
Enterobiasis
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Synonyms and keywords: Pinworm infection; oxyuriasis; threadworm infection ; enterobius vermicularis infection; oxyuris vermicularis infection ; enterobius gregorii infection ; seatworm infection
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
Enterobiasis is an infection commonly caused by Enterobius vermicularis (pinworm). It usually affects children and causes perianal pruritus, restlessness, and irritability. The diagnosis is made by physical examination and repeated scotch-tape tests. This infection is medically treated with two doses of either pyrantel pamoate, albendazole, or mebendazole. The transmission of enterobiasis can be prevented by treating all the household members of the infected person and improving personal and household hygienic conditions (e.g., frequent hand washing, changing clothes, and covering food).
Historical Perspective
Enterobius vermicularis eggs found in western Utah are carbon dated to 7837 BC. In 1983, Jean-Pierre Hugot isolated a new species Enterobius gregorii which is identical to Enterobius vermicularis.
Classification
There is no established classification system for enterobiasis, though it may be classified on the basis of the organisms causing it; Enterobius vermicularis and Enterobius gregorii.
Pathophysiology
Enterobius vermicularis is usually transmitted via the feco-oral route to the human host. It reproduces in the small intestine of humans only. The gravid female worm lays eggs in the perianal area usually at night and causes pruritus. In addition to the fingernail contamination, the infective eggs can be transmitted via the dust and fomites.
Causes
Enterobiasis is caused by pinworm. The pinworm (genus Enterobius), also known as threadworm (in the United Kingdom and Australia) or seatworm, is a parasitic worm. It is a nematode (roundworm) and a common intestinal parasite or helminth, especially in humans.[1] The medical condition associated with pinworm infestation is known as enterobiasis[2] (a type of helminthiasis) or less precisely as oxyuriasis in reference to the family Oxyuridae.[3]
Differentiating (Disease name) from other Conditions
Enterobiasis must be differentiated from other causes of perianal pruritus and the nematode infections.
Epidemiology and Demographics
Enterobiasis is particularly common in children. Annually, around 200 million people are infected worldwide. The pinworm is the most common helminth (i.e., parasitic worm) infection in the United States and Western Europe.
Risk Factors
Common risk factors in the development of enterobiasis are young age, unhygienic practices, and close contact with infected person.
Screening
There is insufficient evidence to recommend routine screening for enterobiasis.
Natural History, Complications and Prognosis
If left untreated, patients with enterobiasis may progress to develop secondary skin infections. Common complications of enterobiasis include bacterial dermatitis, folliculitis, vulvovaginitis, and recurrent cystitis. Prognosis is generally excellent.
Diagnosis
History and Symptoms
The symptoms of enterobiasis may include painful itching around the anus, restless sleep, poor appetite, and failure to gain weight. When the infection is heavy, there can be a secondary bacterial infection due to the irritation and scratching of the anal area.
Physical Examination
Patients with enterobiasis usually appear restless. Physical examination of patients with enterobiasis is remarkable for skin excoriations as a result of scratching (secondary to perianal itch), perianal skin infections, and visualization of adult worms in the perianal area (usually at night).[4][5]
Laboratory Findings
Diagnosis of enterobiasis is often made clinically by observing the female worm(s) in the peri-anal region, but can also be made using the “scotch-tape” test, in which the sticky side of a strip of cellophane tape is pressed against the peri-anal skin, then examined under a microscope for pinworm eggs.
Chest X Ray
There are no X-ray findings associated with enterobiasis.
Echocardiography or Ultrasound
There are no echocardiography or ultrasound findings associated with enterobiasis.
Other Imaging Findings
There are no other imaging findings associated with enterobiasis.
Treatment
Medical Therapy
The treatment of enterobiasis involves the administration of such antiparasitic drugs as either mebendazole (Vermox), albendazole, piperazine (Antepar), or pyrantel pamoate (Combatrin, Povan). A repeat dose is recommended two weeks after the initial treatment. More than one household member is likely to be infected, so the entire household is often treated.
Surgery
Surgical intervention is not recommended for the management of enterobiasis.
Primary Prevention
Effective measures for the primary prevention of enterobiasis include treating family members, frequent handwashing, improving personal and household hygienic condition.
Secondary Prevention
The primary and secondary prevention strategies for enterobiasis are the same.
References
- ↑ Encyclopædia Britannica.
- ↑ Merriam-Webster: Enterobiasis
- ↑ Merriam-Webster: Oxyuriasis
- ↑ Cook GC (1994). “Enterobius vermicularis infection”. Gut. 35 (9): 1159–62. PMC 1375686. PMID 7959218.
- ↑ Caldwell JP (1982). “Pinworms (enterobius vermicularis)”. Can Fam Physician. 28: 306–9. PMC 2306321. PMID 21286054.
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
Enterobius vermicularis eggs found in western Utah are carbon dated to 7837 BC. In 1983, Jean-Pierre Hugot isolated a new species Enterobius gregorii, which is identical to Enterobius vermicularis.
Historical Perspective
Enterobius vermicularis
- The earliest known instance of Enterobius vermicularis is evidenced by pinworm eggs found in coprolite, carbon dated to 7837 BC at western Utah. In 1758, Enterobius vermicularis was first visualized by Linnaeus.[1]
Enterobius gregorii
- In 1983 Jean-Pierre Hugot declared his isolation of a new human parasite.
- While examining oxyuridae of Malagasy Lemurs and in Old World monkeys, he concluded that what had been previously assumed to be a single species of parasite was in fact couples of sister-species.
- Two types of spicules were described, Enterobius vermicularis having the larger spicule (100 to 122 micrometers) and Enterobius gregorii had the shorter spicule (70 to 80 micrometers).[2]
- For all practical purposes, the morphology, life cycle, clinical presentation, and treatment of Enterobius gregorii is identical to Enterobius vermicularis.
References
- ↑ Fry GF, Moore JG (1969). “Enterobius vermicularis: 10,000-year-old human infection”. Science. 166 (3913): 1620. PMID 4900959.
- ↑ Hasegawa H, Takao Y, Nakao M, Fukuma T, Tsuruta O, Ide K (1998). “Is Enterobius gregorii Hugot, 1983 (Nematoda: Oxyuridae) a distinct species?”. J. Parasitol. 84 (1): 131–4. PMID 9488350.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
There is no known classification for enterobiasis but it may be classified on the basis of the organisms causing it; Enterobius vermicularis and Enterobius gregorri.
Classification
Enterobiasis is caused by the two species of Enterobius (pinworm):
E. vermicularis and E. gregorii have a minor difference in the morphology. E. gregorii is the newly discovered species that carries a smaller spicule (sexual organ).The life cycle, clinical presentation, and treatment of E. gregorii is identical to E. vermicularis.[1][2]
References
- ↑ Nakano T, Okamoto M, Ikeda Y, Hasegawa H (2006). “Mitochondrial cytochrome c oxidase subunit 1 gene and nuclear rDNA regions of Enterobius vermicularis parasitic in captive chimpanzees with special reference to its relationship with pinworms in humans”. Parasitol. Res. 100 (1): 51–7. doi:10.1007/s00436-006-0238-4. PMID 16788831.
- ↑ Hasegawa H, Takao Y, Nakao M, Fukuma T, Tsuruta O, Ide K (1998). “Is Enterobius gregorii Hugot, 1983 (Nematoda: Oxyuridae) a distinct species?”. J. Parasitol. 84 (1): 131–4. PMID 9488350.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
Enterobius vermicularis is usually transmitted via the feco-oral route to the human host. It reproduces in the small intestine of humans only. The gravid female worm lays eggs in the perianal area usually at night and causes pruritus. In addition to the fingernail contamination, the infective eggs can be transmitted via the dust and fomites.
Pathophysiology
Pathogenesis
- It is postulated that Enterobius vermicularis triggers an inflammatory response which is associated with the low-grade eosinophilia.
- Allergic response to the worm protein is considered the cause of pruritus; usually pruritus ani (perianal pruritus).[1]
Lifecycle
The lifecycle of Enterobius vermicularis is completed in the human host and comprises of the following stages:[2][3]
- The infective eggs of E. vermicularis are ingested via contaminated hands or fomites (clothing, toys, bed, furniture, animals’ fur etc). The eggs mature into adult Enterobius in 15-40 days.
- Male adult larvae fertilize the female (in lower ileum) and are passed out in stools without producing symptoms. Adult females settle in the lower ileum, caecum, appendix and ascending colon. The gravid worm migrates from the colon to the rectal area. At night eggs laid on the perianal skin by the uterine contraction(s) of the gravid worm.
- At oviposition, the eggs are immature and non-infective. They become infective within 6 hours at body temperature.
- In cool, moist environment with little ventilation eggs remain viable for up to three weeks. However, the infectivity decreases with time. Eggs do not tolerate heat that well which might be the reason that enterobiasis is more common in temperate than tropical climates.
- In rare cases, pinworms are found in the vagina and even more rarely in the uterus, fallopian tubes, liver, and peritoneum, but the worms cannot survive long in these places.
The image shown below depicts the life cycle of the pinworm.[4]

Mode of Transmission
E. Vermicularis is transmitted via these four modes:[2]
- Direct infection from the anal and perianal regions by infected fingernails.
- Exposure to viable eggs on fomites (clothing, toys, bed, furniture, fur of pets etc).
- By dust contaminated with embryonated (infected) eggs.
- Retroinfection; migration of the larvae into sigmoid colon & caecum after hatching on the anal mucosa.
Image
-
![Life cycle of Enterobius vermicularis, otherwise known as the human pinworm. From Public Health Image Library (PHIL). [5]](https://www.wikidoc.org/images/5/53/Pinworm05.jpeg) Life cycle of Enterobius vermicularis, otherwise known as the human pinworm. From Public Health Image Library (PHIL). [5]
Life cycle of Enterobius vermicularis, otherwise known as the human pinworm. From Public Health Image Library (PHIL). [5]
![Life cycle of Enterobius vermicularis, otherwise known as the human pinworm. From Public Health Image Library (PHIL). [5]](https://www.wikidoc.org/index.php/File%3APinworm05.jpeg)
References
- ↑ Katz, Michael (1989). Parasitic Diseases. New York, NY: Springer US. ISBN 978-1-4684-0327-5.
- ↑ 2.0 2.1 Cook GC (1994). “Enterobius vermicularis infection”. Gut. 35 (9): 1159–62. PMC 1375686. PMID 7959218.
- ↑ Caldwell JP (1982). “Pinworms (enterobius vermicularis)”. Can Fam Physician. 28: 306–9. PMC 2306321. PMID 21286054.
- ↑ “CDC – Enterobiasis – Biology”.
- ↑ “Public Health Image Library (PHIL)”.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
The pinworm (genus Enterobius), also known as threadworm (in the United Kingdom and Australia) or seatworm, is a parasitic worm. It is a nematode (roundworm) and a common intestinal parasite or helminth, especially in humans.[5] The medical condition associated with pinworm infestation is known as enterobiasis[6] (a type of helminthiasis) or less precisely as oxyuriasis in reference to the family Oxyuridae.[7]
Throughout this article, the word “pinworm” refers to Enterobius. In British usage, however, pinworm refers to Strongyloides, while Enterobius is called threadworm.[8]
Classification
The pinworm (genus Enterobius) is a type of roundworm (nematode), and three species of pinworm have been identified with certainty.[9] Humans are hosts only to Enterobius vermicularis (formerly Oxyurias vermicularis).[10] Chimpanzees are host to Enterobius anthropopitheci, which is morphologically distinguishable from the human pinworm.[3] Hugot (1983) claims there is another species affecting humans, Enterobius gregorii, which is supposedly a sister species of E. vermicularis, and has a slightly smaller spicule (i.e., sexual organ).[11] Its existence is controversial however; Totkova et al. (2003) consider there to be insufficient evidence,[4] and Hasegawa et al. (2006) contend that E. gregorii is a younger stage of E. vermicularis.[2][3] Regardless of its status as a distinct species, E. gregorii is considered clinically identical to E. vermicularis.[10]
Morphology

The adult female has a sharply pointed posterior end, is 8 to 13 mm long, and 0.5 mm thick.[12] The adult male is considerably smaller, measuring 2 to 5 mm long and 0.2 mm thick, and has a curved posterior end.[12] The eggs are translucent[12] and have a surface that adheres to objects.[13] The eggs measure 50 to 60 μm by 20 to 30 μm, and have a thick shell flattened on one side.[12] The small size and colourlessness of the eggs make them invisible to the naked eye, except in barely visible clumps of thousands of eggs. Eggs may contain a developing embryo or a fully developed pinworm larva.[12] The larvae grow to 140–150 μm in length.[13]
Distribution
The pinworm has a worldwide distribution,[14] and is the most common helminth (i.e., parasitic worm) infection in the United States, western Europe, and Oceania.[15][16] In the United States, a study by the Center of Disease Control reported an overall incidence rate of 11.4% among people of all ages.[16] Pinworms are particularly common in children, with prevalence rates in this age group having been reported as high as 61% in India, 50% in England, 39% in Thailand, 37% in Sweden, and 29% in Denmark.[16] Finger sucking has been shown to increase both incidence and relapse rates,[16] and nail biting has been similarly associated.[17] Because it spreads from host to host through contamination, pinworms are common among people living in close contact, and tends to occur in all people within a household.[14] The prevalence of pinworms is not associated with gender,[14] nor with any particular social class, race, or culture.[16] Pinworms are an exception to the tenet that intestinal parasites are uncommon in affluent communities.[16] The earliest known instance of the pinworms associated with humans is evidenced by pinworm eggs found in coprolite, carbon dated to 7837 BC at western Utah;[13] however 240 million years ago parasitic pinworm nematodes already infested pre-mammalian cynodonts: a fossilized egg was detected in fossil dung.[18]
Lifecycle
The entire lifecycle, from egg to adult, takes place in the human gastrointestinal tract of a single human host,[12][13] from about 2–4 weeks[19] or about 4–8 weeks.[16]
The lifecycle begins with eggs being ingested.[13] The eggs hatch in the duodenum (i.e., first part of the small intestine).[20] The emerging pinworm larvae grow rapidly to a size of 140 to 150 μm,[19] and migrate through the small intestine towards the colon.[13] During this migration, they moult twice and become adults.[13][16] Females survive for 5 to 13 weeks, and males about 7 weeks.[13] The male and female pinworms mate in the ileum (i.e., last part of the small intestine),[13] whereafter the male pinworms usually die,[20] and are passed out with stool.[21] The gravid female pinworms settle in the ileum, caecum (i.e., beginning of the large intestine), appendix and ascending colon,[13] where they attach themselves to the mucosa[16] and ingest colonic contents.[14]
Almost the entire body of a gravid female becomes filled with eggs.[20] The estimations of the number of eggs in a gravid female pinworm range from about 11,000[13] to 16,000.[16] The egg-laying process begins about five weeks after initial ingestion of pinworm eggs by the human host.[13] The gravid female pinworms migrate through the colon towards the rectum at a rate of 12 to 14 cm per hour.[13] They emerge from the anus, and while moving on the skin near the anus, the female pinworms deposit eggs either through (1) contracting and expelling the eggs, (2) dying and then disintegrating, or (3) bodily rupture due to the host scratching the worm.[20] After depositing the eggs, the female becomes opaque and dies.[21] The reason the female emerges from the anus is to obtain the oxygen necessary for the maturation of the eggs.[21]
Infection
E. vermicularis causes the medical condition enterobiasis, whose primary symptom is itching in the anal area.[22] Albendazole or mebendazole is the first-line treatment of pinworm infection. Pyrantel pamoate is alternative.
Transmission
Pinworms spread through human-to-human transmission, by ingesting (i.e., swallowing) infectious pinworm eggs and/or by anal insertion.[16][20] The eggs are hardy and can remain viable (i.e., infectious) in a moist environment up to three weeks.[16][21] They do not tolerate heat well, but can survive in low temperatures: two-thirds of the eggs are still viable after 18 hours at −8 °C (18 °F).[21]
After the eggs have been initially deposited near the anus, they are readily transmitted to other surfaces through contamination.[20] The surface of the eggs is sticky when laid,[13][21] and the eggs are readily transmitted from their initial deposit near the anus to fingernails, hands, night-clothing and bed linen.[19] From here, eggs are further transmitted to food, water, furniture, toys, bathroom fixtures and other objects.[13][16][20] Household pets often carry the eggs in their fur, while not actually being infected.[23] Dust containing eggs can become airborne and widely dispersed when dislodged from surfaces, for instance when shaking out bed clothes and linen.[16][21][23] Consequently, the eggs can enter the mouth and nose through inhalation, and be swallowed later.[16][19][20][21] Although pinworms do not strictly multiply inside the body of their human host,[19] some of the pinworm larvae may hatch on the anal mucosa, and migrate up the bowel and back into the gastrointestinal tract of the original host[16][19] in a process called retroinfection.[16][21] When this retroinfection occurs, it can lead to a heavy parasitic load and ensures the pinworm infestation continues[16] or can be not clinically significant.[21] Despite the limited, 13-week lifespan of individual pinworms,[13] autoinfection (i.e., infection from the original host to itself), either through the anus-to-mouth route or through retroinfection, usually necessitates repeated treatment, at 2-week intervals, in order to remove the infection completely.[24]
Gallery
-
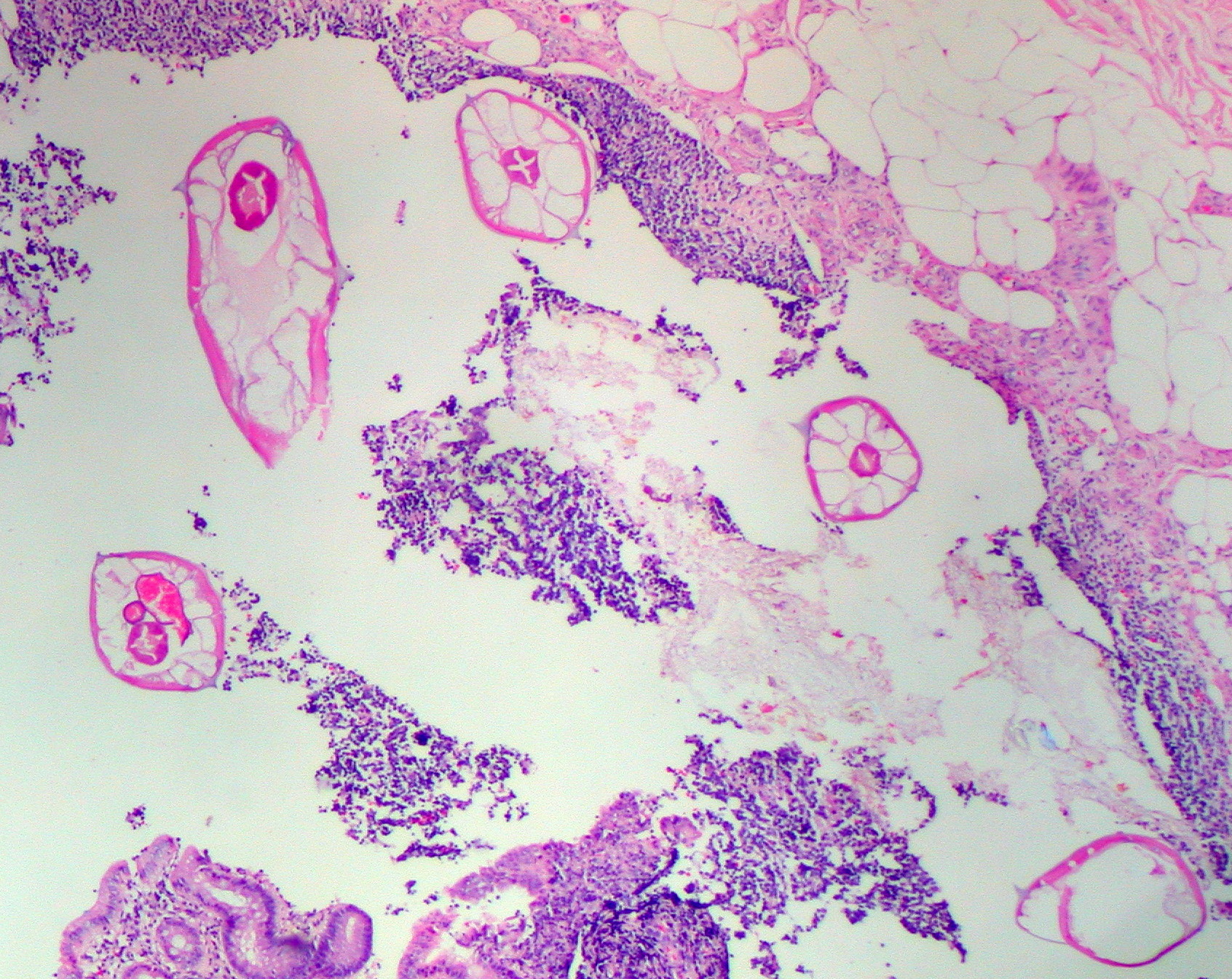 Pinworms are sometimes diagnosed incidentally by pathology. Micrograph of pinworms in the appendix, H&E stain
Pinworms are sometimes diagnosed incidentally by pathology. Micrograph of pinworms in the appendix, H&E stain -

-
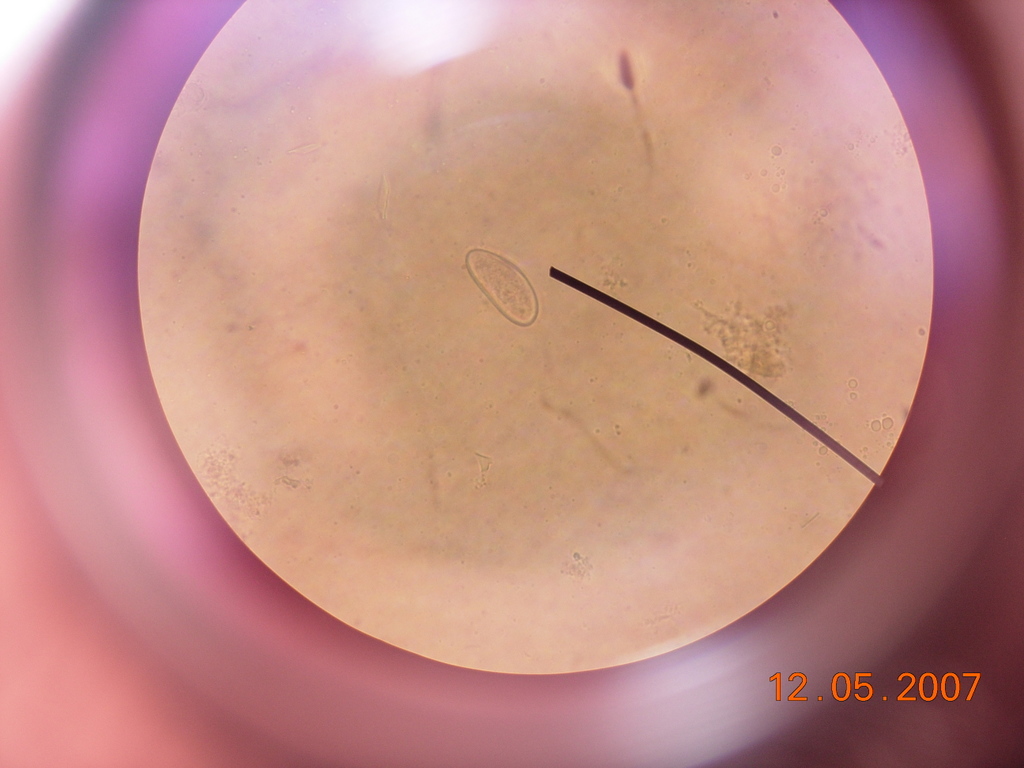 Egg under a light microscope
Egg under a light microscope -
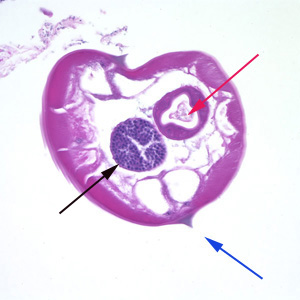 Pinworms are sometimes diagnosed incidentally by pathology: Micrograph of male pinworm in cross section, alae (blue arrow), intestine (red arrow) and testis (black arrow), H&E stain
Pinworms are sometimes diagnosed incidentally by pathology: Micrograph of male pinworm in cross section, alae (blue arrow), intestine (red arrow) and testis (black arrow), H&E stain -
 Pinworm eggs are easily seen under a microscope.
Pinworm eggs are easily seen under a microscope. -
This micrograph reveals the cephalic alae in the head region of E. vermicularis.
-
![This image reveals some of the cytoarchitectural features seen in a lymph node specimen that had been extracted from a patient suspected of a Hantavirus illness. From Public Health Image Library (PHIL). [25]](https://www.wikidoc.org/images/5/59/Pinworm04.jpeg) This image reveals some of the cytoarchitectural features seen in a lymph node specimen that had been extracted from a patient suspected of a Hantavirus illness. From Public Health Image Library (PHIL). [25]
This image reveals some of the cytoarchitectural features seen in a lymph node specimen that had been extracted from a patient suspected of a Hantavirus illness. From Public Health Image Library (PHIL). [25] -
![Photomicrograph reveals some of the ultrastructural details of an Enterobius vermicularis egg, otherwise known as the human pinworm. From Public Health Image Library (PHIL). [25]](https://www.wikidoc.org/images/d/d6/Pinworm03.jpeg) Photomicrograph reveals some of the ultrastructural details of an Enterobius vermicularis egg, otherwise known as the human pinworm. From Public Health Image Library (PHIL). [25]
Photomicrograph reveals some of the ultrastructural details of an Enterobius vermicularis egg, otherwise known as the human pinworm. From Public Health Image Library (PHIL). [25]





![This image reveals some of the cytoarchitectural features seen in a lymph node specimen that had been extracted from a patient suspected of a Hantavirus illness. From Public Health Image Library (PHIL). [25]](https://www.wikidoc.org/index.php/File%3APinworm04.jpeg)
![Photomicrograph reveals some of the ultrastructural details of an Enterobius vermicularis egg, otherwise known as the human pinworm. From Public Health Image Library (PHIL). [25]](https://www.wikidoc.org/index.php/File%3APinworm03.jpeg)
See also
References
- ↑ 1.0 1.1 Hasegawa et al. 2005.
- ↑ 2.0 2.1 Hasegawa et al. 1998
- ↑ 3.0 3.1 3.2 Hasegawa et al. 2006
- ↑ 4.0 4.1 Totkova et al. 2003
- ↑ Encyclopædia Britannica.
- ↑ Merriam-Webster: Enterobiasis
- ↑ Merriam-Webster: Oxyuriasis
- ↑ Vanderkooi 2000, p. B-152 & B-225
- ↑ NCBI taxonomy database 2009
- ↑ 10.0 10.1 dpdx 2009
- ↑ Hugot 1983
- ↑ 12.0 12.1 12.2 12.3 12.4 12.5 Gutiérrez 2005, p. 354.
- ↑ 13.00 13.01 13.02 13.03 13.04 13.05 13.06 13.07 13.08 13.09 13.10 13.11 13.12 13.13 13.14 13.15 Cook 1994, p. 1159
- ↑ 14.0 14.1 14.2 14.3 Gutiérrez 2005, p. 355.
- ↑ http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Worms_pinworms
- ↑ 16.00 16.01 16.02 16.03 16.04 16.05 16.06 16.07 16.08 16.09 16.10 16.11 16.12 16.13 16.14 16.15 16.16 16.17 Burkhart & burkhart 2005, p. 837
- ↑ Cook 1994, p. 1160
- ↑ “Scientists find 240 million-year-old parasite that infected mammals’ ancestor : accessed 8 December 2014.
- ↑ 19.0 19.1 19.2 19.3 19.4 19.5 Cook et al. 2009, p. 1516
- ↑ 20.0 20.1 20.2 20.3 20.4 20.5 20.6 20.7 Garcia 1999, p. 246
- ↑ 21.00 21.01 21.02 21.03 21.04 21.05 21.06 21.07 21.08 21.09 Caldwell 1982, p. 307.
- ↑ “Enterobiasis leads to itching”. Retrieved 20 August 2011.
- ↑ 23.0 23.1 Caldwell 1982, p. 308.
- ↑ http://www.webmd.com/children/tc/pinworms-topic-overview?page=2
- ↑ 25.0 25.1 “Public Health Image Library (PHIL)”.
- Hasegawa H, Ikeda Y, Fujisaki A; et al. (December 2005). “Morphology of chimpanzee pinworms, Enterobius (Enterobius) anthropopitheci (Gedoelst, 1916) (Nematoda: Oxyuridae), collected from chimpanzees, Pan troglodytes, on Rubondo Island, Tanzania”. The Journal of Parasitology. 91 (6): 1314–7. doi:10.1645/GE-569R.1. PMID 16539010.
- “Pinworm”. Encyclopædia Britannica. Retrieved 8 April 2009.
- “Enterobiasis”. Merriam-Webster’s Medical Dictionary. Merriam-Webster. Retrieved 8 April 2009.
- “Oxyuriasis”. Merriam-Webster’s Medical Dictionary. Merriam-Webster. Retrieved 8 April 2009.
- Totkova A, Klobusicky M, Holkova R, Valent M (2003). “Enterobius gregorii—reality or fiction?” (PDF). Bratislavské Lekárske Listy. 104 (3): 130–3. PMID 12940699.
- “Enterobius”. NCBI taxonomy database. National Center for Biotechnology Information, U.S. National Library of Medicine. 2009. Retrieved 8 April 2009.
- “Enterobiasis”. DPDx. Division of Parasitic Diseases, Centers for Disease Control and Prevention. Retrieved 8 April 2009.
- Nakano T, Okamoto M, Ikeda Y, Hasegawa H (December 2006). “Mitochondrial cytochrome c oxidase subunit 1 gene and nuclear rDNA regions of Enterobius vermicularis parasitic in captive chimpanzees with special reference to its relationship with pinworms in humans”. Parasitology Research. 100 (1): 51–7. doi:10.1007/s00436-006-0238-4. PMID 16788831.
- Hugot JP (1983). “[Enterobius gregorii (Oxyuridae, Nematoda), a new human parasite]”. Annales de Parasitologie Humaine et Comparée (in French). 58 (4): 403–4. PMID 6416131.
- Hasegawa H, Takao Y, Nakao M, Fukuma T, Tsuruta O, Ide K (February 1998). “Is Enterobius gregorii Hugot, 1983 (Nematoda: Oxyuridae) a distinct species?”. The Journal of Parasitology. 84 (1): 131–4. doi:10.2307/3284542. PMID 9488350.
- Gutiérrez, Yezid (2000). Diagnostic pathology of parasitic infections with clinical correlations (PDF) (Second ed.). Oxford University Press. pp. 354–366. ISBN 0-19-512143-0. Retrieved 21 August 2009.
- Cook, Gordon C; Zumla, Alimuddin I (2009). Manson’s tropical diseases (22nd ed.). Saunders Elsevier. pp. 1515–1519. ISBN 978-1-4160-4470-3. Retrieved 18 November 2009.
- “B80: Enterobiasis”. International Statistical Classification of Diseases and Related Health Problems (ICD) 10th Revision. World Health Organization. 2007. Retrieved 5 December 2009.
- Cook GC (September 1994). “Enterobius vermicularis infection”. Gut. 35 (9): 1159–62. doi:10.1136/gut.35.9.1159. PMC 1375686. PMID 7959218.
- Garcia, Lynne Shore (2009). Practical guide to diagnostic parasitology. American Society for Microbiology. pp. 246–247. ISBN 1-55581-154-X. Retrieved 5 December 2009.
- Burkhart CN, Burkhart CG (October 2005). “Assessment of frequency, transmission, and genitourinary complications of enterobiasis (pinworms)”. International Journal of Dermatology. 44 (10): 837–40. doi:10.1111/j.1365-4632.2004.02332.x. PMID 16207185.
- Caldwell JP (February 1982). “Pinworms (Enterobius Vermicularis)”. Canadian Family Physician. 28: 306–9. PMC 2306321. PMID 21286054.
- Vanderkooi M (2000). Village Medical Manual (5th ed.).
External links
Differentiating Enterobiasis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
Enterobiasis must be differentiated from other diseases causing pruritis ani such as seborrheic dermatitis, atopic dermatitis, contact dermatitis, skin infections, anal fissure and the nematode infections like ascariasis, ancylostomiasis, and strongyloidiasis.
Differentiating Enterobiasis from other diseases
Enterobiasis should be differentiated from various other causes of anal pruritus and from other nematode infections.
Differentiating Enterobiasis from other causes of Anal Pruritis
The table below summarizes other major causes of pruritus ani (anal pruritus).[1][2][3]
Differentiating Enterobiasis from other nematode infectionsThe table below summarizes the findings that differentiate enterobiasis from other nematode infections.
References
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
Enterobiasis is particularly common in children. Annually, around 200 million people are infected worldwide. The pinworm is the most common helminth (i.e., parasitic worm) infection in the United States and Western Europe.
Epidemiology and Demographics
Enterobiasis is more common in families with school-aged children, in primary caregivers of infected children, and in institutionalized children.
Prevalance
The people most likely to be infected with pinworm are children under 18. In these groups, the prevalence can reach 50%. The prevalence in this age group has been reported to be as high as 61,000 in India, 50,000 in England, 39,000 in Thailand, 37,000 in Sweden, and 29,000 in Denmark per 100,000 population. [1]
Incidence
It is estimated that over 200 million people around the globe and 20 million in USA are infected with pinworm anually. It is more common in the temperate regions and relatively rare in the tropics.[2][3]
Age
School-age children are most commonly infected with Enterobiasis.[4]
Gender
There is no gender predilection for enterobiasis.
Race
There is no racial predilection for enterobiasis.
Developed Countries
It is the most common helminth (i.e., parasitic worm) infection in the United States and Western Europe.
Developing Countries
Enterobiasis has a worldwide distribution.
References
- ↑ Rudolph’s Pediatrics – 21st Ed. 2003; Current Medical Diagnosis & Treatment – 45th Ed. 2006
- ↑ Rudolph’s Pediatrics – 21st Ed. 2003; Current Medical Diagnosis & Treatment – 45th Ed. 2006
- ↑ “CDC – DPDx – Enterobiasis”.
- ↑ Caldwell JP (1982). “Pinworms (enterobius vermicularis)”. Can Fam Physician. 28: 306–9. PMC 2306321. PMID 21286054.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
Common risk factors in the development of enterobiasis include young age, unhygienic practices, and close contact with an infected person.
Risk Factors
Common risk factors associated with enterobiasis include:[1][2]
- Unhygienic practices (e.g., not washing hands, biting nails/pencils)
- Young age
- Close contact with an infected person
- Living in crowded places
References
- ↑ Li HM, Zhou CH, Li ZS, Deng ZH, Ruan CW, Zhang QM, Zhu TJ, Xu LQ, Chen YD (2015). “Risk factors for Enterobius vermicularis infection in children in Gaozhou, Guangdong, China”. Infect Dis Poverty. 4: 28. doi:10.1186/s40249-015-0058-9. PMC 4451960. PMID 26038691.
- ↑ Caldwell JP (1982). “Pinworms (enterobius vermicularis)”. Can Fam Physician. 28: 306–9. PMC 2306321. PMID 21286054.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
If left untreated, patients with enterobiasis may progress to develop secondary skin infections. Common complications of enterobiasis include bacterial dermatitis, folliculitis, vulvovaginitis, and recurrent cystitis. Prognosis is generally excellent.
Natural History
The symptoms of enterobiasis usually develop in the early childhood and start with symptoms such as perianal pruritus, insomnia, restlessness, and tiredness. The symptoms of enterobiasis typically develop five weeks after exposure to infected eggs. Without treatment, the patient will develop symptoms of perianal itching, which may eventually lead to secondary skin infections.
Complications
Complications that can develop as a result of enterobiasis are:[1][2]
- Localized:
- Systemic:
- Vulvovaginitis
- Recurrent cystitis
- Chronic pelvic inflammatory disease
- Repeated infection with the parasite (re-infestation)
- Liver granuloma
Prognosis
Enterobiasis generally has a very good prognosis.
References
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH