
Hepatitis C pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Yazan Daaboul, Serge Korjian, Seyedmahdi Pahlavani, M.D. [2], Javaria Anwer M.D.[3]
Overview
Overview
In isolated acute HCV infection, the host immune system stimulates the secretion of interferon alpha and the activation of natural killer cells, which is followed by the activation of the adaptive immune system. Chronic HCV is characterized by the impairment of these mechanisms. Eventually, chronic HCV infection leads to local inflammation and fibrogenesis, which cause hepatic injury and cirrhosis. Hepatocellular carcinoma, a known complication of chronic HCV infection, arises in cases of cirrhosis; the role of oncogenic proteins of HCV in the pathogenesis of hepatocellular carcinoma has yet to be elucidated.
Transmission
Transmission
The transmission of HCV can be defined as percutaneous, sexual, healthcare-associated, or maternal-infant in nature.
Percutaneous Transmission
- Blood and blood components transfusion
- More than 90% of seronegative recipients who are transfused with blood from HCV-antibody positive donors will acquire infection.[1]
- Contaminated shared needles among intravenous drug users
- Before 1992, at least two-thirds of new HCV infections in the United States were associated with illicit drug use; the number has since decreased significantly.[2]
- Chronic hemodialysis
- The frequency of anti-HCV in patients on hemodialysis ranges from less than 10% in the United States to 55% to 85% in Jordan, Saudi Arabia, and Iran.[3]
Sexual Transmission
- HCV RNA has been detected in semen and saliva.[4] People with multiple sexual partners and commercial sex workers have a high HCV prevalence.[5]
Health care Associated
- Nosocomial transmission has been observed under several different conditions (e.g. needle stick, organ transplant, during surgery); now, however, because of infection control protocols, nosocomial transmission of HCV is rare except in cases of breach of protocols.[6][7]
Maternal Infant Transmission
HCV Clearance and Persistence
HCV Clearance and Persistence
Acute viral infection and HCV replication triggers the activation of host immune responses, first by secretion of type I interferon alpha (IFN-alpha) and activation of natural killer (NK) cells. Nonetheless, secretion of endogenous IFN does not seem to effectively inhibit HCV replication.[10][11][12]
HCV proteins play a crucial role in inhibiting IFN-alpha effectors, such as IFN regulatory factor-3 (IRF-3), double stranded RNA-dependent protein kinase (PKR), and the JAK-STAT signaling pathway.[13][14][15] More importantly, chronic carriage of HCV is associated with impaired activation of NK cells despite IFN-alpha secretion. It is believed that the cross-linking of CD81 and the envelope protein E2 of the virus is a key mechanism by which NK cells are inactivated and INF-gamma is not produced by these cells.[16]
The activation of IFN-gamma is a prerequisite for the appropriate clearance of HCV. When activation occurs normally, antibodies start to form 7-31 weeks later.[17][18][19][20] While most epitopes for antibodies have not been discovered yet, hypervariable region 1 (HVR1) of the E2 envelope glycoprotein was found to be a target for anti-HVR1 antibodies. Antibodies play a role in clearing the virus from the host. It is currently unknown whether “escape” mechanisms are present in HCV that favor persistent HCV infection despite an adequate antibody response.[17][18][19][20]
Similarly, the activation of the CD4+ and CD8+ T-cell response is required for viral clearance. This cellular response allows for the development of long-term immunity against HCV.[21] Studies also proved that delayed or inadequate activation of T-cell response is associated with persistence of infection. It is not known why T-cell response may fail in response to acute infection, but it is hypothesized that persistence might be related to viral inhibition of T-cell maturation, defective dendritic cells, and/or failure of interleukin (IL) 12 activation.[21][22][23][24][25][26]
Liver Injury and Cirrhosis, and Hepatocellular Carcinoma
Liver Injury and Cirrhosis, and Hepatocellular Carcinoma
HCV is directly associated with hepatic steatosis, which is fat accumulation in the liver. It seems that core proteins may play a role in regulating lipid accumulation in hepatocytes, contributing to steatosis. However, steatosis is not observed in all genotypes of HCV infection; it is classically described in genotype 3, which perhaps is the only genotype that has a direct role in the development of steatosis irrespective of alcohol consumption or metabolic elements. Apart from steatosis, HCV per se has not been shown to have damaging effects on hepatocytes. The viral burden also does not seem to be directly related to the extent of liver injury.[27][28][29][30][31][32][33]
In chronic hepatitis C infections, the local immune response leads to portal lymphoid infiltration and chronic inflammation, which give way to bridging necrosis and degenerative lobular lesions.[16] Hepatic injury is directly associated with the degree of Th1 cytokine expression. The adaptive immune system, namely the cytotoxic T-cell response, injures infected cells as well as bystander cells. Nonetheless, it has not been confirmed whether the number of cytotoxic T cells is associated with the extent of liver injury.
Chronic inflammation ultimately leads to fibrogenesis due to deposition extracellular matrix elements in hepatic parenchyma. It is unknown whether viral components are directly responsible in the particular mechanism of hepatic cirrhosis in chronic HCV infection; although cirrhosis is definitely worsened in HCV patients who are also exposed to other risk factors, such as alcohol, obesity, and HIV.[16]
Hepatocellular Carcinoma
Hepatocellular Carcinoma
Hepatocellular carcinoma (HCC) occurs following chronic HCV infection complicated by liver cirrhosis. The precise role of HCV components in the development of HCC is poorly understood. Pinpointing which viral protein is directly related to carcinogenesis has been difficult, but studies have shown that NS3, NS4B, and NS5A all have oncogenic properties.[34][35][36][37][38]
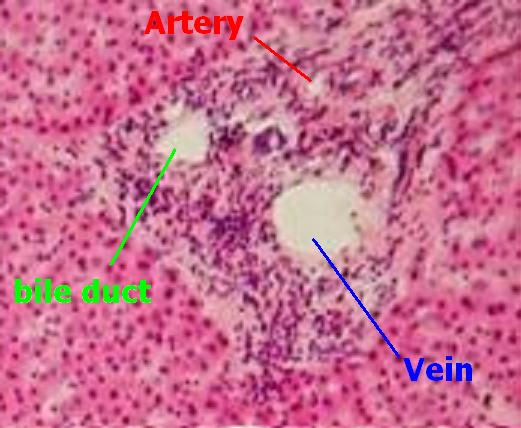
Histology
Histology
Click on the arrow to view the pathologic findings in viral hepatitis: {{#ev:youtube|_hXvbpSxFZw}}
Mechanisms involved in extra-hepatic manifestations
Mechanisms involved in extra-hepatic manifestations
- Cryoglobulinemic vasculitis: Chronic antigen stimulation reduces the threshold for activation and proliferation of B-lymphocyte and induces Bcl-2 activation and t(14;18) translocation. It results in decreased apoptosis. As a result, CD21−CD27+ cells produce antibodies against the Fc portion of IgG, forming immune complexes that precipitate in small blood vessels.[39]
- B-cell lymphoma: A continuous HCV antigen stimulation and permanent genetic damage caused by viral proteins cause clonal proliferation of CD21−CD27+. It also down-regulates tumor-suppressive signals (such as, microRNA-26b). Oncogenic signals are further enhanced and additional tumor suppressor genes such as Bcl-6, p53, and β-catenin undergo mutation. Hence, the reduced levels of caspase 3, 7, and 9 reduce their sensitivity to Fas-induced apoptosis.[39]
- Cardiovascular disease: Local vascular damage is caused by an increased expression of adhesion molecules on endothelial surface. Smooth cells in the media proliferate and apoptosis is inhibited, with local macrophages producing proinflammatory cytokines and free radicals. These processes result in accelerated atherosclerosis, procoagulant effects, and lead to major cardiovascular events.[39]
- Chronic kidney disease: Direct HCV cytopathic effect, chronic inflammation from atherosclerosis and insulin resistance, endothelial and mesangial inflammation, and podocyte and tubular injury caise CKD. Cryoprecipitates deposit at glomeruli also manifested as type I membranoproliferative glomerulonephritis.[39]
- Type 2 diabetes: Caused by both hepatic and peripheral insulin resistance. In the liver, HCV leads to PI3K-AKT insulin-signaling pathway reduction via insulin receptor substrate 1 inhibition and impaired Glut2–mediated hepatic glucose intake. In the extrahepatic tissue, insulin resistance is a consequence of soluble endocrine mediators released by hepatocytes. Up-regulation of TNF, G6P, and resistin, with an imbalance in the adipocytokine profile, increases gluconeogenesis in these sites.[39]
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
The liver is an organ present in vertebrates and some other animals. It plays a major role in metabolism and has a number of functions in the body, including glycogen storage, decomposition of red blood cells, plasma protein synthesis, and detoxification. This organ also is the largest gland in the human body. It lies below the diaphragm in the thoracic region of the abdomen.[1] It produces bile, an alkaline compound which aids in digestion, via the emulsification of lipids. It also performs and regulates a wide variety of high-volume biochemical reactions requiring very specialized tissues.
Medical terms related to the liver often start in hepato- or hepatic from the Greek word for liver, hēpar (ήπαρ).[2]
Anatomy
The adult human liver normally weighs between 1.4 – 1.6 kilograms (3.1 – 3.5 pounds),[3] and it is a soft, pinkish-brown “boomerang shaped” organ. It is the second largest organ (the largest organ being the skin) and the largest gland within the human body. It is located on the right side of the upper abdomen below the diaphragm. The liver lies to the right of the stomach and overlies the gallbladder (which stores bile).
Flow of blood
The splenic vein joins the inferior mesenteric vein, which then together join with the superior mesenteric vein to form the hepatic portal vein, bringing veneous blood from the spleen, pancreas, stomach, small intestine, and large intestine, so that the liver can process the nutrients and byproducts of food digestion.
The hepatic veins of the blood can be from other branches such as the superior mesenteric artery.
Both the portal venules & the hepatic arterioles enter approximately one million identical lobules acini, likened to and changes in the size of chylomicrons lipoproteins of dietary origin brought about by the quantity & types of food fats.
Approximately 60% to 80% of the blood flow to the liver is from the portal venous system, and 1/4 is from the hepatic artery.
Flow of bile

The bile produced in the liver is collected in bile canaliculi, which merge to form bile ducts.
These eventually drain into the right and left hepatic ducts, which in turn merge to form the common hepatic duct. The cystic duct (from the gallbladder) joins with the common hepatic duct to form the common bile duct.
Bile can either drain directly into the duodenum via the common bile duct or be temporarily stored in the gallbladder via the cystic duct. The common bile duct and the pancreatic duct enter the duodenum together at the ampulla of Vater.
The branchings of the bile ducts resemble those of a tree, and indeed the term “biliary tree” is commonly used in this setting.
Regeneration
The liver is among the few internal human organs capable of natural regeneration of lost tissue; as little as 25% of remaining liver can regenerate into a whole liver again.
This is predominantly due to the hepatocytes acting as unipotential stem cells (i.e. a single hepatocyte can divide into two hepatocyte daughter cells). There is also some evidence of bipotential stem cells, called ovalocyte(o´və-lo-sīt), which exist in the Canals of Hering. These cells can differentiate into either hepatocytes or cholangiocytes (cells that line the bile ducts).
Traditional (Surface) anatomy
Peritoneal ligaments
Apart from a patch where it connects to the diaphragm, the liver is covered entirely by visceral peritoneum, a thin, double-layered membrane that reduces friction against other organs. The peritoneum folds back on itself to form the falciform ligament and the right and left triangular ligaments.
These “ligaments” are in no way related to the true anatomic ligaments in joints, and have essentially no functional importance, but they are easily recognizable surface landmarks.
Lobes
Traditional gross anatomy divided the liver into four lobes based on surface features.
The falciform ligament is visible on the front (anterior side) of the liver. This divides the liver into a left anatomical lobe, and a right anatomical lobe.
If the liver flipped over, to look at it from behind (the visceral surface), there are two additional lobes between the right and left. These are the caudate lobe (the more superior), and below this the quadrate lobe.
From behind, the lobes are divided up by the ligamentum venosum and ligamentum teres (anything left of these is the left lobe), the transverse fissure (or porta hepatis) divides the caudate from the quadrate lobe, and the right sagittal fossa, which the inferior vena cava runs over, separates these two lobes from the right lobe.
Each of the lobes is made up of lobules, a vein goes from the centre of each lobule which then joins to the hepatic vein to carry blood out from the liver.
On the surface of the lobules there are ducts, veins and arteries that carry fluids to and from them.
Modern (Functional) anatomy
The central area where the common bile duct, hepatic portal vein, and hepatic artery enter the liver is the hilum or “porta hepatis“. The duct, vein, and artery divide into left and right branches, and the portions of the liver supplied by these branches constitute the functional left and right lobes.
The functional lobes are separated by a plane joining the gallbladder fossa to the inferior vena cava. This separates the liver into the true right and left lobes. The middle hepatic vein also demarcates the true right and left lobes. The right lobe is further divided into an anterior and posterior segment by the right hepatic vein. The left lobe is divided into the medial and lateral segments by the left hepatic vein. The fissure for the ligamentum teres (the ligamentum teres becomes the falciform ligament) also separates the medial and lateral segments. The medial segment is what used to be called the quadrate lobe. In the widely used Couinaud or “French” system, the functional lobes are further divided into a total of eight subsegments based on a transverse plane through the bifurcation of the main portal vein. The caudate lobe is a separate structure which receives blood flow from both the right- and left-sided vascular branches.[4][5] The subsegments corresponding to the anatomical lobes are as follows:
| Segment* | Couinaud segments |
|---|---|
| Caudate | 1 |
| Lateral | 2, 3 |
| Medial | 4a, 4b |
| Right | 5, 6, 7, 8 |
- or lobe in the Caudate’s case.
Each number in the list corresponds to one in the table.
- Caudate
- Superior subsegment of the lateral segment
- Inferior subsegment of the lateral segment
- Superior subsegment of the medial segment
- Inferior subsegment of the medial segment
- Inferior subsegment of the anterior segment
- Inferior subsegment of the posterior segment
- Superior subsegment of the posterior segment
- Superior subsegment of the anterior segment
Physiology
The various functions of the liver are carried out by the liver cells or hepatocytes.
- The liver produces and excretes bile (a greenish liquid) required for emulsifying fats. Some of the bile drains directly into the duodenum, and some is stored in the gallbladder.
- The liver performs several roles in carbohydrate metabolism:
- Gluconeogenesis (the synthesis of glucose from certain amino acids, lactate or glycerol)
- Glycogenolysis (the breakdown of glycogen into glucose) (muscle tissues can also do this)
- Glycogenesis (the formation of glycogen from glucose)
- The breakdown of insulin and other hormones
- The liver is responsible for the mainstay of protein metabolism.
- The liver also performs several roles in lipid metabolism:
- Cholesterol synthesis
- The production of triglycerides (fats).
- The liver produces coagulation factors I (fibrinogen), II (prothrombin), V, VII, IX, X and XI, as well as protein C, protein S and antithrombin.
- The liver breaks down haemoglobin, creating metabolites that are added to bile as pigment (bilirubin and biliverdin).
- The liver breaks down toxic substances and most medicinal products in a process called drug metabolism. This sometimes results in toxication, when the metabolite is more toxic than its precursor.
- The liver converts ammonia to urea.
- The liver stores a multitude of substances, including glucose (in the form of glycogen), vitamin B12, iron, and copper.
- In the first trimester fetus, the liver is the main site of red blood cell production. By the 32nd week of gestation, the bone marrow has almost completely taken over that task.
- The liver is responsible for immunological effects- the reticuloendothelial system of the liver contains many immunologically active cells, acting as a ‘sieve’ for antigens carried to it via the portal system.
- The liver produces albumin, the major osmolar component of blood serum.
Currently, there is no artificial organ or device capable of emulating all the functions of the liver. Some functions can be emulated by liver dialysis, an experimental treatment for liver failure.
Diseases of the liver
Many diseases of the liver are accompanied by jaundice caused by increased levels of bilirubin in the system. The bilirubin results from the breakup of the hemoglobin of dead red blood cells; normally, the liver removes bilirubin from the blood and excretes it through bile.
- Hepatitis, inflammation of the liver, caused mainly by various viruses but also by some poisons, autoimmunity or hereditary conditions.
- Cirrhosis is the formation of fibrous tissue in the liver, replacing dead liver cells. The death of the liver cells can for example be caused by viral hepatitis, alcoholism or contact with other liver-toxic chemicals.
- Haemochromatosis, a hereditary disease causing the accumulation of iron in the body, eventually leading to liver damage.
- Cancer of the liver (primary hepatocellular carcinoma or cholangiocarcinoma and metastatic cancers, usually from other parts of the gastrointestinal tract).
- Wilson’s disease, a hereditary disease which causes the body to retain copper.
- Primary sclerosing cholangitis, an inflammatory disease of the bile duct, autoimmune in nature.
- Primary biliary cirrhosis, autoimmune disease of small bile ducts.
- Budd-Chiari syndrome, obstruction of the hepatic vein.
- Gilbert’s syndrome, a genetic disorder of bilirubin metabolism, found in about 5% of the population.
- Glycogen storage disease type II,The build-up of glycogen causes progressive muscle weakness (myopathy) throughout the body and affects various body tissues, particularly in the heart, skeletal muscles, liver and nervous system.
There are also many pediatric liver disease, including biliary atresia, alpha-1 antitrypsin deficiency, alagille syndrome, and progressive familial intrahepatic cholestasis, to name but a few.
A number of liver function tests are available to test the proper function of the liver. These test for the presence of enzymes in blood that are normally most abundant in liver tissue, metabolites or products.
Liver transplantation
Human liver transplant was first performed by Thomas Starzl in USA and Roy Calne in Cambridge, England in 1963 and 1965 respectively.
Liver transplantation is the only option for those with irreversible liver failure. Most transplants are done for chronic liver diseases leading to cirrhosis, such as chronic hepatitis C, alcoholism, autoimmune hepatitis, and many others. Less commonly, liver transplantation is done for fulminant hepatic failure, in which liver failure occurs over days to weeks.
Liver allografts for transplant usually come from non-living donors who have died from fatal brain injury. Living donor liver transplantation is a technique in which a portion of a living person’s liver is removed and used to replace the entire liver of the recipient. This was first performed in 1989 for pediatric liver transplantation. Only 20% of an adult’s liver (Couinaud segments 2 and 3) is needed to serve as a liver allograft for an infant or small child.
More recently, adult-to-adult liver transplantation has been done using the donor’s right hepatic lobe which amounts to 60% of the liver. Due to the ability of the liver to regenerate, both the donor and recipient end up with normal liver function if all goes well. This procedure is more controversial as it entails performing a much larger operation on the donor, and indeed there have been at least 2 donor deaths out of the first several hundred cases. A recent publication has addressed the problem of donor mortality, and at least 14 cases have been found.[6] The risk of postoperative complications (and death) is far greater in right sided hepatectomy than left sided operations.
With the recent advances of non-invasive imaging, living liver donors usually have to undergo imaging examinations for liver anatomy to decide if the anatomy is feasible for donation. The evaluation is usually performed by multi-detector row computed tomography (MDCT) and magnetic resonence imaging (MRI). MDCT is good in vascular anatomy and volumetry. MRI is used for biliary tree anatomy. Donors with very unusual vascular anatomy, which makes them impossible for donation, could be screened out to avoid unnessary operation.
-
 MDCT image. Arterial anatomy contraindicated for liver donation.
MDCT image. Arterial anatomy contraindicated for liver donation. -
 MDCT image. Portal venous anatomy contraindicated for liver donation.
MDCT image. Portal venous anatomy contraindicated for liver donation. -
 MDCT image. Beautiful 3D image created by MDCT can clearly visualize the liver, measure the liver volume, and plan the dissection plane to facilitate the liver transplantation procedure.
MDCT image. Beautiful 3D image created by MDCT can clearly visualize the liver, measure the liver volume, and plan the dissection plane to facilitate the liver transplantation procedure.



Development
Fetal blood supply
In the growing fetus, a major source of blood to the liver is the umbilical vein which supplies nutrients to the growing fetus. The umbilical vein enters the abdomen at the umbilicus, and passes upward along the free margin of the falciform ligament of the liver to the inferior surface of the liver. There it joins with the left branch of the portal vein. The ductus venosus carries blood from the left portal vein to the left hepatic vein and then to the inferior vena cava, allowing placental blood to bypass the liver.
In the fetus, the liver develops throughout normal gestation, and does not perform the normal filtration of the infant liver. The liver does not perform digestive processes because the fetus does not consume meals directly, but receives nourishment from the mother via the placenta. The fetal liver releases some blood stem cells that migrate to the fetal thymus, so initially the lymphocytes, called T-cells, are created from fetal liver stem cells. Once the fetus is delivered, the formation of blood stem cells in infants shifts to the red bone marrow.
After birth, the umbilical vein and ductus venosus are completely obliterated two to five days postpartum; the former becomes the ligamentum teres and the latter becomes the ligamentum venosum. In the disease state of cirrhosis and portal hypertension, the umbilical vein can open up again.
Liver as food
Template:Nutritionalvalue Mammal and bird livers are commonly eaten as food. Liver can be baked, broiled, or fried (often served as liver and onions) or eaten raw (liver sashimi), but is perhaps most commonly made into a spread (examples including liver pâté, foie gras, Braunschweiger, chopped liver, and leverpostej) or sausage (liverwurst).
Both animal and fish livers are rich in iron and Vitamin A, and cod liver oil is commonly used as a dietary supplement. Very high doses of Vitamin A can be toxic; in 1913, Antarctic explorers Douglas Mawson and Xavier Mertz were both poisoned, the latter fatally, from eating husky liver. In the US, the USDA specifies 3000 μg per day as a tolerable upper limit, which amounts to about 50 g of raw pork liver or, as reported in a non scientific source, 3 g of polar-bear liver.[7] However, acute vitamin A poisoning is not likely to result from liver consumption, since it is present in a less toxic form than in many dietary supplements.[8]
Cultural allusions
In Greek mythology, Prometheus was punished by the gods for revealing fire to humans by being chained to a rock where a vulture (or an eagle) would peck out his liver, which would regenerate overnight. Curiously, the liver is the only human internal organ that actually can regenerate itself to a significant extent; this characteristic may have already been known to the Greeks due to survived injuries in battle.
The Talmud (tractate Berakhot 61b) refers to the liver as the seat of anger, with the gallbladder counteracting this.
In Arabic and Persian language, the liver is used in figurative speech to refer to courage and strong feelings, or “their best,” e.g. “This Mecca has thrown to you the pieces of its liver!” [9]
The legend of Liver-Eating Johnson says that he would cut out and eat the liver of each man killed.
In the motion picture The Message, Hind bint Utbah is implied or portrayed eating the liver of Hamza ibn ‘Abd al-Muttalib during the Battle of Uhud.
Inuit will not eat the liver of polar bears (due to the fact a polar bear’s liver contains so much Vitamin A as to be poisonous to humans) or seals [10]
Further reading
- The following are standard medical textbooks:
- Eugene R. Schiff, Michael F. Sorrell, Willis C. Maddrey, eds. Schiff’s diseases of the liver, 9th ed. Philadelphia : Lippincott, Williams & Wilkins, 2003. ISBN 0-7817-3007-4
- Sheila Sherlock, James Dooley. Diseases of the liver and biliary system, 11th ed. Oxford, UK ; Malden, MA : Blackwell Science. 2002. ISBN 0-632-05582-0
- David Zakim, Thomas D. Boyer. eds. Hepatology: a textbook of liver disease, 4th ed. Philadelphia: Saunders. 2003. ISBN 0-7216-9051-3
- These are for the lay reader or patient:
- Sanjiv Chopra. The Liver Book: A Comprehensive Guide to Diagnosis, Treatment, and Recovery, Atria, 2002, ISBN 0-7434-0585-4
- Melissa Palmer. Dr. Melissa Palmer’s Guide to Hepatitis and Liver Disease: What You Need to Know, Avery Publishing Group; Revised edition May 24, 2004, ISBN 1-58333-188-3. her webpage.
- Howard J. Worman. The Liver Disorders Sourcebook, McGraw-Hill, 1999, ISBN 0-7373-0090-6. his Columbia University web site, “Diseases of the liver”
See also
References
- ↑ KMLE Medical Dictionary. “KMLE Medical Dictionary Definition of liver“. Retrieved 2007-02-16
- ↑ The Greek word “ήπαρ” was derived from hēpaomai (ηπάομαι): to mend, to repair, hence hēpar actually means “repairable”, indicating that this organ can regenerate itself spontaneously in the case of lesion.
- ↑ Robbins and Cotran Pathologic Basis of Disease, 7th Edition, p. 878
- ↑ Three-dimensional Anatomy of the Couinaud Liver Segments – University of Iowa
- ↑ Limitations and Pitfalls of Couinaud`s Segmentation of the Liver in Transaxial Imaging – Prof. Dr. Holger Strunk
- ↑ Bramstedt K (2006). “Living liver donor mortality: where do we stand?”. Am J Gastroenterol. 101 (4): 755–9. PMID 16494593.
- ↑ A. Aggrawal, Death by Vitamin A
- ↑ Myhre et al., “Water-miscible, emulsified, and solid forms of retinol supplements are more toxic than oil-based preparations”, Am. J. Clinical Nutrition, 78, 1152 (2003)
- ↑ THE GREAT BATTLE OF BADAR (Yaum-e-Furqan)
- ↑ Man’s best friend? – Student BMJ
Additional images
-
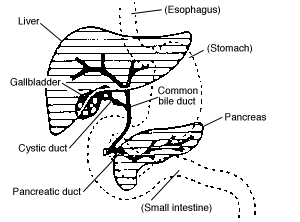 Accessory digestive system.
Accessory digestive system. -
 Digestive organs.
Digestive organs. -
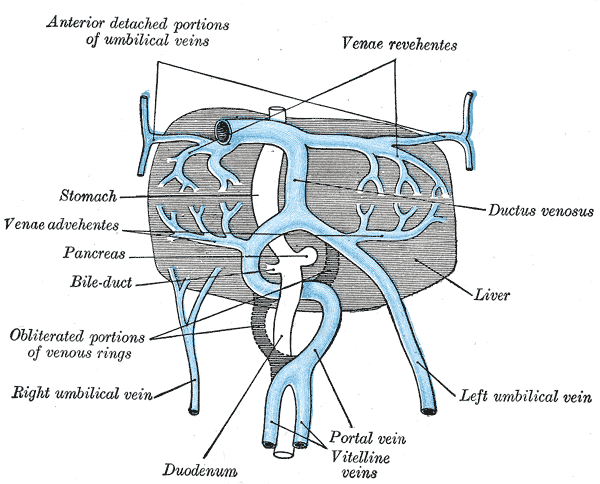 The liver and the veins in connection with it, of a human embryo, twenty-four or twenty-five days old, as seen from the ventral surface.
The liver and the veins in connection with it, of a human embryo, twenty-four or twenty-five days old, as seen from the ventral surface. -
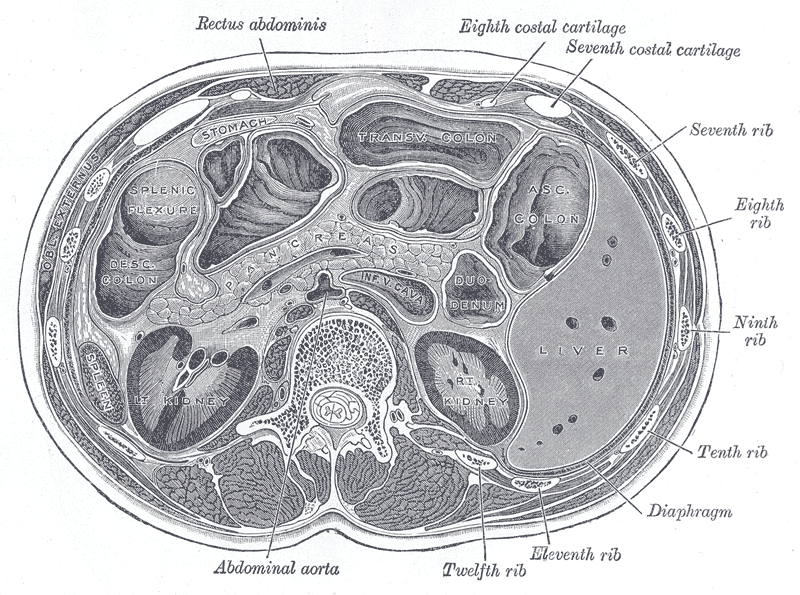 Transverse section through the middle of the first lumbar vertebra, showing the relations of the pancreas.
Transverse section through the middle of the first lumbar vertebra, showing the relations of the pancreas. -
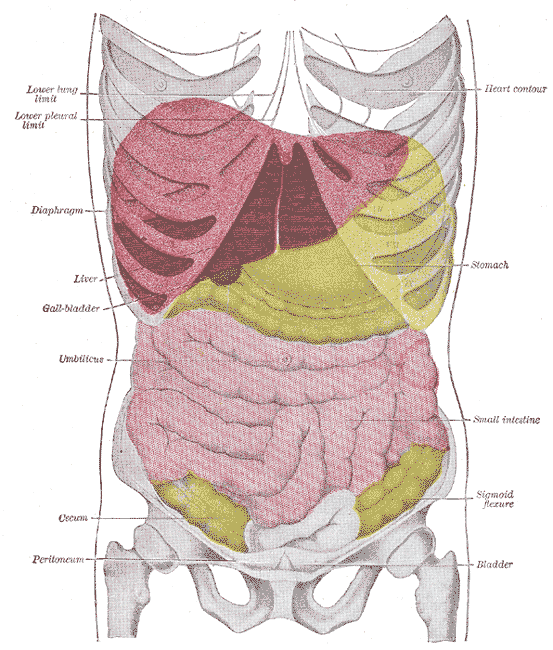
 Front of abdomen, showing surface markings for liver, stomach, and great intestine
Front of abdomen, showing surface markings for liver, stomach, and great intestine -
 Topography of thoracic and abdominal viscera.
Topography of thoracic and abdominal viscera. -
-
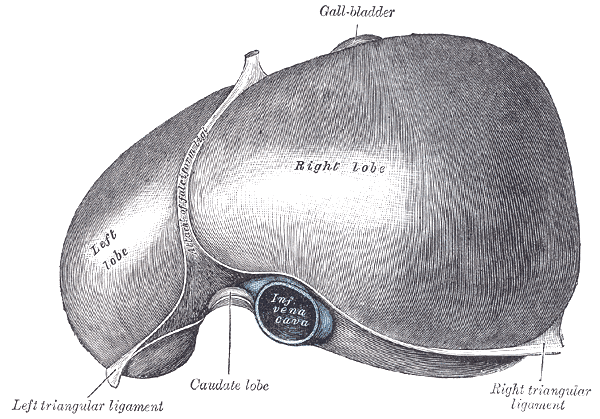 View of the superior (“top”) surface from Gray’s Anatomy (1918)
View of the superior (“top”) surface from Gray’s Anatomy (1918) -
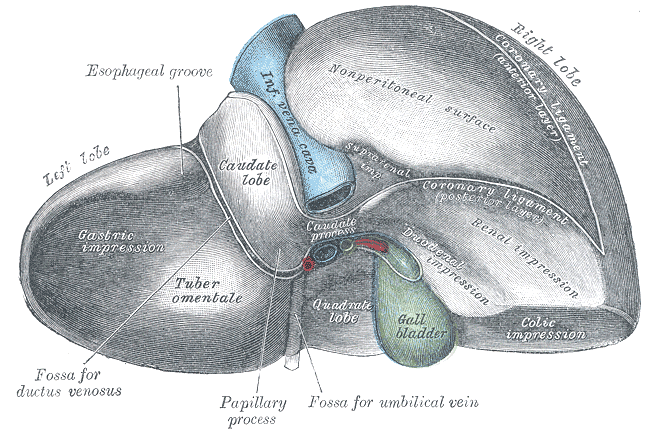 View of the inferior (“bottom”) surface from Gray’s Anatomy (1918)
View of the inferior (“bottom”) surface from Gray’s Anatomy (1918)









External links
- electron microscopic images of the liver (Dr. Jastrow’s EM-atlas)
- Canadian Liver Foundation Official Website
- Liver Info: Youth-Oriented Website. Created by Liver Info Students’ Association (LISA), Official Chapter of Canadian Liver Foundation
- The Liver as an Excretory Organ
- Children’s Liver Association for Support Services, C.L.A.S.S. A large non-profit organization. An online Support Group full of resources, materials and stories; includes a Community Discussion Forum and Chat Room
- The American Liver Foundation
- American Association for the Study of Liver Diseases (AASLD)
- American Liver Society (ALS)
- WikiLiver — a wiki dedicated to the liver
- “It’s Dangerous to Ignore Your Liver” — information provided by the American Liver Foundation
- “The Liver and its Diseases” — information at h2g2
- Liver Families — an online support group for families whose lives have been affected by pediatric liver disease and transplant issues
- Children’s Liver Disease Foundation — an organisation dedicated to fighting childhood liver disease and supporting affected families
- Liver Specialists of Texas: a site designed for patients with liver disease, located in Houston, Texas USA
- Autoimmune immune liver disease
- British Liver Trust – includes patient info oriented to British situations.
ar:كبد ay:K’iwcha zh-min-nan:Koaⁿ bs:Jetra bg:Черен дроб ca:Fetge cv:Пĕвер cs:Játra cy:Afu da:Lever de:Leber dv:ފުރަމޭ et:Maks el:Ήπαρ eo:Hepato eu:Gibel ga:Ae gd:Àdha gl:Fígado ko:간 hi:कलेजा hr:Jetra io:Hepato id:Hati is:Lifur it:Fegato he:כבד jv:Ati ka:ღვიძლი ku:Kezeb la:Iecur lt:Kepenys ln:Libale lmo:Fídech hu:Máj mk:Црн дроб ml:കരള് mt:Fwied ms:Hati nah:Ēltapachtli nl:Lever no:Leveren nn:Lever oc:Fetge pag:Altey qu:Kukupin sq:Mëlçia scn:Fìcatu simple:Liver sk:Pečeň sl:Jetra sr:Јетра sh:Jetra su:Ati fi:Maksa sv:Lever te:కాలేయం th:ตับ tg:Ҷигар uk:Печінка yi:לעבער
References
References
- ↑ Vrielink H, van der Poel CL, Reesink HW, Zaaijer HL, Scholten E, Kremer LC, Cuypers HT, Lelie PN, van Oers MH (1995). “Look-back study of infectivity of anti-HCV ELISA-positive blood components”. Lancet. 345 (8942): 95–6. PMID 7815889.
- ↑ Alter MJ (1997). “Epidemiology of hepatitis C”. Hepatology. 26 (3 Suppl 1): 62S–65S. doi:10.1002/hep.510260711. PMID 9305666.
- ↑ Jadoul M, Barril G (2012). “Hepatitis C in hemodialysis: epidemiology and prevention of hepatitis C virus transmission”. Contrib Nephrol. 176: 35–41. doi:10.1159/000333761. PMID 22310779.
- ↑ Liou TC, Chang TT, Young KC, Lin XZ, Lin CY, Wu HL (1992). “Detection of HCV RNA in saliva, urine, seminal fluid, and ascites”. J. Med. Virol. 37 (3): 197–202. PMID 1331308.
- ↑ van Doornum GJ, Hooykaas C, Cuypers MT, van der Linden MM, Coutinho RA (1991). “Prevalence of hepatitis C virus infections among heterosexuals with multiple partners”. J. Med. Virol. 35 (1): 22–7. PMID 1940879.
- ↑ Martínez-Bauer E, Forns X, Armelles M, Planas R, Solà R, Vergara M, Fàbregas S, Vega R, Salmerón J, Diago M, Sánchez-Tapias JM, Bruguera M (2008). “Hospital admission is a relevant source of hepatitis C virus acquisition in Spain”. J. Hepatol. 48 (1): 20–7. doi:10.1016/j.jhep.2007.07.031. PMID 17998149.
- ↑ Alter MJ (2008). “Healthcare should not be a vehicle for transmission of hepatitis C virus”. J. Hepatol. 48 (1): 2–4. doi:10.1016/j.jhep.2007.10.007. PMID 18023493.
- ↑ Ohto H, Terazawa S, Sasaki N, Sasaki N, Hino K, Ishiwata C, Kako M, Ujiie N, Endo C, Matsui A (1994). “Transmission of hepatitis C virus from mothers to infants. The Vertical Transmission of Hepatitis C Virus Collaborative Study Group”. N. Engl. J. Med. 330 (11): 744–50. doi:10.1056/NEJM199403173301103. PMID 8107740.
- ↑ Zanetti AR, Tanzi E, Paccagnini S, Principi N, Pizzocolo G, Caccamo ML, D’Amico E, Cambiè G, Vecchi L (1995). “Mother-to-infant transmission of hepatitis C virus. Lombardy Study Group on Vertical HCV Transmission”. Lancet. 345 (8945): 289–91. PMID 7530793.
- ↑ Thimme R, Oldach D, Chang KM, Steiger C, Ray SC, Chisari FV (2001). “Determinants of viral clearance and persistence during acute hepatitis C virus infection”. J Exp Med. 194 (10): 1395–406. PMC 2193681. PMID 11714747.
- ↑ Thimme R, Bukh J, Spangenberg HC, Wieland S, Pemberton J, Steiger C; et al. (2002). “Viral and immunological determinants of hepatitis C virus clearance, persistence, and disease”. Proc Natl Acad Sci U S A. 99 (24): 15661–8. doi:10.1073/pnas.202608299. PMC 137773. PMID 12441397.
- ↑ Su AI, Pezacki JP, Wodicka L, Brideau AD, Supekova L, Thimme R; et al. (2002). “Genomic analysis of the host response to hepatitis C virus infection”. Proc Natl Acad Sci U S A. 99 (24): 15669–74. doi:10.1073/pnas.202608199. PMC 137774. PMID 12441396.
- ↑ Katze MG, He Y, Gale M (2002). “Viruses and interferon: a fight for supremacy”. Nat Rev Immunol. 2 (9): 675–87. doi:10.1038/nri888. PMID 12209136.
- ↑ Foy E, Li K, Wang C, Sumpter R, Ikeda M, Lemon SM; et al. (2003). “Regulation of interferon regulatory factor-3 by the hepatitis C virus serine protease”. Science. 300 (5622): 1145–8. doi:10.1126/science.1082604. PMID 12702807.
- ↑ Blindenbacher A, Duong FH, Hunziker L, Stutvoet ST, Wang X, Terracciano L; et al. (2003). “Expression of hepatitis c virus proteins inhibits interferon alpha signaling in the liver of transgenic mice”. Gastroenterology. 124 (5): 1465–75. PMID 12730885.
- ↑ 16.0 16.1 16.2 Pawlotsky JM (2004). “Pathophysiology of hepatitis C virus infection and related liver disease”. Trends Microbiol. 12 (2): 96–102. doi:10.1016/j.tim.2003.12.005. PMID 15036326.
- ↑ 17.0 17.1 Farci P, Alter HJ, Wong DC, Miller RH, Govindarajan S, Engle R; et al. (1994). “Prevention of hepatitis C virus infection in chimpanzees after antibody-mediated in vitro neutralization”. Proc Natl Acad Sci U S A. 91 (16): 7792–6. PMC 44488. PMID 7519785.
- ↑ 18.0 18.1 Shimizu YK, Igarashi H, Kiyohara T, Cabezon T, Farci P, Purcell RH; et al. (1996). “A hyperimmune serum against a synthetic peptide corresponding to the hypervariable region 1 of hepatitis C virus can prevent viral infection in cell cultures”. Virology. 223 (2): 409–12. doi:10.1006/viro.1996.0497. PMID 8806581.
- ↑ 19.0 19.1 Bartosch B, Dubuisson J, Cosset FL (2003). “Infectious hepatitis C virus pseudo-particles containing functional E1-E2 envelope protein complexes”. J Exp Med. 197 (5): 633–42. PMC 2193821. PMID 12615904.
- ↑ 20.0 20.1 Puntoriero G, Meola A, Lahm A, Zucchelli S, Ercole BB, Tafi R; et al. (1998). “Towards a solution for hepatitis C virus hypervariability: mimotopes of the hypervariable region 1 can induce antibodies cross-reacting with a large number of viral variants”. EMBO J. 17 (13): 3521–33. doi:10.1093/emboj/17.13.3521. PMC 1170689. PMID 9649423.
- ↑ 21.0 21.1 Bertoletti A, Ferrari C (2003). “Kinetics of the immune response during HBV and HCV infection”. Hepatology. 38 (1): 4–13. doi:10.1053/jhep.2003.50310. PMID 12829979.
- ↑ Bain C, Fatmi A, Zoulim F, Zarski JP, Trépo C, Inchauspé G (2001). “Impaired allostimulatory function of dendritic cells in chronic hepatitis C infection”. Gastroenterology. 120 (2): 512–24. PMID 11159892.
- ↑ Wedemeyer H, He XS, Nascimbeni M, Davis AR, Greenberg HB, Hoofnagle JH; et al. (2002). “Impaired effector function of hepatitis C virus-specific CD8+ T cells in chronic hepatitis C virus infection”. J Immunol. 169 (6): 3447–58. PMID 12218168.
- ↑ Lechner F, Wong DK, Dunbar PR, Chapman R, Chung RT, Dohrenwend P; et al. (2000). “Analysis of successful immune responses in persons infected with hepatitis C virus”. J Exp Med. 191 (9): 1499–512. PMC 2213430. PMID 10790425.
- ↑ Appay V, Dunbar PR, Callan M, Klenerman P, Gillespie GM, Papagno L; et al. (2002). “Memory CD8+ T cells vary in differentiation phenotype in different persistent virus infections”. Nat Med. 8 (4): 379–85. doi:10.1038/nm0402-379. PMID 11927944.
- ↑ Kittlesen DJ, Chianese-Bullock KA, Yao ZQ, Braciale TJ, Hahn YS (2000). “Interaction between complement receptor gC1qR and hepatitis C virus core protein inhibits T-lymphocyte proliferation”. J Clin Invest. 106 (10): 1239–49. doi:10.1172/JCI10323. PMC 381434. PMID 11086025.
- ↑ Poynard T, Ratziu V, McHutchison J, Manns M, Goodman Z, Zeuzem S; et al. (2003). “Effect of treatment with peginterferon or interferon alfa-2b and ribavirin on steatosis in patients infected with hepatitis C.” Hepatology. 38 (1): 75–85. doi:10.1053/jhep.2003.50267. PMID 12829989.
- ↑ Barba G, Harper F, Harada T, Kohara M, Goulinet S, Matsuura Y; et al. (1997). “Hepatitis C virus core protein shows a cytoplasmic localization and associates to cellular lipid storage droplets”. Proc Natl Acad Sci U S A. 94 (4): 1200–5. PMC 19768. PMID 9037030.
- ↑ Rubbia-Brandt L, Quadri R, Abid K, Giostra E, Malé PJ, Mentha G; et al. (2000). “Hepatocyte steatosis is a cytopathic effect of hepatitis C virus genotype 3”. J Hepatol. 33 (1): 106–15. PMID 10905593.
- ↑ Serfaty L, Andreani T, Giral P, Carbonell N, Chazouillères O, Poupon R (2001). “Hepatitis C virus induced hypobetalipoproteinemia: a possible mechanism for steatosis in chronic hepatitis C.” J Hepatol. 34 (3): 428–34. PMID 11322205.
- ↑ Castéra L, Hézode C, Roudot-Thoraval F, Bastie A, Zafrani ES, Pawlotsky JM; et al. (2003). “Worsening of steatosis is an independent factor of fibrosis progression in untreated patients with chronic hepatitis C and paired liver biopsies”. Gut. 52 (2): 288–92. PMC 1774979. PMID 12524415.
- ↑ Sulkowski MS, Thomas DL (2003). “Hepatitis C in the HIV-Infected Person”. Ann Intern Med. 138 (3): 197–207. PMID 12558359.
- ↑ Pol S, Vallet-Pichard A, Fontaine H, Lebray P (2002). “HCV infection and hemodialysis”. Semin Nephrol. 22 (4): 331–9. PMID 12118398.
- ↑ National Institutes of Health (2002). “National Institutes of Health Consensus Development Conference Statement: Management of hepatitis C: 2002–June 10-12, 2002”. Hepatology. 36 (5 Suppl 1): S3–20. doi:10.1053/jhep.2002.37117. PMID 12407572.
- ↑ Ray RB, Lagging LM, Meyer K, Ray R (1996). “Hepatitis C virus core protein cooperates with ras and transforms primary rat embryo fibroblasts to tumorigenic phenotype”. J Virol. 70 (7): 4438–43. PMC 190377. PMID 8676467.
- ↑ Sakamuro D, Furukawa T, Takegami T (1995). “Hepatitis C virus nonstructural protein NS3 transforms NIH 3T3 cells”. J Virol. 69 (6): 3893–6. PMC 189112. PMID 7745741.
- ↑ Park JS, Yang JM, Min MK (2000). “Hepatitis C virus nonstructural protein NS4B transforms NIH3T3 cells in cooperation with the Ha-ras oncogene”. Biochem Biophys Res Commun. 267 (2): 581–7. doi:10.1006/bbrc.1999.1999. PMID 10631105.
- ↑ Ghosh AK, Steele R, Meyer K, Ray R, Ray RB (1999). “Hepatitis C virus NS5A protein modulates cell cycle regulatory genes and promotes cell growth”. J Gen Virol. 80 ( Pt 5): 1179–83. PMID 10355764.
- ↑ 39.0 39.1 39.2 39.3 39.4 Cacoub P, Desbois AC, Comarmond C, Saadoun D (November 2018). “Impact of sustained virological response on the extrahepatic manifestations of chronic hepatitis C: a meta-analysis”. Gut. 67 (11): 2025–2034. doi:10.1136/gutjnl-2018-316234. PMID 29703790.
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH