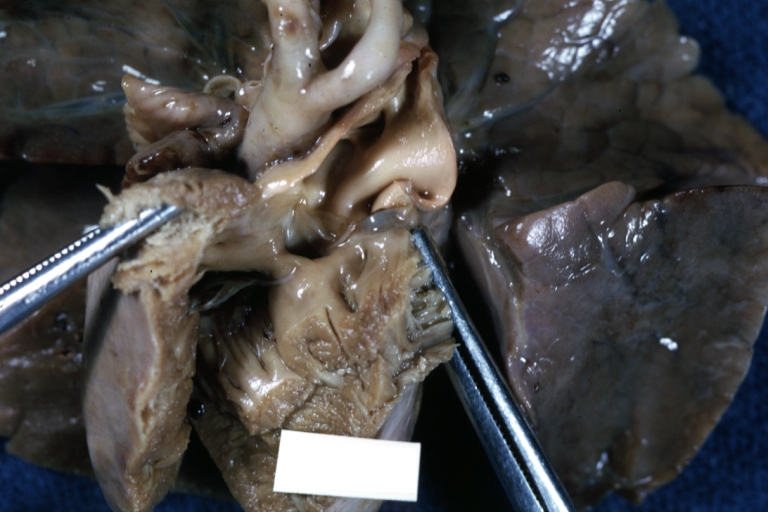
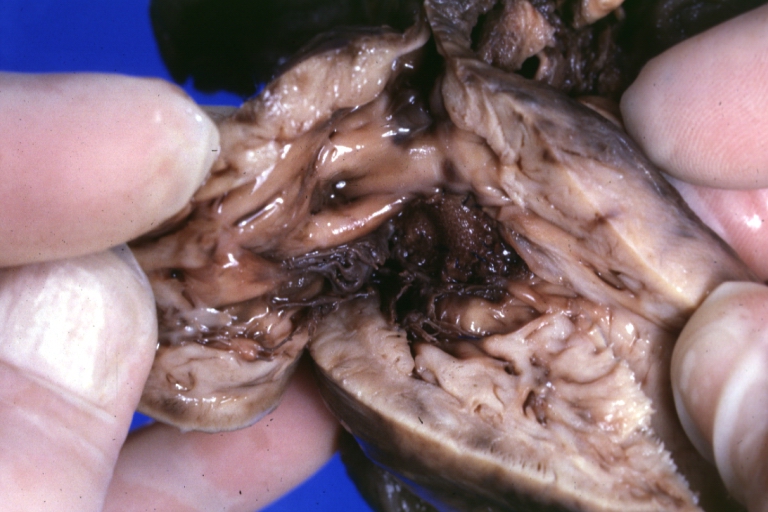
 Ventricular Septal Defect: Gross, natural color, view of opened heart with lungs attached shows rather well a subvalvular VSD
Ventricular Septal Defect: Gross, natural color, view of opened heart with lungs attached shows rather well a subvalvular VSD -
 Double Outlet Right Ventricle: Gross, fixed tissue, close-up view of left ventricular outflow tract and patched ventricular septal defect. The override is obvious in this (very good) close-up view
Double Outlet Right Ventricle: Gross, fixed tissue, close-up view of left ventricular outflow tract and patched ventricular septal defect. The override is obvious in this (very good) close-up view -
 Perimembranous Ventricular Septal Defect: Gross, fixed tissue, opened left ventricular outflow tract into aorta. Defect was patched 3 days prior to death
Perimembranous Ventricular Septal Defect: Gross, fixed tissue, opened left ventricular outflow tract into aorta. Defect was patched 3 days prior to death



-
 Atrial Septal Defect: Gross, (an excellent example) foramen ovale defect with right ventricular hypertrophy and fatty infiltration of the right ventricular wall, enlarged right atrium
Atrial Septal Defect: Gross, (an excellent example) foramen ovale defect with right ventricular hypertrophy and fatty infiltration of the right ventricular wall, enlarged right atrium -
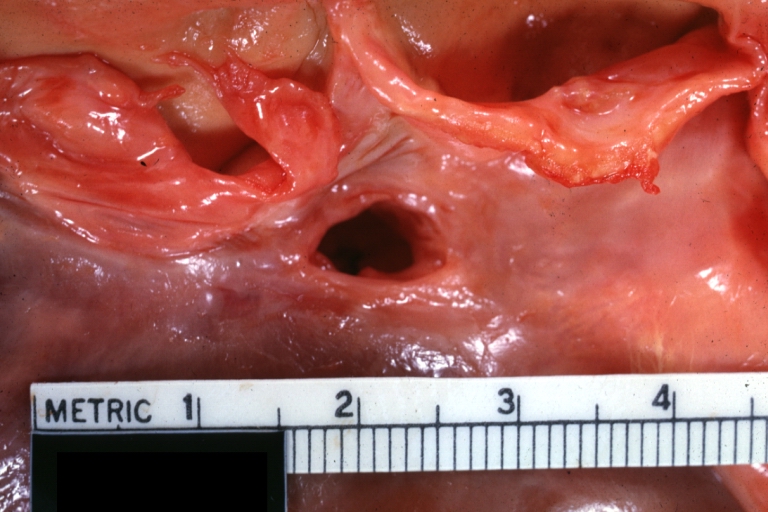
 Ventricular Septal Defect: Gross close-up adult heart, small perimembranous septal defect (very good example)
Ventricular Septal Defect: Gross close-up adult heart, small perimembranous septal defect (very good example) -
 Interventricular Septal Defect (Muscular Septum): Gross, natural color, low septal defect shown from aortic outlet. The same defect (with a probe in hole) shown from right ventricle.
Interventricular Septal Defect (Muscular Septum): Gross, natural color, low septal defect shown from aortic outlet. The same defect (with a probe in hole) shown from right ventricle.



-
 Interventricular Septal Defect (Muscular Septum): Gross natural color right ventricular outlet (probe in defect) view from left ventricular side
Interventricular Septal Defect (Muscular Septum): Gross natural color right ventricular outlet (probe in defect) view from left ventricular side -
 Atrial Septal Defect: Gross natural color infant heart foramen ovale defect, septum secundum
Atrial Septal Defect: Gross natural color infant heart foramen ovale defect, septum secundum -
 Aortic Subvalvular Ventricular Septal Defect: Gross, natural color, septal defect has patch repair. Aortic valve is myxomatous. A complex case of truncus with interrupted arch.
Aortic Subvalvular Ventricular Septal Defect: Gross, natural color, septal defect has patch repair. Aortic valve is myxomatous. A complex case of truncus with interrupted arch.



-
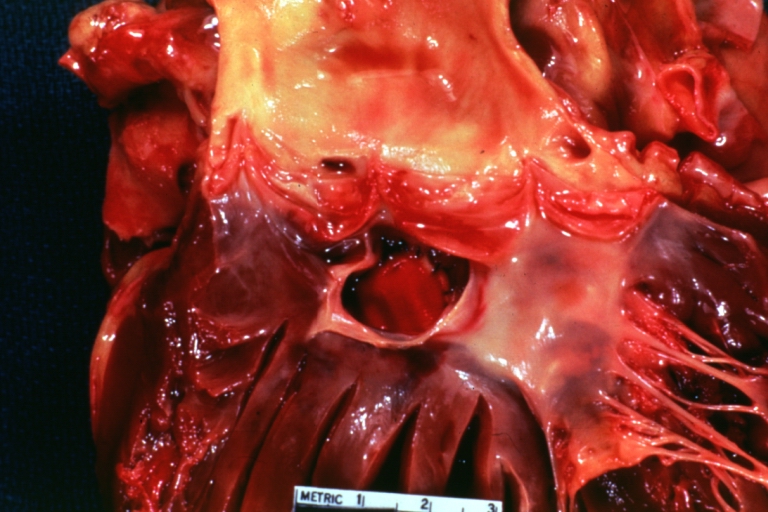
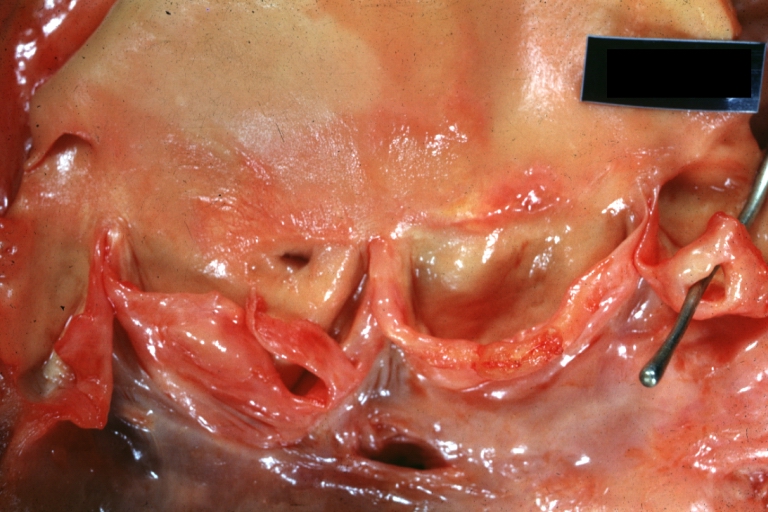
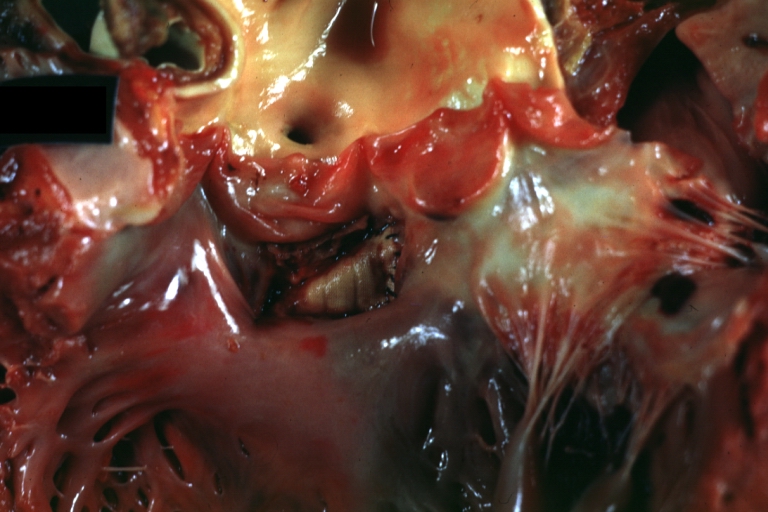
 Interventricular Septal Defect Membranous Septum: Gross natural color close-up (an excellent demonstration)
Interventricular Septal Defect Membranous Septum: Gross natural color close-up (an excellent demonstration) -
 Interventricular Septal Defect Membranous Septum: Gross natural color small defect well shown. Aortic cusps are scarred and one is perforated
Interventricular Septal Defect Membranous Septum: Gross natural color small defect well shown. Aortic cusps are scarred and one is perforated -
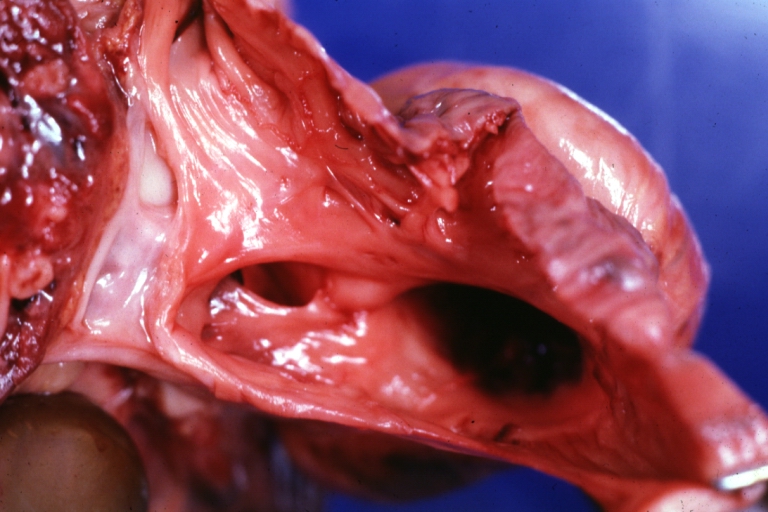
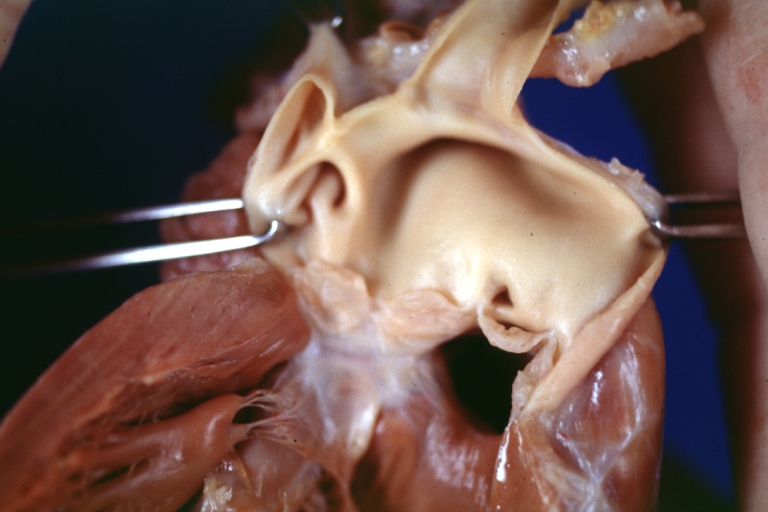
 Subvalvular Ventricular Septal Defect: Gross, natural color, close-up view of aortic outflow tract with a large subvalvular defect
Subvalvular Ventricular Septal Defect: Gross, natural color, close-up view of aortic outflow tract with a large subvalvular defect



-
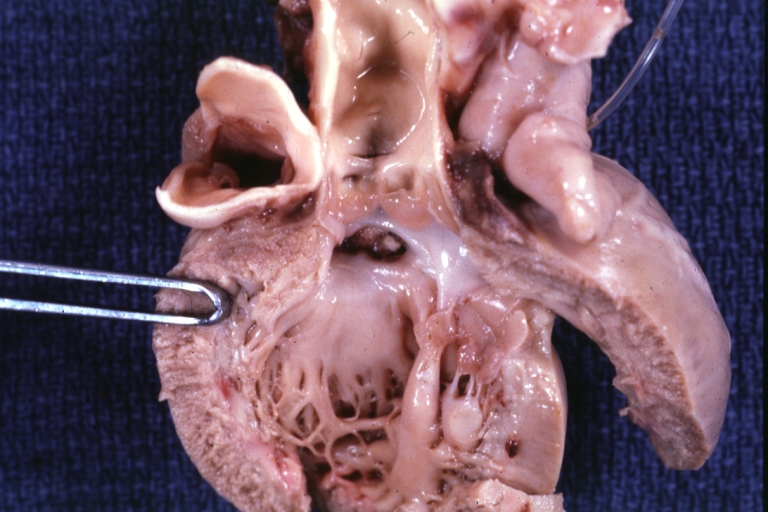
 Membranous Interventricular Septal Defect: Gross natural color subvalvular defect with probe immediately inferior to membranous septum
Membranous Interventricular Septal Defect: Gross natural color subvalvular defect with probe immediately inferior to membranous septum -
 Subvalvular Ventricular Septal Defect: Gross, fixed tissue, large subpulmonic defect apparently represent left displacement of the pulmonary artery
Subvalvular Ventricular Septal Defect: Gross, fixed tissue, large subpulmonic defect apparently represent left displacement of the pulmonary artery -
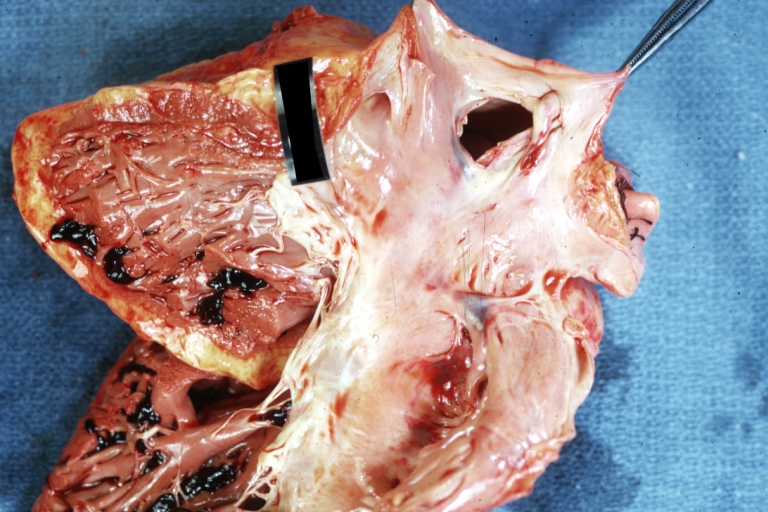
 Interventricular Septal Defect: Gross, fixed tissue, opened right ventricular outflow tract positioned to show perimembranous septal defect (as surgeon would see it during repair)
Interventricular Septal Defect: Gross, fixed tissue, opened right ventricular outflow tract positioned to show perimembranous septal defect (as surgeon would see it during repair)



-
 Ventricular Septal Defect Muscular: Gross, natural color, view from right ventricle with probe in defect right ventricular hypertrophy is evident
Ventricular Septal Defect Muscular: Gross, natural color, view from right ventricle with probe in defect right ventricular hypertrophy is evident -
 Ventricular Septal Defect Muscular: Gross, natural color, view from left ventricle with probe in defect
Ventricular Septal Defect Muscular: Gross, natural color, view from left ventricle with probe in defect -
 Interventricular Septal Defect Subvalvular with Patch Repair: Gross natural color 19yo with Tetralogy of Fallot also shows overriding aorta
Interventricular Septal Defect Subvalvular with Patch Repair: Gross natural color 19yo with Tetralogy of Fallot also shows overriding aorta



-
 Interventricular Septal Defect Subvalvular with Patch Repair: Gross, natural color, close-up
Interventricular Septal Defect Subvalvular with Patch Repair: Gross, natural color, close-up -
 Interventricular Septal Defect (Perimembranous) with Patch Repair: Gross, natural color, view from right ventricle. A case of inverted ventricles
Interventricular Septal Defect (Perimembranous) with Patch Repair: Gross, natural color, view from right ventricle. A case of inverted ventricles -
 Interventricular Septal Defect (Perimembranous) with Patch Repair: Gross, natural color, view from left ventricular outflow tract
Interventricular Septal Defect (Perimembranous) with Patch Repair: Gross, natural color, view from left ventricular outflow tract



-
 Ventricular Septal Defect (Subvalvular): Gross, fixed tissue, small heart with opened aorta and subvalvular defect shown. A case of pulmonary artery atresia
Ventricular Septal Defect (Subvalvular): Gross, fixed tissue, small heart with opened aorta and subvalvular defect shown. A case of pulmonary artery atresia -
 Truncus Arteriosus with Subvalvular Ventricular Septal Defect: Gross, natural color, an excellent view of subvalvular defect. Quadricuspid truncus valve and type I origin of pulmonary arteries
Truncus Arteriosus with Subvalvular Ventricular Septal Defect: Gross, natural color, an excellent view of subvalvular defect. Quadricuspid truncus valve and type I origin of pulmonary arteries -
 Truncus Arteriosus with Subvalvular Interventricular Septal Defect: Gross, natural color, defect is shown from the right side (view toward right ventricular outlet)
Truncus Arteriosus with Subvalvular Interventricular Septal Defect: Gross, natural color, defect is shown from the right side (view toward right ventricular outlet)



-
 Truncus Arteriosus with Subvalvular Interventricular Septal Defect: Gross natural color excellent view of lesion looking at opened aortic ring with quadricuspid aortic valve. A large subvalvular defect (origin of pulmonary arteries is at forceps)
Truncus Arteriosus with Subvalvular Interventricular Septal Defect: Gross natural color excellent view of lesion looking at opened aortic ring with quadricuspid aortic valve. A large subvalvular defect (origin of pulmonary arteries is at forceps) -
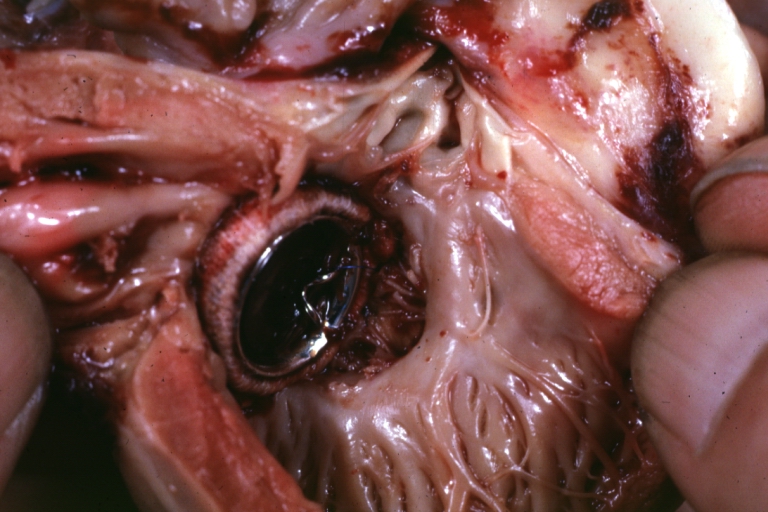 Av Canal with Left Side Bjork Shiley Prosthetic Valve: Gross, natural color, a close-up view of valve and the bridging defect
Av Canal with Left Side Bjork Shiley Prosthetic Valve: Gross, natural color, a close-up view of valve and the bridging defect -
 Interventricular Septal Defect (Perimembranous) with Patch Repair: Gross, fixed tissue, a close-up view of patch repair from right ventricle
Interventricular Septal Defect (Perimembranous) with Patch Repair: Gross, fixed tissue, a close-up view of patch repair from right ventricle



-
 Conduit Right Ventricle to Pulmonary Artery: Gross, fixed tissue, opened conduit showing sutures into ventricle and patch closed perimembranous interventricular septal defect
Conduit Right Ventricle to Pulmonary Artery: Gross, fixed tissue, opened conduit showing sutures into ventricle and patch closed perimembranous interventricular septal defect -
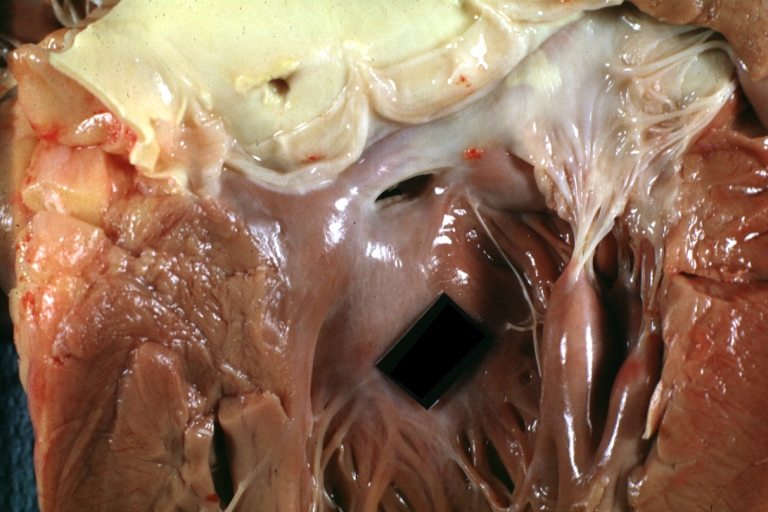
 Ventricular Septal Defect (Perimembranous): Gross, natural color, (quite good photo – lesion before the operation)
Ventricular Septal Defect (Perimembranous): Gross, natural color, (quite good photo – lesion before the operation) -
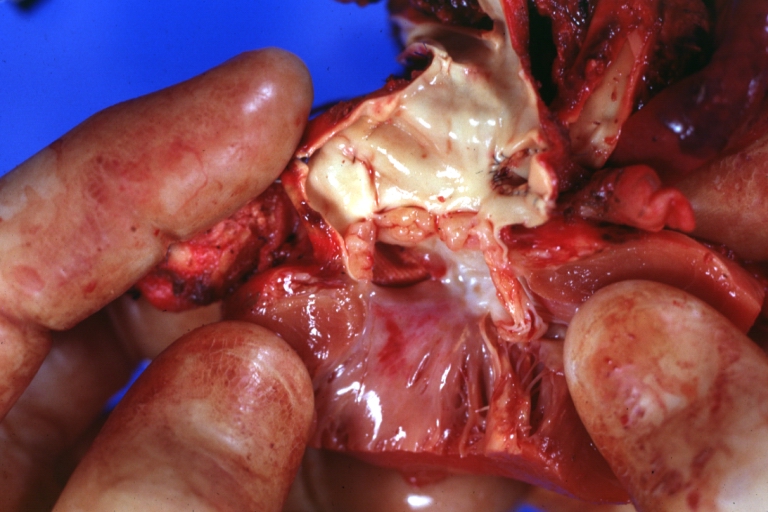
 Ventricular Septal Defect (Subvalvular) Repaired: Tetralogy of Fallot; Gross, fixed tissue, close-up view of a large subvalvular defect repaired with a Dacron patch (overgrown with fibrous tissue prominent subaortic shelf with endocardial thickening).
Ventricular Septal Defect (Subvalvular) Repaired: Tetralogy of Fallot; Gross, fixed tissue, close-up view of a large subvalvular defect repaired with a Dacron patch (overgrown with fibrous tissue prominent subaortic shelf with endocardial thickening).



-
 Ventricular Septal Defect (Subvalvular) Repaired: Tetralogy of Fallot; Gross, fixed tissue, close-up view of a large subvalvular defect repaired with a Dacron patch
Ventricular Septal Defect (Subvalvular) Repaired: Tetralogy of Fallot; Gross, fixed tissue, close-up view of a large subvalvular defect repaired with a Dacron patch -
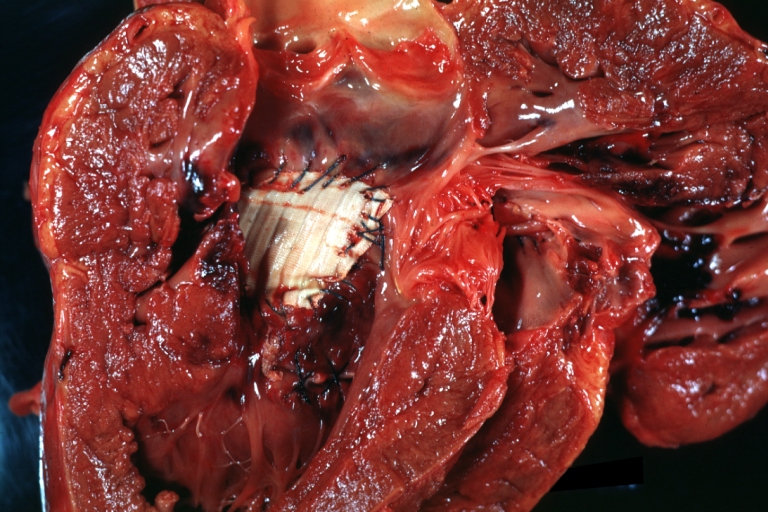
 Ventricular Septal Defect (Subvalvular) Repaired: Gross, fixed tissue, close-up view of Dacron patch. Nearly completely covered with fibrous tissue
Ventricular Septal Defect (Subvalvular) Repaired: Gross, fixed tissue, close-up view of Dacron patch. Nearly completely covered with fibrous tissue -
 Transposition Great Vessels with Interventricular Septal Defect: Gross, fixed tissue, opened left ventricular outflow tract into a pulmonary artery (perimembranous defect)
Transposition Great Vessels with Interventricular Septal Defect: Gross, fixed tissue, opened left ventricular outflow tract into a pulmonary artery (perimembranous defect)



-
 Transposition Great Vessels with Interventricular Septal Defect: Gross, fixed tissue, close-up of interventricular septal defect and pulmonary valve
Transposition Great Vessels with Interventricular Septal Defect: Gross, fixed tissue, close-up of interventricular septal defect and pulmonary valve

References
- ↑ Anderson RH, Sarwark AE, Spicer DE, Backer CL (2014). “Exercises in anatomy: holes between the ventricles”. Multimed Man Cardiothorac Surg. 2014. doi:10.1093/mmcts/mmu026. PMID 25547619.
- ↑ Anderson RH, Webb S, Brown NA, Lamers W, Moorman A (2003). “Development of the heart: (2) Septation of the atriums and ventricles”. Heart. 89 (8): 949–58. PMC 1767797. PMID 12860885.
- ↑ Schleich JM, Abdulla T, Summers R, Houyel L (2013). “An overview of cardiac morphogenesis”. Arch Cardiovasc Dis. 106 (11): 612–23. doi:10.1016/j.acvd.2013.07.001. PMID 24138816.
- ↑ 4.0 4.1 4.2 Anderson RH, Spicer DE, Brown NA, Mohun TJ (2014). “The development of septation in the four-chambered heart”. Anat Rec (Hoboken). 297 (8): 1414–29. doi:10.1002/ar.22949. PMID 24863187.
- ↑ 5.0 5.1 Gittenberger-de Groot AC, Calkoen EE, Poelmann RE, Bartelings MM, Jongbloed MR (2014). “Morphogenesis and molecular considerations on congenital cardiac septal defects”. Ann Med. 46 (8): 640–52. doi:10.3109/07853890.2014.959557. PMID 25307363.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1], Leida Perez, M.D. Associate Editor(s)-In-Chief: Keri Shafer, M.D. [2], Atif Mohammad, M.D., Priyamvada Singh, MBBS
Overview
The causes of VSD are not fully known. The septal defect between the right and left ventricle can be congenital that occurs alone or with other congenital abnormalities. Genetic association suggests the involvement of chromosome band 22q11 microdeletion in the mechanism of VSD development. In adults, Heart attacks can be complicated by the development of VSD.
Causes
- The causes of VSD are not yet known. This defect often occurs along with other congenital heart defects[1]
- In adults, ventricular septal defects are a rare but serious complication of heart attacks. These holes are related to heart attacks and do not result from a birth defect.
- Genetics – The frequent association between arch abnormalities and significant conal VSDs suggests a common mechanism involving a chromosome band 22q11 microdeletion. Deletions in this area have not been linked with isolated supracristal VSDs.
- Maternal Drug use – Clomifene
References
- ↑ Spicer DE, Hsu HH, Co-Vu J, Anderson RH, Fricker FJ (2014). “Ventricular septal defect”. Orphanet J Rare Dis. 9: 144. doi:10.1186/s13023-014-0144-2. PMC 4316658. PMID 25523232.
Differentiating Ventricular Septal Defect from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1], Leida Perez, M.D. Associate Editor(s)-In-Chief: Keri Shafer, M.D. [2], Priyamvada Singh, MBBS
Overview
Differentiating Ventricular Septal Defect from other Disorders
- Alcohol use of the mother
- Chemotherapeutics
- Down’s Syndrome
- Ellis-van Creveld Syndrome
- Genetic disorders
- Hypoxia (Lack of oxygen)
- Immunosuppressives
- Marfan’s Syndrome
- Noonan Syndrome
- Radiation
- Retinoic acid
- Rubella
- Thalidomide
- Trisomy 13
- Turner’s Syndrome
- Differential diagnosis of Ventricular septal defect[1]
| Disease | Signs and Symptoms | Association | Diagnostic modality | Management | Prognosis |
|---|---|---|---|---|---|
| VSD[2] |
|
|
|
|
|
| Atrioventricular septal defect[3] |
|
|
|
Medical treatment
CHF:
feeding difficulties and failure to thrive
|
Without surgery the natural history of complete AVSD, only 4% survival beyond 5 years old
|
| Atrial septal defect[4][5][6][7] |
|
|
|
|
|
| Patent Ductus Arteriosus (PDA)[8] | In adults is usually a coincidental finding during physical examination or echocardiography screening.
|
|
|
|
|
| Infundibular Pulmonary Stenosis[9][10][11][12] |
|
|
|
|
|
References
- ↑ LAMBERT EC, KELSCH JV, VLAD P (1963). “Differential diagnosis of ventricular septal defect in infancy: a common problem”. Am J Cardiol. 11: 447–51. doi:10.1016/0002-9149(63)90003-1. PMID 13928242.
- ↑ Cleves MA, Hobbs CA, Cleves PA, Tilford JM, Bird TM, Robbins JM (2007) Congenital defects among liveborn infants with Down syndrome. Birth Defects Res A Clin Mol Teratol 79 (9):657-63. DOI:10.1002/bdra.20393 PMID: 17696161
- ↑ Craig B (2006). “Atrioventricular septal defect: from fetus to adult”. Heart. 92 (12): 1879–85. doi:10.1136/hrt.2006.093344. PMC 1861295. PMID 17105897.
- ↑ El-Segaier M, Pesonen E, Lukkarinen S, Peters K, Ingemansson J, Sörnmo L; et al. (2006). “Atrial septal defect: a diagnostic approach”. Med Biol Eng Comput. 44 (9): 739–45. doi:10.1007/s11517-006-0094-5. PMID 16941100.
- ↑ Yoshihara K, Ozawa T, Sakuragawa H, Fujii T, Kawasaki M, Shiono N; et al. (1999). “[Noonan syndrome associated with atrial septal defect, pulmonary stenosis, and completely unroofed coronary sinus without LSVC: a case report]”. Kyobu Geka. 52 (2): 134–7. PMID 10036874.
- ↑ Geva T, Martins JD, Wald RM (2014). “Atrial septal defects”. Lancet. 383 (9932): 1921–32. doi:10.1016/S0140-6736(13)62145-5. PMID 24725467.
- ↑ Goldberg JF (2015). “Long-term Follow-up of “Simple” Lesions–Atrial Septal Defect, Ventricular Septal Defect, and Coarctation of the Aorta”. Congenit Heart Dis. 10 (5): 466–74. doi:10.1111/chd.12298. PMID 26365715.
- ↑ Schneider DJ, Moore JW (2006). “Patent ductus arteriosus”. Circulation. 114 (17): 1873–82. doi:10.1161/CIRCULATIONAHA.105.592063. PMID 17060397.
- ↑ Shyu KG, Tseng CD, Chiu IS, Hung CR, Chu SH, Lue HC; et al. (1993). “Infundibular pulmonic stenosis with intact ventricular septum: a report of 15 surgically corrected patients”. Int J Cardiol. 41 (2): 115–21. doi:10.1016/0167-5273(93)90150-f. PMID 8282434.
- ↑ Zaret BL, Conti CR (1973). “Infundibular pulmonic stenosis with intact ventricular septum in the adult”. Johns Hopkins Med J. 132 (1): 50–60. PMID 4682663.
- ↑ Mullins CE, Ludomirsky A, O’Laughlin MP, Vick GW, Murphy DJ, Huhta JC; et al. (1988). “Balloon valvuloplasty for pulmonic valve stenosis–two-year follow-up: hemodynamic and Doppler evaluation”. Cathet Cardiovasc Diagn. 14 (2): 76–81. doi:10.1002/ccd.1810140203. PMID 3365764.
- ↑ Park SJ, Lee CW, Hong MK, Song JK, Park SW, Kim JJ (1997). “Transcoronary alcohol ablation of infundibular hypertrophy in patients with idiopathic infundibular pulmonic stenosis”. Am J Cardiol. 80 (11): 1514–6. doi:10.1016/s0002-9149(97)00724-8. PMID 9399740.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-In-Chief: Priyamvada Singh, MBBS [2]; Cafer Zorkun, M.D., Ph.D. [3]; Assistant Editor-In-Chief: Kristin Feeney, B.S. [4]
Overview
The ventricular septal defect is the most common congenital cardiac malformation with an incidence of 300 to 350 per 100,000 live births,[1] corresponding to 30% of all newborns with a congenital heart defect. There is no predilection based on sex. Incidence rates are similar in different races and seasons and are unrelated to maternal age, birth order, sex, and socioeconomic status. Congential VSDs are frequently associated with other congenital conditions, such as Down syndrome. [2]
Epidemiology and Demographics
Incidence in United States of America
Only in the United States, there are approximately 1 million adults with congenital heart disease, with 20,000 new patients reaching adolescence each year.
Age
Pediatrics
- The incidence has been found to be approximately 300 to 350 infants per 100,000 live births. [1]
Adults
- The prevalence of ventricular septal defects is less in adults compared to the infants. This might be due to the fact that many small ventricular septal defects have spontaneous closure in childhood. [3][4] Due to the improvement in early diagnosis in childhood and improved medical, surgical and ICU care, the number of adults will continue to rise. However, despite improved survival to adulthood, many patients will continue to have problems with residual shunts, valvular heart disease, ventricular dysfunction, heart failure and arrhythmias. The risk of sudden death in adults with congenital heart disease is nearly 25-50 times greater than would be expected for their age.
- In adults (without congenital heart defects), a VSD can form a few days after a myocardial infarction (heart attack). It might be due to mechanical tearing of the septal wall, before scar tissue forms and macrophages start remodeling the dead (heart) tissue.
Gender
There is no predilection based on gender.
Race
There is no significant difference in incidences of ventricular septal defects based on race.
References
- ↑ 1.0 1.1 Hoffman JI, Kaplan S (2002). “The incidence of congenital heart disease”. J Am Coll Cardiol. 39 (12): 1890–900. PMID 12084585.
- ↑ Giuliani et al, Cardiology: Fundamentals and Practice, Second Edition, Mosby Year Book, Boston, 1991.
- ↑ Du ZD, Roguin N, Wu XJ (1998). “Spontaneous closure of muscular ventricular septal defect identified by echocardiography in neonates”. Cardiol Young. 8 (4): 500–5. PMID 9855105.
- ↑ Kidd L, Driscoll DJ, Gersony WM, Hayes CJ, Keane JF, O’Fallon WM; et al. (1993). “Second natural history study of congenital heart defects. Results of treatment of patients with ventricular septal defects”. Circulation. 87 (2 Suppl): I38–51. PMID 8425321.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-In-Chief: Priyamvada Singh, M.B.B.S. [2]; Assistant Editor-In-Chief: Kristin Feeney, B.S. [3]
Risk Factors
It is unclear exactly why certain babies are born with septal defects. There is evidence to suggest that families with a history of genetic problems and other congenital heart disease may be at an increased risk for carrying and expressing the trait. Genetic testing may be performed to assist you in estimating the likelihood that any future children may be born with defect.[1]
During pregnancy, drug and alcohol exposure can also harm the fetus during development and result in potential birth defects.
Refernces
- ↑ “Ventricular septal defect: MedlinePlus Medical Encyclopedia”. Retrieved 2013-01-08.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-In-Chief: Keri Shafer, M.D. [2]; Atif Mohammad, M.D., Priyamvada Singh, MBBS
Natural History
Natural history of unoperated ventricular septal defect. Muscular and membranous defects usually close spontaneously
Restrictive ventricular septal defect
- Small shunt (Qρ/Qѕ < 1.5/1.0 Qρ/Qs is pressure gradient between pulmonary and systemic circulation)
- No significant hemodynamic compromise
Moderately restrictive ventricular septal defect
- Moderate shunt (Qρ/Qѕ=1.5-2.5/1.0)
- Hemodynamic burden on left atrium and ventricle.
- Increase in pulmonary vascular resistance
- Atrial and ventricular arrhythmia can occur
Large or Non restrictive venticular defect
- High left and right ventricular volume overload
- High pulmonary vascular resistance
- Eisenmenger syndrome
Complications
- Endocarditis
- Aortic regurgitation
- Subaortic or subpulmonary stenosis
- Eisenmenger syndrome
- Atrial and ventricular arrhythmia can occur
Prognosis
Many small defects will close on their own. For those defects that do not spontaneously close, the outcome is good with surgical repair. Complications may result if a large defect is not treated.
References
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Electrocardiogram | Chest X Ray | CT | MRI | Echocardiography | Cardiac Catheterization
Treatment
Treatment
Medical Therapy | Surgery | Ventricular Septal Defect Post-Surgical Prognosis | ACC/AHA Guidelines for Surgical and Catheter Intervention Follow-Up | Prevention | ACC/AHA Guidelines for Reproduction | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Acknowledgements and Initial Contributors to Page
Acknowledgements and Initial Contributors to Page
Leida Perez, M.D. Redmond Burke M.D.
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH