
Ovarian cancer
For patient information click here.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Monalisa Dmello, M.B,B.S., M.D. [2], Huda A. Karman, M.D.
Synonyms and keywords: Carcinoma of the ovary, Epithelial ovarian cancer (EOC)
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Huda A. Karman, M.D. Alberto Castro Molina, M.D.
Overview
Ovarian cancer is a malignant tumor arising from the ovary, fallopian tube, or peritoneum. In contemporary classification, epithelial ovarian carcinoma is considered together with fallopian tube and primary peritoneal carcinomas as a single disease entity because these tumors share similar molecular features, patterns of spread, and clinical behavior.[1][2] Epithelial malignancies account for roughly 90% of ovarian cancers, of which 70% to 80% are high-grade serous carcinomas; other major histologic types include endometrioid, clear cell, mucinous, and low-grade serous carcinomas, as well as borderline tumors.[1][3]
Globally, ovarian cancer is an important cause of cancer morbidity and mortality in women. GLOBOCAN 2022 estimates more than 320,000 new cases and over 200,000 deaths worldwide, corresponding to age-standardized incidence and mortality rates of approximately 6–7 and 4 per 100,000 women-years, respectively.[4][5] In the United States, ovarian cancer remains a leading cause of gynecologic cancer death, but both incidence and mortality have declined by roughly 3% per year since the mid-2000s, a trend attributed largely to increased use of oral contraceptives and uptake of risk-reducing salpingo-oophorectomy among women with high-risk genetic variants.[6][1]
The understanding of epithelial ovarian cancer pathogenesis has shifted from the traditional concept of an origin in the ovarian surface epithelium to a model in which many high-grade serous carcinomas arise from serous tubal intraepithelial carcinoma (STIC) in the fimbrial end of the fallopian tube, with subsequent implantation on the ovary and peritoneal surfaces.[7][2] Endometrioid and clear cell carcinomas are strongly associated with endometriosis, whereas some mucinous tumors may originate in the ovary or represent metastases from gastrointestinal primaries.[8] Approximately 50% of high-grade serous ovarian cancers are characterized by homologous recombination deficiency (HRD), including germline or somatic variants in BRCA1, BRCA2, and other DNA-repair genes, which has important implications for platinum sensitivity and benefit from poly (ADP-ribose) polymerase (PARP) inhibitors.[9][10]
Hereditary factors account for roughly one quarter of epithelial ovarian cancers, most commonly germline variants in BRCA1 and BRCA2, although pathogenic variants in other homologous recombination and mismatch repair genes also contribute.[11][12] Current guidelines recommend that all patients with epithelial ovarian, fallopian tube, or peritoneal carcinoma undergo germline testing (and, when indicated, somatic tumor testing) for hereditary cancer susceptibility genes, as this information influences treatment decisions, surveillance strategies, and cascade testing of relatives.[13]
Beyond genetic predisposition, risk factors for ovarian cancer include reproductive and hormonal factors such as endometriosis, infertility, and use of postmenopausal estrogen therapy without adequate progestin, as well as lifestyle and environmental exposures.[8][14] Protective factors include multiparity, breastfeeding, and use of combined oral contraceptives, which are associated with substantial relative risk reductions in both the general population and among BRCA1/2 carriers.[15][16] Risk-reducing salpingo-oophorectomy significantly decreases ovarian cancer risk and overall mortality in BRCA1/2 mutation carriers and is a cornerstone of preventive strategies in this population.[17][18][19]
Early detection of ovarian cancer is challenging because there are no effective screening tests for average-risk women. Large randomized trials of screening with CA-125 and transvaginal ultrasonography have not demonstrated a clear mortality benefit and have led to false-positive results and unnecessary surgery; therefore, routine screening is not recommended for asymptomatic women at average risk.[20][1] Instead, clinical attention is focused on timely evaluation of symptoms and risk assessment in women with hereditary predisposition.[21]
Most patients lack specific symptoms until disease is advanced, and approximately 70% to 80% of epithelial ovarian cancers are diagnosed at stage III or IV.[1][22] When present, symptoms are typically nonspecific and may include abdominal bloating or distension, early satiety, pelvic or abdominal pain, urinary urgency or frequency, changes in bowel habits, and unintentional weight loss.[22][21] Definitive diagnosis and staging require surgical exploration to determine the origin and extent of disease and to obtain tissue for histopathologic and molecular evaluation.[3][23]
Early-stage disease (confined to the ovaries or fallopian tubes) is primarily managed with comprehensive surgical staging and, in selected stage I cases, adjuvant platinum-based chemotherapy; 5-year overall survival for appropriately treated early-stage disease is approximately 70% to 95%.[23][1] Advanced-stage disease typically requires cytoreductive surgery combined with platinum-taxane chemotherapy, delivered either as primary debulking surgery followed by adjuvant chemotherapy or as neoadjuvant chemotherapy followed by interval debulking in patients with high tumor burden or poor performance status.[3][24] For patients with advanced-stage high-grade serous carcinoma who respond to initial platinum-based chemotherapy, maintenance therapy with PARP inhibitors, with or without the anti-angiogenic agent bevacizumab, improves progression-free survival, particularly in those with BRCA1/2 variants or HRD-positive tumors.[10][1] Nonetheless, most patients with advanced epithelial ovarian cancer eventually relapse, and 5-year overall survival in this group remains approximately 10% to 40% despite modern systemic therapy.[3][23]
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 Caruso G, Weroha SJ, Cliby W (2025). “Ovarian cancer: a review”. JAMA.
- ↑ 2.0 2.1 WHO Classification of Tumours Editorial Board (2020). “Female genital tumours”. World Health Organization Classification of Tumours. IARC Press. 5th ed.
- ↑ 3.0 3.1 3.2 3.3 González-Martín A, Harter P, Leary A, et al; ESMO Guidelines Committee (2023). “Newly diagnosed and relapsed epithelial ovarian cancer: ESMO clinical practice guideline for diagnosis, treatment and follow-up”. Ann Oncol. 34 (10): 833–848. doi:10.1016/j.annonc.2023.07.011.
- ↑ Bray F, Laversanne M, Sung H; et al. (2024). “Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries”. CA Cancer J Clin. 74 (3): 229–263. doi:10.3322/caac.21834.
- ↑ Cabasag CJ, Fagan PJ, Ferlay J; et al. (2022). “Ovarian cancer today and tomorrow: a global assessment by world region and Human Development Index using GLOBOCAN 2020”. Int J Cancer. 151 (9): 1535–1541. doi:10.1002/ijc.34002.
- ↑ Siegel RL, Kratzer TB, Giaquinto AN, Sung H, Jemal A (2025). “Cancer statistics, 2025”. CA Cancer J Clin. 75 (1): 10–45. doi:10.3322/caac.21871.
- ↑ Karnezis AN, Cho KR, Gilks CB, Pearce CL, Huntsman DG (2017). “The disparate origins of ovarian cancers: pathogenesis and prevention strategies”. Nat Rev Cancer. 17 (1): 65–74. doi:10.1038/nrc.2016.113.
- ↑ 8.0 8.1 Barnard ME, Farland LV, Yan B; et al. (2024). “Endometriosis typology and ovarian cancer risk”. JAMA. 332 (6): 482–489. doi:10.1001/jama.2024.9210.
- ↑ Konstantinopoulos PA, Ceccaldi R, Shapiro GI, D’Andrea AD (2015). “Homologous recombination deficiency: exploiting the fundamental vulnerability of ovarian cancer”. Cancer Discov. 5 (11): 1137–1154. doi:10.1158/2159-8290.CD-15-0714.
- ↑ 10.0 10.1 Caruso G, Tomao F, Parma G; et al. (2023). “Poly (ADP-ribose) polymerase inhibitors in ovarian cancer: lessons learned and future directions”. Int J Gynecol Cancer. 33 (4): 431–443. doi:10.1136/ijgc-2022-004149.
- ↑ Kotsopoulos J, Gronwald J, Karlan B, et al; Hereditary Ovarian Cancer Clinical Study Group (2018). “Age-specific ovarian cancer risks among women with a BRCA1 or BRCA2 mutation”. Gynecol Oncol. 150 (1): 85–91. doi:10.1016/j.ygyno.2018.05.011.
- ↑ Bonadona V, Bonaïti B, Olschwang S, et al; French Cancer Genetics Network (2011). “Cancer risks associated with germline mutations in MLH1, MSH2, and MSH6 genes in Lynch syndrome”. JAMA. 305 (22): 2304–2310. doi:10.1001/jama.2011.743.
- ↑ Konstantinopoulos PA, Norquist B, Lacchetti C; et al. (2020). “Germline and somatic tumor testing in epithelial ovarian cancer: ASCO guideline”. J Clin Oncol. 38 (11): 1222–1245. doi:10.1200/JCO.19.02960.
- ↑ Tanha K, Mottaghi A, Nojomi M; et al. (2021). “Investigation on factors associated with ovarian cancer: an umbrella review of systematic review and meta-analyses”. J Ovarian Res. 14 (1): 153. doi:10.1186/s13048-021-00911-z.
- ↑ van Bommel MH, IntHout J, Veldmate G; et al. (2023). “Contraceptives and cancer risks in BRCA1/2 pathogenic variant carriers: a systematic review and meta-analysis”. Hum Reprod Update. 29 (2): 197–217. doi:10.1093/humupd/dmac038.
- ↑ Iodice S, Barile M, Rotmensz N; et al. (2010). “Oral contraceptive use and breast or ovarian cancer risk in BRCA1/2 carriers: a meta-analysis”. Eur J Cancer. 46 (12): 2275–2284. doi:10.1016/j.ejca.2010.04.018.
- ↑ Marchetti C, De Felice F, Palaia I; et al. (2014). “Risk-reducing salpingo-oophorectomy: a meta-analysis on impact on ovarian cancer risk and all-cause mortality in BRCA1 and BRCA2 mutation carriers”. BMC Womens Health. 14: 150. doi:10.1186/s12905-014-0150-5.
- ↑ Walker JL, Powell CB, Chen LM; et al. (2015). “Society of Gynecologic Oncology recommendations for the prevention of ovarian cancer”. Cancer. 121 (13): 2108–2120. doi:10.1002/cncr.29321.
- ↑ American College of Obstetricians and Gynecologists (2019). “ACOG Committee Opinion No. 774: opportunistic salpingectomy as a strategy for epithelial ovarian cancer prevention”. Obstet Gynecol. 133 (4): e279–e284. doi:10.1097/AOG.0000000000003164.
- ↑ US Preventive Services Task Force (2018). “Screening for ovarian cancer: US Preventive Services Task Force recommendation statement”. JAMA. 319 (6): 588–594. doi:10.1001/jama.2017.21926.
- ↑ 21.0 21.1 Huepenbecker SP, Sun CC, Fu S; et al. (2021). “Factors impacting the time to ovarian cancer diagnosis based on classic symptom presentation in the United States”. Cancer. 127 (22): 4151–4160. doi:10.1002/cncr.33778.
- ↑ 22.0 22.1 Goff BA, Mandel LS, Melancon CH, Muntz HG (2004). “Frequency of symptoms of ovarian cancer in women presenting to primary care clinics”. JAMA. 291 (22): 2705–2712. doi:10.1001/jama.291.22.2705.
- ↑ 23.0 23.1 23.2 Berek JS, Renz M, Kehoe S, Kumar L, Friedlander M (2021). “Cancer of the ovary, fallopian tube, and peritoneum: 2021 update”. Int J Gynaecol Obstet. 155 (suppl 1): 61–85. doi:10.1002/ijgo.13878.
- ↑ Fleming ND, Nick AM, Coleman RL; et al. (2018). “Laparoscopic surgical algorithm to triage the timing of tumor reductive surgery in advanced ovarian cancer”. Obstet Gynecol. 132 (3): 545–554. doi:10.1097/AOG.0000000000002796.
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Huda A. Karman, M.D.
Overview
Ovarian cancer was first linked to gene mutations by Dr. King who found and named BRCA1 gene on chromosome 17 in 1990 and BRCA2 gene on chromosome 13 in 1994.
Historical Perspective
- In the 16th and 17th centuries, Dr. Lusitani and Dr. Tulp from Holand, believed that cancers are contagious after they noticed the presence of breast cancers in the same household members.[1][2][3]
- In 1990, Dr. Mary-Claire King, the professor of genome sciences from Chicago, was the first one to link the single gene on chromosome 17 to many breast and ovarian cancers, after many years of research to find evidence that there is a genetic pattern linked to the incidence of complex diseases.
- In 1991, King named the gene that is linked to many breast and ovarian cancers as BRCA1.[4]
- In 1994, King also found and named the second gene, BRCA2 on chromosome 13.[5]
- 1996, King and the Breast Cancer research foundation, conducted a study on women of Ashkenazi Jewish ancestry in NYC and also on Palestinian women, which lead to the definitive confirmation that mutations in BRCA1 and BRCA2 is linked to the incidence of ovarian and breast cancer.
References
- ↑ Winer E, Gralow J, Diller L, Karlan B, Loehrer P, Pierce L; et al. (2009). “Clinical cancer advances 2008: major research advances in cancer treatment, prevention, and screening–a report from the American Society of Clinical Oncology”. J Clin Oncol. 27 (5): 812–26. doi:10.1200/JCO.2008.21.2134. PMC 2645086. PMID 19103723.
- ↑ Diamandopoulos GT (1996). “Cancer: an historical perspective”. Anticancer Res. 16 (4A): 1595–602. PMID 8712676.
- ↑ Hajdu SI (2011). “A note from history: landmarks in history of cancer, part 1”. Cancer. 117 (5): 1097–102. doi:10.1002/cncr.25553. PMID 20960499.
- ↑ Apostolou, Paraskevi; Fostira, Florentia (2013). “Hereditary Breast Cancer: The Era of New Susceptibility Genes”. BioMed Research International. 2013: 1–11. doi:10.1155/2013/747318. ISSN 2314-6133.
- ↑ Godet, Inês; M. Gilkes, Daniele (2017). “BRCA1 and BRCA2 mutations and treatment strategies for breast cancer”. Integrative Cancer Science and Therapeutics. 4 (1). doi:10.15761/ICST.1000228. ISSN 2056-4546.
Classifications
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Huda A. Karman, M.D.
Overview
Ovarian cancer may be classified according to the histology of the tumor, obtained in a pathology report. Based on the classification, the management of ovarian cancer is directed and determined. The main four types of ovarian cancer are Surface epithelial-stromal tumour, Sex cord-stromal tumor, Germ cell tumor, and Mixed tumors.
Classification
- Histology dictates many aspects of clinical treatment, management, and prognosis.[1][2][3][4]
- Surface epithelial-stromal tumor, including serous and mucinous cystadenocarcinoma, is the most common type of ovarian cancer.
- Sex cord-stromal tumor, including estrogen-producing granulosa cell tumor and virilizing Sertoli-Leydig cell tumor or arrhenoblastoma, accounts for 8% of ovarian cancers.
- Germ cell tumor accounts for approximately 5% of ovarian cancers. It tends to occur in young women and girls, and has a better prognosis than other ovarian tumors.
- Mixed tumors, containing elements of more than one tumor histology
- Ovarian cancer often is primary, but can also be secondary, the result of metastasis from a primary cancer elsewhere in the body. For example, from breast cancer, or from gastrointestinal cancer (in which case the ovarian cancer is a Krukenberg cancer). Surface epithelial-stromal tumor can originate in the lining of the abdominal cavity, in which case the ovarian cancer is secondary to primary peritoneal cancer, but treatment is basically the same as for primary ovarian cancer of this type. [1][2][3][4][5][6]
| Ovarian cancer Types | Ovarian cancer subtypes |
|---|---|
| Surface epithelial-stromal tumour (60-70%) | Ovarian serous tumor |
| |
| |
| |
| Ovarian mucinous tumor | |
| |
| |
| |
| Ovarian endometrioid tumour | |
| |
| Brenner tumour | |
| |
| Squamous cell carcinoma of the ovary | |
| |
| Ovarian cystadenofibroma / ovarian adenofibroma | |
| |
| Ovarian cystadenocarcinofibroma | |
| |
| Undifferentiated carcinoma of the ovary | |
| |
| Germ cell ovarian tumor (~20%) | Ovarian teratoma: commonest primary benign tumour of ovary |
| |
| |
| |
| |
| |
| Ovarian dysgerminoma | |
| Ovarian yolk sac tumour | |
| |
| Ovarian embryonal carcinoma | |
| Ovarian choriocarcinoma | |
| |
| Pure primary ovarian choriocarcinoma | |
| |
| Malignant mixed germ cell tumour of the ovary | |
| Sex cord / stromal ovarian tumor (8-10%)[5][6] | Ovarian fibrothecoma |
| |
| Ovarian fibroma | |
| |
| Sclerosing stromal tumour of the ovary | |
| |
| Ovarian Sertoli-Leydig cell tumour – ovarian androblastoma | |
| |
| Granulosa cell tumour of ovary | |
| |
| Juvenile granulosa cell tumour of ovary | |
| Adult granulosa cell tumour of ovary | |
| Others | Ovarian carcinosarcoma <1% |
| |
| |
| Metastases to the ovary | Krukenburg tumour |
| Other metastatic lesions to ovary |
References
- ↑ 1.0 1.1 Heintz AP, Odicino F, Maisonneuve P, Beller U, Benedet JL, Creasman WT; et al. (2001). “Carcinoma of the ovary”. J Epidemiol Biostat. 6 (1): 107–38. PMID 11385772.
- ↑ 2.0 2.1 Banks E (2001). “The epidemiology of ovarian cancer”. Methods Mol Med. 39: 3–11. doi:10.1385/1-59259-071-3:3. PMID 21340753.
- ↑ 3.0 3.1 Singer G, Oldt R, Cohen Y, Wang BG, Sidransky D, Kurman RJ; et al. (2003). “Mutations in BRAF and KRAS characterize the development of low-grade ovarian serous carcinoma”. J Natl Cancer Inst. 95 (6): 484–6. doi:10.1093/jnci/95.6.484. PMID 12644542.
- ↑ 4.0 4.1 Singer G, Stöhr R, Cope L, Dehari R, Hartmann A, Cao DF; et al. (2005). “Patterns of p53 mutations separate ovarian serous borderline tumors and low- and high-grade carcinomas and provide support for a new model of ovarian carcinogenesis: a mutational analysis with immunohistochemical correlation”. Am J Surg Pathol. 29 (2): 218–24. PMID 15644779.
- ↑ 5.0 5.1 Chen VW, Ruiz B, Killeen JL, Coté TR, Wu XC, Correa CN (2003). “Pathology and classification of ovarian tumors”. Cancer. 97 (10 Suppl): 2631–42. doi:10.1002/cncr.11345. PMID 12733128.
- ↑ 6.0 6.1 Young RH (2005). “Sex cord-stromal tumors of the ovary and testis: their similarities and differences with consideration of selected problems”. Mod Pathol. 18 Suppl 2: S81–98. doi:10.1038/modpathol.3800311. PMID 15502809.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Huda A. Karman, M.D.
Overview
Ovarian cancer is usually diagnosed late resulting in a poor overall outcome for the patient. Pathological findings, therefore, often only occur in advanced symptomatic onset and tend to present more as severe pathologic outcomes.
Pathophysiology
Clear Cell Tumor
- Clear cell tumors are part of the surface epithelial-stromal tumor group of ovarian cancers, accounting for 6% of all neoplastic cases. Clear cell tumors are also associated with the pancreas and salivary glands.
- Benign and borderline variants of this neoplasm are rare, and most cases are malignant.
- Typically, they are cystic neoplasms with polypoid masses that protrude into the cyst.
Endometrioid Tumor
Endometrioid tumors are part of the surface epithelial tumor group of ovarian neoplasms (10-20% of which are the endometrioid type). Benign and borderline variants are rare, as the majority are malignant. There is an association with endometriosis and concurrent primary endometrial carcinoma (endometrial cancer).
Gross Patholgy
| Ovarian Carcinomas Subtype | Features on Gross Pathology |
| Ovarian serous cystadenocarcinoma |
|
| Ovarian mucinous cystadenocarcinoma |
|
| Endometrioid carcinoma of the ovary |
|
Microscopic Pathology
Histologic subtypes of epithelial ovarian tumor include:[1][2][3][4]
- Surface epithelial stromal ovarian tumor (60-70%)
- Ovarian serous tumor
- Ovarian serous cystadenoma: ~60% of serous tumor
- Ovarian borderline serous cystadenoma: ~15% of serous tumor
- Ovarian serous cystadenocarcinoma: ~25% of serous tumor. Commonest malignant ovarian tumor
- Ovarian mucinous tumor: ~20% of all ovarian tumor
- Ovarian mucinous cystadenoma: ~80% of mucinous tumor
- Ovarian bordeline mucinous cystadenoma: 10-15% of mucinous tumor
- Ovarian mucinous cystadenocarcinoma: 5-10% of mucinous tumor
- Ovarian endometrioid tumour: 8-15% of all ovarian tumor
- Clear cell ovarian carcinoma: ~5% of ovarian cancer
- Brenner tumour: ~2.5% of ovarian epithelial neoplasms
- Squamous cell carcinoma of the ovary
- Ovarian cystadenofibroma / ovarian adenofibroma: can be serous, mucinous, endometrioid, clear cell or mixed
- Ovarian cystadenocarcinofibroma: extremely rare
- Undifferentiated carcinoma of the ovary: ~4% of all ovarian tumor
| Vulvar Carcinomas Subtype | Features on Histopathological Microscopic Analysis | Image |
| Ovarian serous cystadenocarcinoma |
|
|
| Ovarian mucinous cystadenocarcinoma |
|
|
| Endometrioid carcinoma of the ovary |
|
Clear cell tumor
Clear cell tumors can be either clear cell adenocarcinomas or clear cell sarcomas.On microscopic pathological examination, they are composed of cells with clear cytoplasm (that contains glycogen) and hob nail cells (from which the glycogen has been secreted).The pattern may be glandular, papillary or solid.
Shown below is an image of Overian clear cell adenocarcinoma.(H&E stain,very high mag)
-
 In this TAH-BSO specimen, the right ovary (on the left of the image) has been replaced by a solid serous carcinoma. The contralateral ovarian tumor is grossly cystic and could be termed a “cystadenocarcinoma.” The patient had omental metastases and positive peritoneal fluid cytology. This cancer, which was discovered at exploratory laparotomy, apparently developed very rapidly; the patient had a normal pelvic ultrasound exam only 2 months before. (Courtesy of Ed Uthman, MD)
In this TAH-BSO specimen, the right ovary (on the left of the image) has been replaced by a solid serous carcinoma. The contralateral ovarian tumor is grossly cystic and could be termed a “cystadenocarcinoma.” The patient had omental metastases and positive peritoneal fluid cytology. This cancer, which was discovered at exploratory laparotomy, apparently developed very rapidly; the patient had a normal pelvic ultrasound exam only 2 months before. (Courtesy of Ed Uthman, MD) -
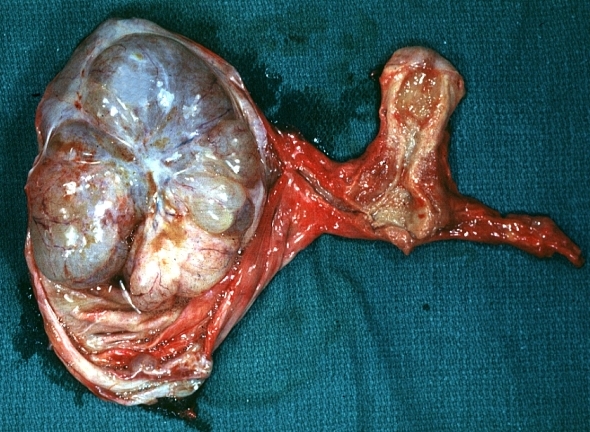 Ovary: Mucinous cystadenocarcinoma: Gross, an excellent image of uterus is in picture and thus illustrates the very large size of the ovarian tumor.
Ovary: Mucinous cystadenocarcinoma: Gross, an excellent image of uterus is in picture and thus illustrates the very large size of the ovarian tumor.
Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology


Video
Shown below is a video of clear cell adenocarcinoma of the vagina.
{{#ev:youtube|qO2w8VLf690}}
References
- ↑ Hoffman, Barbara (2012). Williams gynecology. New York: McGraw-Hill Medical. ISBN 9780071716727.
- ↑ Malignant melanoma. Libre pathology. http://librepathology.org/wiki/index.php/Malignant_melanoma. URL Accessed on September 30, 2015
- ↑ Basal cell carcinoma . Libre pathology. http://librepathology.org/wiki/index.php/Basal_cell_carcinoma. URL Accessed on September 30, 2015
- ↑ Squamous cell carcinoma. Libre pathology. http://librepathology.org/wiki/index.php/Squamous_cell_carcinoma. URL Accessed on September 30, 2015
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Huda A. Karman, M.D.
Overview
Ovarian cancer etiology is not completely understood but there are multiple risk factors that can play a role in its occurrence. The theories of the etiology of ovarian cancer suggest that repeated ovulation injures the ovarian epithelium and eventually leads to ovarian cancer development. The other theories discuss the origin of ovarian cancer that can be cortical inclusion cysts that become neoplastic or metaplastic or dysplastic changes of the fallopian tube. Direct effect of persistent Gonadotrophin release from the pituitary gland on the ovary also believed to play a role in ovarian cancer etiology.
Causes
- Ovarian cancer etiology is not completely understood but there are multiple risk factors that can play a role in its occurrence such as:
- Follicle stimulation or fertility drugs as Clomiphene[1]
- Based on multiple studies, the following are theories of the etiology of ovarian cancer:
- Theory 1:
- Repeated ovulations lead to injury of the ovarian epithelium and subsequent exposure to the inflammatory cytokine, transformation of the mesenchymal epithelium, alteration of the genes and hence cancer.
- With increased age, cortical inclusion cysts develop and its ovarian surface epithelium become metaplastic or neoplastic under the effect of accumulated inflammatory cytokines or stromal factors stimulation [2]
- Theory 2:
- Ovarian cancer originates from the fallopian tube. This theory evidenced by the presence of dysplastic changes in the fallopian tubes of women who underwent prophylactic removal of their ovaries.
- Theory 3:
- Persistent Gonadotrophin release from the pituitary gland has a direct effect on the ovarian epithelium and is considered carcinogenic [3]
- Theory 1:
Drug Side Effect
References
- ↑ Spirtas, Robert; Kaufman, Steven C.; Alexander, Nancy J. (1993). “Fertility drugs and ovarian cancer: red alert or red herring?”. Fertility and Sterility. 59 (2): 291–293. doi:10.1016/S0015-0282(16)55670-2. ISSN 0015-0282.
- ↑ Ottevanger, Petronella Beatrix (2017). “Ovarian cancer stem cells more questions than answers”. Seminars in Cancer Biology. 44: 67–71. doi:10.1016/j.semcancer.2017.04.009. ISSN 1044-579X.
- ↑ Fishel S, Jackson P (1989). “Follicular stimulation for high tech pregnancies: are we playing it safe?”. BMJ. 299 (6694): 309–11. doi:10.1136/bmj.299.6694.309. PMC 1837149. PMID 2535637.
Differentiating Ovarian cancer from other Disorders
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Fahimeh Shojaei, M.D. Huda A. Karman, M.D.
Overview
On the basis of age of onset, vaginal discharge, and constitutional symptoms, ovarian cancer must be differentiated from tubo-ovarian abscess, ectopic pregnancy, hydrosalpinx, salpingitis, fallopian tube carcinoma, uterine leiomyoma, choriocarcinoma, leiomyosarcoma, pregnancy, appendiceal abscess, appendiceal neoplasm, diverticular abscess, colorectal cancer, pelvic kidney, advanced bladder cancer, and retroperitoneal sarcoma.
Differentiating ovarian cancer from other Diseases
Differentiating ovarian cancer from other diseases on the basis of age of onset, vaginal discharge and constitutional symptoms
On the basis of age of onset, vaginal discharge, and constitutional symptoms, ovarian cancer must be differentiated from tubo-ovarian abscess, ectopic pregnancy, hydrosalpinx, salpingitis, fallopian tube carcinoma, uterine leiomyoma, choriocarcinoma, leiomyosarcoma, pregnancy, appendiceal abscess, appendiceal neoplasm, diverticular abscess, colorectal cancer, pelvic kidney, advanced bladder cancer, and retroperitoneal sarcoma.[1][2][3][4][5][6][7][8][9][10][11][12][13][14][15][16][17][18][19][20][21][22][23][24][25][26][27][28][29][30][31][32][33][34][35][36][37][38][39][40][41][42][43][44][45][46][47][48][49][50][51][52][53][54][55][56][57][58][59][60][61][62][63][64][65][66][67][68][69][70][71][72][73][74][75][76][77][78][79][80][81]
| Diseases | Clinical manifestations | Para-clinical findings | Gold standard | Additional findings | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age of onset | Symptoms | Physical examination | |||||||||||
| Lab Findings | Imaging | Immunohistopathology | |||||||||||
| Pelvic/abdominal pain or pressure | Vaginal bleeding/discharge | GI dysturbance | Fever | Tenderness | CT scan/US | MRI | |||||||
| Gynecologic | |||||||||||||
| Ovarian | Follicular cysts [1] |
|
+/– | – | – | – | +/– |
|
|
| |||
| Theca lutein cysts [2][3][4] |
|
+/– | – | – | – | +/– |
|
|
|
| |||
| Serous cystadenoma/carcinoma [5][6][7][8] |
|
+/– | – | – | – | +/– |
|
|
| ||||
| Mucinous cystadenoma/carcinoma [9][10][11] |
|
+/– | – | – | – | +/– |
|
|
|
| |||
| Endometrioma [12][13][14] |
|
+ | + | +/– | – | + |
|
|
|
| |||
| Teratoma [15][16][17][18] |
|
+/– | – | – | – | +/– |
|
|
| ||||
| Dysgerminoma [19][20] |
|
+ | +/– | – | – | +/– |
|
|
|
||||
| Yolk sac tumor [21][22][23] |
+ | – | – | – | + |
|
|
|
|
| |||
| Fibroma [24][25][26] |
|
|
– | – | – | +/– |
|
|
|
| |||
| Thecoma [27][28][29] |
|
+/– | – | – | – |
|
|
|
|
| |||
| Granulosa cell tumor [30][31][32][33] |
|
+ | +/– | – | – |
|
| ||||||
| Sertoli-leydig cell tumor [34][35] |
|
+/– | – | – | – | – |
|
|
|
| |||
| Brenner tumor [36][37] |
|
+/– | – | – | – | – | – |
|
|
|
| ||
| Krukenberg tumor [38][39] |
|
+/– | – | +/–
Based on underlying malignancy |
– | – |
|
|
|
| |||
| Tubal | tubo-ovarian abscess [40][41][42][43] |
|
+ | + | – | + | + |
|
|
|
| ||
| Ectopic pregnancy [44] |
|
+ | + | +/– | – | + |
|
|
|
|
| ||
| Hydrosalpinx [45][46][47] |
|
+ | – | – | – | +/– | – |
|
|
| |||
| Salpingitis [48] |
|
+ | + | – | + | + |
|
|
| ||||
| Fallopian tube carcinoma [49] |
|
+ | + | + | – | +/– |
|
|
|
| |||
| Uterine | Leiomyoma [50][51] |
|
+ | + | – | – | +/– |
|
| ||||
| Choriocarcinoma [52][53][54][55] |
|
+ | + | +/– | – | + |
|
|
|
| |||
| Leiomyosarcoma [56][57][58][59][60] |
|
+ | + | – | – | +/– |
|
|
|
| |||
| Pregnancy [61] |
|
+/− | +/− | +/− | – | – |
|
|
|
||||
| Non-gynecologic | |||||||||||||
| GIT | Appendiceal abscess [62] |
|
+ | – | + | +/– | + |
|
|
|
| ||
| Appendiceal neoplasm [63][64][65][66][67] |
|
+ | – | + | – | +/– |
|
|
|
|
| ||
| Diverticular abscess [72] |
|
+ | – | + | +/– | + |
|
|
|
| |||
| Colorectal cancer [68][69][70][71] |
|
+ | – | + | – | +/– |
|
|
|
|
| ||
| Renal | Pelvic kidney [73][74] |
|
−/+
In case of sever hydronephrosis or renal stone we may have pelvic pain |
– | − | − | − | − |
|
|
|
| |
| Bladder cancer [75][76][77] |
|
+ | – | – | – | – |
|
|
|
|
| ||
| Others | Retroperitoneal sarcoma [78][79][80][81] |
|
+ | – | + | − | − |
|
|
|
|
| |
ABBREVIATIONS
BTA=Bladder tumor associated antigen, NMP= Nuclear matrix proteins, CEA= Carcinoembryonic antigen, US= Ultrasound, HCG= Human chorionic gonadotropin, LDH= Lactate dehydrogenase, AFP= Alpha fitoprotein, CA125= Cancer antigen 125, H&E= Hematoxylin and eosin, MRI= Magnetic resonance imaging, GI= Gastrointestinal tract, PID= Pelvic inflammatory disease, CA19-9= Carbohydrate antigen 19-9, 5HIAA= 5-hydroxyindoleacetic acid, MEN syndrome= Multiple endocrine neoplasia syndrome, HNPCC= Hereditary nonpolyposis colorectal cancer, UTI= Urinary tract infection, RCC= Renal cell carcinoma
References
- ↑ 1.0 1.1 Levine D, Brown DL, Andreotti RF, Benacerraf B, Benson CB, Brewster WR, Coleman B, Depriest P, Doubilet PM, Goldstein SR, Hamper UM, Hecht JL, Horrow M, Hur HC, Marnach M, Patel MD, Platt LD, Puscheck E, Smith-Bindman R (September 2010). “Management of asymptomatic ovarian and other adnexal cysts imaged at US: Society of Radiologists in Ultrasound Consensus Conference Statement”. Radiology. 256 (3): 943–54. doi:10.1148/radiol.10100213. PMID 20505067.
- ↑ 2.0 2.1 Montz FJ, Schlaerth JB, Morrow CP (August 1988). “The natural history of theca lutein cysts”. Obstet Gynecol. 72 (2): 247–51. PMID 2455880.
- ↑ 3.0 3.1 Southam, Anna L. (1962). “Massive Ovarian Hyperstimulation with Clomiphene Citrate”. JAMA: The Journal of the American Medical Association. 181 (5): 443. doi:10.1001/jama.1962.03050310083018b. ISSN 0098-7484.
- ↑ 4.0 4.1 Nguyen, K T; Reid, R L; Sauerbrei, E (1986). “Antenatal sonographic detection of a fetal theca lutein cyst: a clue to maternal diabetes mellitus”. Journal of Ultrasound in Medicine. 5 (11): 665–667. doi:10.7863/jum.1986.5.11.665. ISSN 0278-4297.
- ↑ 5.0 5.1 Jung, Seung Eun; Lee, Jae Mun; Rha, Sung Eun; Byun, Jae Young; Jung, Jung Im; Hahn, Seong Tai (2002). “CT and MR Imaging of Ovarian Tumors with Emphasis on Differential Diagnosis”. RadioGraphics. 22 (6): 1305–1325. doi:10.1148/rg.226025033. ISSN 0271-5333.
- ↑ 6.0 6.1 Imai, Shunsuke; Kiyozuka, Yasuhiko; Maeda, Hiroko; Noda, Tuneo; Hosick, Howard L. (1990). “Establishment and Characterization of a Human Ovarian Serous Cystadenocarcinoma Cell Line That Produces the Tumor Markers CA-125 and Tissue Polypeptide Antigen”. Oncology. 47 (2): 177–184. doi:10.1159/000226813. ISSN 0030-2414.
- ↑ 7.0 7.1 Malpica A, Deavers MT, Lu K, Bodurka DC, Atkinson EN, Gershenson DM, Silva EG (April 2004). “Grading ovarian serous carcinoma using a two-tier system”. Am. J. Surg. Pathol. 28 (4): 496–504. PMID 15087669.
- ↑ 8.0 8.1 Li J, Fadare O, Xiang L, Kong B, Zheng W (March 2012). “Ovarian serous carcinoma: recent concepts on its origin and carcinogenesis”. J Hematol Oncol. 5: 8. doi:10.1186/1756-8722-5-8. PMID 22405464.
- ↑ 9.0 9.1 Hoerl HD, Hart WR (December 1998). “Primary ovarian mucinous cystadenocarcinomas: a clinicopathologic study of 49 cases with long-term follow-up”. Am. J. Surg. Pathol. 22 (12): 1449–62. PMID 9850171.
- ↑ 10.0 10.1 Lee KR, Scully RE (November 2000). “Mucinous tumors of the ovary: a clinicopathologic study of 196 borderline tumors (of intestinal type) and carcinomas, including an evaluation of 11 cases with ‘pseudomyxoma peritonei‘“. Am. J. Surg. Pathol. 24 (11): 1447–64. PMID 11075847.
- ↑ 11.0 11.1 Jung, Seung Eun; Lee, Jae Mun; Rha, Sung Eun; Byun, Jae Young; Jung, Jung Im; Hahn, Seong Tai (2002). “CT and MR Imaging of Ovarian Tumors with Emphasis on Differential Diagnosis”. RadioGraphics. 22 (6): 1305–1325. doi:10.1148/rg.226025033. ISSN 0271-5333.
- ↑ 12.0 12.1 Mol BW, Bayram N, Lijmer JG, Wiegerinck MA, Bongers MY, van der Veen F, Bossuyt PM (December 1998). “The performance of CA-125 measurement in the detection of endometriosis: a meta-analysis”. Fertil. Steril. 70 (6): 1101–8. PMID 9848302.
- ↑ 13.0 13.1 Kinkel, Karen; Frei, Kathrin A.; Balleyguier, Corinne; Chapron, Charles (2005). “Diagnosis of endometriosis with imaging: a review”. European Radiology. 16 (2): 285–298. doi:10.1007/s00330-005-2882-y. ISSN 0938-7994.
- ↑ 14.0 14.1 de Ziegler, Dominique; Borghese, Bruno; Chapron, Charles (2010). “Endometriosis and infertility: pathophysiology and management”. The Lancet. 376 (9742): 730–738. doi:10.1016/S0140-6736(10)60490-4. ISSN 0140-6736.
- ↑ 15.0 15.1 Kawai, Michiyasu; Kano, Takeo; Kikkawa, Fumitaka; Morikawa, Yoshimitsu; Oguchi, Hidenori; Nakashima, Nobuo; Ishizuka, Takao; Kuzuya, Kazuo; Ohta, Masahiro; Arii, Yoshitaro; Tomoda, Yutaka (1992). “Seven tumor markers in benign and malignant germ cell tumors of the ovary”. Gynecologic Oncology. 45 (3): 248–253. doi:10.1016/0090-8258(92)90299-X. ISSN 0090-8258.
- ↑ 16.0 16.1 Dunzendorfer, Thomas; deLAS MORENAS, ANTONIO; Kalir, Tamara; Levin, Robert M. (1999). “Struma Ovarii and Hyperthyroidism”. Thyroid. 9 (5): 499–502. doi:10.1089/thy.1999.9.499. ISSN 1050-7256.
- ↑ 17.0 17.1 Outwater, Eric K.; Siegelman, Evan S.; Hunt, Jennifer L. (2001). “Ovarian Teratomas: Tumor Types and Imaging Characteristics”. RadioGraphics. 21 (2): 475–490. doi:10.1148/radiographics.21.2.g01mr09475. ISSN 0271-5333.
- ↑ 18.0 18.1 Saba, Luca; Guerriero, Stefano; Sulcis, Rosa; Virgilio, Bruna; Melis, GianBenedetto; Mallarini, Giorgio (2009). “Mature and immature ovarian teratomas: CT, US and MR imaging characteristics”. European Journal of Radiology. 72 (3): 454–463. doi:10.1016/j.ejrad.2008.07.044. ISSN 0720-048X.
- ↑ 19.0 19.1 Dgani, R.; Shoham(Schwartz), Z.; Czernobilsky, B.; Kaftori, A.; Borenstein, R.; Lancet, M. (1988). “Lactic dehydrogenase, alkaline phosphatase and human chorionic gonadotropin in a pure ovarian dysgerminoma”. Gynecologic Oncology. 30 (1): 44–50. doi:10.1016/0090-8258(88)90044-3. ISSN 0090-8258.
- ↑ 20.0 20.1 Tanaka YO, Kurosaki Y, Nishida M, Michishita N, Kuramoto K, Itai Y, Kubo T (1994). “Ovarian dysgerminoma: MR and CT appearance”. J Comput Assist Tomogr. 18 (3): 443–8. PMID 8188914.
- ↑ 21.0 21.1 Yang, Grace C.H. (2000). “Fine-needle aspiration cytology of Schiller-Duval bodies of yolk-sac tumor”. Diagnostic Cytopathology. 23 (4): 228–232. doi:10.1002/1097-0339(200010)23:4<228::AID-DC2>3.0.CO;2-M. ISSN 8755-1039.
- ↑ 22.0 22.1 Levitin, A; Haller, K D; Cohen, H L; Zinn, D L; O’Connor, M T (1996). “Endodermal sinus tumor of the ovary: imaging evaluation”. American Journal of Roentgenology. 167 (3): 791–793. doi:10.2214/ajr.167.3.8751702. ISSN 0361-803X.
- ↑ 23.0 23.1 Talerman, A.; Haije, W. G. (1974). “Alpha-fetoprotein and germ cell tumors: A possible role of yolk sac tumor in production of alpha-fetoprotein”. Cancer. 34 (5): 1722–1726. doi:10.1002/1097-0142(197411)34:5<1722::AID-CNCR2820340521>3.0.CO;2-F. ISSN 0008-543X.
- ↑ 24.0 24.1 MEIGS JV (May 1954). “Fibroma of the ovary with ascites and hydrothorax; Meigs’ syndrome”. Am. J. Obstet. Gynecol. 67 (5): 962–85. PMID 13148256.
- ↑ 25.0 25.1 Sivanesaratnam, V.; Dutta, R.; Jayalakshmi, P. (1990). “Ovarian fibroma – clinical and histopathological characteristics”. International Journal of Gynecology & Obstetrics. 33 (3): 243–247. doi:10.1016/0020-7292(90)90009-A. ISSN 0020-7292.
- ↑ 26.0 26.1 Abad, Antonio; Cazorla, Eduardo; Ruiz, Fernando; Aznar, Ismael; Asins, Enrique; Llixiona, Joaquin (1999). “Meigs’ syndrome with elevated CA125: case report and review of the literature”. European Journal of Obstetrics & Gynecology and Reproductive Biology. 82 (1): 97–99. doi:10.1016/S0301-2115(98)00174-2. ISSN 0301-2115.
- ↑ 27.0 27.1 Yaghoobian, Jahanguir; Pinck, Robert L. (1983). “Ultrasound findings in thecoma of the ovary”. Journal of Clinical Ultrasound. 11 (2): 91–93. doi:10.1002/jcu.1870110207. ISSN 0091-2751.
- ↑ 28.0 28.1 Li, Xinchun; Zhang, Weidong; Zhu, Guangbin; Sun, Congpeng; Liu, Qingyu; Shen, Yuechun (2012). “Imaging Features and Pathologic Characteristics of Ovarian Thecoma”. Journal of Computer Assisted Tomography. 36 (1): 46–53. doi:10.1097/RCT.0b013e31823f6186. ISSN 0363-8715.
- ↑ 29.0 29.1 Proctor, Francis E.; Greeley, Joseph P.; Rathmell, Thomas K. (1951). “Malignant thecoma of the ovary”. American Journal of Obstetrics and Gynecology. 62 (1): 185–192. doi:10.1016/0002-9378(51)91109-X. ISSN 0002-9378.
- ↑ 30.0 30.1 Pectasides D, Pectasides E, Psyrri A (February 2008). “Granulosa cell tumor of the ovary”. Cancer Treat. Rev. 34 (1): 1–12. doi:10.1016/j.ctrv.2007.08.007. PMID 17945423.
- ↑ 31.0 31.1 Stenwig, Jan Trygve; Hazekamp, Johan The.; Beecham, Jackson B. (1979). “Granulosa cell tumors of the ovary. A clinicopathological study of 118 cases with long-term follow-up”. Gynecologic Oncology. 7 (2): 136–152. doi:10.1016/0090-8258(79)90090-8. ISSN 0090-8258.
- ↑ 32.0 32.1 Morikawa K, Hatabu H, Togashi K, Kataoka ML, Mori T, Konishi J (1997). “Granulosa cell tumor of the ovary: MR findings”. J Comput Assist Tomogr. 21 (6): 1001–4. PMID 9386298.
- ↑ 33.0 33.1 Ko SF, Wan YL, Ng SH, Lee TY, Lin JW, Chen WJ, Kung FT, Tsai CC (May 1999). “Adult ovarian granulosa cell tumors: spectrum of sonographic and CT findings with pathologic correlation”. AJR Am J Roentgenol. 172 (5): 1227–33. doi:10.2214/ajr.172.5.10227493. PMID 10227493.
- ↑ 34.0 34.1 Lantzsch, T.; Stoerer, S.; Lawrenz, K.; Buchmann, J.; Strauss, H.-G.; Koelbl, H. (2001). “Sertoli-Leydig cell tumor”. Archives of Gynecology and Obstetrics. 264 (4): 206–208. doi:10.1007/s004040000114. ISSN 0932-0067.
- ↑ 35.0 35.1 Jung, Seung Eun; Rha, Sung Eun; Lee, Jae Mun; Park, Soo Youn; Oh, Soon Nam; Cho, Kyoung Sik; Lee, Eun Ju; Byun, Jae Young; Hahn, Seong Tai (2005). “CT and MRI Findings of Sex Cord–Stromal Tumor of the Ovary”. American Journal of Roentgenology. 185 (1): 207–215. doi:10.2214/ajr.185.1.01850207. ISSN 0361-803X.
- ↑ 36.0 36.1 Shevchuk, Maria M.; Fenoglio, Cecilia M.; Richart, Ralph M. (1980). “Histogenesis of brenner tumors, I: Histology and ultrastructure”. Cancer. 46 (12): 2607–2616. doi:10.1002/1097-0142(19801215)46:12<2607::AID-CNCR2820461213>3.0.CO;2-Q. ISSN 0008-543X.
- ↑ 37.0 37.1 Outwater, Eric K; Siegelman, Evan S; Kim, Bohyun; Chiowanich, Peerapod; Blasbalg, Roberto; Kilger, Alex (1998). “Ovarian Brenner tumors: MR imaging characteristics”. Magnetic Resonance Imaging. 16 (10): 1147–1153. doi:10.1016/S0730-725X(98)00136-2. ISSN 0730-725X.
- ↑ 38.0 38.1 Kim SH, Kim WH, Park KJ, Lee JK, Kim JS (1996). “CT and MR findings of Krukenberg tumors: comparison with primary ovarian tumors”. J Comput Assist Tomogr. 20 (3): 393–8. PMID 8626898.
- ↑ 39.0 39.1 Al-Agha OM, Nicastri AD (November 2006). “An in-depth look at Krukenberg tumor: an overview”. Arch. Pathol. Lab. Med. 130 (11): 1725–30. doi:10.1043/1543-2165(2006)130[1725:AILAKT]2.0.CO;2. PMID 17076540.
- ↑ 40.0 40.1 Landers, D. V.; Sweet, R. L. (1983). “Tubo-ovarian Abscess: Contemporary Approach to Management”. Clinical Infectious Diseases. 5 (5): 876–884. doi:10.1093/clinids/5.5.876. ISSN 1058-4838.
- ↑ 41.0 41.1 Stewart Taylor, E.; McMillan, James H.; Greer, Benjamin E.; Droegemueller, William; Thompson, Horace E. (1975). “The intrauterine device and tubo-ovarian abscess”. American Journal of Obstetrics and Gynecology. 123 (4): 338–348. doi:10.1016/S0002-9378(16)33434-2. ISSN 0002-9378.
- ↑ 42.0 42.1 Ha, H. K.; Lim, G. Y.; Cha, E. S.; Lee, H. G.; Ro, H. J.; Kim, H. S.; Kim, H. H.; Joo, S. W.; Jee, M. K. (1995). “MR Imaging of Tubo-Ovarian Abscess”. Acta Radiologica. 36 (5): 510–514. doi:10.1080/02841859509173418. ISSN 0284-1851.
- ↑ 43.0 43.1 Varras M, Polyzos D, Perouli E, Noti P, Pantazis I, Akrivis C (2003). “Tubo-ovarian abscesses: spectrum of sonographic findings with surgical and pathological correlations”. Clin Exp Obstet Gynecol. 30 (2–3): 117–21. PMID 12854857. Vancouver style error: initials (help)
- ↑ 44.0 44.1 Barnhart, Kurt T. (2009). “Ectopic Pregnancy”. New England Journal of Medicine. 361 (4): 379–387. doi:10.1056/NEJMcp0810384. ISSN 0028-4793.
- ↑ 45.0 45.1 Kim, Mi Young; Rha, Sung Eun; Oh, Soon Nam; Jung, Seung Eun; Lee, Young Joon; Kim, You Sung; Byun, Jae Young; Lee, Ahwon; Kim, Mee-Ran (2009). “MR Imaging Findings of Hydrosalpinx: A Comprehensive Review”. RadioGraphics. 29 (2): 495–507. doi:10.1148/rg.292085070. ISSN 0271-5333.
- ↑ 46.0 46.1 Atri M, Nazarnia S, Bret PM, Aldis AE, Kintzen G, Reinhold C (July 1994). “Endovaginal sonographic appearance of benign ovarian masses”. Radiographics. 14 (4): 747–60, discussion 761–2. doi:10.1148/radiographics.14.4.7938766. PMID 7938766.
- ↑ 47.0 47.1 Chanelles, Olivier; Ducarme, Guillaume; Sifer, Christophe; Hugues, Jean-Noel; Touboul, Cyril; Poncelet, Christophe (2011). “Hydrosalpinx and infertility: what about conservative surgical management?”. European Journal of Obstetrics & Gynecology and Reproductive Biology. 159 (1): 122–126. doi:10.1016/j.ejogrb.2011.07.004. ISSN 0301-2115.
- ↑ 48.0 48.1 Czerwenka K, Heuss F, Hosmann J, Manavi M, Jelincic D, Kubista E (October 1994). “Salpingitis caused by Chlamydia trachomatis and its significance for infertility”. Acta Obstet Gynecol Scand. 73 (9): 711–5. PMID 7976247.
- ↑ 49.0 49.1 Niloff, Jonathan M.; Klug, Thomas L.; Schaetzl, Elena; Zurawski, Vincent R.; Knapp, Robert C.; Bast, Robert C. (1984). “Elevation of serum CA125 in carcinomas of the fallopian tube, endometrium, and endocervix”. American Journal of Obstetrics and Gynecology. 148 (8): 1057–1058. doi:10.1016/S0002-9378(84)90444-7. ISSN 0002-9378.
- ↑ 50.0 50.1 Bulletti, Carlo; De Ziegler, Dominique; Polli, Valeria; Flamigni, Carlo (1999). “The role of leiomyomas in infertility”. The Journal of the American Association of Gynecologic Laparoscopists. 6 (4): 441–445. doi:10.1016/S1074-3804(99)80008-5. ISSN 1074-3804.
- ↑ 51.0 51.1 Murase, Eiko; Siegelman, Evan S.; Outwater, Eric K.; Perez-Jaffe, Liza A.; Tureck, Richard W. (1999). “Uterine Leiomyomas: Histopathologic Features, MR Imaging Findings, Differential Diagnosis, and Treatment”. RadioGraphics. 19 (5): 1179–1197. doi:10.1148/radiographics.19.5.g99se131179. ISSN 0271-5333.
- ↑ 52.0 52.1 Seckl, Michael J; Fisher, Rosemary A; Salerno, Giovanni; Rees, Helene; Paradinas, Fernando J; Foskett, Marianne; Newlands, Edward S (2000). “Choriocarcinoma and partial hydatidiform moles”. The Lancet. 356 (9223): 36–39. doi:10.1016/S0140-6736(00)02432-6. ISSN 0140-6736.
- ↑ 53.0 53.1 Nishikawa, Yoshiki; Kaseki, Shigeaki; Tomoda, Yutaka; Ishizuka, Takao; Asai, Yasumasa; Suzuki, Toshio; Ushijima, Hiroshi (1985). “Histopathologic classification of uterine choriocarcinoma”. Cancer. 55 (5): 1044–1051. doi:10.1002/1097-0142(19850301)55:5<1044::AID-CNCR2820550520>3.0.CO;2-7. ISSN 0008-543X.
- ↑ 54.0 54.1 Libshitz HI, Baber CE, Hammond CB (April 1977). “The pulmonary metastases of choriocarcinoma”. Obstet Gynecol. 49 (4): 412–6. PMID 558566.
- ↑ 55.0 55.1 Diouf A, Cissé ML, Laïco A, Ndiaye D, Moreau JC, Diadhiou F (May 2005). “[Sonographic features of gestational choriocarcinoma]”. J Radiol (in French). 86 (5 Pt 1): 469–73. PMID 16114202.
- ↑ 56.0 56.1 Seki, K.; Hoshihara, T.; Nagata, I. (1992). “Leiomyosarcoma of the Uterus: Ultrasonography and Serum Lactate Dehydrogenase Level”. Gynecologic and Obstetric Investigation. 33 (2): 114–118. doi:10.1159/000294861. ISSN 1423-002X.
- ↑ 57.0 57.1 Juang CM, Yen MS, Horng HC, Twu NF, Yu HC, Hsu WL (2006). “Potential role of preoperative serum CA125 for the differential diagnosis between uterine leiomyoma and uterine leiomyosarcoma”. Eur. J. Gynaecol. Oncol. 27 (4): 370–4. PMID 17009628.
- ↑ 58.0 58.1 Pattani, Sita J.; Kier, Ruben; Deal, Robert; Luchansky, Edward (1995). “MRI of uterine leiomyosarcoma”. Magnetic Resonance Imaging. 13 (2): 331–333. doi:10.1016/0730-725X(95)93813-5. ISSN 0730-725X.
- ↑ 59.0 59.1 McLeod, A J; Zornoza, J; Shirkhoda, A (1984). “Leiomyosarcoma: computed tomographic findings”. Radiology. 152 (1): 133–136. doi:10.1148/radiology.152.1.6729102. ISSN 0033-8419.
- ↑ 60.0 60.1 Robboy, Stanley J.; Bentley, Rex C.; Butnor, Kelly; Anderson, Malcolm C. (2000). “Pathology and Pathophysiology of Uterine Smooth-Muscle Tumors”. Environmental Health Perspectives. 108: 779. doi:10.2307/3454306. ISSN 0091-6765.
- ↑ 61.0 61.1 Cacctatore, Bruno; Tttttnen, Atla; Stenman, Ulf-Hakan; Ylostalo, Pekka (1990). “Normal early pregnancy: serum hCG levels and vaginal ultrasonography findings”. BJOG: An International Journal of Obstetrics and Gynaecology. 97 (10): 899–903. doi:10.1111/j.1471-0528.1990.tb02444.x. ISSN 1470-0328.
- ↑ 62.0 62.1 Pinto Leite N, Pereira JM, Cunha R, Pinto P, Sirlin C (August 2005). “CT evaluation of appendicitis and its complications: imaging techniques and key diagnostic findings”. AJR Am J Roentgenol. 185 (2): 406–17. doi:10.2214/ajr.185.2.01850406. PMID 16037513.
- ↑ 63.0 63.1 Chapter 5: Tumours of the Appendix – IARC. https://www.iarc.fr/en/publications/pdfs-online/pat-gen/bb2/bb2-chap5.pdf Accessed on January 15, 2019
- ↑ 64.0 64.1 Goede, A. C.; Caplin, M. E.; Winslet, M. C. (2003). “Carcinoid tumour of the appendix”. British Journal of Surgery. 90 (11): 1317–1322. doi:10.1002/bjs.4375. ISSN 0007-1323.
- ↑ 65.0 65.1 Pablo Carmignani, C.; Hampton, Regina; E. Sugarbaker, Christina; Chang, David; H. Sugarbaker, Paul (2004). “Utility of CEA and CA 19-9 tumor markers in diagnosis and prognostic assessment of mucinous epithelial cancers of the appendix”. Journal of Surgical Oncology. 87 (4): 162–166. doi:10.1002/jso.20107. ISSN 0022-4790.
- ↑ 66.0 66.1 Limsui D, Vierkant RA, Tillmans LS, Wang AH, Weisenberger DJ, Laird PW, Lynch CF, Anderson KE, French AJ, Haile RW, Harnack LJ, Potter JD, Slager SL, Smyrk TC, Thibodeau SN, Cerhan JR, Limburg PJ (July 2010). “Cigarette smoking and colorectal cancer risk by molecularly defined subtypes”. J. Natl. Cancer Inst. 102 (14): 1012–22. doi:10.1093/jnci/djq201. PMC 2915616. PMID 20587792.
- ↑ 67.0 67.1 Duh QY, Hybarger CP, Geist R, Gamsu G, Goodman PC, Gooding GA, Clark OH (July 1987). “Carcinoids associated with multiple endocrine neoplasia syndromes”. Am. J. Surg. 154 (1): 142–8. PMID 2886072.
- ↑ 68.0 68.1 Zhu, Amy; Kaneshiro, Marc; Kaunitz, Jonathan D. (2010). “Evaluation and Treatment of Iron Deficiency Anemia: A Gastroenterological Perspective”. Digestive Diseases and Sciences. 55 (3): 548–559. doi:10.1007/s10620-009-1108-6. ISSN 0163-2116.
- ↑ 69.0 69.1 Macdonald JS (1999). “Carcinoembryonic antigen screening: pros and cons”. Semin Oncol. 26 (5): 556–60. PMID 10528904.
- ↑ 70.0 70.1 Haggar FA, Boushey RP (November 2009). “Colorectal cancer epidemiology: incidence, mortality, survival, and risk factors”. Clin Colon Rectal Surg. 22 (4): 191–7. doi:10.1055/s-0029-1242458. PMC 2796096. PMID 21037809.
- ↑ 71.0 71.1 Taylor AJ, Youker JE (1991). “Imaging in colorectal carcinoma”. Semin Oncol. 18 (2): 99–110. PMID 2014406.
- ↑ 72.0 72.1 Hulnick, D H; Megibow, A J; Balthazar, E J; Naidich, D P; Bosniak, M A (1984). “Computed tomography in the evaluation of diverticulitis”. Radiology. 152 (2): 491–495. doi:10.1148/radiology.152.2.6739821. ISSN 0033-8419.
- ↑ 73.0 73.1 Weizer, Alon Z.; Springhart, W. Patrick; Ekeruo, Wesley O.; Matlaga, Brian R.; Tan, Yeh H.; Assimos, Dean G.; Preminger, Glenn M. (2005). “Ureteroscopic management of renal calculi in anomalous kidneys”. Urology. 65 (2): 265–269. doi:10.1016/j.urology.2004.09.055. ISSN 0090-4295.
- ↑ 74.0 74.1 Ross, Jonathan H.; Kay, Robert (1998). “URETEROPELVIC JUNCTION OBSTRUCTION IN ANOMALOUS KIDNEYS”. Urologic Clinics of North America. 25 (2): 219–225. doi:10.1016/S0094-0143(05)70010-0. ISSN 0094-0143.
- ↑ 75.0 75.1 Barentsz JO, Jager GJ, Witjes JA, Ruijs JH (1996). “Primary staging of urinary bladder carcinoma: the role of MRI and a comparison with CT”. Eur Radiol. 6 (2): 129–33. PMID 8797968.
- ↑ 76.0 76.1 Shariat SF, Karam JA, Lotan Y, Karakiewizc PI (2008). “Critical evaluation of urinary markers for bladder cancer detection and monitoring”. Rev Urol. 10 (2): 120–35. PMC 2483317. PMID 18660854.
- ↑ 77.0 77.1 Metts MC, Metts JC, Milito SJ, Thomas CR (June 2000). “Bladder cancer: a review of diagnosis and management”. J Natl Med Assoc. 92 (6): 285–94. PMC 2640522. PMID 10918764.
- ↑ 78.0 78.1 Storm FK, Mahvi DM (July 1991). “Diagnosis and management of retroperitoneal soft-tissue sarcoma”. Ann. Surg. 214 (1): 2–10. PMC 1358407. PMID 2064467.
- ↑ 79.0 79.1 Francis IR, Cohan RH, Varma DG, Sondak VK (August 2005). “Retroperitoneal sarcomas”. Cancer Imaging. 5: 89–94. doi:10.1102/1470-7330.2005.0019. PMID 16154826.
- ↑ 80.0 80.1 Silverstein, Murray N.; Wakim, Khalil G.; Bahn, Robert C. (1964). “Hypoglycemia associated with neoplasia”. The American Journal of Medicine. 36 (3): 415–423. doi:10.1016/0002-9343(64)90168-8. ISSN 0002-9343.
- ↑ 81.0 81.1 Storm FK, Mahvi DM (July 1991). “Diagnosis and management of retroperitoneal soft-tissue sarcoma”. Ann. Surg. 214 (1): 2–10. PMC 1358407. PMID 2064467.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Rim Halaby, M.D. [2] Huda A. Karman, M.D.
Overview
Ovarian cancer is the 7th most common type of cancer in women worldwide and the 8th most common type of cancer in the United States. Ovarian cancer is the second most common gynecologic malignancy and the most common cause of gynecologic cancer death in the United States. Ovarian cancer is the second most common gynecologic malignancy in developed countries, with an incidence of 9.4 per 100,000 women and a mortality rate of 5.1 per 100,000. In developing countries, it is the third most common gynecologic malignancy (cervical cancer is the most common), with an incidence of 5.0 per 100,000 and a mortality rate of 3.1 per 100,000. The age-adjusted prevalence of ovarian cancer in the United States is 71.3 per 100,000 in 2011. The estimated number of new cases of ovarian cancer is approximately 22,000.
Epidemiology and Demographics
Prevalence
- Ovarian cancer is more common in industrialized nations, with the exception of Japan. In the United States, females have a 1.4% to 2.5% (1 out of 40-60 women) lifetime chance of developing ovarian cancer.[1][2]
- In the United States, the age-adjusted prevalence of ovarian cancer is 71.3 per 100,000 in 2011.[3]
Incidence
- The delay-adjusted incidence of ovarian cancer in 2011 was estimated to be 12.46 per 100,000 persons in the United States.[3][4]
- In 2011, the age-adjusted incidence of ovarian cancer was 12.09 per 100,000 persons in the United States.[3]
Age
- Older women are at highest risk. More than half of the deaths from ovarian cancer occur in women between 55 and 74 years of age.
- While the overall age-adjusted incidence of ovarian cancer in the United States between 2007 and 2011 is 12.3 per 100,000, the age-adjusted incidence of ovarian cancer by age category is:[3]
- Under 65 years: 7.5 per 100,000
- 65 and over: 45.2 per 100,000
- Shown below is an image depicting the delay-adjusted incidence and observed incidence of ovarian cancer by age and race in the United States between 1975 and 2011. These graphs are adapted from SEER: The Surveillance, Epidemiology, and End Results Program of the National Cancer Institute.[3]

Race
- Shown below is a table depicting the age-adjusted prevalence of ovarian cancer by race in 2011 in the United States.[3]
| All Races | White | Black | Asian/Pacific Islander | Hispanic | |
| Age-adjusted prevalence | 71.3 per 100,000 | 76.2 per 100,000 | 44.2 per 100,000 | 63.2 per 100,000 | 59.1 per 100,000 |
- Shown below is an image depicting the incidence of ovarian cancer by race in the United States between 1975 and 2011.[3]

API: Asian/Pacific Islander; AI/AN: American Indian/ Alaska Native
Percent Distribution of Ovarian Cancer by Histology
Among patients with histologically confirmed cases of ovarian cancer, the percent distribution of the types of the disease between 2007 and 2011 in the United States are:[3]
- Carcinoma: 91.7%
- Epidermoid carcinoma: 0.7%
- Adenocarcinoma: 84%
- Adenocarcinoma, not otherwise specified: 12.3%
- Papillary adenocarcinoma: 1,5%
- Clear cell adenocarcinoma: 5.2%
- Endometrioid carcinoma: 9.7%
- Cystadenocarcinoma, not otherwise specified: 0.4%
- Serous cystadenocarcinoma: 20.9%
- Papillary serous cystadenocarcinoma: 23.5%
- Mucinous cystadenocarcinoma: 1.5%
- Mucinous adenocarcinoma: 3.5%
- Mucin-producing adenocarcinoma: 0.2%
- Other adenocarcinoma: 5.3%
- Other specific carcinoma: 2.3%
- Stromal cell tumor: 1.6%
- Other: 0.7%
- Unspecified carcinoma, not otherwise specified: 4.6%
- Sarcoma and other soft tissues: 0.4%
- Other specific types: 6.9%
- Mullerian mixed tumor: 3%
- Malignant teratoma: 1.5%
- Other: 2.4%
- Unspecified: 1.1%
References
- ↑ Ovarian cancer incidence statistics. Cancer research UK
- ↑ Brett M., Reid; Brett M., Reid; Jennifer B., Permuth; Thomas A., Sellers; Jennifer B., Permuth; Thomas A., Sellers (2017). “Epidemiology of ovarian cancer: a review”. Cancer Biology & Medicine. 14 (1): 9–32. doi:10.20892/j.issn.2095-3941.2016.0084. ISSN 2095-3941.
- ↑ 3.0 3.1 3.2 3.3 3.4 3.5 3.6 3.7 Howlader N, Noone AM, Krapcho M, Garshell J, Miller D, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z,Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA (eds). SEER Cancer Statistics Review, 1975-2011, National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2011/, based on November 2013 SEER data submission, posted to the SEER web site, April 2014.
- ↑ Siegel R, Ma J, Zou Z, Jemal A (2014). “Cancer statistics, 2014”. CA Cancer J Clin. 64 (1): 9–29. doi:10.3322/caac.21208. PMID 24399786.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Huda A. Karman, M.D.
Overview
The risk of developing ovarian cancer appears to be affected by several factors; in fact, early age at first pregnancy, older ages of final pregnancy, and the use of low dose hormonal contraception have been associated with a lower incidence of ovarian cancer. There is good evidence that in some women genetic factors are important.
Risk Factors
Common risk factors in the development of ovarian cancer include:[1]
| Ovarian cancer risk factors | Characterestics | description |
|---|---|---|
| Known risk factors [2][3][4][5][6][7][8][9][10][11][12] | Age | As age increases, ovarian cancer incidence increases. |
| Hormonal and reproductive factors | Early menarche and late menopause, Nulliparity, Infertility | |
| Early menarche and late menopause | Both increase the frequency of the ovulation and the ovarian epithelium exposure to persistent injury | |
| Nulliparity | Studies have shown that multiparity and full-term pregnancies decrease the risk of ovarian cancer and fallopian tubal carcinoma | |
| Infertility | Infertility is an independent risk factor of ovarian cancer | |
| Endometriosis | Ovarian cancers that arise from endometriotic tissue usually affect young women and have better prognosis and survival rates | |
| Polycystic ovarian syndrome | The association is controversial and complex | |
| Postmenopausal hormone therapy | Estrogen therapy alone has more association with ovarian cancer than combined estrogen–progesteron therapy | |
| Intrauterine device | Regardless of the type of the IUD, studies have shown an increased risk of ovarian cancer with IUD use | |
| Genetic factors | ||
| BRCA gene mutations | The risk is more with BRCA1 carriers than BRCA2 carriers. Ovarian cancer develops at an earlier age in BRCA1-carrier women compared to BRCA2-carrier women. Serous adenocarcinoma is the most common type.General women and women with BRCA mutations usually present with stage III or IV | |
| Lynch syndrome | Hereditary nonpolyposis colorectal cancer (HNPCC) : 1 percent of cases with ovarian cancer have Lynch syndrome. | |
| Other genetic factors | The genes in the Fanconi anemias pathway can undergo different mutations and lead to the development of ovarian and/or breast cancer. The genes that are associated with ovarian cancer are: BRCA1, BRCA2, BRIP1, RAD51C, RAD51D, PALB2, and BARD1 | |
| Family history of certain cancers | BRCA mutation carriers with personal or family history of breast cancer have higher risk of developing ovarian cancer that those without BRCA mutation | |
| Personal history of breast cancer | Increases the risk of breast-ovarian syndrome | |
| Environmental factors | Cigarette smoking associated with mucinous ovarian cancer, asbestos,Talc (Its association is controversial). | |
| Other factors | Diet: dairy food with high animal fat intake is claimed to be associated with ovarian cancer but data are not sufficient to confirm this association, exercise: No clear evidence about the association between physical activity and breast cancer, and obesity: can increases the risk of ovarian cancer and the risk of its mortality, Pelvic inflammatory disease can increase the risk of and might be used as tumor marker for ovarian tumor. | |
| Possible risk factors[12][9] | Obesity | Can increases the risk of ovarian cancer and the risk of its mortality. |
| Talc use on genetals | Its association is controversial). | |
| Unknown risk factors[10][13] | Food types and amount | Dairy food with high animal fat intake is claimed to be associated with ovarian cancer but data are not sufficient to confirm this association |
| Fertility drugs | The role of medications used for ovulation induction in increasing the risks of ovarian cancer is controversial. The association between the fertility drugs and ovarian cancer could be due to the stimulating effect of these drug, however this association is not a causal relation | |
| Sedentary life | Its association is unknown |
- Common risk factors in the development of ovarian cancer include:
- Age:
- There is a proportional association between age and ovarian cancer, as age increases, ovarian cancer incidence increases.[14]
- Hormonal and reproductive factors:
- Early menarche and late menopause:
- Both increase the frequency of the ovulation and the ovarian epithelium exposure to persistent injury.[14][15]
- Nulliparity
- Studies have shown that multiparity and full term pregnancies decrease the risk of ovarian cancer and fallopian tubal carcinoma.[16][17]
- Infertility:
- Type of infertility and its causes should be taken in consideration as different causes can increase the risk of ovarian cancer such as:[18]
- Primary infertility
- Secondary infertility as endometriosis
- The role of medications used for ovulation induction in increasing the risks of ovarian cancer is controversial. The association between the fertility drugs and ovarian cancer could be due to the stimulating effect of these drug, however this association is not a causal relation.[13]
- Regardless to the fertility medications use, infertility is an independent risk factor of ovarian cancer.[13]
- Endometriosis
- Ovarian cancers that arise from endometriotic tissue usually affect young women and have better prognosis and survival rates.[19]
- Polycystic ovarian syndrome:
- The association is controversial and complex. Meta-analysis found an association between PCOS and endometrial cancer in general but not with ovarian cancer specifically.[20]
- Postmenopausal hormone therapy:
- A non statistical significant association found between combined estrogen–progesteron therapy and ovarian carcinoma.[21]
- Meta-analysis found small significant association between ovarian cancer and estrogen therapy alone.[22]
- Intrauterine device:
- Regardless of the type of the IUD, studies have shown an increased risk of ovarian cancer with IUD use.[23]
- Early menarche and late menopause:
- Genetic factors
- BRCA gene mutations: the risk of both ovarian and breast cancers increases in women with BRCA mutations.
- The risk is more with BRCA1 carriers than BRCA2 carriers.[3]
- Ovarian cancer develops at an earlier age in BRCA1-carrier women compared to BRCA2-carrier women. Serous adenocarcinoma is the most common type.[4]
- General women and women with BRCA mutations usually present with stage III or IV.[24]
- However, the grade is higher in women who are BRCA mutations‘ carries.[25]
- The short-term survival rate of ovarian cancer in women with BRCA mutations is higher than non-carriers.[26]
- Prophylactic bilateral salpingo-oophorectomy can be done in BRCA mutation carries who are at higher risk of developing fallopian tube cancer and primary peritoneal carcinoma.[27]
- Lynch syndrome or hereditary nonpolyposis colorectal cancer (HNPCC) :
- 1 percent of cases with ovarian cancer have Lynch syndrome.[5]
- Family history of breast cancer:
- It is not clear whether the family’s pattern of cancer is due to chance, shared lifestyle factors, a genetic risk passed from parents to children or a combination of these factors.
- By American cancer society, about 5 to 10% of ovarian cancers are a part of family cancer syndromes resulting from inherited changes (mutations) in certain genes.
- BRCA mutation carriers with personal or family history of breast cancer have higher risk of developing ovarian cancer that those without BRCA mutation[28]
- Other genetic factors:
- The genes in the Fanconi anemias pathway can undergo different mutations and lead to the development of ovarian and/or breast cancer[6]. The genes that are associated with ovarian cancer are: BRCA1, BRCA2, BRIP1, RAD51C, RAD51D, PALB2, and BARD1[7]
- Environmental factors such as:
- Cigarette smoking associated with mucinous ovarian cancer[8]
- Asbestos,Talc (Its association is controversial)[9]
- Other factors such as:
- Diet:
- Ddairy food with high animal fat intake is claimed to be associated with ovarian cancer but data are not sufficient to confirm this association.[10]
- Exercise:
- No clear evidence about the association between physical activity and breast cancer.[11]
- Obesity:
- Can increases the risk of ovarian cancer and the risk of its mortality.[12]
- Diet:
- Pelvic inflammatory disease can increase the risk of and might be used as tumor marker for ovarian tumor[29]
- Age:
References
- ↑ A. Daniilidis & V. Karagiannis (2007). “Epithelial ovarian cancer. Risk factors, screening and the role of prophylactic oophorectomy”. Hippokratia. 11 (2): 63–66. PMID 19582179. Unknown parameter
|month=ignored (help) - ↑ . doi:10.22034/APJCP.2017.18.1.11. Missing or empty
|title=(help) - ↑ 3.0 3.1 Chen S, Parmigiani G (2007). “Meta-analysis of BRCA1 and BRCA2 penetrance”. J Clin Oncol. 25 (11): 1329–33. doi:10.1200/JCO.2006.09.1066. PMC 2267287. PMID 17416853.
- ↑ 4.0 4.1 Pal T, Permuth-Wey J, Betts JA, Krischer JP, Fiorica J, Arango H; et al. (2005). “BRCA1 and BRCA2 mutations account for a large proportion of ovarian carcinoma cases”. Cancer. 104 (12): 2807–16. doi:10.1002/cncr.21536. PMID 16284991.
- ↑ 5.0 5.1 Rubin SC, Blackwood MA, Bandera C, Behbakht K, Benjamin I, Rebbeck TR; et al. (1998). “BRCA1, BRCA2, and hereditary nonpolyposis colorectal cancer gene mutations in an unselected ovarian cancer population: relationship to family history and implications for genetic testing”. Am J Obstet Gynecol. 178 (4): 670–7. doi:10.1016/s0002-9378(98)70476-4. PMID 9579428.
- ↑ 6.0 6.1 Zhang S, Royer R, Li S, McLaughlin JR, Rosen B, Risch HA; et al. (2011). “Frequencies of BRCA1 and BRCA2 mutations among 1,342 unselected patients with invasive ovarian cancer”. Gynecol Oncol. 121 (2): 353–7. doi:10.1016/j.ygyno.2011.01.020. PMID 21324516.
- ↑ 7.0 7.1 Norquist BM, Harrell MI, Brady MF, Walsh T, Lee MK, Gulsuner S; et al. (2016). “Inherited Mutations in Women With Ovarian Carcinoma”. JAMA Oncol. 2 (4): 482–90. doi:10.1001/jamaoncol.2015.5495. PMC 4845939. PMID 26720728.
- ↑ 8.0 8.1 Jordan SJ, Whiteman DC, Purdie DM, Green AC, Webb PM (2006). “Does smoking increase risk of ovarian cancer? A systematic review”. Gynecol Oncol. 103 (3): 1122–9. doi:10.1016/j.ygyno.2006.08.012. PMID 17005245.
- ↑ 9.0 9.1 9.2 Huncharek M, Geschwind JF, Kupelnick B (2003). “Perineal application of cosmetic talc and risk of invasive epithelial ovarian cancer: a meta-analysis of 11,933 subjects from sixteen observational studies”. Anticancer Res. 23 (2C): 1955–60. PMID 12820486.
- ↑ 10.0 10.1 10.2 Blank MM, Wentzensen N, Murphy MA, Hollenbeck A, Park Y (2012). “Dietary fat intake and risk of ovarian cancer in the NIH-AARP Diet and Health Study”. Br J Cancer. 106 (3): 596–602. doi:10.1038/bjc.2011.572. PMC 3273348. PMID 22223086.
- ↑ 11.0 11.1 Carnide N, Kreiger N, Cotterchio M (2009). “Association between frequency and intensity of recreational physical activity and epithelial ovarian cancer risk by age period”. Eur J Cancer Prev. 18 (4): 322–30. doi:10.1097/CEJ.0b013e32832bf3fa. PMID 19390450.
- ↑ 12.0 12.1 12.2 Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ (2003). “Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults”. N Engl J Med. 348 (17): 1625–38. doi:10.1056/NEJMoa021423. PMID 12711737.
- ↑ 13.0 13.1 13.2 Bristow RE, Karlan BY (1996). “Ovulation induction, infertility, and ovarian cancer risk”. Fertil Steril. 66 (4): 499–507. PMID 8816606.
- ↑ 14.0 14.1 Gates MA, Rosner BA, Hecht JL, Tworoger SS (2010). “Risk factors for epithelial ovarian cancer by histologic subtype”. Am J Epidemiol. 171 (1): 45–53. doi:10.1093/aje/kwp314. PMC 2796984. PMID 19910378.
- ↑ Tsilidis KK, Allen NE, Key TJ, Dossus L, Lukanova A, Bakken K; et al. (2011). “Oral contraceptive use and reproductive factors and risk of ovarian cancer in the European Prospective Investigation into Cancer and Nutrition”. Br J Cancer. 105 (9): 1436–42. doi:10.1038/bjc.2011.371. PMC 3241548. PMID 21915124.
- ↑ Stewart LM, Holman CD, Aboagye-Sarfo P, Finn JC, Preen DB, Hart R (2013). “In vitro fertilization, endometriosis, nulliparity and ovarian cancer risk”. Gynecol Oncol. 128 (2): 260–4. doi:10.1016/j.ygyno.2012.10.023. PMID 23116937.
- ↑ Titus-Ernstoff L, Perez K, Cramer DW, Harlow BL, Baron JA, Greenberg ER (2001). “Menstrual and reproductive factors in relation to ovarian cancer risk”. Br J Cancer. 84 (5): 714–21. doi:10.1054/bjoc.2000.1596. PMC 2363792. PMID 11237375.
- ↑ Brinton LA, Lamb EJ, Moghissi KS, Scoccia B, Althuis MD, Mabie JE; et al. (2004). “Ovarian cancer risk associated with varying causes of infertility”. Fertil Steril. 82 (2): 405–14. doi:10.1016/j.fertnstert.2004.02.109. PMID 15302291.
- ↑ Erzen M, Rakar S, Klancnik B, Syrjänen K, Klancar B (2001). “Endometriosis-associated ovarian carcinoma (EAOC): an entity distinct from other ovarian carcinomas as suggested by a nested case-control study”. Gynecol Oncol. 83 (1): 100–8. doi:10.1006/gyno.2001.6382. PMID 11585420.
- ↑ Barry JA, Azizia MM, Hardiman PJ (2014). “Risk of endometrial, ovarian and breast cancer in women with polycystic ovary syndrome: a systematic review and meta-analysis”. Hum Reprod Update. 20 (5): 748–58. doi:10.1093/humupd/dmu012. PMC 4326303. PMID 24688118.
- ↑ Anderson GL, Judd HL, Kaunitz AM, Barad DH, Beresford SA, Pettinger M; et al. (2003). “Effects of estrogen plus progestin on gynecologic cancers and associated diagnostic procedures: the Women’s Health Initiative randomized trial”. JAMA. 290 (13): 1739–48. doi:10.1001/jama.290.13.1739. PMID 14519708.
- ↑ Zhou B, Sun Q, Cong R, Gu H, Tang N, Yang L; et al. (2008). “Hormone replacement therapy and ovarian cancer risk: a meta-analysis”. Gynecol Oncol. 108 (3): 641–51. doi:10.1016/j.ygyno.2007.12.003. PMID 18221779.
- ↑ Tworoger SS, Fairfield KM, Colditz GA, Rosner BA, Hankinson SE (2007). “Association of oral contraceptive use, other contraceptive methods, and infertility with ovarian cancer risk”. Am J Epidemiol. 166 (8): 894–901. doi:10.1093/aje/kwm157. PMID 17656616.
- ↑ Pal T, Permuth-Wey J, Betts JA, Krischer JP, Fiorica J, Arango H; et al. (2005). “BRCA1 and BRCA2 mutations account for a large proportion of ovarian carcinoma cases”. Cancer. 104 (12): 2807–16. doi:10.1002/cncr.21536. PMID 16284991.
- ↑ Lakhani SR, Manek S, Penault-Llorca F, Flanagan A, Arnout L, Merrett S; et al. (2004). “Pathology of ovarian cancers in BRCA1 and BRCA2 carriers”. Clin Cancer Res. 10 (7): 2473–81. PMID 15073127.
- ↑ Bolton KL, Chenevix-Trench G, Goh C, Sadetzki S, Ramus SJ, Karlan BY; et al. (2012). “Association between BRCA1 and BRCA2 mutations and survival in women with invasive epithelial ovarian cancer”. JAMA. 307 (4): 382–90. doi:10.1001/jama.2012.20. PMC 3727895. PMID 22274685.
- ↑ Levine DA, Argenta PA, Yee CJ, Marshall DS, Olvera N, Bogomolniy F; et al. (2003). “Fallopian tube and primary peritoneal carcinomas associated with BRCA mutations”. J Clin Oncol. 21 (22): 4222–7. doi:10.1200/JCO.2003.04.131. PMID 14615451.
- ↑ Kauff ND, Mitra N, Robson ME, Hurley KE, Chuai S, Goldfrank D; et al. (2005). “Risk of ovarian cancer in BRCA1 and BRCA2 mutation-negative hereditary breast cancer families”. J Natl Cancer Inst. 97 (18): 1382–4. doi:10.1093/jnci/dji281. PMID 16174860.
- ↑ Lin HW, Tu YY, Lin SY, Su WJ, Lin WL, Lin WZ; et al. (2011). “Risk of ovarian cancer in women with pelvic inflammatory disease: a population-based study”. Lancet Oncol. 12 (9): 900–4. doi:10.1016/S1470-2045(11)70165-6. PMID 21835693.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Huda A. Karman, M.D.
Overview
There are no recommendations for screening ovarian cancer in asymptomatic women although better outcome is associated with early diagnosis. Biomarkers from peritoneal fluid can be used as a mean of early detection of ovarian cancer but this is still an emerging proof. Examples of screening and diagnostic methods for ovarian cancer include pelvic examination, cancer antigen 125 (CA125) tumor marker, transvaginal ultrasound (TVU), multimarker panels, and bioinformatic analysis of proteomic patterns.
Screening
- There are no recommendations for screening ovarian cancer in asymptomatic women although better outcome is associated with early diagnosis.[1][2]
- Ovarian cancer is the fifth most common cause of cancer-related mortality in women
- 75% of women with ovarian cancer are diagnosed in an advanced stage
- Ovarian cancer is the most lethal gynecological cancer
- The reason of increased mortality and late detection of ovarian cancer in its advanced stage is because the screening systems that are being used have poor or limited sensitivity and specificity.
- Biomarkers from peritoneal fluid can be used as a mean of ealy detection of ovarian cancer but this is still an emerging proof.
- Examples of screening and diagnostic methods for ovarian cancer include:[3]
- Pelvic examination
- Cancer antigen 125 (CA 125) tumor marker
- Transvaginal ultrasound (TVU)
- Multimarker panels and bioinformatic analysis of proteomic patterns
- The UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS)is evaluating a multimodal screening strategy (MMS) efficacy which consists of:
- Annual CA125 screening, risk of ovarian cancer algorithm (ROCA), TVU
- Patients with family history of ovarian cancer or breast cancer can have ovarian cancer hereditary syndrome as breast-ovarian cancer syndrome which is associated with
- Should undergo the following screening:
- Annual rectovaginal pelvic examinations
- CA125
- TVU until completing childbearing or until age 35 years at least, where at this point prophylactic bilateral oophorectomy is recommended
References
- ↑ Smith RA, Andrews KS, Brooks D, Fedewa SA, Manassaram-Baptiste D, Saslow D; et al. (2017). “Cancer screening in the United States, 2017: A review of current American Cancer Society guidelines and current issues in cancer screening”. CA Cancer J Clin. 67 (2): 100–121. doi:10.3322/caac.21392. PMID 28170086.
- ↑ Galea M, Gauci G, Calleja-Agius J, Schembri-Wismayer P (2017). “Peritoneal biomarkers in the early detection of ovarian cancer”. Minerva Ginecol. 69 (1): 84–99. doi:10.23736/S0026-4784.16.03943-5. PMID 27284942.
- ↑ . doi:10.1158/1940-6207.CAPR-11-0378. Check
|doi=value (help). Missing or empty|title=(help)
Natural History, Complications, and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Huda A. Karman, M.D.
Overview
Ovarian cancer is often diagnosed late resulting in a poor overall outcome for the patient. Ovarian cancer complications can be spread of cancer to other organs, progressive function loss of various organs, ascites (fluid in the abdomen), intestinal obstruction. Ovarian cancer has a poor prognosis. More than 60% of patients presenting with this cancer already have stage III or stage IV cancer, when it has already spread beyond the ovaries.
Natural History, Complications, and Prognosis
Natural History
- Ovarian cancer is often diagnosed late resulting in a poor overall outcome for the patient.
Complications
- Spread of ovarian cancer to other organs
- Progressive function loss of various organs
- Ascites (fluid in the abdomen)
- Intestinal obstruction
Prognosis
- Ovarian cancer has a poor prognosis. It is disproportionately deadly because symptoms are vague and non-specific, hence diagnosis is late. More than 60% of patients presenting with this cancer already have stage III or stage IV cancer, when it has already spread beyond the ovaries.
- Ovarian cancers that are malignant shed cells into the naturally occurring fluid within the abdominal cavity. These cells can implant on other abdominal (peritoneal) structures included the uterus, urinary bladder, bowel, lining of the bowel wall (omentum) and can even spread to the lungs. These cells can begin forming new tumor growths before cancer is even suspected.
- More than 50% of women with ovarian cancer are diagnosed in the advanced stages of the disease because no cost-effective screening test for ovarian cancer exists.
- The five year survival rate for all stages is only 35% to 38%. If, however, diagnosis is made early in the disease, five-year survival rates can reach 90% to 98%.
- Germ cell tumors of the ovary have a much better prognosis than other ovarian cancers, in part because they tend to grow rapidly to a very large size, hence they are detected sooner.
5-Year Survival
- Between 2004 and 2010, the 5-year relative survival of patients with ovarian cancer was 44.6%.[1]
- When stratified by age, the 5-year relative survival of patients with ovarian cancer was 57.5% and 27.3% for patients <65 and ≥ 65 years of age respectively.[1]
- The survival of patients with ovarian cancer varies with the stage of the disease. Shown below is a table depicting the 5-year relative survival by the stage of ovarian cancer:[1]
| Stage | 5-year relative survival (%), (2004-2010) |
| All stages | 44.5% |
|---|---|
| Localized | 92.3% |
| Regional | 71.7% |
| Distant | 27.4% |
| Unstaged | 21.7% |
- Shown below is an image depicting the 5-year conditional relative survival (probability of surviving in the next 5-years given the cohort has already survived 0, 1, 3 years) between 1998 and 2010 of ovarian cancer by stage at diagnosis according to SEER.
- These graphs are adapted from SEER: The Surveillance, Epidemiology, and End Results Program of the National Cancer Institute.[1]

References
- ↑ 1.0 1.1 1.2 1.3 Howlader N, Noone AM, Krapcho M, Garshell J, Miller D, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z,Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA (eds). SEER Cancer Statistics Review, 1975-2011, National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2011/, based on November 2013 SEER data submission, posted to the SEER web site, April 2014.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Staging | Laboratory Findings | X Rays | CT | MRI | Echocardiography or Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgical | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Related Chapters
Related Chapters
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH