
Hemorrhagic stroke
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Sara Mehrsefat, M.D. [2]Tarek Nafee, M.D. [3]
Synonyms and keywords:
Overview
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sara Mehrsefat, M.D. [2]
Overview
Hippocrates (460 to 370 BC) was first to describe the phenomenon of sudden paralysis. In 1658, in his Apoplexia, Johann Jacob Wepfer (1620–1695) identified the cause of hemorrhagic stroke when he suggested that people who had died of apoplexy had bleeding in their brains.[1]
Historical perspective
- Hippocrates (460 to 370 BC) was first to describe the phenomenon of sudden paralysis.
- Apoplexy, from the Greek word meaning “struck down with violence,” first appeared in Hippocratic writings to describe this phenomenon.[1]
- As early as 1599, the word stroke was used as a synonym for apoplectic seizure and is a fairly literal translation of the Greek term.[2]
- In 1658, in his Apoplexia, Johann Jacob Wepfer (1620–1695) identified the cause of hemorrhagic stroke when he suggested that people who had died of apoplexy had bleeding in their brains.[1]
References
- ↑ 1.0 1.1 1.2 Thompson JE (1996). “The evolution of surgery for the treatment and prevention of stroke. The Willis Lecture”. Stroke. 27 (8): 1427–34. PMID 8711815.
- ↑ R. Barnhart, ed. The Barnhart Concise Dictionary of Etymology (1995)
Classification

Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sara Mehrsefat, M.D. [2]
Overview
There are two types of stroke, ischemic and hemorrhagic. Hemorrhagic strokes are less common, only 10-15% of all strokes are hemorrhagic, but they are responsible for about 40 percent of all stroke deaths.[1]
Based on location of the hemorrhage, hemorrhagic stroke may be classified into intracerebral hemorrhage (ICH) and subarachnoid hemorrhage (SAH)
Classification
Based on location of the hemorrhage, hemorrhagic stroke may be classified into:
| Stroke | |||||||||||||||||||||||||||||||||||||||||||||
| Ischemic stoke (85%) | Hemorrhagic stroke (15%) | ||||||||||||||||||||||||||||||||||||||||||||
| Aneurysmal SAH (4%) | Intracerebral hemorrhage (7%) | Others (4%) | |||||||||||||||||||||||||||||||||||||||||||
References
- ↑ Roger VL, Go AS, Lloyd-Jones DM, Adams RJ, Berry JD, Brown TM; et al. (2011). “Heart disease and stroke statistics–2011 update: a report from the American Heart Association”. Circulation. 123 (4): e18–e209. doi:10.1161/CIR.0b013e3182009701. PMC 4418670. PMID 21160056.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sara Mehrsefat, M.D. [2]
Overview
Pathophysiology
A hemorrhagic stroke, or cerebral hemorrhage, is a form of stroke that occurs when a blood vessel in the brain ruptures or bleeds. Like ischemic strokes, hemorrhagic strokes interrupt the brain’s blood supply because the bleeding vessel can no longer carry the blood to its target tissue. In addition, blood irritates brain tissue, disrupting the delicate chemical balance, and, if the bleeding continues, it can cause increased intracranial pressure which physically impinges on brain tissue and restricts blood flow into the brain. In this respect, hemorrhagic strokes are more dangerous than their more common counterpart, ischemic strokes. There are two types of hemorrhagic stroke: intracerebral hemorrhage, and subarachnoid hemorrhage. Amphetamine abuse quintuples, and cocaine abuse doubles, the risk of hemorrhagic strokes.
Intracerebral hemorrhage
The exact cause of brain damage following intracerebral hemorrhage is unknown. It is thought that ICH may result in brain injury by following mechanisms:[1][2]
- Neuronal ischemia following decreased blood flow to the area surrounding the clot
- Overexpression of matrix metalloproteinases (MMPs) which may result in the breakdown of the blood brain barrier and edema
Intraparenchymal hemorrhage
- High blood pressure and aging blood vessels are the most common causes of intracerebral hemorrhage (intraparenchymal hemorrhage).Hypertensive Intracerebral hemorrhage (ICH) usually results from spontaneous rupture of a small artery deep in the brain.[3][4] Breaks in the vessel wall usually occurs following chronic hypertension. Prolonged hypertentsion usually result in intimal hyperplasia and hyalinosis, which may result in focal necrosis and cause in vessel wall breaks. Massive hemorrhage may occur when the patients have a bleeding disorder and clotting system is unable to control the bleeding.[5]
- Intracerebral hemorrhage can also caused by an arteriovenous malformation (AVM). AVM occurs as a result of abnormal connection between arteries and veins in the brain and can result in vessels break and bleed into the brain.
- Additionally, In older people, an abnormal protein called amyloid may accumulate in arteries of the brain and result in amyloid antipathy. Cerebral amyloid angiopathy weakens the arteries and can cause hemorrhage.
Anatomical locations
The most common sites include:
- Basal ganglia (especially the putamen)
- Thalamus
- Cerebellum
- Pons
The small arteries in these areas seem more sensitive to hypertension and as a result, it may progress to vascular injury.
If intracerebral hemorrhage (ICH) occurs in other brain areas or in non hypertensive patients, the other causes of intracerebral hemorrhage should be considered such as:
- Neoplasms
- Hemorrhagic disorders
- Vascular malformations
- Cerebral amyloid angiopathy
Intraventricular hemorrhage
Intraventricular hemorrhage (IVH) can be:[6][7]
- Primary, confined to the ventricles
- Secondary, originating as an extension of an ICH
Most IVH is secondary and related to hypertensive hemorrhages involving the basal ganglia and thalamus.
Microbleeds
It is a clinically silent cerebral microbleeds directly into the brain tissue. It is thought that intimal hyperplasia and hyalinosis following hypertension and amyloid disposition may result in pseudoaneurysm formation and blood vessel leakage.[8][9]
Associated conditions
Anatomical locations
The microbleeds anatomical locations are varies with their etiology:[9]
- Hypertensive microbleeds
- Deep subcortical and infratentorial regions
- Amyloid microbleeds
- Superficial lobar regions of the cerebral hemispheres
Subarachnoid hemorrhage

Subarachnoid hemorrhage is considered a stroke when it occurs spontaneously (not result from external forces and head trauma).
A spontaneous hemorrhage in the brain usually results from:
- Sudden rupture of an aneurysm in an artery in the brain
- Congenital aneurysms
- Secondary to prolonged hypertension (occurs when an artery branches in a weakened area of artery’s wall)
- Rupture of an abnormal connection between arteries and veins (arteriovenous malformation AVM)
- Inflamed artery (Septic emboli) travels to an artery that supplies the brain, and causes inflammation and as a result the inflamed artery may weaken and rupture
Gross pathology
The following are images associated with gross pathology of cerebral hemorrhage:
-
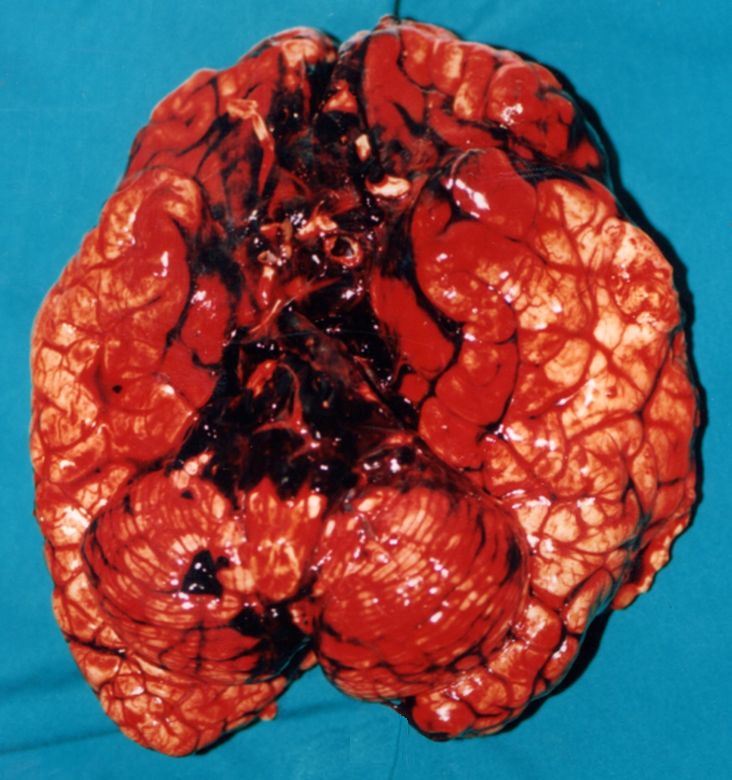 Cerebral hemorrhage
Cerebral hemorrhage -
 Intracerebral hemorrhage
Intracerebral hemorrhage -
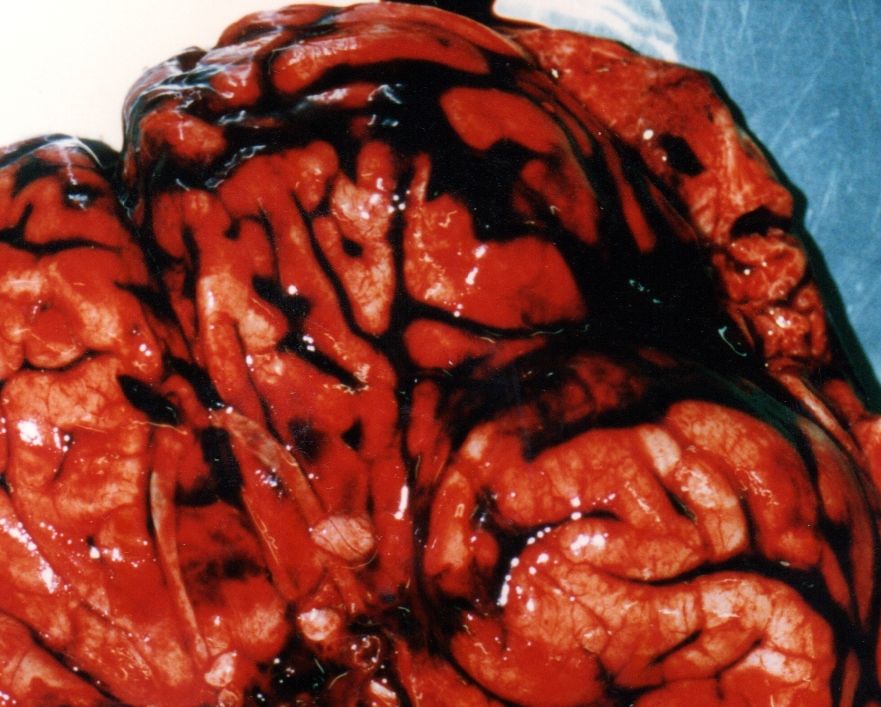 Subarachnoid hemorrhage gross pathology
Subarachnoid hemorrhage gross pathology



References
- ↑ Lee KR, Kawai N, Kim S, Sagher O, Hoff JT (1997). “Mechanisms of edema formation after intracerebral hemorrhage: effects of thrombin on cerebral blood flow, blood-brain barrier permeability, and cell survival in a rat model”. J Neurosurg. 86 (2): 272–8. doi:10.3171/jns.1997.86.2.0272. PMID 9010429.
- ↑ Mendelow AD (1993). “Mechanisms of ischemic brain damage with intracerebral hemorrhage”. Stroke. 24 (12 Suppl): I115–7, discussion I118-9. PMID 8249006.
- ↑ Folsom AR, Yatsuya H, Mosley TH, Psaty BM, Longstreth WT (2012). “Risk of intraparenchymal hemorrhage with magnetic resonance imaging-defined leukoaraiosis and brain infarcts”. Ann Neurol. 71 (4): 552–9. doi:10.1002/ana.22690. PMC 3377969. PMID 22522444.
- ↑ Delgado Almandoz JE, Schaefer PW, Goldstein JN, Rosand J, Lev MH, González RG; et al. (2010). “Practical scoring system for the identification of patients with intracerebral hemorrhage at highest risk of harboring an underlying vascular etiology: the Secondary Intracerebral Hemorrhage Score”. AJNR Am J Neuroradiol. 31 (9): 1653–60. doi:10.3174/ajnr.A2156. PMC 3682824. PMID 20581068.
- ↑ Garcia JH, Ho KL (1992). “Pathology of hypertensive arteriopathy”. Neurosurg Clin N Am. 3 (3): 497–507. PMID 1633473.
- ↑ Engelhard HH, Andrews CO, Slavin KV, Charbel FT. Current manage- ment of intraventricular hemorrhage. Surg Neurol. 2003;60:15–21.
- ↑ Huttner HB, Hartmann M, Köhrmann M, Neher M, Stippich C, Hähnel S, Kress B. Repeated digital substraction angiography after perimesencephalic subarachnoid hemorrhage? J Neuroradiol. 2006;33:87–89.
- ↑ Altmann-Schneider I, Trompet S, de Craen AJ, van Es AC, Jukema JW, Stott DJ; et al. (2011). “Cerebral microbleeds are predictive of mortality in the elderly”. Stroke. 42 (3): 638–44. doi:10.1161/STROKEAHA.110.595611. PMID 21233474.
- ↑ 9.0 9.1 Liu W, Liu R, Sun W, Peng Q, Zhang W, Xu E; et al. (2012). “Different impacts of blood pressure variability on the progression of cerebral microbleeds and white matter lesions”. Stroke. 43 (11): 2916–22. doi:10.1161/STROKEAHA.112.658369. PMID 22949472.
- ↑ Poels MM, Ikram MA, van der Lugt A, Hofman A, Krestin GP, Breteler MM; et al. (2011). “Incidence of cerebral microbleeds in the general population: the Rotterdam Scan Study”. Stroke. 42 (3): 656–61. doi:10.1161/STROKEAHA.110.607184. PMID 21307170.
- ↑ Klarenbeek P, van Oostenbrugge RJ, Rouhl RP, Knottnerus IL, Staals J (2013). “Higher ambulatory blood pressure relates to new cerebral microbleeds: 2-year follow-up study in lacunar stroke patients”. Stroke. 44 (4): 978–83. doi:10.1161/STROKEAHA.111.676619. PMID 23449261.
- ↑ Goos JD, Henneman WJ, Sluimer JD, Vrenken H, Sluimer IC, Barkhof F; et al. (2010). “Incidence of cerebral microbleeds: a longitudinal study in a memory clinic population”. Neurology. 74 (24): 1954–60. doi:10.1212/WNL.0b013e3181e396ea. PMID 20548041.
- ↑ Jeerakathil T, Wolf PA, Beiser A, Hald JK, Au R, Kase CS; et al. (2004). “Cerebral microbleeds: prevalence and associations with cardiovascular risk factors in the Framingham Study”. Stroke. 35 (8): 1831–5. doi:10.1161/01.STR.0000131809.35202.1b. PMID 15155954.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Causes
Intracerebral hemorrhage
The two major causes of intracerebral hemorrhage include:[1][2][3][4][5]
- Long-standing hypertension
- Hypertensive vasculopathy
- Cerebral amyloid angiopathy
Other causes of intracerebral hemorrhage include:[1][2][3][4][5]
- Vascular malformations
- Drugs
- Vasculitis
- Bleeding disorders
- Liver disease
- Anticoagulant medication
- Thrombolytic therapy
- Brain tumor
- Hemorrhagic transformation of an ischemic stroke
- Moyamoya disease
- Tumors
- Central nervous system (CNS) infection
Subarachnoid hemorrhage
Common causes of subarachnoid hemorrhage include:
- Arteriovenous malformation
- Brain tumor
- Drugs– Pergolide, Sumatriptan
- Fibromuscular dysplasia (FMD)
- Hemorrhagic diathesis
- Infections
- Leukemia
- Mycotic aneurysm
- Other aneurysms
- Connective tissue diseases
- Polycystic kidney disease
- Ruptured intracerebral aneurysm
Common locations based on casualty
| Cause | Common Location |
|---|---|
| Hypertensive hemorrhage |
|
| Arteriovenous malformation (AVM) | |
| Transformation of prior ischemic infarction |
|
| Aneurysm | |
| Drug |
|
| Coagulopathy[6] |
|
| Metastatic brain tumor |
|
| Amyloid angiopathy |
|
| Cavernous angioma |
|
| Head trauma |
|
| Capillary telangiectasias | |
| Dural arteriovenous fistula |
|
References
- ↑ 1.0 1.1 Meretoja A, Strbian D, Putaala J, Curtze S, Haapaniemi E, Mustanoja S; et al. (2012). “SMASH-U: a proposal for etiologic classification of intracerebral hemorrhage”. Stroke. 43 (10): 2592–7. doi:10.1161/STROKEAHA.112.661603. PMID 22858729.
- ↑ 2.0 2.1 Hart, Robert G., Bradley S. Boop, and David C. Anderson. “Oral anticoagulants and intracranial hemorrhage facts and hypotheses.” Stroke 26.8 (1995): 1471-1477.
- ↑ 3.0 3.1 Knudsen, Katherine A., et al. “Clinical diagnosis of cerebral amyloid angiopathy: validation of the Boston criteria.” Neurology 56.4 (2001): 537-539.
- ↑ 4.0 4.1 Lovelock, C. E., A. J. Molyneux, and P. M. Rothwell. “Change in incidence and aetiology of intracerebral haemorrhage in Oxfordshire, UK, between 1981 and 2006: a population-based study.” The Lancet Neurology 6.6 (2007): 487-493.
- ↑ 5.0 5.1 Rümke CL (1975). “Letter: Implications of the statement: No side effects were observed”. N Engl J Med. 292 (7): 372–3. PMID 1117973.
- ↑ Uglietta JP, O’Connor CM, Boyko OB, Aldrich H, Massey EW, Heinz ER (1991). “CT patterns of intracranial hemorrhage complicating thrombolytic therapy for acute myocardial infarction”. Radiology. 181 (2): 555–9. doi:10.1148/radiology.181.2.1924804. PMID 1924804.
Differentiating Stroke form other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Differential diagnosis
It is clinically difficult to distinguish an ICH from an ischemic stroke. However, the symptoms like headache, nausea, vomiting, and depressed level of consciousness should raise the suspicion for a hemorrhagic event compared to ischemic stroke.[1][2]
| Disease | Findings |
|---|---|
| Ischemic stroke |
|
| transient ischemic attack (TIA) |
|
| Acute hypertensive crisis/Malignant hypertension |
|
| Sentinel headache[3] |
|
| Sinusitis |
|
| Hypoglycemia |
|
| Pituitary apoplexy[4] |
|
| Cerebral venous thrombosis[5][6] |
|
| Colloid cyst of the third ventricle[7] |
|
| Cervical artery dissection[8][9] |
|
| Reversible cerebral vasoconstriction syndrome |
|
| Spontaneous intracranial hypotension[10][11] |
|
| Differential | Disease | Symptoms | Signs | Laboratory findings | Diagnostic modality | Management |
|---|---|---|---|---|---|---|
| Thunderclap headache | Sentinel headache[3] | Absent of focal neurologic symptoms and signs | Absent of focal neurologic signs | |||
| Pituitary apoplexy[4] | Acute headache
Change in mental status |
Decreased visual acuity | Brain CT and MRI are the preferred imaging techniques | |||
| Cerebral venous thrombosis[5][6] | – | Brain MRI with venography should be considered | ||||
| Colloid cyst of the third ventricle[7] | – | Head CT or MRI of the brain are usually diagnostic | ||||
| Cervical artery dissection[8][9] | – | Brain MRI with MRA and cranial CT with CTA) | ||||
| Reversible cerebral vasoconstriction syndrome | – | |||||
| Spontaneous intracranial hypotension[10][11] | Brain MRI is the preferred imaging techniques | |||||
| Stroke | Ischemic stroke | |||||
| transient ischemic attack (TIA) | ||||||
| Infection | Sinusitis | |||||
| Others | Hypoglycemia | Headache,
Loc Abnormal sensation Palpitations, sweating, dizziness |
Speech difficulty | Low blood glucose | ||
| Acute hypertensive crisis/Malignant hypertension | Urgent evaluation of serum creatinine, urinalysis, metabolic and cardiac evaluation (EKG, chest x ray, and cardiac enzymes) | Urgent evaluation with MRI and CT of the brain | ||||
| Brain tumor[12] | Headache Cachexia | Sensory and motor deficit, Gait abnormality and speech difficulty |
| Diseases | Diagnostic tests | Physical Examination | Symptoms | Past medical history | Other Findings | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Na+, K+, Ca2+ | CT /MRI | CSF Findings | Gold standard test | Motor Deficit | Sensory deficit | Speech difficulty | Gait abnormality | Cranial nerves | Headache | LOC | Motor weakness | Abnormal sensations | |||
| Brain tumour[12] | ✔ | Cancer cells[13] | MRI | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | Cachexia | |||||
| Hemorrhagic stroke | ✔ | Xanthochromia[14] | CT scan without contrast[15][16] | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | Hypertension | Neck stiffness | ||
| Subdural hemorrhage | ✔ | CT scan without contrast[15][16] | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | Trauma/fall | Confusion, dizziness, nausea, vomiting | |||
| Neurosyphilis[17][18] | ✔ | ↑ Leukocytes and protein | CSF VDRL-specifc
CSF FTA-Ab -sensitive[19] |
✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | STIs | Blindness, confusion, depression,
Abnormal gait | |||
| Complex or atypical migraine | Clinical assesment | ✔ | ✔ | ✔ | Family history of migraine | Presence of aura, nausea, vomiting | |||||||||
| Conversion disorder | Diagnosis of exclusion | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | Tremors, blindness, difficulty swallowing | |||||
| Electrolyte disturbance | ↓ or ↑ | Depends on the cause | Confusion, seizures | ||||||||||||
| Meningitis or encephalitis | ↑ Leukocytes,
↑ Protein ↓ Glucose |
CSF analysis[20] | ✔ | ✔ | Fever, neck
rigidity | ||||||||||
| Multiple sclerosis exacerbation | ✔ | ↑ CSF IgG levels
(monoclonal bands) |
Clinical assesment and MRI [21] | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | History of relapses and remissions | Blurry vision, urinary incontinence, fatigue | |||
| Seizure | ↓ or ↑ | Clinical assesment and EEG [22] | ✔ | ✔ | ✔ | ✔ | Previous history of seizures | Confusion, apathy, irritability, | |||||||
| Hypoglycemia or hyperglycemia | ↓ or ↑ | Serum blood glucose | ✔ | ✔ | ✔ | ✔ | ✔ | History of diabetes | Palpitations, sweating, dizziness | ||||||
Hemorrhagic stroke must be differentiated from other causes of headache, seizures and loss of consciousness.
| Diseases | Symptoms | Physical Examination | Past medical history | Diagnostic tests | Other Findings | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Headache | ↓LOC | Motor weakness | Abnormal sensory | Motor Deficit | Sensory deficit | Speech difficulty | Gait abnormality | Cranial nerves | CT /MRI | CSF Findings | Gold standard test | |||
| Meningitis | + | – | – | – | – | + | + | – | – | History of fever and malaise | – | ↑ Leukocytes,
↑ Protein ↓ Glucose |
CSF analysis[20] | Fever, neck |
| Encephalitis | + | + | +/- | +/- | – | – | + | +/- | + | History of fever and malaise | + | ↑ Leukocytes, ↓ Glucose | CSF PCR | Fever, seizures, focal neurologic abnormalities |
| Brain tumor[12] | + | – | – | – | + | + | + | – | + | Weight loss, fatigue | + | Cancer cells[13] | MRI | Cachexia, gradual progression of symptoms |
| Hemorrhagic stroke | + | + | + | + | + | + | + | + | – | Hypertension | + | – | CT scan without contrast[15][16] | Neck stiffness |
| Subdural hemorrhage | + | + | + | + | + | – | – | – | + | Trauma, fall | + | Xanthochromia[14] | CT scan without contrast[15][16] | Confusion, dizziness, nausea, vomiting |
| Neurosyphilis[17][18] | + | – | + | + | + | + | – | + | – | STIs | + | ↑ Leukocytes and protein | CSF VDRL-specifc
CSF FTA-Ab -sensitive[19] |
Blindness, confusion, depression,
Abnormal gait |
| Complex or atypical migraine | + | – | + | + | – | – | + | – | – | Family history of migraine | – | – | Clinical assesment | Presence of aura, nausea, vomiting |
| Hypertensive encephalopathy | + | + | – | – | – | – | + | + | – | Hypertension | + | – | Clinical assesment | Delirium, cortical blindness, cerebral edema, seizure |
| Wernicke’s encephalopathy | – | + | – | – | – | + | + | + | + | History of alcohal abuse | – | – | Clinical assesment and lab findings | Ophthalmoplegia, confusion |
| CNS abscess | + | + | – | – | + | + | + | – | – | History of drug abuse, endocarditis, immunosupression | + | ↑ leukocytes, ↓ glucose and ↑ protien | MRI is more sensitive and specific | High grade fever, fatigue,nausea, vomiting |
| Drug toxicity | – | + | – | + | + | + | – | + | – | – | – | – | Drug screen test | Lithium, Sedatives, phenytoin, carbamazepine |
| Conversion disorder | + | + | + | + | + | + | + | + | History of emotional stress | – | – | Diagnosis of exclusion | Tremors, blindness, difficulty swallowing | |
| Metabolic disturbances (electrolyte imbalance, hypoglycemia) | – | + | + | + | + | + | – | – | + | – | – | Hypoglycemia, hypo and hypernatremia, hypo and hyperkalemia | Depends on the cause | Confusion, seizure, palpitations, sweating, dizziness, hypoglycemia |
| Multiple sclerosis exacerbation | – | – | + | + | – | + | + | + | + | History of relapses and remissions | + | ↑ CSF IgG levels
(monoclonal bands) |
Clinical assesment and MRI [21] | Blurry vision, urinary incontinence, fatigue |
| Seizure | + | + | – | – | + | + | – | – | + | Previous history of seizures | – | Mass lesion | Clinical assesment and EEG [22] | Confusion, apathy, irritability, |
References
- ↑ Linn FH, Rinkel GJ, Algra A, van Gijn J (1998). “Headache characteristics in subarachnoid haemorrhage and benign thunderclap headache”. J Neurol Neurosurg Psychiatry. 65 (5): 791–3. PMC 2170334. PMID 9810961.
- ↑ Markus HS (1991). “A prospective follow up of thunderclap headache mimicking subarachnoid haemorrhage”. J Neurol Neurosurg Psychiatry. 54 (12): 1117–8. PMC 1014694. PMID 1783930.
- ↑ 3.0 3.1 Polmear A (2003). “Sentinel headaches in aneurysmal subarachnoid haemorrhage: what is the true incidence? A systematic review”. Cephalalgia. 23 (10): 935–41. PMID 14984225.
- ↑ 4.0 4.1 Dodick DW, Wijdicks EF (1998). “Pituitary apoplexy presenting as a thunderclap headache”. Neurology. 50 (5): 1510–1. PMID 9596029.
- ↑ 5.0 5.1 de Bruijn SF, Stam J, Kappelle LJ (1996). “Thunderclap headache as first symptom of cerebral venous sinus thrombosis. CVST Study Group”. Lancet. 348 (9042): 1623–5. PMID 8961993.
- ↑ 6.0 6.1 Bousser MG, Chiras J, Bories J, Castaigne P (1985). “Cerebral venous thrombosis–a review of 38 cases”. Stroke. 16 (2): 199–213. PMID 3975957.
- ↑ 7.0 7.1 KELLY R (1951). “Colloid cysts of the third ventricle; analysis of twenty-nine cases”. Brain. 74 (1): 23–65. PMID 14830663.
- ↑ 8.0 8.1 Mitsias P, Ramadan NM (1992). “Headache in ischemic cerebrovascular disease. Part I: Clinical features”. Cephalalgia. 12 (5): 269–74. PMID 1423556.
- ↑ 9.0 9.1 Touzé E, Gauvrit JY, Moulin T, Meder JF, Bracard S, Mas JL; et al. (2003). “Risk of stroke and recurrent dissection after a cervical artery dissection: a multicenter study”. Neurology. 61 (10): 1347–51. PMID 14638953.
- ↑ 10.0 10.1 Rando TA, Fishman RA (1992). “Spontaneous intracranial hypotension: report of two cases and review of the literature”. Neurology. 42 (3 Pt 1): 481–7. PMID 1549206.
- ↑ 11.0 11.1 Schievink WI, Wijdicks EF, Meyer FB, Sonntag VK (2001). “Spontaneous intracranial hypotension mimicking aneurysmal subarachnoid hemorrhage”. Neurosurgery. 48 (3): 513–6, discussion 516-7. PMID 11270540.
- ↑ 12.0 12.1 12.2 Morgenstern LB, Frankowski RF (1999). “Brain tumor masquerading as stroke”. J Neurooncol. 44 (1): 47–52. PMID 10582668.
- ↑ 13.0 13.1 Weston CL, Glantz MJ, Connor JR (2011). “Detection of cancer cells in the cerebrospinal fluid: current methods and future directions”. Fluids Barriers CNS. 8 (1): 14. doi:10.1186/2045-8118-8-14. PMC 3059292. PMID 21371327.
- ↑ 14.0 14.1 Lee MC, Heaney LM, Jacobson RL, Klassen AC (1975). “Cerebrospinal fluid in cerebral hemorrhage and infarction”. Stroke. 6 (6): 638–41. PMID 1198628.
- ↑ 15.0 15.1 15.2 15.3 Birenbaum D, Bancroft LW, Felsberg GJ (2011). “Imaging in acute stroke”. West J Emerg Med. 12 (1): 67–76. PMC 3088377. PMID 21694755.
- ↑ 16.0 16.1 16.2 16.3 DeLaPaz RL, Wippold FJ, Cornelius RS, Amin-Hanjani S, Angtuaco EJ, Broderick DF; et al. (2011). “ACR Appropriateness Criteria® on cerebrovascular disease”. J Am Coll Radiol. 8 (8): 532–8. doi:10.1016/j.jacr.2011.05.010. PMID 21807345.
- ↑ 17.0 17.1 Liu LL, Zheng WH, Tong ML, Liu GL, Zhang HL, Fu ZG; et al. (2012). “Ischemic stroke as a primary symptom of neurosyphilis among HIV-negative emergency patients”. J Neurol Sci. 317 (1–2): 35–9. doi:10.1016/j.jns.2012.03.003. PMID 22482824.
- ↑ 18.0 18.1 Berger JR, Dean D (2014). “Neurosyphilis”. Handb Clin Neurol. 121: 1461–72. doi:10.1016/B978-0-7020-4088-7.00098-5. PMID 24365430.
- ↑ 19.0 19.1 Ho EL, Marra CM (2012). “Treponemal tests for neurosyphilis–less accurate than what we thought?”. Sex Transm Dis. 39 (4): 298–9. doi:10.1097/OLQ.0b013e31824ee574. PMC 3746559. PMID 22421697.
- ↑ 20.0 20.1 Carbonnelle E (2009). “[Laboratory diagnosis of bacterial meningitis: usefulness of various tests for the determination of the etiological agent]”. Med Mal Infect. 39 (7–8): 581–605. doi:10.1016/j.medmal.2009.02.017. PMID 19398286.
- ↑ 21.0 21.1 Giang DW, Grow VM, Mooney C, Mushlin AI, Goodman AD, Mattson DH; et al. (1994). “Clinical diagnosis of multiple sclerosis. The impact of magnetic resonance imaging and ancillary testing. Rochester-Toronto Magnetic Resonance Study Group”. Arch Neurol. 51 (1): 61–6. PMID 8274111.
- ↑ 22.0 22.1 Manford M (2001). “Assessment and investigation of possible epileptic seizures”. J Neurol Neurosurg Psychiatry. 70 Suppl 2: II3–8. PMC 1765557. PMID 11385043.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sara Mehrsefat, M.D. [2]
Overview
In 2013, the prevalence of hemorrhagic stroke was estimated at 116.6 cases per 100,000 individuals.[1] Intracerebral hemorrhage (ICH) constitutes 10,000 to 15,000 cases per 100,000 individuals with all kind of strokes and has a higher risk of morbidity and mortality than cerebral infarction or subarachnoid hemorrhage.
| Epidemiology | Intracerebral hemorrhage | Subarachnoid hemorrhage |
|---|---|---|
| Incidence.[2][3] |
|
|
| Age[4][5] |
|
|
| Gender[5][6] |
|
|
| Race[7][8] |
|
|
| Case fatality rate[9][10] |
|
|
Epidemiology and demographics
Prevalence
In 2013, the prevalence of hemorrhagic stroke was estimated at 116.6 cases per 100,000 individuals.[1]
Incidence
In 2013, the age-adjusted incidence of hemorrhagic stroke was estimated 54.3 cases per 100,000 individuals.[1]
Intracerebral hemorrhage
- The overall incidence of intracerebral hemorrhage (ICH) ranges from 12 to 31 per 100,000 population.[2]
Subarachnoid hemorrhage
- The incidence of subarachnoid hemorrhage was estimated 10.5 per 100 000 person years.[3]
Age
Intracerebral hemorrhage
- The incidence of intracerebral hemorrhage (ICH) increases with age, after age 35 every 10 years, the risk of having ICH is getting doubled.[4]
- Primary lobar hemorrhages, due to cerebral amyloid angiopathy, are typically seen in elderly. Younger patients may also develop lobar hemorrhages, but in such cases they usually have an underlying lesion such as cerebral arteriovenous malformation (AVM).[11]
Subarachnoid hemorrhage
- Subarachnoid hemorrhage (SAH)usually occurs at a relatively young age
- The incidence of aneurysmal subarachnoid hemorrhage (aSAH) increases with age and commonly affects adults ≥50 years of age.[5]
Gender
Intracerebral hemorrhage
The prevalence and incidence of intracerebral hemorrhage does not vary by gender.[6]
Subarachnoid hemorrhage
- Women are slightly more affected with aneurysmal subarachnoid hemorrhage (SAH) than men (1.24 times higher than in men).[5][12]
Race
intracerebral hemorrhage
- The incidence of intracerebral hemorrhage is the highest in Asians, follow by blacks, and is the lowest in whites.
- In African Americans, the incidence of hemorrhagic stroke (intracerebral hemorrhage) is 48 cases per 100,000 persons.
- In whites, the incidence of hemorrhagic stroke (intracerebral hemorrhage) is 48 cases per 100,000 persons. [7]
- The incidence of Intracerebral hemorrhage is higher in Mexican Americans than non-Hispanic whites.[13]
Subarachnoid hemorrhage
- Subarachnoid hemorrhage usually affects individuals of African Americans populations.[8]
- The incidence of aneurysmal subarachnoid hemorrhage (SAH) is higher in Blacks and Hispanics compere to white Americans.
Geographic region
Subarachnoid hemorrhage (SAH)
- In the United States, the incidence of aneurysmal subarachnoid hemorrhage (SAH) is 10 to 15 cases per 100,000 population.[14]
- In China, the incidence of aneurysmal subarachnoid hemorrhage (SAH) is 2 cases per 100,000 population.[15]
- In South and Central America, the incidence of aneurysmal subarachnoid hemorrhage (SAH) is 4 cases per 100,000 population.[16]
- In Finland and Japan, the incidence of aneurysmal subarachnoid hemorrhage (SAH) is 19 to 23 cases per 100,000 population. [17]
Case fatality rate
intracerebral hemorrhage
- The 30-day case fatality rate of intracerebral hemorrhage (ICH) ranges from 37,000 to 52,000 cases per 100,000 individuals.[9][10]
- Death at 1 year for intracerebral hemorrhage (ICH) varies by hemorrhage location:[18]
- Brain steam 65,000 cases per 100,000 individuals
- Lobar ICH 57,000 cases per 100,000 individuals
- Deep ICH 50,000 cases per 100,000 individuals
- Cerebellar ICH 42,000 cases per 100,000 individuals
Subarachnoid hemorrhage
- The 30-day case fatality rate of subarachnoid hemorrhage (SAH) is 32,000 cases per 100,000 individuals.[19]
References
- ↑ 1.0 1.1 1.2 Global Burden of Disease Study 2013 Collaborators (2015). “Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013”. Lancet. 386 (9995): 743–800. doi:10.1016/S0140-6736(15)60692-4. PMC 4561509. PMID 26063472.
- ↑ 2.0 2.1 Gebel JM, Broderick JP (2000). “Intracerebral hemorrhage”. Neurol Clin. 18 (2): 419–38. PMID 10757834.
- ↑ 3.0 3.1 van Gijn J, Rinkel GJ (2001). “Subarachnoid haemorrhage: diagnosis, causes and management”. Brain. 124 (Pt 2): 249–78. PMID 11157554.
- ↑ 4.0 4.1 Stein M, Misselwitz B, Hamann GF, Scharbrodt W, Schummer DI, Oertel MF (2012). “Intracerebral hemorrhage in the very old: future demographic trends of an aging population”. Stroke. 43 (4): 1126–8. doi:10.1161/STROKEAHA.111.644716. PMID 22282880.
- ↑ 5.0 5.1 5.2 5.3 Rinkel GJ, Djibuti M, Algra A, van Gijn J (1998). “Prevalence and risk of rupture of intracranial aneurysms: a systematic review”. Stroke. 29 (1): 251–6. PMID 9445359.
- ↑ 6.0 6.1 van Asch CJ, Luitse MJ, Rinkel GJ, van der Tweel I, Algra A, Klijn CJ (2010). “Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis”. Lancet Neurol. 9 (2): 167–76. doi:10.1016/S1474-4422(09)70340-0. PMID 20056489.
- ↑ 7.0 7.1 Flaherty ML, Woo D, Haverbusch M, Sekar P, Khoury J, Sauerbeck L; et al. (2005). “Racial variations in location and risk of intracerebral hemorrhage”. Stroke. 36 (5): 934–7. doi:10.1161/01.STR.0000160756.72109.95. PMID 15790947.
- ↑ 8.0 8.1 Broderick JP, Brott T, Tomsick T, Huster G, Miller R (1992). “The risk of subarachnoid and intracerebral hemorrhages in blacks as compared with whites”. N Engl J Med. 326 (11): 733–6. doi:10.1056/NEJM199203123261103. PMID 1738378.
- ↑ 9.0 9.1 Dennis, Martin S., et al. “Long-term survival after first-ever stroke: the Oxfordshire Community Stroke Project.” Stroke 24.6 (1993): 796-800.
- ↑ 10.0 10.1 Kleindorfer D., Broderick J., Khoury J., et al: The unchanging incidence and case-fatality of stroke in the 1990s: a population-based study. Stroke 2006; 37: pp. 2473-2478
- ↑ Falcone GJ, Biffi A, Brouwers HB, Anderson CD, Battey TW, Ayres AM; et al. (2013). “Predictors of hematoma volume in deep and lobar supratentorial intracerebral hemorrhage”. JAMA Neurol. 70 (8): 988–94. doi:10.1001/jamaneurol.2013.98. PMC 3808840. PMID 23733000.
- ↑ de Rooij NK, Linn FH, van der Plas JA, Algra A, Rinkel GJ. Incidence of subarachnoid haemorrhage: a systematic review with emphasis on region, age, gender and time trends. J Neurol Neurosurg Psychiatry. 2007;78:1365–1372.
- ↑ Morgenstern LB, Smith MA, Lisabeth LD, Risser JM, Uchino K, Garcia N; et al. (2004). “Excess stroke in Mexican Americans compared with non-Hispanic Whites: the Brain Attack Surveillance in Corpus Christi Project”. Am J Epidemiol. 160 (4): 376–83. doi:10.1093/aje/kwh225. PMC 1524675. PMID 15286023.
- ↑ Shea AM, Reed SD, Curtis LH, Alexander MJ, Villani JJ, Schulman KA (2007). “Characteristics of nontraumatic subarachnoid hemorrhage in the United States in 2003”. Neurosurgery. 61 (6): 1131–7, discussion 1137-8. doi:10.1227/01.neu.0000306090.30517.ae. PMID 18162891.
- ↑ Ingall T, Asplund K, Mahonen M, Bonita R. A multinational com- parison of subarachnoid hemorrhage epidemiology in the WHO MONICA stroke study. Stroke. 2000;31:1054 –1061.
- ↑ de Rooij NK, Linn FH, van der Plas JA, Algra A, Rinkel GJ (2007). “Incidence of subarachnoid haemorrhage: a systematic review with emphasis on region, age, gender and time trends”. J Neurol Neurosurg Psychiatry. 78 (12): 1365–72. doi:10.1136/jnnp.2007.117655. PMC 2095631. PMID 17470467.
- ↑ Ingall T, Asplund K, Mähönen M, Bonita R (2000). “A multinational comparison of subarachnoid hemorrhage epidemiology in the WHO MONICA stroke study”. Stroke. 31 (5): 1054–61. PMID 10797165.
- ↑ Woo, Daniel, and Joseph P. Broderick. “Spontaneous intracerebral hemorrhage: epidemiology and clinical presentation.” Neurosurgery clinics of North America 13.3 (2002): 265-279.
- ↑ Feigin, Valery L., et al. “Stroke epidemiology: a review of population-based studies of incidence, prevalence, and case-fatality in the late 20th century.” The Lancet Neurology 2.1 (2003): 43-53.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Risk Factors
Intracerebral hemorrhage
Common risk factors in the development of intracerebral hemorrhage (ICH) include:[1][2][3]
- Anticoagulation medication
- Vitamin K antagonists (VKAs) such as warfarin
- Acquired or congenital coagulation factor disorders
- Vitamin K deficiency
- Liver disease
- Disseminated Intravascular Coagulation (DIC)
- Hemophilias
- Acquired qualitative or quantitative platelet abnormalities
- Embolic strokes
- Hypertension
- Sickle Cell Anemia
New anticoagulant medications such as dabigatran, rivaroxaban, and apixaban appear to be associated with a lower risk of ICH than VKAs. [4]
Subarachnoid hemorrhage
Common risk factors in the development of subarachnoid hemorrhage (SAH) include:[5][6][7][8][9]
- Positive family history
- Alcoholism
- Hypertension
- Smoking
- Heavy alcohol consumption
- Abnormal connective tissue
- Female gender
- African race
- Japanese or Finnish descent
References
- ↑ Huhtakangas J, Tetri S, Juvela S, Saloheimo P, Bode MK, Hillbom M. Effect of increased warfarin use on warfarin-related cerebral hemor- rhage: a longitudinal population-based study. Stroke. 2011;42:2431– 2435. doi: 10.1161/STROKEAHA.111.615260.
- ↑ Rådberg JA, Olsson JE, Rådberg CT. Prognostic parameters in sponta- neous intracerebral hematomas with special reference to anticoagulant treatment. Stroke. 1991;22:571–576. doi: 10.1161/01.STR.22.5.571.
- ↑ Flaherty ML, Kissela B, Woo D, Kleindorfer D, Alwell K, Sekar P, Moomaw CJ, Haverbusch M, Broderick JP. The increasing incidence of anticoagulant-associated intracerebral hemorrhage. Neurology. 2007;68:116–121. doi: 10.1212/01.wnl.0000250340.05202.8b.
- ↑ Chatterjee S, Sardar P, Biondi-Zoccai G, Kumbhani DJ. New oral anticoagulants and the risk of intracranial hemorrhage: traditional and Bayesian meta-analysis and mixed treatment comparison of random- ized trials of new oral anticoagulants in atrial fibrillation. JAMA Neurol. 2013;70:1486–1490. doi: 10.1001/jamaneurol.2013.4021
- ↑ van Gijn J, Rinkel GJ (2001). “Subarachnoid haemorrhage: diagnosis, causes and management”. Brain. 124 (Pt 2): 249–78. PMID 11157554.
- ↑ Bromberg JEC, Rinkel GJE, Algra A, Greebe P, van Duyn CM, Hasan D, et al. Subarachnoid haemorrhage in first and second degree relatives of patients with subarachnoid haemorrhage. BMJ 1995; 311: 288–9.
- ↑ Schievink, Wouter I., et al. “Saccular intracranial aneurysms in autosomal dominant polycystic kidney disease.” Journal of the American Society of Nephrology 3.1 (1992): 88-95.
- ↑ Van den Berg, J. S. P., M. Limburg, and R. C. M. Hennekam. “Is Marfan syndrome associated with symptomatic intracranial aneurysms?.” Stroke 27.1 (1996): 10-12
- ↑ Teunissen LL, Rinkel GJE, Algra A, van Gijn J. Risk factors for subarachnoid hemorrhage – a systematic review. Stroke 1996; 27: 544–9.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Natural history
In intracerebral hemorrhage (ICH), underlying small vessel disease may result in acute vessel rupture. This acute vessel rupture can progress can result in brain injury by folllowing mechanisms:
- The mass effect from the hematoma itself
- Activation of the coagulation cascade and release of inflammatory cytokines, and blood-brain barrier (BBB) disruption
All of these mechnisems can lead to perihematomal edema formation and secondary brain injury. Additionally, continued bleeding, or hematoma expansion, occurs in many patients—either continued bleeding from the primary source or secondary bleeding at the periphery of the hemorrhage.
Intracerebral hemorrhage also can result in dysphagia and aspiration. These two are the major risk factors for the development of pneumonia in patients with stroke.[1] Heart failure can occur as the result of myocardial ischemia, infarction, stress-induced cardiomyopathy, or uncontrolled hypertension in the setting of acute Intracerebral hemorrhage (ICH).[2][3]
Complications
The frequency of medical complications after acute stroke is high, although there is substantially more information reported for ischemic stroke than intracerebral hemorrhage (ICH).
The most common complications following intracerebral hemorrhage (ICH) include:[4][5][6]
- Hematoma expansion
- Venous thromboembolism (VTE)
- Pneumonia (5.6%)
- Aspiration (2.6%)
- Respiratory failure/distress (2%)
- Pulmonary embolism
- Sepsis
- Neurogenic pulmonary edema
- Acute respiratory distress syndrome
- Acute kidney injury, hyponatremia
- Gastrointestinal bleeding
- Impaired nutritional status
- Urinary tract infections
- Post- stroke depression
Approximately 50% of deaths after stroke are attributed to medical complications, usually after 7 days of hospitalization. Stroke patients who experience medical complications while in the hospital have increased mortality up to 4 years after the initial event.
Prognosis
Wide range of factors associated with outcome after acute hemorrhagic stroke. Identification of these factors result in the development of models to predict mortality and functional outcome. These prediction models include individual patient characteristics such as:[7][8][9][10]
- Score on the GCS
- Score on NIHSS
- Age
- Hematoma volume
- Hematoma location
- The presence and amount of IVH
Prognostic factors
Intracranial hemorrhage
- Despite aggressive and newer management strategies, the prognosis of patients with intracerebral hemorrhage is very poor. However, some studies suggested that excellent medical care has a direct impact on intracerebral hemorrhage (ICH) morbidity and mortality.[11]
- Case-fatality at 1 month is over 40 % and has not improved in last few decades.[12]
Prognsostic factors in Intracerebral hemorrhage include:[9]
| Poor prognostic factors | Associations |
|---|---|
| Fever[13] |
|
| Higher initial blood pressure[14] |
|
| Higher creatinine[15] |
|
| Higher serum glucose[14] |
|
| Warfarin-related hemorrhages[16][17] |
|
| Warfarin therapy with an INR >3[18] |
|
| Intraventricular hemorrhage[19][20] |
|
Subarachnoid hemorrhage
The Hunt and Hess scale describes the severity of subarachnoid hemorrhage, and is used as a predictor of survival.[21]
| Grading | Associations | Survival |
|---|---|---|
| Grade 1 |
|
|
| Grade 2 |
|
|
| Grade 3 |
|
|
| Grade 4 |
|
|
| Grade 5 |
|
|
2015 AHA/ASA Guidelines for the Management of Spontaneous Intracerebral Hemorrhage[22]
Outcome Prediction and Withdrawal of Technological Support: Recommendation
| Class III (Harm) |
| “1. Current prognostic models for individual patients early after ICH are biased by failure to account for the influence of withdrawal of support and early DNAR orders. DNAR status should not limit appropriate medical and surgical interventions unless otherwise explicitly indicated (Level of Evidence: C)” |
| Class IIa |
| “1. Aggressive care early after ICH onset and postponement of new DNAR orders until at least the second full day of hospitalization is probably recommended. Patients with preexisting DNAR orders are not included in this recommendation (Level of Evidence: B)” |
References
- ↑ Lyden PD, Shuaib A, Lees KR, Davalos A, Davis SM, Diener HC, Grotta JC, Ashwood TJ, Hardemark HG, Svensson HH, Rodichok L, Wasiewski WW, Ahlberg G; CHANT Trial Investigators. Safety and tolerability of NXY-059 for acute intracerebral hemorrhage: the CHANT Trial. Stroke. 2007;38:2262–2269. doi: 10.1161/STROKEAHA.106.472746.
- ↑ Gattringer T, Niederkorn K, Seyfang L, Seifert-Held T, Simmet N, Ferrari J; et al. (2014). “Myocardial infarction as a complication in acute stroke: results from the austrian stroke unit registry”. Cerebrovasc Dis. 37 (2): 147–52. doi:10.1159/000357799. PMID 24481543.
- ↑ Maramattom BV, Manno EM, Fulgham JR, Jaffe AS, Wijdicks EF (2006). “Clinical importance of cardiac troponin release and cardiac abnormalities in patients with supratentorial cerebral hemorrhages”. Mayo Clin Proc. 81 (2): 192–6. doi:10.4065/81.2.192. PMID 16471073.
- ↑ Elmer J, Hou P, Wilcox SR, Chang Y, Schreiber H, Okechukwu I; et al. (2013). “Acute respiratory distress syndrome after spontaneous intracerebral hemorrhage*”. Crit Care Med. 41 (8): 1992–2001. doi:10.1097/CCM.0b013e31828a3f4d. PMC 3752686. PMID 23760151.
- ↑ Oleinik A, Romero JM, Schwab K, Lev MH, Jhawar N, Delgado Almandoz JE; et al. (2009). “CT angiography for intracerebral hemorrhage does not increase risk of acute nephropathy”. Stroke. 40 (7): 2393–7. doi:10.1161/STROKEAHA.108.546127. PMC 2726774. PMID 19461032.
- ↑ Malhotra A (2007). “Low-tidal-volume ventilation in the acute respiratory distress syndrome”. N Engl J Med. 357 (11): 1113–20. doi:10.1056/NEJMct074213. PMC 2287190. PMID 17855672.
- ↑ Bernstein RA, Hemphill JC. Critical care of acute ischemic stroke. Curr Neurol Neurosci Rep. 2001;1:587–592.
- ↑ Rost NS, Smith EE, Chang Y, Snider RW, Chanderraj R, Schwab K, FitzMaurice E, Wendell L, Goldstein JN, Greenberg SM, Rosand J. Prediction of functional outcome in patients with primary intracerebral hemorrhage: the FUNC score. Stroke. 2008;39:2304–2309. doi: 10.1161/ STROKEAHA.107.512202
- ↑ 9.0 9.1 Tuhrim S, Horowitz DR, Sacher M, Godbold JH. Volume of ventricular blood is an important determinant of outcome in supratentorial intracere- bral hemorrhage. Crit Care Med. 1999;27:617–621.
- ↑ Broderick JP, Brott TG, Duldner JE, Tomsick T, Huster G. Volume of intracerebral hemorrhage: a powerful and easy-to-use predictor of 30-day mortality. Stroke. 1993;24:987–993.
- ↑ Hemphill JC, Newman J, Zhao S, Johnston SC (2004). “Hospital usage of early do-not-resuscitate orders and outcome after intracerebral hemorrhage”. Stroke. 35 (5): 1130–4. doi:10.1161/01.STR.0000125858.71051.ca. PMID 15044768.
- ↑ Apanasenko BG, Kunitsyn AI, Isaev GA, Khodyrev LP (1976). “[Determination of the weight of disemulsified lipid circulating in the blood as a method of diagnosis of fat embolism]”. Lab Delo (1): 41–3. PMID 0056489.
- ↑ Leira R, Dávalos A, Silva Y, Gil-Peralta A, Tejada J, Garcia M; et al. (2004). “Early neurologic deterioration in intracerebral hemorrhage: predictors and associated factors”. Neurology. 63 (3): 461–7. PMID 15304576.
- ↑ 14.0 14.1 Sawyer GJ, Fabre JW (1997). “Indirect T-cell allorecognition and the mechanisms of immunosuppression by allogeneic blood transfusions”. Transpl Int. 10 (4): 276–83. PMID 9249937.
- ↑ Miller CM, Vespa PM, McArthur DL, Hirt D, Etchepare M (2007). “Frameless stereotactic aspiration and thrombolysis of deep intracerebral hemorrhage is associated with reduced levels of extracellular cerebral glutamate and unchanged lactate pyruvate ratios”. Neurocrit Care. 6 (1): 22–9. doi:10.1385/NCC:6:1:22. PMID 17356187.
- ↑ Cucchiara B, Messe S, Sansing L, Kasner S, Lyden P, CHANT Investigators (2008). “Hematoma growth in oral anticoagulant related intracerebral hemorrhage”. Stroke. 39 (11): 2993–6. doi:10.1161/STROKEAHA.108.520668. PMID 18703803.
- ↑ Broderick JP, Diringer MN, Hill MD, Brun NC, Mayer SA, Steiner T; et al. (2007). “Determinants of intracerebral hemorrhage growth: an exploratory analysis”. Stroke. 38 (3): 1072–5. doi:10.1161/01.STR.0000258078.35316.30. PMID 17290026.
- ↑ Flaherty ML, Tao H, Haverbusch M, Sekar P, Kleindorfer D, Kissela B; et al. (2008). “Warfarin use leads to larger intracerebral hematomas”. Neurology. 71 (14): 1084–9. doi:10.1212/01.wnl.0000326895.58992.27. PMC 2668872. PMID 18824672.
- ↑ Bhattathiri PS, Gregson B, Prasad KS, Mendelow AD; STICH Investigators. Intraventricular hemorrhage and hydrocephalus after spon- taneous intracerebral hemorrhage: results from the STICH trial. Acta Neurochir Suppl. 2006;96:65–68.
- ↑ Hallevi H, Albright KC, Aronowski J, Barreto AD, Martin-Schild S, Khaja AM, Gonzales NR, Illoh K, Noser EA, Grotta JC. Intraventricular hemorrhage: anatomic relationships and clinical implications. Neurology. 2008;70:848–852. doi: 10.1212/01.wnl.0000304930.47751.75.
- ↑ Hunt WE, Hess RM (1968). “Surgical risk as related to time of intervention in the repair of intracranial aneurysms”. J Neurosurg. 28 (1): 14–20. doi:10.3171/jns.1968.28.1.0014. PMID 5635959.
- ↑ 2015 AHA/ASA Guidelines for the Management of Spontaneous Intracerebral Hemorrhage http://stroke.ahajournals.org/content/early/2015/05/28/STR.0000000000000069 Accessed on November 10, 2016
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | CT | MRI | Echocardiography | Ultrasound | Other Imaging Findings
Treatment
Treatment
Early assessment | Medical Therapy | Surgery | Rehabilitation | Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
AHA/ASA Guideline Recommendations For Prevention of Stroke in Women (2014)
AHA/ASA Guideline Recommendations For Prevention of Stroke in Women (2014)
Risk Factors
Sex-Specific Risk Factors
Pregnancy and Complications | Cerebral Venous Thrombosis | Oral Contraceptives | Menopause and Postmenopausal Hormonal Therapy
Risk Factors Commoner Among Women
Migraine with Aura | Obesity, Metabolic Syndrome, and Lifestyle Factors | Atrial Fibrillation
Case Studies
Case Studies
ar:سكتة zh-min-nan:Tiòng-hong ca:Accident vascular cerebral de:Schlaganfall da:Apopleksi el:Εγκεφαλικό επεισόδιο eo:Apopleksio ko:뇌경색 hr:Moždani udar io:Vaskulala cerebrala stroko id:Stroke is:Heilablóðfall it:Ictus he:שבץ מוחי la:Ictus (morbus) hu:Agyvérzés mk:Мозочен удар ms:Angin ahmar nl:Beroerte no:Hjerneslag sl:Možganska kap fi:Aivoverenkiertohäiriö sv:Slaganfall
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH