
Bronchiectasis
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hamid Qazi, MD, BSc [2], Saarah T. Alkhairy, M.D.
Overview
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hamid Qazi, MD, BSc [2], Saarah T. Alkhairy, M.D.
Overview
Bronchiectasis involves cycles of infections and inflammation that result in alveolar damage and inelastic dilated bronchi. Bronchiectasis may be classified based on either severity of localization of the disease. Bronchiectasis can be caused by both, congenital and acquired factors. Bronchiectasis must be differentiated from other diseases that cause dyspnea and cough, such as COPD, asthma, pneumonia, tuberculosis, chronic sinusitis, cough due to gastrointestinal reflux, upper airway cough syndrome, pulmonary carcinoma, and inhaled foreign body. Bronchiectasis is normally diagnosed after months or years of symptoms. The most common symptoms are a chronic cough and daily sputum production. The most common signs of bronchiectasis are coarse crackles, rhonchi, and wheezes on auscultation. There are both routine investigations and special case investigations. Routine investigations include sputum analysis, full blood count, and quantitative immunoglobulin levels. Cystic fibrosis and autoimmune testing are done if the patient is suspected of having an underlying condition. High-resolution computed tomography (HRCT) is the preferred diagnostic tool in identifying bronchiectasis. Along with treatment of bronchiectasis, it is important to treat the underlying condition if one is present. The medical therapy is divided into medical treatment and physiotherapy strategies. Surgical indications are life-threatening hemoptysis or disease that is unresponsive to medical treatment. Primary prevention of bronchiectasis is aimed at the prevention of future development with the avoidance of harmful substances, vaccinations, maintenance of a healthy body mass index (BMI), and the practice of physiologic strategies. To reduce the impact of the disease, patients should lead a healthy lifestyle, use prophylactic treatment when needed, do vaccinations, and practice physiotherapy strategies.
Historical Perspective
In 1819, René Laennec, inventor of the stethoscope, was the first to describe bronchiectasis. In 1880s, Dr. William Osler, a Canadian physican, was the first to research bronchiectasis in detail.
Pathophysiology
Bronchiectasis involves cycles of infections and inflammation that result in alveolar damage and inelastic dilated bronchi. Damage to the airway results in airflow obstruction and impaired clearance of secretions.
Classification
Bronchiectasis may be classified based on either severity of localization of the disease. Based on severity, there are three pathological subtypes of bronchiectasis: Tubular/fusiform, varicose, and saccular. Based on localization, bronchiectasis may be either localized or generalized.
Causes
Bronchiectasis can be caused by both, congenital and acquired factors. Congenital factors include conditions such as kartagener syndrome, cystic fibrosis, young’s syndrome, yellow nail syndrome, alpha 1-antitrypsin deficiency, and primary immunodeficiencies. Acquired factors include post-infectious, AIDS, IBD, APBD, COPD, airway obstructions, alcohol, drugs, and irritants.
Differential Diagnosis
Bronchiectasis must be differentiated from other diseases that cause dyspnea and cough, such as COPD, asthma, pneumonia, tuberculosis, chronic sinusitis, cough due to gastrointestinal reflux, upper airway cough syndrome, pulmonary carcinoma, and inhaled foreign body.
Epidemiology and Demographics
Bronchiectasis affects extremes of age in certain indigenous populations with a slight female dominance. It is difficult to estimate the prevalence because it is often misdiagnosed. In developed countries, it is important to diagnose the underlying cause. The age of onset is adulthood. In developing countries, infection in childhood is a common cause.
Risk Factors
There are some congenital and acquired conditions that cause inflammation and increased mucus secretion and accumulation of the airways. This repeated cycle leads to the increased risk of bronchiectasis.
Screening
There is no routine screening for bronchiectasis. If the patient has an immune deficiency or primary ciliary dyskinesia then pulmonary function tests should be measures four times a year.
Natural History, Complications, and Prognosis
Bronchiectasis is normally diagnosed after months or years of symptoms. Patients have respiratory complications, infection, and hemoptysis. Death can be caused by cardiac and respiratory failure. Bronchiectasis shows a higher mortality with males, advanced age, poor functional status, severe disease based on radiographic findings, and evidence of hypoxemia and hypercapnia.
History and Symptoms
Symptoms of bronchiectasis can take months or even years to develop. The most common symptoms are a chronic cough and daily sputum production.
Physical Symptoms
The most common signs of bronchiectasis are coarse crackles, rhonchi, and wheezes on auscultation.
Diagnostic Studies
Laboratory Findings
There are both routine investigations and special case investigations. Routine investigations include sputum analysis, full blood count, and quantitative immunoglobulin levels. Cystic fibrosis and autoimmune testing are done if the patient is suspected of having an underlying condition.
Chest X-ray
Although the chest x-ray is not used for diagnosing bronchiectasis, it can be used for patients with respiratory symptoms who are suspected in having any of the differential diagnoses.
CT
High-resolution computed tomography (HRCT) is the preferred diagnostic tool in identifying bronchiectasis. Common findings include increased diameter of a bronchus, tree-in-bud abnormalities, and cysts with definable borders.
Other Imaging Findings
The bronchogram is no longer used for the diagnosis of bronchiectasis.
Other Diagnostic Studies
Other diagnostic tools that can be used are pulmonary function tests, electron microscope examination, and bronchoscopy.
Medical Therapy
Along with treatment of bronchiectasis, it is important to treat the underlying condition if one is present. The medical therapy is divided into medical treatment and physiotherapy strategies. The medical treatment consists of patient education and treatment of the acute exacerbations, prophylactic treatment, vaccination, and other therapies. The physiotherapy strategies focuses on airway clearance and pulmonary rehabilitation.
Surgery
Surgical indications are life-threatening hemoptysis or disease that is unresponsive to medical treatment.
Primary Prevention
Primary prevention of bronchiectasis is aimed at the prevention of future development with the avoidance of harmful substances, vaccinations, maintenance of a healthy body mass index (BMI), and the practice of physiologic strategies.
Secondary Prevention
To reduce the impact of the disease, patients should lead a healthy lifestyle, use prophylactic treatment when needed, do vaccinations, and practice physiotherapy strategies.
References
Historical Perspective
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hamid Qazi, MD, BSc [2], Saarah T. Alkhairy, M.D.
Overview
In 1819, René Laennec, inventor of the stethoscope, described bronchiectasis for the first time. In 1880s, Dr. William Osler, a Canadian physican, has performed detailed researchs on bronchiectasis.
Bronchiectasis Historical Perspective
- In 1819, René Laennec, inventor of the stethoscope, described bronchiectasis for the first time.[1]
- René Laennec described bronchiectasis as an “abnormal dilatation of bronchi and bronchioles due to repeated cycles of airway infection and inflammation.”[2]
- In 1880s, Dr. William Osler, a Canadian physican has performed detailed researchs on bronchiectasis.[3]
References
- ↑ Roguin, A. (2006). “Rene Theophile Hyacinthe Laennec (1781-1826): The Man Behind the Stethoscope”. Clinical Medicine & Research. 4 (3): 230–235. doi:10.3121/cmr.4.3.230. ISSN 1539-4182.
- ↑ O’Donnell, Anne E. (2008). “Bronchiectasis”. CHEST Journal. 134 (4): 815. doi:10.1378/chest.08-0776. ISSN 0012-3692.
- ↑ Wrong, O. (2003). “Osler and my father”. JRSM. 96 (9): 462–464. doi:10.1258/jrsm.96.9.462. ISSN 0141-0768.
Classification
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hamid Qazi, MD, BSc [2], Saarah T. Alkhairy, M.D.
Overview
Bronchiectasis may be classified according to its severity into 3 sub types: tubular/fusiform, varicose, and saccular. Bronchiectasis may also be classified according to its location into 2 sub types: localized and generalized.
Classification
Based on Severity
Based on severity, bronchiectasis may be classified as follows:
| Type | Features |
| Tubular or fusiform (cylindrical) bronchiectasis (follicular bronchiectasis) | Most common type. It is characterized by development of mildly inflamed bronchi that fail to taper distally[1][2] |
| Varicose bronchiectasis | The bronchial walls appear beaded because areas of dilation are mixed with areas of constriction |
| Saccular (cystic) bronchiectasis | These are characterized by severe, irreversible ballooning of the bronchi peripherally, with or without air-fluid levels |
Based on Location
Based on localization, bronchiectasis may be classified as follows:
| Location | Features |
|---|---|
| Localized | Confined to one lobe only |
| Generalized | Involves more than one lobe |
References
Pathophysiology
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hamid Qazi, MD, BSc [2], Saarah T. Alkhairy, M.D.
Overview
Bronchiectasis involves cycles of infections and inflammation that result in alveolar damage and inelastic dilated bronchi. Damage to the airway results in airflow obstruction and impaired clearance of secretions.
Pathophysiology
The following events summarize the pathophysiology of bronchiectasis:[1]
- Dilation of the bronchial walls results in airflow obstruction and impaired clearance of secretions.
- The dilated areas interrupt normal air pressure of the bronchial tubes, causing sputum to pool inside the dilated areas instead of being pushed upward.
- The sputum contains elastase, interleukin-8, tumor necrosis factor alpha (TNF-a), and prostanoids.
- The pooled sputum provides an environment favorable to the growth of infectious pathogens.
- Recurrent infections are followed inflammation and infiltration of neutrophils, macrophages, and T-lymphocytes.
- The more infection that the lungs experience, leads to the sustained inflammation, consequently, damage to the alveoli in the lungs.
- With more injury to the lung tissue, the elasticity in the bronchial tubes is reduced and the tubes are dilated, which creates a perpetual destructive cycle
Cole’s Cycle
The following events summarize Cole’s cycle (Cole’s “vicious cycle hypothesis”), which is the most widely known model of the development of bronchiectasis:[2]
- Two factors are required for the development of bronchiectasis:
- Persistent infection
- Host defense derangement
- Impaired mucociliary clearance due to the genetic susceptibility may cause environmental insult.
- Insults result in persistence of microbes in the sinobronchial tree.
- The microbial infection can cause chronic inflammation, which may result in tissue damage and impaired mucociliary motility.
- Inflammation ensues more infection, which in turn ensues more inflammation.
Immune Response
- Bronchiectasis involves the activity of reactive oxygen species (ROS), elastases, and matrix metalloproteinases (MMPs):
- Reactive oxygen species (ROS)
- A by product for the metabolism of oxygen
- Increased concentration may result in cell structure damage
- Reactive oxygen species (ROS)
- Elastase
- Protease that catalyzes the breaks down of elastin.
- Elastin plus collagen determine the mechanical properties of connective tissue.
- Matrix metalloproteinases (MMPs)
- Responsible for the degradation of the majority of the extracellular proteins during normal tissue turn over.
- Inflammation may result in epithelial injury and mucus secretion via increased concentrations of ROS, elastase ciliotoxin, and mucus secretogogues.
- Epithelial injury and mucus hypersecretion lead to chronic bronchial infection, reduced mucociliary clearance, and plugging of the airway – which all eventually leads to airway damage and bronchiectasis.
The diagram below depicts the immune response for bronchiectasis:
-
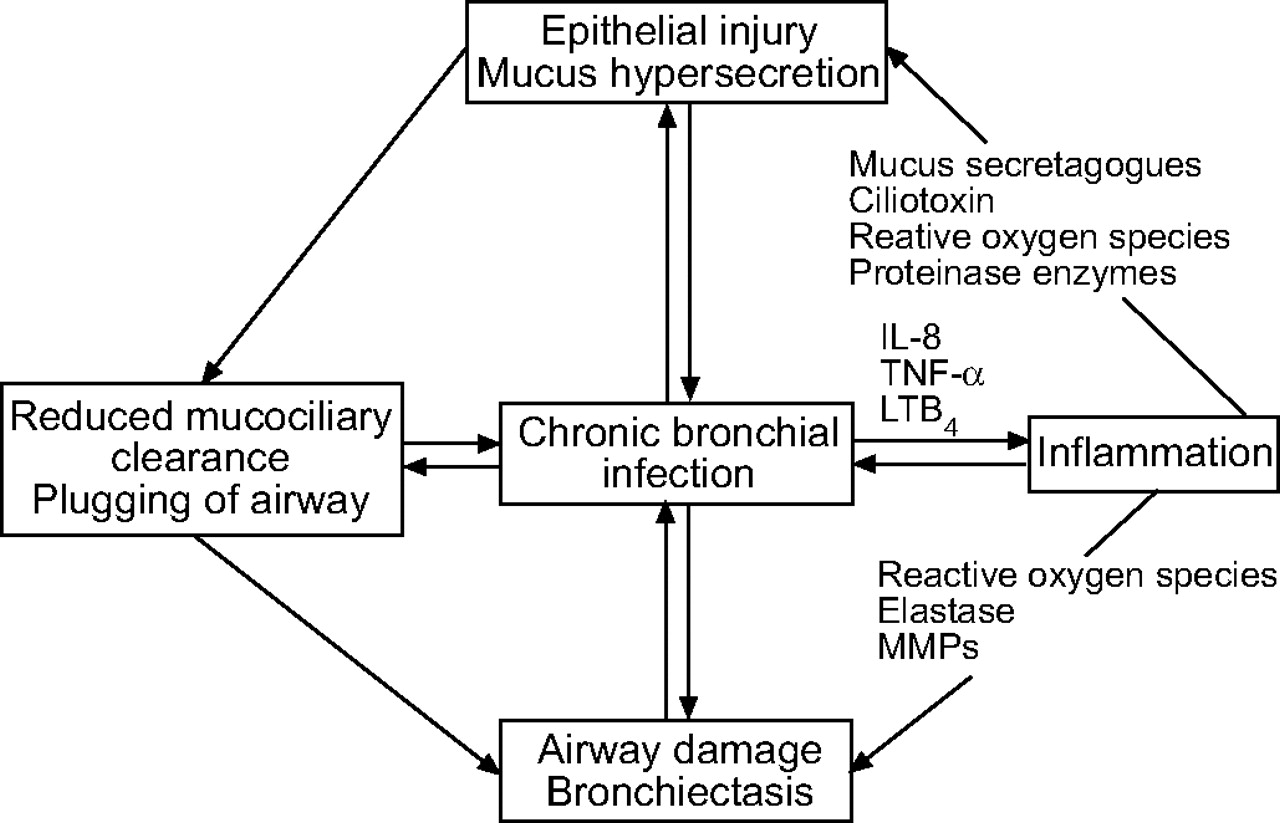 Schematic representation of a vicious circle of events which occurs during chronic bronchial infection. IL: interleukin; TNF: tumour necrosis factor; LT: leukotriene; MMP: matrix metalloproteinase
Schematic representation of a vicious circle of events which occurs during chronic bronchial infection. IL: interleukin; TNF: tumour necrosis factor; LT: leukotriene; MMP: matrix metalloproteinase
European Respiratory Journal

Gross Pathology

References
Template:WH Template:WS
Causes
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hamid Qazi, MD, BSc [2], Saarah T. Alkhairy, M.D., Ogheneochuko Ajari, MB.BS, MS [3]
Overview
Bronchiectasis can be caused by both, congenital and acquired factors. Congenital factors include conditions such as Kartagener syndrome, cystic fibrosis, Young’s syndrome, yellow nail syndrome, alpha 1-antitrypsin deficiency, and primary immunodeficiencies. Acquired factors include post-infectious, AIDS, IBD, ABPA, COPD, airway obstructions, alcohol, drugs, and irritants.
Causes
Life Threatening Causes
Life-threatening causes include conditions which may result in death or permanent disability within 24 hours if left untreated.
Commom causes
- Allergic bronchopulmonary aspergillosis
- Cystic fibrosis
- Kartagener syndrome
- Primary ciliary dyskinesia
Causes by Organ System
Causes in Alphabetical Order
- Adenovirus
- Airway adenoma
- Airway obstruction
- Alcohol
- Allergic bronchopulmonary aspergillosis
- Allergies
- Alpha 1-antitrypsin deficiency
- Ammonia
- Ankylosing spondylitis
- Autoimmune diseases
- Autosomal dominant polycystic kidney disease
- Bloom syndrome
- Bone marrow transplantation
- Bordetella pertussis
- Bronchial cyst
- Bronchiolitis obliterans
- Bronchocentric granulomatosis
- Bronchomalacia
- Bruton’s agammaglobulinemia
- Cartilage deficiency
- Chlorine gas
- Chronic bronchitis
- Chronic granulomatous disease
- Chronic obstructive pulmonary disease
- Common variable immunodeficiency
- Connective tissue disease
- Crohn’s disease
- Cystic fibrosis
- Diffuse panbronchiolitis
- DiGeorge syndrome
- Drug use
- Ectopic bronchus
- Endobronchial teratoma
- Foreign body aspiration
- Heart-lung transplant
- Heroin
- Herpes simplex virus
- Hiatus hernia
- Histoplasmosis
- HIV AIDS
- Hyper-IgE syndrome
- Hypogammaglobulinaemia
- Immotile cilia syndrome
- Immunoglobulin M deficiency
- Inflammatory bowel disease
- Influenza
- Irritable bowel syndrome
- Irritants
- Kartagener syndrome
- Klebsiella
- Laryngeal papillomatosis
- Lipoid pneumonia
- Lung transplantation
- Marfan syndrome
- Measles
- MHC class I deficiency
- Mounier-Kuhn syndrome
- Mycobacterium avium complex
- Mycobacterium tuberculosis
- Mycoplasma pneumoniae
- Nezelof syndrome
- Nitrogen dioxide
- Pertussis
- Pneumonia
- Primary ciliary dyskinesia
- Primary immunodeficiency
- Pseudomonas aeruginosa
- Pulmonary artery aneurysm
- Pulmonary aspiration
- Recurrent aspiration pneumonia
- Relapsing polychondritis
- Respiratory syncytial virus
- Rheumatoid arthritis
- Sarcoidosis
- Selective deficiency of immunoglobulin G
- Selective immunoglobulin A deficiency
- Severe combined immunodeficiency
- Silicates
- Sjögren’s syndrome
- Smoke
- Staphylococcus aureus
- Systemic lupus erythematosus
- Talc
- Tracheobronchial amyloidosis
- Tracheobronchomalacia
- Tracheobronchomegaly
- Tracheoesophageal fistula
- Tuberculosis
- Tumor
- Ulcerative colitis
- WHIM syndrome
- Whooping cough
- Williams-Campbell syndrome
- X-linked agammaglobulinemia
- Yellow nail syndrome
- Young’s syndrome
Causes Based on Mode of Infection
Bronchiectasis may be either congenital or acquired. Acquired bronchiectasis is more common than congenital bronchiectasis.
Congenital
The following table lists the congenital causes of bronchiectasis:
| Causes | Description |
|---|---|
| Kartagener syndrome | Bronchiectasis is secondary to the impaired mobility of cilia in the lungs[1] |
| Cystic fibrosis (CF) | A small number of patients develop severe localized bronchiectasis
Development of bronchiectasis is mainly due to the increased risk of chronic sinopulmonary infections[2] |
| Young’s Syndrome | Similar to CF and may be a genetic variant
Development of bronchiectasis is mainly due to the increased risk of chronic sinopulmonary infections[3] |
| Yellow Nail Syndrome | This is a rare disorder characterized by pleural effusions, lymphedema, and yellow dystrophic nails, chronic bronchitis, sinus infections, and bronchiectasis |
| Alpha 1-Antitrypsin Deficiency (AAD) | The pathophysiology of development of bronchiectasis among these patients is yet to be understood[4] |
| Primary Immunodeficiencies | Bronchiectasis is caused by the weakened immune system’s response to severe, recurrent pulmonary infections[5] |
Acquired
Acquired bronchiectasis is more common than congenital bronchiectasis. The following table lists the acquired causes of bronchiectasis:
| Causes | Description |
|---|---|
| Post Infectious (viral, bacterial, fungal, atypical mycobacterial) | Such as tuberculosis (either from bronchial stenosis or secondary traction from fibrosis), pneumonia, measles, pertussis |
| Acquired Immunodeficiency Syndrome (AIDS) | AIDS is caused by untreated HIV viral infection. Development of bronchiectasis is due to development of opportunistic pulmonary infections[6] |
| Inflammatory Bowel Disease (IBD) | The exact pathogenesis is unknown for the link between inflammatory bowel disease and bronchiectasis
Bronchiectasis is more common among patients with ulcerative colitis than those with Crohn’s disease |
| Allergic Bronchopulmonary Aspergillosis (ABPA) | Development of bronchiectasis is associated with inhalation of fungus spores[7] |
| Connective Tissue Diseases such as Rheumatoid arthritis | Patterns of lung injury are common in connective tissue disease – which eventually leads to bronchiectasis |
| Airway obstructions | Such as tumors or enlarged lymph nodes
These obstructions can block the airways leading to bronchiectasis |
| Chronic Obstructive Pulmonary Disease (COPD) | The mucus build up from COPD can lead to bronchiectasis |
| Environmental exposures such as ammonia | The environmental irritants cause inflammation in the airways that can lead to bronchiectasis |
| Alcoholism | Heavy drinking causes a deficiency of the antioxidant glutathione in the lungs, which increases the susceptibility of various lung diseases including bronchiectasis |
| Drug use such as heroin | Various drugs cause inflammation in the airways that can lead to bronchiectasis |
| Various allergies | Allergies cause inflammation in the airways that can lead to bronchiectasis[8] |
References
- ↑ Morillas HN, Zariwala M, Knowles MR (2007). “Genetic Causes of Bronchiectasis: Primary Ciliary Dyskinesia”. Respiration. 72 (3): 252–63. PMID 17534128.
- ↑ Dalrymple-Hay MJ, Lucas J, Connett G, Lea RE (1999). “Lung resection for the treatment of severe localized bronchiectasis in cystic fibrosis patients”. Acta Chir Hung. 38 (1): 23–5. PMID 10439089.
- ↑ Handelsman DJ, Conway AJ, Boylan LM, & Turtle JR (1984). “Young’s syndrome. Obstructive azoospermia and chronic sinopulmonary infections”. NEJM. 310 (1): 3–9.
- ↑ Shin MS, Ho KJ (1993). “Bronchiectasis in patients with alpha 1-antitrypsin deficiency. A rare occurrence?”. Chest. 104: 1384–86.
- ↑ Notarangelo LD, Plebani A, Mazzolari E, Soresina A, Bondioni MP (2007). “Genetic causes of bronchiectasis: primary immune deficiencies and the lung”. Respiration. 74 (3): 264–75. PMID 17534129.
- ↑ Sheikh S, Madiraju K, Steiner P, Rao M (1997). “Bronchiectasis in pediatric AIDS”. Chest. 112 (5): 1202–7. PMID 9367458.
- ↑ Ferguson HR, Convery RP (2002). “An unusual complication of ulcerative colitis”. Postgrad. Med. J. 78: 503.
- ↑ Lamari NM, Martins ALQ, Oliveira JV, Marino LC, Valério N (2006). “Bronchiectasis and clearence physiotherapy: emphasis in postural drainage and percussion”. Braz. j. cardiovasc. surg. (in Portuguese). 21 (2).
Template:WH Template:WS
Differentiating Bronchiectasis from other Disorders
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hamid Qazi, MD, BSc [2], Saarah T. Alkhairy, M.D.
Overview
Bronchiectasis must be differentiated from other diseases that cause dyspnea and cough, such as COPD, asthma, pneumonia, tuberculosis, chronic sinusitis, lung cancer, postnasal drip and inhaled foreign body.
Bronchiectasis Differential Diagnosis
The following table lists the most common differential diagnoses of bronchiectasis based on chronic cough:[1][2]
| Organ system | Diseases | Clinical manifestations | Diagnosis | Other features | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Symptoms | Physical exam | ||||||||||||||
| Onset | Duration | Productive cough | Hemoptysis | Weight lost | Fever | Dyspnea | Ascultation | Lab findings | Imaging | PFT | Gold standard | ||||
| Respiratory | Upper airway diseases | Laryngopharyngeal reflux[3][4] | Chronic |
|
+ | − | − | − | + |
|
|
|
| ||
| Rhinosinusitis[5][6] | Acute, subacute, chronic, recurrent | + | − | − | + | + |
|
|
|
|
| ||||
| Organ system | Diseases | Clinical manifestations | Diagnosis | Other features | |||||||||||
| Symptoms | Physical exam | ||||||||||||||
| Onset | Duration | Productive cough | Hemoptysis | Weight lost | Fever | Dyspnea | Ascultation | Lab findings | Imaging | PFT | Gold standard | ||||
| Respiratory | Lower airway | Asthma[7] | Chronic |
|
+ Clear mucoid or yellow sputum | − | − | − | + |
|
|
|
|
| |
| Chronic Bronchitis[8][9] | Chronic |
|
+ Clear sputum | − | − | + | + |
|
|
|
| ||||
| Non−asthmatic eosinophilic bronchitis[10][11] | Chronic |
|
+ Eosinophilic sputum | − | − | − | + |
|
|
|
| ||||
| Bronchiectasis[12] | Chronic |
|
+ Mucopurulent sputum | + | − | − | + |
|
|
|
| ||||
| Emphysema [13] | Chronic |
|
+ Mucoid or purulent sputum | − | − | + | + |
|
|
|
|
| |||
| Organ system | Diseases | Clinical manifestations | Diagnosis | Other features | |||||||||||
| Symptoms | Physical exam | ||||||||||||||
| Onset | Duration | Productive cough | Hemoptysis | Weight lost | Fever | Dyspnea | Ascultation | Lab findings | Imaging | PFT | Gold standard | ||||
| Respiratory | Parenchyma | Pneumoconioses[14][15] | Acute, Chronic |
|
− | − | + | + | + |
|
|
||||
| Lung cancer[16][17] | Chronic |
|
+ | + | + | +/− | + | The following investigations may be helpful: |
|
|
| ||||
| Interstitial lung disease[18][19] | Chronic |
|
− | + | + | − | + |
|
The following investigations may be helpful: |
|
|
| |||
| Tuberculosis (TB)[20][21] | Chronic |
|
+ | + | + | + | + |
|
|
|
|
| |||
| Cystic fibrosis (CF)[22][23] | Chronic |
|
+ | − | + | +/− | + |
|
|
| |||||
| Organ system | Diseases | Clinical manifestations | Diagnosis | Other features | |||||||||||
| Symptoms | Physical exam | ||||||||||||||
| Onset | Duration | Productive cough | Hemoptysis | Weight lost | Fever | Dyspnea | Ascultation | Lab findings | Imaging | PFT | Gold standard | ||||
| [[[Heart|Cardiac]] | Mitral Stenosis[24][25] | Chronic |
|
+ Pink frothy | + | − | − | + |
|
|
|
|
|||
| Pulmonary hypertension[26][27] | Chronic |
|
− | + | + | − | + | The following investigations may be helpful: |
|
|
| ||||
| Gastrointestinal | Gastroesophageal reflux[28][29] | Chronic |
|
+ | − | + | − | + |
|
|
|
|
−− | ||
| Organ system | Diseases | Clinical manifestations | Diagnosis | Other features | |||||||||||
| Symptoms | Physical exam | ||||||||||||||
| Onset | Duration | Productive cough | Hemoptysis | Weight lost | Fever | Dyspnea | Ascultation | Lab findings | Imaging | PFT | Gold standard | ||||
| Autoimmune | Goodpasture syndrome[30][31] | Chronic |
|
− | + | − | − | + | The following investigations may be helpful:
|
|
|
||||
| Wegener’s disease (GPA) [32][33] | Chronic |
|
+ | + | + | + | + | The following investigations may be helpful: |
|
|
|
| |||
| Sarcoidosis[34][35] | Chronic |
|
− | − | + | + | + |
|
The following investigations may be helpful: |
|
|
||||
| Microscopic polyangitis (MPA)[36] | Chronic |
|
+ | + | + | + | + | The following investigations may be helpful:
|
|
|
|
| |||
| Churg−Strauss[37][38] | Chronic |
|
+ | + | + | + | + |
|
|
|
|
||||
Cough
The differential diagnosis according to cough for bronchiectasis is shown in the table below:
| Organ system | Diseases | Clinical manifestations | Diagnosis | Other features | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Symptoms | Physical exam | ||||||||||||||
| Onset | Duration | Productive cough | Hemoptysis | Weight lost | Fever | Dyspnea | Ascultation | Lab findings | Imaging | PFT | Gold standard | ||||
| Respiratory | Upper airway diseases | Epiglottitis[39][40] | Abrupt or acute |
|
– | – | – | ✔ | ✔ |
|
|
|
|
| |
| Croup[41] | Acute |
|
✔ | – | – | – | ✔ |
|
|
|
|
| |||
| Pertussis[42][43] | Acute |
|
✔ Whooping sound | – | ✔ | – | ✔ |
|
|
|
|
| |||
| Laryngopharyngeal reflux[3][4] | Chronic |
|
✔ | – | – | – | ✔ |
|
|
|
| ||||
| Common Cold[44] | Acute |
|
✔ | – | – | ✔ | – |
|
|
|
|
||||
| Seasonal Influenza [45] | Acute |
|
– | – | – | ✔ | ✔ |
|
|
|
| ||||
| Rhinosinusitis[5][6] | Acute, subacute, chronic, recurrent | ✔ | – | – | ✔ | ✔ |
|
|
|
|
| ||||
| Lower airway | Asthma[7] | Chronic |
|
✔ Clear mucoid or yellow sputum | – | – | – | ✔ |
|
|
|
|
| ||
| Acute Bronchitis[46] | Acute |
|
✔ | – | – | – | ✔ |
|
|
|
|
| |||
| Chronic Bronchitis[8][9] | Chronic |
|
✔ Clear sputum | – | – | ✔ | ✔ |
|
|
|
| ||||
| Non-asthmatic eosinophilic bronchitis[10][11] | Chronic |
|
✔ Eosinophilic sputum | – | – | ✔ |
|
|
|
| |||||
| Bronchiectasis[12] | Chronic |
|
✔ Mucopurulent sputum | ✔ | – | ✔ |
|
|
|
| |||||
| Emphysema [13] | Chronic |
|
✔ Mucoid or purulent sputum | – | – | ✔ | ✔ |
|
|
|
|
| |||
| Foreing body aspiration[47][48][49] | Acute |
|
✔ | ✔ | – | ✔ | ✔ |
|
|
|
|
| |||
| Bronchiolitis[50][51] | Acute |
|
✔ | – | ✔ | ✔ |
|
|
|
|
| ||||
| Parenchyma | Pneumonia[52][53] | Acute |
|
✔ Mucopurulent sputum | – | – | ✔ | ✔ |
|
|
|
|
|||
| Pneumoconioses[14][15] | Acute, Chronic |
|
– | – | ✔ | ✔ | ✔ |
|
|
||||||
| Lung cancer[16][17] | Chronic |
|
✔ | ✔ | ✔ | – | ✔ |
|
|
| |||||
| Interstitial lung disease[18][19] | Chronic |
|
– | ✔ | ✔ | – | ✔ |
|
|
|
|
| |||
| Tuberculosis (TB)[20][21] | Chronic |
|
✔ | ✔ | ✔ | ✔ | ✔ |
|
|
|
|
| |||
| Cystic fibrosis (CF)[22][23] | Chronic |
|
✔ | – | ✔ | ✔ |
|
|
| ||||||
| Cardiac | Cardiogenic pulmonary edema[54][55] | Acute |
|
✔ Pink frothy, liquid | – | ✔ | – | ✔ |
|
|
|
|
| ||
| Mitral Stenosis[24][25] | Chronic |
|
✔ Pink frothy | ✔ | – | – | ✔ |
|
|
|
|
||||
| Pulmonary hypertension[26][27] | Chronic |
|
– | ✔ | ✔ | – | ✔ |
|
|
| |||||
| Gastrointestinal | Gastroesophageal reflux[28][29] | Chronic |
|
✔ | – | ✔ | – | ✔ |
|
|
|
|
— | ||
| Autoinmune | Goodpasture syndrome[30][31] | Chronic |
|
– | ✔ | – | – | ✔ |
|
|
|
||||
| Wegener’s disease (GPA) [32][33] | Chronic |
|
✔ | ✔ | ✔ | ✔ | ✔ |
|
|
|
| ||||
| Sarcoidosis[34][35] | Chronic |
|
– | – | ✔ | ✔ | ✔ |
|
|
|
|||||
| Microscopic polyangitis (MPA)[36] | Chronic |
|
✔ | ✔ | ✔ | ✔ | ✔ |
|
|
|
|
| |||
| Churg-Strauss[37][38] | Chronic |
|
✔ | ✔ | ✔ | ✔ | ✔ |
|
|
|
|
||||
| Medication | ACE inhibitors[56][57] | Acute (depend on the medication) |
|
– | – | – | – | ✔ |
|
|
|
|
| ||
Features that may suggest bronchiectasis in a patient presenting with chronic respiratory symptoms
- Digital clubbing
- Lack of a significant smoking history (if COPD is suspected)
- History of recurrent and/or severe pneumonia or tuberculosis
- Presence of either Aspergillus, atypical/nontuberculous Mycobacteria, Pseudomonas aeruginosa, Escherichia coli, or Klebsiella pneumoniae in the sputum
References
- ↑ O’Donnell, Anne E. (2008). “Bronchiectasis”. Chest. 134 (4): 815–823. doi:10.1378/chest.08-0776. ISSN 0012-3692.
- ↑ Morrissey BM (2007). “Pathogenesis of bronchiectasis”. Clin Chest Med. 28 (2): 289–96. PMID 17467548.
- ↑ 3.0 3.1 “What is LPR? | American Academy of Otolaryngology-Head and Neck Surgery”.
- ↑ 4.0 4.1 Noordzij JP, Khidr A, Desper E, Meek RB, Reibel JF, Levine PA (2002). “Correlation of pH probe-measured laryngopharyngeal reflux with symptoms and signs of reflux laryngitis”. Laryngoscope. 112 (12): 2192–5. doi:10.1097/00005537-200212000-00013. PMID 12461340.
- ↑ 5.0 5.1 Meltzer EO, Hamilos DL (2011). “Rhinosinusitis diagnosis and management for the clinician: a synopsis of recent consensus guidelines”. Mayo Clin Proc. 86 (5): 427–43. doi:10.4065/mcp.2010.0392. PMC 3084646. PMID 21490181.
- ↑ 6.0 6.1 Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, Brook I, Ashok Kumar K, Kramper M, Orlandi RR, Palmer JN, Patel ZM, Peters A, Walsh SA, Corrigan MD (2015). “Clinical practice guideline (update): adult sinusitis”. Otolaryngol Head Neck Surg. 152 (2 Suppl): S1–S39. doi:10.1177/0194599815572097. PMID 25832968.
- ↑ 7.0 7.1 Ukena D, Fishman L, Niebling WB (2008). “Bronchial asthma: diagnosis and long-term treatment in adults”. Dtsch Arztebl Int. 105 (21): 385–94. doi:10.3238/arztebl.2008.0385. PMC 2696883. PMID 19626179.
- ↑ 8.0 8.1 Brusasco V, Martinez F (2014). “Chronic obstructive pulmonary disease”. Compr Physiol. 4 (1): 1–31. doi:10.1002/cphy.c110037. PMID 24692133.
- ↑ 9.0 9.1 Qaseem A, Snow V, Shekelle P, Sherif K, Wilt TJ, Weinberger S, Owens DK (2007). “Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline from the American College of Physicians”. Ann. Intern. Med. 147 (9): 633–8. PMID 17975186.
- ↑ 10.0 10.1 Brightling CE (2006). “Chronic cough due to nonasthmatic eosinophilic bronchitis: ACCP evidence-based clinical practice guidelines”. Chest. 129 (1 Suppl): 116S–121S. doi:10.1378/chest.129.1_suppl.116S. PMID 16428700.
- ↑ 11.0 11.1 Cho J, Choi SM, Lee J, Park YS, Lee SM, Yoo CG; et al. (2018). “Clinical Outcome of Eosinophilic Airway Inflammation in Chronic Airway Diseases Including Nonasthmatic Eosinophilic Bronchitis”. Sci Rep. 8 (1): 146. doi:10.1038/s41598-017-18265-2. PMC 5760521. PMID 29317659.
- ↑ 12.0 12.1 King PT, Holdsworth SR, Freezer NJ, Villanueva E, Holmes PW (2006). “Characterisation of the onset and presenting clinical features of adult bronchiectasis”. Respir Med. 100 (12): 2183–9. doi:10.1016/j.rmed.2006.03.012. PMID 16650970.
- ↑ 13.0 13.1 Rossi A, Butorac-Petanjek B, Chilosi M, Cosío BG, Flezar M, Koulouris N; et al. (2017). “Chronic obstructive pulmonary disease with mild airflow limitation: current knowledge and proposal for future research – a consensus document from six scientific societies”. Int J Chron Obstruct Pulmon Dis. 12: 2593–2610. doi:10.2147/COPD.S132236. PMC 5587130. PMID 28919728.
- ↑ 14.0 14.1 Jp NA, Imanaka M, Suganuma N (2017). “Japanese workplace health management in pneumoconiosis prevention”. J Occup Health. 59 (2): 91–103. doi:10.1539/joh.16-0031-RA. PMC 5478517. PMID 27980247.
- ↑ 15.0 15.1 Weiland DA, Lynch DA, Jensen SP, Newell JD, Miller DE, Crausman RS, Kuhn C, Kern DG (2003). “Thin-section CT findings in flock worker’s lung, a work-related interstitial lung disease”. Radiology. 227 (1): 222–31. doi:10.1148/radiol.2271011063. PMID 12668748.
- ↑ 16.0 16.1 Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D (2011). “Global cancer statistics”. CA Cancer J Clin. 61 (2): 69–90. doi:10.3322/caac.20107. PMID 21296855.
- ↑ 17.0 17.1 Ost DE, Jim Yeung SC, Tanoue LT, Gould MK (2013). “Clinical and organizational factors in the initial evaluation of patients with lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines”. Chest. 143 (5 Suppl): e121S–e141S. doi:10.1378/chest.12-2352. PMC 4694609. PMID 23649435.
- ↑ 18.0 18.1 Lama VN, Martinez FJ (2004). “Resting and exercise physiology in interstitial lung diseases”. Clin. Chest Med. 25 (3): 435–53, v. doi:10.1016/j.ccm.2004.05.005. PMID 15331185.
- ↑ 19.0 19.1 Chetta A, Marangio E, Olivieri D (2004). “Pulmonary function testing in interstitial lung diseases”. Respiration. 71 (3): 209–13. doi:10.1159/000077416. PMID 15133338.
- ↑ 20.0 20.1 Perlman DC, el-Sadr WM, Nelson ET, Matts JP, Telzak EE, Salomon N, Chirgwin K, Hafner R (1997). “Variation of chest radiographic patterns in pulmonary tuberculosis by degree of human immunodeficiency virus-related immunosuppression. The Terry Beirn Community Programs for Clinical Research on AIDS (CPCRA). The AIDS Clinical Trials Group (ACTG)”. Clin. Infect. Dis. 25 (2): 242–6. PMID 9332519.
- ↑ 21.0 21.1 Barnes PF, Verdegem TD, Vachon LA, Leedom JM, Overturf GD (1988). “Chest roentgenogram in pulmonary tuberculosis. New data on an old test”. Chest. 94 (2): 316–20. PMID 2456183.
- ↑ 22.0 22.1 Farrell PM, Rosenstein BJ, White TB, Accurso FJ, Castellani C, Cutting GR, Durie PR, Legrys VA, Massie J, Parad RB, Rock MJ, Campbell PW (2008). “Guidelines for diagnosis of cystic fibrosis in newborns through older adults: Cystic Fibrosis Foundation consensus report”. J. Pediatr. 153 (2): S4–S14. doi:10.1016/j.jpeds.2008.05.005. PMC 2810958. PMID 18639722.
- ↑ 23.0 23.1 Kerem E, Reisman J, Corey M, Canny GJ, Levison H (1992). “Prediction of mortality in patients with cystic fibrosis”. N. Engl. J. Med. 326 (18): 1187–91. doi:10.1056/NEJM199204303261804. PMID 1285737.
- ↑ 24.0 24.1 MUNROE DS, RALLY CR (1963). “The diagnosis of mitral stenosis”. Can Med Assoc J. 88: 611–22. PMC 1921207. PMID 13936649.
- ↑ 25.0 25.1 Chandrashekhar Y, Westaby S, Narula J (2009). “Mitral stenosis”. Lancet. 374 (9697): 1271–83. doi:10.1016/S0140-6736(09)60994-6. PMID 19747723.
- ↑ 26.0 26.1 Brown LM, Chen H, Halpern S, Taichman D, McGoon MD, Farber HW, Frost AE, Liou TG, Turner M, Feldkircher K, Miller DP, Elliott CG (2011). “Delay in recognition of pulmonary arterial hypertension: factors identified from the REVEAL Registry”. Chest. 140 (1): 19–26. doi:10.1378/chest.10-1166. PMC 3198486. PMID 21393391.
- ↑ 27.0 27.1 Sun XG, Hansen JE, Oudiz RJ, Wasserman K (2003). “Pulmonary function in primary pulmonary hypertension”. J Am Coll Cardiol. 41 (6): 1028–35. PMID 12651053.
- ↑ 28.0 28.1 Kahrilas PJ, Hughes N, Howden CW (2011). “Response of unexplained chest pain to proton pump inhibitor treatment in patients with and without objective evidence of gastro-oesophageal reflux disease”. Gut. 60 (11): 1473–8. doi:10.1136/gut.2011.241307. PMID 21508423.
- ↑ 29.0 29.1 Badillo R, Francis D (2014). “Diagnosis and treatment of gastroesophageal reflux disease”. World J Gastrointest Pharmacol Ther. 5 (3): 105–12. doi:10.4292/wjgpt.v5.i3.105. PMC 4133436. PMID 25133039.
- ↑ 30.0 30.1 Boyce NW, Holdsworth SR (1986). “Pulmonary manifestations of the clinical syndrome of acute glomerulonephritis and lung hemorrhage”. Am. J. Kidney Dis. 8 (1): 31–6. PMID 3728460.
- ↑ 31.0 31.1 Foster MH (2017). “Basement membranes and autoimmune diseases”. Matrix Biol. 57-58: 149–168. doi:10.1016/j.matbio.2016.07.008. PMC 5290253. PMID 27496347.
- ↑ 32.0 32.1 Hoffman GS, Kerr GS, Leavitt RY, Hallahan CW, Lebovics RS, Travis WD, Rottem M, Fauci AS (1992). “Wegener granulomatosis: an analysis of 158 patients”. Ann. Intern. Med. 116 (6): 488–98. PMID 1739240.
- ↑ 33.0 33.1 Falk RJ, Gross WL, Guillevin L, Hoffman GS, Jayne DR, Jennette JC, Kallenberg CG, Luqmani R, Mahr AD, Matteson EL, Merkel PA, Specks U, Watts RA (2011). “Granulomatosis with polyangiitis (Wegener’s): an alternative name for Wegener’s granulomatosis”. Arthritis Rheum. 63 (4): 863–4. doi:10.1002/art.30286. PMID 21374588.
- ↑ 34.0 34.1 Carmona EM, Kalra S, Ryu JH (2016). “Pulmonary Sarcoidosis: Diagnosis and Treatment”. Mayo Clin. Proc. 91 (7): 946–54. doi:10.1016/j.mayocp.2016.03.004. PMID 27378039.
- ↑ 35.0 35.1 Yanardağ H, Pamuk GE, Karayel T, Demirci S (2002). “Bone marrow involvement in sarcoidosis: an analysis of 50 bone marrow samples”. Haematologia (Budap). 32 (4): 419–25. PMID 12803116.
- ↑ 36.0 36.1 Jennette, J. Charles; Falk, Ronald J. (1997). “Small-Vessel Vasculitis”. New England Journal of Medicine. 337 (21): 1512–1523. doi:10.1056/NEJM199711203372106. ISSN 0028-4793.
- ↑ 37.0 37.1 Vaglio A, Buzio C, Zwerina J (2013). “Eosinophilic granulomatosis with polyangiitis (Churg-Strauss): state of the art”. Allergy. 68 (3): 261–73. doi:10.1111/all.12088. PMID 23330816.
- ↑ 38.0 38.1 Lanham JG, Elkon KB, Pusey CD, Hughes GR (1984). “Systemic vasculitis with asthma and eosinophilia: a clinical approach to the Churg-Strauss syndrome”. Medicine (Baltimore). 63 (2): 65–81. PMID 6366453.
- ↑ Stroud RH, Friedman NR (2001). “An update on inflammatory disorders of the pediatric airway: epiglottitis, croup, and tracheitis”. Am J Otolaryngol. 22 (4): 268–75. doi:10.1053/ajot.2001.24825. PMID 11464324.
- ↑ Solomon P, Weisbrod M, Irish JC, Gullane PJ (1998). “Adult epiglottitis: the Toronto Hospital experience”. J Otolaryngol. 27 (6): 332–6. PMID 9857318.
- ↑ Cherry, James D. (2008). “Croup”. New England Journal of Medicine. 358 (4): 384–391. doi:10.1056/NEJMcp072022. ISSN 0028-4793.
- ↑ Bellamy EA, Johnston ID, Wilson AG (1987). “The chest radiograph in whooping cough”. Clin Radiol. 38 (1): 39–43. PMID 3816065.
- ↑ “Pertussis | Whooping Cough | Clinical | Information | CDC”.
- ↑ Eccles R (2005). “Understanding the symptoms of the common cold and influenza”. Lancet Infect Dis. 5 (11): 718–25. doi:10.1016/S1473-3099(05)70270-X. PMID 16253889.
- ↑ Kim EA, Lee KS, Primack SL, Yoon HK, Byun HS, Kim TS, Suh GY, Kwon OJ, Han J (2002). “Viral pneumonias in adults: radiologic and pathologic findings”. Radiographics. 22 Spec No: S137–49. doi:10.1148/radiographics.22.suppl_1.g02oc15s137. PMID 12376607.
- ↑ Wenzel RP, Fowler AA (2006). “Clinical practice. Acute bronchitis”. N. Engl. J. Med. 355 (20): 2125–30. doi:10.1056/NEJMcp061493. PMID 17108344.
- ↑ Hewlett JC, Rickman OB, Lentz RJ, Prakash UB, Maldonado F (2017). “Foreign body aspiration in adult airways: therapeutic approach”. J Thorac Dis. 9 (9): 3398–3409. doi:10.21037/jtd.2017.06.137. PMC 5708401. PMID 29221325.
- ↑ Rafanan AL, Mehta AC (2001). “Adult airway foreign body removal. What’s new?”. Clin. Chest Med. 22 (2): 319–30. PMID 11444115.
- ↑ Haddadi S, Marzban S, Nemati S, Ranjbar Kiakelayeh S, Parvizi A, Heidarzadeh A (2015). “Tracheobronchial Foreign-Bodies in Children; A 7 Year Retrospective Study”. Iran J Otorhinolaryngol. 27 (82): 377–85. PMC 4639691. PMID 26568942.
- ↑ Bordley WC, Viswanathan M, King VJ, Sutton SF, Jackman AM, Sterling L, Lohr KN (2004). “Diagnosis and testing in bronchiolitis: a systematic review”. Arch Pediatr Adolesc Med. 158 (2): 119–26. doi:10.1001/archpedi.158.2.119. PMID 14757603.
- ↑ “www.nice.org.uk”.
- ↑ Bartlett JG, Dowell SF, Mandell LA, File Jr TM, Musher DM, Fine MJ (2000). “Practice guidelines for the management of community-acquired pneumonia in adults. Infectious Diseases Society of America”. Clin. Infect. Dis. 31 (2): 347–82. doi:10.1086/313954. PMID 10987697.
- ↑ Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, Dowell SF, File TM, Musher DM, Niederman MS, Torres A, Whitney CG (2007). “Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults”. Clin. Infect. Dis. 44 Suppl 2: S27–72. doi:10.1086/511159. PMID 17278083.
- ↑ Gheorghiade M, Zannad F, Sopko G, Klein L, Piña IL, Konstam MA, Massie BM, Roland E, Targum S, Collins SP, Filippatos G, Tavazzi L (2005). “Acute heart failure syndromes: current state and framework for future research”. Circulation. 112 (25): 3958–68. doi:10.1161/CIRCULATIONAHA.105.590091. PMID 16365214.
- ↑ Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, Johnson MR, Kasper EK, Levy WC, Masoudi FA, McBride PE, McMurray JJ, Mitchell JE, Peterson PN, Riegel B, Sam F, Stevenson LW, Tang WH, Tsai EJ, Wilkoff BL (2013). “2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines”. Circulation. 128 (16): e240–327. doi:10.1161/CIR.0b013e31829e8776. PMID 23741058.
- ↑ Israili ZH, Hall WD (1992). “Cough and angioneurotic edema associated with angiotensin-converting enzyme inhibitor therapy. A review of the literature and pathophysiology”. Ann. Intern. Med. 117 (3): 234–42. PMID 1616218.
- ↑ Wood R (1995). “Bronchospasm and cough as adverse reactions to the ACE inhibitors captopril, enalapril and lisinopril. A controlled retrospective cohort study”. Br J Clin Pharmacol. 39 (3): 265–70. PMC 1365002. PMID 7619667.
Epidemiology and Demographics
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hamid Qazi, MD, BSc [2], Saarah T. Alkhairy, M.D.
Overview
Bronchiectasis affects extremes of age in certain indigenous populations with a slight female dominance. It is difficult to estimate the prevalence because it is often misdiagnosed. In developed countries, it is important to diagnose the underlying cause and in these countries the age of onset mostly is in adulthood. In developing countries, infection in childhood period is a common cause.
Epidemiology and Demographics
Prevalence and Incidence
- The true prevalence of bronchiectasis is uknown, given that bronchiectasis remains underdiagnosed and is often misdiagnosed as either asthma or COPD. The estimated prevalence of bronchiectasis in USA is approximately 30 to 40 per 100,000 individuals.[1]
- In USA, the average annual bronchiectasis-associated hospitalization rate approximately 16.5 per 100,000 hospitalizations.[1]
Age
- Bronchiectasis predominantly affect extremes of age.[1]
- The prevalence of bronchiectasis rises steeply from 4-5 per 100,000 adults aged 18-34 years to 250 to 300 per 100,000 individuals aged > 75 years.[1]
Gender
- Predominantly women
- The women that are infected with primary Mycobacterium avium complex (MAC) tend to be Caucasian, slender, and older than 60 years. It is given the name of Lady Windermere syndrome which is named after a character in a novel by Oscar Wilde.
- Annual increase of about 2.4% in men and 3.0% in women for bronchiectasis-associated hospitalizations.[1]
Race
- There is no known association of increased incidence of the bronchiectasis and a particular race.
- Very high prevalence in certain indigenous populations such as Alaskan natives with 10-20/1000 children affected.[1]
Developed Countries
- Before antibiotics, the symptoms on bronchiectasis began in the patient’s first decade of life. In developed countries, the age of onset has move to adulthood (except those with cysts fibrosis).[2]
- It is important to understand the underlying cause before initiating treatment.[2]
Developing Countries
- Infections are an important cause of bronchiectasis because the disease may not be diagnosed or be treated properly in the developing countries.[3]
- Bronchiectasis is a large concern for pediatricians because children are largely affected.[3]
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 McDonnell MJ, Ward C, Lordan JL, Rutherford RM (2013). “Non-cystic fibrosis bronchiectasis”. QJM. 106 (8): 709–15. doi:10.1093/qjmed/hct109. PMID 23728208.
- ↑ 2.0 2.1 Bilton, Diana (2008). “Update on non-cystic fibrosis bronchiectasis”. Current Opinion in Pulmonary Medicine. 14 (6): 595–599. doi:10.1097/MCP.0b013e328312ed8c. ISSN 1070-5287.
- ↑ 3.0 3.1 Karadag, B.; Karakoc, F.; Ersu, R.; Kut, A.; Bakac, S.; Dagli, E. (2005). “Non-Cystic-Fibrosis Bronchiectasis in Children: A Persisting Problem in Developing Countries”. Respiration. 72 (3): 233–238. doi:10.1159/000085362. ISSN 1423-0356.
Template:WH Template:WS
Risk Factors
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hamid Qazi, MD, BSc [2], Saarah T. Alkhairy, M.D.
Overview
Common risk factors in the development of bronchiectasis include cystic fibrosis, primary ciliary dyskinesia, exposure to chemical irritants, connective tissue disease, immunodeficiencies, allergic bronchopulmonary aspergillosis (ABPA), and history of childhood infections such as pneumonia, tuberculosis, measles, whooping cough, adenovirus, and Mycoplasma pneumoniae.
Bronchiectasis Risk Factors
The risk factors are mainly the primary causes of bronchiectasis.
The following table lists the most common risk factors of bronchiectasis:[1]
| Risk | Factor Description |
|---|---|
| Cystic fibrosis | Due to ciliary dysfunction, the mucous secretion accumulates in the airways. This leads to increased infection and damage to the airways. |
| Primary ciliary dyskinesia | Due to ciliary dysfunction, the mucous secretion accumulates in the airways. This leads to increased infection and damage to the airways. |
| Childhood infections such as pneumonia, tuberculosis, measles, whooping cough, adenovirus, and Mycoplasma pneumoniae | These infections damage the airways, which leads to more infections |
| Retained foreign object | This prevents mucus from clearing from the airway |
| Exposure to chemical irritants | This leads to inflammation and mucous secretion |
| Connective tissue disease | This leads to pulmonary fibrosis, inflammation of the airways, and traction bronchiectasis |
| Immunodeficiencies | There are increased infections and mucus secretion |
| Allergic Bronchopulmonary Aspergillosis (ABPA) | The allergic reaction to the fungus aspergillus causes inflammation of the airways, repeated infections, and accumulation of mucus |
| Toxic fumes, gases, smoke, and other harmful substances | There cause irritation and inflammation of the airways |
| Low BMI | It is associated with low immune function, leading to increased infections |
References
Template:WH Template:WS
Screening
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hamid Qazi, MD, BSc [2], Saarah T. Alkhairy, M.D.
Overview
There is no routine screening for bronchiectasis. If the patient has an immune deficiency or primary ciliary dyskinesia then pulmonary function tests should be measures four times a year.
Bronchiectasis Screening
- There is no routine screening for bronchiectasis.
- If the patient has an immune deficiency or primary ciliary dyskinesia, the forced expiratory volume in one second (FEV1), forced vital capacity (FVC), and peak expiratory flow (PEF) should be measured four times a year.[1]
References
- ↑ van der Bruggen-Bogaarts BA, van der Bruggen HM, van Waes PF, Lammers JW (1996). “Screening for bronchiectasis. A comparative study between chest radiography and high-resolution CT”. Chest. 109 (3): 608–11. PMID 8617064.
Natural History, Complications and Prognosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hamid Qazi, MD, BSc [2], Saarah T. Alkhairy, M.D.
Overview
Bronchiectasis is normally diagnosed after months or years of symptoms. Patients have respiratory complications, infection, and hemoptysis. Death can be caused by cardiac and respiratory failure. Bronchiectasis shows a higher mortality with males, advanced age, poor functional status, severe disease based on radiographic findings, and evidence of hypoxemia and hypercapnia.
Natural History
- There is often a delay between the onset of symptoms and diagnosis
- The classic symptoms are cough, daily mucopurulent sputum production, and dyspnea
- These symptoms are usually present for months to years
- The symptoms are manifestations of the lung being repeatedly damaged due to any number of causes
- Over the years the patient can develop recurrent infections, massive hemoptysis, and pulmonary hypertension
- In about 8-10 years, there is a high mortality rate due to cor pulmonale or respiratory failure
Complications
- Recurrent infection
- Increased sputum production
- Dyspnea
- Massive hemoptysis
- Pulmonary hypertension
Prognosis
- Bronchiectasis has been shown to contribute to early mortality[1]
- Early mortality is associated with
- Infected with Pseudomonas aeruginosa, severe exacerbations, and systemic inflammation are associated with disease advancement
- Up to 10% of adults die within 5-8 years of diagnosis (majority being respiratory related)[6]
References
- ↑ 1.0 1.1 McDonnell MJ, Ward C, Lordan JL, Rutherford RM (2013). “Non-cystic fibrosis bronchiectasis”. QJM. 106 (8): 709–15. doi:10.1093/qjmed/hct109. PMID 23728208.
- ↑ Onen ZP, Eris Gulbay B, Sen E, Akkoca Yildiz O, Saryal S, Acican T, Karabiyikoglu G (2007). “Analysis of the factors related to mortality in patients with bronchiectasis”. Respir Med. 101 (7): 1390–97. PMID 17374480.
- ↑ Onen ZP, Eris Gulbay B, Sen E, Akkoca Yildiz O, Saryal S, Acican T, Karabiyikoglu G (2007). “Analysis of the factors related to mortality in patients with bronchiectasis”. Respir Med. 101 (7): 1390–97. PMID 17374480.
- ↑ Onen ZP, Eris Gulbay B, Sen E, Akkoca Yildiz O, Saryal S, Acican T, Karabiyikoglu G (2007). “Analysis of the factors related to mortality in patients with bronchiectasis”. Respir Med. 101 (7): 1390–97. PMID 17374480.
- ↑ Onen ZP, Eris Gulbay B, Sen E, Akkoca Yildiz O, Saryal S, Acican T, Karabiyikoglu G (2007). “Analysis of the factors related to mortality in patients with bronchiectasis”. Respir Med. 101 (7): 1390–97. PMID 17374480.
- ↑ Onen ZP, Eris Gulbay B, Sen E, Akkoca Yildiz O, Saryal S, Acican T, Karabiyikoglu G (2007). “Analysis of the factors related to mortality in patients with bronchiectasis”. Respir Med. 101 (7): 1390–97. PMID 17374480.
Diagnosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory Findings | Chest X Ray | CT | Other Imaging Findings | Other Diagnostic Studies
Treatment
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Looking for the patient version?
© 2026 MyEClinic – IFTM Institut für Telematik in der Medizin GmbH