
Patent ductus arteriosus
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Priyamvada Singh, M.B.B.S. [2], Cafer Zorkun, M.D., Ph.D. [3] Ramyar Ghandriz MD[4]; Assistant Editor-In-Chief: Kristin Feeney, B.S. [5]
Diagram
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Priyamvada Singh, M.B.B.S. [2], Cafer Zorkun, M.D., Ph.D. [3], Assistant Editor-In-Chief: Kristin Feeney, B.S. [4]
Overview
References
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Priyamvada Singh, M.B.B.S. [2], Cafer Zorkun, M.D., Ph.D. [3], Assistant Editor-In-Chief: Kristin Feeney, B.S. [4]
Overview
Patent Ductus Arteriosus (PDA) is a remnant of the distal sixth aortic arch and connects the pulmonary artery at the junction of the main pulmonary artery and the origin of the left pulmonary artery to the proximal descending aorta just after the origin of the left subclavian artery. Normally, the ductus closes within a few hours or days of birth; when it does not, the result is patent ductus arteriosus. This defect is common in premature infants but rare in full-term infants. Symptoms include shortness of breath and cardiac arrhythmia, and may progress to congestive heart failure if left uncorrected.
{{#ev:youtube|5iWbYGkCtCg}}
Anatomy
Patent ductus arteriosus is a heart condition that is normal but reverses soon after birth. In a persistent PDA, there is an irregular transmission of blood between two of the most important arteries (aorta and pulmonary artery) in close proximity to the heart. Although the ductus arteriosus normally seals off within a few days, in PDA, the newborn’s ductus arteriosus does not close but remains patent.
Historical Perspective
PDA is a congenital heart defect when a child’s ductus arteriosus fails to close after birth, producing a heart murmur described in 1898 by Gibson as the classic machinery murmur.
Pathophysiology
The pathophysiological consequences depend on the size of the defect and the pulmonary vascular resistance.
Causes
Causes of patent ductus arteriosus is not known. However, increased incidence have been associated with mother’s rubella and genetic causes
Epidemiology and Demographics
The PDA is commonly found in infants and constitutes only 2% of all congenital defects found in adults. The incidence is greater is in children who are born prematurely with history of perinatal asphyxia and infants with congenital rubella.
Risk Factors
Like many congenital heart disease, the cause of patent ductus arteriosus is not clear. Clinical studies suggest that the genetic and environmental factors both play an important role during the pregnancy.
Natural History, Complications and Prognosis
The natural history of unoperated patients of patent ductus arteriosus depends on the amount of left to right shunting. The left to right shunting, in turn, depends on the size of the ductus and the difference in resistance between the left and right side of heart. PDA can cause complications such as heart failure, infective endocarditis, rhythm disturbance, pulmonary hypertension and Eisenmenger syndrome.
Diagnosis
Laboratory Findings
Polycythemia may be present if the child has any other congenital heart disease. Hypoxemia or hypercarbia may be present.
Chest X Ray
The findings on chest x ray depends on the degree of shunting between left and right system.
MRI
Magnetic resonance imaging can be helpful as a diagnostic tool in conditions where the echocardiographic findings are inconclusive.
CT
Computed tomography can be helpful as a diagnostic tool in conditions where the echocardiographic findings are inconclusive.
Echocardiography
Echocardiogram is the non-invasive method and can diagnose patent ductus arteriosus. Echo along with doppler can be used to visualize the shunt from the aorta to the left pulmonary artery.
Other Imaging Findings
Cardiac Catheterization
Cardiac catheterization serves to establish the presence of a PDA by assessment of the increase of oxygen in the pulmonary artery. It also serves to identify the anatomy of the PDA, the severity of a left-to-right shunt, and the presence of pulmonary hypertension.
Treatment
Medical Therapy
Preterm Infants
Prostaglandin E2 plays a key role in maintaining the patency of ductus arteriosus before birth. Thus, prostaglandin E2 inhibitors are used as a therapeutic options to close the patent ductus arteriosus.
Term and Older Children
In term infants and older patients, the prostaglandin E2 inhibitors (indomethacin and ibuprofen) have not shown to be effective. This is so because the ductus in premature baby is different histological from in older patients. As a result, pharmacologic therapy is only used routinely in preterm infants.
Surgery
Infants without overt symptoms may simply be monitored as outpatients, while symptomatic PDA can be treated with both surgical and non-surgical methods. Surgically, the ductus arteriosus may be closed by ligation, wherein the DA is manually tied shut, or with intravascular coils or plugs that lead to the formation of a thrombus in the duct. Surgical ligation of the PDA can be accomplished with excellent results in uncomplicated patients. Recent experience with transcatheter closure has also been favorable, being today the procedure of choice for most patients.In certain cases it may be beneficial to the newborn to prevent the closure of the ductus arteriosus. For example, in transposition of the great vessels, a PDA may prolong the child’s life until surgical correction is possible. The ductus arteriosus can be induced to remain open by administering prostaglandin analogs.
Primary Prevention
The development of a fetal heart starts during the first trimester of pregnancy. Thus, many times the fetal heart has already developed, by the time the female becomes aware of being pregnant. There are some risk factors that if avoided before and during pregnancy can decrease the occurrence of congenital heart diseases.
References
Anatomy
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Priyamvada Singh, M.B.B.S. [2], Cafer Zorkun, M.D., Ph.D. [3], Assistant Editor-In-Chief: Kristin Feeney, B.S. [4]
Overview
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ramyar Ghandriz MD[2]
Overview
Ductus arteriosus was introduced centuries ago, but it is proven that from the 17th century the presence of such a duct was announced by many anatomists working on cadavers. It’s management and treatment underwent many controversies and caregivers always had their own management criteria for surgery or not overtime.
Historical Perspective
Discovery
- Ductus arteriosus has been identified at least from the 17th century by anatomists studying cadavers.
- For centuries caregivers had a controversy over treating PDA and many approaches evaluated.
- Evolution of the knowledge about ductus arteriosus can be reviewed in four overlapping epochs[1]:
- “The age of anatomical observation”
- “Early decades of cardiac surgery”
- “Golden age of fetal physiology”
- “Era of modern neonatal intensive care”
Landmark Events in the Development of Treatment Strategies
- In 1938 The first Surgery of PDA (ligation of the duct) by DR.Robert Gross at Boston Children’s Hospital.
- It was done on a 7 years old girl with PDA.
References
- ↑ Raju, Tonse N. K. (2019). “From Galen to Gross and beyond: a brief history of the enigmatic patent ductus arteriosus”. Journal of Perinatology. 39 (11): 1442–1448. doi:10.1038/s41372-019-0517-4. ISSN 0743-8346.
References
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Priyamvada Singh, M.B.B.S. [2], Cafer Zorkun, M.D., Ph.D. [3], Assistant Editor-In-Chief: Kristin Feeney, B.S. [4] Ramyar Ghandriz MD[5]
Overview
The pathophysiological consequences depend on the size of the defect and the pulmonary vascular resistance.Patent ductus arteriosus is a heart condition that is normal but reverses soon after birth. In a persistent PDA, there is an irregular transmission of blood between two of the most important arteries (aorta and pulmonary artery) in close proximity to the heart. Although the ductus arteriosus normally seals off within a few days, in PDA, the newborn‘s ductus arteriosus does not close, but remains patent.
Pathophysiology
Normal Ductus Arteriosus Closure
In the developing fetus, the ductus arteriosus (DA) is a shunt connecting the pulmonary artery to the aortic arch that allows much of the blood from the right ventricle to bypass the fetus’ fluid-filled lungs.[1] During fetal development, this shunt protects the right ventricle from pumping against the high resistance in the lungs, which can lead to right ventricular failure if the DA closes in-utero.
When the newborn takes its first breath, the lungs open and pulmonary pressure decreases below that of the left heart.[2] At the same time, the lungs release bradykinin to constrict the smooth muscle wall of the DA and reduce blood flow. Additionally, because of reduced pulmonary resistance, more blood flows from the pulmonary arteries to the lungs and thus the lungs deliver more oxygenated blood to the left heart. This further increases aortic pressure so that blood no longer flows from the pulmonary artery to the aorta via the DA. In normal newborns, the DA is closed within 15 hours after birth and is completely sealed after three weeks. The fall in circulating maternal prostaglandins contributes to this. A nonfunctional vestige of the DA, called the ligamentum arteriosum, remains in the normal adult heart.[1]
Abormal Closure of Ductus Arteriosus
The abnormal closure of the ductus arteriosus results in patent ductus arteriosus. Patent ductus arteriosus is a heart condition that is normal but reverses soon after birth. In a persistent PDA, there is an irregular transmission of blood between two of the most important arteries in close proximity to the heart. Although the ductus arteriosus normally seals off within a few days, in PDA, the newborn’s ductus arteriosus does not close, but remains patent.[3] PDA is common in infants with persistent respiratory problems such as hypoxia, and has a high occurrence in premature children. In hypoxic newborns, too little oxygen reaches the lungs to produce sufficient levels of bradykinin and subsequent closing of the DA. Premature children are more likely to be hypoxic and thus have PDA because of their underdeveloped heart and lungs.In some babies, on the other hand, the ductus arteriosus remains open. This opening permits blood to surge unswerving starting from the aorta into the pulmonary artery.
A patent ductus arteriosus allows oxygenated blood to flow down its pressure gradient from the aorta to the pulmonary arteries. Thus, some of the infant‘s oxygenated blood does not reach the body, and the infant becomes short of breath. The heart rate hastens, thereby increasing the speed with which blood is oxygenated and delivered to the body. Left untreated, the infant will likely suffer from congestive heart failure, as his heart is unable to meet the metabolic demands of his body.
In some cases, such as in transposition of the great vessels (the pulmonary artery and the aorta), a PDA may need to remain open. In this cardiovascular condition, the PDA is the only way that oxygenated blood can mix with deoxygenated blood. In these cases, prostaglandins are used to keep the patent ductus arteriosus open.
Shown below is the image below shows the gross anatomy of heart with patent ductus arteriosus.

Small-Sized PDA
- Small left-to-right shunt (Qp/Qs < 1.5)
- Normal ratio of pulmonary artery (PA) to systemic pressure.
- Shunt throughout the cardiac cycle, continuous murmur.
Medium-Sized PDA
- Qp/Qs 1.5 to 2.0 yet small enough to offer some resistance to flow.
- PA systolic to systemic pressures are < 0.5
- Unusual for this group to have markedly increased PVR.
- Due to increased return to the left heart, there is volume overload of the left atrium (LA) and the left ventricle (LV).
Large PDA
- Defect does not restrict flow.
- There is pulmonary hypertension at near systemic pressures (PA systolic/systolic pressure is >0.5).
- Because of the physiologic decrease in the PVR over the first three months of life there is a large left-to-right shunt with Qp/Qs > 2.
- The large volume overload of the left ventricle may result in LV failure.
- There is pulmonary hypertension.
- There may be two courses:
- A decrease in the relative size of the ductus compared with other cardiovascular structures. This results in a medium-sized defect compared with the course expected for a medium-sized defect.
- The development of severe pulmonary vascular obstructive disease, can occur at any time from age 3 until early adulthood. The left-to-right shunt converts to a right-to-left shunt with cyanosis and disappearance of the continuous murmur.
Gross Pathology
-
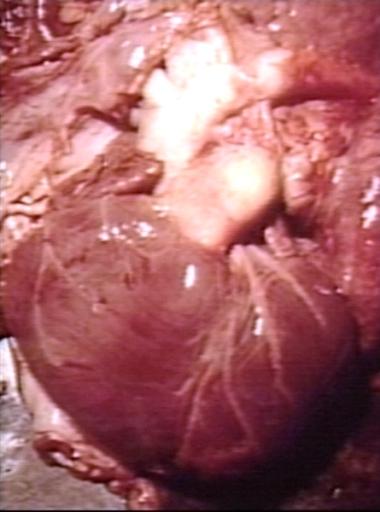
 Patent Ductus Arteriosus: Gross example in an infant heart
Patent Ductus Arteriosus: Gross example in an infant heart -
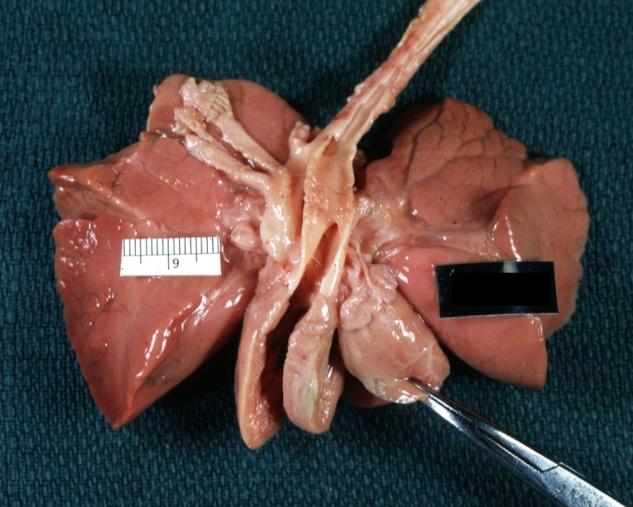
 Patent Ductus Arteriosus: Gross fixed tissue probe in ductus
Patent Ductus Arteriosus: Gross fixed tissue probe in ductus -
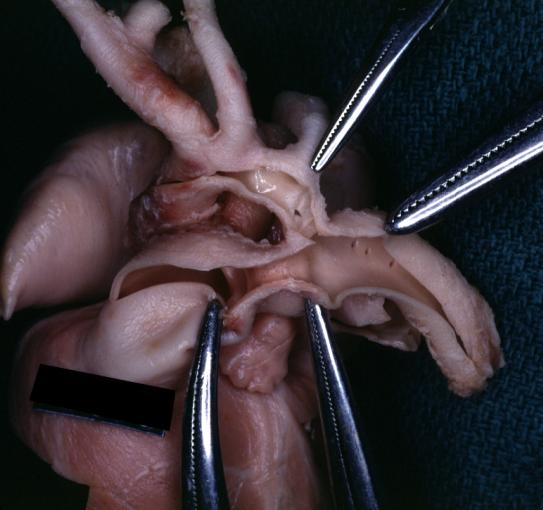
 Patent Ductus Arteriosus: Gross fixed tissue view of ductus opened from pulmonary artery into aorta with edematous appearing intimal surface
Patent Ductus Arteriosus: Gross fixed tissue view of ductus opened from pulmonary artery into aorta with edematous appearing intimal surface -
 Patent Ductus Arteriosus: Gross natural color opened ductus in infant shows apparent intimal edema in ductus.
Patent Ductus Arteriosus: Gross natural color opened ductus in infant shows apparent intimal edema in ductus.




-
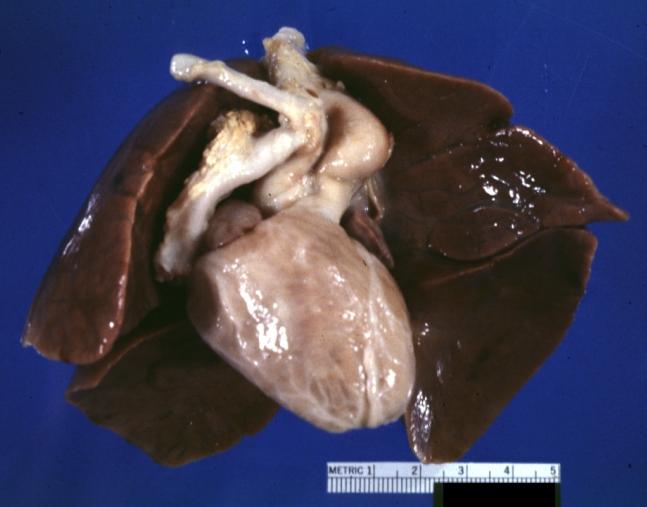 Patent Ductus Arteriosus with Aneurysmal Dilation: Gross fixed tissue external photo of heart shows the lesion
Patent Ductus Arteriosus with Aneurysmal Dilation: Gross fixed tissue external photo of heart shows the lesion -
 Patent Ductus Arteriosus with Aneurysmal Dilation: Gross fixed tissue aorta and ductus have been cross sectioned showing arch of aorta and huge ductus in a 5 day old infant
Patent Ductus Arteriosus with Aneurysmal Dilation: Gross fixed tissue aorta and ductus have been cross sectioned showing arch of aorta and huge ductus in a 5 day old infant -
 Patent Ductus Arteriosus with Aneurysmal Dilation: Gross fixed tissue opened aortic arch and descending thoracic showing very large opening of ductus into aorta
Patent Ductus Arteriosus with Aneurysmal Dilation: Gross fixed tissue opened aortic arch and descending thoracic showing very large opening of ductus into aorta -
 Patent Ductus Arteriosus
Patent Ductus Arteriosus




Shown below is the pictoral image of pathophysiology of patent ductus arteriosus

Shown below is the image of pathophysiology of patent ductus arteriosus in the cross-section of the heart

Videos
{{#ev:youtube|watch?v=7DKaCqubuSg}}
Diagram
Diagram of heart showing a patent ductus arteriosus

References
- ↑ 1.0 1.1 Hermes-DeSantis, E R; Clyman, R I (2006). “Patent ductus arteriosus: pathophysiology and management”. Journal of Perinatology. 26 (S1): S14–S18. doi:10.1038/sj.jp.7211465. ISSN 0743-8346.
- ↑ Clyman, Ronald I. (2006). “Mechanisms Regulating the Ductus Arteriosus”. Neonatology. 89 (4): 330–335. doi:10.1159/000092870. ISSN 1661-7800.
- ↑ Giuliani et al, Cardiology: Fundamentals and Practice, Second Edition, Mosby Year Book, Boston, 1991, pp. 1653-1663.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Priyamvada Singh, M.B.B.S. [2], Cafer Zorkun, M.D., Ph.D. [3], Assistant Editor-In-Chief: Kristin Feeney, B.S. [4] Ramyar Ghandriz MD[5]
Overview
Causes of Patent ductus arteriosus is not known. However, increased incidence have been associated with mother’s rubella and genetic causes
Causes
Common Causes
Common causes of patent ductus arteriosus may include:
- Genetic factors[1]
- PDA has is highly familial. It is shown that with the effect of environmental elements.
- Studies shown the inheritance is more contributed to autosomal dominant.[2]
- Congenital rubella[3]
- Fetal alcohol syndrome[4]
Less Common Causes
Less common causes of PDA include:
Causes by Organ System
| Cardiovascular | No underlying causes |
| Chemical/Poisoning | No underlying causes |
| Dental | No underlying causes |
| Dermatologic | No underlying causes |
| Drug Side Effect | Maternal Amphetamine, Clomifene, Phenytoin, Alcohol use |
| Ear Nose Throat | No underlying causes |
| Endocrine | No underlying causes |
| Environmental | Many underlying co founders in research |
| Gastroenterologic | No underlying causes |
| Genetic | Autosomal dominant inheritance reported |
| Hematologic | No underlying causes |
| Iatrogenic | No underlying causes |
| Infectious Disease | Congenital rubella infection |
| Musculoskeletal/Orthopedic | No underlying causes |
| Neurologic | No underlying causes |
| Nutritional/Metabolic | No underlying causes |
| Obstetric/Gynecologic | No underlying causes |
| Oncologic | No underlying causes |
| Ophthalmologic | No underlying causes |
| Overdose/Toxicity | No underlying causes |
| Psychiatric | No underlying causes |
| Pulmonary | No underlying causes |
| Renal/Electrolyte | No underlying causes |
| Rheumatology/Immunology/Allergy | No underlying causes |
| Sexual | No underlying causes |
| Trauma | No underlying causes |
| Urologic | No underlying causes |
| Miscellaneous | No underlying causes |
References
- ↑ Davidson HR (1993). “A large family with patent ductus arteriosus and unusual face”. J Med Genet. 30 (6): 503–5. PMC 1016426. PMID 8326495.
- ↑ Bhandari, V.; Zhou, G.; Bizzarro, M. J.; Buhimschi, C.; Hussain, N.; Gruen, J. R.; Zhang, H. (2009). “Genetic Contribution to Patent Ductus Arteriosus in the Premature Newborn”. PEDIATRICS. 123 (2): 669–673. doi:10.1542/peds.2008-1117. ISSN 0031-4005.
- ↑ Mekonnen, Demeke (2017). “Clinically confirmed congenital rubella syndrome: the role of echocardiography”. Ethiopian Journal of Health Sciences. 27 (2): 197. doi:10.4314/ejhs.v27i2.13. ISSN 1029-1857.
- ↑ Arishima, Kazuyoshi; Yamamoto, Masako; Takizawa, Tatsuya; Sohmiya, Hiroaki; Eguchi, Yasunobu; Shiota, Kohei (1993). “Effect of Acute Maternal Alcohol Consumption on the Fetal Ductus arteriosus in the Rat”. Neonatology. 63 (1): 40–43. doi:10.1159/000243906. ISSN 1661-7800.
- ↑ Reese, Jeff; Veldman, Alex; Shah, Lisa; Vucovich, Megan; Cotton, Robert B. (2010). “Inadvertent Relaxation of the Ductus Arteriosus by Pharmacologic Agents that are Commonly Used in the Neonatal Period”. Seminars in Perinatology. 34 (3): 222–230. doi:10.1053/j.semperi.2010.02.007. ISSN 0146-0005.
Differentiating Patent Ductus Arteriosus from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief:Cafer Zorkun, M.D., Ph.D. [2]; Keri Shafer, M.D. [3] Priyamvada Singh, MBBS[4] Ramyar Ghandriz MD[5]
Overview
Patent ductus arteriosus is very famouse due to its continuous machine-like murmur. There are some certain conditions that may make continuous murmur.
Differentiating Patent Ductus Arteriosus from other Diseases
- Patent ductus arteriosus should be differentiated from other conditions producing machine-like continuous murmur.
Differentiating Patent ductus arteriosus from other acyanotic congenital heart diseases:
| Diseases | Clinical manifestations | Para-clinical findings | Gold standard | Additional findings | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Symptoms | Physical examination | ||||||||||
| Imaging | |||||||||||
| Exertional dyspnea | Failure to thrive | Recurrent respiratory infections | Murmur on auscultation | Peripheral edema | Clubbing | Echocardiography | Chest x-ray | Cardiac CT | |||
| Patent ductus arteriosus |
|
|
– |
|
– |
|
|
|
|
|
|
| Atrial septal defect | +/− | +/− | +/− |
|
+/− | +/− |
|
|
|
|
|
| Ventricular septal defect | -/+ | -/+ | After Eisenmenger syndrome |
|
-/+ | -/+ |
|
|
|
|
– |
| Diseases | Exertional dyspnea | Failure to thrive | Recurrent respiratory infections | Murmur on auscultation | Peripheral edema | Clubbing | Echocardiography | Chest x-ray | Cardiac CT | Gold standard | Additional findings |
| Coarctation of the aorta | +/− | +/− | − |
|
– | – |
|
|
|
|
|
| Patent foramen ovale | − | − | − | − | − | − |
|
Non specific | − |
|
|
| Aortic stenosis | + | + | + |
|
+/- |
|
|
|
|
| |
| Pulmonary stenosis |
|
– | -/+ |
|
– | -/+ |
|
|
|
|
– |
Differential diagnosis of patent ductus arteriosus from other continuous machine-like murmur:[7][8][9]
| Diseases | Clinical manifestations | Para-clinical findings | Gold standard | Additional findings | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Symptoms | Physical examination | ||||||||||
| Imaging | |||||||||||
| Exercise intolerance | Respiratory distress | Failure to thrive | Cardiac auscultation | Cyanosis | Wide pulse pressure | Chest X-ray | Doppler Echocardiography | CT-scan | |||
| Patent Ductus Arteriosus | In medium to large size | In large size | In large size | Continuous Machine-like murmur | + | + | Left sided cardiomegaly | Left to right shunt | krichenco criteria | Charachtristic murmur | Increased QT-intrerval maybe seen |
| Venus Hum | – | – | – | Continuous murmur | – | – | Normal | Normal | Normal | ||
| Mammary Souffle | – | – | Does not apply | Continuous murmur | – | -/+ | Normal | Normal | Normal | Pregnancy related | |
| Diseases | Exercise intolerance | Respiratory distress | Failure to thrive | Machine-like murmur | Cyanosis | Wide pulse pressure | Chest X-ray | Doppler Echocardiography | CT-scan | Gold standard | Additional findings |
| Aortopulmonary Window | + | + | + | Continuous murmur | + | + | Cardiomegaly | Left to right shunt, Eisenmenger’s syndrome | Aortic aneurysm | ||
| Rupture of the Sinus of Valsalva | + | + | Does not apply | Continuous murmur | – | + | No change | Turbulent flow | Saccular aneurysm | Emergent surgery needed, more over after MI | |
| Fistulas of the Coronary Circulation | + | + | Does not apply | Continuous murmur | – | + | Unremarkable / Cardiomegaly | Not applied | Suggestive markers | Coronary artery Angiography | |
Differentiating Patent Ductus Arteriosus from other Diseases
Venous Hum
- Frequently heard in children over the base of the neck, usually best on the right side.
- Changes with position. Disappears in the supine position or with compression.
- Louder in diastole
Mammary Souffle
- Heard during late pregnancy and the early postpartum period in lactating women.
- Thought to be arterial in origin
- Can be bilateral
- Is louder, peaks in systole
- Vanishes in the upright position
- Abolishes by local compression
Aortopulmonary Window
- It’s a rare congenital opening between the aorta and the pulmonary trunk just above the aortic valve.
- It can be associated with other abnormalities like anomalous origin of the coronary arteries from the pulmonary trunk and coarctation of the aorta.
- The murmur is lower and more medial in location.
- In adults is presented without a murmur and clinical features of the Eisenmenger’s syndrome.
Rupture of the Sinus of Valsalva
- It can rupture into a cardiac chamber. Almost always arise from the right or the noncoronary cusps and rupture into the RV and RA respectively. Occasionally is acquired as a result of endocarditis. Large acute perforations tend to occur between puberty and age 30 causing severe retrosternal chest pain, dyspnea related to the large left-to-right shunt. The murmur is louder in a lower parasternal position. People with VSDs and sudden development of chest pain have frequently experienced rupture of a coexistent sinus of valsalva aneurysm. A rupture of the sinus of valsalva can distort or compress the coronary arteries and cause an infarction, distort the conduction system, cause AV block, distort the aortic valve, and cause AS or AI. Patients with rupture of the sinus of valsalva, should undergo surgical correction because mortality is high within a year of rupture.
Fistulas of the Coronary Circulation
- Generally a coronary artery that arises normally will communicate with the RV.
- Occasionally drain into the pulmonary trunk.
- The artery that forms the fistula is generally dilated, elongated, and tortuous. The left-to-right shunt is small.
- It may not be recognized radiographically.
- Patients with small fistula are generally asymptomatic. Therefore, no justification to repair it.
- On the other hand, if the shunt is extremely large, then failure may develop in the 4th, 5th or 6th decade of life. It can be treated with ligation.
Anomalous Origin of the Coronary Artery from the Pulmonary Trunk
- Usually refers to the origin of the left coronary artery from the pulmonary trunk.
- Approximately, 80 to 90% of the patients die in their first year of life due to ischemia.
- Blood from the high pressure RCA flows to the low pressure left coronary artery and the pulmonary artery.
- Anomalous origin of the RCA from the PA is much rarer, but these patients stand a better chance of surviving into adulthood because it is less likely to cause ischemia early in life.
Pulmonary Arteriovenous Fistula
- Instead of being localized to the precordium, these murmurs are localized to the lung fields. Cyanosis is presented with a normal heart size. Seen in Rendu-Osler-Weber syndrome. A fistula causing cyanosis could be treated with lobectomy if it is confined to a single lobe.
VSD and AR
Coarctation(Rarely)
References
- ↑ Morgan-Hughes, Gareth J.; Marshall, Andrew J.; Roobottom, Carl (2003). “Morphologic Assessment of Patent Ductus Arteriosus in Adults Using Retrospectively ECG-Gated Multidetector CT”. American Journal of Roentgenology. 181 (3): 749–754. doi:10.2214/ajr.181.3.1810749. ISSN 0361-803X.
- ↑ Edwards, DK; Higgins, CB; Merritt, TA; DiSessa, TG; Friedman, WF (1978). “Radiographic and echocardiographic evaluation of newborns treated with indomethacin for patent ductus arteriosus”. American Journal of Roentgenology. 131 (6): 1009–1013. doi:10.2214/ajr.131.6.1009. ISSN 0361-803X.
- ↑ Goitein, Orly; Fuhrman, Carl R.; Lacomis, Joan M. (2005). “Incidental Finding on MDCT of Patent Ductus Arteriosus: Use of CT and MRI to Assess Clinical Importance”. American Journal of Roentgenology. 184 (6): 1924–1931. doi:10.2214/ajr.184.6.01841924. ISSN 0361-803X.
- ↑ 4.0 4.1 Kellenberger, Christian J.; Yoo, Shi-Joon; Büchel, Emanuela R. Valsangiacomo (2007). “Cardiovascular MR Imaging in Neonates and Infants with Congenital Heart Disease”. RadioGraphics. 27 (1): 5–18. doi:10.1148/rg.271065027. ISSN 0271-5333.
- ↑ Wang, Zhen J.; Reddy, Gautham P.; Gotway, Michael B.; Yeh, Benjamin M.; Higgins, Charles B. (2003). “Cardiovascular Shunts: MR Imaging Evaluation”. RadioGraphics. 23 (suppl_1): S181–S194. doi:10.1148/rg.23si035503. ISSN 0271-5333.
- ↑ Gotway, Michael B.; Nagai, Brian K.; Reddy, Gautham P.; Patel, Rita A.; Higgins, Charles B.; Webb, W. Richard (2001). “Incidentally Detected Cardiovascular Abnormalities on Helical CT Pulmonary Angiography”. American Journal of Roentgenology. 176 (2): 421–427. doi:10.2214/ajr.176.2.1760421. ISSN 0361-803X.
- ↑ Groom, Dale (1955). “VENOUS HUM IN CARDIAC AUSCULTATION”. Journal of the American Medical Association. 159 (7): 639. doi:10.1001/jama.1955.02960240005002. ISSN 0002-9955.
- ↑ Scott, James T.; Murphy, Edmond A. (1958). “Mammary Souffle of Pregnancy”. Circulation. 18 (5): 1038–1043. doi:10.1161/01.CIR.18.5.1038. ISSN 0009-7322.
- ↑ Ghaderian, Mehdi (2012). “Aortopulmonary window in infants”. Heart Views. 13 (3): 103. doi:10.4103/1995-705X.102153. ISSN 1995-705X.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Priyamvada Singh, M.B.B.S. [2], Cafer Zorkun, M.D., Ph.D. [3], Ramyar Ghandriz MD[4]Assistant Editor-In-Chief: Kristin Feeney, B.S. [5]
Overview
The Patent ductus arteriosus (PDA) is commonly found in infants and constitutes only 2% of all congenital defects found in adults. The incidence is greater is in children who are born prematurely with history of perinatal asphyxia and infants with congenital rubella.
Epidemiology and Demographics
Prevalence
- The PDA is commonly found in infants and constitutes only 2% of all congenital defects found in adults.[1][2][3][4]
- It is an isolated defect in 75% of cases, and is isolated in almost all adult cases.
Incidence
- In the United States, the estimated incidence in children born at term is between 3 to 8 per 10,000 live births.[5][6]
- The incidence of patent ductus arteriosus has increased over the past few decades. This is in part due to increased survival in the premature infants.
- The incidence is greater in children who are born:[7][8][9]
- Prematurely, with a history of perinatal asphyxia, perinatal asphyxia delays the closure of the ductus.
- Approximately, 20% of neonates with respiratory distress syndrome have a patent ductus arteriosus.
- In babies who are less than 1500 g at birth, many studies show the incidence of a PDA to exceed 30%.
- The increased patency in these groups is thought to be due to both hypoxia in babies with respiratory distress and premature ductal closure mechanisms in premature babies.
- Increased incidences in infants with congenital rubella.
- Children born at high altitude.
Gender
- Females are more commonly affected by PDA than males. The female-to-male ratio is approximately 2:1.[10]
References
- ↑ El Hajjar, M (2005). “Severity of the ductal shunt: a comparison of different markers”. Archives of Disease in Childhood – Fetal and Neonatal Edition. 90 (5): F419–F422. doi:10.1136/adc.2003.027698. ISSN 1359-2998.
- ↑ Reller MD, Strickland MJ, Riehle-Colarusso T, Mahle WT, Correa A (2008). “Prevalence of congenital heart defects in metropolitan Atlanta, 1998-2005”. J Pediatr. 153 (6): 807–13. doi:10.1016/j.jpeds.2008.05.059. PMC 2613036. PMID 18657826.
- ↑ van der Linde D, Konings EE, Slager MA, Witsenburg M, Helbing WA, Takkenberg JJ; et al. (2011). “Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis”. J Am Coll Cardiol. 58 (21): 2241–7. doi:10.1016/j.jacc.2011.08.025. PMID 22078432.
- ↑ Riehle-Colarusso T, Strickland MJ, Reller MD, Mahle WT, Botto LD, Siffel C; et al. (2007). “Improving the quality of surveillance data on congenital heart defects in the metropolitan Atlanta congenital defects program”. Birth Defects Res A Clin Mol Teratol. 79 (11): 743–53. doi:10.1002/bdra.20412. PMID 17990334.
- ↑ Clyman, Ronald I. (2000). “Ibuprofen and Patent Ductus Arteriosus”. New England Journal of Medicine. 343 (10): 728–730. doi:10.1056/NEJM200009073431009. ISSN 0028-4793.
- ↑ Hoffman JI, Kaplan S (2002). “The incidence of congenital heart disease”. J Am Coll Cardiol. 39 (12): 1890–900. doi:10.1016/s0735-1097(02)01886-7. PMID 12084585.
- ↑ Hammerman C (1995). “Patent ductus arteriosus. Clinical relevance of prostaglandins and prostaglandin inhibitors in PDA pathophysiology and treatment”. Clin Perinatol. 22 (2): 457–79. PMID 7671547.
- ↑ Tanner K, Sabrine N, Wren C (2005). “Cardiovascular malformations among preterm infants”. Pediatrics. 116 (6): e833–8. doi:10.1542/peds.2005-0397. PMID 16322141.
- ↑ Forsey JT, Elmasry OA, Martin RP (2009). “Patent arterial duct”. Orphanet J Rare Dis. 4: 17. doi:10.1186/1750-1172-4-17. PMC 2716300. PMID 19591690.
- ↑ Record, R. G.; McKeown, T. (1953). “OBSERVATIONS RELATING TO THE AeTIOLOGY OF PATENT DUCTUS ARTERIOSUS”. Heart. 15 (4): 376–386. doi:10.1136/hrt.15.4.376. ISSN 1355-6037.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Priyamvada Singh, M.B.B.S. [2], Cafer Zorkun, M.D., Ph.D. [3],Ramyar Ghandriz MD[4] Assistant Editor-In-Chief: Kristin Feeney, B.S.[5]
Overview
Like many congenital heart disease, the cause of patent ductus arteriosus is not clear. Clinical studies suggest that the genetic and environmental factors both play an important role during the pregnancy.
Risk factors
Factors in the mother that may increase the risk of patent ductus arteriosus condition include:[1]
- Age over 40
- Alcoholism
- Diabetes
- Prenatal nutrition
- Rubella or other viral illness during pregnancy
- Genetic disorders such as Down syndrome
References
- ↑ Cotton, Robert B.; Lindstrom, Daniel P.; Stahlman, Mildred T. (1981). “EARLY PREDICTION OF SYMPTOMATIC PATENT DUCTUS ARTERIOSUS FROM PERINATAL RISK FACTORS: A DISCRIMINANT ANALYSIS MODEL”. Acta Paediatrica. 70 (5): 723–727. doi:10.1111/j.1651-2227.1981.tb05775.x. ISSN 0803-5253.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Priyamvada Singh, M.B.B.S. [2], Cafer Zorkun, M.D., Ph.D. [3], Ramyar Ghandriz MD[4] Assistant Editor-In-Chief: Kristin Feeney, B.S. [5]
Overview
The natural history of unoperated patients of patent ductus arteriosus (PDA) depends on the amount of left to right shunting. The left to right shunting in turn depends on the size of ductus and the difference in resistance between the left and right side of heart. PDA can cause complications such as heart failure, infective endocarditis, rhythm disturbance, pulmonary hypertension and Eisenmenger syndrome.
Natural History, Complications, and Prognosis
Natural History
Small PDA
- May remain asymptomatic[1]
- Rarely can increase the risk of endarteritis[2]
Moderate PDA
- Left sided heart dysfunction
- Rhythm disturbances like atrial fibrillation as a result of left sided dysfunction
Large PDA
- Left ventricular volume overload
- Increased pulmonary resistance
- Eisenmenger’s syndrome
Complications
Heart Failure
- Clinical feature – failure to thrive, feeding difficulties and respiratory distress[3]
- If PDA left untreated it will lead to cardiac volume overload which ultimately results in heart failure
- Management involves:[4]
Infective Endocarditis
- Infective endocarditis is a very complication of persistent ductus arteriosus.[5]
- Increases risk of septic emboli to lung[6]
- PDA complicated with infective endocarditis is an indication for closure of PDA.[7]
Rhythm Disturbance
- Often associated with atrial fibrillation (left sided dysfunction).[8]
Pulmonary Hypertension
- Right ventricular impulse on palpation[9][10]
- Pulmonary ejection sound
- A loud single second heart sound
- Graham-Steel murmur: The Graham-Steel murmur of pulmonic regurgitation and hypertension. It is high-pitched and “blowing.”
Complications during pregnancy
- In pregnancy PDA posses a very high significant risk for both the mother and the baby.[11][12][13][14]
- If PDA is small it is mostly asymptomatic.
- If PDA is moderate it might lead to increased pulmonary vascular resistance which complicates the pregnancy.
- If PDA is large it might lead to eisenmenger syndrome which increases both morbidity and mortality of the baby and the mother.
Prognosis
Prognosis of patent ductus arteriosus varies widely. It depends on:[15]
- The size of patent ductus arteriosus
- Whether the patient has been treated with closure medicines.
- Whether surgery has been done.
- Whether the patient with complications or not, such as heart failure, problems with lung development, or infective endocarditis.
References
- ↑ Campbell, M (1968). “Natural history of persistent ductus arteriosus”. Heart. 30 (1): 4–13. doi:10.1136/hrt.30.1.4. ISSN 1355-6037.
- ↑ Sadiq M, Latif F, Ur-Rehman A (2004). “Analysis of infective endarteritis in patent ductus arteriosus”. Am J Cardiol. 93 (4): 513–5. doi:10.1016/j.amjcard.2003.10.062. PMID 14969641.
- ↑ Gillam-Krakauer, Maria; Reese, Jeff (2018). “Diagnosis and Management of Patent Ductus Arteriosus”. NeoReviews. 19 (7): e394–e402. doi:10.1542/neo.19-7-e394. ISSN 1526-9906.
- ↑ “StatPearls”. 2020. PMID 28613509.
- ↑ Morris CD, Reller MD, Menashe VD (1998). “Thirty-year incidence of infective endocarditis after surgery for congenital heart defect”. JAMA. 279 (8): 599–603. doi:10.1001/jama.279.8.599. PMID 9486754.
- ↑ Satoh, Tadashi; Nishida, Naoki (2008). “Patent Ductus Arteriosus with Infective Endocarditis at Age 92”. Internal Medicine. 47 (4): 263–268. doi:10.2169/internalmedicine.47.0445. ISSN 0918-2918.
- ↑ Thilén U, Aström-Olsson K (1997). “Does the risk of infective endarteritis justify routine patent ductus arteriosus closure?”. Eur Heart J. 18 (3): 503–6. doi:10.1093/oxfordjournals.eurheartj.a015272. PMID 9076389.
- ↑ Wiyono, S. A.; Witsenburg, M.; de Jaegere, P. P. T.; Roos-Hesselink, J. W. (2008). “Patent ductus arteriosus in adults”. Netherlands Heart Journal. 16 (7): 255–259. doi:10.1007/BF03086157. ISSN 1568-5888.
- ↑ Lehner, Anja; Ulrich, Sarah; Happel, Christoph M.; Fischer, Marcus; Kantzis, Marinos; Schulze-Neick, Ingram; Haas, Nikolaus A. (2017). “Closure of very large PDA with pulmonary hypertension: Initial clinical case-series with the new Occlutech®PDA occluder”. Catheterization and Cardiovascular Interventions. 89 (4): 718–725. doi:10.1002/ccd.26856. ISSN 1522-1946.
- ↑ Chen WJ, Chen JJ, Lin SC, Hwang JJ, Lien WP (1995). “Detection of cardiovascular shunts by transesophageal echocardiography in patients with pulmonary hypertension of unexplained cause”. Chest. 107 (1): 8–13. doi:10.1378/chest.107.1.8. PMID 7813317.
- ↑ Kumar P, Sinha SK, Pandey U, Thakur R, Varma CM, Sachan M; et al. (2016). “Patent Ductus Arteriosus With Eisenmenger Syndrome: Difficult Diagnosis Made Easily With Saline Contrast Echocardiography”. Cardiol Res. 7 (3): 117–118. doi:10.14740/cr447w. PMC 5295518. PMID 28197278.
- ↑ Kumar P, Sinha SK, Pandey U, Thakur R, Varma CM, Sachan M; et al. (2016). “Patent Ductus Arteriosus With Eisenmenger Syndrome: Difficult Diagnosis Made Easily With Saline Contrast Echocardiography”. Cardiol Res. 7 (3): 117–118. doi:10.14740/cr447w. PMC 5295518. PMID 28197278.
- ↑ Kumar, Prakash; Sinha, Santosh Kumar; Pandey, Umeshwar; Thakur, Ramesh; Varma, Chandra Mohan; Sachan, Mohit; Goel, Amit (2016). “Patent Ductus Arteriosus With Eisenmenger Syndrome: Difficult Diagnosis Made Easily With Saline Contrast Echocardiography”. Cardiology Research. 7 (3): 117–118. doi:10.14740/cr447w. ISSN 1923-2829.
- ↑ Ryan, John J.; Suksaranjit, Promporn; Hatton, Nathan; Bull, David A.; Wilson, Brent D. (2015). “Eisenmenger Syndrome With Unrepaired Patent Ductus Arteriosus”. Circulation. 131 (16). doi:10.1161/CIRCULATIONAHA.114.013810. ISSN 0009-7322.
- ↑ Benn J (1947). “THE PROGNOSIS OF PATENT DUCTUS ARTERIOSUS”. Br Heart J. 9 (4): 283–91. doi:10.1136/hrt.9.4.283. PMC 503595. PMID 18610079.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | Chest X Ray | CT | MRI | Echocardiography | Other Imaging Findings
Treatment
Treatment
Medical Therapy: Preterm Infants | Term and Older Children
Surgery | Primary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH