
Coronary artery bypass surgery
For the WikiPatient page for this topic, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-In-Chief: Mohammed A. Sbeih, M.D. [2]; Anahita Deylamsalehi, M.D.[3]; Cafer Zorkun, M.D., Ph.D. [4]; Varun Kumar, M.B.B.S. [5] Prince Tano Djan, BSc, MBChB [6]
Synonyms and keywords: Coronary artery bypass grafting, and colloquially heart bypass, bypass, bypass surgery, open heart surgery, or CABG (pronounced like cabbage), aortocoronary bypass (ACB). The term Coronary Artery Graft Surgery (CAGS) is often used outside the United States and should not be confused with Coronary Angiography (CAG). OPCAB refers to Off-pump coronary artery bypass, a procedure during which the patient is not placed on extracorporeal circulation (“the pump”).
Overview
Coronary artery bypass surgery (CABG) is a surgical revascularization procedure that is used to circumvent or bypass blockages in the epicardial coronary arteries associated with acute coronary syndromes (including ST elevation MI, non ST elevation MI, unstable angina) and stable angina. The technique was pioneered by Argentine cardiac surgeon René Favaloro at the Cleveland Clinic in the late 1960s. As part of the procedure, arteries or veins from elsewhere in the patient‘s body are grafted from the aorta to the coronary arteries to bypass atherosclerotic narrowings and improve the blood supply to the coronary circulation supplying the myocardium (heart muscle). This surgery is usually performed with the heart stopped, necessitating the usage of cardiopulmonary bypass. However, recent advances allow the procedure to be performed with the heart beating and through smaller incisions. Currently, about 500,000 Coronary artery bypass surgery (CABG) are performed in the United States each year.
Pathophysiology
Pathophysiology
Saphenous Vein Graft Disease | Other Non-Atherosclerotic Saphenous Vein Graft Diseases
Indications for CABG
CABG in Patients with Acute MI | CABG in Patients with Ventricular Arrhythmias | Emergency CABG after Failed PCI | CABG in Association with Other Cardiac Procedures | Heart Team Approach to Revascularization Decisions | Revascularization of Left Main CAD to Improve Survival | Revascularization of Non-Left Main CAD to Improve Survival | Revascularization to Improve Symptoms | CABG in Left Ventricular Dysfunction
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-in-Chief: Cafer Zorkun, M.D., Ph.D. [2], Mohammed A. Sbeih, M.D. [3] Anahita Deylamsalehi, M.D.[4]
Overview
- Coronary artery bypass surgery (CABG) is the preferred treatment with:
- Disease of the left main coronary artery (LMCA). LMCA disease is associated with sudden death; therefore, lesions of the LMCA are sometimes referred to as widow makers.
- Disease of all three coronary vessels (LAD, LCX and RCA).
- Diffuse disease not amenable to treatment with PCI.
- Coronary artery bypass surgery (CABG) is likely the preferred treatment with other high-risk patients such as those with severe ventricular dysfunction (i.e. low ejection fraction), or diabetes mellitus patients, particularly those with disease involving the left anterior descending artery.
- Alternative treatments for coronary artery disease include:
- Medical management (statins, antihypertensives, smoking cessation, and tight blood sugar control in diabetics).
- Both Percutaneous coronary intervention (PCI) and Coronary artery bypass surgery (CABG) are more effective than medical management at relieving symptoms, (e.g. angina, dyspnea, fatigue), but repeated procedures are required more frequently after PCI.
- When optimal treatment strategy is unclear for a patient, it is recommended to have a multidisciplinary Heart Team approach.[1]
- Decision regarding the treatment should be patient centered.[1]
Surgery Indications
- You can read in greater detail about each of the indications for CABG below in greater detail by clicking on the link.
CABG in Patients with Acute MI | CABG in Patients with Ventricular Arrhythmias | Emergency CABG after Failed PCI | CABG in Association with Other Cardiac Procedures | Heart Team Approach to Revascularization Decisions | Revascularization of Left Main CAD to Improve Survival | Revascularization of Non-Left Main CAD to Improve Survival | Revascularization to Improve Symptoms | CABG in Left Ventricular Dysfunction
- ↑ 1.0 1.1 Writing Committee Members. Lawton JS, Tamis-Holland JE, Bangalore S, Bates ER, Beckie TM; et al. (2022). “2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines”. J Am Coll Cardiol. 79 (2): e21–e129. doi:10.1016/j.jacc.2021.09.006. PMID 34895950 Check
|pmid=value (help).
Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-in-Chief: Cafer Zorkun, M.D., Ph.D. [2], Mohammed A. Sbeih, M.D. [3] Anahita Deylamsalehi, M.D.[4]
Overview
Prognosis following Coronary artery bypass surgery (CABG) depends on a variety of factors. In general, CABG improves the chances of survival of patients who are at high risks, such as those patients with the left main disease. After approximately 5 years the difference in survival rate between those who have had surgery and those treated by medication therapy diminishes. Age at the time of CABG is critical to the prognosis, therefore younger patients with no complicating diseases have a high probability of greater longevity. Recommended by ACC 2021 guideline, STS score system can be used to predict adverse outcomes of CABG such as death, renal failure, prolonged hospital stay, and mediastinitis.
Prognosis
Age
- Age at the time of CABG is critical factor to determine the prognosis. Younger patients with no complicating diseases have a high probability of greater longevity.
- In a cohort study of 1,388 patients who were 48.9 years in average at the time of their first surgery survival rate were as follows:
- 5 years: 93.6%
- 10 years: 81.1%
- 15 years: 62.1%
- 20 years: 46.7%
- 23 years: 38.4%
Society of Thoracic Surgery (STS) Risk Score
- Based on ACC 2021 revascularization guideline, STS risk score is recommended to predict the prognosis of CABG.[1]
- This score system can predict the adverse outcomes of CABG such as death, permanent stroke, renal failure, repeated surgery, deep sternal wound infection, prolonged mechanical ventilation, and hospitalization.[1]
- Compared to EuroSCORE II (the European System for Cardiac Operative Risk Evaluation), STS risk score is more accurate in predicting CABG outcomes, especially at mortality rates higher than 5%.[1]
- STS risk score is limited in evaluating the effect of conditions such as cirrhosis, malnutrition, and frailty on CABG‘s outcome. Therefore, for patients who are candidates for CABG and have those conditions other tools should be used.
- STS risk score is derived from the United States’ data on patients who had CABG.[1] The following table shows last updated STS risk score (2018) for patients who had only CABG or CABG with a heart value surgery.[2]
| Adverse Outcomes | CABG | CABG and heart value surgery |
|---|---|---|
| Mortality rate | 0.804 | 0.761 |
| Permanent stroke | 0.697 | 0.632 |
| Renal failure | 0.826 | 0.759 |
| Prolonged mechanical ventilation | 0.772 | 0.744 |
| Repeated surgery | 0.621 | 0.588 |
| Composite morbidity and mortality | 0.738 | 0.712 |
| Prolonged post operation hospitalization | 0.777 | 0.739 |
| Deep sternal wound infection/Mediastinitis | 0.681 | 0.659 |
2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery (DO NOT EDIT)[3]
Public Reporting of Cardiac Surgery Outcomes (DO NOT EDIT)[3]
| Class I |
| “1. Public reporting of cardiac surgery outcomes should use risk-adjusted results based on clinical data.[4][5][6][7][8][9][10][11] (Level of Evidence: B)” |
Use of Outcomes or Volume as CABG Quality Measures (DO NOT EDIT)[3]
| Class I |
| “1. All cardiac surgery programs should participate in a state, regional, or national clinical data registry and should receive periodic reports of their risk-adjusted outcomes. (Level of Evidence: C)” |
| Class IIa |
| “1. When credible risk-adjusted outcomes data are not available, volume can be useful as a structural metric of CABG quality.[12][13][14][15][16][17][18][19][20][21][22][23][24][25][26] (Level of Evidence: B)” |
| Class IIb |
| “1. Affiliation with a high-volume tertiary center might be considered by cardiac surgery programs that perform fewer than 125 CABG procedures annually. (Level of Evidence: C)” |
References
- ↑ 1.0 1.1 1.2 1.3 Writing Committee Members. Lawton JS, Tamis-Holland JE, Bangalore S, Bates ER, Beckie TM; et al. (2022). “2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines”. J Am Coll Cardiol. 79 (2): e21–e129. doi:10.1016/j.jacc.2021.09.006. PMID 34895950 Check
|pmid=value (help). - ↑ O’Brien SM, Feng L, He X, Xian Y, Jacobs JP, Badhwar V; et al. (2018). “The Society of Thoracic Surgeons 2018 Adult Cardiac Surgery Risk Models: Part 2-Statistical Methods and Results”. Ann Thorac Surg. 105 (5): 1419–1428. doi:10.1016/j.athoracsur.2018.03.003. PMID 29577924.
- ↑ 3.0 3.1 3.2 Hillis LD, Smith PK, Anderson JL, Bittl JA, Bridges CR, Byrne JG; et al. (2011). “2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines”. Circulation. doi:10.1161/CIR.0b013e31823c074e. PMID 22064599.
- ↑ Geraci JM, Johnson ML, Gordon HS, Petersen NJ, Shroyer AL, Grover FL; et al. (2005). “Mortality after cardiac bypass surgery: prediction from administrative versus clinical data”. Med Care. 43 (2): 149–58. PMID 15655428.
- ↑ Hannan EL, Kilburn H, Lindsey ML, Lewis R (1992). “Clinical versus administrative data bases for CABG surgery. Does it matter?”. Med Care. 30 (10): 892–907. PMID 1405795.
- ↑ Hannan EL, Racz MJ, Jollis JG, Peterson ED (1997). “Using Medicare claims data to assess provider quality for CABG surgery: does it work well enough?”. Health Serv Res. 31 (6): 659–78. PMC 1070152. PMID 9018210.
- ↑ Hartz AJ, Kuhn EM (1994). “Comparing hospitals that perform coronary artery bypass surgery: the effect of outcome measures and data sources”. Am J Public Health. 84 (10): 1609–14. PMC 1615096. PMID 7943479.
- ↑ Jones RH, Hannan EL, Hammermeister KE, Delong ER, O’Connor GT, Luepker RV; et al. (1996). “Identification of preoperative variables needed for risk adjustment of short-term mortality after coronary artery bypass graft surgery. The Working Group Panel on the Cooperative CABG Database Project”. J Am Coll Cardiol. 28 (6): 1478–87. PMID 8917261.
- ↑ Mack MJ, Herbert M, Prince S, Dewey TM, Magee MJ, Edgerton JR (2005). “Does reporting of coronary artery bypass grafting from administrative databases accurately reflect actual clinical outcomes?”. J Thorac Cardiovasc Surg. 129 (6): 1309–17. doi:10.1016/j.jtcvs.2004.10.036. PMID 15942571.
- ↑ Shahian DM, Silverstein T, Lovett AF, Wolf RE, Normand SL (2007). “Comparison of clinical and administrative data sources for hospital coronary artery bypass graft surgery report cards”. Circulation. 115 (12): 1518–27. doi:10.1161/CIRCULATIONAHA.106.633008. PMID 17353447.
- ↑ Tu JV, Sykora K, Naylor CD (1997). “Assessing the outcomes of coronary artery bypass graft surgery: how many risk factors are enough? Steering Committee of the Cardiac Care Network of Ontario”. J Am Coll Cardiol. 30 (5): 1317–23. PMID 9350934.
- ↑ Clark RE (1996). “Outcome as a function of annual coronary artery bypass graft volume. The Ad Hoc Committee on Cardiac Surgery Credentialing of The Society of Thoracic Surgeons”. Ann Thorac Surg. 61 (1): 21–6. PMID 8561556.
- ↑ Grumbach K, Anderson GM, Luft HS, Roos LL, Brook R (1995). “Regionalization of cardiac surgery in the United States and Canada. Geographic access, choice, and outcomes”. JAMA. 274 (16): 1282–8. PMID 7563533.
- ↑ Hannan EL, Kilburn H, Bernard H, O’Donnell JF, Lukacik G, Shields EP (1991). “Coronary artery bypass surgery: the relationship between inhospital mortality rate and surgical volume after controlling for clinical risk factors”. Med Care. 29 (11): 1094–107. PMID 1943270.
- ↑ Hannan EL, Siu AL, Kumar D, Kilburn H, Chassin MR (1995). “The decline in coronary artery bypass graft surgery mortality in New York State. The role of surgeon volume”. JAMA. 273 (3): 209–13. PMID 7807659.
- ↑ Hannan EL, Wu C, Ryan TJ, Bennett E, Culliford AT, Gold JP; et al. (2003). “Do hospitals and surgeons with higher coronary artery bypass graft surgery volumes still have lower risk-adjusted mortality rates?”. Circulation. 108 (7): 795–801. doi:10.1161/01.CIR.0000084551.52010.3B. PMID 12885743.
- ↑ Kalant N, Shrier I (2004). “Volume and outcome of coronary artery bypass graft surgery: are more and less the same?”. Can J Cardiol. 20 (1): 81–6. PMID 14968146.
- ↑ Nallamothu BK, Saint S, Ramsey SD, Hofer TP, Vijan S, Eagle KA (2001). “The role of hospital volume in coronary artery bypass grafting: is more always better?”. J Am Coll Cardiol. 38 (7): 1923–30. PMID 11738295.
- ↑ Peterson ED, Coombs LP, DeLong ER, Haan CK, Ferguson TB (2004). “Procedural volume as a marker of quality for CABG surgery”. JAMA. 291 (2): 195–201. doi:10.1001/jama.291.2.195. PMID 14722145.
- ↑ Rathore SS, Epstein AJ, Volpp KG, Krumholz HM (2004). “Hospital coronary artery bypass graft surgery volume and patient mortality, 1998-2000”. Ann Surg. 239 (1): 110–7. doi:10.1097/01.sla.0000103066.22732.b8. PMC 1356200. PMID 14685108.
- ↑ Shahian DM, O’Brien SM, Normand SL, Peterson ED, Edwards FH (2010). “Association of hospital coronary artery bypass volume with processes of care, mortality, morbidity, and the Society of Thoracic Surgeons composite quality score”. J Thorac Cardiovasc Surg. 139 (2): 273–82. doi:10.1016/j.jtcvs.2009.09.007. PMID 20022608.
- ↑ Showstack JA, Rosenfeld KE, Garnick DW, Luft HS, Schaffarzick RW, Fowles J (1987). “Association of volume with outcome of coronary artery bypass graft surgery. Scheduled vs nonscheduled operations”. JAMA. 257 (6): 785–9. PMID 3492614.
- ↑ Shroyer AL, Marshall G, Warner BA, Johnson RR, Guo W, Grover FL; et al. (1996). “No continuous relationship between Veterans Affairs hospital coronary artery bypass grafting surgical volume and operative mortality”. Ann Thorac Surg. 61 (1): 17–20. doi:10.1016/0003-4975(95)00830-6. PMID 8561546.
- ↑ Sowden AJ, Deeks JJ, Sheldon TA (1995). “Volume and outcome in coronary artery bypass graft surgery: true association or artefact?”. BMJ. 311 (6998): 151–5. PMC 2550219. PMID 7613425.
- ↑ Welke KF, Barnett MJ, Sarrazin MS, Rosenthal GE (2005). “Limitations of hospital volume as a measure of quality of care for coronary artery bypass graft surgery”. Ann Thorac Surg. 80 (6): 2114–9. doi:10.1016/j.athoracsur.2005.05.017. PMID 16305854.
- ↑ Wu C, Hannan EL, Ryan TJ, Bennett E, Culliford AT, Gold JP; et al. (2004). “Is the impact of hospital and surgeon volumes on the in-hospital mortality rate for coronary artery bypass graft surgery limited to patients at high risk?”. Circulation. 110 (7): 784–9. doi:10.1161/01.CIR.0000138744.13516.B5. PMID 15302792.
Imaging in the patient undergoing CABG
Imaging in the patient undergoing CABG
Chest x-ray | Coronary Angiography | CT Angiography | MRI Angiography | Trans-Esophageal Echocardiography | Epiaortic Ultrasound
Goals of Treatment
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-in-Chief: Cafer Zorkun, M.D., Ph.D. [2], Mohammed A. Sbeih, M.D.[3]
Goals of treatment
The main goal of this procedure is treat Ischemic heart disease where the main problems are narrowing of the coronary arteries from fatty deposits in these vessels which then obstruct blood flow to the heart muscle. This causes the heart muscle to starve of oxygen, thus causing anginal pain. A complete blockage may causes a myocardial infarction (MI), where the heart muscle starts to die and is irreversible. It is therefore vital to correct any partial blockage before a complete obstruction occurs.
Coronary artery bypass grafting (CAGB) involves removing veins from other parts of the patients body, most commonly from legs or the chest wall (the Internal mammary artery) and inserting them around the blocked heart vessel so that blood flows through these new vessels instead. A number of blood vessels can be replaced at the same time. For example, a triple heart bypass replaces 3 coronary arteries in the same operation.
Recently CABG started to be done through a keyhole (laparoscopic) incision while the heart is still pumping, this new technique decreases the recovery time. Tradtionally, a large incision through the centre of the chest (sternum) was made, the heart stopped and the patient put onto a bypass machine, but recovery took longer due to the trauma to the chest wall. This procedure is particularly useful when other methods such as angioplasty are not suitable or have failed.
Perioperative and Intraoperative Management
Aspirin and Clopidogrel | Beta-Blockers | ACE Inhibitors/ARBs | Management of Hyperlipidemia | Management of Mediastinitis/Perioperative Infection | Percutaneous Coronary Intervention (PCI) To Treat Saphenous Vein Graft Failure | Maintaining Glucose Level | Coronary artery bypass surgery bleeding/transfusion | Management of Dysrhythmias | Smoking Cessation | Perioperative Management of Myocardial Dysfunction | Perioperative Carotid Artery Noninvasive Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Varun Kumar, M.B.B.S. [2]
Aspirin and Clopidogrel | Beta-Blockers | ACE Inhibitors/ARBs | Management of Hyperlipidemia | Hormonal manipulation | Management of Mediastinitis/Perioperative Infection | Percutaneous Coronary Intervention (PCI) To Treat Saphenous Vein Graft Failure | | Maintaining Glucose Level | Coronary artery bypass surgery bleeding/transfusion | Management of Dysrhythmias | Smoking Cessation | Perioperative Management of Myocardial Dysfunction | Perioperative Carotid Artery Noninvasive Screening
General procedular issues for CABG. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization (Please do not edit)
| Class I |
| “1. For patients undergoing CABG, establishment of multidisciplinary, evidence based perioperative management programs is recommended to optimize analgesia, minimize opioid exposure, prevent complications and to reduce time to extubation, length of stay, and health care costs(Level of Evidence: B-NR) ” |
References
- ↑ “Correction to: 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines”. Circulation. 145 (11): e771. 2022. doi:10.1161/CIR.0000000000001061. PMID 35286170 Check
|pmid=value (help).
Perioperative and Intraoperative Monitoring
Electrocardiographic Monitoring | Pulmonary Artery Catheterization | Central Nervous System Monitoring
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editors-in-Chief: Cafer Zorkun, M.D., Ph.D. [2],Mohammed A. Sbeih, M.D. [3]
Electrocardiographic Monitoring | Pulmonary Artery Catheterization | Central Nervous System Monitoring
References
Surgical Procedure
Anesthetic Considerations | The Traditional Coronary Artery Bypass Grafting Procedure (Simplified) | Minimally Invasive CABG | Conduits Used for Bypass | Videos on Saphenous Vein-Graft Harvesting | Videos on Coronary Artery Bypass Surgery | Cardiopulmonary Bypass
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [2]
Associate Editors-in-Chief: Cafer Zorkun, M.D., Ph.D. [3],Mohammed A. Sbeih, M.D. [4]
The Traditional coronary artery bypass grafting procedure (simplified)
- The patient is brought to the operating room and moved onto the operating table.
- An anesthetist places a variety of intravenous lines, often including a pulmonary artery catheter and injects an induction agent (usually propofol) to render the patient unconscious and to anesthetize the patient.
- An endotracheal tube is inserted and secured by the anesthetist or a respiratory therapist and mechanical ventilation is started.
- The chest is opened via a median sternotomy and the heart is examined by the surgeon.
- The grafts are harvested – frequent conduits are the internal thoracic arteries, radial arteries and saphenous veins.
- The surgeon stops the heart and initiates cardiopulmonary bypass; or in the case of “off-pump” surgery, places devices to stabilize the heart.
- One end of each graft is sewn onto the coronary arteries beyond the blockages and the other end is attached to the aorta.
- The heart is restarted; or in “off-pump” surgery, the stabilizing devices are removed. In some cases, the aorta is partially occluded by a C shaped clamp, the heart is restarted and suturing of the grafts to the aorta is done in this partially occluded section of the aorta while the heart is beating. This reduces time spent on the heart lung machine.
- The sternum is wired together and the incisions are sutured closed.
- The patient is moved to the intensive care unit (ICU) to recover. After awakening and stabilizing in the ICU (approximately 1 day), the patient is transferred to the cardiac surgery unit until ready to go home (approximately 4 days).
Minimally invasive CABG
Alternate methods of minimally invasive coronary artery bypass surgery have been developed in recent times. Off-pump coronary artery bypass surgery (OPCAB) is a technique of performing bypass surgery without the use of cardiopulmonary bypass (the heart-lung machine). Futher refinements to OPCAB have resulted in Minimally invasive direct coronary artery bypass surgery (MIDCAB) which is a technique of performing bypass surgery through a 5 to 10 cm incision. People with multi-vessel coronary disease and desire a minimally invasive approach to surgery may be eligible for hybrid bypass. A hybrid approach combines coronary bypass (using the MIDCAB approach) and coronary stenting.
Conduits used for bypass
The choice of conduits (arteries and/or veins from elsewhere in the body) to bypass the blockages is dependent on the surgeon and institution. Typically, the left internal thoracic artery (LITA) (also referred to as the left internal mammary artery or LIMA) is grafted to the Left Anterior Descending artery and a combination of other arteries and veins is used for other coronary arteries. The right internal thoracic artery (RITA), the great saphenous vein from the leg and the radial artery from the forearm are frequently used. The right gastroepiploic artery from the stomach is infrequently used given the difficult mobilization from the abdomen.
Saphenous vein anatomy
The great saphenous vein (GSV) is frequently used as a conduit for CABG. It originates from where the dorsal vein of the first digit (the large toe) merges with the dorsal venous arch of the foot.
After passing anterior to the medial malleolus (where it often can be visualized and palpated), it runs up the medial side of the leg. At the knee, it runs over the posterior border of the medial epicondyle of the femur bone.
The great saphenous vein then courses laterally to lie on the anterior surface of the thigh before entering an opening in the fascia lata called the saphenous opening. It joins with the femoral vein in the region of the femoral triangle at the saphenofemoral junction.
The small saphenous vein (also lesser saphenous vein) originates where the dorsal vein from the fifth digit (smallest toe) merges with the dorsal venous arch of the foot, which attaches to the great saphenous vein. It is considered a superficial vein and is subcutaneous (just under the skin). From its origin, it courses around the lateral aspect of the foot (inferior and posterior to the lateral malleolus) and runs along the posterior aspect of the leg (with the sural nerve), passes between the heads of the gastrocnemius muscle, and drains into the popliteal vein, approximately at or above the level of the knee joint.
-
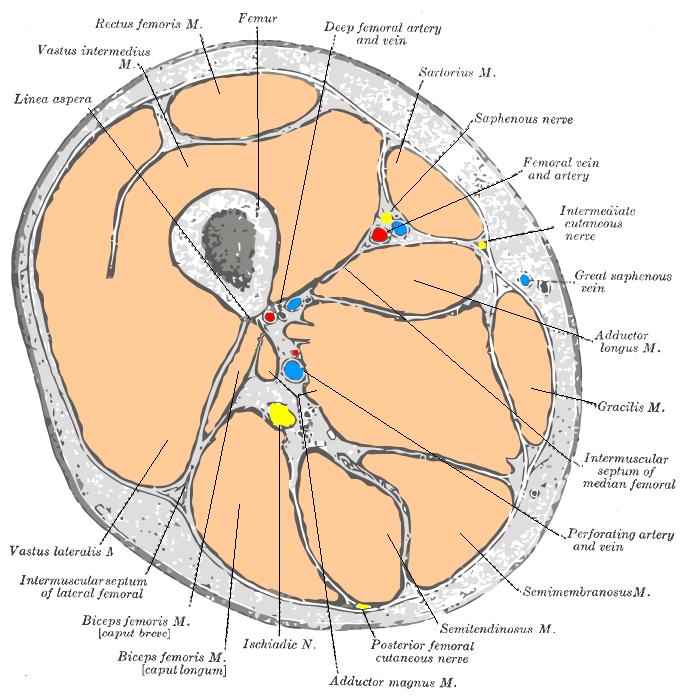 Cross-section through the middle of the thigh.
Cross-section through the middle of the thigh. -
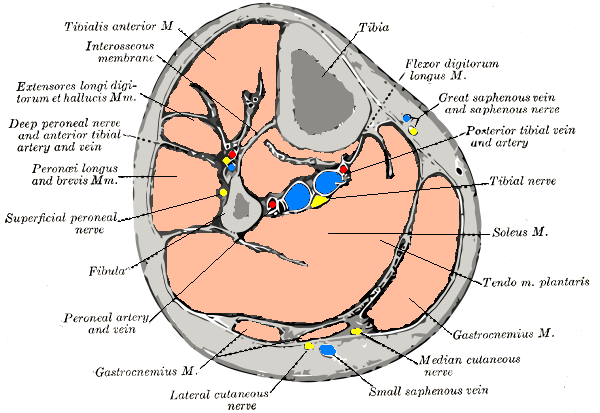 Cross-section through middle of leg.
Cross-section through middle of leg. -
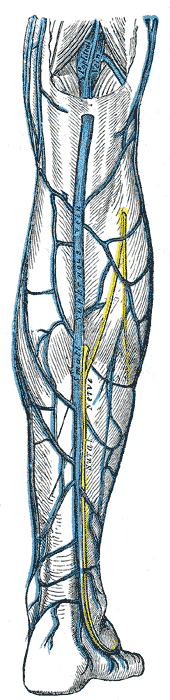
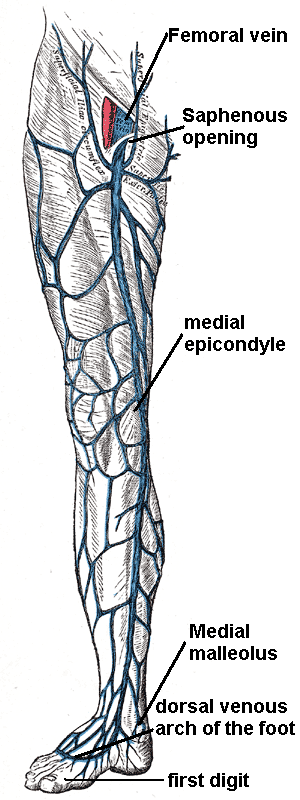 The great saphenous vein and landmarks along its course
The great saphenous vein and landmarks along its course -
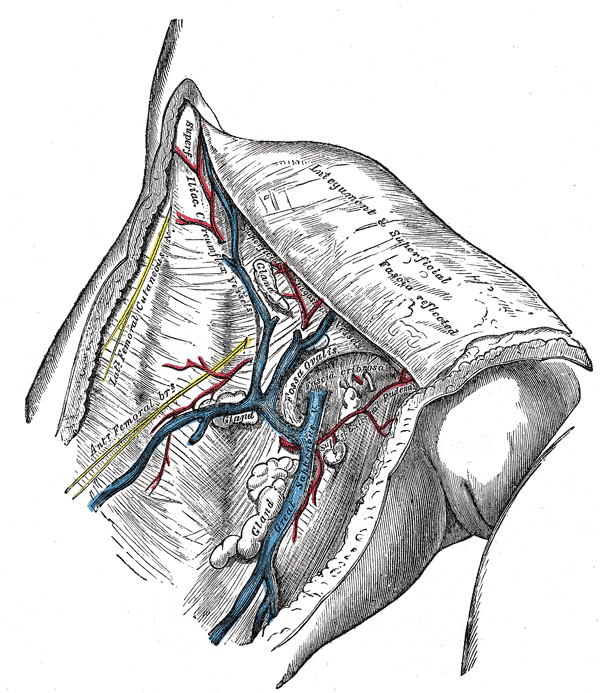 The great saphenous vein and its tributaries at the fossa ovalis in the groin.
The great saphenous vein and its tributaries at the fossa ovalis in the groin. -
 Small saphenous vein and its tributaries.
Small saphenous vein and its tributaries.



Saphenous vein harvesting
The saphenous vein can be harvested by either direct visualization or via an endoscopic approach. Veins that are used either have their valves removed or are turned around so that the valves in them do not occlude blood flow in the graft. The technique of saphenous vein harvesting may influence later SVG patency. The process of harvesting the vein and pressure testing the vein for a leak may damage the endothelium.[1][2]
The endoscopic approach has been associated with lower rates of wound infection, greater patient satisfaction, and earlier mobilization.[3][4][5][6] One small randomized study of 144 patients showed no difference in histologic findings between the traditional and endoscopic techniques.[3]In another small study of 40 patients randomized to the two techniques, no difference was seen in angiographic patency at 3 months.[6]Another small randomized study of 144 patients who returned for angiography demonstrated an occlusion rate of 21.7% for the endoscopic approach vs 17.6% for the open approach.[5] However, non- randomized data from a much larger multicenter study does suggest that endoscopic harvesting may be associated with higher rates of failure and adverse events such as death and MI.[4]
Complications associated with saphenous vein harvesting include the following:
- Saphenous nerve injury
- Infection at incision sites or sepsis.
- Deep vein thrombosis (DVT)
- Keloid scarring
- Chronic pain at incision sites
Videos on spahenous vein graft harvesting
{{#ev:youtube|VbdE6JWdY1s}}
{{#ev:youtube|QthyR0bTHzc}}
{{#ev:youtube|sV-qE2SIkJU}}
Conduit nomenclature
The terms single bypass, double bypass, triple bypass, quadruple bypass and quintuple bypass refer to the number of coronary arteries bypassed in the procedure.
In other words, a double bypass means two coronary arteries are bypassed (e.g. the left anterior descending (LAD) coronary artery and right coronary artery (RCA)); a triple bypass means three vessels are bypassed (e.g. LAD, RCA, left circumflex artery (LCX)); a quadruple bypass means four vessels are bypassed (e.g. LAD, RCA, LCX, first diagonal artery of the LAD) while quintuple means five. Less commonly more than four coronary arteries may be bypassed.
A greater number of bypasses does not imply a person is “sicker,” nor does a lesser number imply a person is “healthier.”[7] A person with a large amount of coronary artery disease (CAD) may receive fewer bypass grafts owing to the lack of suitable “target” vessels.
A patient with a single stenosis (“narrowing”) of the left main coronary artery often requires only two bypasses (to the LAD and the LCX). However, depending upon the anatomy, grafts may also need to be placed to a large diagonal artery, or to additional large obtuse marginal branches.
Assessment of target vessels for saphenous vein grafting
A coronary artery may be unsuitable for bypass grafting for the following reasons:
- Size: If the native target artery is small (< 1 mm or < 1.5 mm depending on surgeon preference)
- Location: Some distal locations of the native target artery may not be accessible, or a conduit may not reach the far down the native artery.
- Native artery calcification: Heavily calcified native arteries are sometimes technically not amenable to anastamosis of a conduit.
- Diffuse disease: The native artery may not have a section of vessel that has minimal disease where a conduit can be grafted to.
- The native artery lies in the heart muscle or is intramyocardial: In this scenario the native coronary artery is located within the heart muscle rather than on the surface of the heart and a graft cannot be attached to it.
Although the cardiothoracic surgeon reviews the coronary angiogram prior to surgery and identifies the lesions (or “blockages”) in the coronary arteries and will estimate the number of bypass grafts prior to surgery, the final decision is made in the operating room based upon the direct examination of the heart and the suitability of the native target vessel for bypassing.
Pathophysiology of saphenous vein graft disease
The pathophysiology of aortocoronary saphenous vein graft disease has classically been divided into three components:[8]
- Early degeneration in the first month due to thrombosis
- Mid course degeneration from month one to one year due to intimal hyperplasia
- Late degeneration due to atherosclerosis
Early failure of saphenous vein grafts
While thrombosis predominates during this period, early failure of saphenous vein grafts can be precipitated by a variety of factors.
Technical failures
This is due to a technical failure at the site where the conduit is sutured to the aorta proximately or to the native target vessel distally. This technical failure then leads to thrombosis of the conduit. This failure can in some cases be treated by emergency re-operation or percutaneously by angioplasty and stenting. Care must be taken during the percutaneous approach to assure that the sutures are not disrupted and that there is not a rupture at the site of the anastomosis.
No reflow downstream in the myocardium
Despite restoration of into or improved flow down the epicardial artery, myocardial edema, embolization, and capillary blistering may result in impaired perfusion into the myocardium. This in turn may lead to poor flow through the graft, and subsequent thrombosis.
Midcourse failures of saphenous vein grafts
Midcourse degeneration from one month to one year is classically described as being due to intimal hyperplasia.[9]The process is complex and the response of the SVG wall is likely biphasic. Days to weeks after CABG, there is an increase in the area of both the intima (due to smooth muscle cell proliferation) [10]and the adventitia (due to fibroblast proliferation)[11]. After the first 4 to 6 weeks, the SVGs then undergo “negative remodeling”, that is to say there is a loss in the total vessel diamter. In one study using CT angiography, there was a mean loss of SVG lumen diameter of 9% (a decrease from 3.69 mm to 3.36 mm) but a decrease in the thickness of 0.13 mm in the SVG wall thickness over this time.[12] The mechanism underlying this negative remodeling thought to be the reaction of the venous conduit to the greater than normal flow, wall stretch, shear stress as well as humoral factors such as cytokines and vasoactive substances.
Late failure of saphenous vein grafts
Multiple pathophysiologic processes contribute to late graft degeneration or late graft failure. These processes including intimal hyperplasia, atherosclerotic plaque formation, and graft remodeling. Additionally, arterialization of the graft accelerates atherosclerosis. In addition to mechanically obstructing flow, these blockages are more “friable” (i.e. they easily break into small pieces and embolize downstream into the myocardium impairing perfusion) and more prone to thrombus than plaques found in native vessels. Another pathophysiologic mechanism whereby SVGs are more susceptible to thrombotic occlusion is the fact that they lack side branches.
Saphenous vein graft patency
Definitions
The rate of saphenous vein graft failure varies depending upon the definition used and the nature of the study design. [13][14][15][16] Rates estimated based upon retrospective studies of patients who are symptomatic underestimate the true rate of SVG failure because only those patients who survive who are symptomatic undergo catheterization. The most accurate assessment is based upon prospective studies in which all patients undergo mandatory cardiac catheterization at a uniform timepoint. The rates will also vary depending upon the complexity of disease, the diffuse nature of the disease, the extent of revascularization, and whether a per-lesion or a per-patient analysis is undertaken.
Saphenous vein graft occlusion is defined as a complete, 100% occlusion of a saphenous vein graft. [17]
Saphenous vein failure is defined as an occlusion of the vein graft or a 75% or greater stenosis.
The rate of occlusion or failure of saphenous vein grafts is calculated on a per graft basis and a per patient basis. The per patient basis is higher, because only one vein graft out of several must fail for the patient to be characterized as a failure.
Current rates of graft occlusion and failure are as follows:[17]
The rate of per patient vein graft occlusion at 12-18 months is about 42%
The rate of per patient vein graft failure at 12-18 months is about 46%
The rate of per graft vein graft occlusion at 12-18 months is about 26%
The rate of per graft vein graft failure at 12-18 months is about 29%
As a comparison, the rate of internal mammary artery failure at 12-18 months was only 8%.
Time course of SVG failure
- Early failure: Withing the first month, 8% to 18% of SVGs fail again largely due to the factors cited above that precipitate thrombosis. [18][19]
- Mid course failure: From one month through a year an additional 10—15% of SVGs occlude. Again, during this period the pathophysiology is predominantly due to smooth muscle cell hyperplasia emanating from the intima of the vein.[8]
- Late Failure:After year 1, the annual rate of occlusion is about 1—4% per per year. Again, this process of late failure is predominantly due to atherosclerosis and some intimal hyperplasia.
- Very Late Failure: SVG occlusion after 5 years is predominantly mediated by atherosclerosis. A convenient and often quoted statistic is that at 10 years, approximately 50% of SVGs remain patent[20]
Determinants of sapheous vein graft patency
Graft patency is dependent on a number of factors, including the type of graft used (internal thoracic artery, radial artery, or great saphenous vein), the size or the coronary artery that the graft is anastomosed with, and, of course, the skill of the surgeon(s) performing the procedure. Arterial grafts (e.g. left internal mammary (LIMA), radial) are far more sensitive to rough handling than the saphenous veins and may go into spasm if handled improperly.
Technical factors during surgery
A large VA cooperative study evaluated the technical factors associated with 3 year patency among those SVGs that were patent at 7 to 10 days following CABG. SVG occlusion was associated with the following:[21]
- Cross-clamp time > 80 min (p < 0.001)
- Vein preservation solution temperature > 5 degrees C (p = 0.009)
- Bypass time > 2 hours (p = 0.042)
- Number of proximal anastomoses > 2 (p = 0.018)
- Operation time > 5 hours (p = 0.044)
- Intermittent instead of continuous cross-clamp technique (p = 0.024).
- Sequential vs single Y vein graft (p = 0.060).
In-situ vs free grafts
Generally the best patency rates are achieved with the in-situ (the proximal end is left connected to the subclavian artery) left internal thoracic artery (a LIMA) with the distal end being anastomosed with the coronary artery (typically the left anterior descending artery or a diagonal branch artery). Lesser patency rates can be expected with radial artery grafts and “free” internal thoracic artery grafts (where the proximal end of the thoracic artery is excised from its origin from the subclavian artery and re-anastomosed with the ascending aorta).
Venous vs Arterial conduits
Saphenous vein grafts have poorer patency rates than arterial grafts, but are more available, as the patients can have multiple segments of the saphenous vein used to bypass different arteries.
LITA grafts are longer-lasting than vein grafts, both because the artery is more robust than a vein and because, being already connected to the arterial tree, the LITA need only be grafted at one end. The LITA is usually grafted to the left anterior descending coronary artery (LAD) because of its superior long-term patency when compared to saphenous vein grafts.[22][23]
Impact of harvesting method on saphenous vein graft patency
The method of harvesting vein grafts may be associated with late vein graft patency. In one small study of 40 patients randomized to endoscopic vs traditional techniques, no difference was seen in angiographic patency at 3 months.[6]Another small randomized study of 144 patients who returned for angiography at 6 months and demonstrated an occlusion rate of 21.7% for the endoscopic approach vs 17.6% for the open approach.[5] In a non-randomized subgroup analysis from the PREVENT IV study, harvesting of vein-grafts with the use of endoscopy (endoscopic harvesting) was associated with a higher rate of saphenous vein graft failure at 12-18 months compared with open harvesting of the veins under direct visualization (46.7% vs. 38.0%, P<0.001 at 12-18 months).[4] Likewise, clinical outcomes were worse at 3 years: use of endoscopy was associated with higher rates of death, myocardial infarction, or repeat revascularization (20.2% vs. 17.4%; p=0.04), death or myocardial infarction (9.3% vs. 7.6%; p=0.01), and death (7.4% vs. 5.8%; adjusted hazard ratio, 1.52; 95% CI, 1.13 to 2.04; p=0.005). Although these observational data are provocative, further randomized clinical trials involving large numbers of patients from multiple centers with long term follow-up would be needed to compare the safety and effectiveness of the two harvesting techniques.
Perioperative MI is associated with a higher rate of SVG failure
The rate of one-year saphenous vein graft failure has been documented to be 62.4% of patients with and 43.8% of patients without perioperative MI (p <0.001).[24]
Smaller target vessels are associated with a higher rate of SVG failure
The rate of SVG occlusion at one year is about twice as high in those SVGs that are anastomosed to a target vessel with a diameter < 2.0 mm.[25] The rate of SVG occlusion at one year in target vessels less than or equal to 2.0 mm in diameter was 20.1% on aspirin and 32.3% off aspirin (p = 0.008), while in those SVGs anastomosed to target vessels > 2.0 mm in diameter the rates were lower: 8.7% and 9.0% respectively. The converse of this, is that larger conduits have been associated with higher rates of SVG occlusion.[5]
Target artery location
In a multivariate model in a small study, SVG grafting to the diagonal branch has been associated with 1.76 times higher rates of SVG occlusion.[5]
Graft flow
Poor graft flow has been associated with higher rates of SVG occlusion.[5]
Serum cholesterol
A serum cholesterol > 225 mg/dl has been associated with higher rates of SVG failure at 3 years in a multivariate model from a large VA cooperative study.[21]
Pharmacotherapy
Early post-operative aspirin has been associated with a lower rate of SVG failure for the first 3 years after CABG in a large number of randomized trials.[26][27][28][29][30][31][32][33] [34][35][36][37][38][39]
Factors not associated with saphenous vein graft patency
Although a creatinine clearance < 60 ml/sec has been associated with higher rates of death, MI, and revascularization, it was not associated with a higher rate of SVG or internal thoracic artery failure rates. [40] In one large VA cooperative study, age, race, smoking history, high density lipoprotein cholesterol, vein source (thigh vs. calf) were not associated with 3 year SVG patency.[21]
Association of saphenous vein graft failure with clinical events
In the PREVENT IV study, SVG failure was associated with a 13.9% rate of death and MI (122/878) vs 0.9% (9/1,042) for those patients without SVG failure (these numbers exclude peri-operative MI).[17] Likewise, the rate of death, MI, and revascularization was higher among patients with SVG failure (26.0% vs 1.8%). Despite these elevated rates of adverse events, it shoud be noted that about half of the patients with SVG failure did not have clinical events. This may be because the native artery remained open or because there was extensive collaterals. It should slo be noted that the development of heart failure or angina following SVG failure may not be captured in the endpoint of death, MI, and revascularization.
In a large cohort of 1,388 patients who underwent a first coronary artery bypass graft procedure, vein graft patency was temporally related both to reoperation as well as survival.[41]
Other non-atherosclerotic saphenous vein graft diseases
Saphenous vein graft aneurysms
This disease process is also known as SVGA, aortocoronary saphenous vein graft aneurysms, saphenous vein graft aneurysm disease, or saphenous vein graft aneurysmal dilatation and is defined as a local dilation of the vessel more than 1.5X the adjacent reference segment. The aneurysms can be up to 14 cm in diameter.
Classification
- True aneurysms: All 3 layers of the vessel wall are involved
- Pseudoaneurysms: There is disruption of 1 or more layers of the vessel wall.
Epidemiology and demographics
Over the course f a SVGs 7 year lifetime, the risk of aneurysm development is 14%. True aneurysms outnumber false ones by a ratio of 2:1.
Pathophysiology
Causes of saphenous vein graft aneurysms include the following:
- Atherosclerosis
- Hypertension
- Mycotic
- Postoperative mediastinitis
- Previous aneurysms
- Torn sutures
Natural history and complications
SVGAs can rupture which is associated with a high rate of morbidity and even mortality. They can also be a nidus for embolization.
Diagnosis
History
If a patient with a history of CABG develops chest pain and has a mediastinal mass, an SVGA should be suspected.
The majority of patients are asymptomatic with a true aneurysm, and most often the SVGA is an incidental finding on an imaging study. If the patient is symptomatic, about half the time it presents as an acute coronary syndrome. Very rarely tamponade from compression of the right atrium or ischemia due to compression of the left internal mammary artery bypass graft has been observed.
In contrast to true aneurysms, patients with false aneurysms are symptomatic in 85% of cases. About two thirds of the time they present with an acute coronary syndrome. If a patient with an SVGA does present with chest pain or hemoptysis, it may be due to the formation of a fistula.
Physical examination
Rarely on physical examination a murmur will be auscultated or cutaneous bleeding will be observed (both due to a fistula).
Imaging
SVGA can be definitively diagnosed on either coronary angiography or CT angiography. On occasion, an SVGA can be observed as either hilar or mediastinal mass on chest x ray.
Management
Pharmacologic management consists of aspirin and lipid-lowering therapy. The benefit if any of coumadin and beta-blockers is not known.
A surgery or a percutaneous intervention is suggested if:
- A pseudoaneurysm is present
- The aneurysm is more than 2 cm greater than the adjacent vessel
- A fistula is present (surgery, coiling, or stenting)
- If the aneurysm is mycotic (surgery)
Surgery
There are multiple surgical approaches to repairing an aneurysm:
- Ligate the aneurysm-containing SVG and place a new SVG.
- Resect the aneurysmal portion of the diseased graft and sew a new SVG segment in in an end-to-end fashion
- Ligate the old SVG without revascularization
- Evacuate the hematoma and repair the SVG with a venous patch graft.
Percutaneous intervention
In the past, percutaneous intervention was reserved for patients who were too sick to undergo surgery. However, due to the improved tools that are available, more patients are undergoing percutaneous intervention as described below:
- Coil embolization: This technique has evolved so that a stent excludes the coil form lying in the lumen of the SVG.
- Covered stents: The JOSTENT Coronary Stent Graft (Abbott Vascular, Redwood City, Calif) can be used to exclude the aneurysm form the body of the SVG. The device is made up of an ultra-thin layer of polytetrafluoroethylene (PTFE).
- Multiple overlapping stents can be used to exclude the aneurysm.
Amyloidosis of saphenous coronary bypass grafts
Amyloid has been associated with accelarated disease in saphenous vein grafts.[42] [43] [44] [45] [46]
Rupture of the saphenous vein coronary artery bypass grafts
Aspergillus species causing a necrotizing vasculitis have been associated with rupture of a saphenous vein grafts.
References
- ↑ Lawrie GM, Weilbacher DE, Henry PD. Endothelium-dependent relaxation in human saphenous vein grafts. Effects of preparation and clinicopathologic correlations. J Thorac Cardiovasc Surg 1990;100:612—20.
- ↑ Souza DS, Johansson B, Bojo¨ L, Karlsson R, Geijer H, Filbey D, Bodin L, Arbeus M, Dashwood MR. Harvesting the saphenous vein with surrounding tissue for CABG provides long-term graft patency comparable to the left internal thoracic artery: results of a randomized longitudinal trial. J Thorac Cardiovasc Surg 2006;132:373—8.
- ↑ 3.0 3.1 Kiaii B, Moon BC, Massel D, Langlois Y, Austin TW, Willoughby A, Guiraudon C, Howard CR, Guo LR (2002). “A prospective randomized trial of endoscopic versus conventional harvesting of the saphenous vein in coronary artery bypass surgery”. J. Thorac. Cardiovasc. Surg. 123 (2): 204–12. PMID 11828277. Retrieved 2010-07-23. Unknown parameter
|month=ignored (help) - ↑ 4.0 4.1 4.2 Lopes RD, Hafley GE, Allen KB, Ferguson TB, Peterson ED, Harrington RA, Mehta RH, Gibson CM, Mack MJ, Kouchoukos NT, Califf RM, Alexander JH (2009). “Endoscopic versus open vein-graft harvesting in coronary-artery bypass surgery”. The New England Journal of Medicine. 361 (3): 235–44. doi:10.1056/NEJMoa0900708. PMID 19605828. Retrieved 2010-07-12. Unknown parameter
|month=ignored (help) - ↑ 5.0 5.1 5.2 5.3 5.4 5.5 Yun KL, Wu Y, Aharonian V, Mansukhani P, Pfeffer TA, Sintek CF, Kochamba GS, Grunkemeier G, Khonsari S (2005). “Randomized trial of endoscopic versus open vein harvest for coronary artery bypass grafting: six-month patency rates”. J. Thorac. Cardiovasc. Surg. 129 (3): 496–503. doi:10.1016/j.jtcvs.2004.08.054. PMID 15746730. Retrieved 2010-07-23. Unknown parameter
|month=ignored (help) - ↑ 6.0 6.1 6.2 Perrault LP, Jeanmart H, Bilodeau L, Lespérance J, Tanguay JF, Bouchard D, Pagé P, Carrier M (2004). “Early quantitative coronary angiography of saphenous vein grafts for coronary artery bypass grafting harvested by means of open versus endoscopic saphenectomy: a prospective randomized trial”. J. Thorac. Cardiovasc. Surg. 127 (5): 1402–7. doi:10.1016/j.jtcvs.2003.10.040. PMID 15115999. Retrieved 2010-07-23. Unknown parameter
|month=ignored (help) - ↑ Ohki S, Kaneko T, Satoh Y; et al. (2002). “[Coronary artery bypass grafting in octogenarian]”. Kyobu geka. The Japanese journal of thoracic surgery (in Japanese). 55 (10): 829–33, discussion 833–6. PMID 12233100.
- ↑ 8.0 8.1 Motwani JG, Topol EJ (1998). “Aortocoronary saphenous vein graft disease: pathogenesis, predisposition, and prevention”. Circulation. 97 (9): 916–31. PMID 9521341. Retrieved 2010-07-22. Unknown parameter
|month=ignored (help) - ↑ Lau GT, Lowe HC, Kritharides L (2004). “Cardiac saphenous vein bypass graft disease”. Semin Vasc Med. 4 (2): 153–9. doi:10.1055/s-2004-835373. PMID 15478036. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Yamada T, Itoh T, Nakano S, Tokunaga O (1995). “Time-dependent thickening of the intima in aortocoronary saphenous vein grafts: clinicopathological analysis of 24 patients”. Heart Vessels. 10 (1): 41–5. PMID 7730246.
|access-date=requires|url=(help) - ↑ Shi Y, Pieniek M, Fard A, O’Brien J, Mannion JD, Zalewski A (1996). “Adventitial remodeling after coronary arterial injury”. Circulation. 93 (2): 340–8. PMID 8548908. Retrieved 2010-07-23. Unknown parameter
|month=ignored (help) - ↑ Lau GT, Ridley LJ, Bannon PG, Wong LA, Trieu J, Brieger DB, Lowe HC, Freedman BS, Kritharides L (2006). “Lumen loss in the first year in saphenous vein grafts is predominantly a result of negative remodeling of the whole vessel rather than a result of changes in wall thickness”. Circulation. 114 (1 Suppl): I435–40. doi:10.1161/CIRCULATIONAHA.105.001008. PMID 16820615. Retrieved 2010-07-23. Unknown parameter
|month=ignored (help) - ↑ FitzGibbon GM, Leach AJ, Keon WJ, Burton JR, Kafka HP. Coronary bypass graft fate. J Thorac Cardiovasc Surg. 1986;91:773-778.
- ↑ Fitzgibbon GM, Kafka HP, Leach AJ, Keon WJ, Hooper GD, Burton JR. Coronary bypass graft fate and patient outcome. J AmColl Cardiol. 1996;28:616-626.
- ↑ Desai ND, Cohen EA, Naylor CD, Fremes SE; Radial Artery Patency Study Investigators. A randomized comparison of radial-artery and saphenous-vein coronary bypass grafts. N Engl JMed. 2004;351:2302-2309.
- ↑ Goldman S, Zadina K, Moritz T, et al. Long-term patency of saphenous vein and left internal mammary artery grafts after coronary artery bypass surgery. J Am Coll Cardiol. 2004;44:2149-2156.
- ↑ 17.0 17.1 17.2 Alexander JH, Hafley G, Harrington RA, Peterson ED, Ferguson TB, Lorenz TJ, Goyal A, Gibson M, Mack MJ, Gennevois D, Califf RM, Kouchoukos NT (2005). “Efficacy and safety of edifoligide, an E2F transcription factor decoy, for prevention of vein graft failure following coronary artery bypass graft surgery: PREVENT IV: a randomized controlled trial”. JAMA : the Journal of the American Medical Association. 294 (19): 2446–54. doi:10.1001/jama.294.19.2446. PMID 16287955. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Fuster V, Chesebro JH. Aorto-coronary artery vein graft disease: experimental and clinical approach for the understanding of the role of platelets and platelet inhibitors. Circulation 1985;72(Suppl. V):65—70.
- ↑ Fuster V, Chesebro JH. Role of platelets and platelet inhibitors in aortocoronary artery vein-graft disease. Circulation 1986;73:227—32.
- ↑ Fitzgibbon GM, Kafka HP, Leach AJ, Keon WJ, Hooper GD, Burton JR. Coronary bypass graft fate and patient outcome: angiographic follow-up of 5,065 grafts related to survival and reoperation in 1,388 patients during 25 years. J Am Coll Cardiol 1996;28:616—26.
- ↑ 21.0 21.1 21.2 Goldman S, Zadina K, Krasnicka B, Moritz T, Sethi G, Copeland J, Ovitt T, Henderson W (1997). “Predictors of graft patency 3 years after coronary artery bypass graft surgery. Department of Veterans Affairs Cooperative Study Group No. 297”. J. Am. Coll. Cardiol. 29 (7): 1563–8. PMID 9180120. Retrieved 2010-07-23. Unknown parameter
|month=ignored (help) - ↑ Kitamura S, Kawachi K, Kawata T, Kobayashi S, Mizuguchi K, Kameda Y, Nishioka H, Hamada Y, Yoshida Y. [Ten-year survival and cardiac event-free rates in Japanese patients with the left anterior descending artery revascularized with internal thoracic artery or saphenous vein graft: a comparative study] Nippon Geka Gakkai Zasshi. 1996 Mar;97(3):202-9. PMID 8649330.
- ↑ Arima M, Kanoh T, Suzuki T, Kuremoto K, Tanimoto K, Oigawa T, Matsuda S. Serial Angiographic Follow-up Beyond 10 Years After Coronary Artery Bypass Grafting. Circ J. 2005 Aug;69(8):896-902. PMID 16041156. [1].
- ↑ Yau JM, Alexander JH, Hafley G, Mahaffey KW, Mack MJ, Kouchoukos N, Goyal A, Peterson ED, Gibson CM, Califf RM, Harrington RA, Ferguson TB (2008). “Impact of perioperative myocardial infarction on angiographic and clinical outcomes following coronary artery bypass grafting (from PRoject of Ex-vivo Vein graft ENgineering via Transfection [PREVENT] IV)”. The American Journal of Cardiology. 102 (5): 546–51. doi:10.1016/j.amjcard.2008.04.069. PMID 18721510. Retrieved 2010-07-14. Unknown parameter
|month=ignored (help) - ↑
ref name=”pmid2680158″>Goldman S, Copeland J, Moritz T, Henderson W, Zadina K, Ovitt T, Doherty J, Read R, Chesler E, Sako Y (1989). “Saphenous vein graft patency 1 year after coronary artery bypass surgery and effects of antiplatelet therapy. Results of a Veterans Administration Cooperative Study”. Circulation. 80 (5): 1190–7. PMID 2680158. Retrieved 2010-07-22. Unknown parameter
|month=ignored (help) - ↑ Goldman S, Copeland J, Moritz T, Henderson W, Zadina K, Ovitt T, Doherty J, Read R, Chesler E, Sako Y (1988). “Improvement in early saphenous vein graft patency after coronary artery bypass surgery with antiplatelet therapy: results of a Veterans Administration Cooperative Study”. Circulation. 77 (6): 1324–32. PMID 3286040. Retrieved 2010-07-22. Unknown parameter
|month=ignored (help) - ↑ Goldman S, Copeland J, Moritz T, Henderson W, Zadina K, Ovitt T, Doherty J, Read R, Chesler E, Sako Y (1989). “Saphenous vein graft patency 1 year after coronary artery bypass surgery and effects of antiplatelet therapy. Results of a Veterans Administration Cooperative Study”. Circulation. 80 (5): 1190–7. PMID 2680158. Retrieved 2010-07-22. Unknown parameter
|month=ignored (help) - ↑ Goldman S, Copeland J, Moritz T, Henderson W, Zadina K, Ovitt T, Kern KB, Sethi G, Sharma GV, Khuri S (1994). “Long-term graft patency (3 years) after coronary artery surgery. Effects of aspirin: results of a VA Cooperative study”. Circulation. 89 (3): 1138–43. PMID 8124800. Retrieved 2010-07-22. Unknown parameter
|month=ignored (help) - ↑ Chesebro JH, Clements IP, Fuster V, Elveback LR, Smith HC, Bardsley WT, Frye RL, Holmes DR, Vlietstra RE, Pluth JR, Wallace RB, Puga FJ, Orszulak TA, Piehler JM, Schaff HV, Danielson GK (1982). “A platelet-inhibitor-drug trial in coronary-artery bypass operations: benefit of perioperative dipyridamole and aspirin therapy on early postoperative vein-graft patency”. N. Engl. J. Med. 307 (2): 73–8. PMID 7045659. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Chesebro JH, Fuster V, Elveback LR, Clements IP, Smith HC, Holmes DR, Bardsley WT, Pluth JR, Wallace RB, Puga FJ (1984). “Effect of dipyridamole and aspirin on late vein-graft patency after coronary bypass operations”. N. Engl. J. Med. 310 (4): 209–14. PMID 6361561. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Mangano DT (2002). “Aspirin and mortality from coronary bypass surgery”. N. Engl. J. Med. 347 (17): 1309–17. doi:10.1056/NEJMoa020798. PMID 12397188. Retrieved 2010-07-22. Unknown parameter
|month=ignored (help) - ↑ Lorenz RL, Schacky CV, Weber M; et al. (1984). “Improved aortocoronary bypass patency by low-dose aspirin (100 mg daily). Effects on platelet aggregation and thromboxane formation”. Lancet. 1 (8389): 1261–4. PMID 6144975. Unknown parameter
|month=ignored (help) - ↑ Hockings BE, Ireland MA, Gotch-Martin KF, Taylor RR (1993). “Placebo-controlled trial of enteric coated aspirin in coronary bypass graft patients. Effect on graft patency”. Med. J. Aust. 159 (6): 376–8. PMID 8377686. Unknown parameter
|month=ignored (help) - ↑ Sanz G, Pajarón A, Alegría E; et al. (1990). “Prevention of early aortocoronary bypass occlusion by low-dose aspirin and dipyridamole. Grupo Español para el Seguimiento del Injerto Coronario (GESIC)”. Circulation. 82 (3): 765–73. PMID 2203555. Unknown parameter
|month=ignored (help) - ↑ Gavaghan TP, Gebski V, Baron DW (1991). “Immediate postoperative aspirin improves vein graft patency early and late after coronary artery bypass graft surgery. A placebo-controlled, randomized study”. Circulation. 83 (5): 1526–33. PMID 2022014. Unknown parameter
|month=ignored (help) - ↑ Sharma GV, Khuri SF, Josa M, Folland ED, Parisi AF (1983). “The effect of antiplatelet therapy on saphenous vein coronary artery bypass graft patency”. Circulation. 68 (3 Pt 2): II218–21. PMID 6347428. Unknown parameter
|month=ignored (help) - ↑ Brown BG, Cukingnan RA, DeRouen T; et al. (1985). “Improved graft patency in patients treated with platelet-inhibiting therapy after coronary bypass surgery”. Circulation. 72 (1): 138–46. PMID 3874009. Unknown parameter
|month=ignored (help) - ↑ McEnany MT, Salzman EW, Mundth ED; et al. (1982). “The effect of antithrombotic therapy on patency rates of saphenous vein coronary artery bypass grafts”. J. Thorac. Cardiovasc. Surg. 83 (1): 81–9. PMID 7033673. Unknown parameter
|month=ignored (help) - ↑ Goldman S, Copeland J, Moritz T; et al. (1990). “Internal mammary artery and saphenous vein graft patency. Effects of aspirin”. Circulation. 82 (5 Suppl): IV237–42. PMID 2225410. Unknown parameter
|month=ignored (help) - ↑ Mehta RH, Hafley GE, Gibson CM, Harrington RA, Peterson ED, Mack MJ, Kouchoukos NT, Califf RM, Ferguson TB, Alexander JH (2008). “Influence of preoperative renal dysfunction on one-year bypass graft patency and two-year outcomes in patients undergoing coronary artery bypass surgery”. The Journal of Thoracic and Cardiovascular Surgery. 136 (5): 1149–55. doi:10.1016/j.jtcvs.2008.02.085. PMID 19026795. Retrieved 2010-07-14. Unknown parameter
|month=ignored (help) - ↑ Fitzgibbon GM, Kafka HP, Leach AJ, Keon WJ, Hooper GD, Burton JR (1996). “Coronary bypass graft fate and patient outcome: angiographic follow-up of 5,065 grafts related to survival and reoperation in 1,388 patients during 25 years”. J. Am. Coll. Cardiol. 28 (3): 616–26. PMID 8772748. Retrieved 2010-07-22. Unknown parameter
|month=ignored (help) - ↑ Marti MC, Bouchardy B, Cox JN. Aortocoronary bypass with autogenous saphenous vein grafts: histopathological aspects. Virchows Arch Abt A Path Anat 1971; 352: 255–66.
- ↑ Garrett HE, Dennis EW, DeBakey ME. Aortocoronary bypass with saphenous vein graft. JAMA 1973; 223: 792–4.
- ↑ Zemva A, Ferluga D, Zorc M, Popovic M, Porenta OV, Radovanovic N. Amyloidosis in saphenous vein aortocoronary bypass grafts. J Cardiovasc Surg 1990; 31: 441–4.
- ↑ Salerno TA, Wasan SM, Charrette EJ. Prospective analysis of heart biopsies in coronary artery surgery. Ann Thorac Surg 1979; 28: 436–9.
- ↑ Pelosi F, Capehart J, Roberts WC. Effectiveness of cardiac transplantation for primary (AL) cardiac amyloidosis. Am J Cardiol 1997; 79: 532–5.
Post-Operative Care and Complications
Postoperative Antiplatelet Therapy
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-in-Chief: Cafer Zorkun, M.D., Ph.D. [2], Mohammed A. Sbeih, M.D. [3]
Post-Operative Complications
Patients undergoing coronary artery bypass grafting are at risk for the same complications as any surgery. There are also additional risks associated specifically with CABG.
CABG Associated Complications
- Postperfusion syndrome (also known as “pumphead”), is a transient neurocognitive impairment associated with cardiopulmonary bypass. Some research demonstrates that the incidence is initially decreased by Off-pump coronary artery bypass, but no difference in neurocognitive function was observed beyond three months after surgery. A neurocognitive decline over time has been demonstrated in people with coronary artery disease regardless of treatment (OPCAB, conventional CABG or medical management). The neurocognitive decline has also been attributed to the administration of general anesthesia as part of the procedure.
- Nonunion of the sternum; internal thoracic artery (LIMA) harvesting devascularizes the sternum and may increase the risk.
- Myocardial infarction due to hypoperfusion, reperfusion injury, early graft occlusion due to thrombosis or technical failures at the anastomotic site, or graft failure. In the PREVENT IV study, perioperative MI was defined as a creatinine kinase-MB increase > or = 10 X the upper limit of normal or a > or = 5 X the upper limit of normal with the development of new 30-ms Q waves within 24 hours of surgery. Perioperative MI was observed in 9.8% of patients. Perioperative MI was associated with 1) longer surgery (250 vs 230 minutes; p <0.001), higher rates of on-pump surgery as compared with minimally invasive surgery (83% vs 78%; p = 0.048), and worse quality of target vessels (p <0.001). Perioperative MI was associated with more frequent angiography within 30 days of the procedure (1.7% vs 0.6%; p = 0.021) as well as higher rates of SVG failure at one year (62.4% vs 43.8%, p <0.001). Perioperative MI was associated with an increased risk of death, MI, or revascularization at two years(19.4% vs 15.2%; p = 0.039, multivariate hazard ratio 1.33, 95% confidence interval 1.00 to 1.76, p = 0.046) adjusting for differences in significant predictors. [1]
- Late graft stenosis, particularly of saphenous vein grafts due to atherosclerosis and excessive intimal hyperplasia causing recurrent angina or myocardial infarction.
- Acute renal failure due to hypoperfusion, embolization of debris from the aorta, and reperfusion injury. The incidence is approximately 3.6%. The mortality is approximately 20%. The length of hospitalization is prolonged from 4 days to 20 days in patients with post-operative renal failure.
- Stroke, secondary to aortic manipulation or hypoperfusion and reperfusion injury.
- Delirium may occur the postoperative period in 46% of patients:[2]
- Patients without postoperative delirium: cognition may take one yeaer to return to normal. At 6 months, 40% returned to their original cognition
- Patients with postoperative delirium: cognition returns to normal after one month. At 6 months, 24% returned to their original cognition
- Shunting due to SVG anastomosis into the great cardiac vein
General Surgical Complications
- Infection at incision sites or sepsis. Women, obese patients, and diabetic patients are at greater risk of this complication.
- Deep vein thrombosis (DVT)
- Anesthetic complications such as malignant hyperthermia.
- Keloid scarring
- Chronic pain at incision sites
- Chronic stress related illnesses
- Death
2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines[3]
Recommendations for Patients With Prior CABG Surgery With Stable Chest Pain
| Class I |
| 1.In patients who have had prior CABG surgery presenting with stable chest pain whose noninvasive stress test results show moderate to severe ischemia,1-7 or in those suspected to have myocardial ischemia with indeterminate/ non-diagnostic stress test, ICA is recommended for guiding therapeutic decision-making (Level of Evidence C-LD) |
| Class IIa |
| 1. In patients who have had prior CABG surgery presenting with stable chest pain who are suspected to have myocardial ischemia, it is reasonable to perform stress imaging or CCTA to evaluate for myocardial ischemia or graft stenosis or occlusion. (Level of Evidence: C-LD) |
2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery (DO NOT EDIT)[4]
Emotional Dysfunction and Psychosocial Considerations (DO NOT EDIT)[4]
| Class IIa |
| “1. Cognitive behavior therapy or collaborative care for patients with clinical depression after CABG can be beneficial to reduce objective measures of depression.[5][6][7][8][9] (Level of Evidence: B)” |
Cardiac Rehabilitation (DO NOT EDIT)[4]
| Class I |
| “1. Cardiac rehabilitation is recommended for all eligible patients after CABG.[10][11][12][13][14][15][16] (Level of Evidence: A)” |
Recommendations for duration of DAPT in patients undergoing CABG
| Class I |
| “1. In patients treated with DAPT after coronary stent implantation who subsequently undergo CABG, P2Y12 inhibitor therapy should be resumed postoperatively so that DAPT continues until the recommended duration of therapy is completed.(Level of Evidence: C-EO)” |
| “2. In patients with ACS (NSTE-ACS or STEMI) being treated with DAPT who undergo CABG, P2Y12 inhibitor therapy should be resumed after CABG to complete 12 months of DAPT therapy after ACS(Level of Evidence: C-LD)” |
| “3. In patients treated with DAPT, a daily aspirin dose of 81 mg (range, 75 mg to 100 mg) is recommended(Level of Evidence: B-NR)” |
| Class IIb |
| “1. In patients with SIHD, DAPT (with clopidogrel initiated early postoperatively) for 12 months after CABG may be reasonable to improve vein graft patency (Level of Evidence: B-NR)” |
Postoperative Antiplatelet Therapy (DO NOT EDIT)[4]
| Class I |
| “1. If aspirin (100 mg to 325 mg daily) was not initiated preoperatively, it should be initiated within 6 hours postoperatively and then continued indefinitely to reduce the occurrence of saphenous vein graft closure and adverse cardiovascular events.[17][18][19] (Level of Evidence: A)” |
| Class IIa |
| “1. For patients undergoing CABG, clopidogrel 75 mg daily is a reasonable alternative in patients who are intolerant of or allergic to aspirin. (Level of Evidence: C)” |
References
- ↑ Yau JM, Alexander JH, Hafley G, Mahaffey KW, Mack MJ, Kouchoukos N, Goyal A, Peterson ED, Gibson CM, Califf RM, Harrington RA, Ferguson TB (2008). “Impact of perioperative myocardial infarction on angiographic and clinical outcomes following coronary artery bypass grafting (from PRoject of Ex-vivo Vein graft ENgineering via Transfection [PREVENT] IV)”. The American Journal of Cardiology. 102 (5): 546–51. doi:10.1016/j.amjcard.2008.04.069. PMID 18721510. Retrieved 2010-07-14. Unknown parameter
|month=ignored (help) - ↑ Saczynski JS, Marcantonio ER, Quach L, Fong TG, Gross A, Inouye SK; et al. (2012). “Cognitive trajectories after postoperative delirium”. N Engl J Med. 367 (1): 30–9. doi:10.1056/NEJMoa1112923. PMID 22762316.
- ↑ Gulati M, Levy PD, Mukherjee D, Amsterdam E, Bhatt DL, Birtcher KK; et al. (2021). “2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines”. Circulation. 144 (22): e368–e454. doi:10.1161/CIR.0000000000001029. PMID 34709879 Check
|pmid=value (help). - ↑ 4.0 4.1 4.2 4.3 Hillis LD, Smith PK, Anderson JL, Bittl JA, Bridges CR, Byrne JG; et al. (2011). “2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines”. Circulation. 124 (23): e652–735. doi:10.1161/CIR.0b013e31823c074e. PMID 22064599.
- ↑ Blumenthal JA, Lett HS, Babyak MA, White W, Smith PK, Mark DB; et al. (2003). “Depression as a risk factor for mortality after coronary artery bypass surgery”. Lancet. 362 (9384): 604–9. doi:10.1016/S0140-6736(03)14190-6. PMID 12944059.
- ↑ Connerney I, Shapiro PA, McLaughlin JS, Bagiella E, Sloan RP (2001). “Relation between depression after coronary artery bypass surgery and 12-month outcome: a prospective study”. Lancet. 358 (9295): 1766–71. doi:10.1016/S0140-6736(01)06803-9. PMID 11734233.
- ↑ Freedland KE, Skala JA, Carney RM, Rubin EH, Lustman PJ, Dávila-Román VG; et al. (2009). “Treatment of depression after coronary artery bypass surgery: a randomized controlled trial”. Arch Gen Psychiatry. 66 (4): 387–96. doi:10.1001/archgenpsychiatry.2009.7. PMID 19349308.
- ↑ Rollman BL, Belnap BH, LeMenager MS, Mazumdar S, Houck PR, Counihan PJ; et al. (2009). “Telephone-delivered collaborative care for treating post-CABG depression: a randomized controlled trial”. JAMA. 302 (19): 2095–103. doi:10.1001/jama.2009.1670. PMC 3010227. PMID 19918088. Review in: Evid Based Nurs. 2010 Apr;13(2):37 Review in: Evid Based Med. 2010 Apr;15(2):57-8
- ↑ Rollman BL, Belnap BH, LeMenager MS, Mazumdar S, Schulberg HC, Reynolds CF (2009). “The Bypassing the Blues treatment protocol: stepped collaborative care for treating post-CABG depression”. Psychosom Med. 71 (2): 217–30. doi:10.1097/PSY.0b013e3181970c1c. PMID 19188529.
- ↑ Engblom E, Korpilahti K, Hämäläinen H, Rönnemaa T, Puukka P (1997). “Quality of life and return to work 5 years after coronary artery bypass surgery. Long-term results of cardiac rehabilitation”. J Cardiopulm Rehabil. 17 (1): 29–36. PMID 9041068.
- ↑ Hansen D, Dendale P, Leenders M, Berger J, Raskin A, Vaes J; et al. (2009). “Reduction of cardiovascular event rate: different effects of cardiac rehabilitation in CABG and PCI patients”. Acta Cardiol. 64 (5): 639–44. PMID 20058510.
- ↑ Milani RV, Lavie CJ (1998). “The effects of body composition changes to observed improvements in cardiopulmonary parameters after exercise training with cardiac rehabilitation”. Chest. 113 (3): 599–601. PMID 9515831.
- ↑ Taylor RS, Brown A, Ebrahim S, Jolliffe J, Noorani H, Rees K; et al. (2004). “Exercise-based rehabilitation for patients with coronary heart disease: systematic review and meta-analysis of randomized controlled trials”. Am J Med. 116 (10): 682–92. doi:10.1016/j.amjmed.2004.01.009. PMID 15121495. Review in: ACP J Club. 2004 Nov-Dec;141(3):62
- ↑ Clark AM, Hartling L, Vandermeer B, McAlister FA (2005). “Meta-analysis: secondary prevention programs for patients with coronary artery disease”. Ann Intern Med. 143 (9): 659–72. PMID 16263889. Review in: Evid Based Med. 2006 Jun;11(3):87 Review in: Evid Based Nurs. 2006 Jul;9(3):77
- ↑ Thomas RJ, King M, Lui K, Oldridge N, Piña IL, Spertus J; et al. (2007). “AACVPR/ACC/AHA 2007 performance measures on cardiac rehabilitation for referral to and delivery of cardiac rehabilitation/secondary prevention services”. Circulation. 116 (14): 1611–42. doi:10.1161/CIRCULATIONAHA.107.185734. PMID 17885210.
- ↑ Walther C, Möbius-Winkler S, Linke A, Bruegel M, Thiery J, Schuler G; et al. (2008). “Regular exercise training compared with percutaneous intervention leads to a reduction of inflammatory markers and cardiovascular events in patients with coronary artery disease”. Eur J Cardiovasc Prev Rehabil. 15 (1): 107–12. doi:10.1097/HJR.0b013e3282f29aa6. PMID 18277195.
- ↑ Mangano DT (2002). “Aspirin and mortality from coronary bypass surgery”. The New England Journal of Medicine. 347 (17): 1309–17. doi:10.1056/NEJMoa020798. PMID 12397188. Retrieved 2011-12-14. Unknown parameter
|month=ignored (help) - ↑ Sethi GK, Copeland JG, Goldman S, Moritz T, Zadina K, Henderson WG (1990). “Implications of preoperative administration of aspirin in patients undergoing coronary artery bypass grafting. Department of Veterans Affairs Cooperative Study on Antiplatelet Therapy”. Journal of the American College of Cardiology. 15 (1): 15–20. PMID 2404046. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ “Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients”. BMJ (Clinical Research Ed.). 324 (7329): 71–86. 2002. PMC 64503. PMID 11786451. Retrieved 2011-12-14. Unknown parameter
|month=ignored (help)
Special Scenarios
Special Scenarios
Anomalous Coronary Arteries | Chronic Obstructive Pulmonary Disease/Respiratory Insufficiency | Existing Renal Disease | Concomitant Valvular Disease | Previous Cardiac Surgery | Menopause | Carotid Disease Evaluation Before Surgery
Related Chapters
Related Chapters
External Links
External Links
- Advances in Cardiovascular Surgery and Cardiothoracic Surgical Procedures
- Cardiothoracic Surgery Notes an online interactive review developed by residents in cardiothoracic surgery
- Contenidos de Enfermería y Cirugía Cardiaca
- CTSNet: The Cardiothoracic Surgery Network
- Curso de Enfermería y Cirugía Cardiaca
- Heart Assist Devices
- LVAD Simulator
- Perfusion Line
- The CardioThoracic Surgery Network: Residents Section
- The Implantable Artificial Heart Project
- The Virtual Textbook Of Extracorporeal Technology
- Yale: Introduction to Cardiothoracic Imaging
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH