
Leprosy
Template:DiseaseDisorder infobox
For patient information, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: João André Alves Silva, M.D. [2] Kiran Singh, M.D. [3]
Synonyms and keywords: Hansen’s disease
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: João André Alves Silva, M.D. [2]
Overview
Leprosy is a chronic infectious disease caused by the bacterium Mycobacterium leprae.[1] Leprosy is primarily a granulomatous disease of the peripheral nerves and mucosa of the upper respiratory tract; skin lesions are the primary external symptom. Left untreated, leprosy can be progressive, causing permanent damage to the skin, nerves, limbs, and eyes.
Historical Perspective
Mycobacterium leprae, the causative agent of leprosy, was discovered by G. H. Armauer Hansen in Norway in 1873, making it the first bacterium to be identified as causing disease in man.[2][3] Historically, individuals with leprosy have been known as lepers, however, this term is falling into disuse due the pejorative connotation of the term.
Classification
The Ridley Jopling classification and the WHO classification are the two most widely used systems to classify Leprosy. These classification systems are based on clinical, microbiologic and histopathological features, and are used to determine the patient’s prognosis and the treatment regimen.[4][5][6]
Pathophysiology
The clinical manifestations of leprosy largely reflect the immune response of the host towards the infection. Once the bacterial cells penetrate and multiply within the hosts skin and peripheral nerve cells, the immune system mounts a response toward the infected cells, which results in clinical symptoms. Several single-nucleotide polymorphisms such as TNF-α, IL-10, IFN-γ, TLR 1 have been associated with a greater susceptibility to leprosy as have other genetic markers.
Causes
Mycobacterium leprae is a gram-positive obligate intracellular, acid-fast bacillus, responsible for the development of leprosy, or Hansen’s disease. This organism has a very slow growth and has a predilection to affect colder parts of the body, such as the skin, superficial nerves and upper respiratory mucous membranes. Although a route of transmission has not been absolutely defined yet, studies are pointing to a colonization of the dermis and respiratory mucosa of the infected patients. It is an uncommon bacteria, since it has only been noticed to infect and grow in some species of primates and in the nine-banded armadillo.[6]
Differential Diagnosis
Leprosy must be differentiated from other diseases that cause skin lesions, nodules, plaques paresthesias and nerve pain, such as autoimmune diseases, SLE, parasitic infections, vitiligo or cutaneous tuberculosis.
Epidemiology and Demographics
Current prevalence rate of leprosy per 100,000 is 3.7. The disease is more prevalent in endemic areas, which represent a potential source of spread of the disease to the rest of the world.
Risk Factors
Risk factors for contracting leprosy include close contact with an untreated, active multibacillary disease patient with the subtype of lepromatous leprosy, living in an endemic region (Angola, Brazil, Central African Republic, Democratic Republic of Congo, Federated States of Micronesia, India, Kiribati, Madagascar, Mozambique, Nepal, Republic of Marshall Islands, United Republic of Tanzania), age between 5 and 15 as well as over 30, Armadillo contact, tattoos, and genetic variants of the NOD2-mediated signaling pathway.
Natural History, Complications and Prognosis
Leprosy may lead to severe complications if not diagnosed and treated early, which will affect the prognosis.
Diagnosis
Diagnostic Criteria
The diagnosis of leprosy requires at least 1 of 3 criteria to be present: 1) loss of sensation of a hipopigmented skin patch, 2) a thickened peripheral nerve concomitantly with weakness or loss of sensation of the area, and/or 3) confirmation of mycobacterium leprae in a skin smear.
History and Symptoms
Common symptoms of leprosy include hypopigmented, anesthetic, red skin lesions, that are hard to heal, nodular growths on the skin, muscle weakness and paresthesia of the extremities and eye problems. If left untreated blindness and paralysis may occur.
Physical Examination
Although the findings on physical examination may vary depending upon the subytpe of leprosy, common findings include hypopigmented skin lesions, thickened dermis, and loss of sensation.
Laboratory Findings
There are no laboratory tests that diagnose leprosy.
X Ray
Osteoporosis is a common finding in leprosy patients which along with the loss of sensation may lead to fractures.
Other Imaging Findings
There are no other imaging studies that diagnose leprosy.
Other Diagnostic Studies
Biopsy of skin lesions and skin smear tests are important for the diagnosis of leprosy in patients whose clinical examination is suspicious of the disease.
Treatment
Medical Therapy
The medical treatment of leprosy is made with a multiple drug regimen, for 6 to 12 months. This drug regimen may include 2 or 3 drugs: rifampicin, dapsone and clofazimine, or rifampicin and dapsone, depending on the class of the disease.
Surgery
Surgery is not indicated in the treatment of leprosy, yet it may treat or decrease the impact of some of the complications that may arise from the disease.
Primary prevention
Primary prevention of leprosy includes immunoprophylaxis, chemoprophylaxis and education of the populations to prevent infection by the Mycobacterium leprae.
Secondary Prevention
There is no secondary prevention of leprosy available because it is not possible to know if contact with leprosy will lead to the development of the disease, until first symptoms appear.
Tertiary prevention
After treatment has been initiated, other measures to minimize further damage to the patient include: education of the individual and family members to monitor and treat skin ulcers and other lesions, primary care facilities to provide help to the populations and to direct patients to a specialist, whenever necessary.[7]
Cost-effectiveness of Therapy
After the results of the campaign of the WHO to eradicate leprosy, the treatment of this disease may be considered cost-effective.
Future or Investigational Therapies
Ongoing research focuses on the the mechanism of leprosy transmission as well as the identification of patients at high risk of infection in order to improve disease prevention and to treat infected individuals earlier. [7] Identification of alternatives to existing drugs, such as rifampicin is also critical in so far as these agents may be contraindicated either because of toxicity or resistance. [7]
References
- ↑ Sasaki S, Takeshita F, Okuda K, Ishii N (2001). “Mycobacterium leprae and leprosy: a compendium”. Microbiol Immunol. 45 (11): 729–36. PMID 11791665.
- ↑ Hansen GHA (1874). “Undersøgelser Angående Spedalskhedens Årsager (Investigations concerning the etiology of leprosy)”. Norsk Mag. Laegervidenskaben (in Norwegian). 4: pp. 1–88.
- ↑ Irgens L (2002). “The discovery of the leprosy bacillus”. Tidsskr Nor Laegeforen. 122 (7): 708–9. PMID 11998735.
- ↑ Walker, Stephen L.; Lockwood, Dina N.J. (2007). “Leprosy”. Clinics in Dermatology. 25 (2): 165–172. doi:10.1016/j.clindermatol.2006.05.012. ISSN 0738-081X.
- ↑ Eichelmann, K.; González González, S.E.; Salas-Alanis, J.C.; Ocampo-Candiani, J. (2013). “Leprosy. An Update: Definition, Pathogenesis, Classification, Diagnosis, and Treatment”. Actas Dermo-Sifiliográficas (English Edition). 104 (7): 554–563. doi:10.1016/j.adengl.2012.03.028. ISSN 1578-2190.
- ↑ 6.0 6.1 Bhat, Ramesh Marne; Prakash, Chaitra (2012). “Leprosy: An Overview of Pathophysiology”. Interdisciplinary Perspectives on Infectious Diseases. 2012: 1–6. doi:10.1155/2012/181089. ISSN 1687-708X.
- ↑ 7.0 7.1 7.2 “Enhanced global strategy for further reducing the disease burden due to leprosy (2011-2015)” (PDF).
Historical Perspective

Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: João André Alves Silva, M.D. [2]
Overview
Mycobacterium leprae, the causative agent of leprosy, was discovered by G. H. Armauer Hansen in Norway in 1873, making it the first bacterium to be identified as causing disease in man.[1][2] Historically, individuals with leprosy have been known as lepers, however, this term is falling into disuse due the pejorative connotation of the term.
Etymology
The word “leprosy” derives from the ancient Greek words lepros, a scale, and lepein, to peel.[3] The word came into the English language via Latin and Old French. The first attested English use is in the Ancrene Wisse, a 13th-century manual for nuns (“Moyseses hond..bisemde o þe spitel uuel & þuhte lepruse.” The Middle English Dictionary, s.v., “leprous”). A roughly contemporaneous use is attested in the Anglo-Norman Dialogues of Saint Gregory, “Esmondez i sont li lieprous” (Anglo-Norman Dictionary, s.v., “leprus”).
Leper Hospitals
Numerous leprosaria, or leper hospitals, sprang up in the Middle Ages, particularly in England, and numbered 250 by A.D. 1230. The first recorded leprosarium was in Harbledown. (See Leper colony.) These institutions were run along monastic lines and, while lepers were encouraged to live in these monastic-type establishments, this was for their own health as well as quarantine.
Misdiagnosis Through History
Historically, the term Tzaraath from the Hebrew Bible was, erroneously, commonly translated as leprosy, although the symptoms of Tzaraath were not entirely consistent with leprosy and rather referred to a variety of disorders other than Hansen’s disease.[4] In particular tinea capitis (fungal scalp infection) and related infections on other body parts caused by the dermatophyte fungus Trichophyton violaceum are abundant throughout the Middle East and North Africa today and might also have been common in biblical times. Similarly, the related agent of the disfiguring skin disease favus, Trichophyton schoenleinii, appears to have been common throughout Eurasia and Africa before the advent of modern medicine. Persons with severe favus and similar fungal diseases (and potentially also with severe psoriasis and other diseases not caused by microorganisms) tended to be classed as having leprosy as late as the 17th century in Europe.[5] This is clearly shown in the painting Governors of the Home for Lepers at Haarlem 1667 by Jan de Bray (Frans Hals Museum, Haarlem, the Netherlands), where a young Dutch man with a vivid scalp infection, almost certainly caused by a fungus, is shown being cared for by three officials of a charitable home intended for leprosy sufferers. The use of the word “leprosy” before the mid-19th century, when microscopic examination of skin for medical diagnosis was first developed, can seldom be correlated reliably with Hansen’s disease as we understand it today.
Cultural Impact
Some medieval people believed that those suffering from leprosy were considered to be going through Purgatory on Earth, and for this reason their suffering was considered more holy than the ordinary person’s. More frequently, lepers were seen to exist in a place between life and death: they were still alive, yet many chose or were forced to completely separate themselves from mundane existence. Radegund was noted for washing the feet of lepers. Orderic Vitalis writes of a monk, Ralf, who was so overcome by the plight of lepers that he prayed to catch leprosy himself (which he eventually did). The leper would carry a clapper and bell to warn of his approach, and this was as much to attract attention for charity as to warn people that a diseased person was near.
References
- ↑ Hansen GHA (1874). “Undersøgelser Angående Spedalskhedens Årsager (Investigations concerning the etiology of leprosy)”. Norsk Mag. Laegervidenskaben (in Norwegian). 4: pp. 1–88.
- ↑ Irgens L (2002). “The discovery of the leprosy bacillus”. Tidsskr Nor Laegeforen. 122 (7): 708–9. PMID 11998735.
- ↑ Barnhart RK (1995). Barnhart Concise Dictionary of Etymology. New York: Harper Collins. ISBN 0062700847.
- ↑ Artscroll Tanakh, Leviticus 13:59, 1996
- ↑ Kane J, Summerbell RC, Sigler L, Krajden S, Land G (1997). Laboratory Handbook of Dermatophytes: A clinical guide and laboratory manual of dermatophytes and other filamentous fungi from skin, hair and nails. Star Publishers (Belmont, CA). ISBN 0898631572.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: João André Alves Silva, M.D. [2]Kiran Singh, M.D. [3]
Overview
The Ridley Jopling classification and the WHO classification are the two most widely used systems to classify Leprosy. These classification systems are based on clinical, microbiologic and histopathological features, and are used to determine the patient’s prognosis and the treatment regimen.[1][2][3]
Classification
There are different systems for classifying leprosy. However, the two more common classification schemes include the WHO and the Ridley-Jopling systems.
| WHO | Ridley-Jopling | ICD-10 | MeSH | Description | Lepromin test | Immune target |
|---|---|---|---|---|---|---|
| Paucibacillary | Tuberculoid (“TT”), Borderline Tuberculoid (“BT”) | A30.1, A30.2 | Tuberculoid | It is characterized by one or more hypopigmented skin macules and anaesthetic patches, where skin sensations are lost because of damaged peripheral nerves that have been attacked by the host’s immune cells. | Positive | Bacillus (Th1) |
| Multibacillary | Midborderline or Borderline (“BB”) | A30.3 | Borderline | Borderline leprosy is of intermediate severity and is the most common form. Skin lesions resemble tuberculoid leprosy but are more numerous and irregular; large patches may affect a whole limb, and peripheral nerve involvement with weakness and loss of sensation is common. This type is unstable and may become lepromatous, or may undergo a reversal reaction, becoming more like the tuberculoid form. | ||
| Multibacillary | Borderline Lepromatous (“BL”), and Lepromatous (“LL”) | A30.4, A30.5 | Lepromatous | It is associated with symmetric skin lesions, nodules, plaques, thickened dermis and frequent involvement of the nasal mucosa resulting in nasal congestion and epistaxis but detectable nerve damage is late. | Negative | Plasmid inside Bacillus (Th2) |
Ridley Jopling Classification
There are 6 classes in the Ridley Jopling classification scheme. This classification is based on the following:[4]
- Cutaneous elements
- Neurological elements
- Biopsy findings
- Immunological status
- Presence of acid-fast bacilli in dermis
Tuberculoid or Paucibacillary Pole
This is the least severe form of the disease. In this form of the disease the following are present:
- 1 to 3 well-defined lesions with central hypopigmented area and hypoesthesia
- Well-developed immune response
- Granulomatous inflammation
- Rare acid-fast bacilli
Skin
Ear
-
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/b/b4/Tuberculoid_leprosy40.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/8/84/Tuberculoid_leprosy81.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy40.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy81.jpg)
Trunk
-
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/6/6c/Tuberculoid_leprosy06.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/e/e6/Tuberculoid_leprosy17.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/c/cc/Tuberculoid_leprosy18.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/6/67/Tuberculoid_leprosy27.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/1/1d/Tuberculoid_leprosy36.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/3/38/Tuberculoid_leprosy41.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/a/ac/Tuberculoid_leprosy45.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/c/ca/Tuberculoid_leprosy49.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/6/60/Tuberculoid_leprosy50.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/e/ea/Tuberculoid_leprosy56.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/a/a1/Tuberculoid_leprosy57.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/5/51/Tuberculoid_leprosy58.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/4/49/Tuberculoid_leprosy62.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/e/e8/Tuberculoid_leprosy63.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/c/c2/Tuberculoid_leprosy64.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/a/a5/Tuberculoid_leprosy65.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/0/0f/Tuberculoid_leprosy66.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/f/f8/Tuberculoid_leprosy88.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy06.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy17.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy18.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy27.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy36.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy41.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy45.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy49.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy50.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy56.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy57.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy58.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy62.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy63.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy64.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy65.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy66.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy88.jpg)
Extremity
-
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/a/a5/Tuberculoid_leprosy01.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/f/f6/Tuberculoid_leprosy02.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/0/0a/Tuberculoid_leprosy03.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/2/24/Tuberculoid_leprosy04.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/2/2f/Tuberculoid_leprosy07.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/3/39/Tuberculoid_leprosy08.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/0/03/Tuberculoid_leprosy10.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/d/db/Tuberculoid_leprosy11.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/b/b9/Tuberculoid_leprosy12.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/0/0c/Tuberculoid_leprosy13.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/0/08/Tuberculoid_leprosy14.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/d/d6/Tuberculoid_leprosy16.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/e/ef/Tuberculoid_leprosy19.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/c/c9/Tuberculoid_leprosy20.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/f/f9/Tuberculoid_leprosy25.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/5/58/Tuberculoid_leprosy31.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/e/e5/Tuberculoid_leprosy32.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/3/30/Tuberculoid_leprosy34.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/7/79/Tuberculoid_leprosy35.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/7/79/Tuberculoid_leprosy37.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/b/bc/Tuberculoid_leprosy38.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/f/f4/Tuberculoid_leprosy39.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/c/c0/Tuberculoid_leprosy42.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/6/65/Tuberculoid_leprosy43.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/8/89/Tuberculoid_leprosy44.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/b/b6/Tuberculoid_leprosy51.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/2/22/Tuberculoid_leprosy52.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/3/33/Tuberculoid_leprosy53.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/9/9e/Tuberculoid_leprosy54.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/2/2c/Tuberculoid_leprosy55.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/4/4a/Tuberculoid_leprosy67.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/a/a4/Tuberculoid_leprosy68.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/c/c3/Tuberculoid_leprosy69.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/b/b1/Tuberculoid_leprosy70.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/7/7e/Tuberculoid_leprosy71.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/5/5e/Tuberculoid_leprosy73.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/e/e7/Tuberculoid_leprosy74.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/1/18/Tuberculoid_leprosy77.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/a/ad/Tuberculoid_leprosy78.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/4/4f/Tuberculoid_leprosy75.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/2/2e/Tuberculoid_leprosy79.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/7/71/Tuberculoid_leprosy80.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/9/9e/Tuberculoid_leprosy82.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/3/39/Tuberculoid_leprosy83.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/7/7b/Tuberculoid_leprosy84.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/5/50/Tuberculoid_leprosy86.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/5/58/Tuberculoid_leprosy87.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy01.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy02.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy03.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy04.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy07.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy08.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy10.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy11.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy12.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy13.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy14.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy16.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy19.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy20.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy25.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy31.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy32.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy34.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy35.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy37.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy38.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy39.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy42.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy43.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy44.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy51.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy52.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy53.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy54.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy55.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy67.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy68.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy69.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy70.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy71.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy73.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy74.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy77.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy78.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy75.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy79.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy80.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy82.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy83.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy84.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy86.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy87.jpg)
Genitalia
-
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/7/70/Tuberculoid_leprosy21.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/b/b4/Tuberculoid_leprosy22.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/f/fe/Tuberculoid_leprosy23.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/4/4d/Tuberculoid_leprosy24.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/1/16/Tuberculoid_leprosy48.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/c/cf/Tuberculoid_leprosy47.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/2/2e/Tuberculoid_leprosy59.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/b/b6/Tuberculoid_leprosy60.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/4/45/Tuberculoid_leprosy61.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy21.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy22.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy23.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy24.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy48.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy47.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy59.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy60.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy61.jpg)
Head
-
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/7/72/Tuberculoid_leprosy28.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/3/30/Tuberculoid_leprosy29.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/c/c2/Tuberculoid_leprosy30.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5] -
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/2/20/Tuberculoid_leprosy33.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy28.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy29.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy30.jpg)
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy33.jpg)
Gluteal Region
-
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/5/59/Tuberculoid_leprosy05.jpg) Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]
![Tuberculoid leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ATuberculoid_leprosy05.jpg)
Nodular leprosy of childhood
Face
-
![Nodular leprosy of childhood. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/0/01/Nodular_leprosy_of_childhood01.jpg) Nodular leprosy of childhood. Adapted from Dermatology Atlas.[5]
Nodular leprosy of childhood. Adapted from Dermatology Atlas.[5]
![Nodular leprosy of childhood. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ANodular_leprosy_of_childhood01.jpg)
Trunk
-
![Nodular leprosy of childhood. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/4/44/Nodular_leprosy_of_childhood02.jpg) Nodular leprosy of childhood. Adapted from Dermatology Atlas.[5]
Nodular leprosy of childhood. Adapted from Dermatology Atlas.[5] -
![Nodular leprosy of childhood. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/8/81/Nodular_leprosy_of_childhood03.jpg) Nodular leprosy of childhood. Adapted from Dermatology Atlas.[5]
Nodular leprosy of childhood. Adapted from Dermatology Atlas.[5]
![Nodular leprosy of childhood. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ANodular_leprosy_of_childhood02.jpg)
![Nodular leprosy of childhood. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ANodular_leprosy_of_childhood03.jpg)
Lepromatous or Multi-Bacillary Pole
In this form of the disease the following are present:
- Multiple undefined nodular lesions throughout the body
- Weak immune response
- Evidence of foamy macrophages in dermis filled with mycobacteria
- Patients are immunocompetent, despite not being able to fight mycobacterium leprae
Skin
Face
-
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/9/99/Lepromatous_leprosy01.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/f/f5/Lepromatous_leprosy02.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/e/ee/Lepromatous_leprosy11.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/e/eb/Lepromatous_leprosy12.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/2/29/Lepromatous_leprosy17.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/9/94/Lepromatous_leprosy22.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/a/a9/Lepromatous_leprosy25.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/0/06/Lepromatous_leprosy34.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/1/1d/Lepromatous_leprosy82.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/0/0e/Lepromatous_leprosy85.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/e/e2/Lepromatous_leprosy93.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/b/b2/Lepromatous_leprosy94.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/4/4b/Lepromatous_leprosy95.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy01.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy02.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy11.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy12.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy17.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy22.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy34.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy82.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy85.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy93.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy94.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy95.jpg)
Trunk
-
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/2/2b/Lepromatous_leprosy03.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/9/9c/Lepromatous_leprosy04.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/b/b2/Lepromatous_leprosy05.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/d/d6/Lepromatous_leprosy06.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/d/df/Lepromatous_leprosy07.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/c/c6/Lepromatous_leprosy08.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/f/f5/Lepromatous_leprosy14.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/7/79/Lepromatous_leprosy29.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/5/5d/Lepromatous_leprosy37.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/7/73/Lepromatous_leprosy38.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/d/d9/Lepromatous_leprosy39.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/3/30/Lepromatous_leprosy41.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/8/87/Lepromatous_leprosy42.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/6/6d/Lepromatous_leprosy43.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/7/75/Lepromatous_leprosy44.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/d/db/Lepromatous_leprosy45.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/0/04/Lepromatous_leprosy47.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/3/38/Lepromatous_leprosy57.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/c/cc/Lepromatous_leprosy59.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/2/2d/Lepromatous_leprosy60.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/e/e1/Lepromatous_leprosy61.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/e/ed/Lepromatous_leprosy63.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/6/64/Lepromatous_leprosy64.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/1/11/Lepromatous_leprosy69.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/e/e1/Lepromatous_leprosy70.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/b/b7/Lepromatous_leprosy71.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/9/95/Lepromatous_leprosy77.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/3/3d/Lepromatous_leprosy78.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/f/ff/Lepromatous_leprosy86.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/b/b3/Lepromatous_leprosy87.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/c/c2/Lepromatous_leprosy88.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/5/55/Lepromatous_leprosy90.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/d/d3/Lepromatous_leprosy89.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/b/b6/Lepromatous_leprosy92.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/9/92/Lepromatous_leprosy96.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/9/9c/Lepromatous_leprosy97.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/c/c4/Lepromatous_leprosy98.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy03.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy04.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy05.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy06.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy07.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy08.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy14.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy29.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy37.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy38.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy39.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy41.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy42.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy43.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy44.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy45.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy47.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy57.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy59.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy60.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy61.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy63.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy64.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy69.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy70.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy71.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy77.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy78.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy86.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy87.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy88.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy90.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy89.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy92.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy96.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy97.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy98.jpg)
Extremity
-
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/e/e7/Lepromatous_leprosy10.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/d/d4/Lepromatous_leprosy13.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/d/d2/Lepromatous_leprosy15.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/8/8b/Lepromatous_leprosy16.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/1/14/Lepromatous_leprosy19.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/5/5e/Lepromatous_leprosy20.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/9/98/Lepromatous_leprosy21.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/b/b1/Lepromatous_leprosy24.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/8/8f/Lepromatous_leprosy26.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/2/2b/Lepromatous_leprosy30.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/d/d8/Lepromatous_leprosy31.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/a/ac/Lepromatous_leprosy32.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/0/0b/Lepromatous_leprosy33.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/4/4f/Lepromatous_leprosy46.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/a/ac/Lepromatous_leprosy48.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/5/53/Lepromatous_leprosy49.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/5/50/Lepromatous_leprosy50.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/0/07/Lepromatous_leprosy51.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/5/51/Lepromatous_leprosy52.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/8/8b/Lepromatous_leprosy53.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/e/ea/Lepromatous_leprosy54.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/6/60/Lepromatous_leprosy55.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/0/0d/Lepromatous_leprosy56.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/f/f5/Lepromatous_leprosy58.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/6/67/Lepromatous_leprosy62.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/f/f9/Lepromatous_leprosy65.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/b/be/Lepromatous_leprosy66.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/3/3a/Lepromatous_leprosy67.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/7/7d/Lepromatous_leprosy68.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/c/c0/Lepromatous_leprosy72.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/5/5e/Lepromatous_leprosy73.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/c/c7/Lepromatous_leprosy74.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/2/2d/Lepromatous_leprosy75.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/5/5e/Lepromatous_leprosy76.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/1/1f/Lepromatous_leprosy79.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/5/57/Lepromatous_leprosy80.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/5/54/Lepromatous_leprosy81.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/a/a0/Lepromatous_leprosy91.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/f/f3/Lepromatous_leprosy99.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/8/85/Lepromatous_leprosy100.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5] -
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/images/3/3f/Lepromatous_leprosy101.jpg) Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
Lepromatous leprosy. Adapted from Dermatology Atlas.[5]
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy10.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy13.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy15.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy16.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy19.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy20.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy21.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy24.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy26.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy30.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy31.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy32.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy33.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy46.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy48.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy49.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy50.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy51.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy52.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy53.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy54.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy55.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy56.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy58.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy62.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy65.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy66.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy67.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy68.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy72.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy73.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy74.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy75.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy76.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy79.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy80.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy81.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy91.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy99.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy100.jpg)
![Lepromatous leprosy. Adapted from Dermatology Atlas.[5]](https://www.wikidoc.org/index.php/File%3ALepromatous_leprosy101.jpg)
Ear
Image:Lepromatous leprosy09.jpg|Lepromatous leprosy. Adapted from Dermatology Atlas.[5] Image:Lepromatous leprosy18.jpg|Lepromatous leprosy. Adapted from Dermatology Atlas.[5] Image:Lepromatous leprosy23.jpg|Lepromatous leprosy. Adapted from Dermatology Atlas.[5] Image:Lepromatous leprosy27.jpg|Lepromatous leprosy. Adapted from Dermatology Atlas.[5] Image:Lepromatous leprosy28.jpg|Lepromatous leprosy. Adapted from Dermatology Atlas.[5] Image:Lepromatous leprosy35.jpg|Lepromatous leprosy. Adapted from Dermatology Atlas.[5] Image:Lepromatous leprosy36.jpg|Lepromatous leprosy. Adapted from Dermatology Atlas.[5] Image:Lepromatous leprosy40.jpg|Lepromatous leprosy. Adapted from Dermatology Atlas.[5] Image:Lepromatous leprosy83.jpg|Lepromatous leprosy. Adapted from Dermatology Atlas.[5] </gallery>
Intermediate, Dimorphous or Borderline State
This last category is divided into 3 subcategories:
Borderline Tuberculoid, or BT
In this form of the disease the following are present:
- Progression towards the tuberculoid pole
- Increasing cell-mediated immunity
- Inflammation of the nerves and skin
Mid-Borderline, Borderline-Borderline, or BB
This is considered to be where the disease usually begins, progressing towards one of the poles afterwards.[1]
Borderline Lepromatous, or BL
In this form of the disease the following are present:
- Progression towards the lepromatous pole
- Common before treatment initiation
- Loss of cell-mediated immunity
Indeterminate
In this form of the disease the following are present:
- Early unspecific lesions
- Nerve infiltrates, lacking required criteria for being classified as above mentioned
- Used only when there is diagnostic proof of leprosy, from a biopsy sample, with evidence of mycobacterium leprae and perineural infiltrates but the disease is not advanced enough to show the clear patient position in the leprosy classification.
Skin
Extremity
-
 Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite
Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite -
 Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite
Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite -
 Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite
Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite -
 Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite
Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite -
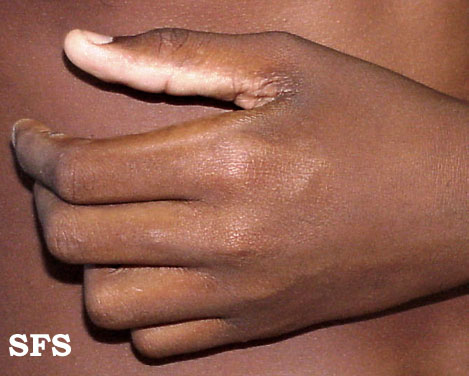 Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite
Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite -
 Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite
Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite -
 Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite
Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite -
 Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite
Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite -
 Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite
Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite









Trunk
-
 Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite
Indeterminate leprosr. Adapted from Dermatology Atlas.<ref name=”Dermatology Atlas”>{{Cite

WHO classification
The WHO organization classification scheme is simpler, and it is based upon the number of skin lesions. This simpler classification scheme can be applied in the absence of laboratory support or clinical expertise. It allows a rapid diagnosis, selection and initiation of treatment. The leprosy subtypes include:[6][4]
Paucibacillary or PB
- Higher level of immunity
- Lower number of bacilli
- Up to five skin lesions in total body examination
- Requires less intensive treatment
Multibacillary or MB
- Lower level of immunity
- Higher number of bacilli
- Six or more skin lesions in total body examination
- Requires intensive treatment
If a skin smear is done and shows a positive result, then that patient will immediately be classified as multibacillary, irrespective of the number of skin lesions identified on physical examination. Despite its ease of use, this classification scheme may unfortunately mis-classify some patients resulting in under treatment of those cases.
References
- ↑ 1.0 1.1 Walker, Stephen L.; Lockwood, Dina N.J. (2007). “Leprosy”. Clinics in Dermatology. 25 (2): 165–172. doi:10.1016/j.clindermatol.2006.05.012. ISSN 0738-081X.
- ↑ Eichelmann, K.; González González, S.E.; Salas-Alanis, J.C.; Ocampo-Candiani, J. (2013). “Leprosy. An Update: Definition, Pathogenesis, Classification, Diagnosis, and Treatment”. Actas Dermo-Sifiliográficas (English Edition). 104 (7): 554–563. doi:10.1016/j.adengl.2012.03.028. ISSN 1578-2190.
- ↑ Bhat, Ramesh Marne; Prakash, Chaitra (2012). “Leprosy: An Overview of Pathophysiology”. Interdisciplinary Perspectives on Infectious Diseases. 2012: 1–6. doi:10.1155/2012/181089. ISSN 1687-708X.
- ↑ 4.0 4.1 Pardillo FE, Fajardo TT, Abalos RM, Scollard D, Gelber RH (2007). “Methods for the classification of leprosy for treatment purposes”. Clin Infect Dis. 44 (8): 1096–9. doi:10.1086/512809. PMID 17366457.
- ↑ 5.000 5.001 5.002 5.003 5.004 5.005 5.006 5.007 5.008 5.009 5.010 5.011 5.012 5.013 5.014 5.015 5.016 5.017 5.018 5.019 5.020 5.021 5.022 5.023 5.024 5.025 5.026 5.027 5.028 5.029 5.030 5.031 5.032 5.033 5.034 5.035 5.036 5.037 5.038 5.039 5.040 5.041 5.042 5.043 5.044 5.045 5.046 5.047 5.048 5.049 5.050 5.051 5.052 5.053 5.054 5.055 5.056 5.057 5.058 5.059 5.060 5.061 5.062 5.063 5.064 5.065 5.066 5.067 5.068 5.069 5.070 5.071 5.072 5.073 5.074 5.075 5.076 5.077 5.078 5.079 5.080 5.081 5.082 5.083 5.084 5.085 5.086 5.087 5.088 5.089 5.090 5.091 5.092 5.093 5.094 5.095 5.096 5.097 5.098 5.099 5.100 5.101 5.102 5.103 5.104 5.105 5.106 5.107 5.108 5.109 5.110 5.111 5.112 5.113 5.114 5.115 5.116 5.117 5.118 5.119 5.120 5.121 5.122 5.123 5.124 5.125 5.126 5.127 5.128 5.129 5.130 5.131 5.132 5.133 5.134 5.135 5.136 5.137 5.138 5.139 5.140 5.141 5.142 5.143 5.144 5.145 5.146 5.147 5.148 5.149 5.150 5.151 5.152 5.153 5.154 5.155 5.156 5.157 5.158 5.159 5.160 5.161 5.162 5.163 5.164 5.165 5.166 5.167 5.168 5.169 5.170 5.171 5.172 5.173 5.174 5.175 5.176 5.177 5.178 5.179 5.180 5.181 5.182 5.183 “Dermatology Atlas”.
- ↑ “Enhanced global strategy for further reducing the disease burden due to leprosy (2011-2015)” (PDF).
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: João André Alves Silva, M.D. [2]
Overview
The clinical manifestations of leprosy largely reflect the immune response of the host towards the infection. Once the bacterial cells penetrate and multiply within the hosts skin and peripheral nerve cells, the immune system mounts a response toward the infected cells, which results in clinical symptoms. Several single-nucleotide polymorphisms such as TNF-α, IL-10, IFN-γ, TLR 1 have been associated with a greater susceptibility to leprosy as have other genetic markers.
Genetics
The infection by the mycobacterium leprae and the course of the disease are influenced by genetic factors in the host.[1][2] Some single-nucleotide polymorphism have been associated with a higher incidence of leprosy. These include:[1][3][4][5][6]
- Low occurrence of a lymphotoxin-α-producing allele
- Vitamin D receptor gene.
- TNF-α gene
- IL-10 gene
- IFN-γ gene
- TLR 1 gene
Another study has suggested a possible relationship between genetic variants of the NOD2 gene, increased susceptibility to leprosy and the development of type I and II reactions.[7]
It has also been suggested an association between leprosy and a locus in chromosome 10p13, in the proximity of the mannose receptor 1 gene. Since the mannose receptors are located on the macrophage‘s surface, they play an important role in phagocytosis.[8]
Additionally, the subtype of leprosy developed in a patient has been associated with genes of the class II HLA/major histocompatibility complex, at chromosome 6. Accordingly:
- HLA-DR2 and HLA-DR3 are considered to be linked with the tuberculoid class.
- HLA-DQ1 is considered to be linked with the lepromatous class.
Pathogenesis
Mycobacterium leprae has predisposition to infect macrophages. It is usually collected inside these, in intracellular groups, called globi. This organism has an ideal growth temperature of 27-30ºC, which explains why it usually infects areas such as the skin, upper respiratory mucosa and peripheral nerves. It is able to infect cells, particularly due to 2 structures:[9][10][11][12]
- Capsule – target of intense humoral immune response (immunoglobulin M-mediated).
- Cell wall – particularly the lipoarabinomannan, works as an antigen for the macrophages.
The bacillus is known to target Schwann cells, specifically the G domain of the laminin-α2 chain. This domain is predominantly expressed in the basal lamina of peripheral nerves, thereby explaining the neuropathy felt in this condition. The pathogen then penetrates the cell, at which time it will multiply, until the infected cell is finally recognized by the immune system and a an inflammatory reaction is started.[9][13]
This mechanism explains the reason why the clinical manifestations of the disease will depend on the immunologic status of the patient and the intensity of the response developed following the infection of the host cells.[9]
Transmission
The locations of the body thought to be the source of transmission of Mycobacterium leprae include:
- Skin – studies have shown presence of large amounts of bacteria in the dermis of leprosy patients, however, it is not known if these are able to reach the epidermis in order to be transmitted to other individuals.[1][14] Conflicting reports have been issued on this matter, therefore whether or not the bacteria are able to reach the cell surface, remains uncertain.[15]A study showed presence of these organisms in sebaceous secretions of lepromatous leprosy patients, which leads to the hypothesis that these pathogens may exist the host’s body through this manner.[16]
- Nasal mucosa – secretions from the nasal mucosa of lepromatous patients are rich in viable mycobacterium leprae, and may therefore be a source of transmission.[17][1]
The entry route into the human body is also still unknown, however, recent studies point to a predominance of the respiratory route as well.[1][18][19]
Associated Conditions
Leprosy Among Patients with HIV
There is no increased susceptibility to Mycobacterium leprae in HIV patients, nor are the clinical features altered. After initiation of antiretroviral therapy, latent leprosy can become clinically apparent in an HIV patient once the immune response is reestablished.[20][21]
Gross Pathology
Type of Leprosy
Tuberculoid Leprosy
- May resolve spontaneously
- Well-defined macules
- Hypopigmented skin lesions
- Borders of lesions are commonly erythematous and elevated, with depressed centers
- Sensation on the face commonly unaffected
- Anhidrosis
- Loss of adnexal structures
Lepromatous Leprosy
- Papules and nodules, usually bilateral, symmetrical with ovoid shape
- Leonine facies
- Severe nerve involvement
Immunologic Reactions
Systemic inflammatory reactions may occur before, during or after the treatment of leprosy.[22] These are thought to be related to changes in the immune system, such as following stressful situations, pregnancy or leprosy medications.[9] There are two different types of reactions, which are thought to have different underlying immunologic mechanisms:
Tipe 1 (T1R) or Reversal Reaction (RR)
- Predominant in borderline disease
- Predominant type IV hypersensitivity[23]
- Red patches developing in previous skin lesions, commonly on the face or nerve trunks
- Erythema of previous skin lesions
- Inflammation may lead to nerve lesion and paralysis
- Edema of hands and feet
- Arthralgia, predominantly of smaller joints
- Ulcerated lesions
- Pain or tenderness on lesions
Type 2 (T2R) or Erythema Nodosum Leprosum (ENL)
- Predominant in lepromatous disease
- Predominant type III hypersensitivity
- Sudden occurrence of painful nodules
- Nodules may lead to pustules or ulcers
- Pustules may discharge pus containing polymorphonuclear cells and degenerating mycobacteria
- After lesions resolve, brawn skin lesions may remain
- Occasionally may occur: orchitis, muscle and lymphadenopathy tenderness and/or swollen joints
- Without treatment usually lasts for 2 weeks
Microscopic Pathology
Histopathology
The clinical manifestations of leprosy depend on the host’s immune response towards the mycobacteria. Therefore, tuberculoid and lepromatous patients will show different histopathologic findings:[1][22][24]
Tuberculoid patients
These patients will show a strong immune response towards the bacteria, with:
- Production of IFN-γ
- Inflammatory infiltrate with multiple granulomas
- Granulomas containing giant cells, differentiated macrophages and epithelioid cells
- Predominance of CD4 cells
- Low bacterial index
- Commonly positive lepromin skin test
Lepromatous patients
These patients will show a weaker immune response, with:
- Weak cell-mediated response
- Absence of granulomas
- Straightened skin
- Predominance of CD8 cells
- High bacterial index
Gallery
-
![Case of lepromatous or multibacillary leprosy, with photomicrograph revealing histopathologic changes in human testicular tissue, including a large number of “foam cells”. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]](https://www.wikidoc.org/images/8/88/Leprosy-18.jpg) Case of lepromatous or multibacillary leprosy, with photomicrograph revealing histopathologic changes in human testicular tissue, including a large number of “foam cells”. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]
Case of lepromatous or multibacillary leprosy, with photomicrograph revealing histopathologic changes in human testicular tissue, including a large number of “foam cells”. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25] -
![Acid-fast-stained photomicrograph of tissue sample from a patient with leprosy, revealing chronic inflammatory lesion (granuloma) within which numerous red-colored Mycobacterium leprae bacteria are visible. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]](https://www.wikidoc.org/images/f/f1/Leprosy-27.jpg) Acid-fast-stained photomicrograph of tissue sample from a patient with leprosy, revealing chronic inflammatory lesion (granuloma) within which numerous red-colored Mycobacterium leprae bacteria are visible. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]
Acid-fast-stained photomicrograph of tissue sample from a patient with leprosy, revealing chronic inflammatory lesion (granuloma) within which numerous red-colored Mycobacterium leprae bacteria are visible. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25] -
![Photomicrograph of a skin tissue sample from patient with leprosy revealing cutaneous nerve, which had been invaded by numerous Mycobacterium leprae bacteria. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]](https://www.wikidoc.org/images/7/7a/Leprosy-28.jpg) Photomicrograph of a skin tissue sample from patient with leprosy revealing cutaneous nerve, which had been invaded by numerous Mycobacterium leprae bacteria. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]
Photomicrograph of a skin tissue sample from patient with leprosy revealing cutaneous nerve, which had been invaded by numerous Mycobacterium leprae bacteria. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25] -
![Photomicrograph of histopathologic changes in skin section extracted from a case of leprosy, possibly tuberculoid form, is uncertain. Note depicted here a nerve, which had been surrounded by dense infiltrate of undifferentiated histiocytes and many lymphocytes. The nerve sheath and endoneural region were also infiltrated. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]](https://www.wikidoc.org/images/4/44/Leprosy-30.jpg) Photomicrograph of histopathologic changes in skin section extracted from a case of leprosy, possibly tuberculoid form, is uncertain. Note depicted here a nerve, which had been surrounded by dense infiltrate of undifferentiated histiocytes and many lymphocytes. The nerve sheath and endoneural region were also infiltrated. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]
Photomicrograph of histopathologic changes in skin section extracted from a case of leprosy, possibly tuberculoid form, is uncertain. Note depicted here a nerve, which had been surrounded by dense infiltrate of undifferentiated histiocytes and many lymphocytes. The nerve sheath and endoneural region were also infiltrated. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25] -
![Light photomicrograph revealing histopathologic cytoarchitectural characteristics in a mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]](https://www.wikidoc.org/images/f/f6/Leprosy-34.jpg) Light photomicrograph revealing histopathologic cytoarchitectural characteristics in a mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]
Light photomicrograph revealing histopathologic cytoarchitectural characteristics in a mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25] -
![Light photomicrograph revealing histopathologic cytoarchitectural characteristics seen in mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]](https://www.wikidoc.org/images/7/79/Leprosy-35.jpg) Light photomicrograph revealing histopathologic cytoarchitectural characteristics seen in mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]
Light photomicrograph revealing histopathologic cytoarchitectural characteristics seen in mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25] -
![Light photomicrograph revealing histopathologic cytoarchitectural characteristics seen in mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]](https://www.wikidoc.org/images/6/60/Leprosy-36.jpg) Light photomicrograph revealing histopathologic cytoarchitectural characteristics seen in mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]
Light photomicrograph revealing histopathologic cytoarchitectural characteristics seen in mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25] -
![Light photomicrograph revealing histopathologic cytoarchitectural characteristics seen in mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]](https://www.wikidoc.org/images/9/93/Leprosy-37.jpg) Light photomicrograph revealing histopathologic cytoarchitectural characteristics seen in mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]
Light photomicrograph revealing histopathologic cytoarchitectural characteristics seen in mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25] -
![Light photomicrograph revealing histopathologic cytoarchitectural characteristics seen in mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]](https://www.wikidoc.org/images/b/b5/Leprosy-38.jpg) Light photomicrograph revealing histopathologic cytoarchitectural characteristics seen in mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]
Light photomicrograph revealing histopathologic cytoarchitectural characteristics seen in mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]
![Case of lepromatous or multibacillary leprosy, with photomicrograph revealing histopathologic changes in human testicular tissue, including a large number of “foam cells”. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]](https://www.wikidoc.org/index.php/File%3ALeprosy-18.jpg)
![Acid-fast-stained photomicrograph of tissue sample from a patient with leprosy, revealing chronic inflammatory lesion (granuloma) within which numerous red-colored Mycobacterium leprae bacteria are visible. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]](https://www.wikidoc.org/index.php/File%3ALeprosy-27.jpg)
![Photomicrograph of a skin tissue sample from patient with leprosy revealing cutaneous nerve, which had been invaded by numerous Mycobacterium leprae bacteria. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]](https://www.wikidoc.org/index.php/File%3ALeprosy-28.jpg)
![Photomicrograph of histopathologic changes in skin section extracted from a case of leprosy, possibly tuberculoid form, is uncertain. Note depicted here a nerve, which had been surrounded by dense infiltrate of undifferentiated histiocytes and many lymphocytes. The nerve sheath and endoneural region were also infiltrated. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]](https://www.wikidoc.org/index.php/File%3ALeprosy-30.jpg)
![Light photomicrograph revealing histopathologic cytoarchitectural characteristics in a mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]](https://www.wikidoc.org/index.php/File%3ALeprosy-34.jpg)
![Light photomicrograph revealing histopathologic cytoarchitectural characteristics seen in mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]](https://www.wikidoc.org/index.php/File%3ALeprosy-35.jpg)
![Light photomicrograph revealing histopathologic cytoarchitectural characteristics seen in mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]](https://www.wikidoc.org/index.php/File%3ALeprosy-36.jpg)
![Light photomicrograph revealing histopathologic cytoarchitectural characteristics seen in mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]](https://www.wikidoc.org/index.php/File%3ALeprosy-37.jpg)
![Light photomicrograph revealing histopathologic cytoarchitectural characteristics seen in mycobacterial skin infection. Adapted from Public Health Image Library (PHIL), Centers for Disease Control and Prevention.[25]](https://www.wikidoc.org/index.php/File%3ALeprosy-38.jpg)
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 Bhat, Ramesh Marne; Prakash, Chaitra (2012). “Leprosy: An Overview of Pathophysiology”. Interdisciplinary Perspectives on Infectious Diseases. 2012: 1–6. doi:10.1155/2012/181089. ISSN 1687-708X.
- ↑ Alter A, Alcaïs A, Abel L, Schurr E (2008). “Leprosy as a genetic model for susceptibility to common infectious diseases”. Hum Genet. 123 (3): 227–35. doi:10.1007/s00439-008-0474-z. PMID 18247059.
- ↑ Alcaïs A, Alter A, Antoni G, Orlova M, Nguyen VT, Singh M; et al. (2007). “Stepwise replication identifies a low-producing lymphotoxin-alpha allele as a major risk factor for early-onset leprosy”. Nat Genet. 39 (4): 517–22. doi:10.1038/ng2000. PMID 17353895.
- ↑ Mira MT, Alcais A, di Pietrantonio T, Thuc NV, Phuong MC, Abel L; et al. (2003). “Segregation of HLA/TNF region is linked to leprosy clinical spectrum in families displaying mixed leprosy subtypes”. Genes Immun. 4 (1): 67–73. doi:10.1038/sj.gene.6363911. PMID 12595904.
- ↑ Correa-Oliveira, Rodrigo; Misch, Elizabeth A.; Macdonald, Murdo; Ranjit, Chaman; Sapkota, Bishwa R.; Wells, Richard D.; Siddiqui, M. Ruby; Kaplan, Gilla; Hawn, Thomas R. (2008). “Human TLR1 Deficiency Is Associated with Impaired Mycobacterial Signaling and Protection from Leprosy Reversal Reaction”. PLoS Neglected Tropical Diseases. 2 (5): e231. doi:10.1371/journal.pntd.0000231. ISSN 1935-2735.
- ↑ Cardoso CC, Pereira AC, Brito-de-Souza VN, Dias-Baptista IM, Maniero VC, Venturini J; et al. (2010). “IFNG +874 T>A single nucleotide polymorphism is associated with leprosy among Brazilians”. Hum Genet. 128 (5): 481–90. doi:10.1007/s00439-010-0872-x. PMID 20714752.
- ↑ Berrington WR, Macdonald M, Khadge S, Sapkota BR, Janer M, Hagge DA; et al. (2010). “Common polymorphisms in the NOD2 gene region are associated with leprosy and its reactive states”. J Infect Dis. 201 (9): 1422–35. doi:10.1086/651559. PMC 2853728. PMID 20350193.
- ↑ Alter A, Grant A, Abel L, Alcaïs A, Schurr E (2011). “Leprosy as a genetic disease”. Mamm Genome. 22 (1–2): 19–31. doi:10.1007/s00335-010-9287-1. PMID 20936290.
- ↑ 9.0 9.1 9.2 9.3 Eichelmann, K.; González González, S.E.; Salas-Alanis, J.C.; Ocampo-Candiani, J. (2013). “Leprosy. An Update: Definition, Pathogenesis, Classification, Diagnosis, and Treatment”. Actas Dermo-Sifiliográficas (English Edition). 104 (7): 554–563. doi:10.1016/j.adengl.2012.03.028. ISSN 1578-2190.
- ↑ Eichelmann K, González González SE, Salas-Alanis JC, Ocampo-Candiani J (2013). “Leprosy. An update: definition, pathogenesis, classification, diagnosis, and treatment”. Actas Dermosifiliogr. 104 (7): 554–63. doi:10.1016/j.adengl.2012.03.028. PMID 23870850.
- ↑ Britton, Warwick J; Lockwood, Diana NJ (2004). “Leprosy”. The Lancet. 363 (9416): 1209–1219. doi:10.1016/S0140-6736(04)15952-7. ISSN 0140-6736.
- ↑ Gulia, Andrea; Fried, Isabella; Massone, Cesare (2010). “New insights in the pathogenesis and genetics of leprosy”. F1000 Medicine Reports. 2. doi:10.3410/M2-30. ISSN 1757-5931.
- ↑ Shimoji Y, Ng V, Matsumura K, Fischetti VA, Rambukkana A (1999). “A 21-kDa surface protein of Mycobacterium leprae binds peripheral nerve laminin-2 and mediates Schwann cell invasion”. Proc Natl Acad Sci U S A. 96 (17): 9857–62. PMC 22300. PMID 10449784.
- ↑ Scollard DM, Joyce MP, Gillis TP (2006). “Development of leprosy and type 1 leprosy reactions after treatment with infliximab: a report of 2 cases”. Clin Infect Dis. 43 (2): e19–22. doi:10.1086/505222. PMID 16779736.
- ↑ Truman R (2005). “Leprosy in wild armadillos”. Lepr Rev. 76 (3): 198–208. PMID 16248207.
- ↑ Valverde CR, Canfield D, Tarara R, Esteves MI, Gormus BJ (1998). “Spontaneous leprosy in a wild-caught cynomolgus macaque”. Int J Lepr Other Mycobact Dis. 66 (2): 140–8. PMID 9728446.
- ↑ Gillis T, Vissa V, Matsuoka M, Young S, Richardus JH, Truman R; et al. (2009). “Characterisation of short tandem repeats for genotyping Mycobacterium leprae”. Lepr Rev. 80 (3): 250–60. PMID 19994470.
- ↑ Han XY, Sizer KC, Tan HH (2012). “Identification of the leprosy agent Mycobacterium lepromatosis in Singapore”. J Drugs Dermatol. 11 (2): 168–72. PMID 22270197.
- ↑ Han XY, Sizer KC, Thompson EJ, Kabanja J, Li J, Hu P; et al. (2009). “Comparative sequence analysis of Mycobacterium leprae and the new leprosy-causing Mycobacterium lepromatosis”. J Bacteriol. 191 (19): 6067–74. doi:10.1128/JB.00762-09. PMC 2747882. PMID 19633074.
- ↑ Walker, Stephen L.; Lockwood, Dina N.J. (2007). “Leprosy”. Clinics in Dermatology. 25 (2): 165–172. doi:10.1016/j.clindermatol.2006.05.012. ISSN 0738-081X.
- ↑ Ustianowski AP, Lawn SD, Lockwood DN (2006). “Interactions between HIV infection and leprosy: a paradox”. Lancet Infect Dis. 6 (6): 350–60. doi:10.1016/S1473-3099(06)70493-5. PMID 16728321.
- ↑ 22.0 22.1 Modlin RL, Hofman FM, Taylor CR, Rea TH (1983). “T lymphocyte subsets in the skin lesions of patients with leprosy”. J Am Acad Dermatol. 8 (2): 182–9. PMID 6219136.
- ↑ Balagon, M. V. F.; Gelber, R. H.; Abalos, R. M.; Cellona, R. V. (2010). “Reactions Following Completion of 1 and 2 Year Multidrug Therapy (MDT)”. American Journal of Tropical Medicine and Hygiene. 83 (3): 637–644. doi:10.4269/ajtmh.2010.09-0586. ISSN 0002-9637.
- ↑ Wallach D, Flageul B, Bach MA, Cottenot F (1984). “The cellular content of dermal leprous granulomas: an immuno-histological approach”. Int J Lepr Other Mycobact Dis. 52 (3): 318–26. PMID 6332791.
- ↑ 25.0 25.1 25.2 25.3 25.4 25.5 25.6 25.7 25.8 “Public Health Image Library (PHIL), Centers for Disease Control and Prevention”.
Causes
 |
 |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: João André Alves Silva, M.D. [2]
Overview
Mycobacterium leprae is a gram-positive obligate intracellular, acid-fast bacillus, responsible for the development of leprosy, or Hansen’s disease. This organism has a very slow growth and has a predilection to affect colder parts of the body, such as the skin, superficial nerves and upper respiratory mucous membranes. Although a route of transmission has not been absolutely defined yet, studies are pointing to a colonization of the dermis and respiratory mucosa of the infected patients. It is an uncommon bacteria, since it has only been noticed to infect and grow in some species of primates and in the nine-banded armadillo.[1]
Taxonomy
Bacteria; Actinobacteria; Actinobacteria; Actinobacteridae; Actinomycetales; Corynebacterineae; Mycobacteriaceae; Mycobacterium[2][3]
- Mycobacterium leprae
- Mycobacterium leprae 3125609
- Mycobacterium leprae 7935681
- Mycobacterium leprae Br4923
- Mycobacterium leprae Kyoto-2
- Mycobacterium leprae TN
- Mycobacterium lepromatosis
Biology
Mycobacterium leprae and Mycobacterium lepromatosis are the causative agents of leprosy. M. lepromatosis is a relatively newly identified mycobacterium isolated from a fatal case of diffuse lepromatous leprosy in 2008.[4][5]
Mycobacterium leprae a gram-positive bacterium that causes leprosy (Hansen’s disease).[5] It is an intracellular, pleomorphic, acid-fast bacterium.[6] M. leprae is a slow growing aerobic bacillus with a replication period that usually takes 11 – 13 days, surrounded by a characteristic waxy coating, unique to mycobacteria. In size and shape, it closely resembles Mycobacterium tuberculosis. [6]
Due to extensive loss of genes necessary for independent growth, M. leprae and M. lepromatosis are obligate intracellular parasites, and unculturable in the laboratory, a factor that leads to difficulty in definitively identifying the organism under a strict interpretation of Koch’s postulates.[4][7] Due to the slow onset of leprosy and the absence of adequate immunological tools, it is not possible to know the specific incubation period for Mycobacterium leprae, however, according to multiple sources, this period may be settled between 3 to 10 years, since exposure to the viable bacteria.[1][8][9]
Studies performed in animal models show that the ideal temperature for growth of the M. leprae is at 27 – 33ºC, which is compatible with the preferred location in the body of this pathogen, the skin, mucous membranes and nerves close to the skin. This also explains the growth of bacteria in armadillos, since those animals have a core temperature of 34ºC.[10]
Origin
Leprosy, caused by Mycobacterium leprae is thought to have been originated in Middle Eastern countries, particularly in Egipt, around 2400 BC. Due to the lack of knowledge about the bacteria and treatment, the disease was then spread throughout the world. The Mycobacterium leprae would only be later discovered by G. H. Armauer Hansen in 1873, thereby being the first bacterium to be known as the cause of a human disease.[1]
Tropism
Mycobacterium leprae, unlike other mycobacteria, has tropism for cells of the peripheral nervous system, such as schwann cells, as well as for cells of the reticuloendothelial system.[11] This bacillus preferably infects macrophages, being collected in intracellular pockets called globi.[11]
Natural reservoir
Mycobacterium leprae is a bacillus with very specific needs for its growth. Until now, it has only been identified in 3 species of primates and in the nine-banded armadillo.[1][12]
While the causative organisms have been impossible to culture in vitro so far, it is possible to grow them in animals. Charles Shepard, chairman of the United States Leprosy Panel, successfully grew the organisms in the footpads of mice in 1960. This method was improved with the use of congenitally athymic mice (nude mice) in 1970 by Joseph Colson and Richard Hilson at St George’s Hospital, London.
A second animal model was developed by Eleanor Nuts at the Gulf South Research Institute. Dr Storrs had worked on the nine-banded armadillo for her PhD, because this animal had a lower body temperature than humans and might therefore be a suitable animal model. These experiments proved unsuccessful, but additional work in 1970 with material provided by Chapman Binford, medical director of the Leonard’s Wood Memorial, was successful. The papers describing this model led to a dispute of priority. Further controversy was generated when it was discovered that wild armadillos in Louisiana were naturally infected with leprosy.
References
- ↑ 1.0 1.1 1.2 1.3 Bhat, Ramesh Marne; Prakash, Chaitra (2012). “Leprosy: An Overview of Pathophysiology”. Interdisciplinary Perspectives on Infectious Diseases. 2012: 1–6. doi:10.1155/2012/181089. ISSN 1687-708X.
- ↑ “Taxonomy browser (Mycobacterium leprae)”.
- ↑ “Taxonomy browser (Mycobacterium lepromatosis)”.
- ↑ 4.0 4.1 “New Leprosy Bacterium: Scientists Use Genetic Fingerprint To Nail ‘Killing Organism‘“. ScienceDaily. 2008-11-28. Retrieved 2010-01-31.
- ↑ 5.0 5.1 Kenneth J. Ryan, C. George Ray, editors. (2004). Ryan KJ, Ray CG, ed. Sherris Medical Microbiology (4th ed.). McGraw Hill. pp. 451–3. ISBN 0-8385-8529-9. OCLC 52358530 61405904 Check
|oclc=value (help). - ↑ 6.0 6.1 McMurray DN (1996). “Mycobacteria and Nocardia.”. In Baron S. et al., eds. Baron’s Medical Microbiology (4th ed.). University of Texas Medical Branch. ISBN 0-9631172-1-1.
- ↑ Bhattacharya S, Vijayalakshmi N, Parija SC (1 October 2002). “Uncultivable bacteria: Implications and recent trends towards identification”. Indian journal of medical microbiology. 20 (4): 174–7. PMID 17657065.
- ↑ Han XY, Jessurun J (2013). “Severe leprosy reactions due to Mycobacterium lepromatosis”. Am J Med Sci. 345 (1): 65–9. doi:10.1097/MAJ.0b013e31826af5fb. PMC 3529828. PMID 23111393.
- ↑ Gillis TP, Scollard DM, Lockwood DN (2011). “What is the evidence that the putative Mycobacterium lepromatosis species causes diffuse lepromatous leprosy?”. Lepr Rev. 82 (3): 205–9. PMID 22125927.
- ↑ Scollard DM, Adams LB, Gillis TP, Krahenbuhl JL, Truman RW, Williams DL (2006). “The continuing challenges of leprosy”. Clin Microbiol Rev. 19 (2): 338–81. doi:10.1128/CMR.19.2.338-381.2006. PMC 1471987. PMID 16614253.
- ↑ 11.0 11.1 Eichelmann, K.; González González, S.E.; Salas-Alanis, J.C.; Ocampo-Candiani, J. (2013). “Leprosy. An Update: Definition, Pathogenesis, Classification, Diagnosis, and Treatment”. Actas Dermo-Sifiliográficas (English Edition). 104 (7): 554–563. doi:10.1016/j.adengl.2012.03.028. ISSN 1578-2190.
- ↑ Lockwood, Diana; Moet, Fake J.; Schuring, Ron P.; Pahan, David; Oskam, Linda; Richardus, Jan Hendrik (2008). “The Prevalence of Previously Undiagnosed Leprosy in the General Population of Northwest Bangladesh”. PLoS Neglected Tropical Diseases. 2 (2): e198. doi:10.1371/journal.pntd.0000198. ISSN 1935-2735.
Differentiating Leprosy from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: João André Alves Silva, M.D. [2]
Overview
Leprosy must be differentiated from other diseases that cause skin lesions, nodules, plaques paresthesias and nerve pain, such as autoimmune diseases, SLE, parasitic infections, vitiligo or cutaneous tuberculosis.
Differential diagnosis
Leprosy has a wide range of clinical manifestations, each with different degrees of intensity. Other diseases that may mimic, or have similar features of leprosy, include:[1]
- Congenital lesions – such as nevus depigmentosus are generally present at birth and do not present with changes in sensation.
- Vitiligo – a benign lesion that presents with depigmented areas, instead of hypopigmented.
- Pityriasis alba – may be hard to distinguish from leprosy, particularly in early stages of the second, however, it is a common skin condition, mostly occurring in children and usually seen as dry, fine scaled, pale patches on their faces.[2]
- Pityriasis versicolor – common skin infection caused by the yeast Malassezia furfur. This yeast is normally found on the human skin and only becomes troublesome under certain circumstances, such as a warm and humid environment, causing: generally oval or irregularly-shaped spots of 1/4 to 1 inch in diameter, often merging together to form a larger patch with a sharp border; occasional fine scaling of the skin producing a very superficial ash-like scale; and pale, dark tan, or pink in color spots, with a reddish undertone that can darken when the patient is overheated, such as in a hot shower or during/after exercise.
- Dermatophyte – parasitic fungus that infects the the skin, hair and nails due to its ability to obtain nutrients from keratinized material. The infection is usually restricted to the nonliving cornified layer of the epidermis because of their inability to penetrate viable tissue of an immunocompetent host.
- Systemic Lupus Erythematosus – potential fatal chronic autoimmune disease, common initial and chronic complaints include skin rash, fever, malaise, joint pains, myalgias and fatigue.
- Postinflammatory hypopigmented skin – a cutaneous condition characterized by decreased pigment in the skin following inflammatory reaction of the skin.
- Granuloma multiforme – a cutaneous condition most commonly seen in central Africa, and rarely elsewhere, characterized by skin lesions that are located predominantly on the upper trunk and arms in sun-exposed areas.[3]
- Cutaneous tuberculosis – a form of tuberculosis involving the skin. The diagnosis may be difficult, since this condition shares many similarities with other skin conditions. It may be caused by Mycobacterium tuberculosis, Mycobacterium bovis, and the BCG vaccination. Commonly the skin lesion begins as an irregular red-brown papule or nodule, with a granulomatous base. Later this lesion evolves into a painless ulcer, usually with ≤ 1cm of diameter. The most common sites of this lesion are: face and extremities.[4]
- Granuloma annulare – chronic skin disease, with unknown cause, consisting of a rash with reddish bumps arranged in a circle or ring. It most often affects children, young and older adults and it is slightly more common in females (60/40 ratio). The condition is usually seen in otherwise healthy people. Occasionally, it may be associated with diabetes or thyroid disease.
- Cutaneous leishmaniasis – a skin infection caused by a single-celled parasite that is transmitted by sand-fly bites the, constituting the most common form of leishmaniasis. The lesions typically progress from small papules to nodular plaques, and eventually lead to open sores with a raised border and central crater (ulcer), which can be covered with scales or [[crust]. These lesions are usually painless but can be painful, particularly if open sores become infected with bacteria. Satellite lesions, regional lymphadenopathy (swollen glands), and nodular lymphangitis can be noted. Commonly this condition produces less nodules than the lepromatous form of leprosy, with the skin lesions commonly resolving after a few weeks, which is uncommon in leprosy.
- Post kala-azar dermal leishmaniasis – may mimic leprosy in its presentation with hypopigmented macules, papules and nodular lesions.
- Mycosis fungoides – is a rare form of cutaneous T-cell non-Hodgkin’s lymphoma, generally affects the skin, but may progress internally over time. Common symptoms include rashlike patches, tumors, or lesions and pruritus in about 20% of patients.
- Hereditary sensory motor neuron neuropathy type III – commonly causes nerve thickening, which is present in leprosy and may therefore complicate the diagnosis.
- Refsum’s disease – like hereditary sensory motor neuron neuropathy type III, it commonly causes nerve thickening, which is present in leprosy and may therefore complicate the diagnosis.
- Amyloid – insoluble fibrous protein aggregations sharing specific structural traits. Is able to cause a wide spectrum of symptoms, of which skin changes is a common form of presentation. These include: petechiae, ecchymoses, [[waxy papular nodules around the eyes, neck and in the groin region, patches of hair loss and brittle nails. May be a complication of leprosy and be responsible for part of the nerve thickening seen in this condition.
- Mycosis – may be classified according to the affected tissue. When it affects the superficial and more inner layers of skin it may mimic leprosy.
- Keloid – A keloid is a type of scar which results in an overgrowth of tissue at the site of a healed skin injury. Keloids are firm, rubbery lesions or shiny, fibrous nodules, and can vary from pink to flesh-colored or red to dark brown in color.
References
- ↑ Walker, Stephen L.; Lockwood, Dina N.J. (2007). “Leprosy”. Clinics in Dermatology. 25 (2): 165–172. doi:10.1016/j.clindermatol.2006.05.012. ISSN 0738-081X.
- ↑ Pinto FJ, Bolognia JL (1991). “Disorders of hypopigmentation in children”. Pediatr. Clin. North Am. 38 (4): 991–1017. PMID 1870914.
- ↑ James, William D.; Berger, Timothy G.; et al. (2006). Andrews’ Diseases of the Skin: clinical Dermatology. Saunders Elsevier. ISBN 0-7216-2921-0.
- ↑ MacGregor RR (1995). “Cutaneous tuberculosis”. Clin Dermatol. 13 (3): 245–55. PMID 8521366.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: João André Alves Silva, M.D. [2]
Overview
Current prevalence rate of leprosy per 100,000 is 3.7. The disease is more prevalent in endemic areas, which represent a potential source of spread of the disease to the rest of the world.
Epidemiology and Demographics
In 1990, the WHO defined a goal of eliminating leprosy as a public health issue within 10 years. Between the years of 1985 and 2010, the number of registered cases of leprosy fell from 5.4 million to 244,796, with prevalence rate per 100,000 falling from 211 to 3.7. However this prevalence is very variable according to the region, since most reported cases come from developing countries, such as India, Brazil and Indonesia. Efforts have been made to decrease the number of cases in endemic areas and to avoid transmission of the disease to other parts of the world, since international travel represents an important vehicle of the bacteria into other parts of the globe. This transmission has such impact that among the cases reported annually in the United States, 75% occur in emigrants.
Incidence
Due to the long incubation period, delay in diagnosis, and lack of laboratory infrastructures it is difficult to measure the true incidence of leprosy.
Two to three million people are estimated to be permanently disabled due to leprosy. India has the greatest number of cases, followed by Brazil and Myanmar.
In 1999, the world incidence of leprosy was estimated to be 640,000; in 2000, 738,284 cases were identified. In 1999, 108 cases occurred in the United States. In 2000, the World Health Organization (WHO) listed 91 countries in which leprosy was endemic.
According to the WHO, the number of new cases has decreased by approximately 107,000 cases (or 21%) from 2003 to 2004. This decreasing trend has been consistent for the past three years.
Prevalence
Registered prevalence reflects the number of active leprosy cases diagnosed with the disease and retrieving treatment with multi-drug therapy (MDT) at a given point in time. In fact, the global registered prevalence of leprosy at the beginning of 2012 was 181,941; 219,075 new cases were detected during 2011.
As reported to the WHO by 105 countries and territories in 2012 the global registered prevalence of leprosy at the beginning of 2012 was 181,941 cases. [1] New case detection during the previous year (2011) was 219,075. The number of new cases detected annually continues to increase in all regions other than the Americas and African Regions. The significant decline in the African Region reflects the low number of reports submitted, particularly from member states reporting high number of new cases in the past. Increased coverage along with provision of better services in South Sudan and Somalia were the main factors that led to detection of more new cases in the Eastern Mediterranean Region.[1]
The prevalence of Leprosy in the United States is believed to be rising and underreported. There are a rising number of cases worldwide, though pockets of high prevalence continue in certain areas such as Brazil, South Asia (India, Nepal), some parts of Africa (Tanzania, Madagascar, Mozambique) and the western Pacific.

The above image shows an increase in the number of new cases detected from 2010 to 2011, with exception of the Americas and African regions

The above image shows prevalence of leprosy at the beginning of 2012. In 2011, the number of new cases, from 105 countries was 219,075. At the beginning of 2012, the registered prevalence was 181,941
Due to the rising numbers, several support groups exist, the headquarters of which is currently in Lynbrook, NY and headed by Brian Marasco, leprosy survivor.

Endemic countries also report the number of new cases with established disabilities at the time of detection, as an indicator of the backlog prevalence. However, determination of the time of onset of the disease is generally unreliable, is very labour-intensive and is seldom done in recording these statistics.
Elimination of Leprosy as a Public Health Problem
In 1991 WHO‘s governing body, the World Health Assembly (WHA) passed a resolution to eliminate leprosy by the year 2000. Elimination of leprosy is defined as a prevalence rate of less than 1 case per 10 000 persons. The target was achieved on time and the widespread use of multi drug therapy reduced the disease burden dramatically.
- Over the past 20 years, more than 14 million leprosy patients have been cured, about 4 million since 2000.
- The prevalence rate of the disease has dropped by 90% – from 21.1 per 10 000 inhabitants to less than 1 per 10 000 inhabitants in 2000.
- Dramatic decrease in the global disease burden: from 5.2 million in 1985 to 805 000 in 1995 to 753 000 at the end of 1999 to 181 941 cases at the end of 2011.
- Leprosy has been eliminated from 119 countries out of 122 countries where the disease was considered as a public health problem in 1985.
- So far, there has been no resistance to antileprosy treatment when used as multi drug therapy.
- Efforts currently focus on eliminating leprosy at a national level in the remaining endemic countries and at a sub-national level from the others.
References
- ↑ 1.0 1.1 “global leprosy situation, 2012” (PDF).
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: João André Alves Silva, M.D. [2]
Overview
Risk factors for contracting leprosy include close contact with an untreated, active multibacillary disease patient with the subtype of lepromatous leprosy, living in an endemic region (Angola, Brazil, Central African Republic, Democratic Republic of Congo, Federated States of Micronesia, India, Kiribati, Madagascar, Mozambique, Nepal, Republic of Marshall Islands, United Republic of Tanzania), age between 5 and 15 as well as over 30, Armadillo contact, tattoos, and genetic variants of the NOD2-mediated signaling pathway.
Close Contact
Close contacts with leprosy patients increases the risk of contracting the disease.[1]
Subtype
lepromatous leprosy patients have a higher risk of transmitting the disease.[1][2]
Immunosuppresion
Immunosuppressed patients have a higher risk of being infected by the mycobacteria. In the particular case of HIV patients, the infection by the HIV has not been noted to increase vulnerability for development of leprosy. Additionally some studies have reported activation of latent mycobacteria leprae with exacerbation of previous lesions, once the antiretroviral therapy is started, possibly due to reconstitution of the immune response against the bacteria.[3][4][5][6][7]
Armadillo Contact
Armadillo’s serve as a reservoir for disease, and armadillo contact increases the risk of transmission of disease.[8]
Genetic Risk Factors
The immune response mounted against the mycobacteria has both innate and acquired components. It has been noted that variants of the NOD2-mediated signaling pathway, a regulator of the innate component, have a higher risk of developing leprosy.[9][10]
Age
There is a bimodal distribution in the incidence of leprosy, with an increased incidence between the ages of 5 and 15 years, and than another increase after the age of 30.[11]
Endemic Regions
People living in endemic regions along with poor-higiene and poor nutritional status are at increased risk of contracting leprosy.[12]
These countries include:
- Angola
- Brazil
- Central African Republic
- Democratic Republic of Congo
- Federated States of Micronesia
- India
- Kiribati
- Madagascar
- Mozambique
- Nepal
- Republic of Marshall Islands
- United Republic of Tanzania
Tattooing
The bacteria have been transferred during tattooing in India.[13][14]
Vertical Transmission from Mother
Cases of vertical transmission from the mother have been reported.[13][15]
References
- ↑ 1.0 1.1 van Beers SM, Hatta M, Klatser PR (1999). “Patient contact is the major determinant in incident leprosy: implications for future control”. Int J Lepr Other Mycobact Dis. 67 (2): 119–28. PMID 10472363.
- ↑ Eiglmeier K, Parkhill J, Honoré N, Garnier T, Tekaia F, Telenti A; et al. (2001). “The decaying genome of Mycobacterium leprae”. Lepr Rev. 72 (4): 387–98. PMID 11826475.
- ↑ Trindade MA, Palermo ML, Pagliari C, Valente N, Naafs B, Massarollo PC; et al. (2011). “Leprosy in transplant recipients: report of a case after liver transplantation and review of the literature”. Transpl Infect Dis. 13 (1): 63–9. doi:10.1111/j.1399-3062.2010.00549.x. PMID 20678090.
- ↑ Martiniuk F, Rao SD, Rea TH, Glickman MS, Giovinazzo J, Rom WN; et al. (2007). “Leprosy as immune reconstitution inflammatory syndrome in HIV-positive persons”. Emerg Infect Dis. 13 (9): 1438–40. doi:10.3201/eid1309.070301. PMC 2857291. PMID 18252138.
- ↑ Sarno EN, Illarramendi X, Nery JA, Sales AM, Gutierrez-Galhardo MC, Penna ML; et al. (2008). “HIV-M. leprae interaction: can HAART modify the course of leprosy?”. Public Health Rep. 123 (2): 206–12. PMC 2239330. PMID 18457073.
- ↑ Deps PD, Lockwood DN (2008). “Leprosy occurring as immune reconstitution syndrome”. Trans R Soc Trop Med Hyg. 102 (10): 966–8. doi:10.1016/j.trstmh.2008.06.003. PMID 18639911.
- ↑ Couppié P, Domergue V, Clyti E, El Guedj M, Vaz T, Sainte-Marie D; et al. (2009). “Increased incidence of leprosy following HAART initiation: a manifestation of the immune reconstitution disease”. AIDS. 23 (12): 1599–600. doi:10.1097/QAD.0b013e32832bb5b7. PMID 19487911.
- ↑ Truman, Richard W.; Singh, Pushpendra; Sharma, Rahul; Busso, Philippe; Rougemont, Jacques; Paniz-Mondolfi, Alberto; Kapopoulou, Adamandia; Brisse, Sylvain; Scollard, David M.; Gillis, Thomas P.; Cole, Stewart T. (2011). “Probable Zoonotic Leprosy in the Southern United States”. New England Journal of Medicine. 364 (17): 1626–1633. doi:10.1056/NEJMoa1010536. ISSN 0028-4793.
- ↑ Alter A, Alcaïs A, Abel L, Schurr E (2008). “Leprosy as a genetic model for susceptibility to common infectious diseases”. Hum Genet. 123 (3): 227–35. doi:10.1007/s00439-008-0474-z. PMID 18247059.
- ↑ Zhang FR, Huang W, Chen SM, Sun LD, Liu H, Li Y; et al. (2009). “Genomewide association study of leprosy”. N Engl J Med. 361 (27): 2609–18. doi:10.1056/NEJMoa0903753. PMID 20018961.
- ↑ Moet FJ, Pahan D, Schuring RP, Oskam L, Richardus JH (2006). “Physical distance, genetic relationship, age, and leprosy classification are independent risk factors for leprosy in contacts of patients with leprosy”. J Infect Dis. 193 (3): 346–53. doi:10.1086/499278. PMID 16388481.
- ↑ Bhat, Ramesh Marne; Prakash, Chaitra (2012). “Leprosy: An Overview of Pathophysiology”. Interdisciplinary Perspectives on Infectious Diseases. 2012: 1–6. doi:10.1155/2012/181089. ISSN 1687-708X.
- ↑ 13.0 13.1 Walker, Stephen L.; Lockwood, Dina N.J. (2007). “Leprosy”. Clinics in Dermatology. 25 (2): 165–172. doi:10.1016/j.clindermatol.2006.05.012. ISSN 0738-081X.
- ↑ Ghorpade A (2009). “Ornamental tattoos and skin lesions. Tattoo inoculation borderline tuberculoid leprosy”. Int J Dermatol. 48 (1): 11–3. doi:10.1111/j.1365-4632.2009.03767.x. PMID 19126044.
- ↑ Duncan ME, Melsom R, Pearson JM, Menzel S, Barnetson RS (1983). “A clinical and immunological study of four babies of mothers with lepromatous leprosy, two of whom developed leprosy in infancy”. Int J Lepr Other Mycobact Dis. 51 (1): 7–17. PMID 6683260.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: João André Alves Silva, M.D. [2]
Overview
Leprosy may lead to severe complications if not diagnosed and treated early, which will affect the prognosis.
Natural History
Leprosy, or Hansen’s disease, is caused by Mycobacterium leprae, a gram-positive obligate intracellular, acid-fast bacillus.
Although the mechanism of transmission is not well understood, it is though that the respiratory mucosa and skin play an important role in the transmission of the disease.
The symptoms of the disease might not occur until 12 years after the exposure to the bacteria. Common initial symptoms may include loss of sensation of a hipopigmented skin patch and a thickened peripheral nerve concomitantly with weakness or loss of sensation of the area
Without treatment symptoms will develop and include skin ulcers, eye problems, nasal congestion, epistaxis, muscle contractures and eventually complicate into paralysis and blindness.
Complications
One to two million persons worldwide are permanently disabled as a result of leprosy.[1] The number and degree of complications will depend on how early the condition is diagnosed and treatment with multidrug therapy is started. A late diagnosis will increase the number and severity of the complications. These may include:[2][3]
- Cosmetic disfigurement with skin ulceration and scars.
- Permanent nerve damage, with sensory loss, numbness and pain particularly around skin lesions.
- Muscle weakness and paralysis with predominance in the hands and feet.
- Blindness – conditions such as corneal abrasion and corneal ulceration may occur, potentially leading to blindness.
- Burns and trauma – attending to the loss of sensation, following the nerve damage caused by this condition, a potential complication is the non voluntary self-inflicted trauma as a result of the absence of pain.
- Infection – following painless injuries, due to the nerve damage, that become infected by bacteria and complicate.
- Thick and dry skin
- Lucio phenomenon – rare but potentially fatal complication, occurring predominantly in untreated lepromatous patients, as an acute necrotizing vasculopathy. It is common to observe painful irregular patches that usually become pruritic, developing bullae. This phenomenon has been noted to occur predominantly in descendants from mexican populations.[4][5]
Prognosis
Leprosy is a curable disease when adequately treated. With early diagnosis and treatment, the damages inflicted in patients by the disease may be reduced. Therefore, early recognition and prompt treatment are essential to improve the prognosis of patients, increasing the chances of a normal lifestyle. To improve the chances of a better prognosis, physicians, particularly of endemic areas, must be aware of the early signs and symptoms of the disease and the population must be educated to avoid infection and search medical attention when such symptoms appear, thereby minimizing complications.
References
- ↑ Walker, Stephen L.; Lockwood, Dina N.J. (2007). “Leprosy”. Clinics in Dermatology. 25 (2): 165–172. doi:10.1016/j.clindermatol.2006.05.012. ISSN 0738-081X.
- ↑ Daniel E, Ffytche TJ, Kempen JH, Rao PS, Diener-West M, Courtright P (2006). “Incidence of ocular complications in patients with multibacillary leprosy after completion of a 2 year course of multidrug therapy”. Br J Ophthalmol. 90 (8): 949–54. doi:10.1136/bjo.2006.094870. PMC 1857220. PMID 16707521.
- ↑ “P Hansen’s Disease (Leprosy)”. line feed character in
|title=at position 2 (help) - ↑ Rea, Thomas H. (1977). “Current Concepts in the Immunology of Leprosy”. Archives of Dermatology. 113 (3): 345. doi:10.1001/archderm.1977.01640030091017. ISSN 0003-987X.
- ↑ Sehgal VN, Srivastava G, Sharma VK (1987). “Contemplative immune mechanism of Lucio phenomenon and its global status”. J Dermatol. 14 (6): 580–5. PMID 3329658.
Diagnosis
Diagnosis
Diagnostic Criteria | History and Symptoms | Physical Examination | Laboratory Findings | X Ray | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Tertiary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
External Links
External Links
| Wikimedia Commons has media related to Leprosy. |
- National Hansen’s Disease Programs (NHDP), U.S. Health Resources and Services Administration
- [4]
- World Health Organization (WHO) leprosy website
ar:جذام
az:Cüzəm
bn:কুষ্ঠ
ca:Lepra
zh-min-nan:Hansen ê pīⁿ
cs:Lepra
da:Spedalskhed
de:Lepra
eo:Lepro
fa:جذام
ko:한센병
hi:कुष्ठ
is:Holdsveiki
it:Lebbra
he:צרעת
la:Lepra
hu:Lepra
ms:Penyakit kusta
nl:Lepra
no:Spedalskhet
qu:Lliqti unquy
simple:Leprosy
sl:Gobavost
su:Lépra
fi:Lepra
sv:Lepra
ur:جذام
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH