
Urethritis
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Synonyms and keywords: Urethrorrhea; urethral discharge
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Urethritis is due to inflammation of the urethra. Based on etiology it is classified into two main groups, infectious and non-infectious. Infectious causes are further classified into gonorrheal and non-gonorrheal. Urethritis is an inflammation of the genital tract that is mostly due to infectious causes. Its pathogenesis depends on the causative pathogen. Microscopic findings for gonococcal urethritis include, presence of gram-negative intracellular diplococci (GNID), invaded epithelial cells, vacuoles that contain multiple organisms, and >2 WBC per oil immersion field. Nongonococcal urethritis (NGU) is [[microscopically characterized by signs of inflammation with absence of gram-negative intracellular diplococci. If symptoms are present but no evidence of urethral inflammation is present, Nucleic Acid Amplification Tests (NAATs) for C. trachomatis and N. gonorrhoeae might identify infections.The most potent risk factor for urethritis is unprotected sex, especially among men who have sex with men. Other risk factors include low socioeconomic status, history of sexually transmitted diseases, and multiple sex partners. Urethritis is primarily diagnosed based on symptoms, signs of urethral inflammation and microscopic findings. Symptoms may comprise of dysuria, urethral pruritus, burning, Signs of urethral inflammation include urethral discharge, which can be mucoid, mucopurulent, or purulent. Microscopic findings in gonorrheal urethritis include, identification of gram-negative intracellular diplococci (GNID) or purple intracellular diplococci on methylene blue, or gentian violet stain. Presence of Invaded epithelial cells, vacuoles that contain multiple organisms and >2 WBC per oil immersion field. Nongonococcal urethritis (NGU) is microscopically characterized by signs of inflammation with absence of gram-negative intracellular diplococci. If symptoms are present but no evidence of urethral inflammation is present, Nucleic Acid Amplification Tests (NAATs) for C. trachomatis and N. gonorrhoeae might identify infections.Once the diagnosis is confirmed, the appropriate antibiotic regimen should be initiated to reduce the risk of complications. Doxycycline 100 mg PO bid for 7 days is administered to treat Non-gonococcal Urethritis, as an alternative therapy azithromycin 1 g PO in a single dose or azithromycin 500 mg orally in a single dose; then 250 mg orally daily for 4 days is recommended. For gonococcal urethritis, ceftriaxone 500 mg IM in a single dose (for patients weighing ≥150 kg (300 lbs) ceftriaxone 1 g IM in a single dose), for alternate therapy gentamicin 240 mg PO in a single dose plus azithromycin 2 g PO in a single dose, or cefixime 800 mg PO in a single dose is recommended.
Historical Perspective
The first known case of urethritis was described by Albert Neisser, a German doctor, in 1879. In 1904, Ludwig Waelsch described mild non-gonococcal urethritis (NGU). In the 1930s and later, Philip Thygeson and others in the United States confirmed the vertical transmission of nongonococcal urethritis (NGU).
Classification
Urethritis is classified into two main groups of infectious and non-infectious based on the etiology. Infectious causes are further classified into gonorrheal and non-gonorrheal.
Pathophysiology
Urethritis is an inflammation of the genital tract that is mostly due to infectious causes. Its pathogenesis depends on the causative pathogen. N. gonorrhea is usually transmitted via the genital tract to the human host. Following attachment to host cell, which is mediated by pili, gonococci become engulfed in a process known as parasite-directed endocytosis. This organism will survive inside the vacuoles and replicate. Among non-gonorrheal causes, Chlamydia trachomatis is the most common. The infectious process begins with cell surface attachment and phagocytosis by the host cell. The pathogen survives inside the cell by debilitating the cellular lysosomes and replicating as elementary bodies which is considered as the infective form of the pathogen. Microscopic findings for gonococcal urethritis include, presence of gram-negative intracellular diplococci (GNID), invaded epithelial cells, vacuoles that contain multiple organisms, and >2 WBC per oil immersion field. Nongonococcal urethritis (NGU) is microscopically characterized by signs of inflammation with absence of gram-negative intracellular diplococci.
Causes
Urethritis may be caused by either infectious or non-infectious causes. Infectious causes are divided into gonorrheal and non-gonorrheal. Non-gonorrheal pathogens are the most common cause of urethritis; Chlamydia trachomatis is the most common among them.
Differentiating Urethritis from Other Diseases
Urethritis must be differentiated from other causes of dysuria and urethral discharge, which include acute cystitis, epididymitis, prostatitis, cervicitis, and vulvovaginitis.
Epidemiology and Demographics
Urethritis is the cause of several millions of healthcare visits in the United States. Chlamydia trachomatis is the most common reportable disease in the US. In 2014, a total of 350,062 gonorrhea cases were reported to the CDC in the US. Based on The National Health and Nutrition Examination Survey, the overall prevalence of chlamydia among persons aged 14–39 years was 1.7% during 2007-2012. Urethritis has a very good prognosis with proper treatment. Mortality is very uncommon in patients with gonococcal and non-gonococcal urethritis. Almost two-thirds of chlamydia infections occur among youths aged 15-24 years. The highest prevalence rates of gonococcal urethritis were found in ages 20 to 24 years both in men and women. In 2014, the overall rate of chlamydia infection in the United States among women was 627.2 cases per 100,000 females, over two times the rate among men (278.4 cases per 100,000 males). In 2014, the incidence of gonorrhea in the United States was reported as 120 cases per 100,000 males, while it was reported as 100 cases per 100,000 females.
Risk Factors
The most potent risk factor for urethritis is unprotected sex, especially among men who have sex with men. Other risk factors include low socioeconomic status, history of sexually transmitted diseases, and multiple sex partners.
Screening
High-risk individuals should be screened for sexually transmitted diseases. The U.S. Preventive Service Task Force (USPSTF) developed recommendations for the screening of for Chlamydia trachomatis and N. gonorrhea.
Natural History, Complications, and Prognosis
Urethritis has a good prognosis and most patients are treated with appropriate antibiotics. If left untreated, it can resolve within 3 months in 95% of people with gonococcalurethritis. The symptoms of nongonococcal urethritis generally abate within 3 months in 30-70% of untreated people. Rarely, complications such as epididymitis, prostatitis, urethral stricture, chronic gonorrhea carrier state, may occur.
Diagnosis
Diagnostic Study of Choice
Urethritis is primarily diagnosed based on symptoms, signs of urethral inflammation and microscopic findings. Symptoms may comprise of dysuria, urethral pruritus, burning, Signs of urethral inflammation include urethral discharge, which can be mucoid, mucopurulent, or purulent. Microscopic findings in gonorrheal urethritis include, identification of gram-negative intracellular diplococci (GNID) or purple intracellular diplococci on methylene blue, or gentian violet stain. Presence of Invaded epithelial cells, vacuoles that contain multiple organisms and >2 WBC per oil immersion field. Nongonococcal urethritis (NGU) is microscopically characterized by signs of inflammation with absence of gram-negative intracellular diplococci. If symptoms are present but no evidence of urethral inflammation is present, Nucleic Acid Amplification Tests (NAATs) for C. trachomatis and N. gonorrhoeae might identify infections.
History and Symptoms
A detailed history, particularly with regard to sexual activity, must be taken. Symptoms suggestive for urethritis include dysuria and urethral discharge. History should specifically include, recent sexual activities, number of sex partners, or any new partner, use of condoms, history of prior STDs, and history of recent urethral instrumentation (e.g., urethral catheters).
Symptoms
Symptoms suggestive of urethritis include dysuria and urethral discharge.
Physical Examination
The most common physical finding in urethritis is urethral discharge. The entire genital area must be examined in order to rule out other possibilities. Patients should be examined for inguinal lymphadenopathy, ulcers, and urethral discharge.
Laboratory Findings
Urethritis may be considered on the basis of any of the following, mucoid, mucopurulent, or purulent discharge on examination, Gram stain of urethral secretions demonstrating ≥2 WBC per field, positive leukocyte esterase test on first-void urine or microscopic examination of sediment from a spun first-void urine demonstrating ≥10 WBC per high power field.
Electrocardiogram
There are no ECG findings associated with urethritis.
X-ray
There are no x-ray findings associated with urethritis.
Echocardiography and Ultrasound
There are no echocardiography/ultrasound findings associated with urethritis.
CT scan
There are no CT scan findings associated with urethritis.
MRI
There are no MRI findings associated with urethritis.
Other Imaging Findings
There are no other imaging findings associated with urethritis.
Other Diagnostic Studies
There are no additional diagnostic findings for urethritis.
Treatment
Medical Therapy
Once the diagnosis is confirmed, the appropriate antibiotic regimen should be initiated to reduce the risk of complications. Doxycycline 100 mg PO bid for 7 days is administered to treat Non-gonococcal Urethritis, as an alternative therapy azithromycin 1 g PO in a single dose or azithromycin 500 mg orally in a single dose; then 250 mg orally daily for 4 days is recommended. For gonococcal urethritis, ceftriaxone 500 mg IM in a single dose (for patients weighing ≥150 kg (300 lbs) ceftriaxone 1 g IM in a single dose), for alternate therapy gentamicin 240 mg PO in a single dose plus azithromycin 2 g PO in a single dose, or cefixime 800 mg PO in a single dose is recommended. Metronidazole 2 g PO in a single dose is used for patients with recurrent and persistent urethritis. Following treatment, patients should be instructed to return for evaluation if symptoms persist or recur after completion of therapy. Providers should be alert to the possibility of chronic prostatitis/chronic pelvic pain syndrome in male patients experiencing persistent pain (perineal, penile, or pelvic), discomfort, irritating voiding symptoms, pain during or after ejaculation, or new onset premature ejaculation lasting for >3 months. All sex partners within the preceding 60 days should be referred for evaluation, testing, and empiric treatment with a drug regimen effective against Chlamydia. Clinicians must report both chlamydia and gonorrhea to health departments.
Interventions
There are no recommended therapeutic interventions for the management of urethritis.
Surgery
Surgical intervention is not recommended for the management of urethritis.
Primary Prevention
Effective measures for the primary prevention of urethritis include limiting the number of sex partners and using condoms.
Secondary Prevention
In order to prevent transmission to one’s partner and decrease the risk of antibiotic resistance, all patients must be instructed on safe sex practices and screening requirements after treatment.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
The first known case of urethritis was described by Albert Neisser, a German doctor, in 1879. In 1904, Ludwig Waelsch described mild non-gonococcal urethritis (NGU). In the 1930s and later, Philip Thygeson and others in the United States confirmed the vertical transmission of nongonococcal urethritis (NGU).
Historical Perspective
- In 1879, Neisser discovered the gonococcus and, for the first time, the term “urethritis non‐gonorrhoica” was coined.
- In 1904, Ludwig Waelsch described mild non-gonococcal urethritis (NGU).
- After that Chlamydozoa, was described as infectious agent, that may cause NGU, which was, at that time, called Waelsch urethritis.
- In the 1930s and later, Philip Thygeson and others in the United States confirmed the vertical transmission of nongonococcal urethritis (NGU).[1]
References
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2] Zehra Malik, M.B.B.S[3]
Overview
Urethritis is an inflammation of the genital tract that is mostly due to infectious causes. Its pathogenesis depends on the causative pathogen. N. gonorrhea is usually transmitted via the genital tract to the human host. Following attachment to host cell, which is mediated by pili, gonococci become engulfed in a process known as parasite-directed endocytosis. This organism will survive inside the vacuoles and replicate. Among non-gonorrheal causes, Chlamydia trachomatis is the most common. The infectious process begins with cell surface attachment and phagocytosis by the host cell. The pathogen survives inside the cell by debilitating the cellular lysosomes and replicating as elementary bodies which is considered as the infective form of the pathogen.
Pathophysiology
Urethritis is divided into gonorrheal and non-gonorrheal causes. The pathophysiology of each one of them is different.
Gonorrheal
- N. gonorrhea is usually transmitted via the genital tract to the human host.
- Following attachment to host cell, which is mediated by pili, gonococci become engulfed in a process known as parasite-directed endocytosis. This organism will survive inside the vacuoles and replicate.[1]
- Gonococcal virulence factors include:[2][3][4]
- Pili
- The ability to attach to urethral epithelial cells
- Production of extracellular proteases that cleave IgA
Non-Gonorrheal
- Among non-gonorrheal causes, Chlamydia trachomatis is the most common.
- The infectious process begins with cell surface attachment and phagocytosis by the host cell. The pathogen survives inside the cell by debilitating the cellular lysosomes and replicating as elementary bodies which is considered as the infective form of the pathogen.[5][6]
Genetics
Urethritis does not follow any genetic pattern.
Associated Conditions
- Stevens-Johnson syndrome
- Nongonococcal urethritis (NGU) due to C. trachomatis may be associated with:
- HIV transmission is facilitated by co-existing non-gonococcal urethritis, however treatment of NGU is the same in HIV negative or positive patients.
Gross Pathology
On gross pathology, mucoid, mucopurulent, or purulent discharge can be observed.
Microscopy
Gonorrheal
Characteristic findings include:[7]
- Gram-negative intracellular diplococci (GNID) or purple intracellular diplococci on methylene blue, or gentian violet stain.
- Invaded epithelial cells
- Vacuoles that contain multiple organisms
- Polymorphic nuclear cellss
Non-Gonorrheal
- Absence of gram-negative intracellular diplococci (GNID)
- Signs of inflammation present
References
- ↑ Scheuerpflug I, Rudel T, Ryll R, Pandit J, Meyer TF (1999). “Roles of PilC and PilE proteins in pilus-mediated adherence of Neisseria gonorrhoeae and Neisseria meningitidis to human erythrocytes and endothelial and epithelial cells”. Infect. Immun. 67 (2): 834–43. PMC 96394. PMID 9916098.
- ↑ Sparling PF (1966). “Genetic transformation of Neisseria gonorrhoeae to streptomycin resistance”. J Bacteriol. 92 (5): 1364–71. PMC 276432. PMID 4958881.
- ↑ Swanson J (1973). “Studies on gonococcus infection. IV. Pili: their role in attachment of gonococci to tissue culture cells”. J Exp Med. 137 (3): 571–89. PMC 2139381. PMID 4631989.
- ↑ Wolfgang M, Lauer P, Park HS, Brossay L, Hébert J, Koomey M (1998). “PilT mutations lead to simultaneous defects in competence for natural transformation and twitching motility in piliated Neisseria gonorrhoeae”. Mol Microbiol. 29 (1): 321–30. PMID 9701824.
- ↑ Beatty, Wandy L., Richard P. Morrison, and Gerald I. Byrne. “Persistent chlamydiae: from cell culture to a paradigm for chlamydial pathogenesis.” Microbiological reviews 58.4 (1994): 686-699.
- ↑ Baron, Samuel. Medical microbiology. Galveston, Tex: University of Texas Medical Branch at Galveston, 1996. Print.
- ↑ Apicella MA, Ketterer M, Lee FK, Zhou D, Rice PA, Blake MS (1996). “The pathogenesis of gonococcal urethritis in men: confocal and immunoelectron microscopic analysis of urethral exudates from men infected with Neisseria gonorrhoeae”. J. Infect. Dis. 173 (3): 636–46. PMID 8627027.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Urethritis may be caused by either infectious or non-infectious causes. Infectious causes are divided into gonorrheal and non-gonorrheal. Non-gonorrheal pathogens are the most common cause of urethritis; Chlamydia trachomatis is the most common among them.
Causes
Urethritis may be caused by either infectious or non-infectious causes. Infectious causes are divided into gonococcal and non-gonococcal. Non-gonorrheal pathogens are the most common cause of urethritis; Chlamydia trachomatis is the most common among them.[1][2][3]
| Causes | |||||||||||||||||||||||||||||||||||||||||||||||||
| Non-infectious causes[4] | Infectious causes[3] | ||||||||||||||||||||||||||||||||||||||||||||||||
| Heavy precipitation of urinary crystals, chemicals, bubble bath, Stevens-Johnson syndrome, spermicides | Gonococcal urethritis[1] | Non-gonococcal urethritis[5][6][7] | |||||||||||||||||||||||||||||||||||||||||||||||
| Chlamydia trachomatis Trichomonas vaginalis Mycoplasma genitalium Herpes simplex virus Adenovirus Ureaplasma urealyticum Neisseria meningitidis Haemophilus influenza Haemophilus parainfluenzae | |||||||||||||||||||||||||||||||||||||||||||||||||
Causes by Organ System
| Cardiovascular | No underlying causes |
| Chemical/Poisoning | Bath salts, bubble bath, spermicides, talcum powder |
| Dental | No underlying causes |
| Dermatologic | No underlying causes |
| Drug Side Effect | No underlying causes |
| Ear Nose Throat | No underlying causes |
| Endocrine | No underlying causes |
| Environmental | No underlying causes |
| Gastroenterologic | No underlying causes |
| Genetic | No underlying causes |
| Hematologic | No underlying causes |
| Iatrogenic | Urethral catheterization, instrumentation |
| Infectious Disease | Adenovirus, Candida albicans, Chlamydia trachomatis, Group D streptococcus, Herpes simplex virus, Lymphogranuloma venereum, Mycoplasma genitalium, Mycoplasma hominis, Neisseria gonorrheae, Pelvic inflammatory disease, protozoa, Treponema pallidum, Trichomonas vaginalis, Ureaplasma parvum, Ureaplasma urealyticum |
| Musculoskeletal/Orthopedic | No underlying causes |
| Neurologic | No underlying causes |
| Nutritional/Metabolic | No underlying causes |
| Obstetric/Gynecologic | No underlying causes |
| Oncologic | No underlying causes |
| Ophthalmologic | No underlying causes |
| Overdose/Toxicity | No underlying causes |
| Psychiatric | No underlying causes |
| Pulmonary | No underlying causes |
| Renal/Electrolyte | No underlying causes |
| Rheumatology/Immunology/Allergy | Balanitis xerotica obliterans, Reiter syndrome, Stevens-Johnson syndrome |
| Sexual | No underlying causes |
| Trauma | Urethral trauma |
| Urologic | No underlying causes |
| Miscellaneous | Bicycle riding, diaphragm use (contraception), foreign body insertion, heavy precipitation of urinary crystals, physical irritation of the urethra |
Causes in Alphabetical Order
- Adenovirus
- Balanitis xerotica obliterans
- Bath salts
- Bicycle riding
- Bubble bath
- Candida albicans
- Chemical irritation
- Chlamydia trachomatis
- Diaphragm contraception
- Foreign body insertion
- Group D streptococcus
- Heavy precipitation of urinary crystals
- Herpes simplex virus
- Instrumentation
- Lymphogranuloma venereum
- Mycoplasma genitalium
- Mycoplasma hominis
- Neisseria gonorrheae
- Pelvic inflammatory disease
- Physical irritation of the urethra
- Protozoa
- Reiter syndrome
- Spermicides
- Stevens-Johnson syndrome
- Talcum powder
- Treponema pallidum
- Trichomonas vaginalis
- Ureaplasma parvum
- Ureaplasma urealyticum
- Urethral catheterization
- Urethral trauma
References
- ↑ 1.0 1.1 Kimberly A. Workowski & Gail A. Bolan (2015). “Sexually transmitted diseases treatment guidelines, 2015”. MMWR. Recommendations and reports : Morbidity and mortality weekly report. Recommendations and reports / Centers for Disease Control. 64 (RR-03): 1–137. PMID 26042815. Unknown parameter
|month=ignored (help) - ↑ Al-Sweih NA, Khan S, Rotimi VO (2011). “The prevalence of Chlamydia trachomatis and Neisseria gonorrhoeae infections among men with urethritis in Kuwait”. J Infect Public Health. 4 (4): 175–9. doi:10.1016/j.jiph.2011.07.003. PMID 22000844.
- ↑ 3.0 3.1 Le Roux MC, Ramoncha MR, Adam A, Hoosen AA (2010). “Aetiological agents of urethritis in symptomatic South African men attending a family practice”. Int J STD AIDS. 21 (7): 477–81. doi:10.1258/ijsa.2010.010066. PMID 20852197.
- ↑ Herz D, Weiser A, Collette T, Reda E, Levitt S, Franco I (2005). “Dysfunctional elimination syndrome as an etiology of idiopathic urethritis in childhood”. J. Urol. 173 (6): 2132–7. doi:10.1097/01.ju.0000157686.28359.c7. PMID 15879866.
- ↑ K. K. Holmes, H. H. Handsfield, S. P. Wang, B. B. Wentworth, M. Turck, J. B. Anderson & E. R. Alexander (1975). “Etiology of nongonococcal urethritis”. The New England journal of medicine. 292 (23): 1199–1205. doi:10.1056/NEJM197506052922301. PMID 165407. Unknown parameter
|month=ignored (help) - ↑ David H. Martin (2008). “Nongonococcal urethritis: new views through the prism of modern molecular microbiology”. Current infectious disease reports. 10 (2): 128–132. PMID 18462587. Unknown parameter
|month=ignored (help) - ↑ Michael J. Schlicht, Steven D. Lovrich, Jeffrey S. Sartin, Patricia Karpinsky, Steven M. Callister & William A. Agger (2004). “High prevalence of genital mycoplasmas among sexually active young adults with urethritis or cervicitis symptoms in La Crosse, Wisconsin”. Journal of clinical microbiology. 42 (10): 4636–4640. doi:10.1128/JCM.42.10.4636-4640.2004. PMID 15472322. Unknown parameter
|month=ignored (help)
Differentiating Urethritis from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Urethritis presents with urinary irritative symptoms and urethral discharge. Differential diagnosis is based on gender and chronicity of symptoms.
Differential Diagnosis
Urethritis must be differentiated from other diseases that cause lower urinary tract irritation symptoms (e.g., dysuria, urgency and frequency in addition to urethral discharge); these include cystitis, cervicitis, vulvovaginitis, epididymitis, prostatitis, and syphilis.[1][2][3][4][5][6][7][8][9]
- The following table summarizes the differential diagnosis for urethritis.
| Diseases | Symptoms | Physical Examination | Diagnostic tests | Past medical history | Other Findings | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hematuria | Pyuria | Frequency | Urgency | Dysuria | Fever | Tenderness | Discharge | Inguinal Lymphadenopathy | Urinalysis | Urine Culture | Gold Standard | |||
| Urethritis | – | + | – | – | + | + | – | Urethral discharge | + |
|
– | Gram stain & mucoid or purulent discharge |
|
|
| Pyelonephritis | + | + | – | – | + | + | Flank or costovertebral angle | + | + |
|
Identifies causative bacteria | Urine culture |
|
|
| Cystitis | + | + | + | + | + | + | Suprapubic | – | + |
|
>100,000CFU/mL | Urine culture |
|
|
| Prostatitis | – | + | + | + | + | + | – | – | – |
|
Identifies causative bacteria (in bacterial subtypes) | Urine culture |
|
|
| Diseases | Symptoms | Physical Examination | Diagnostic tests | Past medical history | Other Findings | |||||||||
| Hematuria | Pyuria | Frequency | Urgency | Dysuria | Fever | Tenderness | Discharge | Inguinal Lymphadenopathy | Urinalysis | Urine Culture | Gold Standard | |||
| Vulvovagintis | – | – | – | – | + | + | – | Vaginal discharge | + | – | – | Gram stain & culture of discharge |
|
|
| Cervicitis | – | + | – | – | + | + | Cervical | Endocervical exudate | – | – | – | Culture for gonococcal cervicitis |
|
|
| Epididymitis | + | – | + | + | + | + | Testicular & suprapubic | +/– urethral discharge | + |
|
+ | Culture |
|
|
| Syphilis
(STD) |
– | – | – | – | – | +/– | – | – | + | – | – | Darkfield microscopy |
|
|
References
- ↑ Stephen Bent, Brahmajee K. Nallamothu, David L. Simel, Stephan D. Fihn & Sanjay Saint (2002). “Does this woman have an acute uncomplicated urinary tract infection?”. JAMA. 287 (20): 2701–2710. PMID 12020306. Unknown parameter
|month=ignored (help) - ↑ W. E. Stamm (1981). “Etiology and management of the acute urethral syndrome”. Sexually transmitted diseases. 8 (3): 235–238. PMID 7292216. Unknown parameter
|month=ignored (help) - ↑ W. E. Stamm, K. F. Wagner, R. Amsel, E. R. Alexander, M. Turck, G. W. Counts & K. K. Holmes (1980). “Causes of the acute urethral syndrome in women”. The New England journal of medicine. 303 (8): 409–415. doi:10.1056/NEJM198008213030801. PMID 6993946. Unknown parameter
|month=ignored (help) - ↑ Leonie G. M. Giesen, Grainne Cousins, Borislav D. Dimitrov, Floris A. van de Laar & Tom Fahey (2010). “Predicting acute uncomplicated urinary tract infection in women: a systematic review of the diagnostic accuracy of symptoms and signs”. BMC family practice. 11: 78. doi:10.1186/1471-2296-11-78. PMID 20969801.
- ↑ Taylor-Robinson D (1996). “The history of nongonococcal urethritis. Thomas Parran Award Lecture”. Sex Transm Dis. 23 (1): 86–91. PMID 8801649.
- ↑ Bennett, John (2015). Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. Philadelphia, PA: Elsevier/Saunders. ISBN 9781455748013.
- ↑ Brill JR (2010). “Diagnosis and treatment of urethritis in men”. Am Fam Physician. 81 (7): 873–8. PMID 20353145.
- ↑ Daniel V. Landers, Harold C. Wiesenfeld, R. Phillip Heine, Marijane A. Krohn & Sharon L. Hillier (2004). “Predictive value of the clinical diagnosis of lower genital tract infection in women”. American journal of obstetrics and gynecology. 190 (4): 1004–1010. doi:10.1016/j.ajog.2004.02.015. PMID 15118630. Unknown parameter
|month=ignored (help) - ↑ Felix Millan-Rodriguez, J. Palou, Anna Bujons-Tur, Mireia Musquera-Felip, Carlota Sevilla-Cecilia, Marc Serrallach-Orejas, Carlos Baez-Angles & Humberto Villavicencio-Mavrich (2006). “Acute bacterial prostatitis: two different sub-categories according to a previous manipulation of the lower urinary tract”. World journal of urology. 24 (1): 45–50. doi:10.1007/s00345-005-0040-4. PMID 16437219. Unknown parameter
|month=ignored (help)
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Urethritis is the cause of several millions of healthcare visits in the United States. Chlamydia trachomatis is the most common reportable disease in the US. In 2014, a total of 350,062 gonorrhea cases were reported to the CDC in the US. Based on The National Health and Nutrition Examination Survey, the overall prevalence of chlamydia among persons aged 14–39 years was 1.7% during 2007-2012. Urethritis has a very good prognosis with proper treatment. Mortality is very uncommon in patients with gonococcal and non-gonococcal urethritis. Almost two-thirds of chlamydia infections occur among youths aged 15-24 years. The highest prevalence rates of gonococcal urethritis were found in ages 20 to 24 years both in men and women. In 2014, the overall rate of chlamydia infection in the United States among women was 627.2 cases per 100,000 females, over two times the rate among men (278.4 cases per 100,000 males). In 2014, the incidence of gonorrhea in the United States was reported as 120 cases per 100,000 males, while it was reported as 100 cases per 100,000 females.
Epidemiology and Demographics
Incidence
- Chlamydia trachomatis is the most common reportable disease in the US. In 2014, a total of 1,441,789 chlamydial infections were reported to the CDC.
- In 2014, the incidence of urethritis due to Chlamydia trachomatis infection was estimated to be 456 cases per 100,000 individuals in the US.
- In 2014, a total of 350,062 gonorrhea cases were reported to the CDC in the US.[1]
- In 2014, the incidence of urethritis due to N. gonorrhea infection was estimated to be 110.7 cases per 100,000 individuals in the US.
- Worldwide, there are an estimated 78 million gonorrhea cases, and 131 million cases of chlamydia yearly.[2][3]
Prevalence
- Based on The National Health and Nutrition Examination Survey, the overall prevalence of chlamydia among persons aged 14–39 years was 1.7% during 2007-2012.[4]
Mortality rate
- Urethritis has a very good prognosis with proper treatment. Mortality is very uncommon in patients with gonococcal and non-gonococcal urethritis.
Age
- Chlamydia trachomatis
- Gonorrhea
- The highest prevalence rates were found in ages 20 to 24 years both in men and women.
Race
- Chlamydia trachomatis[4]
- In 2014, the chlamydia rate in African-Americans was 6 times the rate in Caucasians.
- The rate among American Indians/Alaska Natives was almost 4 times the rate among Caucasians.
- Gonorrhea[4]
- In 2014, the rate of reported gonorrhea cases remained highest among African-Americans (405.4 cases per 100,000 individuals).
- The rate among African-Americans was 10.6 times the rate among Caucasians (38.3 cases per 100,000 population).
- The gonorrhea rate among American Indians/Alaska natives was 159.4 cases per 100,000 individuals, 4.2 times that of Caucasians.
-
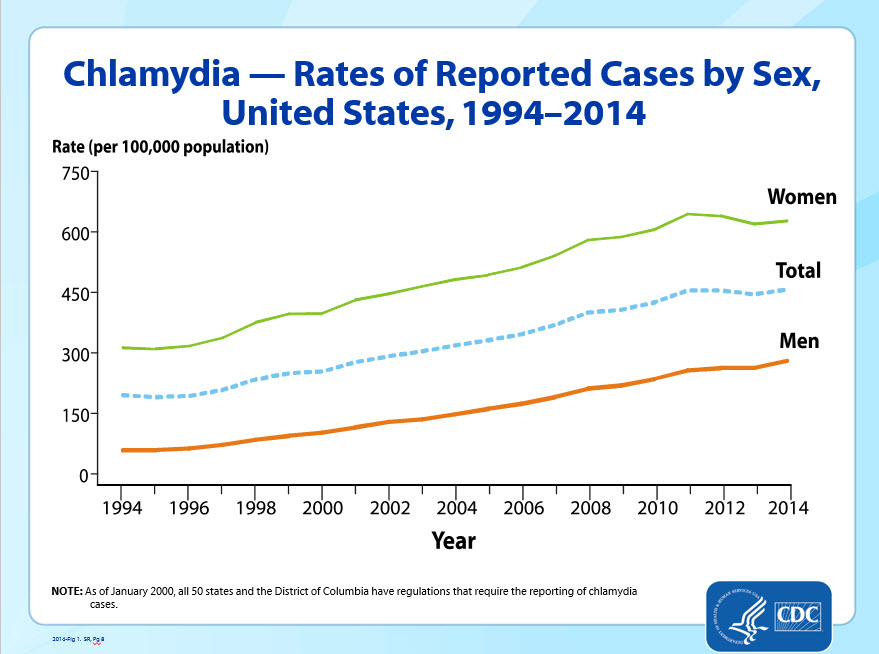 Rate of Chlamydia reported cases by gender
Rate of Chlamydia reported cases by gender -
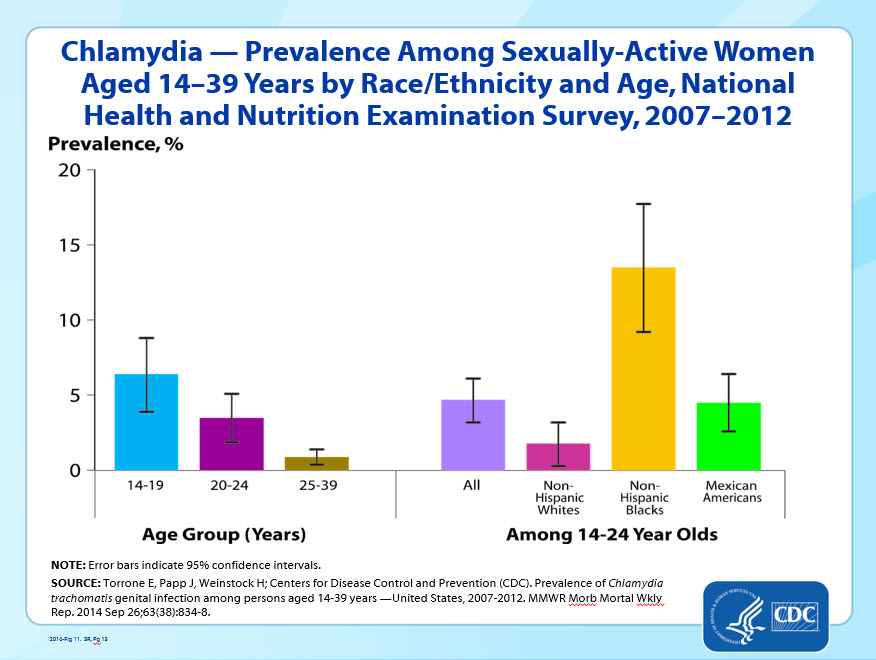 Chlamydia Prevalence by race and age
Chlamydia Prevalence by race and age -
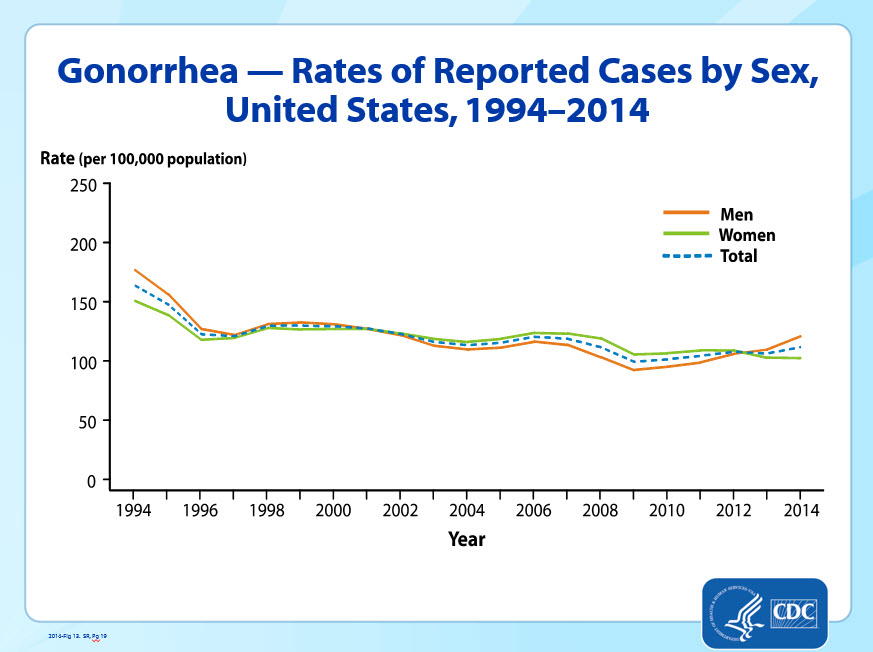 Rate of Gonorrhea reported cases by sex
Rate of Gonorrhea reported cases by sex -
 Gonorrhea Prevalence by race
Gonorrhea Prevalence by race




Graphs adapted from https://www.cdc.gov/
Gender
- Chlamydia trachomatis
- Gonorrhea
- In 2014, incidence of gonorrhea in the United States was reported as 120 cases per 100,000 males, while it was reported as 100 cases per 100,000 female.
References
- ↑ 1.0 1.1 “National Overview – 2014 STD Surveillance”.
- ↑ WHO epidemiology http://www.who.int/mediacentre/factsheets/fs110/en/ (2016) Accessed on September 26, 2016
- ↑ Torrone E, Papp J, Weinstock H (2014). “Prevalence of Chlamydia trachomatis genital infection among persons aged 14-39 years–United States, 2007-2012”. MMWR Morb. Mortal. Wkly. Rep. 63 (38): 834–8. PMID 25254560.
- ↑ 4.0 4.1 4.2 “Chlamydia – 2014 STD Surveillance”.
- ↑ Chlamydia CDC Fact Sheet. CDC.http://www.cdc.gov/std/chlamydia/stdfact-chlamydia-detailed.htm#_ENREF_3. Accessed on September 28,2016
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
The most potent risk factor for urethritis is unprotected sex, especially among men who have sex with men. Other risk factors include low socioeconomic status, history of sexually transmitted diseases, and multiple sex partners.
Risk Factors
The most important risk factors for urethritis is unprotected sex, especially among men who have sex with men. The following are other risk factors:[1][2]
- Low socioeconomic status
- Prior or current STD
- New or multiple sex partners
- Circumcision
References
- ↑ Chacko MR, Lovchik JC (1984). “Chlamydia trachomatis infection in sexually active adolescents: prevalence and risk factors”. Pediatrics. 73 (6): 836–40. PMID 6547226.
- ↑ Van Howe RS (2007). “Genital ulcerative disease and sexually transmitted urethritis and circumcision: a meta-analysis”. Int J STD AIDS. 18 (12): 799–809. doi:10.1258/095646207782717045. PMID 18073009.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
High-risk individuals should be screened for sexually transmitted diseases. The U.S. Preventive Service Task Force (USPSTF) developed recommendations for the screening of for Chlamydia trachomatis and N. gonorrhea.
Screening
According to the U.S. Preventive Service Task Force (USPSTF), screening for sexually transmitted disease is recommended as outlined below for Chlamydia trachomatis and N. gonorrhea.[1][2]
| Chlamydia trachomatis | |
|---|---|
| Population | Recommendations |
| Women |
|
| Men |
|
| Pregnant women |
|
| Men Who have Sex With Men (MSM) |
|
| HIV positive patients |
|
| Neisseria Gonorrhea | |
|---|---|
| Population | Recommendations |
| Women |
|
| Men Who have Sex With Men (MSM) |
|
| Pregnant women |
|
| HIV positive patients |
|
References
- ↑ Screening recommendation for chlamydia. UPSTF. http://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/chlamydia-and-gonorrhea-screening?ds=1&s=chlamydia(2014). Acessed on September 28, 2016
- ↑ US preventive services task forces. Gonorrhea and chlamydia screening (2014) https://www.uspreventiveservicestaskforce.org/Page/Document/ClinicalSummaryFinal/chlamydia-and-gonorrhea-screening Accessed on September 28, 2016
Natural History, Complications and Prognosis
- Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Seyedmahdi Pahlavani, M.D. [2]
Overview
Urethritis has a good prognosis and most patients are treated with appropriate antibiotics. If left untreated, it can resolve within 3 months in 95% of people with gonococcal urethritis. The symptoms of nongonococcal urethritis generally abate within 3 months in 30-70% of untreated people. Rarely, complications such as epididymitis, prostatitis, urethral stricture, chronic gonorrhea carrier state, may occur.
Natural History, Complications, and Prognosis
Natural History
- If left untreated, it can resolve within 3 months in 95% of people with gonococcal urethritis. The symptoms of nongonococcal urethritis generally abate within 3 months in 30-70% of untreated people.[1]
- Prolonged asymptomatic urethral carriage of gonococci occurs in 2% to 3% of newly infected men if left untreated.[2]
Complications
Common complications of urethritis include:
- Acute epididymitis
- Prostatitis
- It occurs in 20% to 30% of men with non-gonorrheal urethritis (NGU); however, it is usually asymptomatic and responds to standard treatment.[3]
- Urethral stricture
- Gonorrhea may cause urethral stricture.
- Oculogenital syndrome
- Consisting of conjunctivitis and non-gonorrheal urethritis (NGU) may be seen in approximately 4% of patients with urethritis.[4]
- Rare complications include:[6]
- Salpingitis
- Cervicitis
- Seminal vesiculitis
- Penile edema
- Periurethral abscess
- Regional lymphadenitis
- Infertility
Prognosis
- The prognosis is generally good following standard therapy.
References
- ↑ Bennett, John (2015). Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. Philadelphia, PA: Elsevier/Saunders. ISBN 9781455748013.
- ↑ Detels R, Green AM, Klausner JD, Katzenstein D, Gaydos C, Handsfield H, Pequegnat W, Mayer K, Hartwell TD, Quinn TC (2011). “The incidence and correlates of symptomatic and asymptomatic Chlamydia trachomatis and Neisseria gonorrhoeae infections in selected populations in five countries”. Sex Transm Dis. 38 (6): 503–9. PMC 3408314. PMID 22256336.
- ↑ Holmes KK, Handsfield HH, Wang SP, Wentworth BB, Turck M, Anderson JB, Alexander ER (1975). “Etiology of nongonococcal urethritis”. N. Engl. J. Med. 292 (23): 1199–205. doi:10.1056/NEJM197506052922301. PMID 165407.
- ↑ Rönnerstam R, Persson K (1982). “Chlamydial eye infection in adults”. Scand J Infect Dis Suppl. 32: 111–5. PMID 6958007.
- ↑ Carter JD, Gérard HC, Espinoza LR, Ricca LR, Valeriano J, Snelgrove J, Oszust C, Vasey FB, Hudson AP (2009). “Chlamydiae as etiologic agents in chronic undifferentiated spondylarthritis”. Arthritis Rheum. 60 (5): 1311–6. doi:10.1002/art.24431. PMC 2757404. PMID 19404948.
- ↑ Holmes, King (2008). Sexually transmitted diseases. New York: McGraw-Hill Medical. ISBN 978-0071417488.
Diagnosis
Diagnosis
Diagnostic study of choice | History and Symptoms | Physical Examination | Laboratory Findings | Electrocardiogram | X-Ray Findings | Echocardiography and Ultrasound | CT-Scan Findings | MRI Findings | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Interventions | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH