
Lung abscess
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Aditya Ganti M.B.B.S. [2]
Synonyms and keywords: Pulmonary abscess
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Aditya Ganti M.B.B.S. [2]
Overview
Lung abscess is necrosis of the pulmonary tissue and formation of cavities (more than 2 cm) containing necrotic debris or fluid caused by microbial infection. This pus-filled cavity is often caused by aspiration, which may occur during altered consciousness. Alcoholism is the most common condition predisposing to lung abscesses. Lung abscess is considered primary (60%) when it results from existing lung parenchymal process and is termed secondary when it is complicated by another process e.g. vascular emboli or follows rupture of extrapulmonary abscess into the lung.[1]
Historical Perspective
Lung abscess has been a disease entity since the days of Hippocrates. Postural physiotherapy had been the mainstay of treatment until Harold Neuhof described his concept of new one-stage open drainage for the acute abscess in 1930’s. With the invention of antibiotics in late 1940’s and their promising results led the change in management of lung abscess.[2]
Pathophysiology
Aspiration of bacteria is the inciting event for the development of lung abscess. Once the aspirate is localized it results in pneumonitis. Inflammatory mediators are released, resulting in the formation of colliquative necrosis. The right side lung is more commonly affected than the left. On gross morphology, the lesions are well circumscribed filled with necrotic debris and do not demonstrate well-defined borders with the surrounding lung parenchyma. Microscopic examination demonstrates neutrophils with dilated blood vessels and inflammatory edema.[3] [4]
Causes
Lung abscess is commonly caused by bacterial infections and these include bacteroides, peptostreptococcus and prevotella.[5]Lung abscess is commonly caused by bacterial infections and these include bacteroides, peptostreptococcus and prevotella. Most of the lung abscess is caused by polymicrobial organisms of which anaerobes play a crucial role . Less common include nocardia, actinomyces and fungi. If left untreated, life-threatening conditions may develop which may result in death or permanent disability within 24 hours .
Differentiating Lung Abscess from other Diseases
Lung abscess must be differentiated from other lesions that present with similar symptoms such as cough, fever with chills and rigor and chest includes malignancy, tuberculosis, Wegener’s granulomatosis, rheumatoid nodules.[6]
Epidemiology and Demographics
The incidence from lung abscess have greatly declined during the past several decades due to the widespread use of antibiotics and the availability of other treatment options. Lung abscess accounts for up to 4.0 to 5.5 per 10,000 hospital admissions each year in the US.[7]
Risk Factors
Factors resulting in the altered level of consciousness and decreased immune response play a key role in the development of lung abscess includes alcoholism, diabetes mellitus, neurological disorder and bronchial obstruction.[8]
Screening
There is no screening recommendations for lung abscess.
Natural history, Complications and Prognosis
Symptoms of lung abscess begin approximately 10 days after aspiration of infected material. Acute symptoms include a prodrome accompanied by fever, productive cough, pleuritic chest pain and occasional episodes of hemoptysis. Patients with chronic lung abscess develop weight loss and malaise.Without treatment based on the immune status of the patient, lung abscess can either resolve by forming a granulation tissue scar, or progressively worsens and can result in septicemia, hemorrhage, and death.The prognosis of lung abscess is good with appropriate antibiotic treatment with a high success rate. The outcomes depend on the other associated conditions underlying lung abscess such as size of the cavity, age of the patient and other underlying lung diseases. Complications include hemorrhage pyopneumothorax, pleural empyema and sepsis.[9][10]
Diagnosis
History and Symptoms
Patient history is important to establish a diagnosis of lung abscess. Common history findings include conditions associated with a risk of gastric content aspiration, a recent history of hospitalization or surgery. Common symptoms include high fever (>101°F [>38.5°C]), productive cough with purulent sputum, and pleuritic chest pain. Anaerobic bacteria is responsible for purulent sputum in acute lung abscess.
Physical Examination
Patients with acute lung abscess may present with fever, cough with purulent sputum, gag reflex may be absent in patients with an underlying neurological disorder such as stroke. Digital clubbing is present in patients with a chronic abscess.On examination of the chest, there will be features of consolidation. Abscess typically localizes in the upper lobes or apical segments of the lower lobes.[10]
Laboratory Findings
Diagnosis of lung abscess is made based on clinical symptoms, physical examination, radiographic studies and bacterial culture. Laboratory findings include increased acute phase reactants (ESR and CRP) levels and leukocytosis with consolidation being evident in a segmental or lobar distribution with central cavitation an air-fluid level on lung x-ray. Blood cultures should be performed in all suspected cases.
Treatment
Medical Therapy
The mainstay of management for lung abscess is hospital admission for chest drain and systemic antibiotics. Antimicrobial therapy is based on predisposing host factors and local resistance patterns.Empiric treatment should be commenced after culture samples are obtained. The regimens should penetrate the lung parenchyma and target both anaerobes, aerobic and microaerophilic streptococci. Any combination of a beta-lactam–beta-lactamase inhibitor or a carbapenem are reasonable to use. The standard duration of the treatment of lung abscess is ≥ 4–6 weeks of parenteral antibiotics. [11]
Surgical Therapy
Surgery is considered as the last resort of therapy when both medical and chest drain failed to resolve symptoms. Options for surgery includes chest tube drainage and surgical resection of the lung abscess with the surrounding lung tissue.Percutaneous and endoscopic drainage techniques are considered as a first-line management, especially for patients who are not candidates for surgery. Percutaneous drainage of lung abscesses is characterized by high therapeutic effectiveness and preservation of functional lung tissue, it is a minimally invasive method with fewer complications and lower mortality rates (approximately 4%) in comparison to surgical management. Surgical resection is considered in about 10% of the patients when the chest drain has failed to improve symptoms and patients presenting with one of the following conditions. The surgical approach is thoracotomy and the extent of surgical resection depends on the size of the underlying lesion.[12]
Reference
- ↑ Bartlett JG, Finegold SM (1972). “Anaerobic pleuropulmonary infections”. Medicine (Baltimore). 51 (6): 413–50. PMID 4564416.
- ↑ Neuhof H, Hurwitt E (1943). “ACUTE PUTRID ABSCESS OF THE LUNG : VII. RELATIONSHIP OF THE TECHNIC OF THE ONE-STAGE OPERATION TO RESULTS”. Ann. Surg. 118 (4): 656–64. PMC 1617784. PMID 17858299.
- ↑ “Lung abscess”. West. J. Med. 124 (6): 476–82. 1976. PMC 1130102. PMID 936601.
- ↑ Green LH, Green GM (1968). “Differential suppression of pulmonary antibacterial activity as the mechanism of selection of a pathogen in mixed bacterial infection of the lung”. Am. Rev. Respir. Dis. 98 (5): 819–24. doi:10.1164/arrd.1968.98.5.819. PMID 5683476.
- ↑ Cesar L, Gonzalez C, Calia FM (1975). “Bacteriologic flora of aspiration-induced pulmonary infections”. Arch. Intern. Med. 135 (5): 711–4. PMID 28705.
- ↑ Chaudhuri MR (1973). “Primary pulmonary cavitating carcinomas”. Thorax. 28 (3): 354–66. PMC 470041. PMID 4353362.
- ↑ Bartlett JG, Finegold SM (1974). “Anaerobic infections of the lung and pleural space”. Am. Rev. Respir. Dis. 110 (1): 56–77. doi:10.1164/arrd.1974.110.1.56. PMID 4834618.
- ↑ Hagan JL, Hardy JD (1983). “Lung abscess revisited. A survey of 184 cases”. Ann. Surg. 197 (6): 755–62. PMC 1352910. PMID 6859981.
- ↑ Adebonojo SA, Osinowo O, Adebo O (1979). “Lung abscess: a review of three years’ experience at the University College Hospital, Ibadan”. J Natl Med Assoc. 71 (1): 39–43. PMC 2537236. PMID 423274.
- ↑ 10.0 10.1 Hirshberg B, Sklair-Levi M, Nir-Paz R, Ben-Sira L, Krivoruk V, Kramer MR (1999). “Factors predicting mortality of patients with lung abscess”. Chest. 115 (3): 746–50. PMID 10084487.
- ↑ Allewelt M, Schüler P, Bölcskei PL, Mauch H, Lode H (2004). “Ampicillin + sulbactam vs clindamycin +/- cephalosporin for the treatment of aspiration pneumonia and primary lung abscess”. Clin. Microbiol. Infect. 10 (2): 163–70. PMID 14759242.
- ↑ Kelogrigoris, M; Tsagouli, P; Stathopoulos, K; Tsagaridou, I; Thanos, L (2011). “Ct-guided percutaneous drainage of lung abscesses: review of 40 cases”. Journal of the Belgian Society of Radiology. 94 (4): 191. doi:10.5334/jbr-btr.583. ISSN 1780-2393.
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Aditya Ganti M.B.B.S. [2]
Overview
Lung abscess has been a disease entity since the days of Hippocrates. Postural physiotherapy had been the mainstay of treatment until Harold Neuhof described his concept of new one-stage open drainage for the acute abscess in 1930’s. With the invention of antibiotics in late 1940’s and their promising results led the change in management of lung abscess.
Historical perspective
- In 1904, Guillemot first put weight to the theory that aspirated oropharyngeal organisms are responsible for cause of lung abscess[1]
- In 1920-1930, Harold Neuhof was the first thoracic surgeon to develop a valid and reliable therapeutic concept of drainage operation for acute pulmonary abscess.[2]
- In 1938, the first percutaneous drain of lung abscess was performed.[3]
- In 1942, Brock added evidence in stating that aspirated contents gravitated to the dependent part of the lungs.
- In 1946, owing to the advent of antibiotics, and treatment of acute putrid lung abscess with penicillin showed good results and henceforth patients received antibiotics rather than surgical procedures.[2]
Reference
- ↑ Lima, Mario (01/24/2011). Pediatric thoracic surgery Softcover reprint of hardcover 1st ed. 2009. Harvard Medical School: Springer London. p. 145. ISBN 978-8847052017. Check date values in:
|date=(help) - ↑ 2.0 2.1 Neuhof H, Hurwitt E (1943). “ACUTE PUTRID ABSCESS OF THE LUNG : VII. RELATIONSHIP OF THE TECHNIC OF THE ONE-STAGE OPERATION TO RESULTS”. Ann. Surg. 118 (4): 656–64. PMC 1617784. PMID 17858299.
- ↑ Wali SO (2012). “An update on the drainage of pyogenic lung abscesses”. Ann Thorac Med. 7 (1): 3–7. doi:10.4103/1817-1737.91552. PMC 3277038. PMID 22347342.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Aditya Ganti M.B.B.S. [2]
Overview
Lung abscess is defined as an infection of lung resulting in necrosis of lung parenchyma. It can be classified into three categories based on the duration of symptoms, etiology, and mode of spread as acute or chronic, primary or secondary and bronchogenic or hematogenic.
Classification
Based on duration of symptoms
- Acute: If the duration of symptoms is less than 4-6 weeks before presenting to medical care.[1]
- Chronic: If the symptoms persist for more than 6 weeks.
Based on Etiology
- Primary: When the abscess develops after lung infection in previously healthy persons or in patients prone to aspiration. [2]
- Secondary: Abscess formation in patients due to complications of a co-existing lung disease such as post obstructive process (bronchial obstruction due to tumor, foreign body or enlarged lymphnodes) and systemic process resulting in decreased immune response like HIV, and patients on immunosuppressants and corticosteroids.
Based on mode of spread
Bronchiogenic: Abscess formation is due to aspiration and inhalation.[1]
- Aspiration of oropharyngeal secretions.
- Bronchial obstruction by a tumor.
- Foreign body, congenital malformations, and enlarged lymph nodes.
Hematogenic: Abscess formation due to dissemination of causative agents from other infected sites
Reference
- ↑ 1.0 1.1 Puligandla PS, Laberge JM (2008). “Respiratory infections: pneumonia, lung abscess, and empyema”. Semin. Pediatr. Surg. 17 (1): 42–52. doi:10.1053/j.sempedsurg.2007.10.007. PMID 18158141.
- ↑ Bennett, John (2015). Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. Philadelphia, PA: Elsevier/Saunders. ISBN 978-1455748013.
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Aditya Ganti M.B.B.S. [2]
Overview
Aspiration of anaerobic bacteria is the inciting event for the development of lung abscess. Once the aspirate is localized it results in pneumonitis. Inflammatory mediators are released, resulting in the formation of colliquative necrosis. The right side lung is more commonly affected than the left. On gross morphology, the lesions are well circumscribed filled with necrotic debris and do not demonstrate well-defined borders with the surrounding lung parenchyma. Microscopic examination demonstrates neutrophilic granulocytes with dilated blood vessels and inflammatory edema. .
Pathophysiology
- Aspiration of anaerobic bacteria from the oropharynx, due to altered level of consciousness, absent gag reflex or inability to swallow is the inciting event for the development of primary lung abscess.[1]
- In healthy individuals, defense mechanisms cope up with the small amounts of aspirates with no effects, however, in conditions like alcoholism, diabetes mellitus, and immunocompromised state these defense mechanisms can be compromised leading to decreased activity of alveolar macrophages and mobility of leukocytes. [2].
- In secondary lung abscess, abscess formation depends on the underlying lung disease and predisposing factors, for example, bronchial obstruction from benign or malignant intrabronchial lesions or extrinsic compression of bronchus as in middle lobe syndrome results in distal abscess formation due to decreased oropharyngeal clearance and favoring abscess formation.
- Once the aspirate is localized it results in pneumonitis. [3]
- Inflammatory mediators along with various bacterial toxins and proteolytic enzymes from the neutrophils are released, leading to the rupture of small blood vessels resulting in the formation of colliquative necrosis. [4]
Location of abscess
- The right side lung is more commonly affected than the left because the right bronchus is more acutely angulated when compared to left bronchi.
- The most common location is the posterior segment of the right apical lobe or apical segments of lower lobes of both the lungs.[5]
- In alcoholics and hospitalized patients are in the supine position, right lateral part of the posterior segment of the upper lobe is more commonly involved.
Genetics
- Congenital diseases such as cystic fibrosis, vasculitis, pulmonary sequestration and bronchial cysts are associated with increased the risk of lung abscess in children.[6]
Gross Pathology
- In acute lung abscess, the lesions are well circumscribed filled with necrotic debris and do not demonstrate well-defined borders with the surrounding lung parenchyma.[7]
- In chronic long standing abscess, the lesions are irregular and filled with grayish thick debris.
-
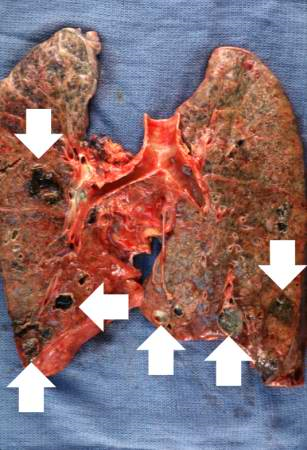 Gross photograph of the lung abscess. Note the abscesses (arrows) especially in the lower lobes.
Gross photograph of the lung abscess. Note the abscesses (arrows) especially in the lower lobes. -
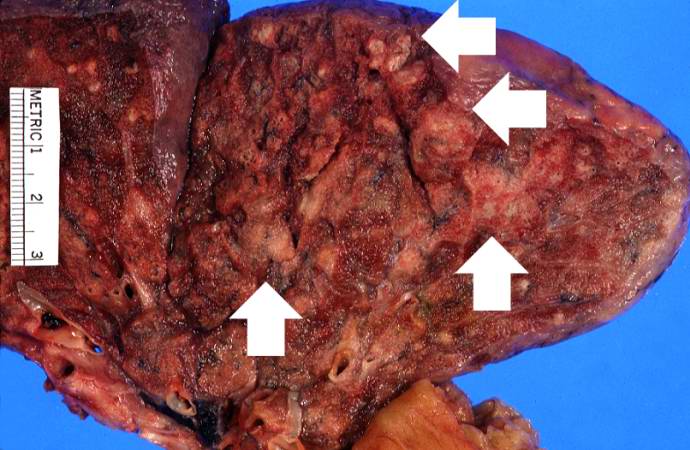 In this section of upper lobe there are multiple areas of early abscess formation (arrows). Note the circumscribed whitish-tan lesions. These lesions are filled with white blood cells.
In this section of upper lobe there are multiple areas of early abscess formation (arrows). Note the circumscribed whitish-tan lesions. These lesions are filled with white blood cells.


Microscopic Findings
- In acute lung abscess, neutrophilic granulocytes are demonstrated with dilated blood vessels and inflammatory edema.[7]
- In chronic lung abscess, biopsy specimen demonstrates lymphocytes, plasma cells, and histiocytes around a layer of pyogenic membrane surrounding the abscess cavity which is filled with pus.
-
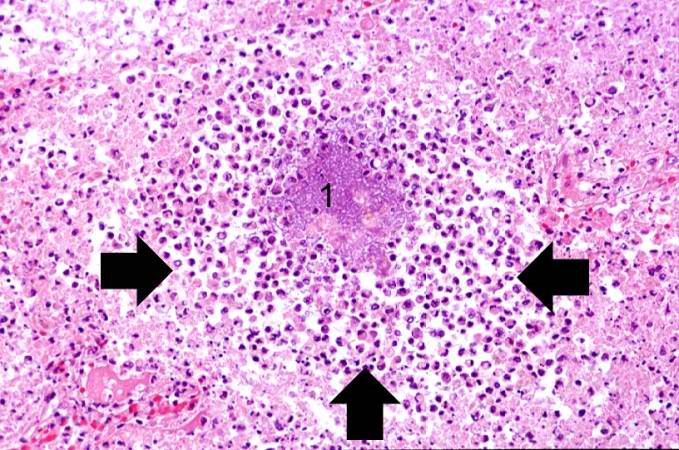 Acute lung abscess abscess full of inflammatory cells (primarily neutrophils) (arrows). There is a bacterial colony in the center of this abscess (1)..
Acute lung abscess abscess full of inflammatory cells (primarily neutrophils) (arrows). There is a bacterial colony in the center of this abscess (1).. -
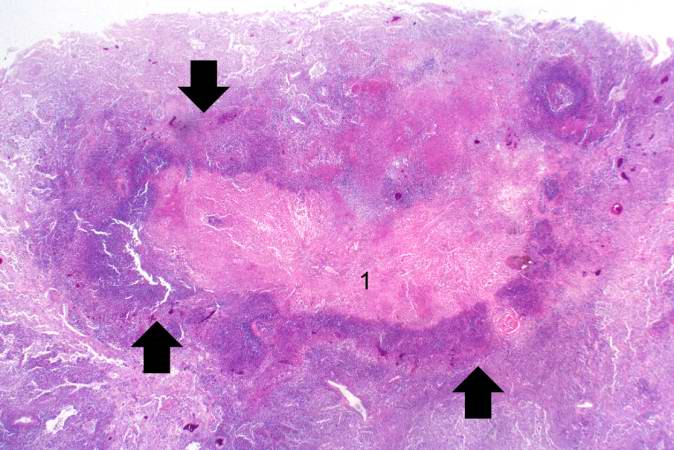 Chronic lung abscess containing necrotic debris (1) and there is a rim of viable inflammatory cells (arrows) surrounding this abscess..
Chronic lung abscess containing necrotic debris (1) and there is a rim of viable inflammatory cells (arrows) surrounding this abscess..


Reference
- ↑ “Lung abscess”. West. J. Med. 124 (6): 476–82. 1976. PMC 1130102. PMID 936601.
- ↑ Green LH, Green GM (1968). “Differential suppression of pulmonary antibacterial activity as the mechanism of selection of a pathogen in mixed bacterial infection of the lung”. Am. Rev. Respir. Dis. 98 (5): 819–24. doi:10.1164/arrd.1968.98.5.819. PMID 5683476.
- ↑ Brook I (2004). “Anaerobic pulmonary infections in children”. Pediatr Emerg Care. 20 (9): 636–40. PMID 15599270.
- ↑ Tsai YF, Ku YH (2012). “Necrotizing pneumonia: a rare complication of pneumonia requiring special consideration”. Curr Opin Pulm Med. 18 (3): 246–52. doi:10.1097/MCP.0b013e3283521022. PMID 22388585.
- ↑ Bartlett JG (1993). “Anaerobic bacterial infections of the lung and pleural space”. Clin. Infect. Dis. 16 Suppl 4: S248–55. PMID 8324127.
- ↑ Canny GJ, Marcotte JE, Levison H (1986). “Lung abscess in cystic fibrosis”. Thorax. 41 (3): 221–2. PMC 460300. PMID 3715782.
- ↑ 7.0 7.1 Kuhajda I, Zarogoulidis K, Tsirgogianni K, Tsavlis D, Kioumis I, Kosmidis C, Tsakiridis K, Mpakas A, Zarogoulidis P, Zissimopoulos A, Baloukas D, Kuhajda D (2015). “Lung abscess-etiology, diagnostic and treatment options”. Ann Transl Med. 3 (13): 183. doi:10.3978/j.issn.2305-5839.2015.07.08. PMC 4543327. PMID 26366400.
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ogheneochuko Ajari, MB.BS, MS [2] ,Aditya Ganti M.B.B.S. [3]
Overview
Lung abscess is commonly caused by bacterial infections and these include bacteroides, peptostreptococcus and prevotella. Most of the lung abscess is caused by polymicrobial organisms,of which anaerobes play a crucial role. Less common include nocardia, actinomyces and fungi.
Causes
Life-threatening causes
- Include conditions which may result in death or permanent disability within 24 hours if left untreated.
- Aerobic bacteria are most commonly associated with rapid and flumiant course with high grade fever and worsening symptoms. These bacteria Include Staphylococcus aureus, Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa, Streptococcus pneumonia.
Microbiology
- About 90% of the lung abscess is caused by polymicrobial infection.[1] [2]
- Anaerobes are the predominant pathogens involved in primary lung abscess, followed by Streptococcus pneumoniae.
- Klebsiella pneumoniae is the more commonly seen in alcoholics.[3]
- Staphylococcus aureus is the most common pathogen responsible for lung abscess in children with cystic fibrosis.[4]
The following table elaborates the most common etiological pathogens responsible for lung abscess [5]
Common Causes
Less Common Causes
Causes by Organ System
| Cardiovascular | Infective endocarditis |
| Chemical/Poisoning | No underlying causes |
| Dental | No underlying causes |
| Dermatologic | No underlying causes |
| Drug Side Effect | Drug injection, porfimer |
| Ear Nose Throat | No underlying causes |
| Endocrine | Diabetes mellitus |
| Environmental | No underlying causes |
| Gastroenterologic | Cystic fibrosis |
| Genetic | Cystic fibrosis |
| Hematologic | No underlying causes |
| Iatrogenic | Hospital-acquired pneumonia |
| Infectious Disease | Actinomyces, actinomycosis, alveolar hydatid disease, amoebiasis, aspergilloma, aspergillus, bacteroides, blastomyces dermatitidis, bronchiectasis, burkholderia pseudomallei, candida, capnocytophaga, coccidioides immitis, community-acquired pneumonia, cryptococcus neoformans, cryptococcus, entamoeba histolytica, escherichia coli, fusobacterium, haemophilus influenzae, histoplasma capsulatum, HIV, hospital-acquired pneumonia, infective endocarditis, klebsiella pneumoniae, klebsiella, legionella, Lemierre’s syndrome, listeriosis, melioidosis, mycobacterium tuberculosis, nocardia, paragonimiasis, paragonimus westermani, paragonimus, peptostreptococcus, pneumonia, prevotella, pseudomonas aeruginosa, rhodococcus equi, staphylococcus aureus, streptococcus milleri, streptococcus pneumoniae, streptococcus pyogenes, streptococcus, yersinia |
| Musculoskeletal/Orthopedic | No underlying causes |
| Neurologic | No underlying causes |
| Nutritional/Metabolic | Cystic fibrosis |
| Obstetric/Gynecologic | No underlying causes |
| Oncologic | Bronchogenic carcinoma |
| Ophthalmologic | No underlying causes |
| Overdose/Toxicity | No underlying causes |
| Psychiatric | No underlying causes |
| Pulmonary | Alveolar hydatid disease, aspiration, bronchiectasis, bronchogenic carcinoma, community-acquired pneumonia, cystic fibrosis, hospital-acquired pneumonia, mycobacterium tuberculosis, pneumonia, Wegener’s granulomatosis |
| Renal/Electrolyte | Wegener’s granulomatosis |
| Rheumatology/Immunology/Allergy | Chronic granulomatous disease, common variable immunodeficiency, Sjogren’s syndrome, vasculitis, Wegener’s granulomatosis |
| Sexual | No underlying causes |
| Trauma | No underlying causes |
| Urologic | No underlying causes |
| Miscellaneous | Foreign body |
Causes in Alphabetical Order
- Actinomyces
- Actinomycosis
- Alveolar hydatid disease
- Amoebiasis
- Aspergilloma
- Aspergillus
- Aspiration
- Bacteroides
- Blastomyces dermatitidis
- Bronchiectasis
- Bronchogenic carcinoma
- Burkholderia pseudomallei
- Candida
- Capnocytophaga
- Chronic granulomatous disease
- Coccidioides immitis
- Common variable immunodeficiency
- Community-acquired pneumonia
- Cryptococcus
- Cryptococcus neoformans
- Cystic fibrosis
- Diabetes mellitus
- Drug injection
- Entamoeba histolytica
- Escherichia coli
- Foreign body
- Fusobacterium
- Haemophilus influenzae
- Histoplasma capsulatum
- HIV
- Hospital-acquired pneumonia
- Infective endocarditis
- Klebsiella
- Klebsiella pneumoniae [6][7]
- Legionella
- Lemierre’s syndrome
- Listeriosis
- Melioidosis
- Mycobacterium tuberculosis
- Nocardia
- Paragonimiasis
- Paragonimus
- Paragonimus westermani
- Peptostreptococcus
- Pneumonia
- Porfimer
- Prevotella
- Pseudomonas aeruginosa [7]
- Rhodococcus equi
- Sjogren’s syndrome
- Staphylococcus aureus [7]
- Streptococcus
- Streptococcus milleri
- Streptococcus pneumoniae
- Streptococcus pyogenes
- Vasculitis
- Wegener’s granulomatosis
- Yersinia
Reference
- ↑ Cesar L, Gonzalez C, Calia FM (1975). “Bacteriologic flora of aspiration-induced pulmonary infections”. Arch. Intern. Med. 135 (5): 711–4. PMID 28705.
- ↑ Bartlett JG (2012). “Anaerobic bacterial infection of the lung”. Anaerobe. 18 (2): 235–9. doi:10.1016/j.anaerobe.2011.12.004. PMID 22209937.
- ↑ Wang JL, Chen KY, Fang CT, Hsueh PR, Yang PC, Chang SC (2005). “Changing bacteriology of adult community-acquired lung abscess in Taiwan: Klebsiella pneumoniae versus anaerobes”. Clin. Infect. Dis. 40 (7): 915–22. doi:10.1086/428574. PMID 15824979.
- ↑ “www.iosrjournals.org” (PDF).
- ↑ Lorber B, Swenson RM (1974). “Bacteriology of aspiration pneumonia. A prospective study of community- and hospital-acquired cases”. Ann. Intern. Med. 81 (3): 329–31. PMID 4850729.
- ↑ Bartlett JG (2005). “The role of anaerobic bacteria in lung abscess”. Clin. Infect. Dis. 40 (7): 923–5. doi:10.1086/428586. PMID 15824980.
- ↑ 7.0 7.1 7.2 Hirshberg B, Sklair-Levi M, Nir-Paz R, Ben-Sira L, Krivoruk V, Kramer MR (1999). “Factors predicting mortality of patients with lung abscess”. Chest. 115 (3): 746–50. PMID 10084487.
Differentiating Lung abscess from other Diseases
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Aditya Ganti M.B.B.S. [2]
Overview
Lung abscess must be differentiated from other lesions that present with similar symptoms such as cough, fever with chills and rigor and chest includes malignancy, pulmonary tuberculosis, Wegener’s granulomatosis, rheumatoid nodules.
Differential
| Disease | Clinical features
Signs & symptoms |
Radiological Findings | Characterstic feature | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Fever | Cough | Hemoptysis | Dyspnea | Chest pain | Weight loss | Night sweats | |||||
| High-grade | Low grade | Productive | Dry | ||||||||
| Acute Lung abscess | + | + | + |
|
| ||||||
| Malignancy | + | + | + | + | + |
|
|||||
| Pulmonary Tuberculosis | + | + | + | + |
| ||||||
| Necrotizing Pneumonia | + | + | + | + |
|
| |||||
| empyema | + | + | + | + | + |
|
| ||||
| Bronchiectasis | + | + |
|
High resolution CT helps in diagnosis . | |||||||
| Wegners granulomatosis | + | + | + |
| |||||||
| Sarcoidosis | + | + | + | + | + |
|
| ||||
| Rheumatoid nodule | + | + |
| ||||||||
| Langerhans cell Histiocytosis | + | + | + |
|
| ||||||
| Bronchiolitis obliterans | + | + | + | + |
|
| |||||
| Causes of
lung cavities |
Differentiating Features | Differentiating lab findings | Diagnosis
confirmation |
|---|---|---|---|
|
|
| |
|
|
|
|
|
|
| |
|
|
|
|
|
|
| |
|
|
| |
|
|
||
|
|
| |
|
|
|
Reference
- ↑ 1.0 1.1 Chaudhuri MR (1973). “Primary pulmonary cavitating carcinomas”. Thorax. 28 (3): 354–66. PMC 470041. PMID 4353362.
- ↑ Mouroux J, Padovani B, Elkaïm D, Richelme H (1996). “Should cavitated bronchopulmonary cancers be considered a separate entity?”. Ann. Thorac. Surg. 61 (2): 530–2. doi:10.1016/0003-4975(95)00973-6. PMID 8572761.
- ↑ Onn A, Choe DH, Herbst RS, Correa AM, Munden RF, Truong MT, Vaporciyan AA, Isobe T, Gilcrease MZ, Marom EM (2005). “Tumor cavitation in stage I non-small cell lung cancer: epidermal growth factor receptor expression and prediction of poor outcome”. Radiology. 237 (1): 342–7. doi:10.1148/radiol.2371041650. PMID 16183941.
- ↑ 4.0 4.1 Langford CA, Hoffman GS (1999). “Rare diseases.3: Wegener’s granulomatosis”. Thorax. 54 (7): 629–37. PMC 1745525. PMID 10377211.
- ↑ Lee KS, Kim TS, Fujimoto K, Moriya H, Watanabe H, Tateishi U, Ashizawa K, Johkoh T, Kim EA, Kwon OJ (2003). “Thoracic manifestation of Wegener’s granulomatosis: CT findings in 30 patients”. Eur Radiol. 13 (1): 43–51. doi:10.1007/s00330-002-1422-2. PMID 12541109.
- ↑ Baughman RP, Teirstein AS, Judson MA, Rossman MD, Yeager H, Bresnitz EA, DePalo L, Hunninghake G, Iannuzzi MC, Johns CJ, McLennan G, Moller DR, Newman LS, Rabin DL, Rose C, Rybicki B, Weinberger SE, Terrin ML, Knatterud GL, Cherniak R (2001). “Clinical characteristics of patients in a case control study of sarcoidosis”. Am. J. Respir. Crit. Care Med. 164 (10 Pt 1): 1885–9. doi:10.1164/ajrccm.164.10.2104046. PMID 11734441.
- ↑ Brauner MW, Grenier P, Mompoint D, Lenoir S, de Crémoux H (1989). “Pulmonary sarcoidosis: evaluation with high-resolution CT”. Radiology. 172 (2): 467–71. doi:10.1148/radiology.172.2.2748828. PMID 2748828.
- ↑ Murphy J, Schnyder P, Herold C, Flower C (1998). “Bronchiolitis obliterans organising pneumonia simulating bronchial carcinoma”. Eur Radiol. 8 (7): 1165–9. doi:10.1007/s003300050527. PMID 9724431.
- ↑ 9.0 9.1 Al-Ghanem S, Al-Jahdali H, Bamefleh H, Khan AN (2008). “Bronchiolitis obliterans organizing pneumonia: pathogenesis, clinical features, imaging and therapy review”. Ann Thorac Med. 3 (2): 67–75. doi:10.4103/1817-1737.39641. PMC 2700454. PMID 19561910.
- ↑ Cordier JF, Loire R, Brune J (1989). “Idiopathic bronchiolitis obliterans organizing pneumonia. Definition of characteristic clinical profiles in a series of 16 patients”. Chest. 96 (5): 999–1004. PMID 2805873.
- ↑ Lee KS, Kullnig P, Hartman TE, Müller NL (1994). “Cryptogenic organizing pneumonia: CT findings in 43 patients”. AJR Am J Roentgenol. 162 (3): 543–6. doi:10.2214/ajr.162.3.8109493. PMID 8109493.
- ↑ Suri HS, Yi ES, Nowakowski GS, Vassallo R (2012). “Pulmonary langerhans cell histiocytosis”. Orphanet J Rare Dis. 7: 16. doi:10.1186/1750-1172-7-16. PMC 3342091. PMID 22429393.
- ↑ Moore AD, Godwin JD, Müller NL, Naidich DP, Hammar SP, Buschman DL, Takasugi JE, de Carvalho CR (1989). “Pulmonary histiocytosis X: comparison of radiographic and CT findings”. Radiology. 172 (1): 249–54. doi:10.1148/radiology.172.1.2787035. PMID 2787035.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Aditya Ganti M.B.B.S. [2]
Overview
The incidence from lung abscess have greatly declined during the past several decades due to the widespread use of antibiotics and the availability of other treatment options.
Epidemiology and Demographics
- Incidence has declined in the late 1940s and 1950s, after the practice of performing oral surgery and tonsillectomy in the sitting position was abandoned, as it became clear that this could result in lung abscess formation.[1]
- Lung abscess accounts for up to 40 to 55 per 100,000 hospital admissions each year in the US.
- It occurs at any age, but most frequently from the sixth to eighth decades, and is predominantly seen in men. [2]
Reference
- ↑ SCHWEPPE HI, KNOWLES JH, KANE L (1961). “Lung abscess. An analysis of the Massachusets General Hospital cases from 1943 through 1956”. N. Engl. J. Med. 265: 1039–43. doi:10.1056/NEJM196111232652104. PMID 14039097.
- ↑ Bartlett JG, Finegold SM (1974). “Anaerobic infections of the lung and pleural space”. Am. Rev. Respir. Dis. 110 (1): 56–77. doi:10.1164/arrd.1974.110.1.56. PMID 4834618.
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Aditya Ganti M.B.B.S. [2]
Overview
Factors resulting in altered level of consciousness and decreased immune response play a key role in the development of lung abscess includes alcoholism, diabetes mellitus, neurological disorder and bronchial obstruction.[1]
Risk Factors
Common Risk Factors
- Alcoholism[2]
- Seizure disorder
- Mechanical ventilation
- Decrease level of consciousness
- Neuromuscular disorders with bulbar dysfunction[3]
- Nocturnal aspiration [4]
- Bronchial obstruction
- Gingivo–dental sepsis
- Diabetes mellitus
- Immunosuppression[4]
Less Common Risk factors
Reference
- ↑ Pohlson EC, McNamara JJ, Char C, Kurata L (1985). “Lung abscess: a changing pattern of the disease”. Am. J. Surg. 150 (1): 97–101. PMID 4014575.
- ↑ Hagan JL, Hardy JD (1983). “Lung abscess revisited. A survey of 184 cases”. Ann. Surg. 197 (6): 755–62. PMC 1352910. PMID 6859981.
- ↑ Bartlett JG, Finegold SM (1974). “Anaerobic infections of the lung and pleural space”. Am. Rev. Respir. Dis. 110 (1): 56–77. doi:10.1164/arrd.1974.110.1.56. PMID 4834618.
- ↑ 4.0 4.1 Hirshberg B, Sklair-Levi M, Nir-Paz R, Ben-Sira L, Krivoruk V, Kramer MR (1999). “Factors predicting mortality of patients with lung abscess”. Chest. 115 (3): 746–50. PMID 10084487.
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Aditya Ganti M.B.B.S. [2]
Overview
There is no screening recommendations for lung abscess.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1];Associate Editor(s)-in-Chief: Aditya Ganti M.B.B.S. [2]
Overview
Symptoms of lung abscess begin approximately 10 days after aspiration of infected material. Symptoms lasting less than 14 days is considered acute lung abscess, while longer lasting symptoms constitute chronic lung abscess. Acute symptoms include a prodrome accompanied by fever, productive cough, pleuritic chest pain and occasional episodes of hemoptysis. Patients with chronic lung abscess develop weight loss and malaise. The prognosis of lung abscess is good with appropriate antibiotic treatment with a high success rate. Complications include hemorrhage, pyopneumothorax, pleural empyema and sepsis.
Natural History
- The symptoms of lung abscess usually develop during the fifth decade of life with risk factors, and start with symptoms such as fever, productive cough, pleuritic chest pain and occasional episodes of hemoptysis, typically developing 8-14 days after aspiration [1]
- Without treatment based on the immune status of the patient, lung abscess can either resolve by forming a granulation tissue scar, or progressively worsens and can result in septicemia, hemorrhage, and death.
Prognosis
The prognosis of lung abscess is good with appropriate antibiotic treatment with a high success rate. The outcomes depend on the other associated conditions underlying lung abscess. The mortality rate of lung abscess is as high as 75% in patients with underlying immunocompromised state and bronchial obstruction favoring poor prognosis. The following factors are considered to be associated with poor prognosis among patients.[2]
- Large size cavities (> 6 cm)
- Old age
- Necrotizing pneumonia
- Prolonged symptoms
- Abscess due to aerobic bacteria and hospital acquired
- Bronchial obstruction due to tumors or foreign body (secondary abscess)
- Immunocompromised individuals
Complications
Without treatment, lung abscess can result in the following complications:
- Hemorrhage [3]
- Pyopneumothorax
- Pleural empyema[4]
- Fibrosis and calcification of lung tissue
- Mediastinal, pleural and cutaneous fistulas
- Sepsis
Reference
- ↑ Adebonojo SA, Osinowo O, Adebo O (1979). “Lung abscess: a review of three years’ experience at the University College Hospital, Ibadan”. J Natl Med Assoc. 71 (1): 39–43. PMC 2537236. PMID 423274.
- ↑ Hirshberg B, Sklair-Levi M, Nir-Paz R, Ben-Sira L, Krivoruk V, Kramer MR (1999). “Factors predicting mortality of patients with lung abscess”. Chest. 115 (3): 746–50. PMID 10084487.
- ↑ Philpott NJ, Woodhead MA, Wilson AG, Millard FJ (1993). “Lung abscess: a neglected cause of life threatening haemoptysis”. Thorax. 48 (6): 674–5. PMC 464615. PMID 8346503.
- ↑ Schattner A, Dubin I, Gelber M (2016). “Double jeopardy – concurrent lung abscess and pleural empyema”. QJM. 109 (8): 545–6. doi:10.1093/qjmed/hcw078. PMID 27208219.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Chest X Ray | CT | MRI | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Related Chapters
Related Chapters
- Other chronic lung infections
- Abscess
- Pleural effusion
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH